Back to Journals » Cancer Management and Research » Volume 13
The Participatory Approach: A Specific French Organizational Model at the Department Level to Serve the Quality of Work Life of Healthcare Providers and the Quality of Care in Pediatric Oncology
Authors Lejeune J, Fouquereau E ![]() , Chênevert D, Coillot H, Chevalier S, Gillet N, Michon JM, Gandemer V, Colombat P
, Chênevert D, Coillot H, Chevalier S, Gillet N, Michon JM, Gandemer V, Colombat P ![]()
Received 6 November 2020
Accepted for publication 19 January 2021
Published 25 March 2021 Volume 2021:13 Pages 2763—2771
DOI https://doi.org/10.2147/CMAR.S284439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Julien Lejeune,1 Evelyne Fouquereau,2 Denis Chênevert,3 Helene Coillot,2 Severine Chevalier,2 Nicolas Gillet,2 Jean M Michon,4 Virginie Gandemer,5 Philippe Colombat2
1Service d’Onco-Hématologie Pédiatrique, Hôpital Clocheville, Tours, France; 2Qualipsy EE 1901, Université de Tours, Tours, France; 3Ecole des Hautes Etudes Commerciales, Montréal, Canada; 4Département de Pédiatrie, Institut Curie, Paris, France; 5Service d’Onco-Hématologie Pédiatrique, CHU Hôpital Sud, Rennes, France
Correspondence: Philippe Colombat Tel +33 0 2 47 4747 51
Email [email protected]
Background: Care providers ‘psychological health at work is an important issue because it directly affects the quality of patient care. So far, few studies have studied the psychological health at work of care providers in paediatric oncology. The participatory approach (PA) is an innovative organizational model of department specific to France and previously associated with quality of work life (QWL) and job performance. The aim of the present study was to explore the relationships between the participatory approach, care providers’ QWL and quality of care of children in pediatric oncology departments in France.
Methods: A multicentre survey was carried out in pediatric cancer units in France. Care providers completed a questionnaire assessing PA, QWL, consequences of QWL, and their perception of quality of care. The children or their parents completed a questionnaire assessing their perception of quality of care.
Results: Five hundred and ten healthcare professionals working in French pediatric oncology centres (more than 40% of the healthcare staff in paediatric oncology in France), 142 children and 298 parents responded to the survey. PA was associated with the care providers’ QWL (β = 0.274; p < 0.001), work engagement (β = 0.167; p< 0.001), job satisfaction (β = 0.166; p< 0.001) and perception of quality of care (β = 0.236; p< 0.001). PA was also related to patients’ perception of quality of care notably regarding quality of communication (β = 0.161; p< 0.001) and information (β = 0.226; p< 0.001).
Conclusion: PA is an innovative organizational model that appears to play a role in all aspects of healthcare providers’ QWL, and in the quality of care perceived by both care providers and patients.
Keywords: quality of work life, quality of care, organization, management, pediatric oncology
Introduction
The quality of work life (QWL) of healthcare providers is an important issue because it directly affects the quality of patient care.1–3 Psychological health at work can be defined with negative markers as burnout or positive markers as well-being. However, most of the research on QWL of healthcare providers in the last twenty years studied exclusively negative markers. For example, in this area, some authors underlined levels of burnout ranging from 40 to 70% depending on the profession and the specialty.1 Other studies in the USA indicate that the prevalence of professional burnout among physicians rose from 37.6% in 2011 to 52.5% in 2014, which is 36% higher than among the general population.4
It is important to note that the absence of professional burnout is not necessarily synonymous with well-being and quality of work life (QWL). In other words, endeavouring to reduce the level of professional burnout among care staff is clearly essential, but insufficient to create a healthy work environment.5 Studies suggest that QWL affects individual performance and organizational efficiency by acting on factors such as job satisfaction.6 A number of factors related to management (i.e., perceived autonomy support, transformational leadership) and the organization (i.e., perceived organizational support, organizational justice) have emerged as major determinants of care providers’ QWL,5 and the quality of care.7 These factors have mainly been investigated in studies of Magnet hospitals.8 These are hospitals that have developed an organizational and managerial model that attracts and retains nurses. The main factors highlighted by care providers in these hospitals are autonomy in work, the support of their organization, inter-disciplinary collaboration, and good relationships among care staff. Together, these lead to a better quality of life, a stronger commitment to work, and reduced absenteeism and turnover.9 Published studies also report improvements in the quality of care evaluated by the patients and lower levels of mortality.10
In France, the participatory approach (PA) is a specific French model of department organization that has been recognized by the Ministry of Health,11 and whose objective is to improve the management of patients in palliative care by reducing the suffering of caregivers. The participatory approach is based on two major lines of action: enhancing team communication and implementing a project approach. Communication is developed through various tools (multi-professional team meetings, in-service training, team support meetings, management meetings). Multi-professional team meetings bring together all the health providers working in the department to discuss the overall management of patients. In-service training ensures that all members of the care team (physicians, nurses, nursing assistants, etc.) receive comparable and consistent training; it provides opportunities for the team members to talk about their experiences, particularly for those who do not often express themselves. It also promotes inter-professional relations as part of team building. Team support meetings, led by a psychotherapist, are set up to debrief care staff in crisis situations. The project approach involves identifying a problem or a need, and setting up multi-professional working groups to put forward and discuss ways of dealing with it. In France, according to the law, PA has been compulsory for all in-patients (i.e., in all departments where patients die) and domiciliary services for patients in palliative care since 2004 and is a key accreditation factor for healthcare establishments. Studies to date suggest that this organizational model is positively linked to caregivers’ QWL, job satisfaction, commitment to the organization, and also to work performance.12,13
Paediatric oncology clearly has specific challenges for care providers, with stress factors linked to looking after sick children with often life-threatening diseases: risk of identifying with parents, guilt about treatment-related problems, difficult relationships with parents, end-of-life care.14–18 The organization of care in paediatric oncology also differs from adult specialities, due to the unique situation of each child and the relationship of staff with parents. This requires the organization of regular case conferences with all the care providers, the involvement of a psychologist and social worker for each child, school support, the involvement of a special needs’ teacher or other specialist support professionals or volunteers.
The present research focuses on factors determining psychological health. More specifically, its aim is to evaluate the impact of PA on QWL of caregivers and quality of patient care in paediatric oncology in France. Studying this link is of paramount importance in order to understand the managerial and organizational factors underlying the quality of care delivered to children with cancer, and hence to improve their quality of life and the quality of their care. To the best of our knowledge, this is the first study worldwide to examine how certain managerial and organizational factors affect the QWL of care providers and the quality of care of children in paediatric oncology, based on a very large sample.
Materials and Methods
Study Design
With the agreement of the French Society of Paediatric Oncology (Société Française de lutte contre les Cancers et les leucémies de l’Enfant et de l’adolescent), 30 specialized paediatric cancer centres in France were contacted. Of these, 25 agreed to participate in the study. They were sent two questionnaires: one to be completed by the healthcare providers, and one to be completed by children aged 12 and over or by the parents of children under 12 years of age. A contact person was identified in each centre, generally the nurse manager, who distributed the paper questionnaires to members of the healthcare team and to patients. These questionnaires were returned anonymously in a sealed envelope. For patients, the questionnaires were distributed the day of discharge or the day before discharge. Anonymous questionnaires have not to be signed in France and informed consent for parents was included at the top of each questionnaire. The study was approved by the local research ethics committee (Agreement number 2014/011 of 21 November 2014 of Ethics Committee in Human Research of Region Centre in Tours) and was conducted in accordance with the Declaration of Helsinki.
Participants
Healthcare providers who participated voluntarily in the study included physicians, nurse managers, nurses and allied health professionals (nurse assistant, dietician, psychologist, etc.). Patients were children hospitalized in a French paediatric cancer centre for more than 48 hours for cancer treatment (hematologic malignancies and solid tumours). Exclusion criteria were parents or children who refused to participate in the study, hospitalization of less than 48 hours or for the first time, insufficient French language skills, severe psychological symptom burden.
Measures
All the scales used in our study are validated tools whose psychometric qualities have been attested in previous studies.
The questionnaire completed by healthcare providers included the assessment of:
- A range of demographic and job-related variables including age, gender, professional discipline, length of time working in oncology.
QWL
The four dimensions of QWL (psychological (β=0.86), physical (β=0.87), social (β=0.83), and cultural (β=0.88)) were measured using the sixteen-item French version of Elizur and Shye’s scale.19 A sample item: “To what extent does your work allow you to keep a good balance between your personal qualities and current working conditions?”.
Management Determinants of QWL
(i) Transformational leadership (defined as a type of management involving inspirational motivation, individualized consideration of each employee, and encouragement to work together). Seven items taken from the Global Transformational Leadership scale,20 were used to assess care providers’ perceptions of transformational leadership (e.g., “My health manager instils pride and respect for others and inspires me by being highly competent”). Responses were made on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree) (β=0.96).
(ii) Perceived autonomy support (defined as care providers’ perceptions of supervisor autonomy support) was assessed with the French version of the scale used by Moreau and Mageau.21 This is a nine-item self-report questionnaire assessing the extent to which employees perceive their supervisor to be autonomy-supportive (e.g., “My health manager often gives me opportunities to take decisions in my work”). Answers were given on a 7-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree) (β=0.94).
Organizational Determinants of QWL
(i) Perceived organizational support (i.e., care providers’ beliefs concerning the extent to which the organization values their contributions and cares about their well-being) was measured with an eight-item version of the Perceived Organizational Support Scale developed by Rhoades and Eisenberger,22 (e.g., “In my department, people will help me if I have a problem”). A higher score reflects a higher level of perceived organizational support (β=0.82).
(ii) Organizational justice (defined as the perception of the treatment an individual receives in the workplace) was assessed using the justice scale developed by Niehoff and Moorman,23 which consists of five items measuring perceptions of distributive justice (e.g., “My work schedule is fair”) and 9 items measuring perceptions of interactional justice (eg, “When decisions are made about my job, the head nurse treats me with kindness and consideration”). Items were rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree)(β=0.93).
PA
PA was evaluated with six items measuring the four components described by Pronost et al:12 multi-professional meetings, in-house training, team support, and a project approach. Multi-professional meetings were evaluated with one item (“Is there a lack of multidisciplinary team meetings?”). Responses were made on a 4-point Likert scale from 1 (very often) to 4 (rarely). In-house training was evaluated with two items (e.g., “Is it possible to attend training courses related to pain in your department?”). Responses were made on a 4-point Likert scale from 1 (“No, it’s impossible”) to 4 (“Yes, very easily”). Team support was measured with one item (“Do you have support group sessions in your department?”), rated on a 4-point Likert scale, from 1 (“No, never) to 4 (“Yes, very regularly”). The project approach was evaluated with two items (e.g., “Do you know the exact content of the department’s project?”), rated on a 4-point Likert scale from 1 (“No, not at all”) to 4 (“Yes, very well”). An overall score for the participatory approach was calculated by averaging the scores of the four components.
Consequences of QWL
(i) Work engagement was measured using the nine-item version of the Utrecht Work Engagement Scale,24 tapping three dimensions, namely vigour (3 items, e.g., “At my work, I feel bursting with energy”), dedication (3 items, e.g., “I am enthusiastic about my job”), and absorption (3 items, e.g., “I am immersed in my work”). Responses were given on a Likert scale ranging from 1 (“never”) to 7 (“always”). To reduce the number of variables, a global score was computed, with higher scores being indicative of a higher level of work engagement (β=0.92).
(ii) Job satisfaction (defined as “a pleasurable or positive emotional state resulting from the appraisal of one’s job or job experiences”)25 was evaluated with a single item (“In your current job, are you satisfied?”) rated on a Likert scale ranging from 1 (“very unsatisfied”) to 5 (“very satisfied”).
(iii) The quality of care perceived by the team was measured with a single item (“Are you satisfied with the quality of care given to patients?”) rated on a 5-point Likert scale.
The questionnaire completed by patients included the assessment of:
- Quality of care: We used the questionnaire validated by SAPHORA-MCO,26 to evaluate different dimensions of children’s satisfaction with the quality of their care: overall quality of care (5 items), medical information (6 items, e.g., “nurses were attentive, listening to my problems”), relationship with the care staff (5 items), and attitude of the health professionals (5 items). Since 2011, the Ministry of Health has sent this questionnaire to all health establishments in France. Here, we report its first use in a paediatric population. The questionnaire was completed by children aged 12 and over or by the parents of children under 12 years of age. This age limit was based on the children’s ability to complete the tool and reading level and was approved by the ethics committee. However, due to the large number of outliers in the questionnaires completed by the children, we only retained the questionnaires completed by the parents. For the purposes of the study, we averaged the scores for each dimension to obtain an overall score of satisfaction with the care received (β=0.89).
Analysis
Data were analyzed using SPSS 25 statistical software. Simple regression analyses were conducted for all analyses. First, the relationships between PA (global and specific dimensions) and the caregivers’ quality of life at work and its consequences were analysed. Secondly, we focused on the link between PA and the parents and children’s satisfaction with quality of care. As it was impossible to match the data of specific caregivers and patients because each caregiver looks after several patients in the same unit, patient data were aggregated at the centre level and integrated into the caregiver database using correspondences between oncology centres. Simple regression analyses were then conducted. Thirdly, we examined the relationships between other organizational/managerial factors, caregivers’ QWL and its consequences. Finally, we studied the relationships between PA and these organizational/managerial factors.
Results
Participants
Participants were 510 healthcare professionals working in French paediatric oncology centres (i.e., more than 40% of the healthcare staff in paediatric oncology in France). They included physicians (n = 64), nurses (n = 261) and allied health staff (n = 185) (Table 1).
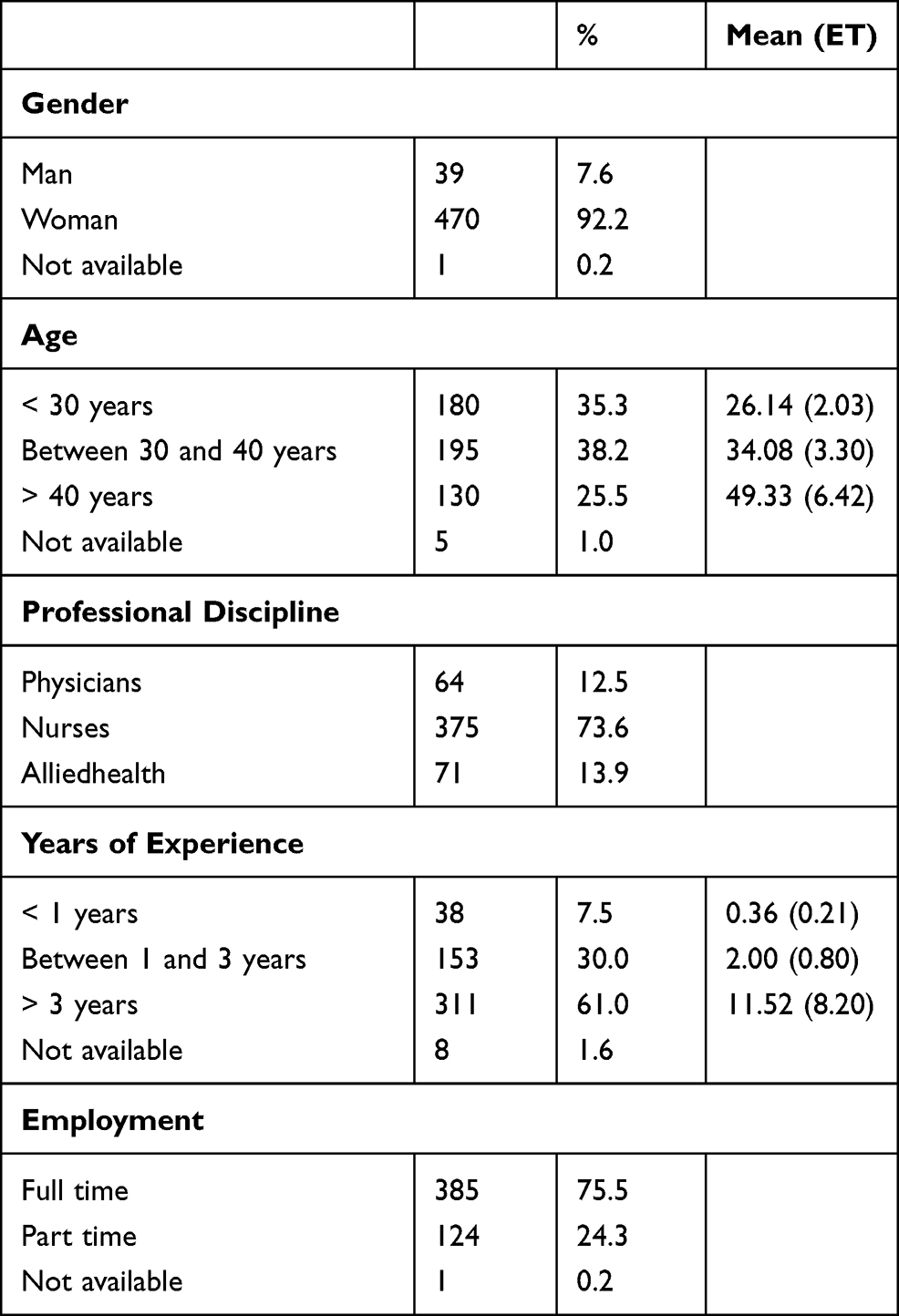 |
Table 1 Demographic and Job-Related Variable of Healthcare Providers |
A total of 142 children and 298 parents participated in this study. However, as previously detailed, we only retained the 298 questionnaires completed by the parents.
PA, QWL and Consequences of QWL
A significant relationship was observed between overall PA and care providers’ QWL, both in general (β = 0.274; p < 0.001) and at the psychological (β = 0.284; p < 0.001), social (β = 0.183; p < 0.001), cultural (β = 0.284; p < 0.001) and physical (β = 0.110; p < 0.05) levels of QWL (Table 2). More precisely, the four components of the participatory approach were also linked significantly and positively to overall QWL: in-house training (β= 0.159; p < 0.001), multi-professional team meetings (β= 0.204; p < 0.001), the project approach (β= 0.198; p < 0.001), and team support (β= 0.136; p < 0.01). PA also had a positive relationship with the care providers’ work engagement (β = 0.167; p < 0.001) and job satisfaction (β = 0.166; p < 0.001). Finally, PA had a significant and positive relationship with satisfaction with the quality of care assessed by care providers (β = 0.236; p < 0.001) (Table 2), particularly the “project approach” (β = 0.216; p < 0.001) and “multi-professional team meetings” (β = 0.196; p < 0.001).
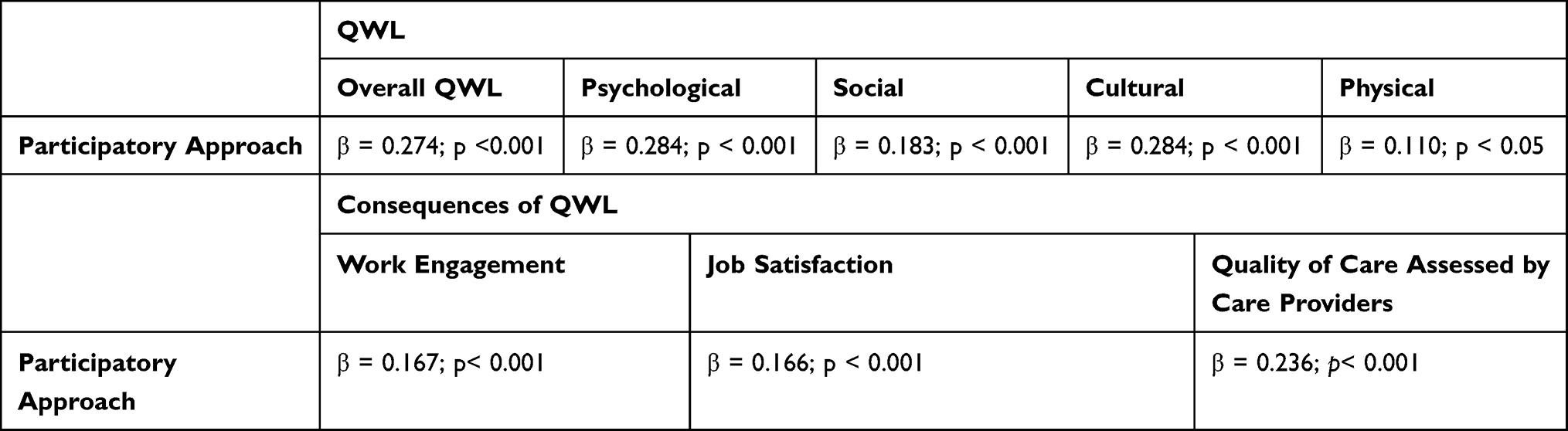 |
Table 2 Participatory Approach, QWL and Consequences of QWL (n = 510) |
PA and Quality of Care Perceived by Patients
As mentioned above, the SAPHORA-MCO questionnaires evaluating the quality of care were completed by the parents of children aged under 12, and by the children aged 12 and over. Due to the large number of outliers in the questionnaires completed by the children, we only retained the 298 questionnaires completed by the parents. Regarding the participatory approach, team support was positively linked to the quality of communication with the children and their families (β = 0.161; p < 0.005) and information (β = 0.226; p < 0.001), multi-professional team meetings to the attitude of the health professionals (β = 0.176; p < 0.005), and in-house training to the quality of communication with the children and their families (β = 0.136; p < 0.005).
Managerial/Organizational Factors, QWL and Quality of Care
As previously mentioned, many published studies have shown a link between QWL and certain managerial/organizational factors,6 but never in paediatric oncology. All factors studied were linked positively to overall QWL: perceived organizational support (β = 0.372; p < 0.001), transformational leadership (β = 0.245; p < 0.001), organizational justice (β = 0.367; p < 0.001), and perceived autonomy support (β = 0.298; p < 0.001). Moreover, these managerial and organizational factors were also related to QWL consequences: job satisfaction, work engagement and quality of care perceived by care providers (Table 3). Finally, these managerial/organizational factors were associated with quality of care perceived by parents. Transformational leadership was positively linked to the quality of communication (β = 0.209; p < 0.001); organizational justice to the quality of communication (β = 0.125; p < 0.005), information (β = 0.117; p <0.01), and to the attitude of the health professionals (β = 0.105; p < 0.02); perceived organizational support to communication (β = 0.145; p < 0.002), information (β = 0.108; p < 0.02), and to the attitude of the health professionals (β = 0.167; p < 0.001); and finally, perceived autonomy support to the quality of communication (β = 0.180; p < 0.001)
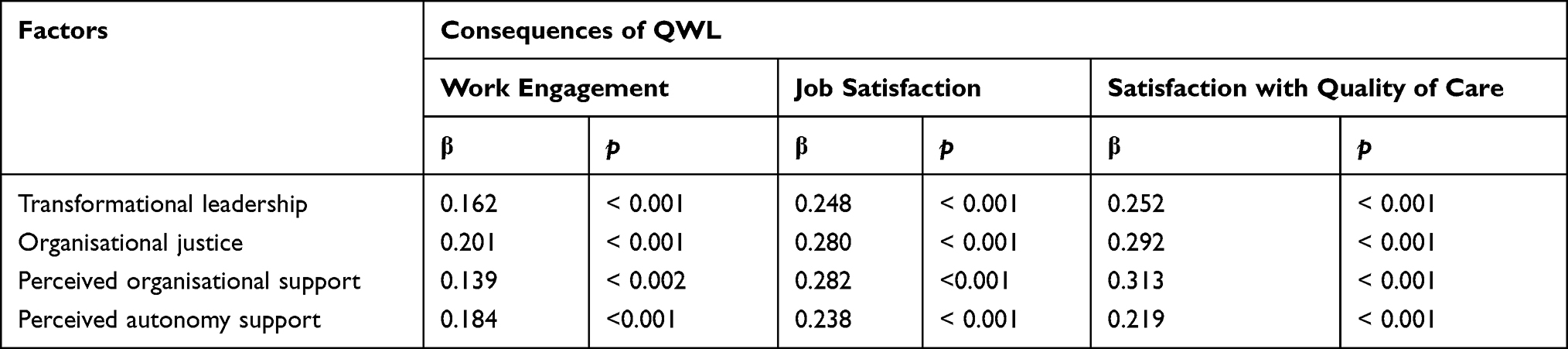 |
Table 3 QWL and Organizational/Managerial Factors Studied (n=510) |
PA and Managerial/Organizational Factors
We studied the links between the global participatory approach and the managerial and organizational factors selected in this study. The overall PA was positively linked to organizational and managerial factors: perceived organizational support (β = 0.414; p < 0.001), transformational leadership (β = 0.324; p< 0.001), organizational justice (β = 0.408; p < 0.001), and perceived autonomy support (β = 0.323; p < 0.001) (Table 4).
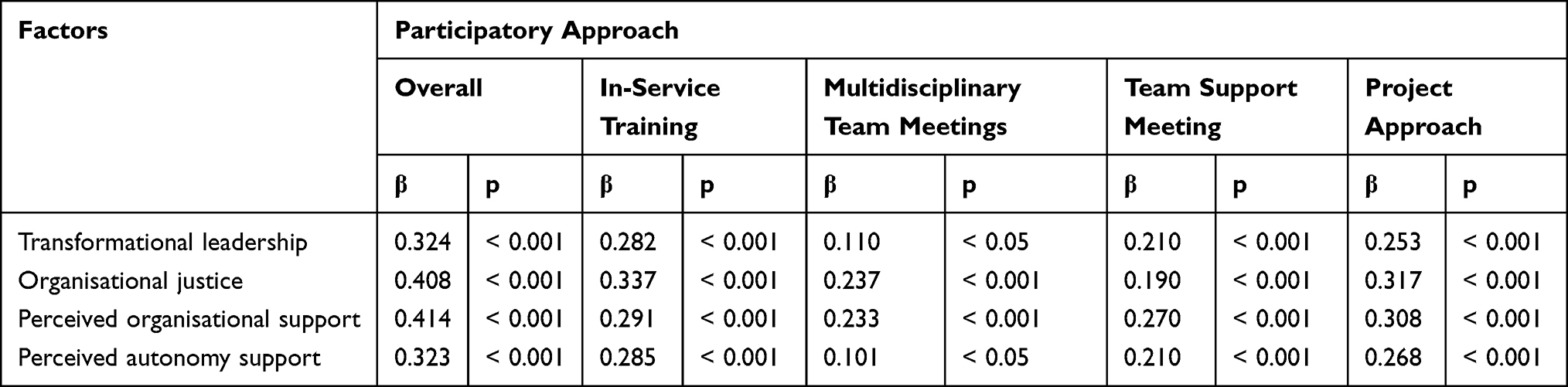 |
Table 4 Participatory Approach and Managerial/Organizational Factors (n=510) |
Discussion
This is the first study in paediatric oncology, based on a very large sample representing more than a third of healthcare providers in paediatric oncology in France, to examine the relationships between an innovative organizational model (Participatory Approach) on the one hand, and the caregivers’ quality of life at work and the quality of patient care (quality of communication, quality of information and satisfaction with the attitude of the care staff) on the other.
In 2009, Mukherjee et al18 carried out a meta-analysis of burnout, psychiatric disorders and stress related to working in paediatric oncology. They concluded that the literature was very inadequate and that further studies were required in order to make recommendations for managing these teams. Studies that have been published to date, generally involving small numbers of care providers, have highlighted the role of demographic and care-related factors in the rate of professional burnout among paediatric oncology staff.27–31
The only study to have examined the quality of care of children in the paediatric oncology sector carried out semi-directive interviews with 19 parents, 17 children and 16 paediatric oncologists.32 The results showed that the children and/or parents’ satisfaction with care was related to the friendliness and responsive nature of healthcare staff, communication, and professionals going beyond the call of duty to care for the children. On the other hand, they found that lack of continuity of care and language problems were associated with lower satisfaction.32 In contrast, our study is a quantitative study evaluating a much larger population.
Furthermore, our study investigated the relationships between certain organizational and managerial factors and both the care providers’ quality of work life and the quality of patient care. Very few studies33,34 have investigated the relationships between managerial or organizational factors and the patients’ perception of quality of care, except in the “Magnet” Facility Management Model. To our knowledge, no studies have been published investigating the impact of a comprehensive team organization model either on the quality of care assessed by patients or in the field of paediatric oncology.
Our findings demonstrate that overall PA and each of its four components (multi-professional team meetings, in-service training, team support and project approach) appear to play a role in all aspects of the healthcare providers’ QWL, and also in their work engagement, job satisfaction, and satisfaction with quality of care. Moreover, this specific organizational model also has an impact on the quality of care evaluated by the patients, an issue that has been discussed little, if at all, in the literature. For us, this model should be implemented for in-patients of all medical specialties, including those treating patients with chronic disease, rehabilitation, psychiatry, geriatrics or paediatrics.
PA comes within the framework of clinical governance, entailing joint team management, as well as strong participation of the nursing teams and other professionals.35,36 This model, providing the basis for discussion among health managers worldwide, and based on responsibility sharing by the care staff, should enable the organization to fulfil its role of delivering care and services to ensure the health and wellbeing of both patients and care providers. Joint management is indeed increasingly advocated in health care in order to successfully manage a collaborative activity. This new form of clinical governance introduces the idea of self-managed teams with a degree of autonomy but working interdependently with other units. A clinical director should be at the head of these teams, which should also function on the principle of cross-functional coordination processes operating throughout the organization. These initiatives provide ways of shifting from working “in silos” to cross-functional processes, focusing on flexibility and collaboration to improve the quality of care and services delivered in complex organizations such as paediatric oncology centres. Power-sharing and the collaborative action arising from clinical governance will lead to improvements in the quality of health care and services, by aligning the hierarchical levels of patient, care teams, the organization, and the system, and by coordinating their work.
Our findings also confirm and extend the results of a relatively abundant literature on the impact of certain managerial and organizational factors on the mental health of healthcare providers, namely transformational leadership,13 perceived organizational support,22 organizational justice,37 and perceived autonomy support,21 in the specific but little studied field of paediatric oncology.
Finally, another interesting finding of this study is the significant link between the organizational model of PA and the managerial and organizational characteristics of perceived organizational support, transformational leadership, organizational justice, and perceived autonomy support. This in turn raises a very important question: is it a particular type of manager that leads to this method of organization, or is it the method of organization that attracts this type of manager? Longitudinal studies are needed to investigate this issue.
To sum up, this research, which is the largest study investigating the links between organizational and managerial factors, caregivers’ QWL and quality of care in paediatric oncology demonstrates that PA is a very promising organizational model. The challenge is to successfully implement this model in the field of all chronic diseases, geriatrics, paediatrics and psychiatry in particular. The training front-line managers with a view to improving the QWL of the health professionals delivering care to patients appear essential.38
Acknowledgments
We would like to thank all the centres of the Société Française de lutte contre les Cancers et les leucémies de l’Enfant et de l’adolescent who participated in this study: Amiens (CDevoldere, C Douadi), Angers (I Pellier, S Mareni), Besançon (N Cheikh, K Ancelin-Chauvin), Bordeaux (Y Perel, S Sangare), Brest (LCarausu, B de Lapasse), Caen (O Minckes, C Langlois), Clermont-Ferrand (J Kanold, M Gaudio), Dijon (G Couillault, A Latroyes), Grenoble (D Plantaz, F Maxit), Lille CHU (W Abouchalah, C Letout), Limoges (C Piguet, H Nomme), Lyon (Y Bertrand, A Famery), Marseille (G Michel, M Guiraud), Nancy (C Chastagner, MC Mirouf), Nantes (C Thomas, K Roux), Nice (C Soler, P Cozzi), Poitiers (F Millot, R Grollier), Reims (C Pluchart, L Lefort), Rennes (V Gandemer, M Boishu), Rouen (JP Vannier, O Dupray), Strasbourg (P Lutz, F Meyer), Toulouse (I Bertozzi-Salamon, ML Leygues), Tours (P Blouin, S Panneau), IGR Villejuif (D Valteau-Couannet, P Usubelli), Trousseau Paris (G Leverger, V Tanguy), Curie Paris (J Michon, AG Briand).We would also like to thank the national “Qualité de vie et cancer” platform and Cancéropôle Grand-Ouest.
Funding
This study was supported by the Fondation de France and CANCEN.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yates M, Samuel V. Burnout in oncologists and associated factors: a systematic literature review and meta-analysis. Eur J Cancer Care. 2019;28(3):13094. doi:10.1111/ecc.13094
2. Dewa CS, Loong D, Bonato S, Trojanowski L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open. 2017;7:e015141. doi:10.1136/bmjopen-2016-015141
3. Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB. Healthcare staff, wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016;11(7):e0159015. doi:10.1371/journal.pone.0159015
4. Schrijvers I. Pathology in the medical profession. Taking the pulse of physician wellness and burnout. Arch Pathol Lab Med. 2016;140(9):976–982. doi:10.5858/arpa.2015-0524-RA
5. Jaspaerse M, Herst P, Dungey G. Evaluating stress, burnout and job satisfaction in New Zealand radiation oncology department. Eur J Cancer Care. 2014;23:83–88. doi:10.1111/ecc.12098
6. Maleki F, Hasanmoradi N. Studying the relationship between quality of work-life and efficiency of employees. Int J Econ Perspect. 2017;11(1):979–987.
7. Vahey DC, Aiken LH, Sloane DM, Clarke SP, Vargas D. Nurse burnout and patient satisfaction. Med Care. 2014;42(Suppl):II57–II66. doi:10.1097/01.mlr.0000109126.50398.5a
8. Petit Dit Dariel O, Regnaux JP. Do Magnet®-accredited hospitals show improvements in nurse and patient outcomes compared to non-Magnet hospitals: a systematic review. JBI Database System Rev Implement Rep. 2015;13(6):168–219. doi:10.11124/jbisrir-2015-2262
9. Warren N, Hodgson M, Craig L, Dyrenforth S, Perlin J, Murphy F. Employee working conditions and healthcare system performance: the veterans health administration experience. J Occup Environ Med. 2017;4:417–429. doi:10.1097/JOM.0b013e31803b94ce
10. McHugh MD, Kelly LA, Smith HL, Wu ES, Vanak JM, Aiken LH. Lower mortality in magnet hospitals. Med Care. 2013;51(5):382–388. doi:10.1097/MLR.0b013e3182726cc5
11. Haute Autorité de Santé. Critère de certification 13a de la V3 2010. Prise en charge et droits des patients en fin de vie. Manuel de certification des établissements de santé. 2010. Available from: https://www.has-sante.fr/upload/docs/application/pdf/2014-03/manuel_v2010_janvier2014.pdf.
12. Pronost AM, Le Gouge A, Leboul D, et al. Relationship between the characteristics of onco-haematology services providing palliative care and the socio-demographic characteristics of caregivers using health indicators: social support, perceived stress, coping strategies, quality of work life. Support Care Cancer. 2012;3:607–614. doi:10.1007/s00520-011-1139-3
13. Gillet N, Fouquereau E, Bonnaud-Antignac A, Mokounkolo R, Colombat P. The mediating role of organizational justice in the relationship between transformational leadership and nurses’ quality of work life: a cross-sectional questionnaire survey. Int J Nurs Stud. 2013;10:1359–1367. doi:10.1016//j.ijnurstu.2012.12.012
14. Whitford B, Nadel AL, Fish JD. Burnout in pediatric hematology/oncology-time to address the elephant by name. Pediatr Blood Cancer. 2018;65(10):e27244. doi:10.1002/pbc.27244
15. Granek L, Bartels U, Scheinemann K, Labrecque M, Barrera M. Grief reactions and impact of patient death on pediatric oncologists. Pediatr Blood Cancer. 2015;62(1):134–142. doi:10.1002/pbc.25228
16. Bowden MJ, Mukherjee S, Williams LK, De Graves S, Jackson M, McCarthy MC. Work-related stress and reward: an Australian study of multidisciplinary pediatric oncology healthcare providers. Psycho-Oncology. 2015;24(11):1432–1438. doi:10.1002/pon.3810
17. Klassen A, Gulati S, Dix D. Health care provider’s perspectives about working with parents of children with cancer: a qualitative study. J Pediatr Oncol Nurs. 2012;29(2):92–97. doi:10.1177/1043454212438405
18. Mukherjee S, Beresford B, Glaser A, Sloper P. Burnout, psychiatric morbidity, and work-related sources of stress in paediatric oncology staff: a review of the literature. Psycho Oncol. 2009;18:1019–1028. doi:10.1002/pon.1534
19. Elizur D, Shye S. Quality of work and its relation to quality of life. Appl Psychol. 1990;3:275–291. doi:10.1111/j.1464-0597.1990.tb01054.x
20. Carless SA, Wearing AJ, Mann LA. A short measure of transformational leadership. J Bus Psychol. 2000;14(3):389–405. doi:10.1023/A:1022991115523
21. Moreau E, Mageau GA. The importance of perceived autonomy support for the psychological health and work satisfaction of health professionals; not only supervisors count, colleagues too! Motiv Emot. 2012;36(3):268–286. doi:10.1007/s11031-011-9250-9
22. Rhoades L, Eisenberger R. Perceived organizational support: a review of the literature. J Appl Psychol. 2002;87:698–714. doi:10.1037/0021-9010.87.4.698
23. Niehoff BP, Moorman RH. Justice as a mediator of the relation- ship between methods of monitoring and organizational citizenship behaviour. Acad Manage J. 1993;36(3):527–556. doi:10.5465/256591
24. Schaufeli W, Bakker A. Utrecht work engagement scale: preliminary manual, Utrecht: occupational Health Psychology Unit. Utrecht University; 2003. Available from: http://www.schaufeli.com.
25. Locke EA. The Nature and Causes of Satisfaction. Handbook of Industrial and Organizational Psychology. Chicago: Rand McNally; 1976:1297–1349.
26. Salomon L, Gasquet I, Mesbah M, Ravaud P. Construction of a scale measuring patient’s opinion on quality. Int J Qual Health Care. 1999;6:507–527. doi:10.1093/intghc/11.6.507
27. Sekol MA, Kim SC. Job satisfaction, burnout and stress among pediatric nurses in various specialty units as an acute care hospital. J Nurs Educ Pract. 2014;4:115–124. doi:10.5430/jnep.v4n12p115
28. Zanatta AB, de Lucca SR. Prevalence of burnout syndrome in health professionals of an onco-hematological pediatric hospital. Rev Esc Enferm USP. 2015;49(2):253–260. doi:10.1590/S0080-623420150000200010
29. Davis S, Lind BK, Sorensen C. A comparison of burnout among oncology nurses working in adult and pediatric inpatient and outpatient settings. Oncol Nurs Forum. 2013;40:303–311. doi:10.1188/13.ONF.E303-E311
30. Liakopoulou M, Panaretaki I, Papadakis V, et al. Burnout, staff support, and coping in pediatric oncology. Support Care Cancer. 2008;16(2):143–150. doi:10.1007/s00520-007-0297-9
31. Roth M, Morrone K, Moody K, et al. Career burnout among pediatric oncologists. Pediatr Blood Cancer. 2011;57(7):1168–1173. doi:10.1002/pbc.23121
32. Wangmo T, Ruhe KM, Badarau DO, Kühne T, Niggli F, Elger BS. Parents’ and patients’ experiences with paediatric oncology care in Switzerland–satisfaction and some hurdles. Swiss Med Wkly. 2016;146:w14309. doi:10.4414/smw.2016.14309
33. Flood AB. The impact of organizational and managerial factors on the quality of care in health care organizations. Med Care Rev. 1994;51(4):381–428. doi:10.1177/107755879405100402
34. Mosadeghrad AM. Factors influencing healthcare service quality. Int J Health Policy Manag. 2014;3(2):77–89. doi:10.15171/ijhpm.2014.65
35. Gesme DH, Towle EL, Wiseman M. Essentials of staff development and why you should care. J Oncol Pract. 2010;6(2):104–106. doi:10.1200/JOP.091089
36. Rosen MA, Diaz Granados D, Dietz AS, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;73(4):433–450. doi:10.1037/amp0000298
37. Gillet N, Colombat P, Michinov E, Pronost AM, Fouquereau E. Procedural justice, supervisor autonomy support, work satisfaction, organizational identification and job performance: the mediating role of need satisfaction and perceived organizational support. J Adv Nurs. 2013;11:2560–2571. doi:10.1111/jan.12144
38. Bass BM. The future of leadership in learning organizations. J Leadersh Stud. 2000;7(i3):18–40. doi:10.1177/107179190000700302
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.