")
Back to Journals » Clinical Interventions in Aging » Volume 18
The PAPA Questionnaire: Assessment of Long-Term Engagement in Activities, with Separate Quantification of Their Physical, Cognitive, and Social Components
Authors Loggia G , Pellichero A, Moutoussamy I, Morello R, Pothier K, Chavoix C
Received 18 June 2022
Accepted for publication 6 December 2022
Published 2 March 2023 Volume 2023:18 Pages 327—341
DOI https://doi.org/10.2147/CIA.S377917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Gilles Loggia,1,2 Alice Pellichero,3 Ilona Moutoussamy,4,5 Rémy Morello,6 Kristell Pothier,1,4 Chantal Chavoix1
1COMETE, Normandie Univ, UNICAEN, INSERM, Caen, 14000, France; 2Department of Geriatrics, Normandie Univ, UNICAEN, CHU de Caen Normandie, Caen, 14000, France; 3Centre for Interdisciplinary Research in Rehabilitation and Social Integration (Cirris), Centre Intégré Universitaire de Santé et de Services Sociaux de la Capitale-Nationale (CIUSSS-CN), Quebec City, QC, G1M 2S8, Canada; 4EA 2114, Psychologie des Âges de la Vie et Adaptation, University of Tours, Tours, 37000, France; 5UMR CNRS 7295, Centre de Recherche sur la Cognition et l’Apprentissage, University of Tours and University of Poitiers, Tours, 37000, France; 6Department of Statistics and Clinical Research, Normandie Univ, UNICAEN, CHU de Caen Normandie, Caen, 14000, France
Correspondence: Gilles Loggia, INSERM-UniCaen U1075, COMETE, PFRS, 3 rue des Rochambelles, Caen, Cedex, 140320, France, Tel +33 2 31 06 82 14, Fax +33 2 31 06 82 19, Email [email protected]
Purpose: Engagement in activities promotes healthy living. Evaluating it is a challenging issue. Assessing engagement in activities while differentiating the physical, cognitive, and social component of each activity and taking into account the intensity level involved in each of the three components would be very relevant. Since none of the currently available cognitive reserve and questionnaires on the activities practiced takes into consideration both points, the purpose of this new questionnaire, called Pertinent Activities Practice in Adults (PAPA) questionnaire, is to fill these gaps.
Patients and Methods: The questionnaire was developed through a literature review and interviews with older adults (n=177 ≥ 55 years). The intensity level of each item (none, light, moderate, or high) was determined by the compendium of physical activities for the physical component and consensus for the cognitive and social components, then validated by 56 professional experts (6 groups: physiotherapists, neuropsychologists, occupational therapists, geriatricians, etc.).
Results: The PAPA questionnaire includes 75 items that give rise to 4 scores (sedentary lifestyle and physical, cognitive, and social activity scores) weighted by the frequency, duration, and intensity level for each component. The weighted percentage of agreement of the expert groups for the intensity levels was never significantly lower than the minimum target threshold (80% of the hypothetical median) except in a single domain (cognitive) for an expert group non-specialized in cognition. Cronbach’s alpha was ≥ 0.85.
Conclusion: This questionnaire, which assesses long-term engagement in activities, with separate quantification of the physical, cognitive, and social components of a wide range of activities, should help guide actions to promote healthy aging and reduce dementia risk.
Keywords: sedentary behavior, physical activity, social participation, intellectual activity, cognitive reserve, evaluation
Introduction
The concept of cognitive reserve (CR) suggests that lifetime enrichment helps to cope with brain damage.1 Various factors such as education, professional occupation, social participation, physical activity, and engagement in leisure activities have been shown to be associated with a decreased risk of dementia. They also have been shown to prolong healthy aging.1–4
With these proxy indicators, several measures have been developed and are now used to assess CR, such as the Cognitive Reserve Index questionnaire (CRIq),5 the Lifetime of Experiences Questionnaire (LEQ),6 or the Cognitive Reserve Scale (CRS).7 Although several of them are promising tools for measuring CR, they mainly focus on cognitively stimulating activities but only to a lesser degree on social participation and even less so on physical activity. Yet, regular engagement in several domains, namely in the physical, cognitive, and social domains, are known to develop CR, preserve neuronal structural integrity, and reduce the risk of dementia.2–4,8
There are also questionnaires that target one of these three domains but whose purpose is not to assess CR, in particular physical activity questionnaires. Physical activity questionnaires are currently very useful for monitoring physical activity levels in various populations. The high-quality physical activity questionnaires,9 such as the Physical Activity and Sedentary Behaviour Questionnaire (PASB-Q),10 Physical Activity Scale for the Elderly (PASE),11 International Physical Activity Questionnaire-Short Form (IPAQ-SF),12 and Community Healthy Activities Model Program for Seniors (CHAMPS)13 give rise to a score weighted by the frequency, duration, and intensity level of the physical activity. This notion of intensity, which is not taken into account in the CR questionnaires, is important because it conditions health status. For instance, the World Health Organization (WHO) recommends adults to do at least 150 minutes of moderate-intensity aerobic physical activity or 75 minutes of vigorous-intensity aerobic physical activity each week.14 It is also well-known that sedentary behavior increases the risk of dementia,15 chronic disease and premature mortality,16,17 and is associated with brain atrophy.18 The intensity level of physical activity can be easily determined using the physical activity compendium19 which classifies numerous activities into 21 categories (for example, sports, domestic activities, home repair, work occupation, transport, etc.) by energy expenditure rate, providing a Metabolic Equivalent of Task (MET) intensity level for each activity. The physical activity questionnaires only quantify physical activity whereas the activities questioned are usually multimodal, thus also involving a cognitive or social component. This applies for both sports and non-sports activities (for instance, tennis, dancing, home housework, and gardening). In addition, they most often target no more than the last 7 days (for example, PASE, and IPAQ-SF) which therefore cannot reflect activities over several years. A few questionnaires assessing physical activity over a lifetime have, however, also been developed.20–22
In the social domain, to our knowledge there is no such questionnaire, and classification of the social activities into several intensity levels does not exist. A few studies have used their own tools based on some specific social aspects (for example, social network size or frequency of social activities in the last 12 months or 6 years).4 More recently, social participation has been assessed based on the frequency of participation in 8 social activities, and further categorized into three categories according to the number of activities lasting at least one hour. The same holds true in the cognitive domain. Various authors have assessed intellectual activities based on participation in a few items without taking into account the intensity level of the activities (for example, Helzner et al23). Only Wilson and collaborators24 estimated both the frequency and intensity of cognitive activity involved in 7 basic activities, on a 5-point scale, in which 3 involved reading (reading newspapers; reading magazines; reading books).
To our knowledge, no questionnaire has been created that assesses engagement in the three activity domains (physical, cognitive, and social). Such a questionnaire should help to measure the various activity domains in which a person is regularly engaged, while the other proxy indicators of CR (education, professional occupation) can easily be obtained through simple and standardized questions. In addition, being able to distinguish the level of engagement in each activity domain could be useful for gaining knowledge on the specific role of each domain and their combined involvement in CR and in the preservation of neuronal integrity, particularly from a health and prevention perspective. Furthermore, since most activities are multimodal (for instance, going to the museum with friends involved physical, cognitive, and social engagement), it would be relevant, for each activity, to have scores for each of these three components, which has not been done until now.
There is thus a need for a questionnaire that separately assesses the physical, cognitive, and social components of the various activities a person can be engaged in, and in a similar way for each component, in particular by applying a weighting factor according to the intensity level for each component of each activity.
The purpose of the present study was to develop a questionnaire, called Pertinent Activities Practice in Adults (PAPA), measuring the engagement, over the past years, in a wide range of activities, focusing on the physical, cognitive, and social components of each activity. To this aim, special attention was paid to the determination of the intensity level of each of the three components. This questionnaire mainly targets activities that older adults engage in since this population is the most likely to be the target of preventive strategies.
Materials and Methods
In order to best assess pertinent activities that adults can be engaged in, - in the physical, cognitive, and social domains -, the elements of the constructs were identified as follows: i) wide selection of items, representative of the main categories of activities practiced in adulthood; ii) consideration of the physical, cognitive, and social components involved in each item; iii) consideration of three parameters for each item: frequency, duration, and intensity level while taking into account putative recent withdrawn from a regularly practiced activity in the past years; and iv) obtaining 4 scores based on the combination of the three above parameters: two in the physical component (sedentary behavior and physical activity) and one in each of the other two components (cognitive and social). A weighting procedure was applied for each three parameters of interest to compensate for the heterogeneity of the items.
The methodology used to develop the PAPA questionnaire is presented below in two parts: 1) content and development of the questionnaire with the help of interviews with older adults, and 2) assessment and determination of the intensity level of each of the three components (physical, cognitive and social) involved in each item by professional experts. An overview of the study procedures is presented in Figure 1. To meet the requirements of high-quality studies on questionnaires, we used an assessment of content validity and standards for study design and evaluation (for example, Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) checklists).25
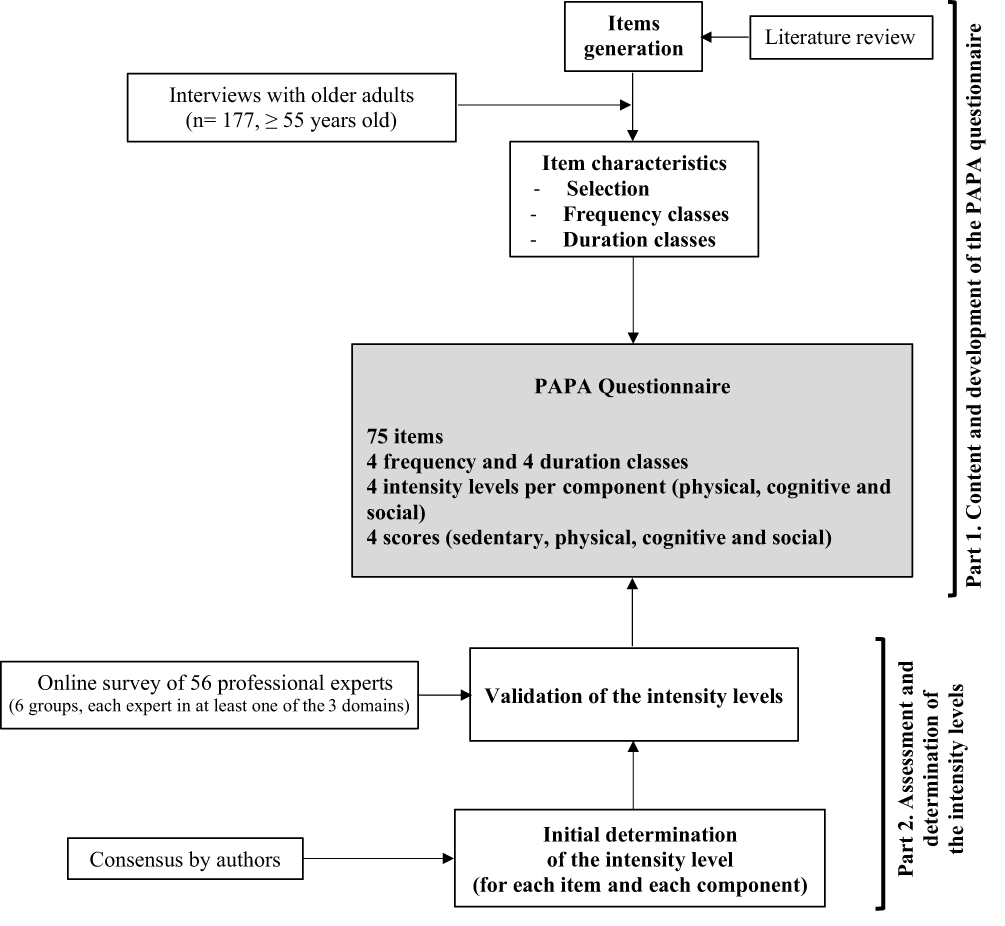 |
Figure 1 Overview of the study procedures. This figure gives an overview of the development process of the papa questionnaire, from the items generation to the 75-item questionnaire allowing to assess the engagement in physical, cognitive and social activities in adults, including the special procedure for determining the intensity levels of the items in each of the three domains. |
The whole study was conducted in accordance with the ethical principles of the declaration of Helsinki.
Part 1. Content and Development of the PAPA Questionnaire
Items Generation
Based on the literature review, more than 100 items that covered many categories (recreational, domestic, professional, etc.), mainly drawn from the compendium of physical activities19,26 while referring to various physical activity questionnaires, were first listed by two co-authors (CC and KP).
Selection of Items and Classes of Frequency and Duration from Interviews with Older Adults
177 older adults aged 55 and over (mean age: 69.8 years ± 9.32) were questioned on this first list of items in order to identify the most common physical, cognitive, and social activities for French older adults together with their most relevant ranges of frequency and duration. These participants were included, before the COVID health crisis, as part of a clinical research program whose main objective was to investigate the role of cognitive impairment in fall-related fractures among older adults. As previously reported, our population can be considered as representative of the general population with regard to functional capacities and health-related characteristics that can have an impact on the lifestyle, such as cognitive and mobility scores which were within the normal range,27,28 and a low number of comorbidities (mean: 1.7 ± 1.4). Furthermore, most were women (81%), and had a high education level (almost 12 years of schooling). This study was approved by the Lower Normandy Ethics Committee (no. 2011A00556-35; clinical trial registration no.: NCT02292316), and each participant provided written informed consent.
Participants were asked by a neuropsychologist to report on which activities they had been regularly engaging in over the past years. They were required to answer yes or no to the items list presented to them, to provide information about the other activities they were engaged in (for example, “Do you practice other sports? Do you have other leisure activities?”) They were also asked to indicate the frequency and duration of each activity, which was detailed in preselected classes (four frequency classes: never, occasionally, quite often, very often/every day, and four duration classes: < 15 min, 16 to 59 min, 1 to 4 h, or >4 h). They were also asked to indicate the activities from which they had withdrawn within the previous five years.
Responses from the participants allowed us to select and adjust, if needed, the final items, together with frequency and duration classes. After reaching a consensus, a new version of the questionnaire was established.
Content Validity
To explore the content of the questionnaire items and assess their representativeness with regard to the main participation and activities practiced in adulthood, the items were mapped to the categories and sub-categories of the international classification of functioning, disability, and health (ICF) developed by WHO.29 This ICF classification defines participation as an individual’s involvement in life situations, a conceptual approach often used for the measurement of participation.
Scoring
Each item gives rise to 3 scores: a sedentary behavior or physical activity score, a cognitive activity score, and a social activity score. Each of the 3 scores is the product of the three parameters for the item considered: frequency x duration x intensity level. The weighting procedure was as follows: weighting from 0 (never) to 3 (very often/every day) for the frequency, from 1 (< 15 min) to 4 (> 4 h) for the duration, and from 1 (light) to 3 (high) for the intensity level. The determination of the latter parameter is extensively detailed in part 2. Moreover, frequency was further weighted (minus 0.5 or 1 depending on the frequency) in the case of withdrawal from an activity within the previous five years. Sedentary lifestyle, and physical, cognitive, and social activity scores were then obtained by adding up the scores of all the items for each component and subcomponent.
Part 2. Assessment and Determination of the Intensity Level of Each of the Three Components of the Items
Intensity levels were first determined by the authors, then validated by studying the agreement between experts.
Initial Determination
The intensity level (none, light, moderate, or high) of each component (physical, cognitive, and social) was first determined for each item as follows. The intensity level for physical component was identified from the compendium of physical activities according to energy expenditure (≤ 1.5 MET for sedentary behavior; 1.5 to < 3, 3 to < 6, and ≥ 6 METs for light, moderate, and vigorous physical activity, respectively).19 Due to the lack of data in the literature for the cognitive and social components, independent rating of the intensity level in each of the two components was performed by three of the authors (GL, AP and CC).
Validation by Professional Experts
Participants
A purposive sample of 67 professionals recognized for their expertise in the three domains of interest was selected. Six expert groups were formed. Three were mainly specialized in one domain: physiotherapists and sport science researchers (Sport-Sci researchers) for the physical activity domain, and neuropsychologists for the cognitive activity domain. The three remaining groups were considered as experts in several domains: geriatricians, physical and rehabilitation physicians (PR physicians), and occupational therapists (OT). When an activity domain was covered by several professionals (for example, physical activity), fewer professionals were deliberately selected compared to those covered by a few professionals (for example, cognitive domain). Inclusion criteria were: being French-speaking and having worked with adults for at least two years. To take into consideration cross-cultural specificities, at least one professional per group had to be working abroad in a French-speaking country (Canada, Switzerland, etc.). Participants were recruited through knowledge networks, and provided informed consent online. This study was performed in accordance with the required ethical rules and standards, and has received approval from the Local Health Research Ethics Committee of Caen University Hospital (CLERS ID n° 1554).
Online Survey
Professional experts completed an online survey that consisted of sociodemographic characteristics and questions on the intensity level of the items divided into three sections (physical, cognitive, and social components). Each section presented the same items in a randomized order. More than 60% of the items on the PAPA questionnaire were included. Most of the non-selected items were those considered as redundant. For instance, numerous items specified “alone” or “with others” so only a few of them were selected.
Within each section, participants were asked to rate the intensity of the activity component of each item on a 4-point Likert Scale (sedentary, light, moderate, or vigorous for the physical component section; none, low, moderate or high for the cognitive and social component sections). Although the intensity level for physical items was already known, we thought it wise to ask the experts to classify these items so as to evaluate the adequacy level of classification between experts and the physical activity compendium. To assist in the choice of the intensity level of the items, a definition and an example for each intensity level were given for each component. This survey was performed using the online tool LimeSurvey® (Limesurvey GmbH. URL http://www.limesurvey.org).
Data Processing and Statistical Analyses
Data Processing
Individual ratings of the intensity levels were extracted from the online tool Limesurvey and analyzed per activity component and expert group. This was done by item, as follows. Responses were first expressed in percentages for each intensity level. These percentages were then weighted according to the expected intensity level identified by consensus, using the weighted Cohen’s kappa30,31 to take into account the percentage of responses obtained for the intensity levels close to the expected response. The weighting procedure was as follows. Percentage (P) were weighted by one for the expected intensity level (PX1), by 0.67 for responses contiguous to this expected response (PX2), and by 0.33 for responses located two levels away from the expected response ((PX3). Responses located three levels away from the expected level were considered incorrect. A weighted percentage of agreement observed (wPAO) was thus obtained for each item and expert group using the following formula: wPAO = 1*PX1 + 0.67*PX2 + 0.33*PX3.
Statistical Analyses
Three types of analyses were performed on the weighted data. The median wPAO of each expert group and that of all professionals were compared to a hypothetical median for each item, using the one-sample Wilcoxon signed-rank test. The minimum target threshold was set at 80% of the hypothetical median, in accordance with an excellent consensus defined by an agreement rate ≥ 80%.30 Intergroup comparisons on the wPAO were performed by the intensity level within each component using the Kruskal-Wallis test. For each of the 3 components, the wPAO of each expert group and all professionals was also compared i) to the minimum target threshold by ICF categories, and ii) between ICF categories, again using the Kruskal-Wallis test. Pairwise comparisons were performed using the Nemenyi post-hoc test. To verify that the intensity levels allocated to each item proportionally and consistently contributed to each component, internal consistency was assessed by component by Cronbach’s alpha coefficient.32
Results
Part 1. Content and Development of the PAPA Questionnaire
Items
From the interviews with older adults, 50 relevant items were identified. Some items were broken down into several activity levels. For instance, for the physical component, “Dancing” was broken down into “Slow ballroom dancing (for example, slow and tango)”, “Fast ballroom dancing (for example, disco and country)”, and “Aerobic” which corresponds to a moderate physical activity for the first item and vigorous physical activity for the last two. Regarding the social component, a number of items were broken down into “alone (no social participation)” and “with others” (moderate or high social participation, depending on the item) such as going to the museum alone or with others. Due to these item divisions that also involved a cognitive component, the total number of items increased from 50 to 75.
Based on the ICF classification,29 items were distributed between “activities and participation” (90%) and “environmental factors” (6%) categories. The remaining items (4%) were not part of the ICF (for example, “Sitting and doing nothing for at least 15 min”). Items from the “activities and participation” category fell into the following sub-categories: mobility (2% of the whole items; such as walking), domestic (16%; for example, housework tasks), major life area (6%; for example, economic life) and community, social and civic life (66%). 12% items of this latter sub-category pertained to community life and 88% recreation and leisure of which about 34% were sport activities.
Duration and Frequency
Frequency of the activities reported by the participants confirmed the usefulness of using the four categories previously identified that were further adapted to the type of activity (“never, ≤ twice a month, once to 3 times a week, ≥ 4 times a week” or “never, ≤ once a year, ~once a year, ≥ twice a year » or “Yes/No” for lifestyle items such as “Cohabiting with a partner”). Recent withdrawal from an activity, and the four duration classes were also found appropriate.
Part 2. Assessment and Determination of the Intensity Level Involved in Each Item for Each of the Three Components
Participant Characteristics
Fifty-six experts of the 67 solicited (83.68%) responded to the online survey. The sample was comprised of 6 geriatricians, 9 physiotherapists, 14 occupational therapists (OT), 11 neuropsychologists, 6 PR physicians, and 10 Sport-Sci researchers. The uneven number of experts in each group was deliberate, as explained in the Methods section. As shown in Table 1, most professionals were between 31 and 40 years old (43%), 45% were women, 48% had more than 10 years of professional experience, and 21% were from French-speaking countries outside France. There was no significant difference between the characteristics of professional groups except for sex (p = 0.007) where women were more numerous among OT than Sport-Sci researchers (20% vs 86%; p = 0.023), in accordance with the representation of these professions in France.33
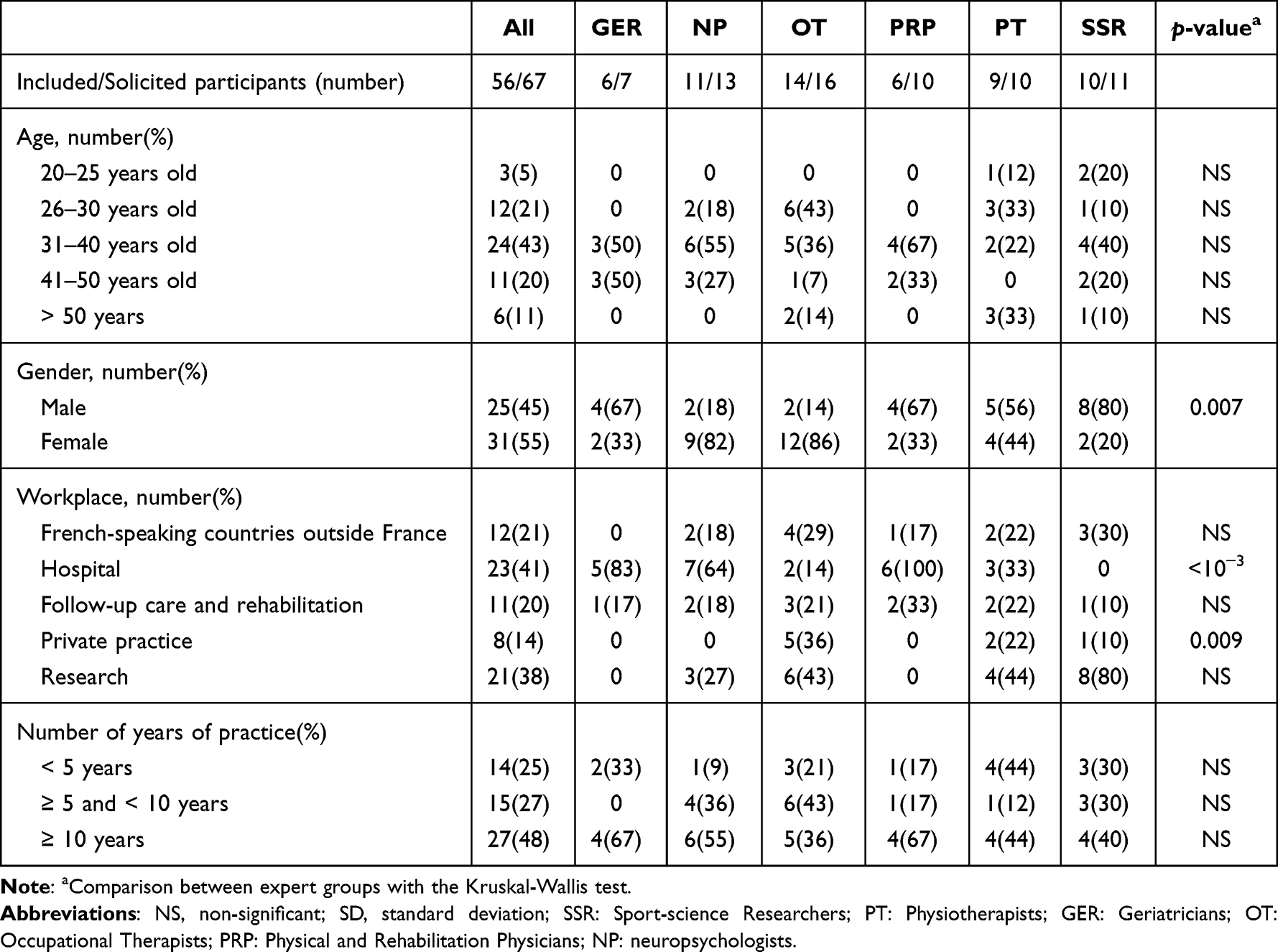 |
Table 1 Demographic Characteristics of the Professional Experts Who Responded to the Online Survey Aiming at Validating the Intensity Levels of the Items in Each of the Three ComponentsStudied |
Intensity Level Involved in Each Item
Median wPAO of the Expert Groups in the Physical, Cognitive, and Social Activity Domains
When all experts were grouped together, the median wPAO was consistently above the minimum target threshold, significantly or not, regardless of the level of intensity of the items and the component (Figure 2). Indeed, for physical component of the items, this median wPAO reached 97.3% (p < 10−3), 87.5% (p < 10−3), 95.8% (p = 0.006) and 95.5% (p = 0.005) ranging from the lowest to the highest intensity level. It was 83.9% (p= 0.176), 84.5% (p= 0.001), 84.6% (p= 0.001) and 86.3% (p= 0.018), respectively, for the cognitive component, and 97.6% (p < 10−3), 83.3% (NS), 82.2% (NS) and 89.6% (p= 0.005), respectively, for the social component. The median wPAO by expert group and intensity level (Figure 2) was never significantly lower than the minimum target threshold for the physical and social component. For the cognitive component, the wPAO for the Sport-Sci researchers was significantly lower than the minimum target threshold (70%, p= 0.018) for the high intensity level. Variability of responses within groups was, however, higher or lower depending on the component and the expert group (for example, min/max = 63.3/100 and 80/93.3 for none and light activity, respectively for the cognitive component in the Sport-Sci researchers). When analyzing the data by items, the median wPAO was usually significantly above the minimum target threshold except for 2, 6, and 10 items for the physical, cognitive, and social component respectively, for which these medians were between 63.1 and 79.77% (Table 2).
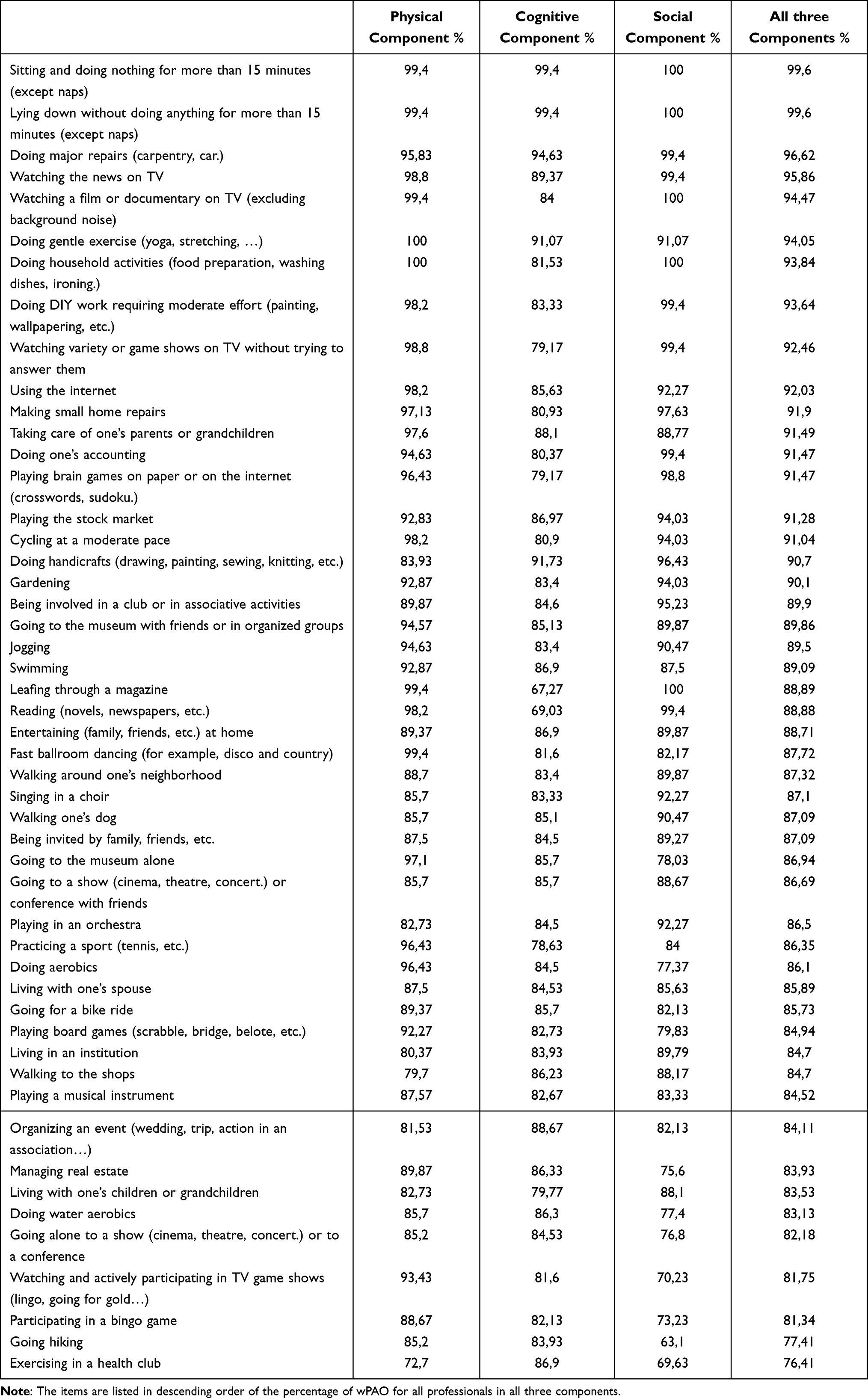 |
Table 2 Mean Weighted Percentage of Agreement Observed (wPAO) of All Professionals for the Physical, Cognitive and Social Components, and All Three Components for the 50 Items of the Online Survey |
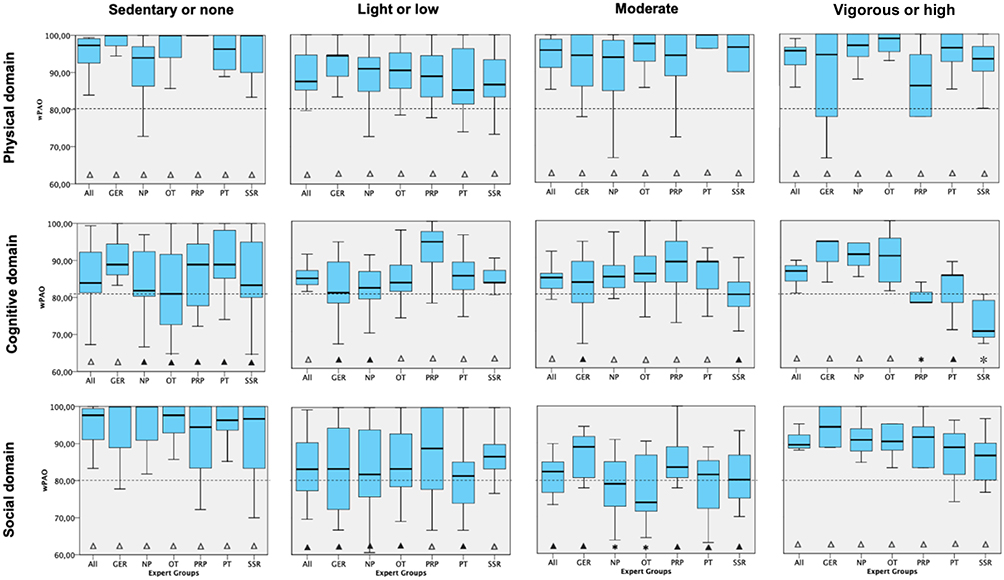 |
Figure 2 Median wPAO for scoring the intensity level of the items in each three domains (physical, cognitive and social) for the whole sample of experts and each expert group. None, Light, Moderate, and High correspond to the four intensity levels for the classification of the items. The horizontal dotted line indicates the minimum target threshold defined by consensus (80% of the hypothetical median). Δ, Significantly above the minimum target threshold; ▲, Above the minimum target threshold but not significantly different; ✱, Lower than the minimum target threshold but not significantly different; ✻, Significantly lower than the minimum target threshold (p= 0.018). Abbreviations: SSR, Sport-science Researchers; PT, Physiotherapists; GER, Geriatricians; OT, Occupational Therapists; PRP, Physical and Rehabilitation Physicians; NP, neuropsychologists. |
Comparison between expert groups showed a few significant differences for each component. Regarding the global wPAO per component, the only significant intergroup difference was found for the cognitive component (p=0.002). Post-hoc analysis indicated that the Sport-Sci researchers had significantly lower wPAO than PR physicians and physiotherapists (81.3±9.8% vs 87.8±8.1%; [p< 10–3] and 85.6±6.2% [p= 0.035], respectively). With regard to wPAO per intensity level (Table 3), significant intergroup differences were found for sedentary and vigorous activity of the physical component (p <10−3 and =0.043, respectively), high activity of the social component (p= 0.036), and low, moderate and high activity of the cognitive component (p<10-3, =0.027, and <10-3, respectively). However, there was only one significant intergroup difference for which wPAO of an expert group was lower than the minimum target threshold. This was found for the items with high activity of the cognitive component. Post-hoc analysis indicated that wPAO of Sport-Sci researchers was significantly lower than that of OT, neuropsychologists, and geriatrics (70% vs 90.5% [p= 0.007], 90.9% [p = 0.003] and 94.4% [p= 0.001], respectively) (Table 3).
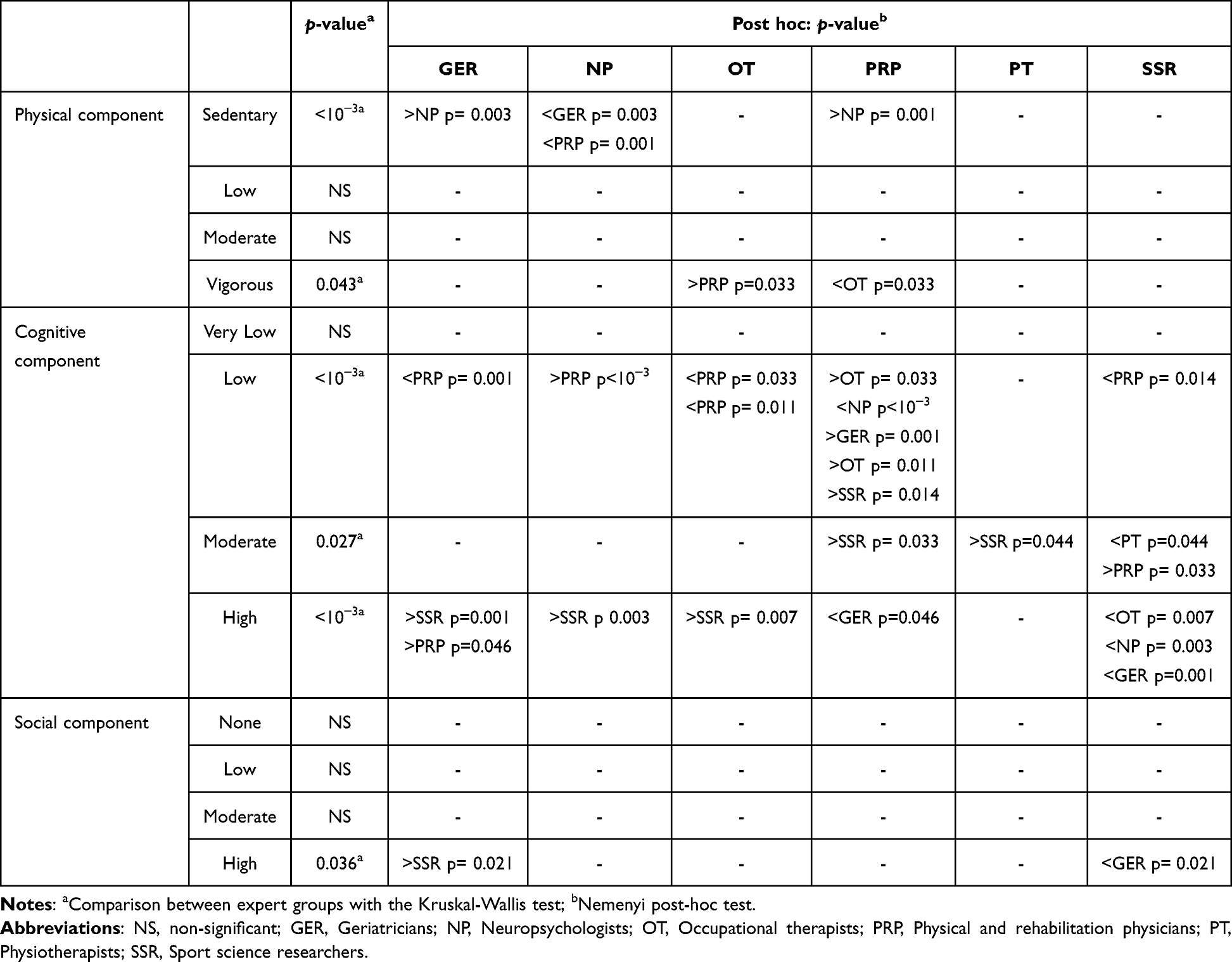 |
Table 3 Intergroup Comparisons of the Mean Weighted Percentage of Agreement Observed (wPAO) for Each Component and Each Intensity Level |
wPAO of the Expert Groups by ICF Categories
To assess the distribution and representativeness of the items, comparisons between wPAO of the expert groups and the minimum target threshold were made on the following ICF categories: mobility, domestic, economic life, community life, sport activities, non-sporting leisure activities, and others (environmental factors plus the single item not part of the ICF). For the physical and social components, the wPAO was not significantly different from the minimum target threshold regardless of the category considered. No significant difference was found between categories for all professionals either, regardless of the expert group considered. The same held true for the cognitive component except for the neuropsychologists (wPAO = 84.83; p= 0.001). However, the wPAO of the neuropsychologist was higher than the minimum target threshold in each category, and post-hoc tests did not reveal any significant difference between categories.
Internal Consistency
Cronbach’s alpha was 0.92, 0.92, and 0.85 for the physical, cognitive, and social components, respectively, which confirmed the excellent internal consistency.
Discussion
This research presents the first questionnaire allowing the precise and separate quantification of the cognitive and social components of a number of activities. More importantly, it allows assessment of lifetime engagement in activities with separate quantification of their physical, cognitive, and social components. This 75-item PAPA questionnaire covers a wide range of activities and gives rise to 4 scores (a sedentary lifestyle score, a physical activity score, a cognitive activity score, and a social activity score), each weighted by the intensity level of the component as well as its duration and frequency. It is the result of a thorough investigation using both a representative group of adults aged 55 years and over and professional experts from different backgrounds. The PAPA questionnaire thus developed should add more information to the existing measures of engagement in activities and deepen knowledge about cognitive reserve.
The selected items encompass a very wide range of representative life activities that adults may be engaged in, as shown by the categories of the ICF classification29 they cover (mainly in the “activities and participation” category). This is in line with most CR questionnaires (for example, CRIq,5 the LEQ6 or the CRS7) but at variance with questionnaires that mainly focus on a single activity domain, such as the physical activity questionnaires (PASE, IPAQ-SF, PASB-Q). Nevertheless, a major difference between the CR questionnaires and the PAPA questionnaire is the classification we used that separately targets the three activity domains highlighted in the CR model (physical, cognitive, and social activities) while giving an equivalent load to each domain. Yet, practicing activities that stimulates both physical, cognitive and social components contributes to the development of CR and can thus prolong healthy aging1–3 and be efficiently used to reduce the risk of dementia.4,8 In the few studies that have assessed social participation4 or cognitive stimulating activities,4,23,24 the number of items was generally low (8 at most). Regarding the physical component, although several existing physical activity questionnaires have been proved to be very useful,34 the PAPA questionnaire evaluates more diverse areas. Indeed, in addition to questions about sport activities, mobility, and conventional leisure activities (for example, gardening, DIY), it often asks questions about neglected items such as caring for grandchildren or going to the museum.
The PAPA questionnaire also provides new advantages over the existing questionnaires regarding the duration of the activities. It is assessed here in terms of duration of the activity itself (from < 15 min to > 4 h) which is not included in the CR questionnaires. Participation is also assessed over the past years, as in the CR questionnaires, but in contrast to physical activity questionnaires that often focus on one to four weeks only (for example, PASE, IPAQ-SF, and CHAMPS). The PAPA questionnaire also takes into account recent disengagement in the activities (within the previous 5 years) as in the CR measures, but not in the physical activity questionnaires. Such disengagement may frequently occur in older adults, and is very useful when studying cognitive reserve. Indeed, knowing both the activity practiced over the recent years as well as those practiced until recently is crucial. As stated by Stern et al,1 cognitive reserve depends largely on lifelong experiences. This has been specifically confirmed by a larger gray matter volume in late-life in physically active versus sedentary persons in midlife.35 The frequency classes of the activities practiced are very similar to those of most questionnaires (for example, CHAMPS, IPAQ-SF, PASB-Q, PASE).
The level of intensity involved in the activities is also a crucial element to which particular attention had been paid in developing the PAPA questionnaire. WHO’s recommendations on physical activity for adults14 are indeed given in terms of both duration and intensity level. This notion of intensity has therefore been integrated into the PAPA questionnaire, not only for the physical component of the activities, as has been done for many years in the physical activity questionnaires, but also for social and cognitive components which, to our knowledge, has been done only in a single study on cognitive activities.24 The intensity level is not included in the CR measures either. For instance, a CRIq item pertains to both “gardening” and ‘knitting’.5 However, gardening involves physical activity at a low to vigorous level of intensity according to the compendium of physical activities,19 whereas knitting is most often a sedentary activity since performed while sitting. Separating items such as gardening and knitting to have a distinct score for each seems therefore more relevant.
The intensity level involved in each item of the PAPA questionnaire was validated by professional experts. Our results showed that, whether the experts are grouped together or considered separately, the median wPAO was consistently higher than the minimum target threshold for each three components except for the high intensity level of the cognitive component in the Sport-Sci researchers who are not specialized in cognition. This indicates that the intensity level of the items initially identified was globally accurate. This was expected for the physical component since the notion of intensity is well-known in the physical activity domain, as illustrated by the WHO recommendations on physical activity.14 This was, however, less expected for the cognitive and social components, the notion of intensity level being less often used in these domains. Several professional groups in the present study usually have little expertise in these areas (for example, physiotherapists and Sport-Sci researchers). The significantly lower wPAO among Sport-Sci researchers versus OTs, neuropsychologists, and geriatricians (70% vs ≥ 90%) for items with a high cognitive load can be easily explained by the fact that the Sport-Sci researchers are not experts in cognition unlike the neuropsychologists, and, to a lesser degree, the OTs and geriatricians. It is important to note that there was often high heterogeneity in wPAO within groups, which would mainly be explained by the variability in the value judgment of the experts, likely reflecting variability between each professional’s expertise.
Finally, the scores obtained from the PAPA questionnaire, that take into account the different elements mentioned above (number of activities, frequency, duration, lifespan, and level of intensity), also have several advantages. The originality and main strength of the questionnaire is to provide a physical, cognitive, and social activity score for each item. Such a multimodal approach would be particularly relevant because an item described as purely physical often shows an implicit social or cognitive dimension as well, and vice versa. For instance, the item “dancing”, an undeniably physical activity, also has a social dimension since it is mainly practised with others and requires various cognitive processes such as learning of complex motor sequences, procedural memory, attention, visuomotor integration, and synchronization in space and time.36,37 In addition, by providing a distinct score for each component, the PAPA questionnaire offers an opportunity to isolate their respective involvement. Another strength is to allow the calculation of two distinct scores for the physical component: a physical activity and a sedentary behavior score. A few questionnaires such as the WHO Global Physical Activity Questionnaire (GPAQ) questionnaire38 and the recent National Observatory for Physical Activity and Sedentariness-Physical Activity Questionnaire (ONAPS-PAQ)39 assessed both sedentary behavior and physical activity. However, most questionnaires, such as the IPAQ-SF and CHAMPS, were not designed to assess sedentary behavior. Yet, a sedentary lifetime measurement facilitates the identification of persons with major risk factors for chronic diseases40 or dementia41 that can lead to premature death and heavy social burden.34,42 This is a major issue, especially in the elderly for whom the prevention of sedentary behavior and promotion of physical activity is essential.42,43
The high Cronbach’s alpha coefficient favors excellent internal consistency, highlighting the excellent coherence of the PAPA questionnaire. Although this supports accurate determination of the activity level for each of the three components of each item, a median wPAO lower than the minimum target threshold for some individual items requires specific attention. Because this might affect the quality of the questionnaire, the following decisions were made regarding the intensity levels of the 17 items whose wPAO of the experts was lower than the minimum target threshold. First, the intensity level identified by the experts was not retained only for the two items concerned in the physical component because we prefer to refer to the physical activity level determined in the compendium19 since it is well-recognized. Second, for 8 items (n=2 and 6 items of the cognitive and social component, respectively), no adjustment was required since the activity level that was predetermined by consensus for these components obtained the highest wPAO from the experts. Finally, for the remaining 7 items, the intensity level was adjusted to the expert’s assessment that was above the minimum target threshold for each of the 7 items. This included 4 items of the cognitive component (playing brain games; leafing through a magazine; reading a novel, and watching variety shows on TV without answering) and 3 items of the social component (going to the museum and shows alone, and watching and actively participating in TV game shows). These changes from the intensity levels initially proposed by consensus were consistent with the choice of intensity level for similar items in the cognitive domain24 and the social domain.44
Following these adjustments, we now have a ready-made and easy-to-use questionnaire to assess the engagement in activities, with separate quantification of their physical, cognitive, and social components. This PAPA questionnaire, which lasts about 15 min, gives rise to automatic calculation of 4 scores (sedentary lifestyle and physical, cognitive, and social activity scores). Its French version can be accessed at: https://www.sphinx.univ-tours.fr/v4/s/rofhtf. It can also be available for use on request from the authors. An English version of the PAPA questionnaire is in progress (in collaboration with the Centre for interdisciplinary research in rehabilitation and social integration (Cirris), Quebec, Canada).
Some limitations can be addressed. First, determination of the intensity level of the items was assessed on only 50 of the 75 items. However, as justified in the Methods section, most on the non-included items were considered as redundant. Second, this PAPA questionnaire was primarily designed for older adults because participation in physical, cognitive and social activities provides extensive health benefits in this population. Yet, involvement in these activities is a major public health challenge at all ages.45 Moreover, because we selected items from the multiple categories included in the physical activity compendium and our senior population was fairly active, this questionnaire should also be relevant for younger adults. If the high education of our population surely had a positive impact on their numerous activities, the high percentage of women may have masked some specifically male activities. Third, although the physical activity score is less objective than classic accelerometer measurements,46 it is more informative and reflects more cognitive reserve since it covers much longer periods and can include the limbs as well as the head (for example, singing). Fourth, sample size differed between expert groups and was rather small for some groups. Nevertheless, altogether, 56 experts were included. Six groups, each with a different professional expertise, were intentionally constituted to highlight different putative perceptions in evaluating the intensity level of each component of the activities according to expert groups. We however found that regardless of the expert group and with rare exceptions, the results were all above or equal to the minimum target threshold. Finally, further studies on a larger sample of specific populations that include comparisons with widely recognized questionnaires and test-retest would be helpful to confirm the usefulness of the PAPA questionnaire. Assessment of other psychometric properties of the questionnaire such as the construct validity would also improve of the quality of the PAPA questionnaire.
Conclusion
The main strength of the present study is that it fills a gap in the assessment of engagement in activities by taking into account their physical, cognitive, and social components, and thus in the assessment of CR. This is the first questionnaire to assess these three components using data from the same items which cover a wide range of activities. In addition, it gives rise to 4 scores (a sedentary lifestyle score, a physical activity score, a cognitive activity score, and a social activity score), each weighted by the intensity level of the component considered, as well as the frequency and duration of each activity, including lifespan. This ready-made and easy-to-use questionnaire is able to assess three components of the activities at the same time and should save time, especially when assessing elderly persons. This would allow users to easily identifying the most frail, isolated, or sedentary persons and help to promote healthy aging and reduce the risk of dementia. This PAPA questionnaire should thus be very useful for a large number of both clinicians and researchers working with elderly individuals, but it can also apply to young and middle-aged adults.
Acknowledgments
The authors would like to thank Valérie Constans for the English proofreading.
Funding
This work was supported by the French Ministry of Health (PHRC, Programme Hospitalier de Recherche Clinique 2011 no. 2011-A00534-37).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stern Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012;11(11):1006–1012. doi:10.1016/S1474-4422(12)70191-6
2. Krivanek TJ, Gale SA, McFeeley BM, Nicastri CM, Daffner KR. Promoting Successful Cognitive Aging: a Ten-Year Update. J Alzheimer’s Dis. 2021;81(3):871–920. doi:10.3233/JAD-201462
3. Pettigrew C, Soldan A. Defining Cognitive Reserve and Implications for Cognitive Aging. Curr Neurol Neurosci Rep. 2019;19:1. doi:10.1007/s11910-019-0917-z
4. Ruthirakuhan M, Luedke AC, Tam A, Goel A, Kurji A, Garcia A. Use of physical and intellectual activities and socialization in the management of cognitive decline of aging and in dementia: a review. J Aging Res. 2012;2012. doi:10.1155/2012/384875
5. Nucci M, Mapelli D, Mondini S. Cognitive Reserve Index questionnaire (CRIq): a new instrument for measuring cognitive reserve. Aging Clin Exp Res. 2012;24(3):218–226. doi:10.3275/7800
6. Valenzuela MJ, Sachdev P. Assessment of complex mental activity across the lifespan: development of the Lifetime of Experiences Questionnaire (LEQ). Psychol Med. 2007;37(7):1015–1025. doi:10.1017/S003329170600938X
7. Leon I, Garcia J, Roldan-Tapia L. Development of the scale of cognitive reserve in Spanish population: a pilot study. Rev Neurol. 2011;52(11):653–660.
8. Fratiglioni L, Marseglia A, Dekhtyar S. Ageing without dementia: can stimulating psychosocial and lifestyle experiences make a difference? Lancet Neurol. 2020;19(6):533–543. doi:10.1016/S1474-4422(20)30039-9
9. Sattler MC, Jaunig J, Tösch C, et al. Current evidence of measurement properties of physical activity questionnaires for older adults: an updated systematic review. Sports Med. 2020;50(7):1271–1315. doi:10.1007/s40279-020-01268-x
10. Fowles JR, O’Brien MW, Wojcik WR, d’Entremont L, Shields CA. A pilot study: validity and reliability of the CSEP-PATH PASB-Q and a new leisure time physical activity questionnaire to assess physical activity and sedentary behaviours. Appl Physiol Nutr Metab. 2017;42(6):677–680. doi:10.1139/apnm-2016-0412
11. Washburn RA, Smith KW, Jette AM, Janney CA. The Physical Activity Scale for the Elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46(2):153–162. doi:10.1016/0895-4356(93)
12. Grimm EK, Swartz AM, Hart T, Miller NE, Strath SJ. Comparison of the IPAQ-Short Form and accelerometry predictions of physical activity in older adults. J Aging Phys Act. 2012;20(1):64–79. doi:10.1123/japa.20.1.64
13. Colbert LH, Matthews CE, Havighurst TC, Kim K, Schoeller DA. Comparative Validity of Physical Activity Measures in Older Adults. Med Sci Sports Exerc. 2011;43(5):867–876. doi:10.1249/MSS.0b013e3181fc7162
14. World Health Organization. Guidelines on physical activity and sedentary behaviour. WHO; 2020. Available from: https://www.who.int/publications/i/item/9789240015128.
15. Yan S, Fu W, Wang C, et al. Association between sedentary behavior and the risk of dementia: a systematic review and meta-analysis. Transl Psychiatry. 2020;10:1. doi:10.1038/s41398-020-0799-5
16. Byrom B, Stratton G, McCarthy M, Muehlhausen W. Objective measurement of sedentary behaviour using accelerometers. Int J Obes. 2016;40(11):1809–1812. doi:10.1038/ijo.2016.136
17. Dohrn IM, Kwak L, Oja P, Sjöström M, Hagströmer M. Replacing sedentary time with physical activity: a 15-year follow-up of mortality in a national cohort. Clin Epidemiol. 2018;10:179–186. doi:10.2147/CLEP.S151613
18. Arnardottir NY, Koster A, van Domelen DR, et al. Association of change in brain structure to objectively measured physical activity and sedentary behavior in older adults: age, Gene/Environment Susceptibility-Reykjavik Study. Behav Brain Res. 2016;296:118–124. doi:10.1016/j.bbr.2015.09.005
19. Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of Physical Activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(Supplement):S498–S516. doi:10.1097/00005768-200009001-00009
20. Friedenreich CM, Courneya KS, Bryant HE. The Lifetime Total Physical Activity Questionnaire: development and reliability. Med Sci Sports Exer. 1998;30:2.
21. de Vera MA, Ratzlaff C, Doerfling P, Kopec J. Reliability and validity of an internet-based questionnaire measuring lifetime physical activity. Am J Epidemiol. 2010;172(10):1190–1198. doi:10.1093/aje/kwq273
22. Vuillemin A, Guillemin F, Denis G, Huot J, Jeandel C. A computer-assisted assessment of lifetime physical activity: reliability and validity of the QUANTAP software. Rev Epidemiol Sante Pub. 2000;48:157–167.
23. Helzner EP, Scarmeas N, Cosentino S, Portet F, Stern Y. Leisure activity and cognitive decline in incident Alzheimer disease. Arch Neurol. 2007;64(12):1749. doi:10.1001/archneur.64.12.1749
24. Wilson RS, Bennett DA, Beckett LA, et al. Cognitive activity in older persons from a geographically defined population. J Gerontol B Psychol Sci Soc Sci. 1999;54B(3):P155–P160. doi:10.1093/geronb/54B.3.P155
25. Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19(4):539–549. doi:10.1007/s11136-010-9606-8
26. Vuillemin A, Speyer E, Simon C, Ainsworth B, Paineau D. Critical review of the physical activity questionnaires directed at the French population and development perspectives. Cah Nutr Diet. 2012;47(5):234–241. doi:10.1016/j.cnd.2012.04.002
27. Attoh-Mensah E, Loggia G, Schumann-Bard P, et al. Adverse effects of anticholinergic drugs on cognition and mobility: cutoff for impairment in a cross-sectional study in young–old and old–old adults. Drugs Aging. 2020. doi:10.1007/s40266-019-00743-z
28. Loggia G, Attoh-mensah E, Pothier K, et al. Psychotropic polypharmacy in adults 55 years or older: a risk for impaired global cognition, executive function, and mobility. Front Pharmacol. 2020;10:1–9. doi:10.3389/fphar.2019.01659
29. World Health Organization. International Classification of Functioning, Disability and Health (ICF). WHO; 2001. Available from: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health.
30. Newman TB, Kohn MA. Evidence-Based Diagnosis. Cambridge University Press; 2009; doi:10.1017/CBO9780511759512
31. Gwet KL. Handbook of Inter-Rater Reliability: The Definitive Guide to Measuring the Extent of Agreement Among Raters. Advanced Analytics, LLC; 2014.
32. Thorndike RM. Book Review: psychometric Theory. Appl Psychol Meas. 1995;19(3):303–305. doi:10.1177/014662169501900308
33. Direction de la recherche des études de l’évaluation et des statistiques. La Démographie Des Professions de Santé, Hors Médecins. DRESS; 2015. Available from: https://drees.solidarites-sante.gouv.fr/sites/default/files/2021-01/les_professions_de_sante_au_1er_janvier_-_sources.pdf.
34. Falck RS, McDonald SM, Beets MW, Brazendale K, Liu-Ambrose T. Measurement of physical activity in older adult interventions: a systematic review. Br J Sports Med. 2016;50(8):464–470. doi:10.1136/bjsports-2014-094413
35. Rovio S, Spulber G, Nieminen LJ, et al. The effect of midlife physical activity on structural brain changes in the elderly. Neurobiol Aging. 2010;31(11):1927–1936. doi:10.1016/j.neurobiolaging.2008.10.007
36. Brown S, Martinez MJ, Parsons LM. The Neural Basis of Human Dance. Cereb Cortex. 2006;16(8):1157–1167. doi:10.1093/cercor/bhj057
37. Predovan D, Julien A, Esmail A, Bherer L. Effects of Dancing on Cognition in Healthy Older Adults: a Systematic Review. J Cogn Dev. 2019;3(2):161–167. doi:10.1007/s41465-018-0103-2
38. Cleland CL, Hunter RF, Kee F, Cupples ME, Sallis JF, Tully MA. Validity of the Global Physical Activity Questionnaire (GPAQ) in assessing levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health. 2014;14(1):1255. doi:10.1186/1471-2458-14-1255
39. Charles M, Thivel D, Verney J, et al. Reliability and validity of the ONAPS physical activity questionnaire in assessing physical activity and sedentary behavior in French adults. Int J Environ Res Public Health. 2021;18:11. doi:10.3390/ijerph18115643
40. Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25:1–72. doi:10.1111/sms.12581
41. Yan S, Fu W, Wang C, et al. Association between sedentary behavior and the risk of dementia: a systematic review and meta-analysis. Transl Psychiatry. 2020;10(1):112. doi:10.1038/s41398-020-0799-5
42. Ekelund U, Tarp J, Steene-Johannessen J, et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ. 2019;366:l4570. doi:10.1136/bmj.l4570
43. Lavie CJ, Ozemek C, Carbone S, Katzmarzyk PT, Blair SN. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ Res. 2019;124(5):799–815. doi:10.1161/CIRCRESAHA.118.312669
44. Krueger KR, Wilson RS, Kamenetsky JM, Barnes LL, Bienias JL, Bennett DA. Social engagement and cognitive function in old age. Exp Aging Res. 2009;35(1):45–60. doi:10.1080/03610730802545028
45. World Health Organization. Global Action Plan on Physical Activity 2018–2030: more Active People for a Healthier World. WHO; 2018. Available from: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf?sequence=1&isAllowed=y.
46. Koolhaas CM, van Rooij FJA, Cepeda M, Tiemeier H, Franco OH, Schoufour JD. Physical activity derived from questionnaires and wrist-worn accelerometers: comparability and the role of demographic, lifestyle, and health factors among a population-based sample of older adults. Clin Epidemiol. 2018;10:1–16. doi:10.2147/CLEP.S147613
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.