")
Back to Journals » Clinical Ophthalmology » Volume 15
The Outcome of One-to-Four Muscle Surgery by Intraoperative Relaxed Muscle Positioning with Adjustable Suture Technique in Thyroid Eye Disease
Authors Lekskul A , Tangtammaruk P , Wuthisiri W
Received 9 August 2021
Accepted for publication 31 August 2021
Published 11 September 2021 Volume 2021:15 Pages 3833—3839
DOI https://doi.org/10.2147/OPTH.S333377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Apatsa Lekskul,1 Phantaraporn Tangtammaruk,1,2 Wadakarn Wuthisiri1
1Department of Ophthalmology, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand; 2Metta Pracharak Hospital, Nakhon Pathom, 73210, Thailand
Correspondence: Wadakarn Wuthisiri
Department of Ophthalmology, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand
Tel +66 2-201-2729
Fax +66 2-201-1516
Email [email protected]
Purpose: To identify the outcome of one-to-four muscle surgery by intraoperative relaxed muscle positioning with adjustable suture technique for the treatment of thyroid eye disease.
Methods: Ninety patients diagnosed with thyroid eye disease who underwent intraoperative relaxed muscle positioning with adjustable suture technique at Ramathibodi Hospital from January 1, 2015 through December 31, 2020 were included in this retrospective study. The patient demographic data were evaluated. Pre- and post-operative ocular alignment and diplopia status were measured after a follow-up period of at least 6 months. Successful outcomes were categorized into two parts: motor outcome and sensory outcome. Successful motor outcome was defined as vertical deviation equal to 4 prism diopters or less and horizontal deviation equal to 10 prism diopters or less in primary position. Successful sensory outcome was defined as the absence of diplopia in primary position.
Results: Ninety patients were included in this study, and the mean age of strabismic surgery was 56.6 ± 10.1 years old. Thirty-nine patients had a history of orbital decompression surgery. Mean follow-up time was 33.7 ± 11.8 months. The success of motor and sensory outcomes exhibited a decrease from one-to-four muscle surgery. Motor success decreased from one-muscle to four-muscle surgery (84.62%, 81.58%, 75.00%, and 64.29%) and sensory success similarly decreased (84.62%, 84.21%, 75.00%, and 78.57%). However, the comparative outcomes of motor success and sensory success were not statistically different among groups (p = 0.58 and 0.84). Lower lid retractions were found in 12 patients (13.33%).
Conclusion: Intraoperative relaxed muscle positioning technique might be a successful option for the correction of thyroid eye disease-associated strabismus. This technique may be done with one-to-four muscle surgery, which yields success in both motor and sensory outcomes.
Keywords: thyroid eye disease, one-to-four strabismus surgery, intraoperative relaxed muscle positioning, restrictive strabismus, adjustable suture technique
Introduction
Thyroid eye disease (TED) is an autoimmune condition characterized by the presence of auto-antibodies to the thyroid stimulating hormone receptor and the insulin-like growth factor receptor in an acute inflammatory phase, followed by a fibrotic phase in the orbit, which leads to restrictive movement of the extraocular muscles that then causes restrictive strabismus and diplopia.1,2
Restrictive strabismus occurs in about 15% of all patients with TED.3 The inferior rectus (IR) and medial rectus (MR) muscles are the most commonly affected muscles, followed by the superior rectus (SR) and lateral rectus (LR) muscles.4 The surgical correction of strabismic TED aims to achieve single binocular vision in primary position.5 However, surgical correction of thyroid-associated strabismus is challenging. There are many previous reports on the success rates of different surgical techniques. The rates of successful surgical outcomes varied between 47–92% with adjustable sutures and 38–82% without adjustable sutures.6,7 In our experience, we found that it was difficult to achieve successful surgical outcomes for thyroid-associated strabismus with regular doses of strabismus surgery. To address this difficulty, the standard TED-associated strabismus surgery in our department is rectus muscle recession with intraoperative adjustable suture technique either under topical (TA) or general anesthesia (GA). This study aims to identify the outcome of one-to-four muscle surgery by intraoperative relaxed muscle positioning with adjustable suture technique to treat TED.
Materials and Methods
The retrospective study used an electronic medical record system to identify all TED patients who underwent strabismic surgery from January 1, 2015 through December 31, 2020 at Ramathibodi Hospital, Thailand. The study protocol was approved by the Human Research Ethics Committee Faculty of Medicine at Ramathibodi Hospital, Mahidol University and adhered to the tenets of the Health Insurance Portability and Accountability Act and the Declaration of Helsinki.
The demographic data of all TED patients was recorded, including age, sex, presence of diplopia or strabismus, and history of orbital decompression surgery. The preoperative and postoperative ocular alignments were recorded by alternated prism cover test at both near and distance in primary position. The surgical procedure used by three of the authors, type and number of rectus muscles corrected, and length of the follow-up period were recorded.
Patients
The diagnosis of strabismic TED was defined by a history of thyroid disease, ocular signs such as conjunctival injection, chemosis, lid retraction, proptosis or limit of ocular gaze movement, presence of enlarged extraocular muscles in orbital computed tomography scan, positive thyroid auto-antibodies, and abnormal thyroid function tests.
Surgical Procedure
Two types of anesthesia were used in this surgical procedure: TA and GA. The type of anesthesia was chosen by the patient after the patient received information from the surgeon regarding both types of anesthesia.
Intraoperative Relaxed Muscle Positioning with Adjustable Suture Technique Under TA
All patients who underwent the TA technique were soaked with topical 2% lidocaine gel in the fornix conjunctiva for at least 10 min before surgery. For intraoperative adjustment, both eyes were prepped and draped in the usual manner. Then, the eye speculum was placed in the eye that was to receive surgery. 1% lidocaine with 1:100,000 epinephrine was injected into the subconjunctiva. Forced duction test (FDT) was performed. Patient was asked to gaze as far as possible into the field of gaze being test and the restricted rectus muscle was recorded. Next, the conjunctiva was incised using the limbal conjunctival incision technique to maximize the operating field. The rectus muscle was identified with Stevens hook, and the intermuscular septum and Tenon capsule were separated from the insertion of the rectus muscle. A 6–0 vicryl suture was placed at the insertion of the muscle to secure the rectus muscle, and then the muscle was disinserted from its insertion point. After disinsertion of the rectus muscle, FDT was repeated to ensure free movement of the globe. The disinserted muscle was then allowed to sit freely on the globe without tension. This position was estimated as the proper position needed for recession of the restricted rectus muscle. The surgeon then re-sutured the 6–0 vicryl suture to the original insertion point, placed the rectus muscle in a position in which it may sit freely without tension, and secured the suture at the insertion point using the bow-tie technique. The position of the eye was evaluated, while the patient was in the supine position, and then the patient was positioned upright. The cover test with a fixation target set at the same level as the patient was performed to evaluate the deviation of the eye. If residual deviation was present, the patient was returned to the supine position, and the rectus muscle was readjusted until there was no deviation and no diplopia. The conjunctiva was secured with 8–0 vicryl sutures using interrupted technique.
Intraoperative Relaxed Muscle Positioning with Adjustable Suture Technique Under GA
All patients who underwent the GA technique were informed that they would be awakened in the middle of the procedure to complete the adjustable surgical technique until there was no diplopia or deviation. The surgical technique was the same as the TA technique up to the point in the procedure at which the 6–0 vicryl suture was re-sutured back to the original insertion. To perform intraoperative adjustment, the patient must be awake. The operative field was covered with a sterile sheet. The anesthesiologist woke the patient and removed the endotracheal tube, and then waited until the patient was fully awake and cooperative for the placement of the adjustable suture. Afterward, the patient was brought to an upright position and the cover test was performed to check the deviation and diplopia. Adjustments were made as needed until there was no deviation or diplopia. The conjunctiva was secured with 8–0 vicryl sutures using interrupted technique.
Outcome Measurement
A successful motor outcome is defined as a vertical deviation equal to 4 prism diopters (PD) or less and a horizontal deviation equal to 10 PD or less in the primary gaze.10
A successful sensory outcome was defined as no diplopia in primary position.
Continuous variables are presented as mean ± standard deviation (SD). Continuous non-normal distributions are presented as median, quartile 1 (Q1), and quartile 3 (Q3). The motor and sensory success rates between the surgeries involving one-to-four muscles were compared using the Chi-square test followed by an estimated odd logistic regression analysis. Statistical analyses were performed using SPSS software (version 23 for Windows). For all the tests, p < 0.05 was considered to be significant.
Results
Of the 90 patients included in this study, the mean age of those undergoing strabismic surgery was 56.6 ± 10.1 years old, with a male-to-female ratio of 1:1. Thirty-nine patients had a history of orbital decompression surgery. All patients developed diplopia before undergoing strabismus surgery. Mean follow-up time was 33.7 ± 11.8 months. In our study, there were 19 patients underwent one-muscle surgery under TA and the others underwent one-to-four muscle surgery under GA.
Mean preoperative vertical deviation was hypertropia from SR restriction measuring 23.1 ±11.9 PD at distance and 18.6 ± 9.7 PD at near, and hypotropia from IR restriction measuring 24.3 ±10.5 PD at distance and 23.6 ± 11.1 PD at near. Mean preoperative horizontal deviation was esotropia from MR restriction measuring 27.5 (20, 35) PD at distance and 30 (16, 40) PD at near and exotropia from LR restriction measuring 12 (10, 25) PD at distance and 12 (10, 25) PD at near, as shown in Table 1.
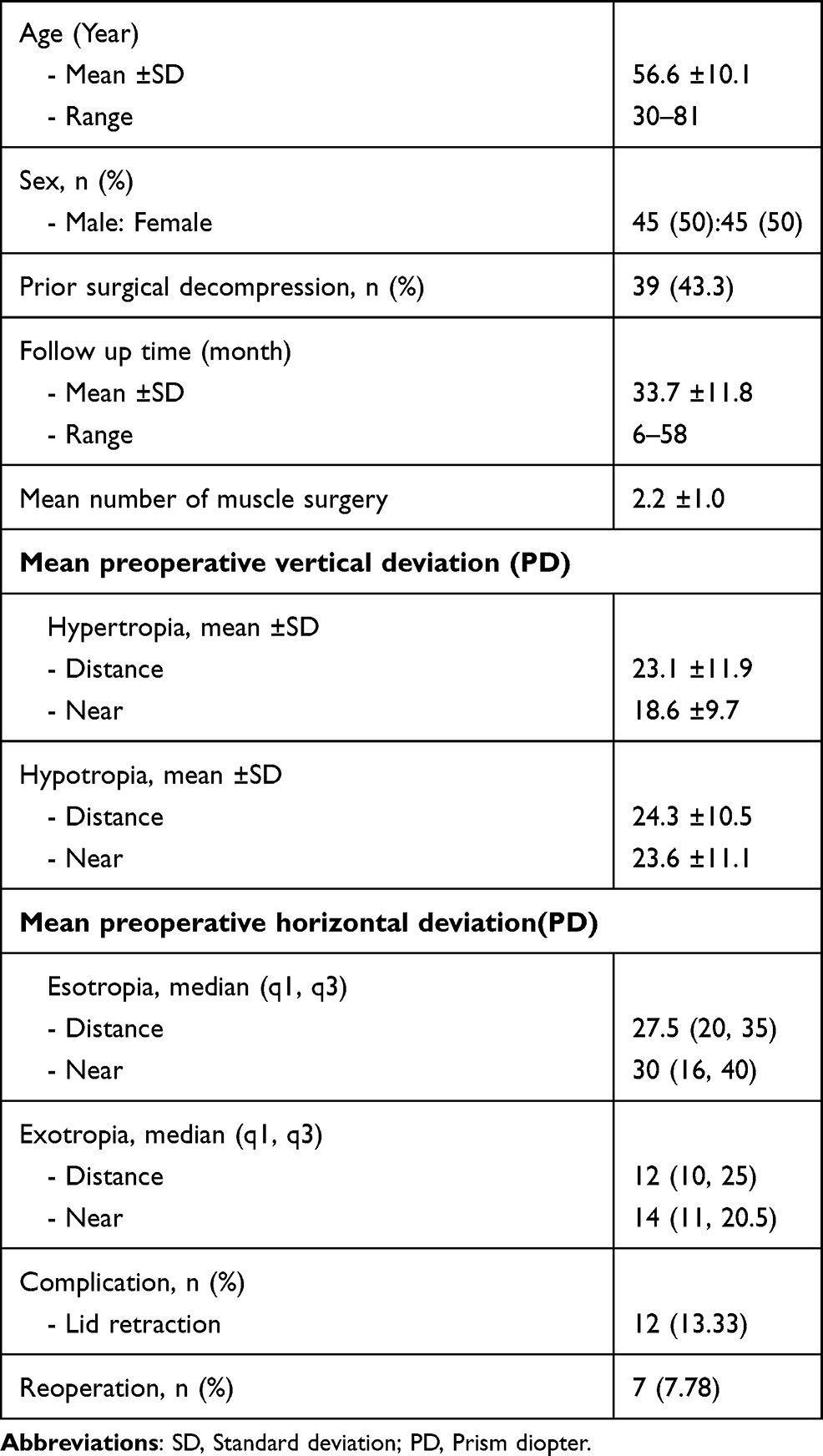 |
Table 1 Demographic Data of TED Patients |
Ninety patients underwent surgery involving one-to-four muscles, as shown in Table 2. The mean number of muscles involved in surgery was 2.2 muscles. In TED, IR was the most common restrictive muscle as assessed by FDT, followed by MR, SR, and LR. In one-muscle surgery, for TED patients with preoperative hypotropia measuring 26.8 ± 6.3 PD at distance and 25.4 ± 9.7 PD at near, IR recession procedure was performed (80.77%). Final alignment for the IR recession procedure was residual hypotropia measuring 2.1 ± 3.3 PD at distance and 2.0 ± 3.1 PD at near. In two-muscle surgery, unilateral IR and MR recession procedure was the most common procedure performed (36.84%). If there were more than two restrictive muscles involved, three-muscle surgery was chosen to adjust muscles in both eyes. In four-muscle surgery, all TED patients underwent bilateral MR recession and bilateral IR recession procedures. The preoperative and postoperative alignments were hypotropia (21.4 ± 12.8 PD at distance and 19.1 ± 12.1 PD at near) and esotropia (42.5 ± 16.3 PD at distance and 38.9 ± 19.9 PD at near). The final alignment was residual hypotropia (0.3 ± 6.8 PD at distance and 1.2 ± 7.7 PD at near) and esotropia (3.1 ± 10.0 PD at distance and 2.9 ± 9.6 PD at near).
 |
Table 2 Surgery by Intraoperative Relaxed Muscle Positioning with Adjustable Suture Technique of TED Patients |
Following the intraoperative relaxed muscle positioning with adjustable suture technique, there was motor and sensory success in all muscle surgery groups. In the one-muscle surgery group, motor success was found in 22 of 26 patients (84.62%), and sensory success was found in 22 of 26 patients (84.62%). Similarly, motor success was achieved in 31 of 36 eyes (81.58%), and sensory success was found in 32 of 36 eyes (84.21%) in the two-muscle surgery group. The three-muscle surgery and four-muscle surgery groups demonstrated lower motor success (75.00% and 64.29%, respectively) and lower sensory success (75.00% and 78.57%, respectively), as shown in Table 3. However, the comparative outcomes of motor success and sensory success were not statistically different among groups (p = 0.58 and 0.84).
 |
Table 3 Outcome of Motor and Sensory Success One to Four Muscles Surgery by Intraoperative Relaxed Muscle Positioning with Adjustable Suture Technique in TED |
Reoperations were necessary in seven patients (7.78%). A second surgery addressed the same restrictive muscle. Details of these patients are shown in Table 4. Demographic information of the seven patients includes male predominance (5/7), smoking risks including smoker and second-hand smoker (5/7), euthyroid state (7/7), varied number of two-to-four muscle surgery, and history of previous orbital decompression (5/7). Lid retractions were found in 12 patients postoperatively (13.33%).
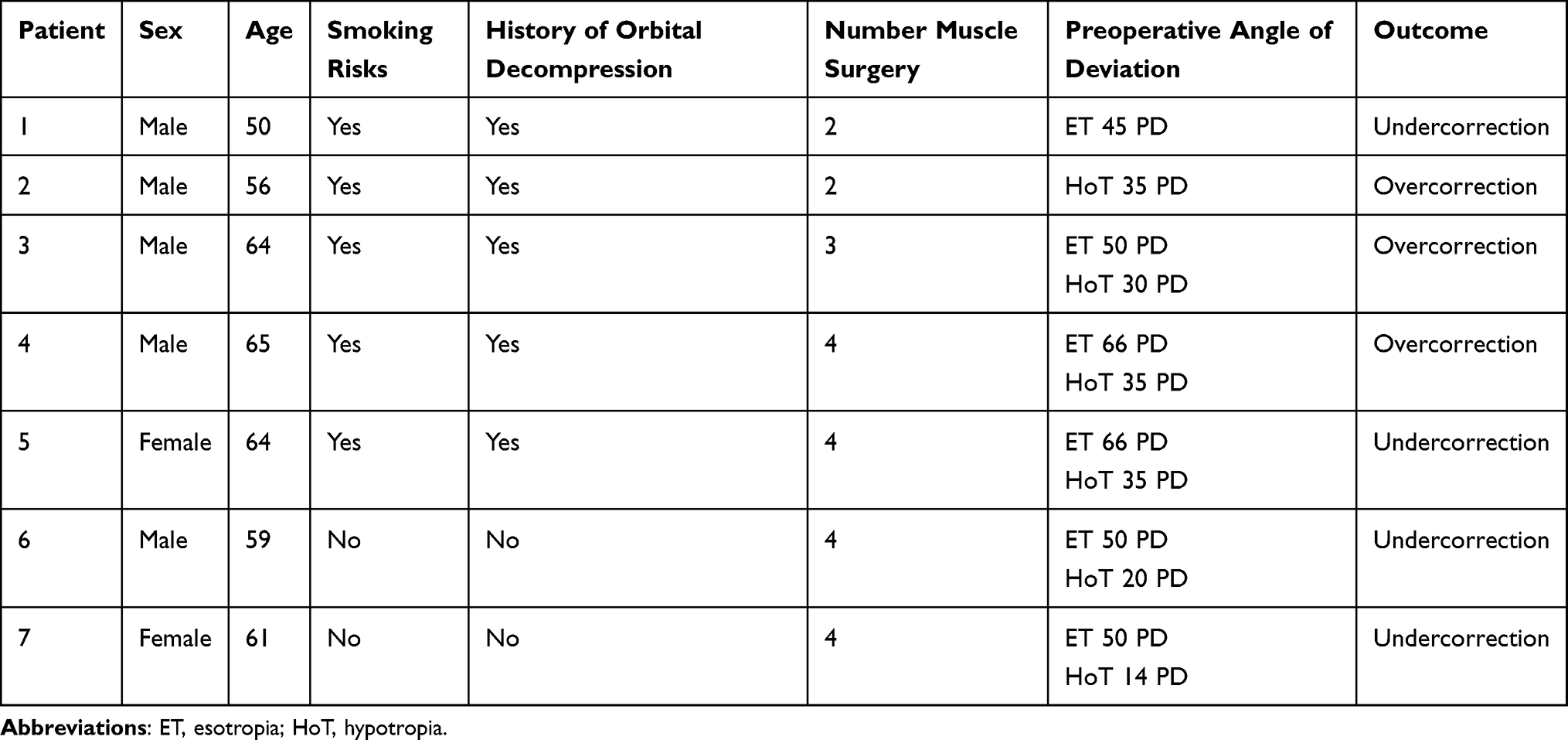 |
Table 4 Details of Patients Who Required Reoperations |
Discussion
The present study included 90 TED patients with diplopia who underwent the intraoperative relaxed muscle positioning with adjustable suture technique. Our study demonstrated an overall motor success rate ranging from 64.29% to 81.58%, which is compatible with other series8–10 that evaluated the intraoperative relaxed muscle positioning technique. The success rates for three previous studies were 74% for Nguyen et al,8 66% for Thomas and Cruz,9 and 74% for Benjamin et al.10 Our technique involved FDT before and after full relaxation of the restrictive muscle. We believed that the corrective cause of the restrictive muscle corrected the diplopia and treated both horizontal and vertical deviations. The nomogram-based approach for pediatric strabismus might not be suitable for TED patients and could not correct vertical deviation by IR restriction. The success rates for nomogram-based strabismus repairs in TED patients vary from 38% to 82%.6,11 Moreover, we reported a longer follow-up period (33.7 ± 11.8 months) and performed an analysis of the ultimate outcomes.
The motor success among surgeries involving one-to-four muscles exhibited a decrease as the number of muscles involved increased. The decision regarding the number of muscles to include in the surgery depended on the number of restrictive muscles and angle of deviation. Jellema et al12,13 compared the outcomes of IR and SR in TED and found less decrease in depression and lower dose-effect response in their combined recession group, despite the higher amount of muscle recession. The study13 also reported a lower dose-effect response in the bilateral MR recession group. In patients with a large angle of deviation, bilateral MR recession should be performed. To treat TED with multiple muscle restrictions and larger angle of deviation, we performed two-to-four muscle surgery. Patients with one-to-two restrictive muscles reached successful motor outcomes of up to 80%, while patients with three to four restrictive muscles saw a success rate of about 75%. However, the success rates among the different number of muscle surgeries did not show statistical significance.
There was no standard sensory success criterion for the surgery. One criterion defined success as having no diplopia in primary and reading positions and used a graded scale that included designations such as excellent, good, acceptable, and failure.10 Another criterion used a tool to quantify binocular single vision free of diplopia.14,15 In our study, recorded single binocular vision in primary position ranged from 75.00% to 84.62%, which is higher than that of several previous studies,10,14,15 which varied from 58% to 74%. These results might be because only the primary position was recorded, and owing to the retrospective nature of the study, we could not provide all records of other sensory measurements. Our surgical technique also provided excellent sensory outcomes with no statistically significant differences among one-to-four muscle surgeries.
Reoperation rates for TED surgery range from 5% to 45%.4,6 In our study, we observed a reoperation rate of 7.78%. Benjamin et al10 reported factors that may be predictive of the need for reoperation, including the history of orbital decompression, diplopia status, and larger angles of strabismus. In our study, the need for reoperation was found to be high in patients with male sex, smoking risks, history of decompression surgery, more than one-muscle surgery, and large angle deviation.
Complications of intraoperative relaxed muscle technique include muscle slippage because of the fibrotic nature of rectus muscles, globe rupture when positioning for suturing onto the sclera, or lower lid retraction after IR recession due to its relationship with the lower lid retractors. Using our technique, we found no muscle slippage or globe rupture during the procedures. Lower lid retractions were found in 13.33% of cases, despite the dissection of tissue from IR when performing our technique.
Conclusion
We suggest that the use of the intraoperative relaxed muscle positioning technique might be a successful option for the correction of TED-associated strabismus. Furthermore, this technique could be performed in one-to-four muscle surgery, which yields successful motor and sensory outcomes. This study’s limitations include its retrospective nature, which led to incomplete sensory data for some patients. Future prospective studies are warranted in order to obtain all sensory data.
Acknowledgment
We thank Edanz (www.edanz.com/ac) for editing a draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eckstein AK, Johnson KT, Thanos M, et al. Current insights into the pathogenesis of Graves’ orbitopathy. Horm Metab Res. 2009;41(6):456–464.
2. Harrad R. Management of strabismus in thyroid eye disease. Eye. 2015;29:234–237.
3. Skov CM, Mazow ML. Managing strabismus in endocrine eye disease. Can J Ophthalmol. 1984;19:269–274.
4. Dyer JA. The oculorotary muscles in Graves’ disease. Trans Am Ophthalmol Soc. 1976;74:425–456.
5. Dagi LR. Management of graves myopathy: understanding and managing vertical strabismus from thyroid eye disease. J AAPOS. 2018;22:252–255.
6. Kaus DJ, Bullock JD. Treatment of thyroid ocular myopathy with adjustable and nonadjustable suture strabismus surgery. Trans Am Ophthalmol Soc. 1993;91:67–84.
7. Evans D, Kennerdell JS. Extraocular muscle surgery for dysthyroid myopathy. Am J Ophthalmol. 1983;95:767–771.
8. Nguyen VT, Park DJ, Levin L, et al. Correction of restricted extraocular muscle motility in surgical management of strabismus in graves’ ophthalmopathy. Ophthalmology. 2002;109:384–388.
9. Thomas SM, Cruz OA. Comparison of two different surgical techniques for the treatment of strabismus in dysthyroid ophthalmopathy. J AAPOS. 2007;11:258–261.
10. Benjamin P, Nicholson BP, De Alba M, et al. Efficacy of the intraoperative relaxed muscle positioning technique in thyroid eye disease and analysis of cases requiring reoperation. J AAPOS. 2011;15:321–325.
11. Flanders M, Hastings M. Diagnosis and surgical management of strabismus associated with thyroid-related orbitopathy. J Pediatr Ophthalmol Strabismus. 1997;34:333–340.
12. Jellema HM, Saeed P, Groenveld L, et al. Outcome of inferior and superior rectus recession in Graves’ orbitopathy patients. Orbit. 2015;34:84–91.
13. Jellema HM, Saeed P, Braaksma-Besselink Y, et al. Unilateral and bilateral medial rectus recession in Graves’ orbitopathy patients. Strabismus. 2014;22:182–187.
14. Nassar MM, Dickinson AJ, Neoh C, et al. Parameters predicting out of strabismus surgery in the management of Graves’ ophthalmopathy. J AAPOS. 2009;13:236–240.
15. Mocan MC, Ament C, Azar NF. The characteristics and surgical outcomes of medial rectus recessions in Graves’ ophthalmopathy. J Pediatr Ophthalmol Strabismus. 2007;44:
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.