Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
The OPTION Scale: Measuring Patients’ Perceptions of Shared Decision-Making in the Kingdom of Saudi Arabia
Authors Alrawiai S ![]() , Aljaffary A
, Aljaffary A ![]() , Al-Rayes S
, Al-Rayes S ![]() , Alumran A
, Alumran A ![]() , Alhuseini M, Hariri B
, Alhuseini M, Hariri B ![]()
Received 23 July 2020
Accepted for publication 13 October 2020
Published 30 October 2020 Volume 2020:13 Pages 1337—1346
DOI https://doi.org/10.2147/JMDH.S273340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sumaiah Alrawiai, Afnan Aljaffary, Saja Al-Rayes, Arwa Alumran, Mishael Alhuseini, Bayan Hariri
Department of Health Information Management & Technology, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam 34212, Saudi Arabia
Correspondence: Sumaiah Alrawiai
Department of Health Information Management & Technology, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam 34212, Saudi Arabia
Email [email protected]
Background: Involving patients in the decision-making process is now widely accepted as appropriate and ethical during consultations, particularly when several options are available. The aim of this study is to measure the patients’ perceptions of shared decision-making practices during clinical encounters in Saudi Arabia.
Methods: This study employs a quantitative cross-sectional design. The OPTION scale was translated to Arabic. The questionnaire’s content validity was assessed using an expert panel review. The questionnaire was then administered to 291 participants through online recruitment.
Results: Participants reported positive perceptions of shared decision-making practices in Saudi Arabia. The lowest perceived shared decision-making scores were from patients who visited the internal medicine department (f = 2.163, P = 0.009). Participants who received care from female physicians reported significantly higher levels of involvement in the shared decision-making process compared to male physicians (t = − 2.732, P = 0.007). Although the majority of the participants in the study were from Eastern Province, this province documented the lowest mean perceived decision-making score by the patients compared to other provinces within Saudi Arabia (f = 3.613, P = 0.007). Female participants in the study had a higher shared decision-making score than the male participants (t = − 3.644, P < 0.0001).
Conclusion: Generally, the study results confirmed that shared decision-making in the Saudi health system includes significant patient involvement. Interventions that enhance the culture of shared decision-making in Saudi Arabia are necessary to ensure better adherence to treatment plans and thus better health outcomes.
Keywords: shared decision-making, patient-centered care, patient experience measure
Background
Involving patients in the decision-making process is now widely accepted as appropriate and ethical during consultations, particularly when several options are available.1 Several studies and systematic reviews have shown that adopting a shared decision-making (SDM) approach results in positive outcomes such as improved patient satisfaction and adherence to treatment plans, especially when compared to the traditional paternalistic way.2–4 SDM has been defined as an approach where clinicians and patients make decisions together using the best available evidence. Patients are encouraged to think about the available screening, treatment, or management options and the likely benefits and harms of each so that they can communicate their preferences and help select the best course of action for them.5
In addition to the SDM approach, other approaches are practiced in clinical settings. One such approach is the paternalistic approach, which used to be the most common approach used by doctors.6,7 In this approach, the doctor controls the consultation, and the patient’s role is simply to answer the doctor’s questions.6 This means that the doctor usually dominates the consultation, both regarding the actual length of talking and in relation to the level of control, which is why it is usually referred to as a doctor-centered consultation.6 Another approach is the informed choice approach, in which the patient makes the final decision and the doctor usually acts as a guide who helps the patient to arrive at their preferred choice.8
These three approaches are usually viewed as being located on a single spectrum, with the paternalistic approach being at one end of the spectrum and the informed choice approach at the opposite end.8 By contrast, SDM is commonly seen as the middle ground between the “two extremes” of paternalism and informed choice.9 Patients usually prefer SDM.10,11
The main issue is the actual implementation of SDM in clinical settings.1 However, one way to help with implementation is by looking at the SDM approach and view it as a process.12 Charles et al identified three steps in the decision-making process: “information exchange, deliberation about treatment options and deciding on the treatment to implement.” These steps show the importance of presenting and discussing the different treatment options with the patient, using language the patient can understand and comprehend. The different options can be presented using a variety of techniques, such as decision trees, to help ensure that the patient has clearly understood what each treatment entails and the possible consequences that could result from each option.12,13
SDM is especially important with chronic conditions, considering that the patient would need to self-manage themselves and adopt certain lifestyle changes; therefore, their input and preferences are important to ensure that these changes are acceptable to the patient over the long-run and doable.14
In the case of the Kingdom of Saudi Arabia (KSA), health concerns have arisen because of its social and cultural characteristics.15 The discovery of oil and the dispersal of wealth have led to shift in burden of disease.16 For instance, most people now rely on cars for transportation and so are less physically active than previously, leading to higher incidences of non-communicable diseases, such as obesity, diabetes mellitus, and cardiovascular disease. Ischemic heart disease is now the main cause of death (16.4% of total deaths) in KSA.17 In addition, patients’ expectations have been increased in KSA,18 which might be resulted from the improved education and literacy levels (94.4% of 15- to 24-year-olds in 2013;19). One of the few studies conducted on this topic in Saudi Arabia found that the majority of the respondents (57%) preferred the shared decision-making approach compared to the paternalistic approach (28%) and the informed approach (14%).20 All these factors increased the importance of assessing the level of SDM in KSA. Without such an evaluation of the decision-making process, patients’ preferences will not be obtained and thus physicians’ will not know what style their patients’ preferred in order to employ it during consultations. Therefore, the development and application of a valid assessment tool can facilitate the practice of SDM and can be seen as the first step that needs to be taken before adopting the SDM approach.21–23
According to a systematic review conducted by Gärtner et al, 2018,24 there are several SDM-related assessment tools available in the literature, including PPC scale to assess patient desire for involvement in making medical decisions;25 CollaboRATE to assess the extent of SDM in clinical encounter;26 and SMDMQ to assess shared medical decision process;27 and Dyadic OPTION scale28 to asses perceived patient involvement in shared decision-making; and the OPTION scale to assess the overall SDM process.26 This scale was developed to measure how much doctors involved their patients in the decision-making process by observing and rating a consultation. In this study, the scale was used to assess patients’ perceptions of the consultation, rather than the doctor’s perceptions, as was the case in a number of studies.24,25 This scale was selected from many other measures because it has been validated by a number of studies worldwide and thus is one of the most common scales used to measure SDM, so it was chosen as the best option for this study.30,31
The aim of this study is to measure the patients’ perceptions of shared decision-making practice during clinical encounters in KSA.
Methods
Study Design
This is a cross-sectional study performed to assess the patient perception on the shared decision-making practice by their physician and whether they were involved in the process.
Participant
Non-probability snowball sampling technique was used to recruit the study participants through distributing the survey online to the public using social media applications. The survey targeted the participant’s last clinic visit. The participants included in the study were adults aged 19 years old or older with a previous visit to the doctor that they could recall.
Variables
Independent variables in the study include patients demographic characteristics, physician’s demographic characteristics, and type and specialty of clinic, while the dependent variable is the patient’s shared decision-making score.
Data Sources/Measurement
The OPTION scale consists of 12 items was used to collect the patients perceptions about their involvement in the decision-making process, the scale is developed by Elwyn et al 2003.28–31
Because the target population is the Saudi public, the scale was translated into Arabic. A forward–backward translation process was conducted to ensure the conceptual equivalence of the scale in Arabic and English, by measuring the instrument’s linguistic validity.32 Furthermore, content and face validity were tested using an expert panel review and interviews with a sample from the general public.
Five experts were involved in establishing content validity.32 The panel were selected using purposive sampling technique and recruited from the Public Health Department at Imam Abdulrahman Bin Faisal University. The experts in this context were those who have written a number of publications or have significant work experience in the field,33 such as academics in health services research who have experience in designing healthcare-related questionnaires. A modification was conducted on the scale following the feedback received. Later on, content and face validity of the modified scale was tested by interviewing 25 members from the general public. The participants were recruited from one of the hospitals in the eastern region of Saudi Arabia using convenient sampling techniques. They have been asked to read the questionnaire carefully and provide their feedback on the clarity and relevancy of the content and the scale overall layout.
The internal consistency reliability of the scale was also tested using the Cronbach’s alpha. A rule of thumb for interpreting the Cronbach’s alpha Likert scale questions is the following; if the value of alpha is >0.9 = Excellent, >0.8 =Good, >0.7 = Acceptable, >0.6 = Questionable, >0.5 poor and < 0.5 = unexpectable.34
Bias
Recall bias could have been introduced, as the data rely solely on the patients recollection of their latest visit to a health facility.
Study Size
The rule of thumb advocated by Comrey and Lee35 was used in this study, where, 100 participants = fair, 200 participants =good, 500 participants = very good, and >1000 participants = excellent. The total number of completed surveys in this study was 291 participants.
Quantitative Variables
The shared decision-making process was assessed through a continuous score by computing the score of all 12 items within the scale, with higher scores indicating better shred decision-making.
The patient demographic characteristics assessed in the study included age, gender, occupation (whether health-related or not), education level, nationality, marital status, current region of residence, whether the patient has health insurance and its type, and the patient’s perception of his/her general health.
Information about the patient’s last clinical visit was measured, including the type of hospital/clinic (whether public or private), the gender of the treating doctor, and the department or specialty the visit was for (eg, obstetrics and gynecology, emergency, or ear, nose, and throat).
Statistical Methods
Statistical Package for Social Science (SPSS) version 25 was used to conduct the statistical analyses.36 The summary statistics are presented as counts and percentages of categorical variables and as measures of central tendency for continuous variables.
The shared decision-making score is a normally distributed variable according to the skewness and kurtosis criteria of normality,37 the shared decision-making score variable was normally distributed. Thus, parametric tests were used. Analysis of variance (ANOVA) and t-tests were used to conduct bivariate analyses.
Further, multivariable linear regression analysis was conducted to find the magnitude of association between the outcome variables (SDM) and the significant variables in the bivariate analysis.
Results
Scale Validity
Invitation email was sent to five experts asking them to participate in the assessment of the content validity of the scale. All of them responded to the invitation. The assessment of the content validity showed that all items had an acceptable Item content validity index (I-CVI) with a score above 0.80, which was considered as excellent.38 Also, the finding revealed an S-CVI/UA= 0.90 and S-CVI/Ave= 0.98, which reflect an adequate and satisfactory content validity.38,39 Based on these results, few changes have been made to the questionnaire.
Overall, for both the Arabic and English versions, the clarity, ability to answer questions, and consistency mean of the face validity form responses was calculated and results in out of 4 the scores was 3.5 and above for all of the 12 items of the questionnaire. As a result, no changes were made. The interviews with the general public that were conducted to measure face and content validity show that there was no need to modify the questionnaire content. Moreover, the internal consistency results show that the scale has an excellent reliability level (alpha = 0.935). The Cronbach’s alpha of the scale if an item deleted was ranged from (alpha = 0.927 to alpha = 0.937). Therefore, there was no item need to be deleted.
Participants
A total of 367 participants completed the questionnaire, of whom 59 did not answer all of the scale questions. These were excluded from the final data set. In addition, 17 records had missing demographic information, so these were excluded as well. The final number of completed records came from 291 patients.
Descriptive Data
Most of the participants indicated that the hospital they last visited was affiliated with the private sector (n = 136, 47%), while only 5% visited teaching hospitals (n = 16). Most of the patients’ last visits were to the emergency department (n = 73, 25%), followed by obstetrics and gynecology (n = 39, 13%), while the fewest visits in this study were to the ophthalmology, cardiology, and cardiac surgery departments (n = 4, 1%, each). Most of the physicians in the study were men (n = 172, 59%).
The majority of patients in the study were women (n = 119, 66%), and most of the patients were aged 30–39 years old (n = 97, 33%). Almost all of the patients in the study were Saudi (n = 285, 98%). Only 1% of patients in the study had an intermediate degree as their highest educational qualification (n = 4), while 63% had a bachelor’s degree (n = 183). The majority of participants in the study were employed in a non-health-related sector (n = 174, 60%), and 82 participants were unemployed (28%). Most of the participants in the study were married (n = 230, 79%), while 58 were not married (19%).
All of the researchers in this study are from the Eastern Province, and most of the participants were from the same province (n =257, 88%). Almost half of the participants had health insurance (n = 130, 45%), and the most common health insurance type in the study was type A or VIP (n = 54, 19%). Lastly, when participants were asked about their general health, most of them indicated that their health was excellent (n = 98, 34%) or very good (n = 102, 35%).
Outcome Data
The shared decision-making score is calculated by computing the results of the OPTION scale, with higher scores indicating better perceived shared decision-making. The shared decision-making variable is normally distributed with a mean of 44.40 (SD= 8.848), maximum score is 60 while the minimum is 12 (Skewness= −.924, Kurtosis= 1.028). Table1 shows responses to all the items in the OPTION scale.
 |
Table 1 Variable Distribution |
Main Results
The type of clinic significantly influenced the patients’ perception about their shared decision-making experience (Surgery x= 47.3,8 Pediatrics x= 47.9,7 Internal Medicine x= 38.3,11 [f = 2.163] p=0.009) (Table 2 and Figure 1).
 |
Table 2 Associations Between Mean Shared Decision-Making Score and Clinic and Physician Information |
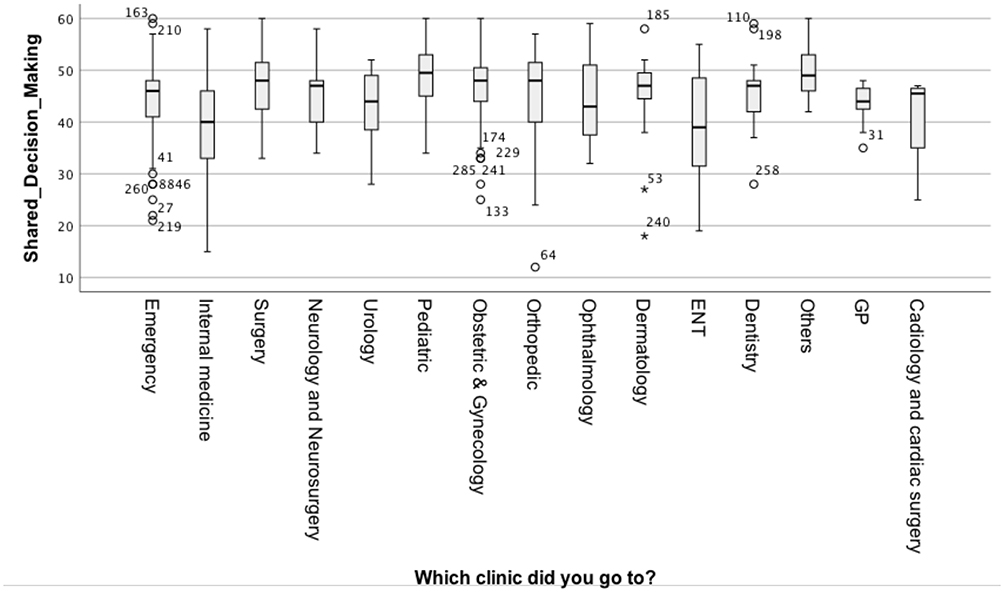 |
Figure 1 Shared decision-making score and type of clinic. |
The gender of the physician influenced the patient’s perceived shared decision-making experience significantly (t = −2.732, P = 0.007). Although the majority of physicians in the study were men, the mean shared decision-making score for female physicians was significantly higher than that of male physicians, according to the patients’ perceptions (Table 2).
Patient gender was significantly associated with their perceived shared decision-making experience (t = −3.644, P < 0.0001). Female participants in the study had a higher shared decision-making score than the male participants did (Table 3). Lastly, although most of the participants in the study were from Eastern Province, this province had the lowest mean shared decision-making score, which was significantly different from those of other regions in Saudi Arabia (f = 3.613, P = 0.007) (Table 3).
 |
Table 3 Associations Between Mean Shared Decision-Making Score and Patients’ Demographic Characteristics |
Multivariable linear regression in Table 4 shows a significant model (Prob > f = 0.0001, R-squared = 0.1736, Adj R-squared= 0.1124). Patient’s gender remained significant in the multivariable linear regression model (bfemale patient= 2.905, t= 2.52, P-value= 0.012). Patients attending Internal medicine clinic and pediatrics clinics have significantly different mean perceived SDM scores compared to other clinics (binternal medicine=−5.147, t= −2.59, P-value= 0.01, and bpediatrics= 4.906, t= 1.97, P-value= 0.049, respectively). Patients from the Southern region have significantly lower mean SDM score compared to other regions in the multivariable regression model (bSouthern Region= −14.791, t= −2.34, P-value= 0.02). While physician’s gender is no longer significant when added in the model (bfemale physician= 1.387, t= 1.19, P-value= 0.234).
 |
Table 4 Linear Regression Analysis to Account for the Magnitude of Association of the Shared Decision-Making Score and Other Variables in the Study |
Discussion
A key aspect of patient-centered care is clinicians’ willingness to share healthcare decisions with patients. The questionnaire results from the current research make significant empirical contributions to the Saudi literature because perceptions of involvement in decision-making have rarely been investigated.
Generally, the study results confirmed that a good deal of patient involvement exists in shared decision-making in the Saudi health system. Many studies have explained the importance of shared decision-making in terms of adherence to treatment plans, health outcomes, and satisfaction with care.26,40,41 According to a systematic literature review,42 patients who are well-informed about their treatment plan options and therefore make decisions with support from their doctors are more likely to adhere to treatment plans, thus increasing the probability of better health outcomes – a core goal in healthcare. The results of this study give preliminary evidence that the Saudi health system is in a good position regarding shared decision-making models in terms of patients’ perceptions. In other countries with a long-standing interest in shared decision-making, such as the UK and the USA, the progress in achieving shared decision-making is still slow.5,43 These differences between countries in shared decision-making score might be due to the variance in patients’ expectations of the healthcare providers.
Based on the study findings, the shared decision-making score was associated with three factors, including the department at which the participants received care during their last visit; their physicians’ gender; and the participants’ personal characteristics, most clearly their gender.
By department, the results revealed that participants who received care from the pediatric department, as compared to from the other departments, reported the highest shared decision-making score. This difference could be due to the strict legislation to ensure child healthcare safety in the Saudi health system. The national accreditation body, named CEBAHI, has a specific standard called Care for Minors mandating specific policies and procedures to ensure safe healthcare in pediatrics departments.44 Moreover, the difference could be explained by the fact that parents are probably concerned about their children’s care.45 Thus, they do not want to lose the opportunity to ask questions, discuss treatment options for their child, and provide their own perspectives on the selected treatment plan, including about the possible side effects of the prescribed medicine. These are all considered to be key components of the shared decision-making process. Positive perceptions of involvement in shared decision-making in pediatric departments have already been supported by literature.46
Conversely, participants who received care at cardiology and cardiac surgery departments reported a low shared decision-making score, which means they perceived themselves as less involved in shared decision-making. This might be explained by the fact that cardiac patients might need to make an immediate life-threatening decision, such as open-heart surgery, which makes their physicians follow a paternalistic approach during the shared decision-making process. However, this was not the case in other studies that supported shared decision-making for chronic conditions,14 as explained earlier, and some reporting that cardiologists usually involve cardiac patients in decision-making processes, especially patients with critical disease.47 In Saudi Arabia, the leading cause of death is cardiovascular disease. Evidence suggests that the more involved cardiac patients are in shared decision-making, the better their adherence to treatment plans and therefore their health outcomes will be.48 Thus, further investigations of shared decision-making practices in cardiac care are needed in Saudi Arabia to ensure better adherence to treatment plans as well as reduce hospital admissions due to cardiac diseases. Interventions that enhance the culture of shared decision-making in cardiac care in Saudi Arabia are necessary to ensure better adherence to treatment plans and thus better health outcomes. One of these interventions could include giving cardiologists tools (eg booklets, websites, and videos) that patients could view after the patients’ clinical encounters to make their final decisions.49 It should be noted that although the sample size is very small for these particular patients’ group. The severity of their condition and it’s being the leading cause of death in Saudi Arabia, we felt it was important to highlight these findings. Policy makers may also want to provide training to improve cardiologists’ ability to involve patients in decision-making processes in Saudi Arabia.
Interestingly, significant differences in patient perceptions of their involvement in shared decision-making were found according to the physician’s gender. Patients who received their care from a female physician reported higher involvement in shared decision-making compared to those who received care from male physicians. Similar results arose from another meta-analysis revealing that female physicians provide better communication and take more time with their patients as compared to their male colleagues.50 With regard to the situation in Saudi Arabia in general and this study in particular, most of the participants in this study were women. Saudi culture might influence the female patients’ intention to ask and challenge male physicians due to their desire to remain polite and non-confrontational. Saudi society advocates women avoiding arguments with men to show respect, this point was supported by study done by.20 Moreover, in healthcare, practices in Saudi hospitals are determined by gender rules, and people usually demand same-gender healthcare providers.51
The patient’s gender also showed differences in shared decision-making score. Female patients had higher scores than the male patients did. This has also been reported in a previous study conducted in Italy.52 This result could have been due to the nature of women, as they may have been more concerned about their health and might have therefore discussed the treatment options with their physician in detail.53
Finally, it is important to address some of this study’s limitations, which might have affected its results. Firstly, this study was conducted using convenience sampling with a small sample size, thus affecting the representativeness of the participants to the whole population of Saudi Arabia. Secondly, only linguistic, content and face validity were tested for the used scale which might affect the accuracy of the collected data. More validation work needs to be conducted if this scale will be used in the future researches (ie construct validity of the scale). Thirdly, there was a limited sample size for some of the clinic (ie cardiology clinic), which might affect the study finding. Finally, the questionnaire was distributed online via several social media platforms, which might have caused sample bias by neglecting populations with less access to the Internet.
With regards to suggestions to future studies, a qualitative study would be important for digging deeper into the reasons behind the positive or negative perceptions of shared decision-making, especially in some departments such as cardiac care. Moreover, it is important to investigate the patients’ expectations and preferences regarding their involvement in shared decision-making processes and its influence on patients’ health-related decisions.
Disclosure
No potential conflicts of interest was reported by the authors.
References
1. Stiggelbout AM, Pieterse AH, De Haes JC. Shared decision making: concepts, evidence, and practice. Patient Educ Couns. 2015;98(10):1172–1179. doi:10.1016/j.pec.2015.06.022
2. Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Making. 2015;35(1):114–131. doi:10.1177/0272989X14551638
3. Colligan E, Metzler A, Tiryaki E. Shared decision-making in multiple sclerosis. Mult Scler. 2017;23(2):185–190. doi:10.1177/1352458516671204
4. Boss EF, Mehta N, Nagarajan N, et al. Shared decision making and choice for elective surgical care: a systematic review. Otolaryngol Head Neck Surg. 2016;154(3):405–420. doi:10.1177/0194599815620558
5. Elwyn G, Laitner S, Coulter A, Walker E, Watson P, Thomson R. Implementing shared decision making in the NHS. BMJ. 2010;341:c5146. doi:10.1136/bmj.c5146
6. Sandman L, Munthe C. Shared decision making, paternalism and patient choice. Health Care Anal. 2010;18(1):60–84. doi:10.1007/s10728-008-0108-6
7. Chin JJ. Doctor-patient relationship: from medical paternalism to enhanced autonomy. Singapore Med J. 2002;43(3):152–155.
8. Elwyn G, Edwards A, Mowle S, et al. Measuring the involvement of patients in shared decision-making: a systematic review of instruments. Patient Educ Couns. 2001;43(1):5–22. doi:10.1016/S0738-3991(00)00149-X
9. Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60(3):301–312. doi:10.1016/j.pec.2005.06.010
10. Baars JE, Markus T, Kuipers EJ, Van Der Woude CJ. Patients’ preferences regarding shared decision-making in the treatment of inflammatory bowel disease: results from a patient-empowerment study. Digestion. 2010;81(2):113–119. doi:10.1159/000253862
11. Marahrens L, Kern R, Ziemssen T, et al. Patients’ preferences for involvement in the decision-making process for treating diabetic retinopathy. BMC Ophthalmol. 2017;17(1):139. doi:10.1186/s12886-017-0526-z
12. Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49(5):651–661. doi:10.1016/S0277-9536(99)00145-8
13. Elwyn G, Edwards A, Eccles M, Rovner D. Decision analysis in patient care. The Lancet. 2001;358(9281):571–574. doi:10.1016/S0140-6736(01)05709-9
14. Peek ME, Drum M, Cooper LA. The association of patient chronic disease burden and self-management requirements with shared decision making in primary care visits. Health Serv Res Manag Epidemiol. 2014;1.
15. De Nicola E, Aburizaiza OS, Siddique A, Khwaja H, Carpenter DO. Obesity and public health in the Kingdom of Saudi Arabia. Rev Environ Health. 2015;30(1):191–205.
16. Memish ZA, Jaber S, Mokdad AH, AlMazroa MA, Murray CJL, Al Rabeeah AA. Burden of disease, injuries, and risk factors in the Kingdom of Saudi Arabia, 1990–2010. Prev Chronic Dis. 2014;11(1):1–12. doi:10.5888/pcd11.140176
17. Mokdad AH, Jaber S, Aziz MIA, et al. The state of health in the Arab world, 1990–2010: an analysis of the burden of diseases, injuries, and risk factors. The Lancet. 2014;383(9914):309–320. doi:10.1016/S0140-6736(13)62189-3
18. Almutairi K, Moussa M. Systematic review of quality of care in Saudi Arabia. Saudi Med J. 2014;35(8):802–809.
19. World Bank. Literacy rate, adult total (% of people ages 15 and above) [online]. The World Bank; 2018. Available from: https://data.worldbank.org/indicator/SE.ADT.LITR.ZS?locations=SA.
20. AlHaqwi A, AlDrees T, AlRumayyan A, et al. Shared clinical decision making. A Saudi Arabian perspective. Saudi Med J. 2015;36(12):1472–1476. doi:10.15537/smj.2015.12.13682
21. Elwyn G, Edwards A, Kinnersley P. Shared decision-making in primary care: the neglected second half of the consultation. Br J Gen Pract. 1999;49(1):477–482.
22. Charles C, Gafni A, Whelan T. Self-reported use of shared decision-making among breast cancer specialists and perceived barriers and facilitators to implementing this approach. Health Expect. 2004;7(1):338–348. doi:10.1111/j.1369-7625.2004.00299.x
23. Bae JM. Shared decision making: relevant concepts and facilitating strategies. Epidemiol Health. 2017;39(1):e2017048. doi:10.4178/epih.e2017048
24. Gärtner FR, Bomhof-Roordink H, Smith IP, Scholl I, Stiggelbout AM, Pieterse AH. The quality of instruments to assess the process of shared decision making: a systematic review. PLoS One. 2018;13(2):e0191747. doi:10.1371/journal.pone.0191747
25. Bradley JG, Zia MJ, Hamilton N. Patient preferences for control in medical decision making: a scenario-based approach. Fam Med. 1996;28(7):496–501.
26. Elwyn G, Barr P, Grande S, Thompson R, Walsh T, Ozanne E. Developing CollaboRATE: a fast and frugal patient-reported measure of shared decision making in clinical encounters. Patient Educ Couns. 2013;93(1):102–107. doi:10.1016/j.pec.2013.05.009
27. Chang C. Developing the first validity of shared medical decision making questionnaires in Taiwan. Glob J Med Res. 2014;14(2):8–15.
28. Melbourne E, Sinclair K, Durand M-A, Légaré F, Elwyn G. Developing a dyadic OPTION scale to measure perceptions of shared decision making. Patient Educ Couns. 2010;78(2):177–183. doi:10.1016/j.pec.2009.07.009
29. Elwyn G, Edwards A, Wensing M, Hood K, Atwell C, Grol R. Shared decision making: developing the OPTION scale for measuring patient involvement. Qual Saf Health Care. 2003;12(2):93–99. doi:10.1136/qhc.12.2.93
30. Hirsch O, Keller H, Muller-Engelmann M, Gutenbrunner MH, Krones T, Donner-Banzhoff N. Reliability and validity of the German version of the OPTION scale. Health Expect. 2012;15(4):379–388. doi:10.1111/j.1369-7625.2011.00689.x
31. Goss C, Fontanesi S, Mazzi MA, et al. Shared decision making: the reliability of the OPTION scale in Italy. Patient Educ Couns. 2007;66(3):296–302. doi:10.1016/j.pec.2007.01.002
32. Rogers R, Bender SD. Clinical Assessment of Malingering and Deception.
33. Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35(6):382–385. doi:10.1097/00006199-198611000-00017
34. George D, Mallery P. SPSS for Windows Step by Step: A Simple Guide and Reference. 11th Update.
35. Comrey AL, Lee HB. A First Course in Factor Analysis. Hillsdale, NJ: Erlbaum; 1992.
36. IBM Corp. IBM SPSS Statistics for Macintosh.
37. West SG, Finch JF, Curran PJ. Structural Equation Models with Nonnormal Variables: Problems and Remedies. Newbery Park, CA: Sage; 1995.
38. Polit D, Beck C. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
39. Shi J, Mo X, Sun Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012;37(2):152–155.
40. Ong LM, de Haes JC, Hoos AM, Lammes FB. Doctor-patient communication: a review of the literature. Soc Sci Med. 1995;40(7):903–918. doi:10.1016/0277-9536(94)00155-M
41. Elwyn G, Tilburt J, Montori V. The ethical imperative for shared decision-making. Eur J Pers Cent Healthc. 2013;1(1):129–131. doi:10.5750/ejpch.v1i1.645
42. Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219–226. doi:10.1159/000126073
43. Eliacin J, Salyers MP, Kukla M, Matthias MS. Factors influencing patients’ preferences and perceived involvement in shared decision-making in mental health care. J Ment Health. 2015;24(1):24–28. doi:10.3109/09638237.2014.954695
44. Alhajjaj FS, Aldamigh AS. Assessment of readiness of academic emergency departments in the central region of Saudi Arabia to receive a sick child. Int J Health Sci (Qassim). 2017;11(3):4–8.
45. Jackson C, Cheater FM, Reid I. A systematic review of decision support needs of parents making child health decisions. Health Expect. 2008;11(3):232–251. doi:10.1111/j.1369-7625.2008.00496.x
46. Hubner LM, Feldman HM, Huffman LC. Parent communication prompt to increase shared decision-making: a new intervention approach. Front Pediatr. 2018;6:60. doi:10.3389/fped.2018.00060
47. Burton D, Blundell N, Jones M, Fraser A, Elwyn G. Shared decision-making in cardiology: do patients want it and do doctors provide it? Patient Educ Couns. 2010;80(2):173–179. doi:10.1016/j.pec.2009.10.013
48. Hess EP, Coylewright M, Frosch DL, Shah ND. Implementation of shared decision making in cardiovascular care: past, present, and future. Circ Cardiovasc Qual Outcomes. 2014;7(5):797–803. doi:10.1161/CIRCOUTCOMES.113.000351
49. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
50. Roter DL, Hall JA, Aoki Y. Physician gender effects in medical communication: a meta-analytic review. JAMA. 2002;288(6):756–764. doi:10.1001/jama.288.6.756
51. AlYaemni A, Theobald S, Faragher B, Jehan K, Tolhurst R. Gender inequities in health: an exploratory qualitative study of Saudi women’s perceptions. Women Health. 2013;53(7):741–759. doi:10.1080/03630242.2013.829169
52. Gualano M, Bert F, Passi S, et al. Could shared decision making affect staying in hospital? A cross-sectional pilot study. BMC Health Serv Res. 2019;19(1):174. doi:10.1186/s12913-019-4002-8
53. Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. 2016;17:38. doi:10.1186/s12875-016-0440-0
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.