Back to Journals » Hepatic Medicine: Evidence and Research » Volume 13
The Need for Alternatives to Liver Biopsies: Non-Invasive Analytics and Diagnostics
Authors Neuberger J ![]() , Cain O
, Cain O ![]()
Received 21 February 2021
Accepted for publication 19 May 2021
Published 14 June 2021 Volume 2021:13 Pages 59—69
DOI https://doi.org/10.2147/HMER.S278076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gerry Lake-Bakaar
James Neuberger,1 Owen Cain2
1Liver Unit, Queen Elizabeth Hospital, Birmingham, B15 2TH, UK; 2Department of Cellular Pathology, Queen Elizabeth Hospital, Birmingham, B15 2TH, UK
Correspondence: James Neuberger
Liver Unit, Queen Elizabeth Hospital, Birmingham, B15 2TH, UK
Tel +44 7827299254
Email [email protected]
Abstract: Histology remains essential for the diagnosis and management of many disorders affecting the liver. However, the biopsy procedure itself is associated with a low risk of harm to the patient and cost to the health services; samples may not be adequate and are subject to sampling variation. Furthermore, interpretation often depends on the skill of the pathologist. Increasingly, new techniques are becoming available that are altering the indications for liver biopsy. Many diseases of the liver can be diagnosed and managed using serological and radiological techniques; the degree of fibrosis and fat can often be assessed by serological or imaging techniques and the nature of space occupying lesions defined by serology, imaging and use of liquid biopsy. However, these techniques, too, are subject to limitations: sensitivity and specificity is not always adequate for diagnosis or management; some techniques are expensive and often also require expert interpretation. Although there may be less need for liver biopsy today, histology remains the gold standard as well as an essential tool for the diagnosis and management of many conditions, especially where there are multiple pathologies, or where a diagnosis cannot or has not been made by alternative approaches. Until less invasive techniques become more reliable and accessible, liver histology will remain a key investigation.
Keywords: imaging, liquid biopsies, multiple liver pathology, unknown pathology, non-invasive tests
Introduction
Liver biopsy is required when clinically important information about the diagnosis, prognosis or management of a patient cannot be obtained by safer means, or for research purposes.1 Percutaneous or transvenous approaches are usually used, although there are other approaches available (such as laparoscopic, endoscopic or open biopsy). In some situations, fine needle aspiration may provide enough material for a diagnosis.
Role of Liver Biopsy and Need for Alternative Approaches to Aid Diagnosis and Management
The examination of liver tissue remains a gold standard for many aspects of diagnosing and treating patients with suspected liver disease and evaluation of liver lesions. As with all investigations, there are limitations with histology, which are discussed below. The development of newernon-invasive tests (NITs) has given the clinician information that was previously available only by evaluation of histology, although these tests have their own limitations. The clinician, therefore, has an increasing armamentarium of investigations available, each with their own strengths and weaknesses.
Limitations of Liver Biopsy
Although liver biopsy has played and continues to play a key role in the diagnosis and management of patients with abnormal liver tests and with liver diseases, there are some limitations.
Safety and Complications
While liver biopsy is a safe procedure, it is associated with some morbidity and even mortality. Death is very rare after liver biopsy but is reported in between 0.05% and 0.1%.1–3 The estimates of death vary in part because of the varying definitions of biopsy-related death, the indications and clinical characteristics, better understanding of hemostasis and the biopsy needle and approach used.
Estimates of complications vary but recent estimates suggest bleeding of any kind occurs in up to 11% of image-guided liver biopsies: major bleeding episodes are reported in between 0.1% and 4.6% and minor bleeding events in up to 10% of biopsies.1,3,4 The overall reported rate of bleeding is generally considered to be less than 2%. The risk of bleeding is affected by several factors including age of patient, indication, in-patient status, co-morbidities, degree of coagulopathy, presence of malignancy, type of needle used, route of biopsy, diameter of needle, number of passes and operator experience.1–4
Other complications include pain which may be present in up to 84% and severe pain in around 20%, biliary sepsis, perforation of organs leading to pneumothorax, hemothorax, perforation of abdominal organs (especially gall bladder and colon) which may lead to bile peritonitis, bacteremia, abscess, sepsis, haemobilia, neuralgia, and rarely ventricular arrhythmia with transvenous biopsy.
Adequacy of Biopsy Size
The specimen must be of sufficient size for histopathological interpretation. As portal tracts and hepatic veins are around 0.8 mm apart, full assessment requires a biopsy with a diameter of approximately 1 mm. The Royal College of Pathologists5 grades the quality of the biopsy as:
good: total core length >20 mm
compromised: total core length 10−20 mm
inadequate: total core length <10 mm.
The adequacy of the tissue obtained will depend in part on the type and size of needle and the approach adopted (percutaneous, transvenous or endoscopic ultrasound assisted); thus, one retrospective study reported that only 20% specimens were adequate for histological diagnosis and 24% were inadequate.6
Sampling Variation
Sampling variation, sometimes erroneously termed sampling error, occurs when there is variation in histological patterns in different parts of the liver or where different parts of the liver are affected differently by the same pathological process. Thus, Ratziu analyzed 51 paired liver biopsies taken to evaluate non-alcoholic fatty liver disease (NAFLD) and reported that there was substantial agreement for the grade of steatosis; moderate agreement for hepatocyte ballooning and perisinusoidal fibrosis and for Mallory bodies, but there was only slight agreement for acidophilic bodies and lobular inflammation.7 The discordance rate for the presence of hepatocyte ballooning was 18%, and ballooning would have been missed in one quarter of patients had only one biopsy been done. Six of 17 patients with bridging fibrosis on one sample had only mild or no fibrosis on the other. Others have reached similar conclusions in the sampling variation in NAFLD that may affect the degree of staging.8,9 The inherent intra-hepatic heterogeneity of fibrosis in chronic biliary disease increases sampling variation in biopsies of these conditions. For example, in examining paired biopsies from explanted liver from 50 patients with primary biliary cholangitis (PBC), Garrido found considerable variation in the range of stages of fibrosis, when using a simulated liver biopsy.10 The same fibrosis stage was assigned to the 30 specimens examined but greater discrepancy when whole section scanning was used, specimens. In those with Hepatitis C virus (HCV) infection, Regev and colleagues examined the histology of samples taken from the left and right lobes: they found that one quarter of 124 patients had a difference of at least one grade, and one third had a difference of at least one stage between the right and left lobes.11 In 18 patients, cirrhosis was described in one lobe, while stage 3 fibrosis was in the other. Comparable conclusions were drawn from another study where patients had two liver biopsies for HBV which showed a significant difference between the samples in terms of histological activity index but not fibrosis.12
Inter and Intra-Observer Variation
Interpretation of liver histology is often complex, relying on the skill, experience and knowledge of the pathologist, and it is not surprising that there will be some degree of variation between pathologists and on repeated examination. Studies have shown that intra-observer variation is low, with good concordance, although the degree of concordance varies with feature assessed; thus, in one study on biopsies from those with NAFLD, the κ-statistic was 1 for fibrosis and steatosis and 0.735 for lobular inflammation.9 Similar conclusions can be drawn for inter-observer variation. For example, in a paired study of 50 biopsies taken from patients with NAFLD, inter-rater agreement on adult cases was assessed and the κ statistics were 0.84 for fibrosis, 0.79 for steatosis, 0.56 for hepatocellular injury and 0.45 for lobular inflammation. Agreement on the diagnostic category was 0.61.13 Comparable data has been found in other conditions, such as alcohol-related liver disease and chronic viral hepatitis.14,15 The use of digitalization may allow for a more objective measure of fibrosis. Another study of 145 Japanese patients showed assessment of the agreement between pathologists showed that concordance was best for steatosis, moderate for ballooning and fibrosis and worst for lobular inflammation.16
However, neither sampling variation nor the observed inter-pathologist variation is a valid reason for discounting the value of liver histology. It is to be expected that different parts of the liver, with different blood supply, will show variation, in a similar manner to a skin rash that rarely affects the entire body surface. Equally, inflammation, fibrosis and fatty infiltration are continuous variables with no robust and validated objective measure of where to draw a line between shades of, say, mild and moderate inflammation, so it will be a matter of judgement whether to label the degree mild or moderate; equally, distinction between advanced fibrosis and cirrhosis may be a matter of opinion and judgement. Histopathology is not unique in showing inter- and intra-personal variation, while other branches of liver medicine show similar degrees of significant variation.17 However, in many cases, such variation is of only limited clinical significance.
Expert analysis: The interpretation of liver histology is complex and, as with other areas of histopathology, even those who are well experienced in the field do not always agree.18,19 In a series of 1265 liver biopsies sent for specialist expert review, Paterson et al found differences between the original and review diagnosis in 59% of cases, the majority of which were judged to have impacted upon patient management.20 It should not be surprising that similar variations in interpretation exist in other areas where the operator relies on imaging.21–23 Use of external validation and audit may help reduce variations in interpretation. However, to derive the best outcome for patients, the pathologist needs to be aware of the clinical situation, the results of serological and other investigations there needs to be close collaboration between pathologist and clinician.1,24
Tumor Seeding
There have been concerns that a liver biopsy taken in an area of malignancy may result in tumor seeding and so render ineffective potentially curative procedures (such as liver transplantation or resection for primary liver cancers). However, the risk of tumor seeding is not great. Thus, in a retrospective analysis, Chen found that in a median follow-up of 25 months, there were no recorded cases of seeding in 155 patients with documented breast cancer, but three of the 279 patients with colo-rectal cancer (CRC), had clear evidence of biopsy-related seeding.25 Slightly higher rates of dissemination of CRC were reported in two earlier studies, with recurrence rates of up to 17% with and one showed recurrence being associated with worse outcomes.26,27 For hepatocellular carcinoma, a recent meta-analysis concluded reported that the reported incidence of needle-tract seeding varies between 0% and 7.7%, with a median of 2.7%.28
Alternatives to Liver Biopsy
There are several alternatives to taking a liver biopsy. The most appropriate methodology depends on the clinical question, and currently there is no single technology that is able to replicate all the benefits of the biopsy. As will be discussed, all non-invasive methodologies are associated with limitations of sensitivity, specificity and observer variation.
Assessment of Fibrosis and Cirrhosis
Assessment of fibrosis has been revolutionized by the widespread use of Fibroscan and, to a lesser extent, by the use of serological markers. In NAFLD, there are several methods of assessing fibrosis. Of the tests based on serological tests, the most commonly used include the Enhanced Liver Fibrosis (ELF) test (calculated from levels of hyaluronic acid, amino-terminal propeptide of type III procollagen (PIIINP), and tissue inhibitor of metalloproteinase 1 (TIMP-1)), NAFLD Fibrosis Score (calculated from age, body mass index, blood glucose, platelet count, albumin, and aspartate aminotransferase (AST) to alanine aminotransferase (ALT) ratio) and the Fibrosis (FIB)-4 Score (calculated from age, AST, ALT, and platelet count). Other serological tests include APRI, Fibrotest, Forns Index, HepaScore, and the more recent NIS4 algorithm.29 Overall, these have reasonably good specificity and but lower sensitivity to significant fibrosis and cirrhosis: specificity ranging from 60% to 90% and sensitivity 27–87% and AUROC ranging from 0.74 to 0.90.30 Likewise, Loomba and Adams concluded that simple serum-based tests (such as FIB-4) and the NAFLD-Fibrosis Score tend to be less accurate than those more expensive serum tests that incorporate direct measures of fibrogenesis or fibrolysis.31 They also stated that while such tests are valuable for excluding advanced fibrosis or cirrhosis, they are not sufficiently predictive when used in isolation.31
Imaging is being increasingly used to determine the presence of fibrosis and cirrhosis. There are many studies comparing the sensitivity and specificity of the different techniques. The conclusions are partly dependent on the underlying liver disease. Ultrasound is relatively poor at diagnosing or excluding cirrhosis.32 Increasingly transient elastography (TE) is being used for the detection of fibrosis and cirrhosis. The technique is easy to do, non-invasive, provides a numeric assessment not subject to individual judgement, is reproducible and the patient can be informed of the findings at the end of the procedure. However, a review concluded that transient elastography may be used as a diagnostic method to rule out liver cirrhosis in people with alcoholic liver disease and may also help in ruling out severe fibrosis (F3 or worse).33 In one study on non-alcoholic fatty liver disease (NAFLD), the authors found the AUROC values for advanced fibrosis in patients with NAFLD using APRI, FIB-4, BARD score, NFS, FibroScan M probe, XL probe, shear wave elastography (SWE), and magnetic resonance elastography (MRE) for diagnosing fatty liver were 0.77, 0.84, 0.76, 0.84, 0.88, 0.85, 0.95, and 0.96, respectively.34 MRE seems more sensitive than TE in NAFLD also.35,36 Another study looking at different modalities of assessing non-alcoholic steatohepatitis in 145 Japanese patients16 using magnetic resonance elastography, multiparametric MRI with LiverMultiScan, vibration-controlled transient elastography and 2D shear-wave elastography concluded MR liver fat and cT1 were the strongest performing individual measures and the multiparametric MRI metrics combined (cT1 and MR liver fat) were the overall best non-invasive test. For identifying fibrosis ≥ 1, MRE performed best and for assessment of steatosis ≥ 1, MR liver fat was the best.
Overall, as concluded by Roccarina and colleagues, non-invasive assessment of liver fibrosis and portal hypertension is a validated tool for the diagnosis and follow-up of patients and the combination of transient elastography and platelet count for ruling out varices needing treatment in patients with compensated advanced chronic liver disease.37 Elastography methods are more accurate than simple serum non-invasive tests but are limited by increasing rates of unreliability with increasing obesity.31 Likewise, Patel and Sebastiani concluded that despite their increased use in clinical practice, these tests were not designed to reflect the dynamic process of fibrogenesis, differentiate between adjacent disease stages, diagnose non-alcoholic steatohepatitis, or follow longitudinal changes in fibrosis or disease activity caused by natural history or therapeutic intervention.38 Furthermore, they stated non-invasive tests should be viewed as complementary to, rather than as a replacement for, liver biopsy.
In some instances, the assessment by transient elastography may be misleading, leading to a false diagnosis of advanced fibrosis: these include hepatic congestion, biliary obstruction, cholestasis, amyloidosis, inflammation, acute viral hepatitis, and benign and malignant liver lesions, as well as time after consumption of food.39 Other imaging techniques, using computerized tomography (CT) or MR and MRE have been useful but require more expensive equipment and sometimes doses of radiation.
A number of tests measuring volatile organic compounds or other metabolites have been shown to be of some benefit in staging liver disease. These include13 C-labelled breath tests, aminopyrine breath test, galactose breath test, methacetin breath test, and keto-isocaproic acid breath test, although these tests are usually of more value in evaluating the prognosis in those with cirrhosis rather than its diagnosis or etiology.40 Measurement of volatile organic compounds, such as erpinene, dimethyl sulfide, and D-limonene, in breath is another approach that may prove useful in diagnosing and managing some liver diseases.41,42 These approaches have also been termed volatomics or breath biopsy. Although many of these tests do show reasonable correlation with other tests of liver function, they are not indicated for the diagnosis of disease and are of limited value in measuring degrees of fibrosis, steatosis or inflammation.
Despite the limitations of elastography, the technology remains especially useful in monitoring the progress of diseases, such as Hepatitis C infection, and the response to treatment, when sequential imaging can be done cheaply and safely.
Assessment of Steatosis
Non-invasive diagnosis and quantification of hepatic steatosis rely predominantly on either biomarkers or imaging techniques, which are either ultrasound-based (mainly liver ultrasonography and controlled attenuation parameter (CAP)), radiological using either CT or MRI. Techniques using MRI have been developed over the last decade: multiparametric MRI refers to the use of multiple quantitative features.43 These methods also allow evaluation of more than one characteristic of the liver pathology. Such methodologies include proton density fat fraction (PDFF), magnetic resonance elastography (MRE), modified Look-Locker inversion recovery (MOLLI), diffusion-weighted imaging (DWI). Proton density fat fraction measurement by MRI is currently the most accurate and sensitive imaging method, simpler and more practical than magnetic resonance spectroscopy, but largely restricted, up to now, just to research and clinical trials. Methods such as chemical-shift-encoded MRI (CSE-MRI)-based proton density fat-fraction (PDFF) have shown promise and are more accurate than CAP but remain expensive and impractical for many clinical situations.44
The LiverMultiScan uses MRI-based imaging software and provides a quantitative assessment of liver fat and an indirect assessment of fibrosis. These technologies are still being developed and not always readily available in the clinic. Furthermore, assessment of fibrosis or fat may be affected by hepatic iron content or inflammation. Unlike Fibroscan, these measures are not immediately available but fast approaches are under development.
A recent meta-analysis of the CAP approach to assessing fat concluded that CAP can effectively recognise significant steatosis in patients with viral hepatitis but cannot grade steatosis in patients with NAFLD adequately.45
Because CT involves radiation, it is not widely used for the detection of fat. Overall, CAP, using the M probe, is a widely used technique; CT and routine ultrasound are less sensitive but helpful in detecting incidental findings of steatosis.
Some serum markers and scores have been developed and proposed as measures of hepatic fat: these include SteatoTest, Fatty Liver Index, Hepatic Steatosis Index, Lipid Accumulation Product; Index of NASH; and NAFLD Liver Fat Score. These NITs are calculated from a variety of blood analytes (including ALT, a2-macroglobulin; apolipoprotein A-1, haptoglobin, bilirubin, gamma-glutamyl transferase, total cholesterol, triglycerides and glucose) and clinical factors, such as age, gender, and BMI. Only the SteatoTest has been shown to have high accuracy compared with histological assessment. Newer studies have investigated the utility of Cytokeratin 18 and microRNAs as potential chemical biomarkers, and these may prove useful in the future. Standard liver tests are of little diagnostic value.46
Diagnosis of Liver Tumors
The diagnosis of primary liver cancer (hepatocellular carcinoma, HCC) is usually made on the basis of imaging and measurement of onco-fetal antigens (notably α-foetoprotein).47 CT performs less well than extracellular contrast-enhanced MRI or gadoxetate-enhanced MRI and all approaches are more specific for tumors larger than 2 cm in diameter. Imaging shows uptake of contrast during the arterial phase and decreased enhancement and washout during the portal phases. Thus, biopsy is not indicated for the diagnosis of HCC, if typical features are present on dynamic imaging techniques. Newer techniques may provide greater specificity and sensitivity.
Likewise, imaging is usually sufficient to characterize benign liver tumours.48,49 Imaging may require single or combined modalities, such as ultrasound (ultrasonography (US), contrast-enhanced ultrasonography (CEUS), and shear wave elastography (SWE)) and CT and MR imaging. Benign nodules, such as hemangioma, focal nodular hyperplasia and inflammatory pseudotumors of the liver are usually readily and reliably diagnosed on imaging so biopsy is rarely required. Differentiation of hepatocellular carcinoma and dysplastic nodules from benign lesions in the cirrhotic liver is especially challenging where macroregenerative nodules, siderotic nodules, arterioportal shunts, hemangiomas, pseudo-masses in chronic portal vein thrombosis and focal fatty changes may mimic neoplasia.50
The primary site of metastatic cancers to the liver can often be identified by imaging techniques using CT, MRI,18-fluorideoxyglucose positron emission tomography (18FDG-PET) and, more recently, diffusion-weighted imaging and hepato-specific contrast media, such as gadoxetic acid in MRI.51 The increasing use of artificial intelligence will further increase the sensitivity and specificity of these tests.52,53
The liquid biopsy (discussed below in the context of parenchymal liver disease) could potentially revolutionize the diagnosis and management of HCC, although the clinical application of this technology is still at an early stage.54
Diagnosis of Parenchymal Liver Diseases
The etiology of many diseases can be determined by serological tests or imaging and biopsy is not needed or helpful.1,2 For example, primary biliary cholangitis on the basis of cholestatic liver dysfunction and characteristic serological markers, and primary sclerosing cholangitis in the context of known inflammatory bowel disease, cholestatic liver dysfunction and characteristic imaging. In contrast, liver histology is considered a pre-requisite for the diagnosis of autoimmune hepatitis and should be considered when withdrawal of immunosuppression is being considered.55,56
Detection of volatile organic compound in a breath biopsy may be a useful alternative to biopsy in identifying alcohol-related liver disease, although this technology is still in the early stages of development.57
The term “liquid liver biopsy” is used to describe the analysis of components, such as microRNA, long non-coding RNA (lncRNA), circulating free DNA, circulating tumor DNA in peripheral blood and other fluids. Liquid biopsies can be used to study cancer driver gene mutations, deregulated DNA methylation, as well as miRNA levels in the diagnosis of HCC.58 Whilst this technique is best established for cancers, the liquid biopsy also has the potential for diagnosing parenchymal diseases of the liver.59–61 This area is developing rapidly and so may become the standard of diagnosis in the future. Liquid biopsy has several advantages above standards clinical tools, providing specific, dynamic and fast access information to different illnesses. Liquid biopsy can also provide information about the individual genetic state of cancers which may allow for a more precision-based approach to care. In a systematic review of 112 studies of the accuracy of liquid biopsy analysis, Chen and colleagues found that assays for circulating tumour cells and cell-free DNA might aid in predicting prognoses and monitoring hepatocellular carcinoma and assays for cell-free DNA might help detect such cancers but cautioned there is a risk of bias in these studies and stressed the need for standardization before the clinical utility of liquid biopsy analysis can be assessed in this situation.62 There remain limitations regarding the technical aspects of isolation of the biomarkers which will doubtless be resolved in the future.
In our view, liquid biopsy represents an exciting and potentially safe and effective way of diagnosing and managing parenchymal disease, but still remains some way off for routine clinical use. There will need to be more studies comparing the performance of liquid liver biopsy with current serologic, histologic and radiologic approaches to the diagnosis.
Current and Future Roles of Liver Histology
Disease Diagnosis
Parenchymal Disease
There remain indications of where liver histology is still required. In essence, these include when non-invasive diagnostic tests are conflicting, when inconclusive or unreliable, multiple etiologies are suspected, liver tests do not improve after clinical intervention or when material is required for additional diagnostic (eg molecular tests). Guidelines for the use of liver biopsy in the diagnosis of liver diseases are under regular revision, as non-invasive diagnostic approaches become more effective. A recent review is given in the Liver Biopsy Guidelines from the British Society of Gastroenterology.1 Selected indications for liver biopsy are summarized in Table 1. There are several examples where current non-invasive diagnostic techniques are inadequate for diagnosis (such as in the donor liver, liver allograft and in pediatric liver diseases).63–65 Conversely, there are several examples in the current practice where liver histology may not be necessary and generally offers little diagnostic or therapeutic benefit over other approaches (for example, in NAFLD and alcoholic hepatitis).66,67 In drug-induced liver injury, liver histology is rarely required but may be indicated when there is no resolution of abnormal liver tests on withdrawal of the putative toxin, when multiple factors may be involved (such as alcohol use) or when there remains uncertainty as to the diagnosis.68
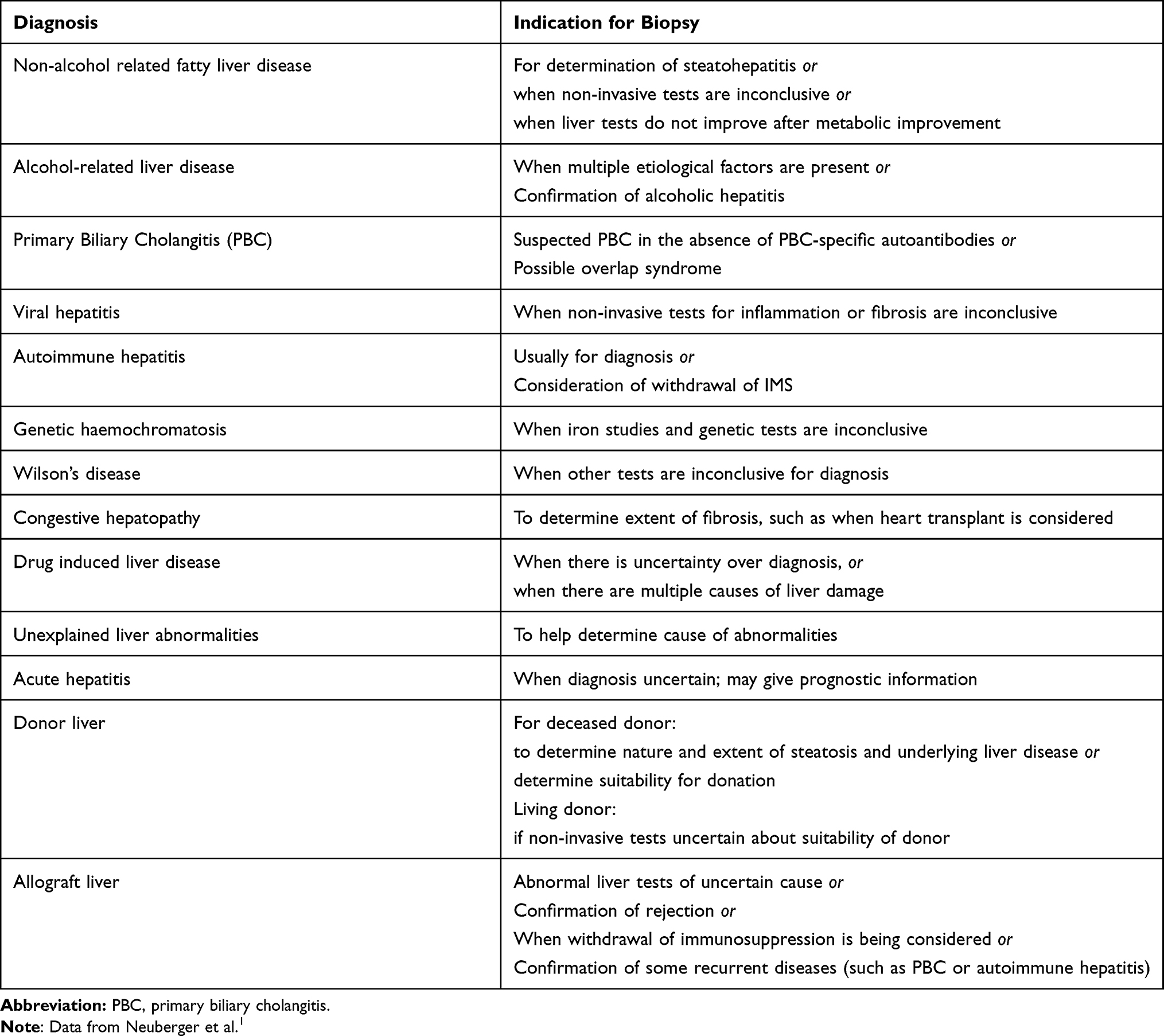 |
Table 1 Some Selected Indications for Liver Biopsy in Parenchymal Disease |
Liver Allograft Pathology
Role of histology in the liver allograft: Liver tests are unreliable as markers of liver allograft pathology.64 Indeed, the liver histology may be within normal limits when the liver biochemistry is abnormal and, conversely, may show inflammation or fibrosis when liver tests and other imaging modalities are normal.64 In the allograft, several pathologies may occur simultaneously, such as rejection (whether T-cell rejection, plasma cell hepatitis or antibody mediated rejection), reperfusion injury, viral infection, recurrence of disease, drug induced liver injury, vascular damage, for example; standard tests are not able to distinguish these causes. Of course, serological tests may help identify some of these causes. Peripheral eosinophilia has long been recognized as a potentially non-invasive marker of acute rejection, although it lacks the sensitivity or specificity to replace liver biopsy.68,69 Measurement of lymphocyte subsets and immunomodulatory molecules in peripheral blood offers a more sophisticated means of monitoring the recipient's immune response. Emerging biomarkers include soluble IL-2R and CD28, although a standardised protocol is yet to be defined.70,71 Graft-derived cell-free DNA released by damaged hepatocytes in the systemic circulation offers an alternative non-invasive marker of graft injury, akin to the liquid biopsy described above.72 Diagnosis of antibody-mediated rejection requires not only the presence of donor-specific antibodies but also the demonstration of tissue injury and complement deposition in the allograft biopsy. Reliable non-invasive AMR-specific markers of liver injury are yet to be defined, although chemokines such as CXCL9 have shown promise in the context of kidney transplantation.73
Research
Liver histology allows for further investigations to be carried out on liver tissue: for example, infiltrating cells can be characterized using immuno and other stains, cells can be cultured and grown in vitro, and patterns of collagen deposition can be studied. Analysis of circulating immune cells does not necessarily reflect those resident in the liver.74 Techniques such as second harmonic generation/two-photon excitation fluorescence (SHG/TPEF) microscopy imaging are showing great promise in characterizing architectural features of fibrosis at the individual collagen fiber level.75 Detailed spatial profiling of lymphocyte subsets within parenchymal liver disease is now possible using multiplex immunostaining and digital analysis, massively enriching the depth of information available from the biopsy.76 Indeed, digital pathology is likely to dramatically enhance the value of the liver biopsy in the coming years.77,78
Recent advances in slide scanners now allow the creation of “digital/virtual” slides that allow whole slide imaging (WSI) and additional techniques, such as combining multiphoton microscopy (MPM) with advanced clearing and fluorescent stains (Clearing Histology with MultiPhoton Microscopy (CHiMP)) or use of matrix assisted laser desorption/ionization (MALDI) mass spectrometry.79 The combination of expert evaluation, digital pathology and artificial intelligence is likely to further enhance the value of histopathology.80
Characterization of Liver Tumors
Imaging techniques alone are unable to detect or exclude the presence of features, such as microvascular invasion, tumor grade or tumor subtype. Indeed, the classification of hepatocellular adenomas is of clinical relevance and is entirely dependent on morphological and immunohistochemical assessment.81 Molecular classification can help predict the risk factors and clinical risk of benign adenomas.82 A range of special stains and immunohistochemical markers is sometimes needed for the diagnosis of HCC.47 This may change as the technologies underlying liquid biopsies improve. Furthermore, histology is also indicated when there is doubt about the nature or malignancy of the tumor.
Indications for liver histology in malignancy are shown in Table 2.
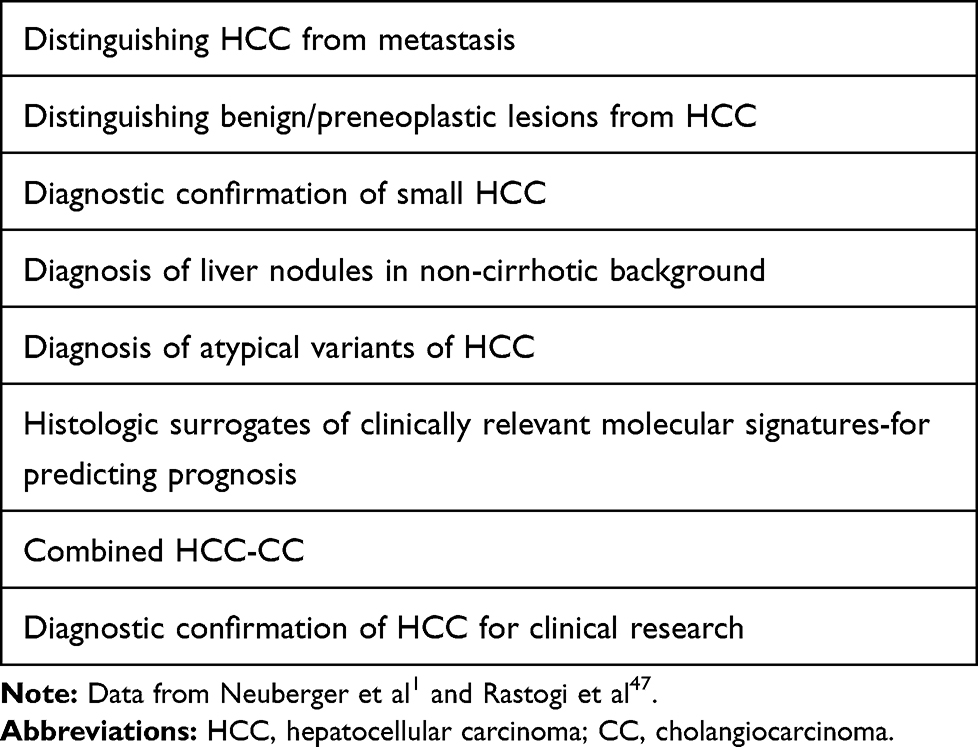 |
Table 2 Indications for Liver Biopsy in Suspected Malignant Liver Lesions |
Research
Liver biopsies will provide material for research to allow in situ characterization of cells and cellular components and isolation and culture of liver and other infiltrating cells. Immunohistochemistry can be used to identify tumour-infiltrating cells, for example, in malignancy, and allow for newer targeted approaches to treatment and a more personalized approach to treatment or better understanding of inflammatory liver disease.83 Clearly, where liver tissue is required, other than from livers donated for transplantation or research or following resection, liver biopsy is the only approach to obtaining such tissue.
Cost of Liver Biopsy and Other Tests
It is difficult to give a useful estimate of the cost of a liver biopsy as the cost will depend on many factors, such as the jurisdiction where the biopsy is done, whether it is done “blind” or under ultrasound or CT guidance and whether it is part of an admission or as a day-case. One website estimates the cost of a liver biopsy varies between US$300 and US$3500 with an average of US$1700.5,84 In our own institution, the laboratory costs of a liver biopsy are approximately £300 (US$424), to which should be added the cost of a day’s hospital stay and the cost of associated imaging;it has been estimated that the total cost of a liver biopsy in the NHS is between £497 and £553 (US$703-782). Note that the cost and the charge for a procedure will differ.
In contrast, the National Institute for Health and Care Excellence estimated in 2020 that the cost of a liver biopsy is around £500 and of a single Fibroscan between £50 and £400 (US$71-566),85 The cost of laboratory testing of serum fibrosis markers or acoustic radiation force impulse is around £199. The cost of an MRI scan of without contrast ranges between £116 and £133 (US$164-188) (a LiverMultiScan will cost about an additional £200 (US$283)) and a liver ultrasound scan costs between £40 and £49 (2018/9 figures) (US$57-69). The derivation of these figures is not always clear, so they should be used more as a guide to the relative costs.
Conclusion
Liver biopsy has been accepted as the gold standard for the diagnosis of liver disease, of many liver masses and for measuring degrees of inflammation, fibrosis and steatosis. Liver biopsy, like all other tests in medicine, has limitations, such as risk to the patient and the need for expert evaluation. Over the last few decades, non-invasive tests have become increasingly expert at characterizing aspects of liver disease and of liver masses. Although these also have limitations with respect to sensitivity and specificity, the use of artificial intelligence will also improve their diagnostic value. The liquid liver biopsy is becoming an increasingly used approach and may further reduce the need for liver biopsy. However, with the advent of digital pathology, the role of the liver biopsy is changing and is likely to have a place in the diagnosis and management of liver disease for the foreseeable future. The clinician now has more choices to help diagnose and manage patients with potential or actual liver disease; understanding the benefits, drawbacks and risks of each option will allow for a more patient-centered approach.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Neuberger J, Patel J, Caldwell H, et al. Guidelines on the use of liver biopsy in clinical practice from the British Society of Gastroenterology, the Royal College of Radiologists and the Royal College of Pathology. Gut. 2020;69:1382–1403.
2. Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD. Liver biopsy. Hepatology. 2009;49:1017–1044.
3. National Institute for Clinical Health and Excellence. What is the safety of a liver biopsy? Available from: https://www.nice.org.uk/guidance/cg100/update/CG100/documents/role-of-liver-biopsy-safety2.
4. Midia M, Odedra D, Shuster A, Midia R, Muir J. Predictors of bleeding complications following percutaneous image-guided liver biopsy: a scoping review. Diagn Interv Radiol. 2019;25:71–80.
5. Wyatt J, Hubscher SG, Bellamy C, Davies S Tissue pathways for liver biopsies for the investigation of medical disease and focal lesions. 2020. Available from: https://www.rcpath.org/asset/2921C666-0F66-4272-820C16DB2AC.
6. Fryer E, Wang LM, Verrill C, Fleming K. How often do our liver core biopsies reach current definitions of adequacy? J Clin Pathol. 2013;66:1087–1089.
7. Ratziu V, Charlotte F, Heurtier A, et al.; and the LIDO Study Group. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005;128:1898–1906.
8. Merriman RB, Ferrell LD, Patti MG, et al. Correlation of paired liver biopsies in morbidly obese patients with suspected nonalcoholic fatty liver disease. Hepatology. 2006;44:874–880.
9. Khurana S, Butt W, Khara HS, et al. Bi-lobar liver biopsy via EUS enhances the assessment of disease severity in patients with non-alcoholic steatohepatitis. Hepatol Int. 2019;13:323–329.
10. Garrido MC, Hubscher SG. Accuracy of staging in primary biliary cirrhosis. J Clin Pathol. 1996;49:556–559.
11. Regev A, Berho M, Jeffers LJ, et al. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am J Gastroenterol. 2002;97:2614–2618.
12. Ekiz F, Yuksel İ, Arikök AT, et al. Will a second biopsy sample affect treatment decisions in patients with chronic hepatitis B? Hepatol Int. 2016;10:602–605.
13. Kleiner DE, Brunt EM, Van Natta M, et al. Nonalcoholic steatohepatitis clinical research network design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41:1313–1321.
14. Bedossa P, Poynard T, Naveau S, Martin ED, Agostini H, Chaput JC. Observer variation in assessment of liver biopsies of alcoholic patients. Alcohol Clin Exp Res. 1988;12:173–178.
15. Goldin RD, Goldin JG, Burt AD, et al. Intra-observer and inter-observer variation in the histopathological assessment of chronic viral hepatitis. J Hepatol. 1996;25:649–654.
16. Imajo K, Tetlow L, Dennis A, et al. Quantitative multiparametric magnetic resonance imaging can aid non-alcoholic steatohepatitis diagnosis in a Japanese cohort. World J Gastroenterol. 2021;27:609–623.
17. Winkfield B, Aubé C, Burtin P, Calès P. Inter-observer and intra-observer variability in hepatology. Eur J Gastroenterol Hepatol. 2003;15:959–966.
18. Piepkorn MW, Longton GM, Reisch LM, et al. Assessment of second-opinion strategies for diagnoses of cutaneous melanocytic lesions. JAMA Netw Open. 2019;2:e1912597.
19. Kaswala DH, Lai M, Afdhal NH. Fibrosis assessment in Nonalcoholic Fatty Liver Disease (NAFLD) in 2016. Dig Dis Sci. 2016;61(5):1356–1364.
20. Paterson AL, Allison ME, Brais R, Davies SE. Any value in a specialist review of liver biopsies? Conclusions of a 4-year review. Histopathology. 2016;69:315–321.
21. Lakhman Y, D’Anastasi M, Miccò M, et al. Second-opinion interpretations of gynecologic oncologic MRI examinations by sub-specialized radiologists influence patient care. Eur Radiol. 2016;26:2089–2098.
22. Hatzoglou V, Omuro AM, Haque S, et al. Second-opinion interpretations of neuroimaging studies by oncologic neuroradiologists can help reduce errors in cancer care. Cancer. 2016;122:2708–2714.
23. Chalian M, Del Grande F, Thakkar RS, Jalali SF, Chhabra A, Carrino JA. Second-opinion subspecialty consultations in musculoskeletal radiology. Am J Roentgenol. 2016;206:1217–1221.
24. Reall G, Jones RL, Wyatt JI. Liver histopathology in the Yorkshire region: a network model. J Clin Pathol. 2009;62:1141–1143.
25. Chen I, Lorentzen T, Linnemann D, et al. Seeding after ultrasound-guided percutaneous biopsy of liver metastases in patients with colorectal or breast cancer. Acta Oncol. 2016;55:638–643.
26. Rodgers MS, Collinson R, Desai S, Stubbs RS, McCall JL. Risk of dissemination with biopsy of colorectal liver metastases. Dis Colon Rectum. 2003;46:454–458.
27. Jones OM, Rees M, John TG, Bygrave S, Plant G. Biopsy of resectable colorectal liver metastases causes tumour dissemination and adversely affects survival after liver resection. Br J Surg. 2005;92:1165–1168.
28. Sparchez Z, Mocan T. Contemporary role of liver biopsy in hepatocellular carcinoma. World J Hepatol. 2018;10:452–461.
29. Harrison SA, Ratziu V, Boursier J, et al. A blood-based biomarker panel (NIS4) for non-invasive diagnosis of non-alcoholic steatohepatitis and liver fibrosis: a prospective derivation and global validation study. Lancet Gastroenterol Hepatol. 2020;5:970–985.
30. Lurie Y, Webb M, Cytter-Kuint R, Shteingart S, Lederkremer GZ. Non-invasive diagnosis of liver fibrosis and cirrhosis. World J Gastroenterol. 2015;21:11567–11583.
31. Loomba R, Adams LA. Advances in non-invasive assessment of hepatic fibrosis. Gut. 2020;69:1343–1352.
32. Pavlov CS, Casazza G, Semenistaia M, et al. Ultrasonography for diagnosis of alcoholic cirrhosis in people with alcoholic liver disease. Cochrane Database Syst Rev. 2016;3(3):CD011602.
33. Pavlov CS, Casazza G, Nikolova D, et al. Transient elastography for diagnosis of stages of hepatic fibrosis and cirrhosis in people with alcoholic liver disease. Cochrane Database Syst Rev. 2015;1(1):CD010542.
34. Xiao G, Zhu S, Xiao X, Yan L, Yang J, Wu G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: a meta-analysis. Hepatology. 2017;66:1486–1501.
35. Hsu C, Caussy C, Imajo K, et al. Magnetic resonance vs transient elastography analysis of patients with nonalcoholic fatty liver disease: a systematic review and pooled analysis of individual participants. Clin Gastroenterol Hepatol. 2019;17(630–637):e8.
36. Imajo K, Honda Y, Kobayashi T, et al. A direct comparison of US and MR elastography for staging liver fibrosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2020;17:
37. Roccarina D, Rosselli M, Genesca J, Tsochatzis EA. Elastography methods for the non-invasive assessment of portal hypertension. Expert Rev Gastroenterol Hepatol. 2018;12:155–164.
38. Patel K, Sebastiani G. Limitations of non-invasive tests for assessment of liver fibrosis. JHEP Rep. 2020;20(2):100067.
39. Zhang X, Wong GL, Wong VW. Application of transient elastography in nonalcoholic fatty liver disease. Clin Mol Hepatol. 2020;26:128–141.
40. Stravitz RT, Reuben A, Mizrahi M, et al. Use of the methacetin breath test to classify the risk of cirrhotic complications and mortality in patients evaluated/listed for liver transplantation. J Hepatol. 2015;63:1345–1351.
41. Sinha R, Lockman KA, Homer NZM, et al. Volatomic analysis identifies compounds that can stratify non-alcoholic fatty liver disease. JHEP Rep. 2020;2:100137.
42. Ferrandino G, Orf I, Smith R, et al. Breath biopsy assessment of liver disease using an exogenous volatile organic compound-toward improved detection of liver impairment. Clin Transl Gastroenterol. 2020;11:e00239. doi:10.14309/ctg.0000000000000239.
43. Thomaides-Brears HB, Lepe R, Banerjee R, Multiparametric DC. MR mapping in clinical decision-making for diffuse liver disease. Abdom Radiol (NY). 2020;45(11):3507–3522.
44. Starekova J, Reeder SB. Liver fat quantification: where do we stand? Abdom Radiol (NY). 2020;45:3386–3399.
45. Petroff D, Blank V, Newsome PN, et al. Assessment of hepatic steatosis by controlled attenuation parameter using the M and XL probes: an individual patient data meta-analysis. Lancet Gastroenterol Hepatol. 2021;15:
46. Pirmoazen AM, Khurana A, El Kaffas A, Kamaya A. Quantitative ultrasound approaches for diagnosis and monitoring hepatic steatosis in nonalcoholic fatty liver disease. Theranostics. 2020;10:4277–4289.
47. Rastogi A. Changing role of histopathology in the diagnosis and management of hepatocellular carcinoma. World J Gastroenterol. 2018;24:4000–4013.
48. Belghiti J, Cauchy F, Paradis V, Vilgrain V. Diagnosis and management of solid benign liver lesions. Nat Rev Gastroenterol Hepatol. 2014;11:737–749.
49. Hu J, Zhou ZY, Ran HL, Yuan XC, Zeng X, Zhang ZY. Diagnosis of liver tumors by multimodal ultrasound imaging. Medicine (Baltimore). 2020;99(32):e21652.
50. Renzulli M, Brocchi S, Ierardi AM, et al. Imaging-based diagnosis of benign lesions and pseudolesions in the cirrhotic liver. Magn Reson Imaging. 2021;75:9–20.
51. Renzulli M, Clemente A, Ierardi AM, et al. Imaging of colorectal liver metastases: new developments and pending issues. Cancers (Basel). 2020;12:151.
52. Le Berre C, Sandborn WJ, Aridhi S, et al. Application of artificial intelligence to gastroenterology and hepatology. Gastroenterology. 2020;158(76–94):e2.
53. Lockhart ME, Smith AD. Fatty liver disease: artificial intelligence takes on the challenge. Radiology. 2020;295:351–352.
54. Trevisan França de Lima L, Broszczak D, Zhang X, Bridle K, Crawford D, Punyadeera C. The use of minimally invasive biomarkers for the diagnosis and prognosis of hepatocellular carcinoma. Biochim Biophys Acta Rev Cancer. 2020;1874:188451.
55. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: autoimmune hepatitis. J Hepatol. 2015;63:971–1004.
56. Tanaka A. Autoimmune Hepatitis: 2019 Update. Gut Liver. 2020;14:430–438.
57. Furnari M, Ahmed I, Erpecum KJ, Savarino V, Giannini EG. Breath Tests to Assess Alcoholic Liver Disease. Rev Recent Clin Trials. 2016;11:185–190.
58. Pezzuto F, Buonaguro L, Buonaguro FM, Tornesello ML. The role of circulating free DNA and MicroRNA in non-invasive diagnosis of HBV- and HCV-related hepatocellular carcinoma. Int J Mol Sci. 2018;19(4):1007.
59. Barrera-Saldaña HA, Fernández-Garza LE, Barrera-Barrera SA. Liquid biopsy in chronic liver disease. Ann Hepatol. 2021;20:100197.
60. Mann J, Reeves HL, Feldstein AE. Liquid biopsy for liver diseases. Gut. 2018;67:2204–2212.
61. Shabangu CS, Huang JF, Hsiao HH, Yu ML, Chuang WL, Wang SC. Liquid biopsy for the diagnosis of viral hepatitis, fatty liver steatosis, and alcoholic liver diseases. Int J Mol Sci. 2020;21:3732.
62. Chen VL, Xu D, Wicha MS, Lok AS, Parikh ND. Utility of liquid biopsy analysis in detection of hepatocellular carcinoma, determination of prognosis, and disease monitoring: a systematic review. Clin Gastroenterol Hepatol. 2020;18(13):2879–2902.
63. Degrassi I, Deheragoda M, Creegen D, et al. Liver histology in children with glycogen storage disorders type VI and IX. Dig Liver Dis. 2021;53:86–93.
64. Mells G, Neuberger J. Protocol liver allograft biopsies. Transplantation. 2008;85:1686–1692.
65. Oliver JB, Machineni P, Bongu A, et al. Liver biopsy in assessment of extended criteria donors. Liver Transpl. 2018;24:182–191.
66. Forrest E, Petts G, Austin A, et al. The diagnostic and prognostic significance of liver histology in alcoholic hepatitis. Aliment Pharmacol Ther. 2021;53:426–431.
67. Ajmera V, Loomba R. Imaging biomarkers of NAFLD, NASH, and fibrosis. Mol Metab. 2021;101167. doi:10.1016/j.molmet.2021.101167.
68. Sandhu N, Navarro V. Drug-induced liver injury in GI practice. Hepatology Communications. 2020;4::631–645.
69. Krenzien F, Keshi E, Splith K, et al. Diagnostic biomarkers to diagnose acute allograft rejection after liver transplantation: systematic review and meta-analysis of diagnostic accuracy studies. Front Immunol. 2019;10:758.
70. Lun A, Cho MY, Müller C, et al. Diagnostic value of peripheral blood T-cell activation and soluble IL-2 receptor for acute rejection in liver transplantation. Clin Chim Acta. 2002;320:69–78.
71. Boix F, Bolarín JM, Mrowiec A, et al. CD28 biomarker quantification and expression level profiles in CD4+ T-lymphocytes in solid organ transplantation. Transpl Immunol. 2017;42:9–17.
72. Schütz E, Fischer A, Beck J, et al. Graft-derived cell-free DNA, a noninvasive early rejection and graft damage marker in liver transplantation: a prospective, observational, multicenter cohort study. PLoS Med. 2017;14:e1002286.
73. Mühlbacher J, Doberer K, Kozakowski N, et al. Non-invasive chemokine detection: improved prediction of antibody-mediated rejection in donor-specific antibody-positive renal allograft recipients. Front Med (Lausanne). 2020;7:114.
74. Bartsch LM, Damasio MPS, Subudhi S, Drescher HK. Tissue-resident memory T cells in the liver—unique characteristics of local specialists. Cells. 2020;9:2457.
75. Soon G, Wee A. Updates in the quantitative assessment of liver fibrosis for nonalcoholic fatty liver disease: histological perspective. Clin Mol Hepatol. 2021;27:44–57.
76. Isse K, Grama K, Abbott IM, et al. Adding value to liver (and allograft) biopsy evaluation using a combination of multiplex quantum dot immunostaining, high-resolution whole-slide digital imaging, and automated image analysis. Clin Liver Dis. 2010;14:669–685.
77. Marti-Aguado D, Rodríguez-Ortega A, Mestre-Alagarda C, et al. Digital pathology: accurate technique for quantitative assessment of histological features in metabolic-associated fatty liver disease. Aliment Pharmacol Ther. 2021;53:160–171.
78. Farris AB, Moghe I, Wu S, et al. Banff Digital Pathology Working Group: going digital in transplant pathology. Am J Transplant. 2020;2392–2399.
79. Jain D, Torres R, Celli R, Koelmel J, Charkoftaki G, Vasiliou V. Evolution of the liver biopsy and its future. Transl Gastroenterol Hepatol. 2021;6:20.
80. Calderaro J, Kather JN. Artificial intelligence-based pathology for gastrointestinal and hepatobiliary cancers. Gut. 2021;70(6):1183–1193.
81. Bioulac-Sage P, Sempoux C, Balabaud C. Hepatocellular adenoma: classification, variants and clinical relevance’. Semin Diagn Pathol. 2017;34:112–125.
82. Nault JC, Paradis V, Cherqui D, Vilgrain V, Zucman-Rossi J. Molecular classification of hepatocellular adenoma in clinical practice. J Hepatol. 2017;67(5):1074–1083.
83. Gao B, Ahmad MF, Nagy LE, Tsukamoto H. Inflammatory pathways in alcoholic steatohepatitis. J Hepatol. 2019;70(2):249–259.
84. Bookimed. https://en.bookimed.com/clinics/procedure=liver-biopsy/#:~:text=Doctors%20calculate%20the%20cost%20of%20the%20Liver%20biopsy,price%20is%20%241%2C600%20and%20the%20highest%20%E2%80%94%20%243%2C500A.
85. National Institute for Health and Care Excellence. https://www.nice.org.uk/advice/mib216/resources/fibroscan-for-assessing-liver-fibrosis-and-cirrhosis-in-primary-care-pdf-2285965454907589.
86. Lu C, Rong D, Zhang B, et al. Current perspectives on the immunosuppressive tumor microenvironment in hepatocellular carcinoma: challenges and opportunities. Mol Cancer. 2019;18(1):130.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.