Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
The modern perspective for long-acting injectables antipsychotics in the patient-centered care of schizophrenia
Authors Pietrini F ![]() , Albert U
, Albert U ![]() , Ballerini A, Calò P
, Ballerini A, Calò P ![]() , Maina G, Pinna F, Vaggi M, Boggian I, Fontana M, Moro C
, Maina G, Pinna F, Vaggi M, Boggian I, Fontana M, Moro C ![]() , Carpiniello B
, Carpiniello B ![]()
Received 20 December 2018
Accepted for publication 18 March 2019
Published 30 April 2019 Volume 2019:15 Pages 1045—1060
DOI https://doi.org/10.2147/NDT.S199048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Francesco Pietrini,1 Umberto Albert,2 Andrea Ballerini,3 Paola Calò,4 Giuseppe Maina,5 Federica Pinna,6 Marco Vaggi,7 Ileana Boggian,8 Maria Fontana,4 Cesare Moro,9 Bernardo Carpiniello10,6
1Department of Mental Health and Addictions, Central Tuscany NHS Trust, Florence, Italy; 2Department of Biomedical and Neuromotor Sciences, Alma Mater Studiorum University of Bologna, Bologna, Italy; 3Department of Health Sciences, Florence University School of Medicine, Florence, Italy; 4Department of Mental Health, Azienda Sanitaria Locale Lecce, Lecce, Italy; 5Rita Levi Montalcini Department of Neuroscience, University of Torino, Torino, Italy; 6Department of Medical Sciences and Public Health, Unit of Psychiatry, University of Cagliari, Cagliari, Italy; 7Department of Mental Health and Drug Addiction ASL 3 Genoa, Azienda Sanitaria 3 Genovese, Genoa, Italy; 8Department of Mental Health, Azienda Ulss 9 Scaligera, Legnago, Italy; 9Department of Mental Health and Addictions, ASST Bergamo Ovest, Treviglio, Italy; 10Psychiatric Clinical Unit, University Hospital of Cagliari, Cagliari, Italy
Abstract: Schizophrenia is a chronic syndrome involving different clinical dimensions, and causes significant disability with a negative impact on the quality of life of patients and their caregivers. Current guidelines for the treatment of schizophrenia focus on maximizing a patient’s adaptive functioning and quality of life in a recovery-oriented approach that encourages active collaboration among patients, caregivers, and mental health professionals to design and manage a customized and comprehensive care plan. In the present study, a panel of experts (psychiatrists, psychologists, nurse, and social worker) gathered to review and explore the need for contemporary use of second-generation antipsychotic long-acting injectables (SGA LAIs) in “recovery-oriented” and “patient-centered” care of schizophrenia. Starting from the available data and from sharing personal attitudes and experiences, the panel selected three clinical dimensions considered useful in characterizing each patient: phase of disease, adherence to treatment, and level of functioning. For each clinical dimension, perspectives of patients and caregivers with regard to needs, expectations, and personal experiences were reviewed and the role of SGA LAIs in achieving shared goals examined. The experts concluded that from today’s modern perspectives, SGA-LAIs may play an important role in breaking the spiral of desocialization and functional decline in schizophrenia, thus favoring the recovery process.
Keywords: long-acting injections, antipsychotic, schizophrenia, quality of life, subjective well-being, recovery
Introduction
Schizophrenia is a chronic psychiatric syndrome involving different clinical dimensions. Positive symptoms (eg, hallucinations, delusions) occur together with negative symptoms (eg, alogia, blunted affect), along with disorganization of speech and behavior and impairment of cognitive and executive functions.1 All these symptoms cause impairment of personal, social, and occupational skills, with profound negative impact on the patient’s quality of life (QoL).2–4 Primary goals in the management of schizophrenia include not only achieving short- and long-term clinical remission but also maintaining physical and mental functioning while improving QoL and promoting the patient’s recovery.5,6 Indeed, key guidelines for the treatment of schizophrenia focus on maximizing QoL and adaptive functioning, as well as assisting patients in attaining personal life goals (eg, in employment, housing, and personal relationships).7,8
In this regard, recovery has been defined as a multidimensional construct comprising two sets of outcomes, belonging to either the “objective” or the “subjective” domain.9 Objective clinical recovery is defined by symptom severity and level of functioning, whereas subjective personal recovery refers to the patient’s QoL, self-confidence, future hopes, willingness to ask for help, reliance on others, and no domination by symptoms. The two dimensions are mutually linked, eg, better cognitive functioning leads to better social integration and lower rates of anxiety and depression.10 Therefore, in the process of extending the definition of remission and recovery, subjective outcomes have been increasingly valued as important components of full remission, encompassing clinical and functional remission together with adequate subjective well-being and QoL.11 Moreover, the fact that the available evidence indicates that personal recovery has a salutogenic effect further supports the importance of patient-centered care in schizophrenia.12,13
A recovery-oriented approach involves different professionals to allow for integrated exchange of expertise.14 This may require a team synergistically working toward the same aim, ie, to help the patient and increase his/her QoL.5 Including patients and their caregivers in the decision-making process can enhance insight into the disease, with a clear expectation of better treatments and outcomes.15 People with schizophrenia are encouraged to be part of the management team and to participate constantly in decisions regarding treatment.16 Despite their symptoms, patients can still provide information on their state of health that caregivers can supplement and contextualize.17
Given these considerations, it is surprising that a thorough evaluation of patients’ and caregivers’ attitudes toward illness, as well as their preferences regarding pharmacological and nonpharmacological treatments, has received little scientific attention.18 There are likely several reasons for this, including the fact that most psychiatrists believe that patients with schizophrenia are not reliable in assessing their subjective well-being. Part of the scarce clinical and scientific interest in the patient’s perspective may also be due to the tendency of psychiatrists to overestimate how well they know their patients, and thus to underestimate the value of asking their point of view.18,19 Conversely, from a clinical perspective, focusing on patient’s subjective experience offers precious insight into each individual’s personal recovery and into his or her strengths, weaknesses, wishes, activities, and preferences. The personal meaning that each person attributes to his/her illness and to the treatment received within his/her life context is central, to address an optimal recovery.20
The increasing interest in patients’ attitudes toward treatment is confirmed by the integration of patient-reported outcomes into the process of developing and testing new antipsychotic medications.21 Understanding the attitudes of patients and caregivers can thus represent a valuable asset in tailoring treatment to expressed needs, and has the potential to improve the therapeutic alliance and medication adherence, thereby enhancing long-term prognosis.22 The recent development of second-generation antipsychotic long-acting injectables (SGA LAIs) has increased the number of options available to personalize pharmacological treatment of schizophrenia.23 SGA LAIs are likely to fit well into the long-term, comprehensive, multimodal treatment plans that are recommended today for schizophrenia in Italy and in other countries.23 Linking the use of SGA LAIs to the goals of patients and caregivers may contribute significantly to achieving remission and recovery.24,25 In this regard, previous evidence suggests that the use of SGA LAIs is an optimal strategy to address the subjective core of a satisfying recovery from schizophrenia. In particular, maintenance treatment with SGA LAIs seems to be related to significant improvements in subjective well-being, attitudes toward treatment, and health-related QoL.25,26
In light of these considerations, the main aim of this paper was to review and explore the effect of SGA LAIs on patient and caregiver expectations of care, personal goals, and QoL. Furthermore, the impact of SGA LAIs on the “recovery-oriented” and “patient-centered” treatment of schizophrenia was evaluated, eg, how SGA LAIs can affect the sharing of therapeutic decisions, assessment of outcomes, and use of mental health–service resources (eg, time management). Toward this end, a panel of eleven experts gathered at a consensus meeting (June 26, 2017 in Milan) with the aim of representing the majority of mental health professionals (psychiatrist, psychologist, nurse, social worker) who treat patients with schizophrenia. The panel included eight psychiatrists, a psychologist, a nurse and a social worker. To be included in the panel, the experts had to have at least 10 years of experience in hospital- or community-based services. The consensus among participants was reached through discussion during the meeting, followed by email correspondence, and was based on the practical experience of the panel, as well as on a review of available literature.
A comprehensive literature search was performed using the PubMed database for biomedical English-language literature. Multiple searches were conducted combining headings and keywords for “long-acting injectable”, “antipsychotic”, “schizophrenia”, “patient-centered”, “recovery”, “recovery-oriented”, “health-related”, “quality of life”, and “subjective well-being”.
Starting from the selected data and sharing of personal attitudes and experiences, the panel selected three clinical dimensions that they considered useful to characterize each patient: phase of disease, adherence to treatment, and level of functioning. For each clinical dimension, perspectives of patients and caregivers with regard to needs, expectations, and personal experiences were reviewed and the role of SGA LAIs in achieving those specific goals examined.
Phase of disease
Each phase of schizophrenia, from the first episode (FES) to the chronic phase, corresponds to different sets of needs and expectations about the disease and its treatment (Table 1). This requires planning specific interventions that should be recovery-oriented and aimed at promoting QoL.
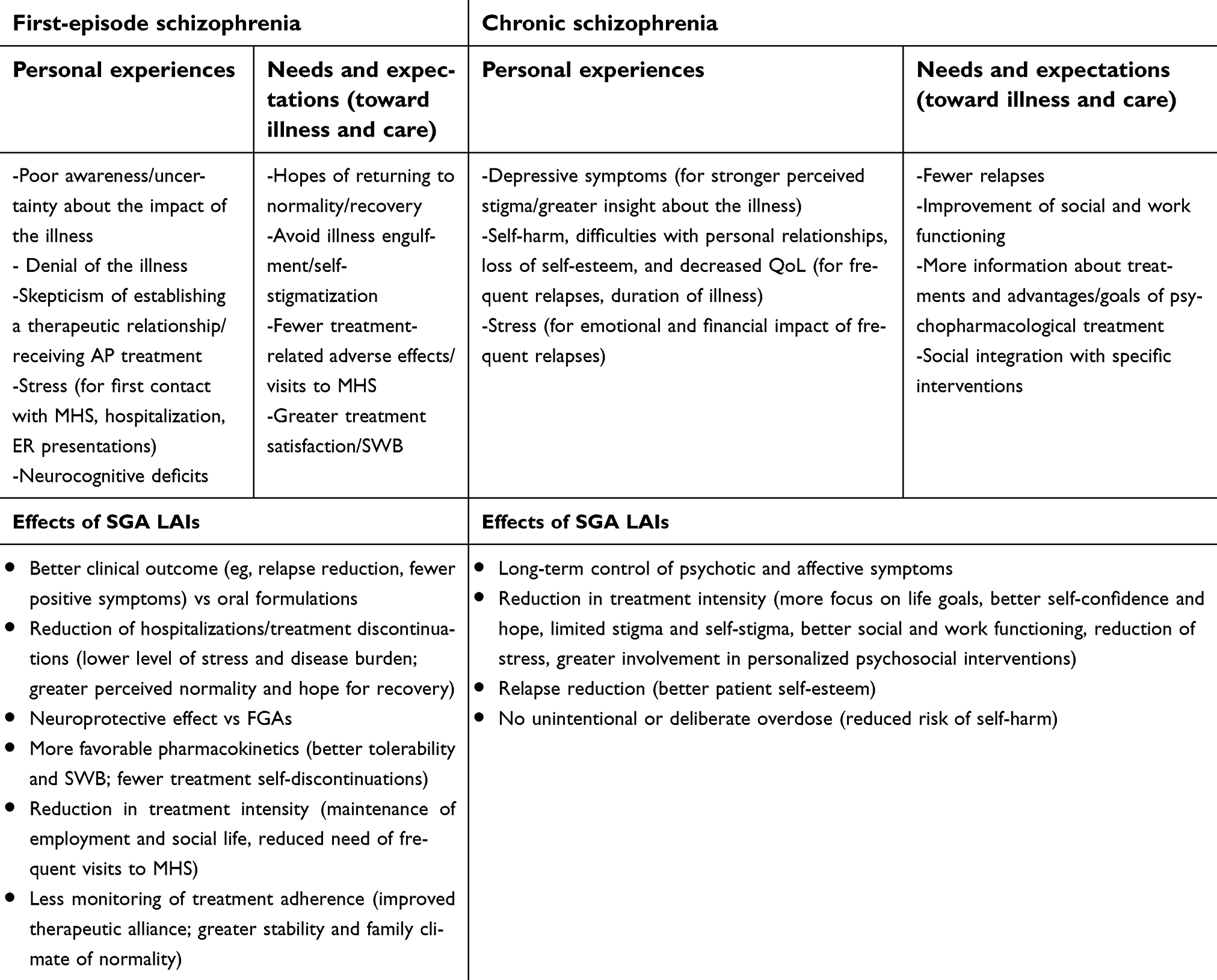 | Table 1 Phase of disease: effects of SGA LAIs on patient and caregiver needs, expectations, and personal experiences |
First-episode schizophrenia
There is increasing consensus that the early phases of psychosis represent a critical period for the treatment of schizophrenia and for its long-term prognosis.27–30 The clinical experience of the panel of experts is that patients with FES often show poor awareness of their disorder. The time between the onset of psychotic symptoms and the beginning of treatment (perhaps triggered by disturbing symptoms or social difficulties) is often characterized by a sense of uncertainty of the patient about the impact of the disease on his/her life and by his/her hopes of returning to normality with no specific interventions. These early expectations of FES patients are often reported by their caregivers,31–33 and may lead them to refuse specialized treatment to avoid stigmatization by self and others.31
Although young patients may recognize that they have some kind of “problem”, their perception of its cause and true nature is often very different from that of their psychiatrists and is permeated by personal values. Most FES patients cannot link difficulties at school or work to a specific mental condition before receiving appropriate specialized support aimed at helping them to cope with the initial stages of illness and to adapt their lifestyle appropriately.33,34 On the other hand, inadequate encounters between psychiatric services and severely disabled young patients may further exacerbate their “need” to deny their state of illness and lead FES patients to become skeptical about the possibility of establishing a therapeutic relationship and receiving help. The first contact with mental health professionals can understandably be perceived as a source of stress by patients and caregivers, especially in cases of early hospitalization due to an acute episode.
In consideration of all of these aspects, it is necessary to actively engage patients, starting with the very first contact with mental health services. This implies investing time in listening and understanding the patient’s feelings and values, in order to create a virtuous circle aimed at achieving practical and individualized goals that can in turn boost treatment adherence.31–33
With regard to adherence, it is well known that interrupting the use of antipsychotics in patients with a first episode of schizophrenia or schizoaffective disorder increases the risk of recurrence by about fivefold.35 Unfortunately, even when patients with FES have responded to antipsychotic treatment and achieved remission, their adherence to treatment is threatened by a number of different issues:
- the need for antipsychotic maintenance treatment is often put into doubt by patients who can become (overtly or covertly) nonadherent36,37
- even from the early phases of illness, FES patients may show significant neurocognitive deficits that can negatively affect adherence to treatment38,39
- FES patients often show higher sensitivity to side effects and negative subjective experiences of antipsychotic treatment, with a negative impact on adherence22
All of these factors, which are related to the characteristics of the disease at its onset and to the overall experience of treatment, can generate feelings of helplessness and impotence in FES patients.40 This can cause what is known as illness engulfment, or the feeling that the illness completely defines the totality of the person’s being, restricting all aspects of patient life, entirely redefining his/her concept of self and inducing self-stigmatization.41
Shared treatment goals and SGA LAIs in first-episode schizophrenia
As discussed, patients with FES need to avoid illness engulfment and perceive themselves as “recovered” as soon as possible. In this regard, the consistent, continuous, and stable release of antipsychotic treatment granted by LAI formulations has been associated with better clinical outcomes compared to oral formulations, which include fewer relapses, fewer positive symptoms, and better adherence.37 In particular, the reduction of hospitalizations and presentations to the ER represents a substantial advantage in terms of lower overall level of stress, disease burden, and contact with specialist care, providing advantages for the patient in terms of perceived normality and hope for recovery (Table 1).42
Since initiating antipsychotic treatment in patients with FES is associated with sustained cognitive improvement for up to 2 years,43 a treatment plan with SGA LAIs may be of significant advantage in terms of neuroprotective effect, especially compared to the use of first-generation antipsychotics (FGAs), with their recognized neurotoxicity.44 Substantial clinical evidence indicates that typical and atypical antipsychotics have diverse effects on neuronal survival and neurogenesis: while the former appear to reduce neuroprotection in the brain, the latter increase the level of BDNF and improve cell survival and neurogenesis.44
Another important point is that long-acting or extended-release antipsychotics have a narrow peak-to-trough fluctuation index and are therefore believed to be better tolerated than drugs with immediate-release formulations.45 The more favorable pharmacokinetic profile can be particularly convenient for patients in the early stages of disease who are more sensitive to treatment-related adverse effects.35,46,47 In fact, the use of SGA LAIs makes intentional self-discontinuation of treatment less frequent compared to oral formulations in patients who have doubts about continuing with their medication and are at risk of becoming nonadherent (something that is crucial to avoid in FES patients).48
Early administration of LAI antipsychotics is also reported to improve the therapeutic alliance, and the reduced need for monitoring treatment adherence allows the treatment team to focus on more patient-centered issues (such as attitudes toward life, personal feelings, and experiences) and facilitates the achievement of patient personal goals.49 LAI formulations may also allow reduction of the frequency and intensity of family/caregiver monitoring of patient treatment adherence and promote a sense of greater stability that can restore a family climate of “normality”.37 All these factors, pivoted on a stable clinical condition, make patients better suited to integrated rehabilitation programs,50 significantly improving long-term prognosis.37,51,52
Chronic schizophrenia
In the panel’s experience, patients with an extensive history of illness and multiple relapses are at risk of developing depressive symptoms, due to stronger perceived stigma and acquisition of greater insight about the course and prognosis of their illness. Frequent relapses and long duration of illness can lead to increased risk of harming themselves or others and difficulties with personal relationships, school, or work, and is associated with loss of self-esteem and decreased QoL. Illness relapses also have a negative emotional and financial impact on families and caregivers.51 Patients with chronic schizophrenia and their caregivers often report a lack of information about possible treatments, as well as about the advantages and goals of psychopharmacological treatment.18 They also express a wish to be involved in specific interventions aimed at social integration and in training and support actions for family members.53
Shared treatment goals and SGA LAIs in chronic schizophrenia
In patients with chronic schizophrenia with an extensive history of illness and multiple relapses, SGA LAIs seem to provide significant benefits in long-term control of both psychotic and affective symptoms.54 During long-term maintenance treatment, the availability of a low-frequency regimen of antipsychotic administration, eg, with SGA LAIs, can allow patients to focus on their life goals, foster self-confidence and hope, and limit the risks of stigma and self-stigma. This can help patients to improve their social and work functioning, while minimizing the risks of relapse.55 The expected greater prevention of relapse with LAI formulations may also improve patients’ self-esteem during long-term management (Table 1).43
A treatment plan with monthly or trimonthly injections of antipsychotic treatment may be preferable for many patients, as it may be less cumbersome than biweekly injections.56 In fact, increasing the time between injections not only reduces psychological stress and injection-associated pain but also reduces the burden of traveling to the local outpatient clinic. In the treatment of later stages of illness, SGA LAIs allow the patient to be more involved in personalized psychosocial interventions, because the overall complexity of the psychopharmacological treatment regimen is reduced.57 This is important for fostering greater involvement of patients in other interventions that can provide better social integration, as well as in training and support actions for their family and caregivers.
Adherence to treatment
Nonadherence in schizophrenia should be destigmatized, given that nonadherence is common even in nonpsychiatric illnesses.58 However, poor medication adherence in schizophrenia is a complex phenomenon that is associated with a number of factors.59 In addition to the disease itself, other factors undoubtedly contribute to medication adherence, such as personal features, comorbidities (eg, substance-use disorders), and treatment-related characteristics.
Treatment satisfaction correlates positively with adherence to therapy,60 and several domains of treatment satisfaction have been associated with the type and mode of medication delivery. These include perceived effectiveness, side effects, ease of treatment regimen, and costs.61,62 The panel of experts reported that previous negative experiences can contribute further to nonadherence: compulsory admission to psychiatric clinics, compulsory acute intramuscular antipsychotic injections, previous exposure to higher-than-necessary antipsychotic doses with associated extrapyramidal symptoms, and negative subjective well-being. The experts broadly identified two types of adherence: full adherence and nonadherence. In the real world, of course, patients show different levels of adherence between these two extremes.
SGA LAIs from the patient’s perspective
In other fields of medicine, LAI medications have been perceived as technological progress that allows not only addressing the issue of nonadherence but also a focus on a patient’s treatment satisfaction and subjective well-being.63 In the field of psychiatry, greater use of LAI antipsychotics might lead to similar advantages.25 In particular, the switch from oral to LAI antipsychotic maintenance treatment seems to induce a sustained improvement in attitude toward the drug in patients with schizophrenia.26
Several factors related to the type of delivery of LAI antipsychotic formulations may promote better adherence. Based on the panel’s experience, the switch from oral antipsychotic to LAI formulations, from FGA-LAIs to SGA-LAIs, and more recently from a monthly to a formulation taken once every 3 months (eg, paliperidone palmitate), can dramatically increase patient satisfaction and retention in treatment. For example, the flexibility associated with a monthly LAI regimen, and even more with once every 3 months (which allows a ±2-week flexible additional interval between doses), may be appreciated by adherent patients, particularly younger ones, who in the early phase of illness are able to maintain an occupation, may be willing to travel, and may appreciate the convenience of this formulation (Table 2).
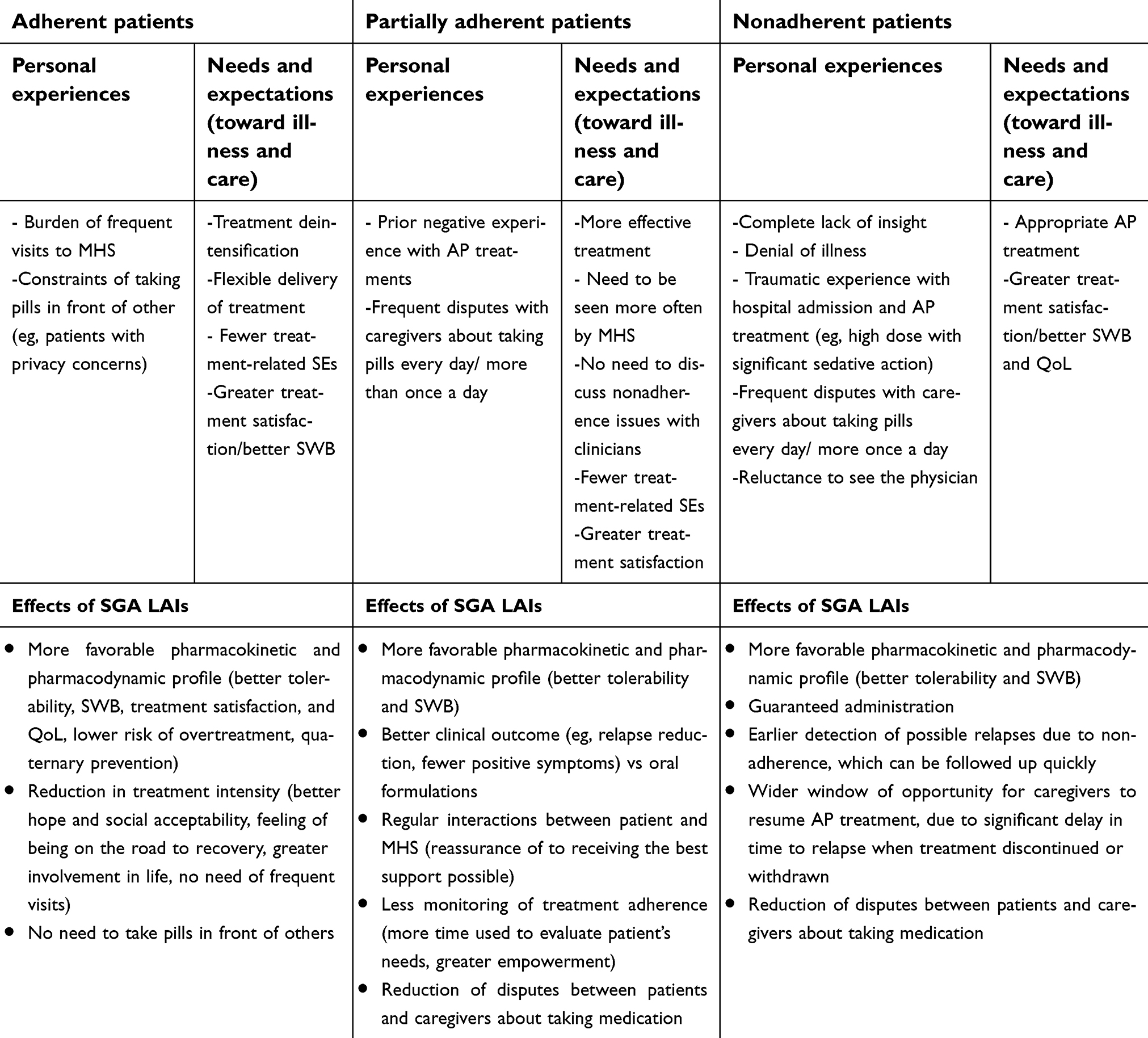 | Table 2 Adherence to treatment: effects of SGA LAIs on patient and caregiver needs, expectations, and personal experiences |
Adherent patients
Fully adherent patients deserve delivery of treatment that is as flexible as possible. They typically do not need to be seen often by mental health professionals (especially if young, at early stages of disease, or with a preserved level of functioning), and may feel constrained when taking pills in front of others. These patients would suffer from the burden of frequent visits to a community mental health center (which is typically open during working hours, so that they have to leave from work). This latter aspect is highly relevant for young persons in early stages of disease and with full-time, competitive work.
The adherent patient expects treatment-related side effects to be minimized. They often suffer from extrapyramidal symptoms, weight gain, and sexual side effects, and ask for better tolerability and subjective well-being under medication.11,64–68 Negative subjective well-being has been related with higher than 70% D2-receptor occupancy in striatal and extrastriatal cerebral areas.69–74 Therefore, higher-than-necessary antipsychotic doses or the concomitant use of multiple antipsychotics should be avoided, as this may expose patients to high D2-receptor occupancy and a reduction in perceived well-being and treatment satisfaction.
Subjective well-being during antipsychotic treatment is likely to be best achieved by using the lowest effective dose of antipsychotics.75 Achieving subjective well-being under treatment is important in patients with good adherence, as well as in those who are not fully adherent. Different types of medication delivery, such as LAI formulations, may help clinicians to titrate the dose slowly to the lowest effective one, while avoiding the risk of relapses.
SGA LAIs from the adherent patient’s perspective
A potentially useful factor associated with SGA LAIs in adherent patients (as well as in partially adherent and nonadherent patients) is reduction of treatment-related discomfort. FGAs are associated with negative subjective well-being and so-called neuroleptic dysphoria,76 both of which have been related to D2-receptor occupancy >70%. As discussed, both LAI and extended-release oral formulations are associated with more favorable pharmacokinetics,45 possibly implying that adequate plasma concentrations are more easily reached and that D2 receptors are optimally occupied.
In addition to the pharmacokinetic advantages of once-monthly SGA LAIs, some patients still report that they feel somewhat “frozen” or “blocked” (mentally and/or physically) in the first few days after LAI administration. This transient state may be related to an initial and rapid increase of the drug plasma level and consequently to temporarily high occupancy of D2 receptors. Similar transient negative subjective well-being may be reported in the first days after administration. In such cases, the panel of experts believe that a formulation once every 3 months (when available) might be preferred by patients, as less frequent injections would reduce this initial negative subjective experience. In some cases, fear of needles and pain at the injection site may be additional issues for which such a formulation may be favored. At the same time, thanks to their pharmacokinetic stability, SGA LAIs can facilitate the titration to the lowest effective dose, thus limiting the risk of overtreatment and promoting quaternary prevention. This characteristic is very desirable, because it can reduce the risk of both negative subjective experience of treatment and dose-related side effects, thus improving overall the patient’s acceptance of medication.77
Preliminary but consistent findings show that SGA LAIs are preferred by adherent patients over FGAs and their corresponding oral formulations, and are associated with greater treatment satisfaction, subjective well-being, and better QoL.25,78–83 In this regard, one aspect to consider is that adherent patients may prefer the LAI option, because it avoids the need for oral treatment, and thus they are not constrained to take their medication in front of others. This may be especially relevant in patients with privacy concerns (eg, patients attending university who live with other students). Less frequent injections, like the use of a formulation once every 3 months, may also be perceived by the patient as being “on the road to recovery”. A reduction in treatment intensity may be associated with hope, social acceptability, greater involvement in life, and be highly appreciated by both patients and caregivers. This may be particularly true for young first-episode patients with high levels of cognitive functioning who are able to maintain employment, have a satisfying social life, and travel. As mentioned, these patients do not need frequent follow-up visits, and thus may find an optimal treatment strategy in SGA LAIs.
Partially adherent patients
In the clinical experience of the experts, the patient with partial adherence is clearly in need of greater treatment satisfaction. He/she is not only less prone to tolerate side effects but also requires more effective treatment and needs to be seen more often by mental health professionals than the fully adherent patient. This patient often fails to take medication appropriately because of the intrinsic symptoms of his/her illness. Typically, blaming these patients for missing doses is not useful. It may also be annoying for the patient to have family members reminding them to take pills every day one or more times per day, and having to spend time during follow-up visits discussing with the clinician treatment-nonadherence implications (Table 2). For this type of patient, there is a clear need for a treatment formulation that can address these issues.
SGA LAIs from the partially adherent patient’s perspective
The better tolerability of LAI formulations and their greater efficacy represent a significant advantage not only for fully adherent patients but also for those who are only partially adherent. This is especially important for the latter group, as they usually ask for a more effective treatment with fewer side effects. Improving efficacy and tolerability of antipsychotic treatment is also important for patients who are completely nonadherent due to prior negative experiences associated with a previous high-dose antipsychotic treatment with significant sedative action.
In patients with partial adherence, the use of SGA-LAIs requires less adherence assessment, so more time can be used to evaluate the patient’s individual needs, fostering greater empowerment and willingness to follow the shared treatment plan to achieve personalized goals.84 The regular schedule of follow-up visits planned for patients under LAI treatment seems to further to reassure the patient and his/her caregivers that they are receiving the best support possible. The use of SGA LAIs also has the potential to reduce disputes of patients with family members/caregivers about adherence. Such an advantage is particularly obvious in patients who are partially adherent or completely nonadherent. SGA-LAI formulations once every 3 months may amplify this advantage by reducing injections to only four times a year.
Nonadherent patients
Most nonadherent patients are characterized by a complete lack of insight. As a consequence, they have often had previous negative experiences of traumatic compulsory admissions to hospital and acute intramuscular antipsychotic injections. For example, it might have been necessary to control acute agitation with rapid tranquilization such that they may have been administered strong sedatives or even unnecessarily high doses of antipsychotics.
Furthermore, denial of illness often compromises relationships with mental health professionals such that the nonadherent patient is reluctant to see the treating physician or general practitioner, thus rendering treatment of comorbid conditions more difficult. Nonetheless, family and caregivers of nonadherent patients generally expect treatment intervention and are often in open conflict with the patient. Disputes about medication adherence often compromise daily life and the patient’s family climate, with a severe negative impact on his/her QoL.
SGA LAIs from the nonadherent patient’s perspective
Consensus guidelines recommend considering LAI antipsychotics in patients who lack insight into their illness and in patients with multiple relapses due to treatment non-adherence.85 The use of SGA LAIs in non-adherent patients may be of great clinical utility because it enables clinicians to proactively detect early signs of possible relapses, while evaluating the efficacy of treatment and need for changes in the treatment plan (Table 2).86
As said before, the use of SGA LAIs also has the potential to reduce disputes of the patients with family members/caregivers about adherence. Such an advantage is particularly obvious in patients who are completely non-adherent. LAI formulations may be preferred in non-adherent patients when considering the significant delay in time to relapse when this treatment formulation is discontinued or withdrawn. In a study by Weiden et al, median time to relapse after discontinuation of oral paliperidone, once-monthly paliperidone, and paliperidone once-every-3-months was 58, 172 and 395 days, respectively.87 Such a delay is likely to be appreciated by a non-adherent patient’s family members/caregivers, as it gives more time to persuade the patient to resume antipsychotic treatment. In fact, when asked whether they would have preferred the patient to be switched from the current oral antipsychotic formulation to a once-every-3-months LAI formulation, 67.5% of caregivers of first-episode patients and 77.8% of multiple-episode patients preferred the once-every-3-months formulation.88
Level of functioning
Life domains related to living independently, productive activities, and social relations are often highly compromised in patients with schizophrenia.89 Functional outcomes of schizophrenia correlate with age of onset, premorbid adaptation, duration of untreated psychosis, and adherence to treatment. Functional impairment of patients with schizophrenia is only partly attributable to the symptoms of the disorder: personal resources and other aspects relating to the family and social context, stigma, and self-discrimination often provide a crucial contribution.89–92 In fact, although remission of symptoms and reduced rate of relapses produce a positive impact on a patient’s everyday life, this is frequently not sufficient to ensure the achievement of functional recovery, especially in low-functioning cases.93,94
Independently of the level of functioning, the suffering experienced by patients and caregivers is caused not only by the disorder itself, but also by the disturbances in social and relationship domains, in terms of marginalization, exclusion, rejection, prejudice, and discrimination.95 The negative stereotypes of weakness and disability add to a sense of self-stigmatization of patients and caregivers, with a negative impact on self-esteem, hope, empowerment, self-efficacy, QoL, social cohesion, and treatment adherence, thus impinging heavily on daily functioning.90 For this reason, in both low- and high-functioning patients, educational support for patients and caregivers should aim to overcome the feeling of being affected by an incurable disease and to raise awareness on the implications of failing to comply with treatment.96 Especially when the patient with schizophrenia has shown competency prior to the onset of the disorder, the hope of clinical and functional recovery should be fostered whenever possible.
Low-functioning patients
In early-onset patients and/or in those characterized by low levels of premorbid adaptation, schizophrenia affects the person during a crucial phase of his/her development, when he/she has not yet consolidated the basic skills required to take on traditional social roles. In these cases, the prognosis is often markedly worse than in later onsets of schizophrenia in which the person has got full or partial social cohesion, a good level of education, social and personal relationships, some degree of independence from family, his/her own family, and a job.97
Early intervention is linked to a higher probability of success since the psychological and behavioral mechanisms that promote low-functioning have not yet become chronic. Recovery is undoubtedly more difficult to achieve in the long-term stages of the disease in which patients and caregivers are resigned to chronically impaired levels of functioning. At the same time, the expectations of low-functioning patients with schizophrenia and their families regarding recovery of previous functioning are more likely to be satisfied when prompt and adequate treatment is established.
Triggered by the belief that schizophrenia is a chronic and incurable condition, the feeling of not being able to lead a productive life convinces low-functioning patients and their caregivers of the need for health and disability benefits.98 Another vicious circle can be activated wherein patients are not prepared to give up their disability benefits for a job that is viewed as being less permanent and more tedious, thus encouraging a regressive need for overall care. As time passes, feelings of frustration and inability arises, promoting a tendency to avoidance, isolation, and confinement with feelings of anger and self-blame (Table 3).
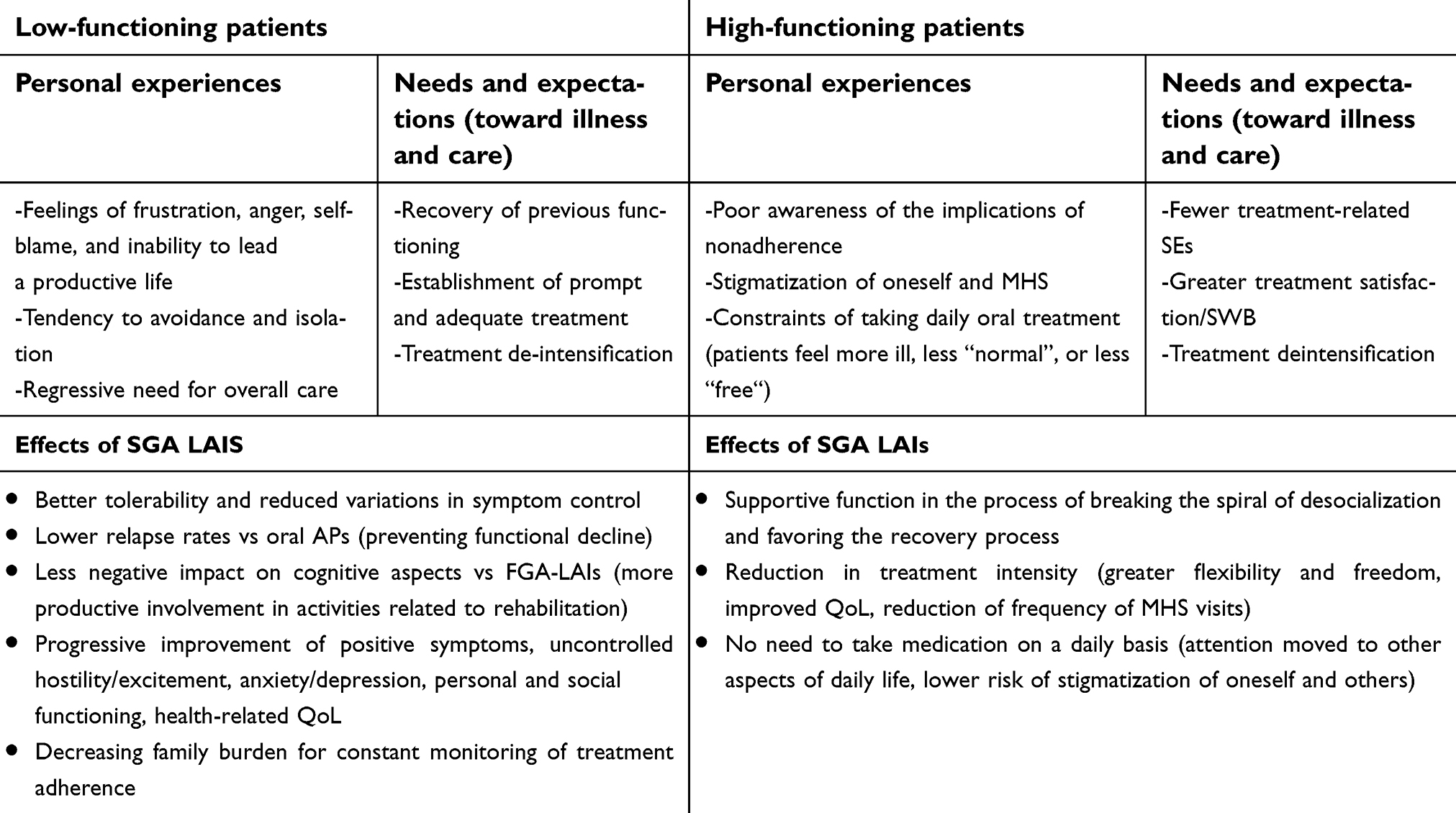 | Table 3 Level of functioning: effects of SGA LAIs on patient and caregiver needs, expectations, and personal experiences |
The added value of SGA LAIs in the low-functioning patient
Access to pharmacologically effective and tolerable treatments combined with antipsychotic formulations that improve adherence, such as SGA LAIs, may be crucial elements to guarantee a stable clinical condition in the recovery process in low-functioning patients with schizophrenia.99 As previously mentioned, each relapse of schizophrenia leads to a progressive decrease of patient’s level of functioning.84 Since LAI antipsychotics have been shown to be associated with fewer relapses compared to conventional oral formulations,37 one of the added values of SGA LAIs may consist in preventing functional decline.
SGA LAIs are also recommended as first line treatment of schizophrenia in patients with cognitive impairment and poor functioning.85 The lesser negative impact of SGA-LAIs on cognitive aspects of the schizophrenic syndrome compared to FGA-LAIs can allow for more productive involvement of the patient in activities related to rehabilitation. Furthermore, in low-functioning patients, the consequent improvement in adherence with LAI formulations,26 due to the simplification of treatment, may decrease the family burden related to the need for constant monitoring of treatment adherence due to the fear that inadequate treatment will lead to relapse (Table 3).
In the last few years, the role of SGA-LAIs in improving both functioning and QoL of patients with schizophrenia has been investigated.84,100–102 For example, Carpiniello et al have recently showed in a literature review that the use of paliperidone palmitate once every 3 months was associated with benefits in PANSS total scores, positive symptoms, uncontrolled hostility/excitement, and anxiety/depression, as well as progressive improvement of personal and social functioning.99 In a case-control study by Pietrini et al, antipsychotic maintenance treatment with an SGA-LAI was associated with better improvements in the PANSS, DAI-10, health-related QoL, and functioning in almost all areas of daily living compared with maintenance treatment with the corresponding oral formulation.25 Surprisingly, during the same treatment period, the group of patients on an oral formulation showed significant worsening of health-related QoL in the areas of emotional role and social functioning.25 All of these aspects allow clinicians and the management team to devote more efforts to psychosocial interventions aimed at achieving functional recovery regardless of the level of baseline functioning, minimizing the time and resources needed to monitor treatment adherence.
High-functioning patients
High-functioning patients with schizophrenia and their caregivers may have poor awareness of the implications of non-adherence to treatment and may tend to limit contact with mental health services (which can be viewed as stigmatizing or constantly exposing to the burden of a disabling illness). In this regard, daily oral treatment forces patients to pay constant attention to their disease and can make them feel more ill, less “normal”, or less “free”. On the other hand, a smaller number of treatment administrations seems to be more acceptable for high-functioning patients. In these cases, the absence of relevant functional impairment together with the fear of intolerable side effects and negative consequences on subjective well-being and functioning might lead patients to inadequate treatment (Table 3).
The added value of SGA LAIs in the high-functioning patient
Access to pharmacologically effective and tolerable treatments combined with formulations that improve treatment adherence, such as SGA LAIs, are often sufficient elements to ensure the achievement and maintenance of recovery in high-functioning patients.99 In high-functioning patients, SGA-LAIs have an important supportive function in the process of breaking the spiral of desocialization and favoring the recovery process.103 As said earlier, treatment deintensification can give patients greater flexibility and freedom to live their own lives,52 thus improving their overall QoL (Table 3).
A smaller number of treatment administrations can reduce the frequency of specialist visits and contacts. This benefit is particularly evident for patients who tend to stigmatize mental health services and who have poor awareness of the implications of non-adherence to treatment. As the patient is no longer called upon to take the drug on a daily basis (and at pre-established times) and to repeatedly face the burden of being affected by an invalidating illness, attention may be diverted from the disorder and moved to other aspects of daily life, with a lower risk of stigmatization of oneself and others.
Discussion and conclusions
Schizophrenia is a chronic syndrome involving different clinical dimensions and causing significant functional impairment with negative impact on QoL of patients and caregivers.2–4 Current key guidelines for the treatment of schizophrenia focus on maximizing patient’s adaptive functioning and QoL in a recovery-oriented approach.7,8 A recovery-oriented treatment team should involve different mental health professionals and include both patients and caregivers in the decision-making process.14,15 Such patient-centered psychiatric care encourages the active collaboration between patients, families, and providers to design and manage a customized and comprehensive care plan.104
In this regard, “modern” use of SGA LAIs is likely to fit well into patient-centered treatment plans for schizophrenia.23 In fact, the available evidence underlines the better tolerability of SGA LAIs vs oral SGA,26,105,106 oral FGA,21 and first-generation depot formulations.107
Beyond their efficacy and tolerability profile, other advantages of SGA LAIs that can be appreciated, in terms of subjective well-being, attitudes towards treatment, and QoL, are probably due to their unique pharmacokinetic and pharmacodynamic profile (ie, allow to control titration to effective dose, to steady plasma drug levels, to avoid first-pass metabolism, and guarantee delivery of medication108), as well as to other individual and environmental factors (ie, not having to take pills may increase social adaptation, autonomy, and may reduce stigma; periodic treatment monitoring may improve therapeutic alliance, etc.).59 For these reasons, we think that SGA LAIs can be seen as an increasingly valuable option to improve compliance and a wide range of other clinical and social outcomes.100,108–110
In the present study, a panel of experts (including psychiatrists, psychologist, nurse and social worker) gathered to review and explore the need for up-to-date use of SGA LAIs in “recovery-oriented” and “patient-centered” care of schizophrenia. First of all, the panel participants agreed that the better clinical outcomes of SGA LAIs compared to oral antipsychotics in terms of fewer relapses, hospitalizations, and presentations to the ER37 may significantly lower patient’s and caregiver’s overall level of stress, disease burden, and medicalization, and increase perceived normality.42
Although this may be valid in all stages of disease and at any level of functional impairment, this is particularly important in the early phases of the disease. In fact, since each relapse of schizophrenia leads to a progressive decrease of the patient’s level of functioning,84 one of the added values of SGA LAIs in recovery-oriented treatment of schizophrenia consists of preventing functional decline and minimizing the patient’s disability.
Each relapse has a negative impact on caregivers of patient’s with schizophrenia, especially of those with a long history of illness.51 These patients must not only be involved in specific interventions aimed at social integration, but also in training and support programs for their family members.53 In the opinion of the expert panel, the low frequency of administration of SGA LAIs in later stages of schizophrenia may allow patients and caregivers to be more involved in recovery-oriented psychosocial interventions and support actions.57 In the participants’ experience, schizophrenic patients are at increased risk of developing depressive symptoms. However, SGA LAIs seem to provide significant benefits in long-term control of both psychotic and affective symptoms.54
Unfortunately, adherence to treatment of patients with schizophrenia is often threatened by overt or covert non-adherence,36,37 significant cognitive symptoms,38,39 and treatment-related side effects.22 However, the early administration of SGA LAIs is reported to improve therapeutic alliance49 and cognitive functioning,43 as well as minimize treatment-related adverse effects.35,46,47 In this regard, the panel of experts agreed that LAI formulations should be preferred in non-adherent patients, especially considering the significant delay in the time to relapse when this treatment formulation is discontinued or withdrawn. Such a delay is likely to be appreciated by family members/caregivers of non-adherent patients, as it gives more time to persuade the patient to resume antipsychotic treatment.88 The reduced need of monitoring treatment adherence provides the following advantages: on one hand, the treatment team can focus on the patient’s personal goals with a consequent improvement of therapeutic alliance;49 on the other hand, patients and caregivers can reduce disputes about medication adherence, which may lead them to feel a sense of greater stability that can consequently restore a family climate of “normality”.37
The panel of experts also underlined how less frequent long-acting antipsychotic injections, for example with the use of a once-every-3-months formulation, may also be perceived by the patient as being “on the road to recovery”. In other terms, a reduction in treatment intensity may be associated with hope, improved social acceptability, limited risk of stigma and self-stigma, and greater involvement in daily life activities, thus being highly appreciated by both patients and caregivers.
In the present study, the panel of experts recommended SGA LAIs as a first line treatment of schizophrenia in patients with cognitive impairment and poor functioning, since the lesser negative impact of SGA-LAIs on cognitive symptoms compared to FGA-LAIs allow for more productive involvement of the patient in rehabilitation activities.85 At the same time, all patients with schizophrenia (especially those with FES or good baseline level of functioning) expect treatment-related side effects to be minimized.11,64–68 The experts suggested that a potentially useful factor associated with SGA LAIs is reduction of treatment-related discomfort. In fact, SGA LAIs seem to have more favorable pharmacokinetics compared to other antipsychotic formulations,45 possibly because adequate plasma concentrations are more easily reached and that D2 receptors are optimally occupied. At the same time, thanks to their pharmacokinetic stability, SGA LAIs can facilitate the titration to the lowest effective dose, thus limiting the risk of overtreatment and promoting quaternary prevention.
A once-every-3-months LAI formulation (when available) might also be preferred over a once-monthly one for patients who refer a negative subjective experience of antipsychotic treatment in the first days after the injection, as well as for those patients who fear needles.
In conclusion, all of the mentioned actions, pivoted on a stable clinical condition, make patients with schizophrenia better suited to integrated rehabilitation programs,50 significantly improving their long-term prognosis.37,51,52 Considered in a contemporary perspective, SGA-LAIs have an important supportive function in the process of breaking the spiral of de-socialization and functional decline in schizophrenia, favoring the recovery process.103 In fact, treatment deintensification can give patients greater flexibility and freedom for living their own lives,52 thus improving their overall QoL.
Patient- and caregiver-centered care of schizophrenia, together with a modern use of SGA LAIs, may allow clinicians and other mental health professionals to devote more efforts to psychosocial interventions aimed at achieving recovery and minimizing the time and resources spent to monitor treatment adherence.
Acknowledgments
We wish to thank Health Publishing and Services SRL (HPS), who provided medical writing assistance. The realization of this article was possible thanks to an unconditional educational grant from Janssen. The various activities needed to write this paper were carried out in complete autonomy by the authors and HPS without any interference from Janssen.
Disclosure
FP is/has been a consultant and/or a speaker for Janssen-Cilag, Lundbeck, Otsuka Pharmaceuticals, and Eli Lilly. UA is/has been a consultant and/or a speaker for Angelini, FB Health, Janssen Cilag, and Lundbeck. GM is/has been a consultant and/or a speaker and/or has received research grants from Angelini, Boheringer Ingelheim, FB Health, Italfarmaco, Janssen, Lundbeck, and Otsuka Pharmaceuticals. BC has participated as a consultant in scientific boards and as a speaker in industry-sponsored courses or symposia supported by Janssen Italy, Lundbeck Italy, Otsuka Italy, and ACRAF Angelini. The other authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
2. DeRosse P, Nitzburg GC, Blair M, Malhotra AK. Dimensional symptom severity and global cognitive function predict subjective quality of life in patients with schizophrenia and healthy adults. Schizophr Res. 2018;195:385–390. doi:10.1016/j.schres.2017.10.018
3. Jobe TH, Harrow M. Long-term outcome of patients with schizophrenia: a review. Can J Psychiatry. 2005;50(14):892–900. doi:10.1177/070674370505001403
4. Wiersma D, Wanderling J, Dragomirecka E, et al. Social disability in schizophrenia: its development and prediction over 15 years in incidence cohorts in six European centres. Psychol Med. 2000;30(5):1155–1167.
5. Brugnoli R, Rapinesi C, Kotzalidis GD, et al. Model of Management (Mo.Ma) for the patient with schizophrenia: crisis control, maintenance, relapse prevention, and recovery with long-acting injectable antipsychotics (LAIs). Riv Psichiatr. 2016;51(2):47–59. doi:10.1708/2246.24194
6. Hasan A, Falkai P, Wobrock T, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effects. World J Biol Psychiatry. 2013;14(1):2–44.
7. NICE Guidance. Psychosis and schizophrenia in adults: prevention and management. NICE guidelines [CG178]. Available from:
8. Lehman A, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia. 2004. Available from:
9. Vita A, Barlati S. Recovery from schizophrenia: is it possible? Curr Opin Psychiatry. 2018;31(3):246–255.
10. Mura G, Petretto DR, Bhat KM, Carta MG. Schizophrenia: from epidemiology to rehabilitation. Clin Pract Epidemiol Ment Health. 2012;8:52–66. doi:10.2174/1745017901208010052
11. Lambert M, Schimmelmann BG, Naber D, et al. Prediction of remission as a combination of symptomatic and functional remission and adequate subjective well-being in 2960 patients with schizophrenia. J Clin Psychiatry. 2006;67(11):1690–1697.
12. Chan RCH, Mak WWS, Chio FHN, Tong ACY. Flourishing with psychosis: a prospective examination on the interactions between clinical, functional, and personal recovery processes on well-being among individuals with schizophrenia spectrum disorders. Schizophr Bull. 2018;44(4):778–786. doi:10.1093/schbul/sbx120
13. Velligan DI, Newcomer J, Pultz J, et al. Does cognitive function improve with quetiapine in comparison to haloperidol? Schizophr Res. 2002;53(3):239–248.
14. Kreyenbuhl J, Buchanan RW, Dickerson FB, Dixon LB. Schizophrenia Patient Outcomes Research T. The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2009. Schizophr Bull. 2010;36(1):94–103. doi:10.1093/schbul/sbp130
15. Schottle D, Schimmelmann BG, Ruppelt F, et al. Effectiveness of integrated care including therapeutic assertive community treatment in severe schizophrenia-spectrum and bipolar I disorders: four-year follow-up of the ACCESS II study. PLoS One. 2018;13(2):e0192929. doi:10.1371/journal.pone.0192929
16. Liberman RP. Recovery from schizophrenia: form follows functioning. World Psychiatry. 2012;11(3):161–162.
17. Karthik MS, Kulhara P, Chakrabarti S. Attitude towards second-generation antipsychotics among patients with schizophrenia and their relatives. Hum Psychopharmacol. 2013;28(5):457–465. doi:10.1002/hup.2332
18. Potkin S, Bera R, Zubek D, Lau G. Patient and prescriber perspectives on long-acting injectable (LAI) antipsychotics and analysis of in-office discussion regarding LAI treatment for schizophrenia. BMC Psychiatry. 2013;13:261. doi:10.1186/1471-244X-13-261
19. Naber D. Subjective effects of antipsychotic drugs and their relevance for compliance and remission. Epidemiol Psichiatr Soc. 2008;17(3):174–176.
20. Roe D, Lachman M. The subjective experience of people with severe mental illness: a potentially crucial piece of the puzzle. Isr J Psychiatry Relat Sci. 2005;42(4):223–230.
21. Awad AG, Voruganti LN. The impact of newer atypical antipsychotics on patient-reported outcomes in schizophrenia. CNS Drugs. 2013;27(8):625–636. doi:10.1007/s40263-013-0070-1
22. Naber D. Subjective effects of antipsychotic treatment. Acta Psychiatr Scand. 2005;111(2):81–83. doi:10.1111/j.1600-0447.2004.00478.x
23. Altamura AC, Aguglia E, Bassi M, et al. Rethinking the role of long-acting atypical antipsychotics in the community setting. Int Clin Psychopharmacol. 2012;27(6):336–349. doi:10.1097/YIC.0b013e328357727a
24. Jakovljevic M. Long-acting injectable (depot) antipsychotics and changing treatment philosophy: possible contribution to integrative care and personal recovery of schizophrenia. Psychiatr Danub. 2014;26(4):304–307.
25. Pietrini F, Spadafora M, Tatini L, et al. LAI versus oral: A case-control study on subjective experience of antipsychotic maintenance treatment. Eur Psychiatry. 2016;37:35–42. doi:10.1016/j.eurpsy.2016.05.008
26. Pietrini F, D’Anna G, Tatini L, et al. Changes in attitude towards LAI antipsychotic maintenance treatment: A two-year follow-up study. Eur Psychiatry. 2018;53:58–65. doi:10.1016/j.eurpsy.2018.06.002
27. Agius M, Butler S, Holt C. Does early diagnosis and treatment of schizophrenia lead to improved long-term outcomes?. Neuropsychiatry. 2011;1(6):553–565. doi:10.2217/npy.11.71
28. Birchwood M, Todd P, Jackson C. Early intervention in psychosis. The critical period hypothesis. Br J Psychiatry Suppl. 1998;172(33):53–59.
29. Buckley PE, Evans D. First-episode schizophrenia. A window of opportunity for optimizing care and outcomes. Postgrad Med. 2006
30. Fleischhacker WW. The first-episode of schizophrenia: a challenge for treatment. Eur Psychiatry. 2002;17(Suppl 4):371s–375s.
31. Tanskanen S, Morant N, Hinton M, et al. Service user and carer experiences of seeking help for a first episode of psychosis: a UK qualitative study. BMC Psychiatry. 2011;11:157. doi:10.1186/1471-244X-11-157
32. Tindall R, Francey S, Hamilton B. Factors influencing engagement with case managers: perspectives of young people with a diagnosis of first episode psychosis. Int J Ment Health Nurs. 2015;24(4):295–303. doi:10.1111/inm.12133
33. van Schalkwyk GI, Davidson L, Srihari V. Too late and too little: narratives of treatment disconnect in early psychosis. Psychiatr Q. 2015;86(4):521–532. doi:10.1007/s11126-015-9348-4
34. Berge D, Mane A, Salgado P, et al. Predictors of relapse and functioning in first-episode psychosis: a two-year follow-up study. Psychiatr Serv. 2016;67(2):227–233. doi:10.1176/appi.ps.201400316
35. Robinson DG, Woerner MG, Alvir JM, Bilder RM, Hinrichsen GA, Lieberman JA. Predictors of medication discontinuation by patients with first-episode schizophrenia and schizoaffective disorder. Schizophr Res. 2002;57(2–3):209–219.
36. Gutierrez-Casares JR, Canas F, Rodriguez-Morales A, Hidalgo-Borrajo R, Alonso-Escolano D. Adherence to treatment and therapeutic strategies in schizophrenic patients: the ADHERE study. CNS Spectr. 2010;15(5):327–337.
37. Subotnik KL, Casaus LR, Ventura J, et al. Long-acting injectable risperidone for relapse prevention and control of breakthrough symptoms after a recent first episode of schizophrenia. A randomized clinical trial. JAMA Psychiatry. 2015;72(8):822–829. doi:10.1001/jamapsychiatry.2015.0270
38. Chung W, Chang HS, Oh SM, Yoon CW. Factors associated with long-stay status in patients with schizophrenia: an analysis of national databases covering the entire Korean population. Int J Soc Psychiatry. 2013;59(3):207–216. doi:10.1177/0020764011431794
39. Olfson M, Marcus SC, Wilk J, West JC. Awareness of illness and nonadherence to antipsychotic medications among persons with schizophrenia. Psychiatr Serv. 2006;57(2):205–211. doi:10.1176/appi.ps.57.2.205
40. Jackson H, McGorry P, Edwards J, et al. Cognitively-oriented psychotherapy for early psychosis (COPE). Preliminary results. Br J Psychiatry Suppl. 1998;172(33):93–100.
41. McCay E, Beanlands H, Zipursky R, et al. A randomised controlled trial of a group intervention to reduce engulfment and self-stigmatisation in first episode schizophrenia. Aust E J Adv Mental Health. 2007;6:212–220. doi:10.5172/jamh.6.3.212
42. Biagi E, Capuzzi E, Colmegna F, et al. Long-acting injectable antipsychotics in schizophrenia: literature review and practical perspective, with a focus on aripiprazole once-monthly. Adv Ther. 2017;34(5):1036–1048. doi:10.1007/s12325-017-0507-x
43. Karson C, Duffy RA, Eramo A, Nylander AG, Offord SJ. Long-term outcomes of antipsychotic treatment in patients with first-episode schizophrenia: a systematic review. Neuropsychiatr Dis Treat. 2016;12:57–67. doi:10.2147/NDT.S96392
44. Nandra KS, Agius M. The difference between typical and atypical antipsychotics: the effects on neurogenesis. Psychiatr Danub. 2012;24(Suppl 1):S95–S99.
45. Sheehan JJ, Reilly KR, Fu DJ, Alphs L. Comparison of the peak-to-trough fluctuation in plasma concentration of long-acting injectable antipsychotics and their oral equivalents. Innov Clin Neurosci. 2012;9(7–8):17–23.
46. Jeong HG, Lee MS. Long-acting injectable antipsychotics in first-episode schizophrenia. Clin Psychopharmacol Neurosci. 2013;11(1):1–6. doi:10.9758/cpn.2013.11.1.1
47. Taylor M, Ng KY. Should long-acting (depot) antipsychotics be used in early schizophrenia? A systematic review. Aust N Z J Psychiatry. 2013;47(7):624–630. doi:10.1177/0004867412470010
48. Seeman MV. Drawbacks of Long-Acting Intramuscular Antipsychotic Injections. J Clin Pract Nursing. 2017;1(1):12–22.
49. Nik Ruzyanei NJ, Hazli Z, Chong YS, Marhani M. A case series on the use of atypical long acting injectable as first-line antipsychotic treatment in Malaysia: Who benefits and how?. Malaysian Journal of Psychiatry. 2013;22(1):61-65.
50. Brissos S, Veguilla MR, Taylor D, Balanza-Martinez V. The role of long-acting injectable antipsychotics in schizophrenia: a critical appraisal. Ther Adv Psychopharmacol. 2014;4(5):198–219. doi:10.1177/2045125314540297
51. Heres S, Lambert M, Vauth R. Treatment of early episode in patients with schizophrenia: the role of long acting antipsychotics. Eur Psychiatry. 2014;29(Suppl 2):1409–1413. doi:10.1016/S0924-9338(14)70001-X
52. Viala A, Cornic F, Vacheron MN. Treatment adherence with early prescription of long-acting injectable antipsychotics in recent-onset schizophrenia. Schizophr Res Treatment. 2012;2012:368687.
53. Moritz S, Berna F, Jaeger S, Westermann S, Nagel M. The customer is always right? Subjective target symptoms and treatment preferences in patients with psychosis. Eur Arch Psychiatry Clin Neurosci. 2017;267(4):335–339. doi:10.1007/s00406-016-0694-5
54. Chue P, Chue J. A critical appraisal of paliperidone long-acting injection in the treatment of schizoaffective disorder. Ther Clin Risk Manag. 2016;12:109–116.
55. Prikryl R, Prikrylova Kucerova H, Vrzalova M, Ceskova E. Role of long-acting injectable second-generation antipsychotics in the treatment of first-episode schizophrenia: a clinical perspective. Schizophr Res Treatment. 2012;2012:764769.
56. Osborne RH, Dalton A, Hertel J, Schrover R, Smith DK. Health-related quality of life advantage of long-acting injectable antipsychotic treatment for schizophrenia: a time trade-off study. Health Qual Life Outcomes. 2012;10:35. doi:10.1186/1477-7525-10-35
57. Malla A, Tibbo P, Chue P, et al. Long-acting injectable antipsychotics: recommendations for clinicians. Can J Psychiatry. 2013;58(5Suppl 1):30S–35S.
58.
59. Kane JM, Kishimoto T, Correll CU. Non-adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry. 2013;12(3):216–226.
60. Juckel G, de Bartolomeis A, Gorwood P, et al. Towards a framework for treatment effectiveness in schizophrenia. Neuropsychiatr Dis Treat. 2014;10:1867–1878.
61. Revicki DA. Patient assessment of treatment satisfaction: methods and practical issues. Gut. 2004;53(Suppl 4):iv40–iv44.
62. Weaver M, Patrick DL, Markson LE, Martin D, Frederic I, Berger M. Issues in the measurement of satisfaction with treatment. Am J Manag Care. 1997;3(4):579–594.
63. Zhang M, Brenneman SK, Carter CT, et al. Patient-reported treatment satisfaction and choice of dosing frequency with biologic treatment for moderate to severe plaque psoriasis. Patient Prefer Adherence. 2015;9:777–784.
64. Karow A, Czekalla J, Dittmann RW, et al. Association of subjective well-being, symptoms, and side effects with compliance after 12 months of treatment in schizophrenia. J Clin Psychiatry. 2007;68(1):75–80.
65. Lambert M, Naber D, Schacht A, et al. Rates and predictors of remission and recovery during 3 years in 392 never-treated patients with schizophrenia. Acta Psychiatr Scand. 2008;118(3):220–229.
66. Lambert M, Schimmelmann BG, Schacht A, et al. Long-term patterns of subjective wellbeing in schizophrenia: cluster, predictors of cluster affiliation, and their relation to recovery criteria in 2842 patients followed over 3 years. Schizophr Res. 2009;107(2–3):165–172.
67. Naber D. A self-rating to measure subjective effects of neuroleptic drugs, relationships to objective psychopathology, quality of life, compliance and other clinical variables. Int Clin Psychopharmacol. 1995;10(Suppl 3):133–138.
68. Vothknecht S, Schoevers RA, de Haan L. Subjective well-being in schizophrenia as measured with the subjective well-being under neuroleptic treatment scale: a review. Aust N Z J Psychiatry. 2011;45(3):182–192.
69. de Haan L, Lavalaye J, Linszen D, Dingemans PM, Booij J. Subjective experience and striatal dopamine D(2) receptor occupancy in patients with schizophrenia stabilized by olanzapine or risperidone. Am J Psychiatry. 2000;157(6):1019–1020.
70. de Haan L, Lavalaye J, van Bruggen M, et al. Subjective experience and dopamine D2 receptor occupancy in patients treated with antipsychotics: clinical implications. Can J Psychiatry. 2004;49(5):290–296.
71. de Haan L, van Bruggen M, Lavalaye J, Booij J, Dingemans PM, Linszen D. Subjective experience and D2 receptor occupancy in patients with recent-onset schizophrenia treated with low-dose olanzapine or haloperidol: a randomized, double-blind study. Am J Psychiatry. 2003;160(2):303–309.
72. Lataster J, van Os J, de Haan L, et al. Emotional experience and estimates of D2 receptor occupancy in psychotic patients treated with haloperidol, risperidone, or olanzapine: an experience sampling study. J Clin Psychiatry. 2011;72(10):1397–1404.
73. Mizrahi R, Mamo D, Rusjan P, Graff A, Houle S, Kapur S. The relationship between subjective well-being and dopamine D2 receptors in patients treated with a dopamine partial agonist and full antagonist antipsychotics. Int J Neuropsychopharmacol. 2009;12(5):715–721.
74. Mizrahi R, Rusjan P, Agid O, et al. Adverse subjective experience with antipsychotics and its relationship to striatal and extrastriatal D2 receptors: a PET study in schizophrenia. Am J Psychiatry. 2007;164(4):630–637.
75. Murray RM, Quattrone D, Natesan S, et al. Should psychiatrists be more cautious about the long-term prophylactic use of antipsychotics?. Br J Psychiatry. 2016;209(5):361–365.
76. Wu HE, Okusaga OO. Antipsychotic medication-induced dysphoria: its meaning, association with typical vs. atypical medications and impact on adherence. Psychiatr Q. 2015;86(2):199–205.
77. Nasrallah HA. The case for long-acting antipsychotic agents in the post-CATIE era. Acta Psychiatr Scand. 2007;115(4):260–267.
78. Fujikawa M, Togo T, Yoshimi A, et al. Evaluation of subjective treatment satisfaction with antipsychotics in schizophrenia patients. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(3):755–760.
79. Hargarter L, Cherubin P, Bergmans P, et al. Intramuscular long-acting paliperidone palmitate in acute patients with schizophrenia unsuccessfully treated with oral antipsychotics. Prog Neuropsychopharmacol Biol Psychiatry. 2015;58:1–7.
80. Kwon JS, Kim SN, Han J, et al. Satisfaction of immediate or delayed switch to paliperidone palmitate in patients unsatisfied with current oral atypical antipsychotics. Int Clin Psychopharmacol. 2015;30(6):320–328.
81. Nordon C, Rouillon F, Barry C, Gasquet I, Falissard B. Determinants of treatment satisfaction of schizophrenia patients: results from the ESPASS study. Schizophr Res. 2012;139(1–3):211–217.
82. Pietrini F, Spadafora M, Talamba GA, et al. The effects of switching from oral to LAI antipsychotic treatment on subjective experience of schizophrenic and schizoaffective patients: preliminary results. Int J Psychiatry Clin Pract. 2015;19(2):106–113.
83. Schreiner A, Bergmans P, Cherubin P, et al. Paliperidone palmitate in non-acute patients with schizophrenia previously unsuccessfully treated with risperidone long-acting therapy or frequently used conventional depot antipsychotics. J Psychopharmacol. 2015;29(8):910–922.
84. Keith SJ, Pani L, Nick B, et al. Practical application of pharmacotherapy with long-acting risperidone for patients with schizophrenia. Psychiatr Serv. 2004;55(9):997–1005.
85. Llorca PM, Abbar M, Courtet P, Guillaume S, Lancrenon S, Samalin L. Guidelines for the use and management of long-acting injectable antipsychotics in serious mental illness. BMC Psychiatry. 2013;13:340.
86. Gardner KN, Nasrallah HA. Managing first-episode psychosis: rationale and evidence for nonstandard first-line treatments for schizophrenia. Curr Psychiatry. 2015;14(7):38–45.
87. Weiden PJ, Kim E, Bermak J, Turkoz I, Gopal S, Berwaerts J. Does half-life matter after antipsychotic discontinuation? A relapse comparison in schizophrenia with 3 different formulations of paliperidone. J Clin Psychiatry. 2017;78(7):e813–e820.
88. Yeo SU, Park JI, Jang JM, et al. Acceptance rate of long-acting injection after short information: a survey in patients with first- and multiple-episode psychoses and their caregivers. Early Interv Psychiatry. 2017;11(6):509–516.
89. Galderisi S, Rossi A, Rocca P, et al. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry. 2014;13(3):275–287.
90. Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: a systematic review and meta-analysis. Soc Sci Med. 2010;71(12):2150–2161.
91. Rossi A, Galderisi S, Rocca P, et al. The relationships of personal resources with symptom severity and psychosocial functioning in persons with schizophrenia: results from the Italian Network for Research on Psychoses study. Eur Arch Psychiatry Clin Neurosci. 2017;267(4):285–294.
92. Wahl OF. Stigma as a barrier to recovery from mental illness. Trends Cogn Sci. 2012;16(1):9–10.
93. Pinna F, Deriu L, Lepori T, et al. Is it true remission? A study of remitted patients affected by schizophrenia and schizoaffective disorders. Psychiatry Res. 2013;210(3):739–744.
94. Pinna F, Tusconi M, Bosia M, Cavallaro R, Carpiniello B;
95. Buizza C, Schulze B, Bertocchi E, Rossi G, Ghilardi A, Pioli R. The stigma of schizophrenia from patients’ and relatives’ view: A pilot study in an Italian rehabilitation residential care unit. Clin Pract Epidemiol Ment Health. 2007;3:23.
96. Dixon LB, Holoshitz Y, Nossel I. Treatment engagement of individuals experiencing mental illness: review and update. World Psychiatry. 2016;15(1):13–20.
97. Clemmensen L, Dl V, Hc S. A systematic review of the long-term outcome of early onset schizophrenia. BMC Psychiatry. 2012;12:150.
98. Lasalvia A, Penta E, Sartorius N, Henderson S. Should the label “schizophrenia” be abandoned? Schizophr Res. 2015;162(1–3):276–284.
99. Carpiniello B, Pinna F. Critical appraisal of 3-monthly paliperidone depot injections in the treatment of schizophrenia. Drug Des Devel Ther. 2016;10:1731–1742.
100. Kaplan G, Casoy J, Zummo J. Impact of long-acting injectable antipsychotics on medication adherence and clinical, functional, and economic outcomes of schizophrenia. Patient Prefer Adherence. 2013;7:1171–1180. doi:10.2147/PPA.S53795
101. Montemagni C, Frieri T, Rocca P. Second-generation long-acting injectable antipsychotics in schizophrenia: patient functioning and quality of life. Neuropsychiatr Dis Treat. 2016;12:917–929. doi:10.2147/NDT.S88632
102. Schreiner A, Bergmans P, Cherubin P, et al. A prospective flexible-dose study of paliperidone palmitate in nonacute but symptomatic patients with schizophrenia previously unsuccessfully treated with oral antipsychotic agents. Clin Ther. 2014;36(10):1372–1388e1371. doi:10.1016/j.clinthera.2014.08.014
103. McCay E, Ryan K. Meeting the patient’s emotional needs. In: Zipursky RB, Carpenter W, editors. First Episode Psychosis. Washington, DC: American Psychiatric Publishing, Inc.; 2002:107–127.
104. Kane JM, Robinson DG, Schooler NR, et al. Comprehensive versus usual community care for first-episode psychosis: 2-year outcomes from the NIMH RAISE early treatment program. Am J Psychiatry. 2016;173(4):362–372. doi:10.1176/appi.ajp.2015.15050632
105. Lloyd K, Latif MA, Simpson S, Shrestha KL. Switching stable patients with schizophrenia from depot and oral antipsychotics to long-acting injectable risperidone: efficacy, quality of life and functional outcome. Hum Psychopharmacol. 2010;25(3):243–252. doi:10.1002/hup.1108
106. Rosa F, Schreiner A, Thomas P, Sherif T. Switching patients with stable schizophrenia or schizoaffective disorder from olanzapine to risperidone long-acting injectable. Clin Drug Investig. 2012;32(4):267–279. doi:10.2165/11599080-000000000-00000
107. Chen WY, Lin SK. Comparison of subjective experiences and effectiveness of first-generation long-acting injectable antipsychotics and risperidone long-acting injectables in patients with schizophrenia. J Clin Psychopharmacol. 2016;36(5):492–495. doi:10.1097/JCP.0000000000000555
108. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(suppl 3):1–24. doi:10.4088/JCP.15032su1
109. Stahl SM. Long-acting injectable antipsychotics: shall the last be first? CNS Spectr. 2014;19(1):3–5. doi:10.1017/S1092852913001016
110. Stevens GL, Dawson G, Zummo J. Clinical benefits and impact of early use of long-acting injectable antipsychotics for schizophrenia. Early Interv Psychiatry. 2016;10(5):365–377. doi:10.1111/eip.12278
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.