Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Miasma Mentality: Investigating the Association Between Beliefs in Noxious Fumes and Obstructive Pulmonary Disease (COPD), Symptoms, and Quality of Life
Authors Zhao Y, Ma Y, Geng L, Nie J, Yu X, Kang Z, Liu Y, Su Y
Received 12 October 2024
Accepted for publication 1 February 2025
Published 19 February 2025 Volume 2025:20 Pages 361—372
DOI https://doi.org/10.2147/COPD.S500502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yexian Zhao,* Yunlei Ma,* Limei Geng, Jia Nie, Xiangyan Yu, Zenglu Kang, Yun Liu, Yinghao Su
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Hebei University of Traditional Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yinghao Su, Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Hebei University of Traditional Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) significantly impacts morbidity and mortality globally. While established risk factors like smoking and occupational exposures are well-documented, patients’ beliefs—especially those from the miasma theory attributing disease to “bad air” in cultures like China—may also significantly influence health outcomes.
Methods: This case-control study was conducted at Hospital of Hebei University of Traditional Chinese, involving 500 individuals diagnosed with COPD and 500 matched control participants. Each participant completed questionnaires that gathered information on demographic details, clinical history, and beliefs about the causes of COPD. Clinical data were collected, including spirometry tests to assess lung function, the COPD Assessment Test (CAT) to evaluate symptom burden, and the St. George’s Respiratory Questionnaire (SGRQ) to measure health-related quality of life.
Results: The study found that 81% of COPD patients endorsed high miasma beliefs, compared to 28% of controls (p < 0.01). Those with strong beliefs reported significantly worse symptoms (mean CAT score: 23 vs 14, p < 0.001) and poorer quality of life (mean SGRQ score: 48 vs 39, p < 0.001) compared to low-belief individuals. Higher levels of anxiety and depression were also observed in patients with strong miasma beliefs. Laboratory biomarkers such as neutrophils, RDW width, and CRP were also elevated in the high-belief group compared to the low-belief group.
Conclusion: The findings suggest that adherence to miasma theory beliefs is associated with adverse health outcomes in COPD patients. Addressing these beliefs through targeted education may enhance patient engagement and adherence to evidence-based treatments, ultimately improving health outcomes.
Keywords: miasma mentality, chronic obstructive pulmonary disease, COPD, quality of life beliefs, treatment adherence
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a major global health concern, known for causing significant illness and death. It is defined by ongoing respiratory issues and restricted airflow.1 The development and progression of COPD have been well-established to be associated with various risk factors, including smoking, occupational exposures, and genetic predisposition.2 However, an individual’s beliefs and perceptions about the causes of their COPD can also significantly influence their health behaviors and, ultimately, disease outcomes.3
The management of COPD relies heavily on patients’ perceptions of their symptoms. This includes not only initiating treatment for acute exacerbations, but also maintaining daily activity.4 Research has shown that patients’ illness beliefs and psychological coping mechanisms play a significant role in determining disability and clinical outcomes, even beyond physical measures of disease severity such as lung function.5 One such belief system that has a long history in various cultures is the miasma theory, which attributes the development of diseases to the presence of “bad air” or miasmas.6 These beliefs, stemming from the miasma theory advanced by Hippocrates in the fourth century BC, are notably present in specific cultural contexts, particularly in China and Europe, but may also be observed in other regions.7,8 Despite the scientific advancements in understanding the pathogenesis of COPD, miasma theory beliefs continue to persist in certain societal and cultural contexts.9 These beliefs may shape how individuals with COPD perceive the nature of their disease and the actions they take to manage it.10
Previous studies have demonstrated that individual beliefs and perceptions can have a profound impact on health behaviors and outcomes in chronic diseases, including COPD.10,11 Patients who hold miasma theory beliefs may be less likely to engage with evidence-based prevention and treatment strategies, as they may attribute their condition to factors outside of their control, such as environmental “bad air”.7 Conversely, patients who have a more accurate understanding of the established risk factors for COPD may be more motivated to adopt behaviors that can positively impact their disease management and outcomes.9
Despite the potential significance of miasma theory beliefs on COPD outcomes, the relationship between these beliefs and disease-related outcomes has not been extensively investigated. A deeper understanding of this association could inform healthcare providers’ approaches to patient education, shared decision-making, and the development of personalized management strategies to improve overall disease outcomes in individuals with COPD.
This study aims to explore the relationship between miasma theory beliefs and disease outcomes in individuals with COPD. Specifically, it investigates whether individuals with COPD who hold miasma theory beliefs experience worse disease outcomes, such as increased symptom burden, exacerbations, and reduced quality of life, compared to those who do not hold these beliefs. The findings of this study have the potential to inform healthcare providers’ strategies for addressing the impact of patients’ beliefs on COPD management and to ultimately improve patient-centered care and outcomes.
Methods
Study Design and Participants
This case-control study took place at Department of Respiratory and Critical Care Medicine, the First Affiliated Hospital of Hebei University of Traditional Chinese Medicine, from January 2022 to May 2024. It involved 500 patients diagnosed with chronic obstructive pulmonary disease (COPD) and 500 control participants. Participants were recruited through outpatient clinics via in-person visits and telephone follow-ups. The study divided participants into two groups: one group consisted of individuals with a confirmed COPD diagnosis based on Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, specifically having a post-bronchodilator forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) ratio below 0.70 and an FEV1 less than 80% of the predicted value, indicating airflow limitation. The control group included individuals without COPD, matched for age (± 5 years), sex, and smoking history (current, former, or never smoker), who visited the outpatient clinics for routine check-ups. Blood samples for complete blood count (CBC) and C-reactive protein (CRP) were collected from both groups. Participants were required to be at least 40 years old and able to provide informed consent. Exclusion criteria included significant cognitive impairment, a primary respiratory diagnosis other than COPD for the COPD group, and a history of lung cancer or other severe respiratory conditions, with cognitive impairment assessed using the Addenbrooke’s Cognitive Examination (ACE)-III12 to ensure participants could provide informed consent.
Sample Size
Based on previous research on the prevalence of miasma theory beliefs in COPD patients,3 we estimated that the proportion of participants with high miasma theory beliefs would be 30% in the COPD group and 15% in the control group. To detect this difference with 80% power and a two-sided alpha of 0.05, a minimum sample size of 900 participants (450 in each group) was required. To account for a potential 10% dropout rate, we aimed to recruit a total of 1000 participants (500 in each group).
This study complies with the Declaration of Helsinki and obtained approval from the Medical Ethics Committee at the First Affiliated Hospital of Hebei University of Traditional Chinese Medicine (ethics approval number: HBZY2024-KY-018–01, China). All participating patients provided informed consent by signing the required documentation. Following the acquisition of written informed consent, participants completed questionnaires assessing their demographic characteristics, clinical history, and beliefs regarding the causes of COPD. Clinical data were collected, including lung function metrics for COPD patients, exacerbation history, and quality of life evaluations. This extensive dataset encompassed demographic factors, body mass index (BMI), smoking habits, pulmonary function, mMRC dyspnea scores, CAT scores, reported respiratory symptoms, comorbidities, medication history, clinical symptoms, laboratory results, drug use, length of hospital stay, and patient outcomes, while also examining comorbidities such as diabetes mellitus, cardiovascular disease, and sleep disorders.
Spirometry
Spirometry assessments were conducted using the ZAN GPI.3.00 device in a specialized laboratory for all patients diagnosed with chronic obstructive pulmonary disease (COPD) during stable periods, and airflow limitation was classified according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines,13 which categorize COPD into four stages based on the forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) ratio; specifically, mild COPD is characterized by an FEV1/FVC ratio of 0.70 or greater and an FEV1 of 80% or more of the predicted value, moderate COPD is indicated by an FEV1/FVC ratio of less than 0.70 and an FEV1 between 50% and 79% of the predicted value, severe COPD is defined by an FEV1/FVC ratio of less than 0.70 and an FEV1 between 30% and 49% of the predicted value, and very severe COPD is characterized by an FEV1/FVC ratio of less than 0.70 and an FEV1 of 30% or less; furthermore, the COPD group was further divided into two subcategories based on data from the hospital’s information system, where “Stable” COPD was defined as a period of at least three months without significant symptom changes or increased medication requirements, while “Acute Exacerbation” COPD was characterized by a prolonged worsening of symptoms such as dyspnea, coughing, or sputum production lasting at least 48 hours, necessitating an increase in maintenance medication usage or the addition of supplementary treatments.
The symptom burden of Chronic Obstructive Pulmonary Disease (COPD) was assessed using the COPD Assessment Test (CAT), a standardized tool that measures the impact of COPD symptoms on a patient’s daily life. The CAT is a 8-item questionnaire that asks patients to rate their symptoms, such as coughing, wheezing, and breathlessness, over the past 4 weeks.14
Measures
Miasma Theory Beliefs
The miasma theory beliefs questionnaire was created following a literature review and pilot-tested on a small group of COPD patients. To refine the questions, cognitive interviewing techniques were employed. This marks the first application of these questions in this specific context. Miasma beliefs were categorized into high, medium, and low levels based on a scoring system derived from the total questionnaire score, and we recognize the absence of established psychometric properties as a limitation. Participants’ beliefs regarding the causes of COPD were evaluated using a 10-item questionnaire specifically designed for this study. This questionnaire assessed the degree to which participants endorsed miasma theory beliefs, such as the notion that COPD is caused by “bad air” or environmental factors beyond their control. Responses were rated on a 5-point Likert scale, with higher scores reflecting stronger beliefs in the miasma theory.
HRQL Questionnaires
The St. George’s Respiratory Questionnaire (SGRQ) is a self-administered instrument that consists of 50 items, which are categorized into three components: symptoms, activity, and impact on daily life, and scores range from 0 to 100, with 0 indicating no impairment in health-related quality of life (HRQL), and higher scores representing worse HRQL, with a minimal important difference (MID) of four points proposed for the total SGRQ score.15 Participants also completed the Hamilton Anxiety Scale (HAM-A) to assess anxiety symptoms and the Beck Depression Inventory (BDI) to assess depressive symptoms. Additionally, participants in the COPD group underwent arterial blood gas (ABG) analysis and reported the presence and severity of COPD-related symptoms, such as chest pain, wheezing, and cough. In cases where blood gas analysis was not performed, oxygen saturation levels were recorded using pulse oximetry. This study aimed to investigate the potential association between miasma beliefs and systemic inflammation, as evidenced by alterations in laboratory biomarkers including neutrophil-to-lymphocyte ratio (NLR), and C-reactive protein (CRP). Furthermore, the study explored potential correlations between changes in miasma beliefs and variations in biomarkers associated with COPD).
Statistical Analysis
Statistical analysis was performed to characterize the study population and examine the relationship between miasma theory beliefs and COPD. Descriptive statistics were used to summarize demographic and clinical characteristics, while bivariate analyses (t-tests and chi-square tests) were conducted to identify differences between the COPD and control groups. Statistical analyses were conducted to evaluate the influence of demographic and health-related variables on beliefs in the miasma theory. Crude and adjusted odds ratios (OR) with 95% confidence intervals (CI) were calculated using logistic regression models. The crude model assessed the relationship between each variable and belief in the miasma theory without controlling for potential confounders. Two adjusted models were employed: Adjusted Model 1 controlled for age and gender, while Adjusted Model 2 further included education, alcohol consumption, body mass index (BMI), and respiratory symptoms. To evaluate the model’s accuracy in classifying beliefs about COPD, we assessed several goodness of fit metrics: sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the proportion of correctly classified instances. The sensitivity indicated the model’s effectiveness in identifying individuals with strong Miasma beliefs, while the specificity reflected its ability to accurately identify those without such beliefs. The PPV and NPV confirmed the reliability of the classifications. Overall, the model demonstrated a high accuracy rate in linking Miasma beliefs to health outcomes in COPD patients. All analyses were performed using SPSS Statistics version 23, with a p-value < 0.05 considered statistically significant.
Results
A comparative study was conducted on 500 patients with COPD who had experienced a stable period and an acute exacerbation, as well as 500 healthy control subjects matched for age, sex, and smoking history. The demographic and laboratory data of participants in both COPD groups and the control group are presented in Table 1. The study cohort had a mean age of 64 years, with a gender distribution of approximately two-thirds male. The results show a significant difference in all complete blood count (CBC) parameters across groups. Specifically, the levels of white blood cells, neutrophils, neutrophil-to-lymphocyte ratio, red blood cell distribution width, and C-reactive protein were higher in the exacerbated COPD group compared to the stable COPD group and the control group (Table 1). Notably, there was no significant difference in age, sex, and smoking history among the groups, indicating a good match between cases and controls. Additionally, patients with COPD had higher scores on anxiety and depression assessments compared to the control group. Furthermore, the results revealed a significant difference in Miasma Belief Level, with COPD patients exhibiting higher scores compared to the control group and exacerbated COPD patients having higher scores compared to those with stable COPD (p = 0.001). The distribution of miasma theory belief levels was skewed towards the higher end, with 81% having high beliefs, 18% moderate, and 1.4% low.
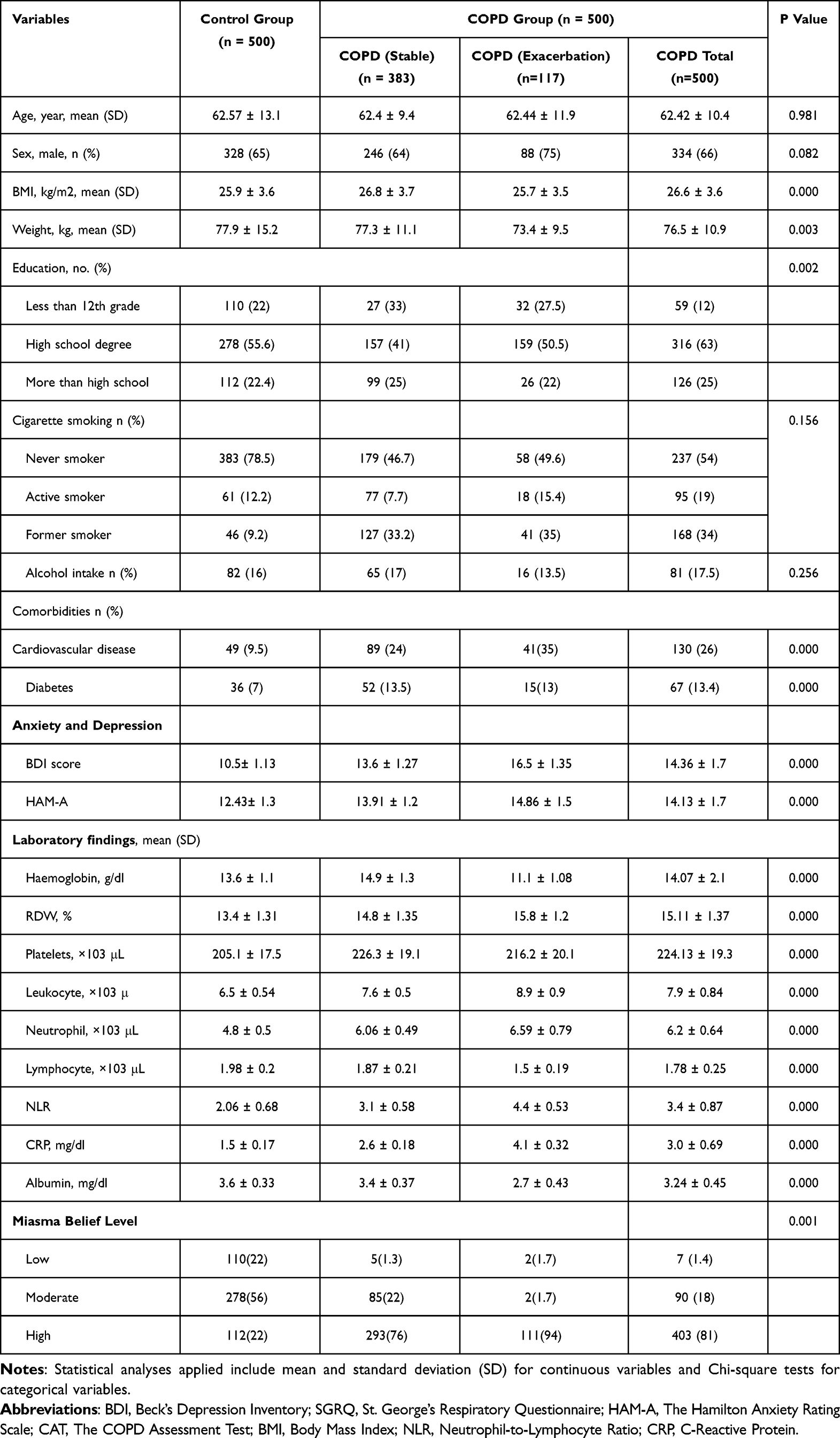 |
Table 1 Comparing Demographic and Laboratory Characteristics in Cases and Controls Groups (n=1000) |
Table 2 presents the anxiety, depression, and SGRQ total scores, as well as pulmonary function tests, for patients with COPD across different GOLD stages. The results show that mean FEV1, FEV1/FVC, and %CAT values were significantly different across GOLD stages (p < 0.001), indicating a decline in lung function as COPD severity increases. Specifically, patients in Stage 4 exhibited the poorest lung function. Additionally, clinical symptoms of depression and anxiety, as measured by BDI, HAM-A, and total SGRQ scores, worsened as the disease progressed (p < 0.001). Notably, these symptoms were more pronounced in patients with more advanced COPD (Table 2).
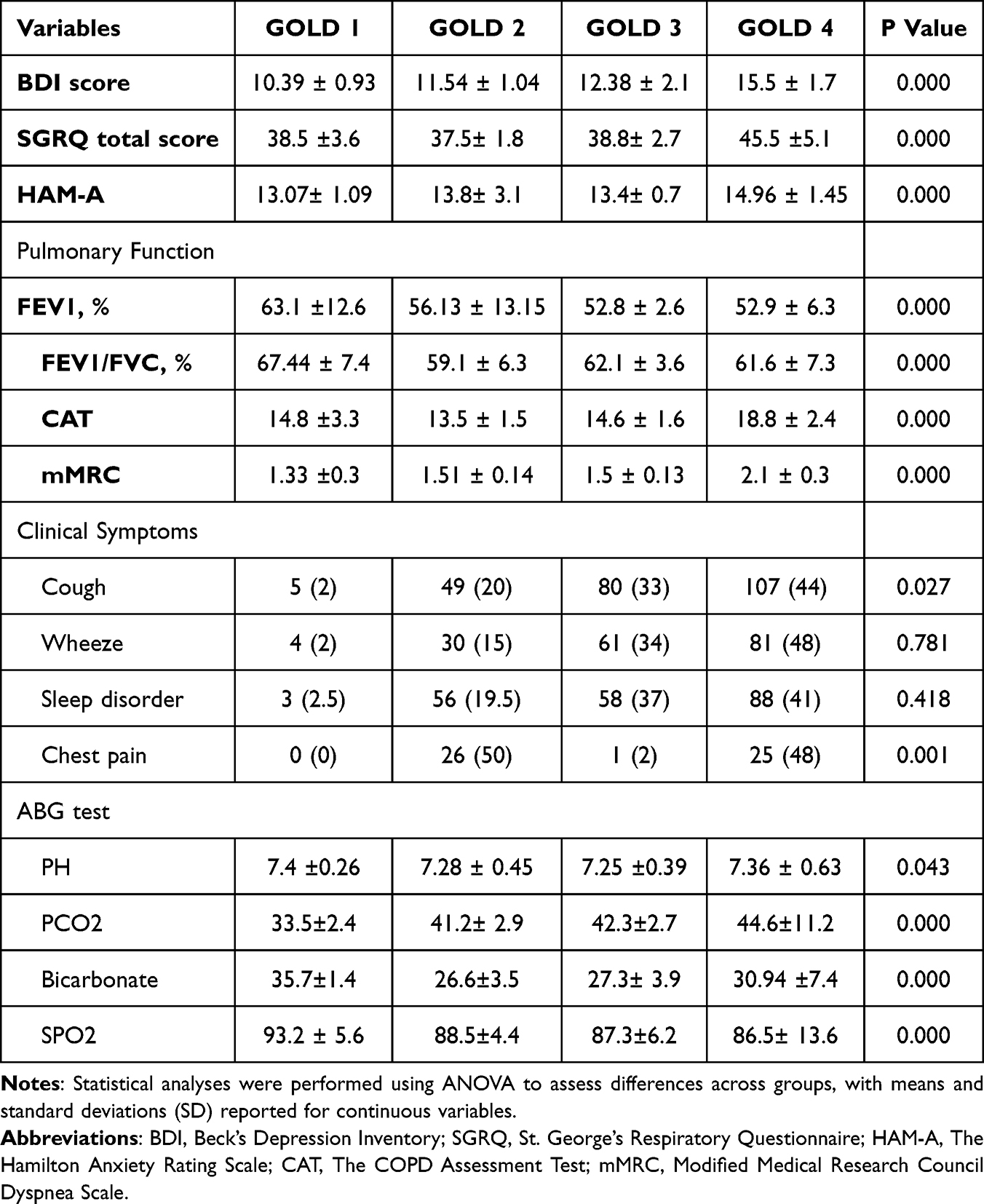 |
Table 2 Anxiety, Depression and Quality-of-Life Score and Pulmonary Function Tests of COPD Patients (n=500) |
Table 3 reveals a significant association between patients’ beliefs in the miasma theory and their COPD outcomes. Specifically, individuals with strong beliefs in the miasma theory exhibited worse dyspnea, with a mean CAT score of 23 compared to 14 in the low-belief group (p < 0.001). They also reported a significantly higher symptom burden related to lung function, as indicated by the FEV1 scores, with mean values of 46 for those with stronger miasma beliefs and 54 for those with weaker beliefs (p < 0.001). These findings suggest that stronger beliefs in the miasma theory correlate with more severe subjective symptoms in COPD. Furthermore, patients with high miasma theory beliefs experienced poorer quality of life, indicated by a mean SGRQ total score of 48, compared to 39 in the low-belief group (p < 0.001). This 9-point difference exceeds the minimal clinically important difference of 4 points for the SGRQ, highlighting substantial quality of life impairment linked to stronger miasma theory beliefs. Notably, laboratory biomarkers such as neutrophils, NLR, RDW width, and CRP were also elevated in the high-belief group compared to the low-belief group (Table 3). Additionally, patients with high miasma theory beliefs reported higher levels of anxiety and depression compared to the control group (p = 0.001). In summary, these detailed results consistently demonstrate that deeply held beliefs in the miasma theory of disease are associated with worse symptom burden, quality of life, and exacerbation of symptoms in COPD patients.
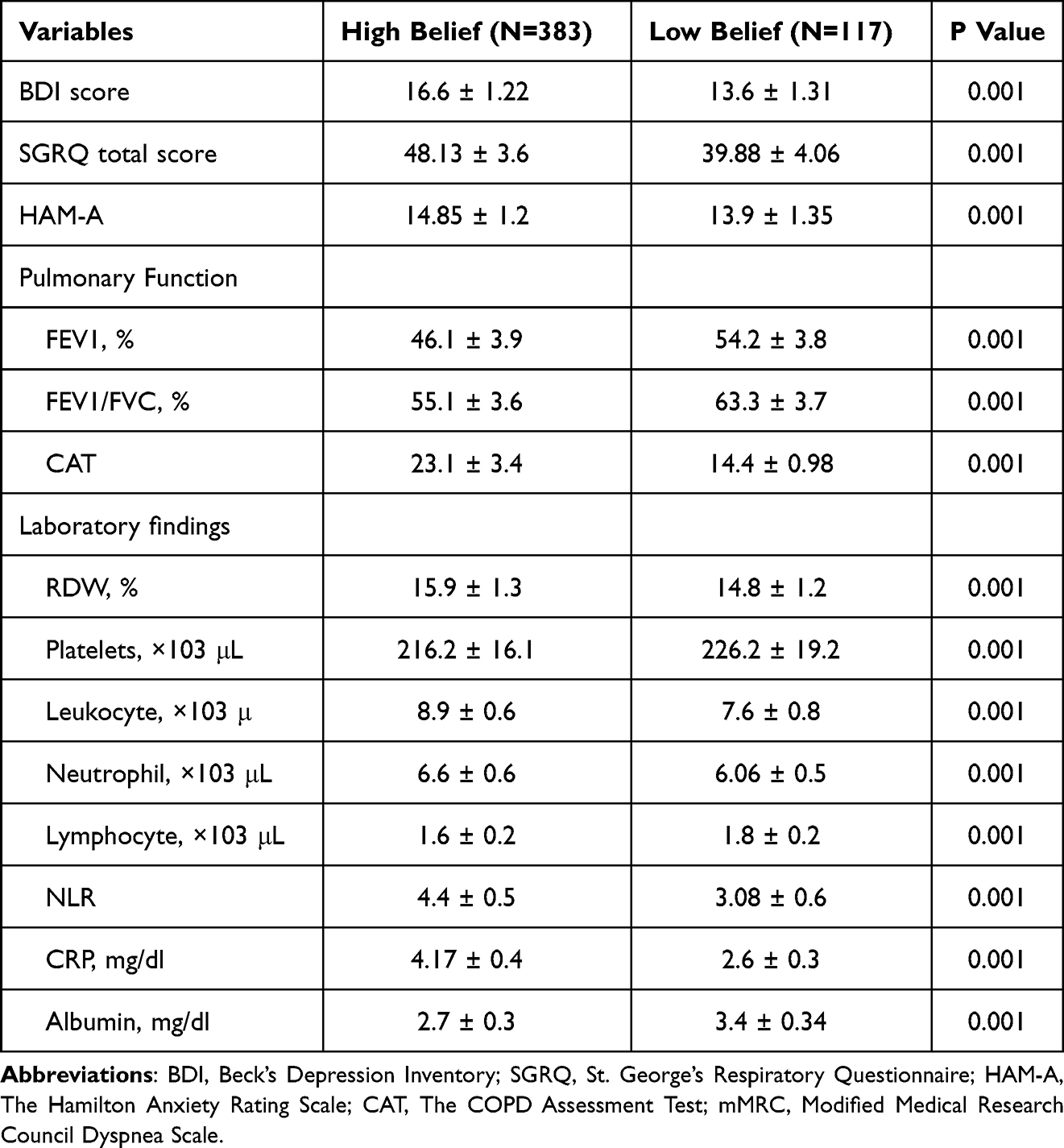 |
Table 3 Relationship Between Miasma Theory Belief and COPD Outcomes |
The examination of Table 4 demonstrates that various demographic and health-related factors significantly influence beliefs in the miasma theory. Notably, males have lower odds of adhering to this belief compared to females, with an odds ratio (OR) of 0.62 (95% CI: 0.47–0.80). Age also plays a variable role, particularly for individuals aged 45–60, who exhibit an increased OR of 1.36 (95% CI: 1.49–46.66) in adjusted models. Education plays a crucial role, as individuals with less education demonstrate significantly higher beliefs in the theory. Alcohol consumption and higher BMI are associated with reduced beliefs, whereas respiratory symptoms, such as cough and chest pain, correlate with increased belief, suggesting a link between health perceptions and environmental health risks. Additionally, individuals with sleep disorders and severe respiratory conditions (GOLD 4) show heightened beliefs. The presence of certain respiratory symptoms was also associated with a greater likelihood of believing in the miasma theory. Specifically, participants who reported experiencing cough, chest pain, dyspnea, wheeze, or sleep disorder were more likely to believe in the miasma theory. Generally, the model indicates a reliable classification of these beliefs, highlighting the complex interplay of these variables. Overall, the model had good goodness of fit indices, with sensitivity and specificity values ranging from 0.65 to 0.96. The positive predictive value was 78.04%, while the negative predictive value was 65.25%.
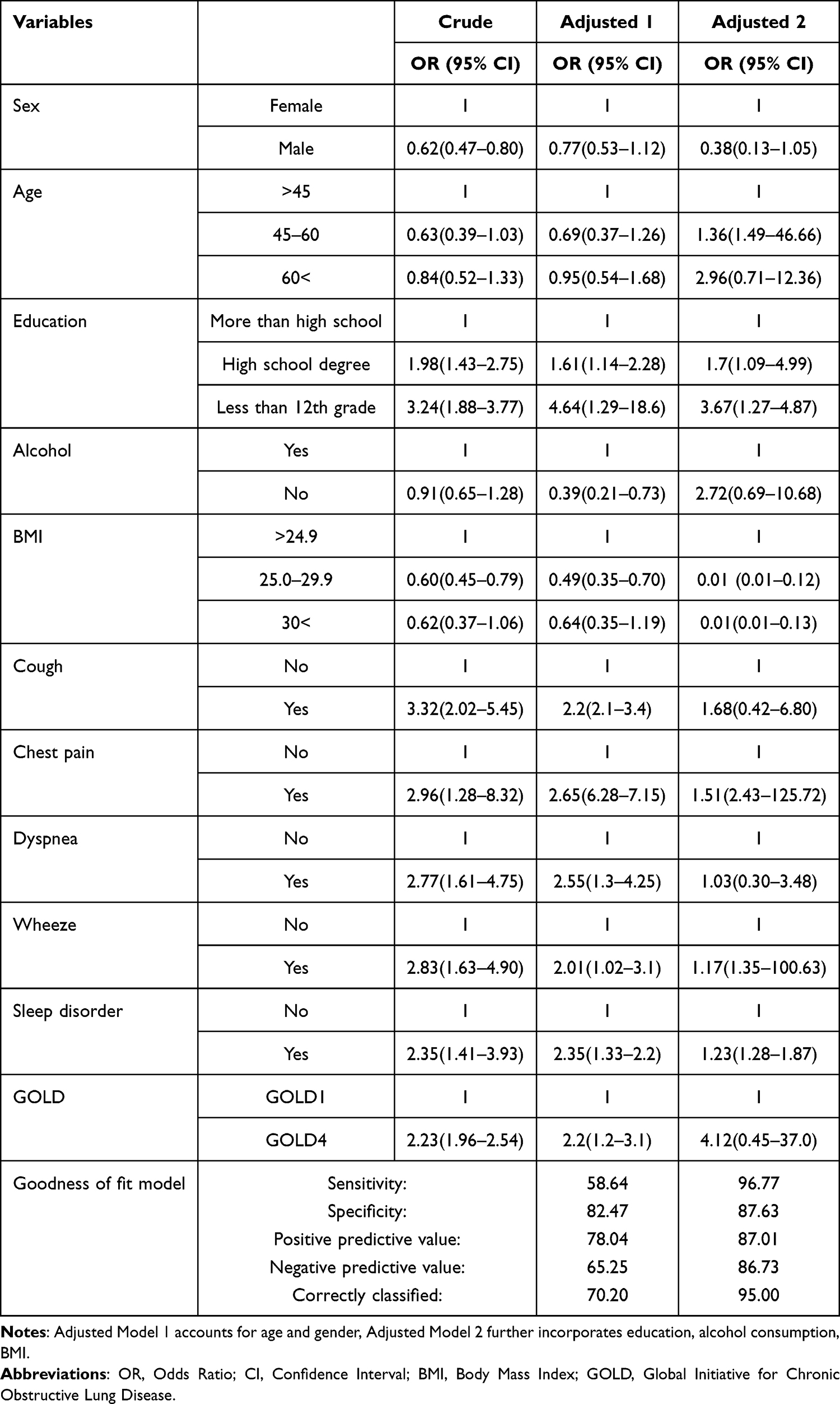 |
Table 4 Influence of Age, Gender, and Other Variables on Miasma Theory Belief |
Discussion
This study provides preliminary evidence that beliefs in the miasma theory significantly impact health outcomes for individuals with COPD. Notably, 81% of COPD patients attribute their condition to “bad air” or noxious fumes, underscoring the enduring influence of historical health beliefs, despite extensive scientific knowledge that contradicts them. Our findings indicate a significant association between adherence to miasma theory beliefs and adverse outcomes in COPD patients. Individuals who adhered to these antiquated beliefs exhibited more severe symptoms, diminished lung function, and a reduced quality of life in comparison to those who did not subscribe to such notions. While our regression analysis supports an independent association between miasma beliefs and these negative outcomes, it is important to recognize that other factors may also contribute to these associations, even after adjusting for demographic and clinical variables.
These findings underscore the enduring influence of the miasma theory on contemporary healthcare, particularly in the context of chronic respiratory diseases. The persistence of such beliefs highlights a critical gap in health education and patient-centered care. Our results suggest that miasma theory beliefs may contribute to a vicious cycle of worsened symptoms, reduced quality of life, and potentially accelerated disease progression. The psychological impact of holding miasma theory beliefs cannot be overstated. The perception of COPD as an uncontrollable, environmentally determined condition may lead to feelings of helplessness, anxiety, and depression, as evidenced by our findings of higher anxiety and depression scores among patients with strong miasma theory beliefs.16 These psychological factors may further exacerbate the physical symptoms of COPD and hinder adherence to treatment regimens. Our findings align with previous research demonstrating the impact of illness perceptions on COPD outcomes. Studies have shown that patients with maladaptive beliefs about their disease are more likely to experience poorer quality of life, higher levels of anxiety and depression, and lower adherence to treatment recommendations.17 However, to our knowledge, this is the first study to specifically examine the association between miasma theory beliefs and COPD outcomes.
The implications of these findings are profound. The association between strong miasma beliefs and worse disease outcomes—characterized by increased symptom severity, poorer lung function, and reduced quality of life—suggests that these beliefs may serve as significant barriers to effective disease management. Patients who subscribe to the miasma theory may perceive their condition as largely influenced by uncontrollable environmental factors. This perception can lead to a sense of helplessness, inhibiting proactive engagement with evidence-based treatment options and self-management strategies.
For instance, patients might avoid smoking cessation programs, pulmonary rehabilitation, or other interventions, believing that their condition is predetermined by external “bad air.” This aligns with previous research indicating that patients with maladaptive illness beliefs often exhibit lower adherence to treatment protocols.9,18 The emotional toll of such beliefs is evident in the higher levels of anxiety and depression reported among those who adhere to miasma theory, suggesting that psychological distress exacerbates physical symptoms, creating a feedback loop that worsens overall health.
Understanding the mechanisms through which miasma beliefs impact health outcomes requires a multi-faceted approach. Psychological frameworks, such as the Health Belief Model, suggest that individuals’ perceptions of susceptibility to illness and the perceived severity of their condition influence health behaviors.17,19 In this context, patients who believe that their COPD is caused by miasma may underestimate the importance of lifestyle modifications, such as smoking cessation or avoiding environmental triggers, viewing their condition as an unavoidable consequence of external factors.
Furthermore, the social implications of adhering to miasma beliefs are complex and warrant further exploration. While it has been suggested that individuals who subscribe to miasma theory may experience stigma or social isolation, it is also plausible that shared beliefs could foster social connections among those with similar perspectives. Current literature indicates that collective beliefs can sometimes enhance social cohesion, although our study did not specifically assess social isolation. Therefore, future research should investigate the relationship between miasma beliefs and social dynamics, as well as their potential impact on patients’ willingness to seek assistance and engage in community support. Additionally, future research should consider the role of self-efficacy in shaping health beliefs and whether these beliefs are more prevalent before or after a COPD diagnosis. Although our study did not specifically assess this aspect, understanding the timing of these beliefs could provide valuable insights into their development and impact on patient outcomes.
The findings of this study resonate with existing literature that emphasizes the role of illness perceptions in chronic disease management. For example, research has shown that patients who understand their illness in terms of controllable risk factors are more likely to engage in health-promoting behaviors.9,20 This study extends those findings by specifically linking miasma beliefs to adverse health outcomes in COPD patients, highlighting a critical area for intervention in clinical practice.
Moreover, previous studies have indicated that cultural beliefs about health can significantly influence health-seeking behavior and treatment adherence.21–23 The persistence of miasma beliefs may reflect broader societal attitudes toward environmental health risks, suggesting that healthcare providers must consider these cultural contexts when developing patient education programs.
Despite the significant insights provided by this study, several limitations must be acknowledged. The cross-sectional design restricts the ability to draw causal conclusions, and reliance on self-reported measures may introduce bias. Future research should aim for longitudinal studies that track changes in beliefs and health outcomes over time, providing a clearer picture of the relationship between miasma beliefs and COPD progression. Additionally, qualitative research could deepen our understanding of how cultural and social factors sustain miasma beliefs. Exploring patients’ narratives may reveal the underlying reasons for these beliefs and how they influence health behaviors. Such insights could inform the development of targeted interventions aimed at reshaping patients’ perceptions and improving treatment adherence.
Given the significant association between miasma beliefs and health outcomes, educational interventions should be prioritized in clinical settings. Healthcare providers can play a crucial role in addressing these beliefs by offering evidence-based information about COPD and its risk factors. Tailored educational programs that demystify the causes of COPD and emphasize the importance of controllable factors may empower patients to take a more active role in their disease management. Incorporating discussions about miasma beliefs into routine care could facilitate open dialogue, allowing healthcare providers to address misconceptions and reinforce the importance of evidence-based practices. This approach not only enhances patient knowledge but also fosters a therapeutic alliance, encouraging patients to engage more fully in their care. Future research should explore the underlying mechanisms linking miasma theory beliefs to adverse COPD outcomes. Qualitative studies can provide deeper insights into patients’ perspectives and experiences, while longitudinal studies can examine the temporal relationship between beliefs and disease progression. Additionally, interventions targeting miasma theory beliefs should be developed and evaluated to assess their effectiveness in improving COPD outcomes.
Conclusion
In conclusion, this study suggests a potential association between miasma theory beliefs and health outcomes in COPD patients. It emphasizes the importance of healthcare providers recognizing these beliefs for effective disease management. Targeted educational interventions may enhance patient engagement and adherence, improving health outcomes. Further research is needed to assess the impact of these initiatives on patient perceptions and management strategies for COPD, particularly in correcting misconceptions to boost treatment adherence.
Data Sharing Statement
All data generated and analyzed during this study are included in the manuscript. The corresponding author can provide access to the datasets used in this study upon a reasonable request.
Ethical Approval
Our study received approval from the Medical Ethics Committee of the First Affiliated Hospital of Hebei University of Traditional Chinese Medicine (ethics approval number: HBZY2024-KY-018–01, China).
Consent for Publication
All authors support the submission to this journal.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors are grateful to the participants who took part in the study.
Author Contributions
Yexian Zhao, Yunlei Ma and Limei Geng obtained designing, conceptualized this study and supervised; Limei Geng and Jia Nie performed experiments, acquired data and analyzed data; Yexian Zhao drafted the manuscript; critically revised the manuscript; All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that there is no conflict of interest.
References
1. Safiri S, Carson-Chahhoud K, Noori M. et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:1. doi:10.1136/bmj-2021-069679
2. Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899–909. doi:10.1016/S0140-6736(14)60446-3
3. Kale MS, Federman AD, Krauskopf K, et al. The association of health literacy with illness and medication beliefs among patients with chronic obstructive pulmonary disease. PLoS One. 2015;10(4):e0123937. doi:10.1371/journal.pone.0123937
4. Laue J, Melbye H, Risør MB. Self-treatment of acute exacerbations of chronic obstructive pulmonary disease requires more than symptom recognition – a qualitative study of COPD patients’ perspectives on self-treatment. BMC Family Pract. 2017;18(1):1–10. doi:10.1186/s12875-017-0582-8
5. Vaske I, Kenn K, Keil DC, et al. Illness perceptions and coping with disease in chronic obstructive pulmonary disease: effects on health-related quality of life. J Health Psychol. 2017;22(12):1570–1581. doi:10.1177/1359105316631197
6. Bergeson K. The Poisonous Night: miasmatic Theory and Medical Astrology in 19th Century Britain. Janus. 2022;2022:3.
7. Kannadan A. History of the miasma theory of disease. Essai. 2018;16(1):18.
8. Jones MG, Richeldi L. Air pollution and acute exacerbations of idiopathic pulmonary fibrosis: back to miasma? European Respiratory Journal. 2014;43(4):956–959. doi:10.1183/09031936.00204213
9. Krauskopf K, Federman AD, Kale MS, et al. Chronic obstructive pulmonary disease illness and medication beliefs are associated with medication adherence. COPD. J Chronic Obstruct Pulmonary Dis. 2015;12(2):151–164. doi:10.3109/15412555.2014.922067
10. Hill K, Hug S, Smith A, et al. The Role of Illness Perceptions in Dyspnoea-Related Fear in Chronic Obstructive Pulmonary Disease. J Clin Med. 2023;13(1):200. doi:10.3390/jcm13010200
11. Blackstock FC, ZuWallack R, Nici L, et al. Why don’t our patients with chronic obstructive pulmonary disease listen to us? The enigma of nonadherence. Ann Am Thoracic Soc. 2016;13(3):317–323. doi:10.1513/AnnalsATS.201509-600PS
12. Moore K. Exploring the Influence of Physical and Mental Health Factors on Older Adults’ Performance on the Addenbrooke’s Cognitive Examination III (ACE-III). 2023.
13. Gómez FP, Rodriguez-Roisin R. Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines for chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2002;8(2):81–86. doi:10.1097/00063198-200203000-00001
14. Burchette JE, Click IA, Johnson L, et al. Relationship of patient self-administered COPD assessment test to physician standard assessment of chronic obstructive pulmonary disease in a family medicine residency training program. J Patient-Center Res Rev. 2019;6(3):210. doi:10.17294/2330-0698.1699
15. Rutten-van Mölken M, Roos B, Van Noord J. An empirical comparison of the St George’s Respiratory Questionnaire (SGRQ) and the Chronic Respiratory Disease Questionnaire (CRQ) in a clinical trial setting. Thorax. 1999;54(11):995–1003. doi:10.1136/thx.54.11.995
16. Halpin D, Hyland M, Blake S, et al. Understanding fear and anxiety in patients at the time of an exacerbation of chronic obstructive pulmonary disease: a qualitative study. JRSM Open. 2015;6(12):2054270415614543. doi:10.1177/2054270415614543
17. Poletti V, Pagnini F, Banfi P, et al. Illness perceptions, cognitions, and beliefs on COPD patients’ adherence to treatment–a systematic review. Patient Preference Adherence. 2023;Volume 17:1845–1866. doi:10.2147/PPA.S412136
18. Rogliani P, Ora J, Puxeddu E, et al. Adherence to COPD treatment: myth and reality. Respir Med. 2017;129:117–123. doi:10.1016/j.rmed.2017.06.007
19. Agarwal P, Lin J, Muellers K, et al. A structural equation model of relationships of health literacy, illness and medication beliefs with medication adherence among patients with chronic obstructive pulmonary disease. Patient Educ Couns. 2021;104(6):1445–1450. doi:10.1016/j.pec.2020.11.024
20. Celebi C, Calik-Kutukcu E, Saglam M, et al. Health-Promoting behaviors, health literacy, and levels of knowledge about smoking-related diseases among smokers and non-smokers: a cross-sectional study. Tuberculosis Respiratory Diseases. 2021;84(2):140. doi:10.4046/trd.2020.0158
21. Rasul FB, Sarker M, Yasmin F, et al. Exploring health-seeking behavior for non-communicable chronic conditions in northern Bangladesh. PLOS Global Public Health. 2022;2(6):e0000497. doi:10.1371/journal.pgph.0000497
22. Zou X, Fitzgerald R, Nie J-B. “Unworthy of Care and Treatment”: cultural Devaluation and Structural Constraints to Healthcare-Seeking for Older People in Rural China. Int J Environ Res Public Health. 2020;17(6):2132. doi:10.3390/ijerph17062132
23. Tang S, Dong D, Ji L, et al. What Contributes to the Activeness of Ethnic Minority Patients with Chronic Illnesses Seeking Allied Health Services?A Cross-Sectional Study in Rural Western China. Int J Environ Res Public Health. 2015;12(9):11579–11593. doi:10.3390/ijerph120911579
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.