Back to Journals » Patient Preference and Adherence » Volume 17
The Medication Use Issues and Challenges of Mental Illness Exacerbation in Patients with Schizophrenia: A Qualitative Study in Thailand
Authors Klinpiboon P ![]() , Chanthapasa K
, Chanthapasa K ![]()
Received 5 September 2023
Accepted for publication 7 November 2023
Published 13 November 2023 Volume 2023:17 Pages 2927—2937
DOI https://doi.org/10.2147/PPA.S420973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Ponglapat Klinpiboon,1,2,* Kornkaew Chanthapasa2,*
1Department of Pharmacy, Nakhon Ratchasima Rajanagarindra Psychiatric Hospital, Nakhon Ratchasima, Thailand; 2Faculty of Pharmaceutical Sciences, Khon Kaen University, Khon Kaen, Thailand
*These authors contributed equally to this work
Correspondence: Kornkaew Chanthapasa, Faculty of Pharmaceutical Science, Khon Kaen University, No. 123, Moo 16, Mittraphap Road, Nai-Muang, Muang District, Khon Kaen, 40002, Thailand, Tel +66 812 618 095, Fax +66 4320 2379, Email [email protected]
Purpose: Patients with schizophrenia often experience mental illness exacerbations, which lead to frequent re-hospitalization. Non-adherence to medication is the main cause of relapses, despite many patients requiring lifelong treatment. Non-adherence consequences include higher re-admission and suicide rates, worse progression of mental illness, higher rates of violence by patients with mental illness, and increased use of emergency psychiatric services. This directly impacts the cost and workload of the mental healthcare system. This study aims to understand medication non-adherence among schizophrenia patients in Thailand based on the country’s specific context.
Patients and Methods: This qualitative research study explored the causes of non-adherence to medication and health perceptions among patients with schizophrenia in Thailand. Five patients with schizophrenia were included in this study. Data was collected through in-depth interviews, recordings of treatments, and field notes based on the interpretive perspective of key informants with the concept of phenomenology.
Results: Thematic analysis revealed two main themes associated with mental illness exacerbation: triggers of exacerbation and medication non-adherence. The triggers that emerged from the data were substance abuse and psychological stress. Medication non-adherence issues were misunderstandings about mental illness and its treatment, lack of participation in treatment, and difficulty accessing mental health services.
Conclusion: This study explored the importance of medication adherence in patients with schizophrenia. Non-adherence to medication can worsen mental illness and create a vicious cycle that makes treatment more challenging. Substance abuse and psychological stress can also exacerbate this cycle. Mental health services should strive to improve medication adherence strategies and offer social support to prevent harmful behaviors and break the vicious cycle.
Keywords: schizophrenia, medication adherence, mental health service, medication management
A Letter to the Editor has been published for this article.
A Response to Letter by Mrs Siahaya has been published for this article.
Introduction
Patients with schizophrenia often experience mental illness exacerbations, leading to frequent re-hospitalization. According to a worldwide study, 43.7% of patients with schizophrenia were re-hospitalized.1 The leading cause of these relapses is non-adherence to medication, despite many patients with schizophrenia requiring lifelong treatment. Global studies report non-adherence rates as high as 56%.2 Medication non-adherence can result in the recurrence of relapses and related problems. A systematic literature review3 identified three types of consequences of non-adherence: 1) adverse effects on patients themselves, such as higher readmission and suicide rates and worse progression of mental illness, 2) consequences for society, including higher rates of violence by patients with mental illness, 3) consequences for the healthcare system include increased emergency psychiatric service use and higher re-admission rates. These consequences directly impact the cost and workload of the mental health service system. A Study on the consequences of medication non-adherence in Thailand4 has yielded results consistent with global studies. However, there is a lack of quality research in Thailand that could help better understand the problem of medication non-adherence in patients with schizophrenia. Because the environmental and social contexts, cultural patterns, and patients’ beliefs differ based on the area, this study aims to understand the causes of medication non-adherence based on the country’s specific context among patients with schizophrenia in Thailand.
Materials and Methods
This study used a qualitative research approach, with data collected through in-depth interviews, recording of some treatments, and field notes. The research method is based on the interpretive perspective of the key informants, in line with the philosophical concept of phenomenology. The goal is to explore the causes of non-adherence to medication among patients with schizophrenia in Thailand.
Data Collection
The data collection period for this study was from March 2022 to February 2023 at Nakhon Ratchasima Rajanagarindra Psychiatric Hospital, Thailand. The participants were all patients with schizophrenia who were staying in the inpatient department and were in the rehabilitation phase, assessed as having good awareness, and had problems related to medication use. Psychiatric nurses in the inpatient department who cared closely for these volunteers recommended those who were willing and qualified according to the research objectives. In-depth interviews were conducted separately in a hospital room for advice. A total of 12 volunteers shared their stories, and five were considered suitable as key informants for this study and were interviewed in-depth several times.
Data Analysis
The data obtained from in-depth interviews was transcribed verbatim and compared with field notes, introductory patient history records, and partial treatment notes recorded by mental health professionals. If any part of the information was unclear or raised doubts, the researchers asked psychiatrists, clinical psychologists, or other mental health professionals for clarification to ensure the accuracy and completeness of the data. Data coding was performed after each interview to ensure accuracy and to prevent confusion in future interviews. Atlas.ti (version 9) software was used for data analysis, with hypothetical names used to replace actual names and paired with the key informant’s sequence number. Thematic analysis5,6 was employed for data analysis. The two researchers reviewed the data obtained from each interview and checked the content disclosure appropriateness with psychiatrists and clinical psychologists from the psychiatric hospital mentioned.
Ethics
This study was approved by the Human Research Ethics Committee of Khon Kaen University, with project number HE642246. The study followed the principles of the Helsinki Declaration and the Good Clinical Practice Guidelines (ICH GCP). Additionally, the Research Ethics Committee of the Nakhon Ratchasima Rajanagarindra Psychiatric Hospital approved the study under project number 05-122564. The informed consent form for this study underwent evaluation and review by both the Human Research Ethics Committee of Khon Kaen University and the Research Ethics Committee of the Nakhon Ratchasima Rajanagarindra Psychiatric Hospital. The purpose of the informed consent form is to inform key informants about the study, including its research objectives, anticipated benefits, data collection procedures through in-depth interviews, the right to participate, the process of giving consent, and the option to refuse to answer questions or withdraw from the study at any time. It also emphasizes the confidentiality of key informants’ personal information and ensures that no real names or identifiable information will be associated with them. The researcher verbally provided information to key informants, particularly the publication with anonymous names, with a relative or guardian present to listen. The Informed consent was obtained through the signature of the key informants, a relative or guardian who co-signed as a witness during the consent process. In cases where the key informant did not have a relative or guardian or could not be contacted, a psychiatric nurse acted as a witness during the consent process and co-signed as a witness. The publication information did not include names and removed any data that may link to key informants.
Results
This study included five key informants diagnosed with schizophrenia for over a year and had a history of re-hospitalization due to non-adherence with their medication. Details of the demographic characteristics are shown in Table 1.
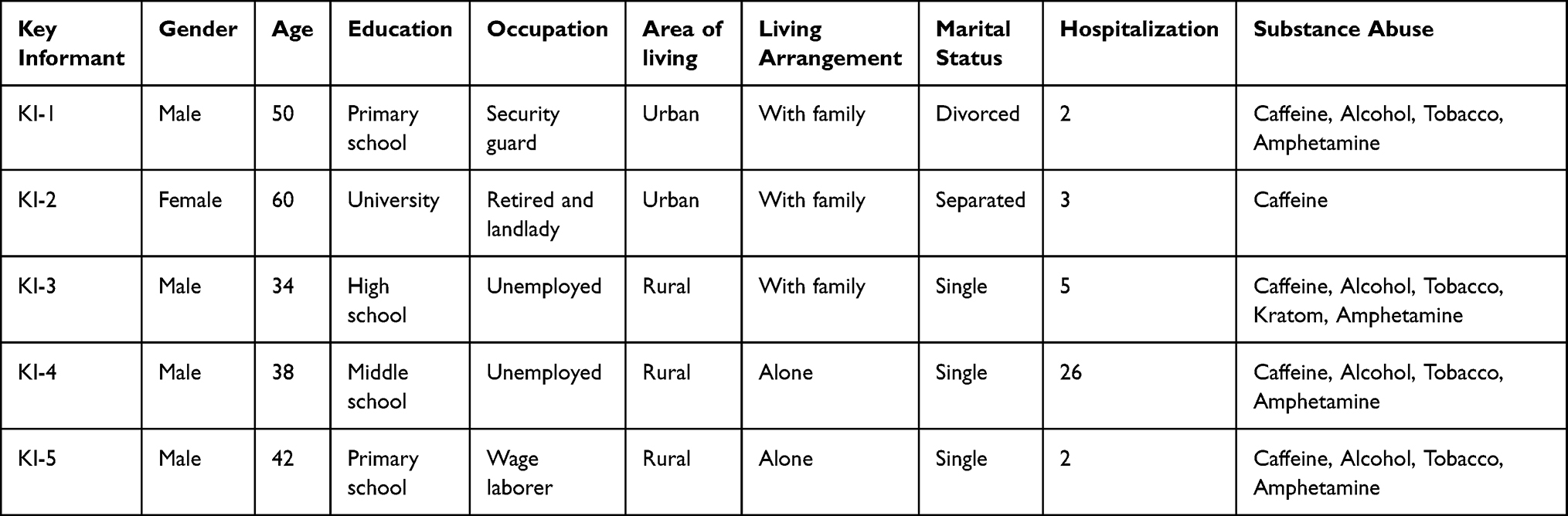 |
Table 1 Demographic Characteristics of Key Informants |
Medication use behavior depends on the mental health condition of the individual. Patients with schizophrenia might experience recurring mental illness exacerbations, during which they are unable to take care of themselves as usual, reducing the likelihood of returning to medication use. Therefore, mental health conditions are crucial in collaboration for medication use, as illustrated in Figure 1.
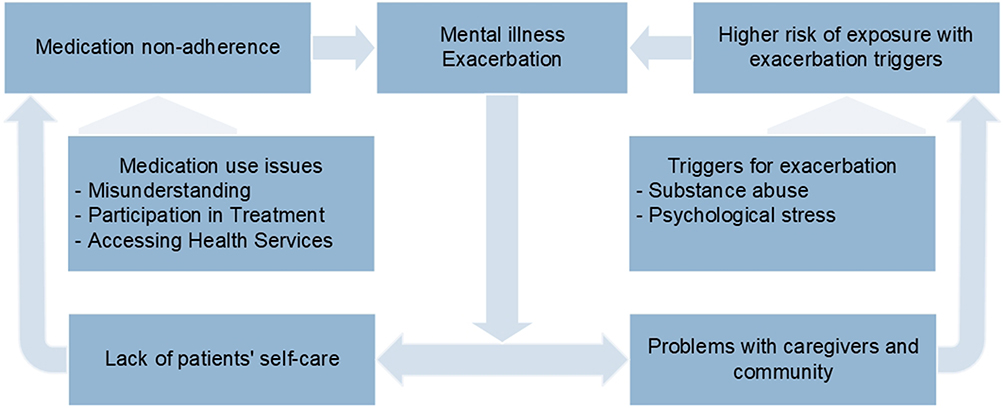 |
Figure 1 The vicious cycle of medication non-adherence and mental illness exacerbation. |
Mental Illness Exacerbation
I cannot control it, the ringing in my ears comes. It cannot be controlled, sir. When people pass by, they can tell that I. have a problem. (KI-1)
When experiencing an exacerbation of a mental illness, KI-1’s behavior changed. He bowed to various things or performed strange postures. He believed his psychotic symptoms were caused by drinking too much alcohol: “It is neurosis, sir. My nerves talk to me because I drink a lot of alcohol”. According to KI-1’s perspective, the only way to improve symptoms was to “only take my medication”. However, it was found that when medication was discontinued and ringing in the ears or his neurosis reappeared, medication had to be retaken for about a month before the symptoms disappeared. It is consistent with the principle of psychotropic medication that if the medication is taken, symptoms will not improve immediately.
It fades away gradually, sir. People speaking in my mind will gradually disappear… little by little… two persons… one person by the time. It takes a full month to disappear.
Therefore, continuous medication use is essential, as it takes a relatively long time to calm mental symptoms. During that time, KI-1’s younger brother cared for various things, limiting his behavior at home. However, his brother still could not care for him completely, and he eventually had to be sent to the psychiatric hospital. The situation is similar to KI-2’s, who also had to be sent to the psychiatric hospital when her daughter could not care for her. As for cases without caregivers like KI-3, KI-4, and KI-5, until they were sent back to the mental health care system, all three had severe mental symptoms, causing problems in their community.
Triggers for Mental Illness Exacerbation
Substance Abuse
The first time, I admit it, I used a lot of drugs… At first, I used a lot of drugs and wanted to see which would win between myself and the drugs. The drugs won (laugh). I used meth. (KI-3)
KI-3 admitted to having used illegal drugs such as “meth” and had a history of various substance abuse.
I have been using it for the past three or four months, meth and tobacco. As for marijuana, I stopped using it. Sometimes, I use kratom, but that is it. Sometimes.
The amount of substance use was relatively high. The reason KI-3 used additive substances was the happiness he experienced during that time. “It is like temporary happiness”. Moreover, to ironize his failed life. “It is self-sarcastic. I want to die”. He had mentioned suicide many times. Furthermore, he waited for when he would die from various problems in his life.
KI-1 talked about an energy drink containing high caffeine he consumes daily. He said
I drink it (energy drink) when I feel drowsy. Yes, I still drink it, sir. Do not drink it if you are not drowsy because it can make you nervous. When I take it too much, it will sound in my ears, and alcoholic drinks will make me neurotic, too.
He knew consuming too many energy drinks might bring back auditory hallucinations, but KI-1 still could not quit drinking. Meanwhile, KI-4 enjoyed drinking high-caffeine drinks such as instant and fresh coffee. However, unlike most people who drink one or two cups daily, he drank more than 4 to 5 cups per day. Substance abuse, not only illegal substances but also drinks or foods that are generally easy to find, may trigger mental illness. KI-4 also suspected that his mental illness might be related to substance abuse.
Psychosis… there was alcohol, drugs, and stimulants. Before, I was normal. But I used too many drugs. It may be related. It is like someone put a microchip in my head (headache and hearing thing in his head).
KI-4 had an unusual history of re-hospitalization at the psychiatric hospital, and “substance abuse” was always recorded alongside his name.
Abused Drugs Received from the Hospital
Before… I ate B5, my nerves were light. It felt like my nerves were tingling. (KI-4)
The letters B and D are imprinted on the medication pills and come with a number indicating the milligram of the medication amount. KI-4 frequently mentioned B and D pills, whether because the symbol was easy to remember or because he liked the effects. For him, Benzhexol 2mg (B) and Diazepam 10 mg (D) were his favorite drugs and could not be missed among the 19 daily pills he received. “After taking B and D pills, I felt relaxed and light”. In addition to feeling relaxed, “light-headed” also came from these drugs. “I feel light-headed, relieved, and then I have coffee”. These symptoms are similar to the euphoric effects of B or Benzhexol.
Psychological Stress
Always thinking about my daughter and her husband. Sometimes, they did not understand each other. My daughter works hard and is employed at a bank. Unfortunately, there were times when her husband went out drinking and ended up physically assaulting her. (KI-2)
KI-2 denied substance abuse, although there had been a history of overdrinking tea. However, her tea consumption seemed much lighter than that of other key informants. In this study, the main trigger issue for KI-2 was psychological stress in the family.
Sometimes, he (the son-in-law) argues with my daughter. I do not want it. They argue in front of my grandchild, their child. But. My husband and I were quietly separated, not arguing or letting my child know. I was saddened by his (husband) going with another person. However, now, I feel that he, he is getting what he deserves. I am happy for him. getting what he deserves.
KI-2 had had stable psychotic symptoms for many years without receiving psychotropic medication, although she still regularly took anti-hypertensive medication at a nearby hospital. When she had to separate from her husband and had problems with her daughter’s family, she lived with them. Her insomnia and anxiety increased before she began to have more psychotic symptoms, such as talking to herself. Periodically, she cried and exhibited strange behaviors.
Psychological stress caused by the family was not limited to the KI-2 case. Other key informants, such as KI-3, had also revealed his stress problems. KI-3 shared his inner struggles with stress, revealing how his relatives responded with indifference and lack of support.
They (KI-3’s relatives) said, ‘It is his problem, why should we care?’ as if I was not a relative or their grandchild. Moreover, my older sister said, ‘It is his problem. Why should I care? He made his own problems.’ As if I had no identity at all in my family.
This lack of understanding and support caused stress problems within KI-3’s family and contributed to stress problems from living in his community. This is a problematic issue for patients with schizophrenia.
I have lost my patience because I have been studying all my life to have a profession. Even before becoming a mechanic, I was already an expert in that field. However, nobody here supports or trusts me, which is the problem. People see me as someone else, as a drug addict, just because of the term WY (meth), even though anyone can buy it elsewhere. I am interested in that drug. It is illegal, right. It is true… illegal. (KI-3)
Stress from various problems is often associated with substance abuse to escape difficulties. For instance, consider the case of KI-3, who sought happiness and fulfillment. KI-3 had lost patience with many things, such as missed job opportunities or lack of trust from those around him.
Medication Use and Treatment Issues
Misunderstanding
Because I wanted to see if the symptoms were still present or had disappeared, sir. Yes, it is a psychosis. I tried stopping the medication for a month or two to see if the symptoms disappeared. Suddenly, I started hearing voices in my head again (laughs). (KI-1)
Many patients with schizophrenia experience the belief that they are cured, only to later relapse. Both KI-1 and KI-2 had stopped taking medication in the past due to this belief. KI-2 stopped taking medication without consulting her psychiatrist because she believed she was cured. Similarly, KI-1 expressed an intention to experiment with stopping medication independently. However, after only a month of not taking medication, KI-1 experienced a return of familiar psychotic symptoms.
Unknown Illness
I do not know what it was either. When I was sick, I behaved in a way that I cannot remember. Then my daughter sent me to the hospital. (KI-2)
Apart from accepting or denying illness, some patients still do not know what disease they have but can still describe their abnormal symptoms. KI-2 exhibited psychiatric symptoms and sometimes could not remember her previous unusual behavior. However, she could learn about her condition from the narratives of those around her, such as erratic behavior, screaming, throwing things, and playing in the water closet. KI-3 also did not know about his mental illness but had experienced symptoms such as ringing in the ears and visual hallucinations. He could describe what had been happening to him. However, when asked about his disease, he answered, “Not known yet”, and “The disease has not been diagnosed”. Indicating that he still did not have clear information about his condition despite receiving treatment for many years.
Treatment of Mental Illness
I do not know either. (KI-4)
This is the answer to an essential question about treatment or medication. KI-4’s answer did not show much motivation to take the medication. In addition, he could not clearly answer the names of each pill or the number of pills that needed to be taken and might have to ask the caregiver or doctor: “You have to ask, ask. Ask the doctor. There are many pills. Have to sort them before so I can tell”. Even though he did not know the reason for taking each medication, because there were 19 pills in one day, divided into five types. At least reading the medication label made him more familiar with his medication than the appearance or shape of the medication he had seen.
It has a B2 (a symbol on the pill) B2, D10, D10, D10. Two of them. I do not know what they are for. It is written on the label to take before bed, after meals. Wait a minute. Before bed like this. Then, how many pills to take.
Narratives like this did not just happen to KI-4 but were also found in other key informants.
Despite their non-adherence history, the key informants could understand medication’s benefits and importance. For instance, KI-2 wanted to take medication more consistently, stating, “I want to take it on time. It has to be continuous. I am afraid of being unable to sleep, waking up, thinking too much, and being restless. That is what I hear (auditory hallucination)”. The benefits she receives motivate her to take medication on time, not just the medication’s benefits alone. However, she also faced obstacles in taking medication.
I am afraid I will develop kidney disease if I take too much medication. I know that taking too much medication may cause kidney disease… but my genetics may cause cancer or tumors.
Her fear stems from common perceptions based on her experiences or events. “I do not know… maybe I am afraid of being like my relatives, uncles, aunts, and grandmothers”. KI-2 also experienced real consequences of medication use, such as excessive drowsiness, which disrupts her daily life. Negative beliefs or perceptions of medication use are associated with unaddressed medication problems, such as side effects and difficulty with medication intake.
Participation in Their Treatment
My sister gave me almost ten pills, too many to take. As a result, I fell asleep and ended up urinating on my bed three or four times. My sister would arrange the pills, usually holding almost ten or fifteen, and I would take them. I am not sure exactly how many pills I took. (KI-4)
KI-4’s older sister, who also suffers from a mental illness, came to take care of KI-4’s medication after he had frequent exacerbations of mental illness. His sister gathered all the medication for bedtime for convenience. However, this approach did not go as planned, and KI-4 experienced side effects from the overmedication. As a result, KI-4’s trust in his sister as a caregiver was compromised. He expressed his desire to organize his own medication, feeling that his sister was not following the real regimen. This highlights a conflict in needs between the caregiver and the patient with schizophrenia, which extends beyond just the treatment itself.
I do not like injections, sir. I prefer oral medication. Getting injections every month poses many obstacles. I have to take a day off from work every time. It hurts, sir. Taking medicine orally is much easier. Getting injections is sore, sir. (KI-1)
Unaddressed medication issues can impact the perception and health behavior of patients with schizophrenia. These issues that hinder may include difficulties in administering medication, medication injection-induced pain, and side effects. Key informants commonly reported drowsiness as a side effect, and KI-3 also experienced excessive salivation and extrapyramidal symptoms. For example, “It (Salivation) is still the same today. A moment ago, my saliva just keeps flowing out. Oh my. Why is it stretching out?” and “My tongue is stiff, and I cannot speak clearly like before”.
KI-2 complained about the recent period; she felt more forgetful and experienced frequent midday drowsiness. This situation led to irregular medication use and having some medication left. “Sometimes I forgot to take it, and still some was left”. In addition, the medication labels received also had small letters, and some parts were in English, which she needed help understanding, making it difficult to use the medication correctly. Non-adherence to medication may be related to the medication regimen, which can be inconvenient for key informants. For example, KI-1 had to leave for work before 6 a.m. daily, so mornings were often rushed with many daily routines, including taking medication.
It is not difficult, sir. When in a hurry, dressing up, taking a shower, or something, it can be forgotten. What to eat, where to go. Many things, sometimes forgotten.
He explained. Although taking medication was not complicated for KI-1, inconvenience could cause him to miss taking his medication. The problems, as mentioned earlier, are visible enough for us to see. Side effects from medication, difficulty in medication use, inappropriate timing of medication, or medication labels that are difficult to see and read may be obstacles.
Accessing Mental Health Services
It has been a long time since I stopped taking the medicine. It (medication) ran out, and I thought I could go to the hospital near my house… Here (the psychiatric hospital) is too far away for me… Moreover, my daughter had a hard time. I thought I was cured, so I did not come here. (KI-2)
One of the challenges faced by patients with schizophrenia is accessing mental health services continuously. In Thailand, not every province has a psychiatric hospital, making it difficult for patients in those provinces to receive ongoing treatment. KI-2, for example, received continuous treatment for six years at the psychiatric hospital but missed appointments three years ago and did not continue to take medication afterward. She lives in a province without a psychiatric hospital, so traveling to receive treatment at the psychiatric hospital takes a long time. She must travel through two provinces and bring her daughter along. When she began to feel better, she stopped taking her medication. Later, KI-2 faced stress within her family, which led to her mental illness exacerbation. She received treatment at a nearby hospital for a while, but her mental condition did not improve.
KI-3 faced challenges in accessing mental health services. He was unemployed and had no regular income, only receiving occasional assistance from relatives. Despite needing monthly injections of long-acting antipsychotic medication, KI-3 sometimes missed appointments due to the cost of treatment at a nearby hospital. “The fee and the cost of gasoline, please give me some”, he said, laughing.
Problems with Caregivers and Community
No one is my friend, huh. Saying that I hurt my own father, even the whole village. Can I fight against all of them? I just think to kill myself or… maybe I just run away. (KI-3)
The stigma surrounding schizophrenia can lead to psychological stress and suicidal thoughts for patients, including from their own families. KI-3 experienced this firsthand when his neighbors viewed him as crazy and abusive toward his father. Although he admitted to hurting his father, he felt upset because he had to care for him alone.
“I do not see any help from them, just witch hunts and accusations. They say I hurt my father like this… like that. These people (neighbors) are just like that”.
The relationship between the patient and their community is closely related to the relationship within the family, which cannot be ignored.
But they blamed me, saying to my aunt that when they entered my house, they smelled urine and a foul odor and accused me of not caring for my father. They accused me without checking or helping before.
People around patients with schizophrenia often view them negatively, and some do not want them to return home and live with community members. Negative views can even arise within their own families.
Lack of Social Opportunities
He would not let me. He said I was sick, so he would not let me go do it. I am just at home, doing nothing. (KI-4)
In that sentence, “he” refers to the brother-in-law who lives nearby and occasionally helps KI-4. Due to his sickness or mental illness, he could not work in agriculture to support his family like most people, which made him feel inferior. KI-5 was also unemployed and spent his free time with friends. The lack of work and income caused him significant stress. Even hanging out with friends, drinking, and smoking do not alleviate the problem. “Insomnia. Maybe I am stressed. I do not know (laughs). Stressed about work, having no work to do like others…. No work to do”. As a temporary laborer, KI-5 had inconsistent jobs. He cut sugarcane temporarily once a year, which did not provide substantial income. However, he occasionally worked transporting rubber sheets, which provided him with more consistent work. For patients with schizophrenia, opportunities to pursue education and work are limited. Even KI-2, with a good education and steady work experience, had to resign due to mental illness.
I was not feeling well, so I quit. Although I received treatment, it kept recurring, and I had to continue receiving treatment. At the time, I was stressed from work, but the manager encouraged me to keep fighting, stating that others continue to work when they are not feeling well. I tried to work for an additional year, KI-2 said.
Other Opportunities That Come to Replace
I am just staying at home. I am not really watching TV. I walk around the neighborhood to play with my neighbor and hang out at my friend’s house. (KI-5)
The emptiness of being unemployed and staying home all day also led KI-4 to use drugs to fill the void. He stated, “I do not use it (meth) often, just two pills (of meth) when there is nothing to do”. Meanwhile, KI-5 must go to hang out with his friends.
I did not really buy it (alcoholic drinks). They just gave it to me. There were many people there… The other villagers call that ‘the drunkard house.’ We also smoked cigarettes together.
These behaviors reflect issues with psychological stress, self-control, and addiction. Society should consider providing opportunities for them to prevent further issues.
These things (meth and other illegal drugs) can be purchased, but not easily. It depends on how familiar you are with the process. If you are unfamiliar with it, ask someone else to buy it for you. You can make the purchase yourself. (KI-3)
Addictive substances were readily available in the community of key informants. Despite undergoing substance abuse rehabilitation several times at the psychiatric hospital, they relapsed from substances-induced upon returning to the community. According to the KI-4 case, although he was aware of the negative impact of consuming excessive coffee and addictive substances on his health, he still frequently indulged in “drinking coffee and smoking tobacco, buying a sachet of tobacco for 15 baht. 15 baht, I can buy it at any store, any store has it”. Although the community was aware that patients with schizophrenia should avoid addictive substances, KI-4 might still try to purchase them.
I can buy (white liquor) at stores near my house. Sometimes, they do not want to sell it to me because they know me. They refuse, but I ask anyway… and they do not refuse to sell it to me.
KI-5 often acquired addictive substances from his friends and his co-workers. “On Sundays, they treat us to some liquor in a rubber plantation. The owner treats us”. The issue of substance abuse, both illegal and legal, reflects societal problems at the national level.
Discussion
This study classifies medication non-adherence behavior of patients with schizophrenia as intentional or unintentional. According to the Health Belief Model,7 medication non-adherence stems from an insufficient understanding of mental illness and its treatment. Key informants did not fully comprehend their treatment plan and could not provide accurate information or instructions for their medication. They only recognized the external characteristics of the medication and how to take it based on the labeling. Key informants who intentionally decided to stop taking medication did not consult a psychiatrist, believing they were cured. Key informants might recognize their mental illness and its consequences. The impact of medication non-adherence was not only on themselves but also on their families, who must care for them during exacerbations of the illness. Furthermore, medication non-adherence behavior might also lead to problems within the community. The patient’s perceptions of mental illness and its treatment may not fully explain medication non-adherence behavior in patients with schizophrenia. All three groups in this study, those who accept their illness, those who deny it, and those who do not know their illness, still experience problems with medication non-adherence.
The medication use behavior of patients with schizophrenia is continuously changing due to various factors that may lead to non-adherence. Therefore, caregivers play an essential role in monitoring the medication adherence behavior of these patients. The understanding of patients with schizophrenia changes as the disease progresses and new insights are gained. Mental health education is crucial for patients and caregivers to have accurate perceptions and promote continuity and consistency, particularly in medication treatment. This study revealed that key informants had relatively low perceptions and did not fully understand the benefits of medication. Negative views or attitudes towards medication could also be observed. Hence, the mental health service system should promote positive medication perceptions and appropriate treatment approaches, reduce negative attitudes towards medication, and build confidence in medication use for patients with schizophrenia.
Exacerbation of mental illness can lead to unintentional non-adherence to medication. Patients with schizophrenia experience altered perception and thinking when psychological symptoms worsen. Frequent exacerbations accelerate this process, increasing the likelihood of non-adherence. As Sheffield et al demonstrated, the progression of mental illness can cause functional and cognitive impairment. These impairments occur during exacerbation and the disease’s progression, with varying severity levels. In contrast, the side effects of antipsychotics have little impact on these impairments, either positively or negatively.8 Medication adherence is essential for effective treatment and to delay the onset of illness. Therefore, preventing the exacerbation of mental illness is crucial.
The mental health conditions of patients with schizophrenia are not solely affected by medication non-adherence or disease progression but also by other hindering factors. Studies have shown that patients with schizophrenia are at a higher risk of psychological exacerbation when other factors are present, such as untreated mental illness duration, substance use, poor relationships with doctors or family, lower pre-illness ability, and lack of self-awareness about their illness. Substance use is also associated with more severe symptoms of disease and increased impairment.9 These triggering factors were reflected in the key informants of this study.
All key informants in this study had a history of using at least one addictive substance, such as methamphetamine, cigarettes, alcohol, kratom, marijuana, caffeinated beverages, and psychotropic medication. According to the meta-analysis by Hunt et al, comorbid substance use disorder in patients with schizophrenia was prevalent in 41.7% of cases, with significantly more men than women affected. Patients used various substances, including illegal drugs, marijuana, alcohol, and psychoactive substances, with a trend of increasing use of illegal drugs.10 Substance use exacerbates mental illness conditions in general.9 Khokhar et al hypothesize that the abnormality of the brain reward circuitry associated with schizophrenia increases the risk of addiction.11 Discontinuing substance use in patients with schizophrenia is more challenging than in the general population.10–12 Trihexyphenidyl and Diazepam were psychotropic medications that key informants might become addicted to or misuse. Additionally, these medications prescribed by hospitals have been known to lead to addiction in patients with schizophrenia.13–15 Stressors or events that lead to stress in the lives of patients with schizophrenia are related to mental illness exacerbation.16–18 Key informants experienced stress from various problems, including violence in their family, missed job opportunities, or a lack of trust from those around them. The psychological stress is also related to substance abuse, not only as a means of escaping difficulties but also due to the neurobiological mechanisms of the nervous system.19,20
The lack of continuous monitoring of patients’ medication adherence is a significant problem that can lead to worsening mental symptoms. Key informants had reported various medication-use problems that had gone unresolved, including side effects, difficulties using the medication, incompatible medications, negative attitudes toward treatment, and substance abuse. Patients’ perceptions of illness and treatment significantly impact medication adherence behavior, with some patients discontinuing treatment due to the belief that it is inappropriate. These problems are also associated with mental health care providers and patients’ families or caregivers. Therefore, patients with schizophrenia must participate in their treatment to identify and resolve medication use issues. To provide patient-centered care, mental health services must ensure accurate and appropriate information and receive feedback from patients and caregivers. Patients with schizophrenia should have a platform to express their understanding and problems with treatment to increase their participation. Medication non-adherence by key informants was often due to limited access to mental health services caused by the cost and travel time burden. In Thailand, many patients with schizophrenia live far away from psychiatric hospitals. As a result, some patients miss treatment, while others choose not to continue treatment even after their symptoms have stabilized. The cost of travel and hospital services further exacerbates the challenges patients face, making it difficult for them to access appropriate care.
Social opportunities in Thailand significantly impact the lives of patients with schizophrenia. Due to negative attitudes from people around them, including family members, these patients have fewer chances to work and generate income, leading to psychological stress. Emotional vulnerability resulting from illness and exposure to psychological stress can trigger exacerbations. Additionally, the inability to manage stress can lead to substance abuse. Substance addiction was also common for key informants who struggled with medication adherence. A lack of meaningful activities can lead to other harmful behaviors that impact their mental health. Mental illness affects work and cognitive abilities, and society’s limitations undermine their proper skills and abilities. Despite the decline in work skills, society and family should provide support and opportunities for these patients to prevent further psychological stress and substance abuse.
Conclusion
The study revealed that medication adherence behavior is a significant factor in patients with schizophrenia. Intentional and unintentional non-adherence are two distinct types of behavior. Patients’ perceptions of their illness and treatment also significantly influence medication adherence. Substance use is associated with more severe symptoms and increased disease impairment. Discontinuing substance use is more challenging for patients with schizophrenia than the general population. Psychological stress can trigger exacerbations of mental illness and complicate treatment. Moreover, limited access to mental health services in Thailand due to cost and travel time burdens can lead to medication non-adherence. Therefore, mental health services in Thailand should provide strategies to improve medication adherence and offer social opportunities and support to prevent further psychological stress and harmful behaviors.
Acknowledgments
We express gratitude to the key informants who have shared their stories and experiences with us. This study was supported by the Research Grants for Master's Thesis and Independent Study and Doctoral Dissertation program provided by the Faculty of Pharmaceutical Sciences at Khon Kaen University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29,823 patients with schizophrenia. JAMA Psychiatry. 2017;74(7):686–693. doi:10.1001/jamapsychiatry.2017.1322
2. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
3. Higashi K, Medic G, Littlewood KJ, Diez T, Granström O, De Hert M. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther Adv Psychopharmacol. 2013;3(4):200–218. doi:10.1177/2045125312474019
4. Dilokthornsakul P, Thoopputra T, Patanaprateep O, Kongsakon R, Chaiyakunapruk N. Effects of medication adherence on hospitalizations and healthcare costs in patients with schizophrenia in Thailand. SAGE Open Med. 2016;4:2050312116637026. doi:10.1177/2050312116637026
5. Javadi M, Zarea K. Understanding thematic analysis and its pitfall. Demo. 2016;1(1):33–39.
6. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):160940691773384. doi:10.1177/1609406917733847
7. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
8. Sheffield JM, Karcher NR, Barch DM. Cognitive deficits in psychotic disorders: a lifespan perspective. Neuropsychol Rev. 2018;28(4):509–533. doi:10.1007/s11065-018-9388-2
9. Porcelli S, Bianchini O, De Girolamo G, Aguglia E, Crea L, Serretti A. Clinical factors related to schizophrenia relapse. Int J Psychiatry Clin Pract. 2016;20(2):54–69. doi:10.3109/13651501.2016.1149195
10. Hunt GE, Large MM, Cleary M, Lai HMX, Saunders JB. Prevalence of comorbid substance use in schizophrenia spectrum disorders in community and clinical settings, 1990–2017: systematic review and meta-analysis. Drug Alcohol Depend. 2018;191:234–258. doi:10.1016/j.drugalcdep.2018.07.011
11. Khokhar JY, Dwiel LL, Henricks AM, Doucette WT, Green AI. The link between schizophrenia and substance use disorder: a unifying hypothesis. Schizophr Res. 2018;194:78–85. doi:10.1016/j.schres.2017.04.016
12. Carey CE, Agrawal A, Bucholz KK, et al. Associations between polygenic risk for psychiatric disorders and substance involvement. Front Genet. 2016;7:149. doi:10.3389/fgene.2016.00149
13. Chiappini S, Mosca A, Miuli A, et al. Misuse of anticholinergic medications: a systematic review. Biomedicines. 2022;10(2):355. doi:10.3390/biomedicines10020355
14. de la Iglesia-Larrad JI, Barral C, Casado-Espada NM, et al. Benzodiazepine abuse, misuse, dependence, and withdrawal among schizophrenic patients: a review of the literature. Psychiatry Res. 2020;284:112660. doi:10.1016/j.psychres.2019.112660
15. Mahal P, Nishanth KN, Mahapatra A, Sarkar S, Balhara YPS. Trihexyphenidyl misuse in delusional disorder. J Neurosci Rural Pract. 2018;9(3):428–430. doi:10.4103/jnrp.jnrp_569_17
16. Kazadi NJB, Moosa MYH, Jeenah FY. Factors associated with relapse in schizophrenia. South Afr J Psychiatry. 2008;14(2):7. doi:10.4102/sajpsychiatry.v14i2.158
17. Moges S, Belete T, Mekonen T, Menberu M. Lifetime relapse and its associated factors among people with schizophrenia spectrum disorders who are on follow up at comprehensive specialized hospitals in Amhara region, Ethiopia: a cross-sectional study. Int J Ment Health Syst. 2021;15:42. doi:10.1186/s13033-021-00464-0
18. Olivares JM, Sermon J, Hemels M, Schreiner A. Definitions and drivers of relapse in patients with schizophrenia: a systematic literature review. Ann Gen Psychiatry. 2013;12:32. doi:10.1186/1744-859X-12-32
19. Perreau-Lenz S, Spanagel R. Clock genes × stress × reward interactions in alcohol and substance use disorders. Alcohol Fayettev N. 2015;49(4):351–357. doi:10.1016/j.alcohol.2015.04.003
20. Sahani V, Hurd YL, Bachi K. Neural underpinnings of social stress in substance use disorders. Curr Top Behav Neurosci. 2022;54:483–515.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Changes in Clinical Management of Patients with Schizophrenia Treated with Long-Acting Injectable Antipsychotics (LAIs), Including Telepsychiatry Use, During the COVID-19 Pandemic
Haider B, O'Sullivan AK, Bessonova L, Keane E, Achtyes E, Harvey PD, Kane JM, Saklad SR, Trotter JP, Claxton A, Polak T, McGrory J, Noori W, Sikora Kessler A, Yarlas A, Velligan D
Neuropsychiatric Disease and Treatment 2023, 19:623-634
Published Date: 17 March 2023
Real-World Effectiveness, Economic, and Humanistic Outcomes of Selected Oral Antipsychotics in Patients with Schizophrenia: A Systematic Review Evaluating Global Evidence
Adhikari K, Kamal KM, Jeun KJ, Nolfi DA, Ashraf MN, Zacker C
ClinicoEconomics and Outcomes Research 2024, 16:621-645
Published Date: 6 September 2024
A Co-Design Study Developing an Early Prototype Intervention to Support Oral Anticancer Medication Use in Breast Cancer
Seo Y, Hudmon KS, Weddle KJ, Yih Y, Miller KD, Abebe E
Patient Preference and Adherence 2026, 20:553015
Published Date: 17 February 2026