")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Mediating Role of Emotion Management, Self-Efficacy and Emotional Intelligence in Clinical Nurses Related to Negative Psychology and Burnout
Authors Yu C, Liu Z, Zhao M, Liu Y, Zhang Y, Lin A, Sang X, Wan H
Received 18 April 2023
Accepted for publication 10 August 2023
Published 24 August 2023 Volume 2023:16 Pages 3333—3345
DOI https://doi.org/10.2147/PRBM.S417729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
ChuoChuo Yu,1,* ZhiQun Liu,2,* Mingyang Zhao,3 Yanhui Liu,2 Yuxin Zhang,1 Ai Lin,2 Xiaohan Sang,1 Huan Wan2
1Department of Nursing, Hunan Normal University School of Medicine, Changsha, 410013, People’s Republic of China; 2Department of Nursing, The First Hospital Affiliated with Hunan Normal University (Hunan Provincial People`s Hospital), Changsha, 410005, People’s Republic of China; 3Operating Room, Guangzhou Dongsheng Hospital, Guangzhou, 510000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huan Wan, Department of Nursing, The First Hospital Affiliated with Hunan Normal University (Hunan Provincial People`s Hospital), No. 61 Jiefang West Road, Changsha City, Hunan Province, 410005, People’s Republic of China, Tel +86 137 8725 7287, Fax +86 731 8227 8012, Email [email protected]
Objective: To explore the influence of negative psychology and burnout in clinical nurses, and to analyse the mediating role between self-efficacy and emotional intelligence in emotion management.
Methods: From January 2022 to December 2022, 12,704 clinical nurses from 32 general hospitals in Hunan Province were selected as research participants by convenience sampling. Negative psychology, emotion management, self-efficacy, emotional intelligence and burnout in clinical nurses were measured, and structural equation models were constructed to explore their impact on burnout in clinical nurses.
Results: Clinical nurses’ negative psychology had a positive effect on burnout (β=0.60, 95% CI: 0.63– 0.66), emotional intelligence (β=˗0.08, 95% CI: ˗0.10, ˗0.06) and the self-efficacy of emotion management (β=− 0.60, 95% CI: ˗0.05, ˗0.03) on burnout. Moreover, emotional intelligence and emotion management self-efficacy played a mediating role between negative psychology and burnout in nurses.
Conclusion: Clinical nurses’ negative psychology had a positive impact on burnout, and emotional intelligence and the self-efficacy of emotion management could alleviate the influence of negative psychology on burnout among nurses. Nurses’ emotional intelligence and emotion management self-efficacy can be improved through practical training to help them cope with emotionally loaded situations and reduce stress responses.
Keywords: clinical nurse, job burnout, negative psychology, emotional management self-efficacy, emotional intelligence
Introduction
In the field of healthcare, caregivers are among the key personnel who play an important role. However, nursing often faces significant occupational pressures, eg time pressure, as well as reduced social support, high workload levels, treatment uncertainty and the risk of negative emotional reactions from exposure to distressed and dying patients.1,2 Since the COVID-19 pandemic, a large number of nurses have experienced considerable levels of anxiety and depression, even though they have gained a sufficient level of self-efficacy.3 The pandemic has also had a stressful impact on the psychological states of nursing students, causing severe distress and exhaustion.4,5 These stressors can lead nurses to experience symptoms of burnout, which, in turn, affect the quality of the care they deliver and patient safety and prognosis.6 Burnout is a state of physical, emotional and mental exhaustion and fatigue, typically caused by work-related demands in a person’s life.7 Notably, as of 1 January 2022, burnout has become the 11th Revision (ICD-11) statistical classification of medically diagnosed diseases and related health problems,8 further highlighting the serious impact of burnout on the health of caregivers. It is particularly important to explore how burnout develops, given its devastating effects on nurses and patients, as well as the high risk of nurses experiencing burnout during their careers due to ineffective management causing chronic work stress that can lead to serious negative psychological problems among caregivers.
In recent years, a growing body of research has focused on burnout and related factors among nurses. A study of 316 nurses caring for COVID-19 patients in Hunan Province revealed that stress was high among nurses and the environment was an important source of this stress.9 Studies have shown significant correlations between negative psychological states, emotional intelligence and emotion management self-efficacy and burnout among caregivers.10,11 The impact of negativity on burnout and intention of leaving the profession may be mediated by emotional intelligence and emotion management self-efficacy. However, few existing studies have examined the direct and indirect effects of these variables. This study aims to explore the effects of nurses’ negative psychology, emotional intelligence and self-efficacy in emotion management on burnout. Additionally, the research also considers the mediating role of emotional intelligence and self-efficacy on nurses’ negative psychology and burnout to provide a reference and basis for nursing managers to formulate effective measures to reduce burnout among hospital nurses, improve the quality of clinical nursing and avoid medical disputes and medical accidents.
Research Participants and Methods
Participants
From January 2022 to December 2022, a convenient sampling method was used to select 12,704 clinical nurses who were active in 32 general hospitals in Hunan Province, China, who volunteered to participate in this study. Inclusion criteria: clinical in-service registered nurse; voluntary participation in this survey. Exclusion criteria: trainee nurses, advanced nurses, nurses who had temporarily left their jobs, and those who anticipated major family changes in the near future. This study passed the review of the Medical Ethics Committee of Hunan Provincial People’s Hospital (ethics approval number: LL-20211221-4) and obtained the informed consent of the research participants before starting the investigation.
Research Tools
General Information Questionnaire
The research team reviewed the literature and designed the information questionnaire by itself, which included aspects such as gender, age, educational background, current department, nursing age and professional title.
Negative Mood Assessment Using the Depression, Anxiety and Stress Self-Rating Scale
The Depression, Anxiety and Stress Self-rating Scale (DASS-21) was compiled by Lovibond et al12 and revised and verified by Chinese researchers13 and includes three dimensions, ie depression (7 items), anxiety (7 items) and stress (7 items) for a total of 21 items, using the Likert 4-level scoring method in which a higher score indicates a higher the level of depression and anxiety. The Cronbach’s α coefficient for the DASS-21 scale in this study was 0.93 (see Table 1 for details).
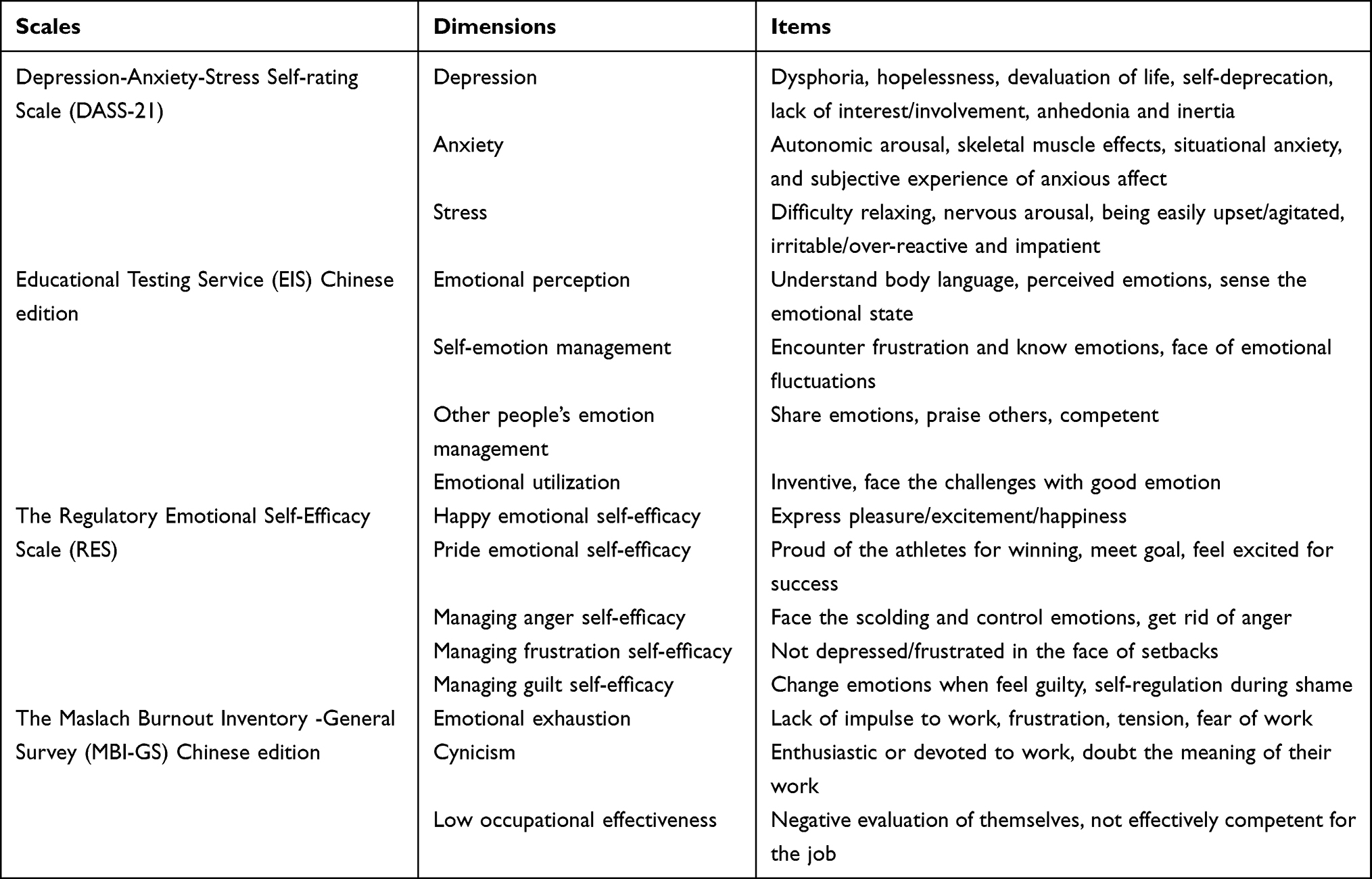 |
Table 1 Dimensions and Items of the Scales |
Educational Testing Service Chinese Edition
The Chinese version of the Educational Testing Service (ETS), as compiled and presented by Schutte et al14 and revised by Wang15 and others, includes four dimensions of emotional perception (12 items), self-emotion management (8 items), other people’s emotion management (6 items) and emotional utilisation (7 items) for a total of 33 items. Using a Likert 5-level scoring method, higher scores indicated higher emotional intelligence. The Cronbach′s α coefficient for the ETS scale in this study was 0.92 (see Table 1 for details).
The Regulatory Emotional Self-Efficacy Scale
The Regulatory Emotional Self-Efficacy Scale (RES) is the latest revision of Caprara16 and the revised Chinese version of Wang et al17 and included happy emotional self-efficacy (3 items), pride emotional self-efficacy (3 items), managing anger self-efficacy (4 items), managing frustration self-efficacy (4 items) and managing guilt self-efficacy (3 items) for a total of 17 items and using a Likert 5-level scoring method, where a higher score indicated the individual’s emotion management self-efficacy was stronger. In this study, the Cronbach′s α coefficient of the RES scale was 0.93 (see Table 1 for details).
The Maslach Burnout Inventory – General Survey (MBI-GS)
The Maslach Burnout Inventory – General Survey (MBI-GS) was developed by Maslach et al18 and has also been translated and verified by Chinese scholars;19 the survey includes emotional exhaustion (5 items) cynicism (4 items) and low occupational effectiveness (6 items) for a total of 15 items, using the Likert 5-level scoring method where the higher the score, the stronger the individual’s burnout. The Cronbach′s α coefficient for the MBI-GS scale in this study was 0.94 (see Table 1 for details).
Methods of Data Collection
Before conducting the formal survey, 31 clinical nurses who met the criteria of this study were selected by purpose sampling for pre-investigation. With the assistance of the nursing department of the hospital, an electronic questionnaire with logic correction and jump functions was distributed via the Questionnaire Star network platform, indicating the purpose of the survey, the completion method, ensuring the principle of confidentiality and setting a limit of one time for each user’s IP address. A total of 12,892 questionnaires were distributed, and 12,704 valid questionnaires were recovered (effective recovery rate, 98.54%).
Methods of Statistical Analysis
The SPSS 26.0 (International Business Machines Corporation, Chicago) and AMOS 24.0 (International Business Machines Corporation, Chicago) software programs were used for data analysis. Measurement data are expressed as mean ± standard deviation (x±s), and counting data are expressed as frequency and percentage (%). Kaiser–Meyer–Olkin (KMO) values and a Bartlett spherical test were used to test whether items were suitable for factor analysis. A KMO value >0.50 indicated good relevance and suitability for factor analysis. The Bartlett spherical test required a significant χ2 value (p<0.05), indicating a suitable factor analysis. The correlation analysis of negative emotions, emotional intelligence, emotion management, self-efficacy and burnout was performed using Pearson’s coefficient (r). The AMOS 23.0 software was used to establish a structural equation model to fit the relationship between negative emotions, emotional intelligence, emotion management, self-efficacy and burnout among nurses. A statistically significant difference was indicated by p<0.05.
Results
General Information for Clinical Nurses
A total of 12,704 clinical nurses were included in this study, 12,456 (98.05%) of whom were women. The age range of the included nurses ranged between 24–35 years. The education level among the participants was mainly college or undergraduate (96.99%). The average annual income was 3–140,000 RMB (80.38%). The departments were mainly internal medicine and surgery (55.22%); 1010 (7.95%) of the nurses had less than 2 years’ experience, 2707 (21.31%) had 2–4 years, 4521 (35.59%) had 5–10 years, 3272 (25.76%) had 11–20 years and 1194 (9.04%) had more than 20 years’ experience. The composition of professional titles included 3293 nurses (25.92%), 4923 Junior nurse (38.75%), 3895 charge nurses (30.66%) and 593 (4.67%) deputy chief nurses and higher. More than 32% of the participants had little knowledge of emotion management, more than 92% said they were interested in emotion management and only 14% were trained in emotion management (see Table 2 for details).
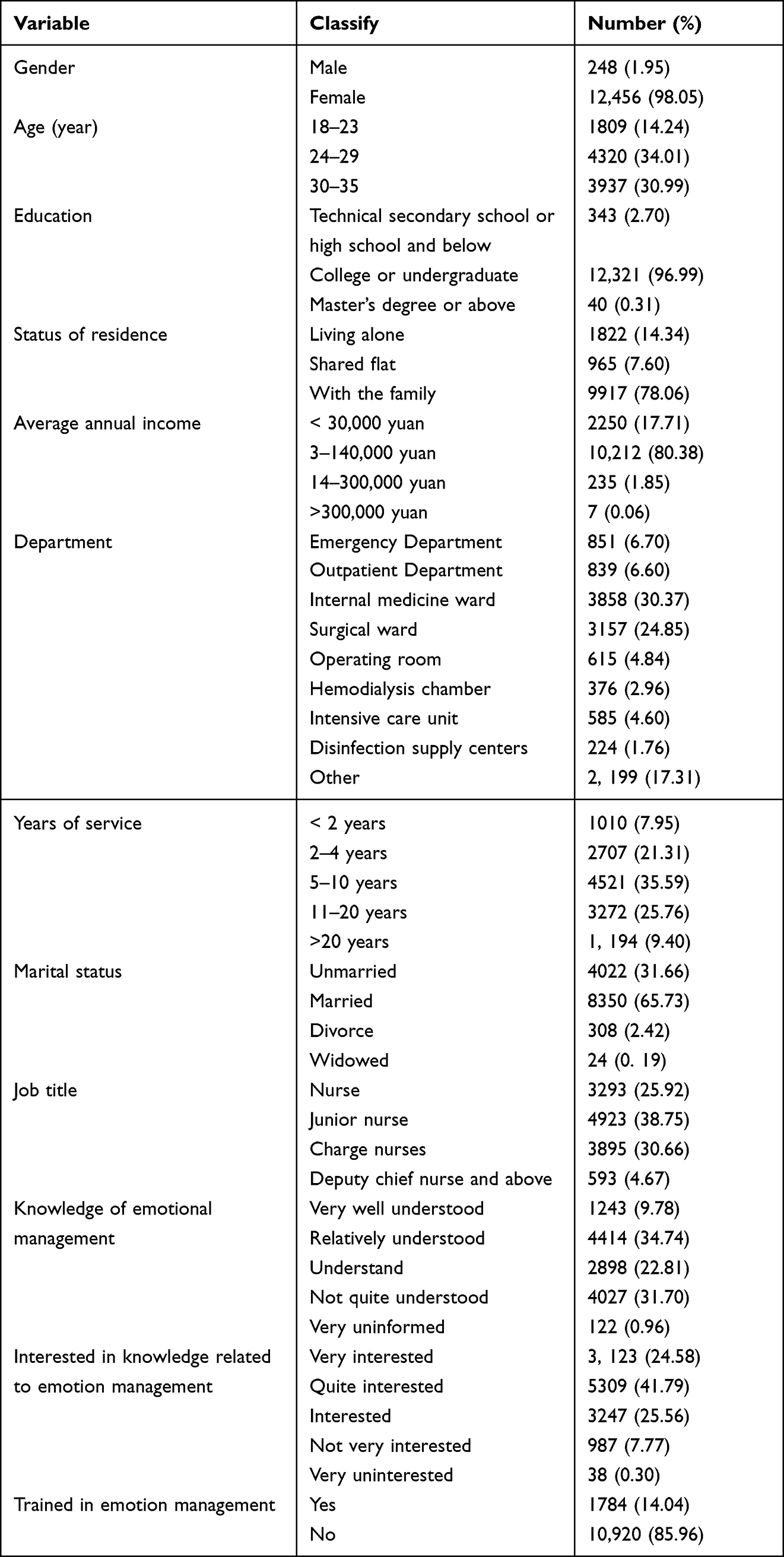 |
Table 2 Basic Characteristics of the Research Object |
Evaluation of Negative Emotions, Emotional Intelligence, Emotion Management, Self-Efficacy and Burnout Among Nurses, and the Reliability and Validity of the Results
This study found that, concerning the negative psychological states-of-mind among clinical nursing staff, nurses scored (4.04±1.20) for anxiety, (3.88±1.37) for depression and (5.23±1.47) for stress. In the self-efficacy of emotion management, the score for happiness-based emotional self-efficacy was (9.26±2.91), the score for pride-based emotional self-efficacy was (10.74±3.03), the self-efficacy score for managing anger was (10.22±3.65), the self-efficacy score for managing frustration was (10.72±3.72) and the self-efficacy score for managing guilt was (7.89±2.85). For emotional intelligence, the score for happiness-based emotional self-efficacy was (9.26±2.91), pride-based emotional self-efficacy was (10.74±3.03), the self-efficacy score for managing anger was (10.22±3.65), the self-efficacy score for managing frustration was (10.72±3.72), and the self-efficacy score for guilt management was (7.89±2.85). Burnout scored (15.87±6.02), cynicism (10.80±5.09) and low occupational effectiveness (25.53±8.65); see Table 3 for details.
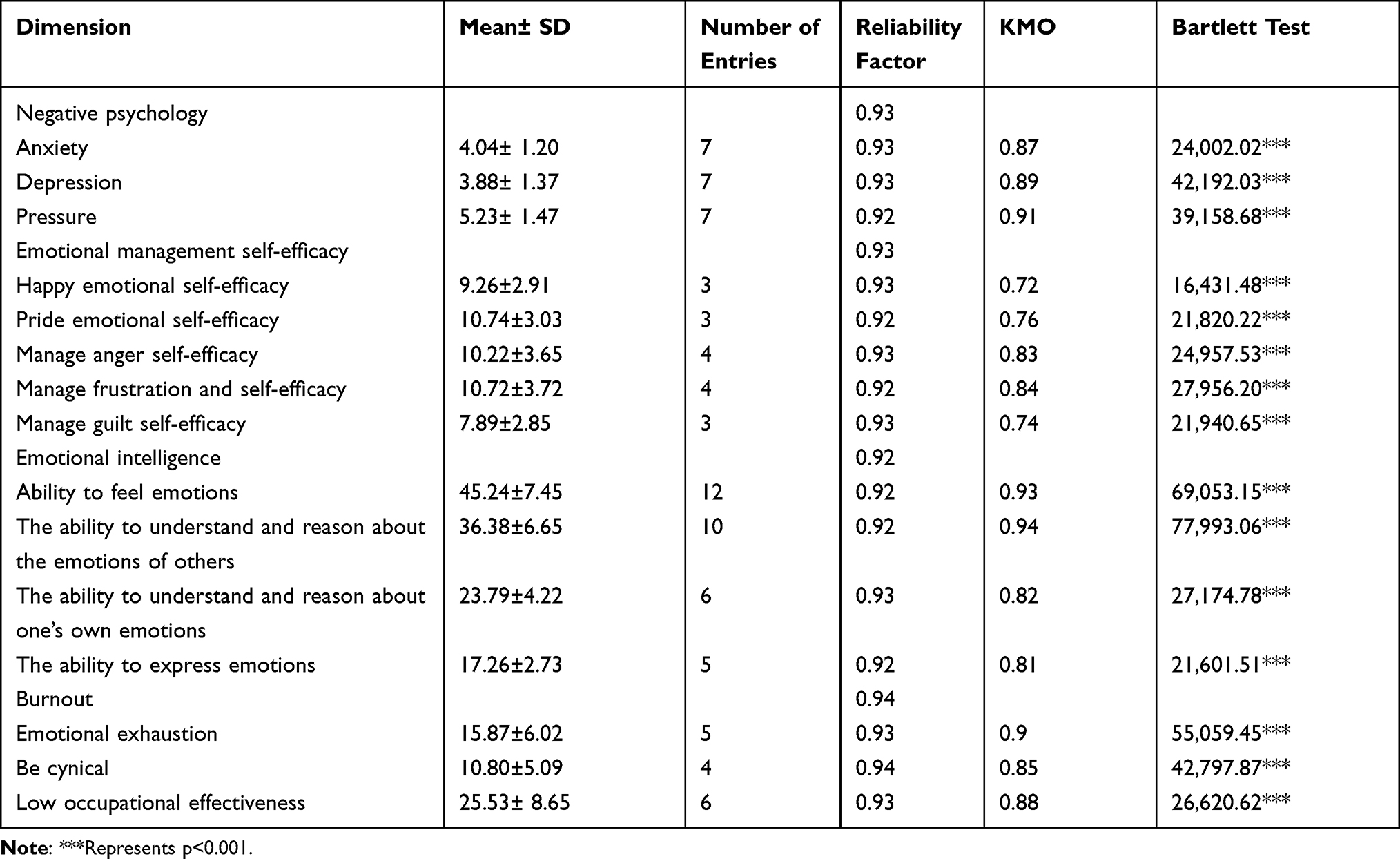 |
Table 3 Description of Each Dimension of the Scale and Reliability Analysis |
Descriptive Analysis of Each Dimension of Burnout
Descriptive analysis of various dimensions of burnout among nurses showed differences within age groups, education levels, average annual income, departments, working years, marital status, titles, emotion management training and understanding of emotion management and emotion management-related knowledge, and the differences were statistically significant (p<0.001). There were differences concerning cynicism among different age groups, education levels, departments, working years, marital status, titles, training in emotion management and understanding of emotion management and knowledge related to emotion management, and the differences were statistically significant (p<0.001). Different ages, average annual income, departments, working years, marital status, professional titles, training in emotion management, understanding of emotion management and interest in knowledge related to emotion management were statistically significant among the nurse with low occupational efficiency (p<0.001); see Table 4 for details.
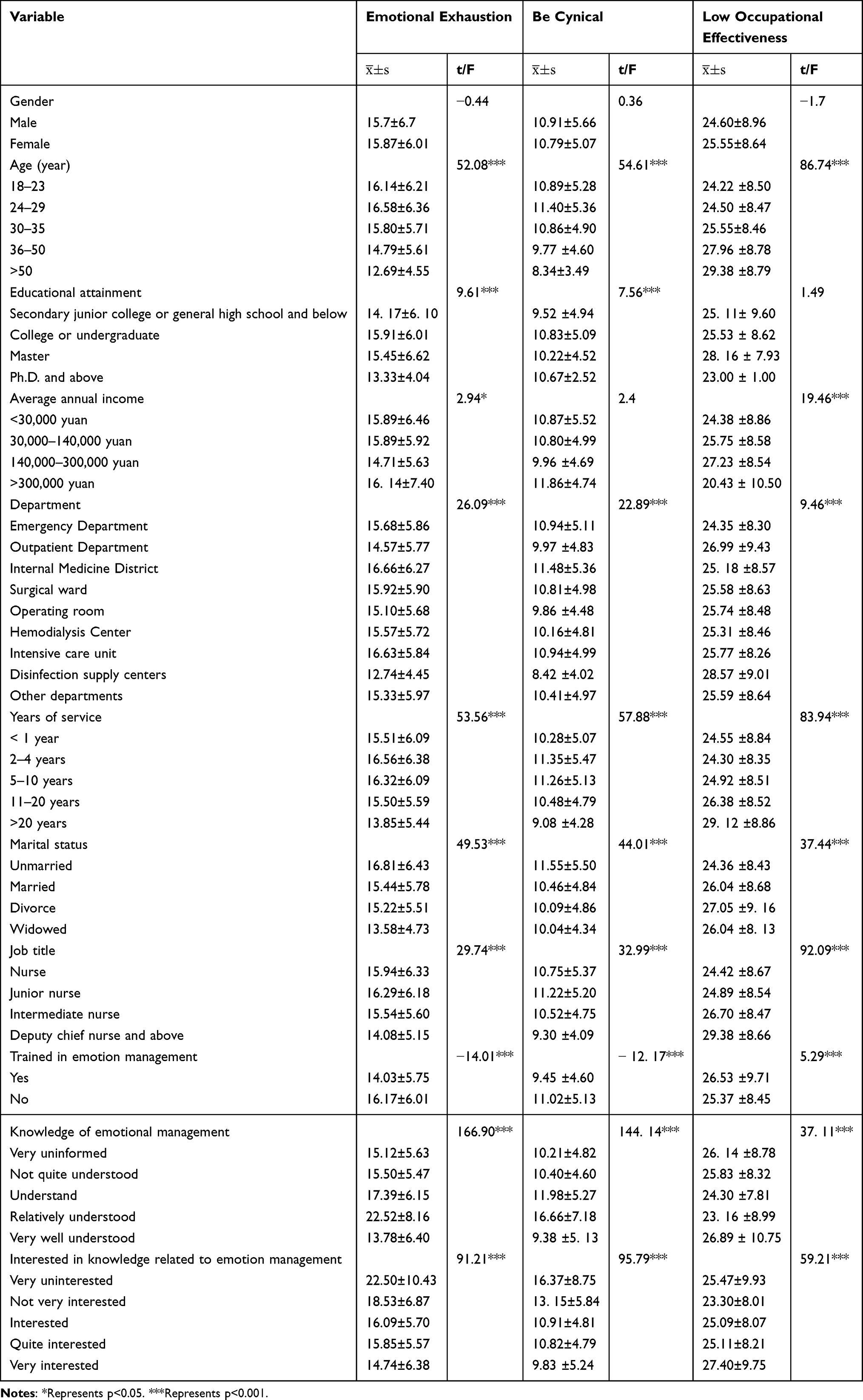 |
Table 4 Descriptive Analysis of Burnout by Dimension |
Correlation Analysis for Each Dimension of the Scale and Burnout
Correlation analysis involving the negative psychology, emotion management self-efficacy energy, emotional intelligence and burnout scales showed that negative psychological scale dimensions positively correlated with dimensions of the burnout scale (r>0, p<0.001), while the dimensions of the emotion management self-efficacy energy scale and emotional intelligence scale were negatively correlated with the dimensions of the burnout scale (r<0, p<0.001); see Table 5 for details.
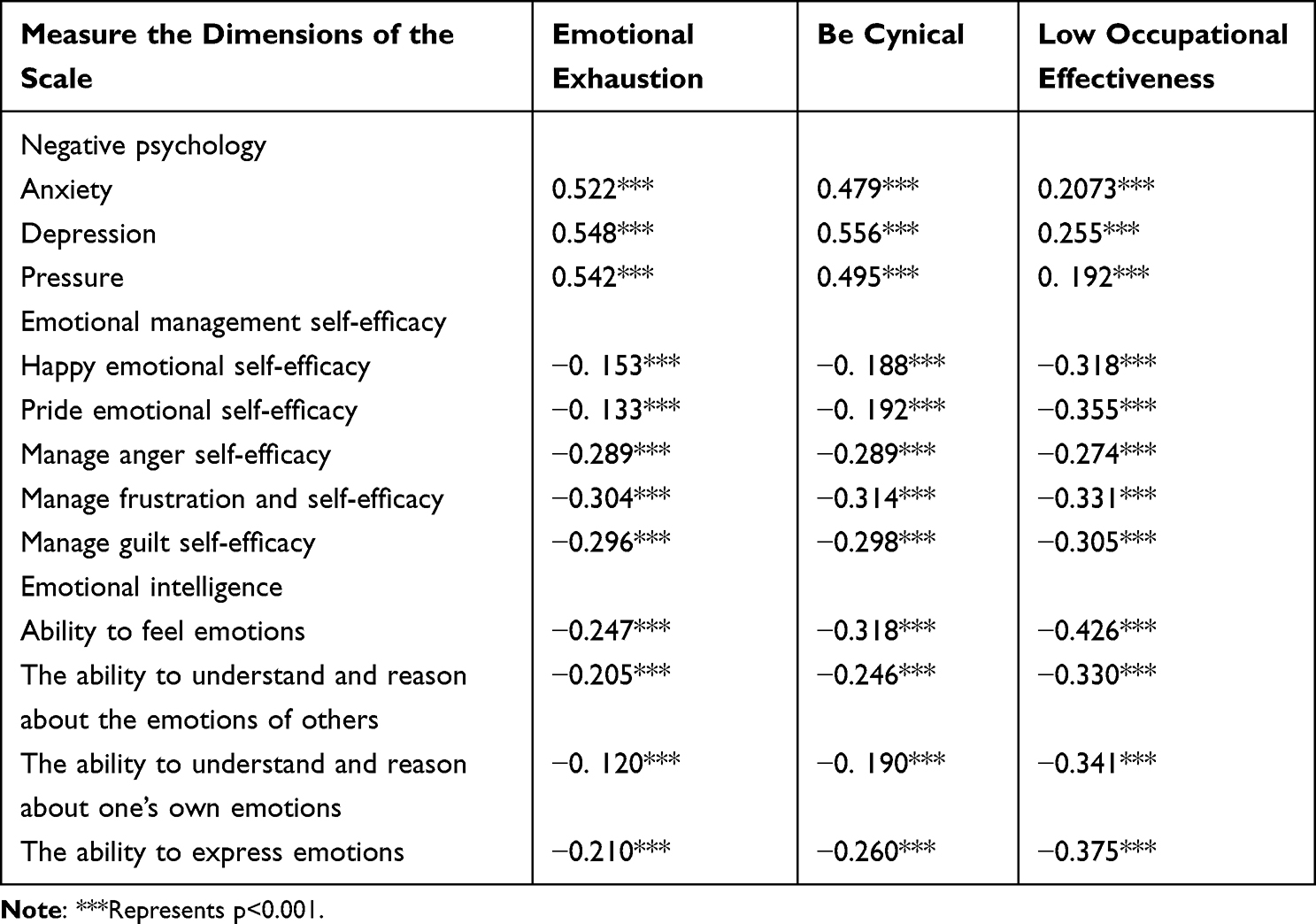 |
Table 5 Correlation Analysis of Each Dimension of the Scale and Burnout |
Model Analysis of the Structural Equations Influencing Factors of Burnout
Structural equation models of the negative psychology, emotion management self-efficacy energy, emotional intelligence and burnout scales were constructed, and the individual characteristic factors with the different dimensions of burnout in the descriptive analysis were included as control variables. Model fitting index: χ²/df was 1.57, the goodness-of-fit index (GFI) was 0.95, the adjusted GFI (AGFI) was 0.93, the scale non-normed FI (NFI) was 0.94, the comparative FI (CFI) was 0.99, root mean square error of approximation (RMSEA) was 0.027 and the standardised root mean square residual (SRMR) was 0.038, indicating a good model fit (see Table 6 for details).
 |
Table 6 Model Fit Tests |
The results of the structural equation model showed that self-efficacy of emotion management had a negative effect on burnout (β=˗0.058, p<0.001), emotional intelligence had a negative effect on burnout (β=˗0.046, p<0.001) and negative psychology had a positive effect on burnout (β=0.599, p <0.001). See Table 7 and Figure 1 for details.
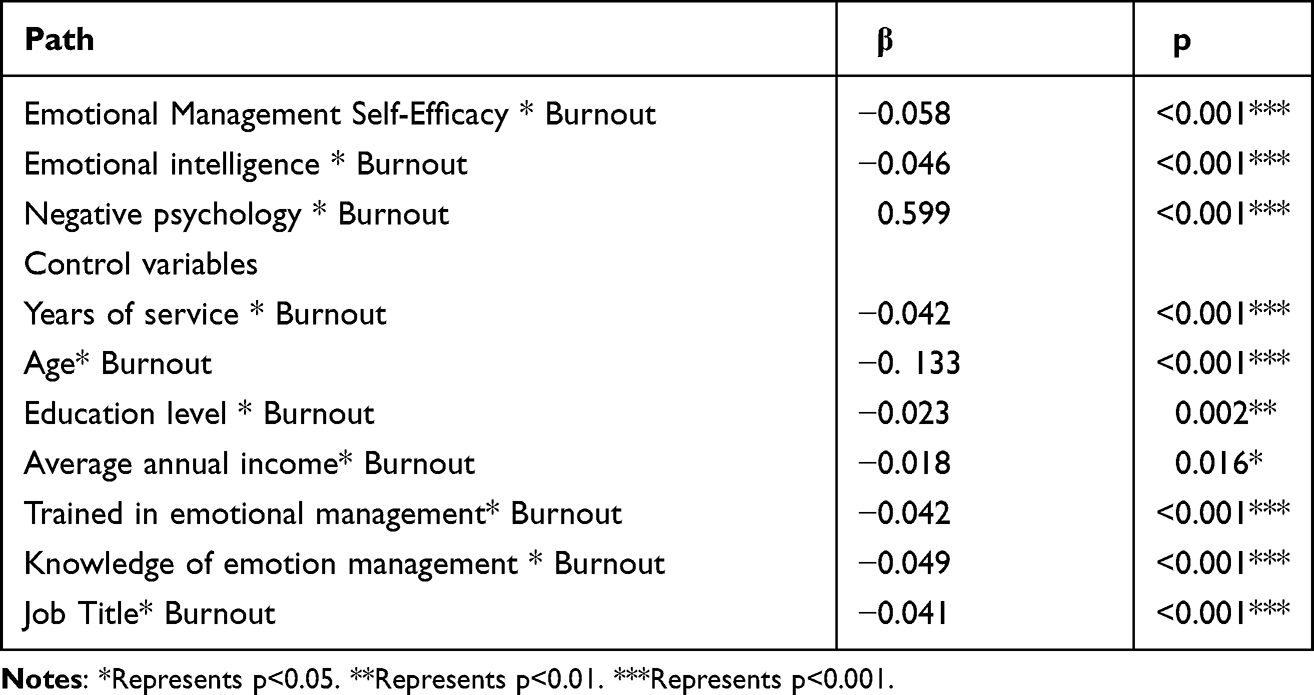 |
Table 7 Path Coefficients for Structural Equation Models |
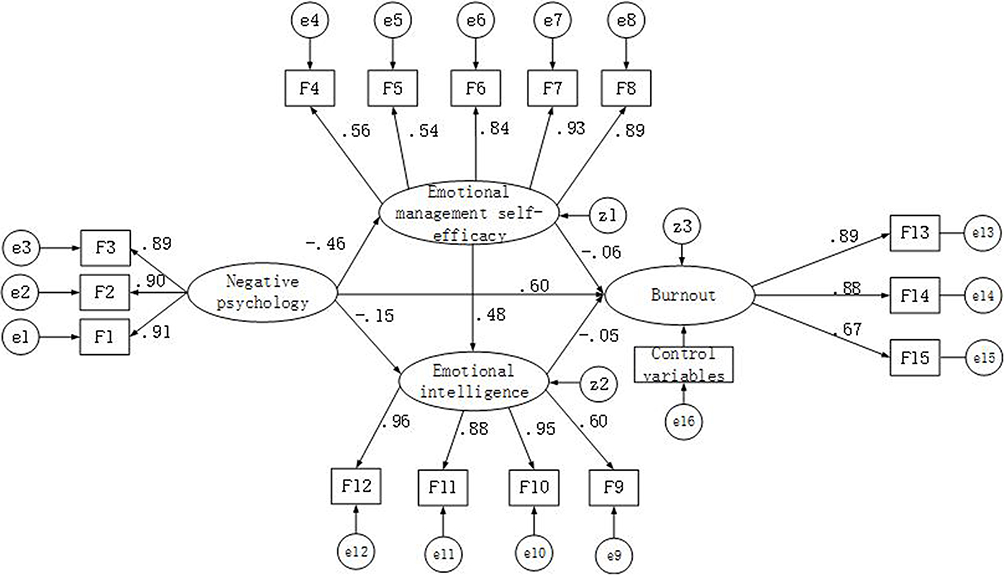 |
Figure 1 Structural equation model of the influencing factors of nurse burnout. Notes: The control variables include age, education level, average annual income, department, working years, marital status, title, trained in emotional management, knowledge of emotional management, and interest in knowledge related to emotional management. |
Using the Bootstrap method for mediation effect testing, the results showed that negative psychology could have an indirect effect on burnout through three paths (β=0.04, p=0.015), ie: (1) Negative psychology * burnout, (2) Emotional self-management effectiveness * burnout and (3) Emotional intelligence * burnout. Therefore, the overall effect of negative psychology was 0.64 (95% CI: 0.63,0.66). Emotion management self-efficacy could have an indirect effect on burnout through emotional intelligence (β=˗0.02, p=0.011), and the total effect of emotion management self-efficacy on burnout was ˗0.08 (95% CI: ˗0.010, ˗0.06). Emotional intelligence had only a direct effect on burnout (β=˗0.05, 95% CI: ˗0.007, ˗0.003); see Table 8 for details.
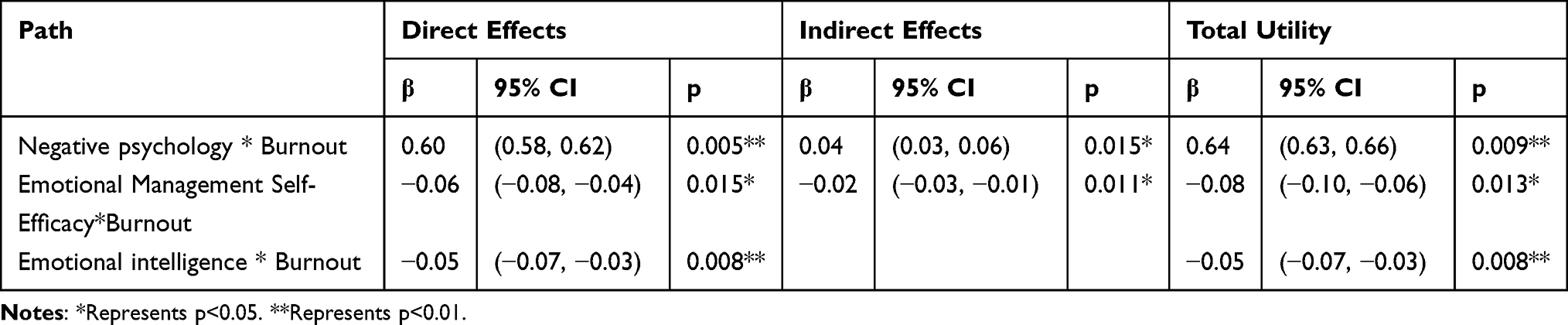 |
Table 8 Direct, Indirect and Total Effects of Burnout Influencing Factors |
Discussion
This study explored the influence of negative psychology on burnout in nurses and identified mediating roles for emotional intelligence and emotion management self-efficacy between negative psychology and burnout in nurses. Specifically, the findings suggest that negative psychology had a direct positive effect on burnout, ie the longer the exposure of caregivers to negative psychology, the more they lost enthusiasm and emotional commitment to their work.20 Studies have shown that nurses are susceptible to stress and burnout because they often work in particularly stressful and burdensome environments.21 Compared with other medical staff, nurses’ mental health levels are generally low, and they tend to experience psychological problems, such as anxiety and depression.22 Clinical nurses are under both physical and psychological pressure in their work and are a group that reflects a high incidence of negative emotions. These negative emotions will not only affect nurses’ own physiological functioning and health status but can also reduce work efficiency and service quality and even affect patient treatment outcomes. This can also reduce job satisfaction and professional identity, leading to burnout and turnover.23
As vital members of the healthcare team, nurses often have to manage busy schedules, a high sense of responsibility and the stress and mood swings that inevitably arise in the work environment. Studies have shown that nurses often encounter a variety of negative emotions at work, eg seeing patients’ health deteriorate, observing them suffer and even die, which may lead to negative psychological reactions and increase nurses’ risk of burnout.24 This study suggests that negative psychological traits in nurses significantly affect burnout. When nurses face greater stress, anxiety and depression, burnout occurs.21 A negative psychological state will lead to greater mood swings among nurses and give rise to dissatisfaction and feeling lost and helpless professionally, thus affecting their work efficiency and quality and negatively affecting their own physical and mental health, leading to fatigue, insomnia and other problems.7,25
This study found an inverse correlation between emotion management self-efficacy and burnout among nurses, a result that was also demonstrated in existing research.11 A similar study showed that burnout syndrome was significantly associated with emotional exhaustion, depression and personality factors.26 Emotion management self-efficacy refers to a nurse’s confidence and belief that they can effectively manage their emotions and those of others. When nurses feel empowered to effectively do so, they are more likely to cope with the stress and challenges of work, thereby reducing burnout.27 When nurses lack emotion management self-efficacy, they may face problems such as loss of emotional control, depression and exhaustion, which can also lead to burnout. This result of this study shows that nurses with high emotion management self-efficacy can effectively manage their emotions when dealing with heavy workloads and stress and believe that they can overcome the influence of negative emotions and actively engage in daily work, thereby reducing the occurrence of burnout.
This study found that emotional intelligence among nurses could reduce the incidence of burnout. Previous studies have also shown that emotional intelligence had a protective effect on the occurrence of burnout and psychosomatic complaints and beneficial effects on job satisfaction.28,29 A study of registered nurse anaesthetists showed that nurses with higher levels of emotional intelligence had significantly lower levels of work-related stress and burnout.30 Emotional intelligence refers to the ability of individuals to perceive and understand their emotions and those of others, correctly assess and express emotional needs and use emotional information intelligently to promote cognitive activities. Individuals with high emotional intelligence can express emotions in socially acceptable ways, understand the causes and consequences of emotions, use them to enhance their thoughts, actions and social relationships and regulate them when they are not goal-appropriate or suitable for the situational context.31,32 Previous studies have shown a negative correlation between emotional intelligence and burnout in healthcare workers, while burnout symptoms were reduced when healthcare professionals were trained in emotional intelligence.33,34
In the model of this study, negative psychology could have an indirect effect on burnout through emotional intelligence and emotion management self-efficacy, a result that has also been traced in other studies.35–37 Previous studies found that emotional intelligence buffered the effects of negative emotions on burnout29 and that emotion management self-efficacy could regulate the relationship between stress and burnout.38 Individuals with high emotional intelligence are more likely to view negative emotional and stressful situations as challenges rather than threats and will be more confident about their ability to cope with them.39 In addition, emotional intelligence is associated with more effective emotion regulation strategies, and nurses with high emotional intelligence will be able to effectively reduce the intensity and duration of negative state of mind, thereby protecting them from burnout.40 Nurses’ emotional intelligence and emotion management self-efficacy can be improved through practical training to help them cope with high-load emotional situations and reduce stress responses.
Novelty of This Study
In this study, the association between negative psychology and burnout among clinical nurses was analysed from the perspectives of emotion management, self-efficacy and emotional intelligence; the internal relationship between variables was explored from various viewpoints and methods, and the key factors of nurse burnout were explored. The study clarified evidence for reducing burnout among nurses, providing a basis for healthcare policymakers and clinical managers to design simple and feasible strategies for reducing burnout among nurses and ensuring clinical safety.
Limitations
This study has certain limitations. First, it is aimed at clinical nurses in Hunan Province, which cannot be extended to the entire country; therefore, research in more regions is needed to confirm the results. Second, this study did not focus on the impacts of hospital level, system and culture on hospital nurses. Finally, all questionnaires included in this study were self-reported, which may have led to reporting bias. Future research should employ a longitudinal approach to determine nurses’ anxiety and self-efficacy levels during the ongoing pandemic.
Conclusion
In summary, clinical nurses must take timely measures to alleviate negative psychological states and reduce the occurrence and development of burnout. Nurses can improve their emotional state and resistance to burnout by attending career development courses, seeking support and guidance and engaging in regular self-reflection. In addition, medical institutions can also take a series of measures to alleviate burnout, such as providing rich career development opportunities, establishing support and communication mechanisms and reducing nurses’ workloads and pressure to improve their work satisfaction and quality and reduce the occurrence of burnout.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of The First Hospital Affiliated with Hunan Normal University (Hunan Provincial People`s Hospital). Written informed consent was obtained from all participants. Ethics ID: LL-20211221-4
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Hunan Provincial Science and Technology Department’s Inclusive Policy and Innovation Environment Construction Plan Science Popularization Special Fund (Project Number:2021ZK4058).
Disclosure
The authors declare that they have no competing interests.
References
1. Kelly LA, Lefton C, Fischer SA. Nurse leader burnout, satisfaction, and work-life balance. J Nurs Adm. 2019;49(9):404–410. doi:10.1097/NNA.0000000000000784
2. Dall’Ora C, Ball J, Reinius M, Griffiths P. Burnout in nursing: a theoretical review. Hum Resour Health. 2020;18(1):41. doi:10.1186/s12960-020-00469-9
3. Dharra S, Kumar R. Promoting mental health of nurses during the coronavirus pandemic: will the rapid deployment of nurses’ training programs during COVID-19 improve self-efficacy and reduce anxiety? Cureus. 2021;13(5):e15213. doi:10.7759/cureus.15213
4. Sharma A, Kumar R. Psychological distress and coping styles among baccalaureate nursing students: promoting mental health of future nurses in COVID-19 pandemic. J Educ Health Promot. 2022;11(1):331. doi:10.4103/jehp.jehp_1140_21
5. Kumar R, Beniwal K, Bahurupi Y. Pandemic fatigue in nursing undergraduates: role of individual resilience and coping styles in health promotion. Front Psychol. 2022;13:940544. doi:10.3389/fpsyg.2022.940544
6. Galletta M, Portoghese I, D’Aloja E, et al. Relationship between job burnout, psychosocial factors and health care-associated infections in critical care units. Intensive Crit Care Nurs. 2016;34:51–58. doi:10.1016/j.iccn.2015.11.004
7. Chen YC, Guo YL, Chin WS, Cheng NY, Ho JJ, Shiao JS. Patient-nurse ratio is related to nurses’ intention to leave their job through mediating factors of burnout and job dissatisfaction. Int J Environ Res Public Health. 2019;16(23):4801. doi:10.3390/ijerph16234801
8. ICD −11 for mortality and morbidity statistics[EB/OL]. /2023 −03 −02. Available from: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281.
9. Li Y, Zhou J, Yin T, et al. Investigation and research on work stressors of front-line nursing staff in the prevention and treatment of COVID-19. Pract Prev Med. 2022;29(2):161–164. doi:10.3969/j.issn.1006-3110.2022.02.009
10. Yan J, Wu C, Du Y, He S, Shang L, Lang H. Occupational stress and the quality of life of nurses in infectious disease departments in China: the mediating role of psychological resilience. Front Psychol. 2022;13:817639. doi:10.3389/fpsyg.2022.817639
11. Hong E, Lee YS. The mediating effect of emotional intelligence between emotional labour, job stress, burnout and nurses’ turnover intention. Int J Nurs Pract. 2016;22(6):625–632. doi:10.1111/ijn.12493
12. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-u
13. Gong X, Xie X, Xu R, Luo Y. Psychometric properties of the Chinese versions of DASS-21 in Chinese college students. Chin J Clin Psychol. 2010;18(04):443–446.
14. Schutte NS, Malouff JM, Hall LE, et al. Development and validation of a measure of emotional intelligence. Pers Indiv Differ. 1998;25(2):167–177. doi:10.1016/S0191-8869(98)00001-4
15. Wang C, He Z. The relationship between parental rearing styles with general self-efficacy and emotional intelligence in middle school students. Chin Mental Health J. 2002;16(11):781–782,785. doi:10.3321/j.issn:1000-6729.2002.11.023
16. Caprara GV, Di Giunta L, Eisenberg N, Gerbino M, Pastorelli C, Tramontano C. Assessing regulatory emotional self-efficacy in three countries. Psychol Assess. 2008;20(3):227–237. doi:10.1037/1040-3590.20.3.227
17. Wang Y, Dou K, Liu Y. Revision of the scale of regulatory emotional self-efficacy. J Guangzhou Univ. 2013;12(01):45–50.
18. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annual Review of Psychology. 2001;52(1):397–422.
19. Hu Q, Schaufeli WB. The factorial validity of the Maslach burnout inventory-student survey in China. Psychol Rep. 2009;105(2):394–408. doi:10.2466/PR0.105.2.394-408
20. Leiter MP, Maslach C. Nurse turnover: the mediating role of burnout. J Nurs Manag. 2009;17(3):331–339. doi:10.1111/j.1365-2834.2009.01004.x
21. Van Bogaert P, Timmermans O, Weeks SM, van Heusden D, Wouters K, Franck E. Nursing unit teams matter: impact of unit-level nurse practice environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events--a cross-sectional survey. Int J Nurs Stud. 2014;51(8):1123–1134. doi:10.1016/j.ijnurstu.2013.12.009
22. National Health and Family Planning Commission of the People’s Republic of China. National nursing development plan (2016–2020). Chinese Journal of Nursing Management. 2017;17(01):1–5. doi:10.3969/j.issn.1672-1756.2017.01.001
23. Barr P. Personality traits, state positive and negative affect, and professional quality of life in neonatal nurses. J Obstet Gynecol Neonatal Nurs. 2018;47(6):771–782. doi:10.1016/j.jogn.2018.08.003
24. Font-Jimenez I, Ortega-Sanz L, Acebedo-Uridales MS, Aguaron-Garcia MJ, deMolina-Fernández I, Jiménez-Herrera MF. Nurses’ emotions on care relationship: a qualitative study. J Nurs Manag. 2020;28(8):2247–2256. doi:10.1111/jonm.12934
25. Zheng L, Zhang L, Chen Y. Current status and relationship between psychological capital, burnout and willingness to leave in clinical nurses. J Gen Nurs. 2022;20(22):3119–3121. doi:10.12104/j.issn.1674-4748.2022.22.025
26. Ramírez-Elvira S, Romero-Béjar JL, Suleiman-Martos N, et al. Prevalence, risk factors and burnout levels in intensive care unit nurses: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(21):11432. doi:10.3390/ijerph182111432
27. Martínez-Morato S, Feijoo-Cid M, Galbany-Estragués P, Fernández-Cano MI, Arreciado Marañón A. Emotion management and stereotypes about emotions among male nurses: a Qualitative Study. BMC Nurs. 2021;20(1):114. doi:10.1186/s12912-021-00641-z
28. Soto-Rubio A, Giménez-Espert MDC, Prado-Gascó V. Effect of emotional intelligence and psychosocial risks on burnout, job satisfaction, and nurses’ health during the COVID-19 pandemic. Int J Environ Res Public Health. 2020;17(21):7998. doi:10.3390/ijerph17217998
29. Szczygiel DD, Mikolajczak M. Emotional intelligence buffers the effects of negative emotions on job burnout in nursing. Front Psychol. 2018;9:2649. doi:10.3389/fpsyg.2018.02649
30. Bittinger AC, Dunn K, Hranchook A, Codier E. Relationship between emotional intelligence and occupational stress levels among certified registered nurse anesthetists. AANA J. 2020;88(5):398–404.
31. Mayer JD, Caruso DR, Salovey P. The ability model of emotional intelligence: principles and updates. Emot Rev. 2016;8(4):290–300. doi:10.1177/1754073916639667
32. Petrides KV, Mikolajczak M, Mavroveli S, Sanchez-Ruiz MJ, Furnham A, Pérez-González JC. Developments in trait emotional intelligence research. Emot Rev. 2016;8(4):335–341. doi:10.1177/1754073916650493
33. Mikolajczak M, Menil C, Luminet O. Explaining the protective effect of trait emotional intelligence regarding occupational stress: exploration of emotional labour processes. J RES PERS. 2007;41(5):1107–1117. doi:10.1016/j.jrp.2007.01.003
34. Karahan TF, Yalcin B. The effects of an emotional intelligence skills training program on anxiety, burnout and glycemic control in type 2 diabetes mellitus patients. Turkiye Klinikleri Tip Bilimleri Dergisi. 2009;29(1):16–24. doi:10.1177/0145721708327303
35. Lin T, Yi L, Tian T, Liu Y. Study on the influence of mindfulness level on job burnout of junior nurses in primary hospitals: based on the mediating effect of emotional intelligence. Health Prof Educ. 2023;41(4):109–113. doi:10.20037/j.issn.1671-1246.2023.04.33
36. Liu H. The Influence and Intervention of Emotion Regulation Self-Efficacy and Cognitive Emotion Regulation on Nurses’ Burnout [D]. Shandong University of Traditional Chinese Medicine; 2016.
37. Yang Y, Zhou W, X HE, Zhang B, He X. Mediating role of emotional intelligence of psychiatric nurses between workplace violence and job burnout. Chin Evidence Based Nurs. 2022;8(18):2501–2506. doi:10.12102/j.issn.2095-8668.2022.18.016
38. Görgens-Ekermans G, Brand T. Emotional intelligence as a moderator in the stress-burnout relationship: a questionnaire study on nurses. J Clin Nurs. 2012;21(15–16):2275–2285. doi:10.1111/j.1365-2702.2012.04171.x
39. Mikolajczak M, Luminet O. Trait emotional intelligence and the cognitive appraisal of stressful events: an exploratory study. Pers Indiv Differ. 2008;44(7):1445–1453. doi:10.1016/j.paid.2007.12.012
40. Peña-Sarrionandia A, Mikolajczak M, Gross JJ. Integrating emotion regulation and emotional intelligence traditions: a meta-analysis. Front Psychol. 2015;6:160. doi:10.3389/fpsyg.2015.00160
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.