Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
The Learning Curve of Reverse-Sequence Endoscopic Nipple-Sparing Mastectomy with Immediate Prepectoral Implant Reconstruction: CUSUM Analysis
Authors Zhao R, He C, Jiang W ![]() , Lin S
, Lin S ![]() , Zhao Y
, Zhao Y ![]()
Received 21 August 2025
Accepted for publication 4 November 2025
Published 8 November 2025 Volume 2025:17 Pages 1041—1050
DOI https://doi.org/10.2147/BCTT.S558984
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Renyang Zhao, Chenyang He, Wei Jiang, Shuai Lin, Yang Zhao
The Comprehensive Breast Care Center, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China
Correspondence: Yang Zhao, The Comprehensive Breast Care Center, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China, Email [email protected]
Background: The reverse-sequence endoscopic nipple-sparing mastectomy with immediate prepectoral implant reconstruction (RSEM-IPI) has been described as a safe and feasible procedure for early-stage breast cancer. The aim of this study was to evaluate the learning curve for RSEM-IPI.
Methods: Between January 2023 and February 2024, we collected data on 104 consecutive patients who underwent RSEM-IPI at our hospital (53 for group 1 and 51 for group 2). The surgeons in group 1 completed the endoscopic training and assistance, whereas the surgeons in group 2 did not. The learning curve was analyzed using the cumulative sum (CUSUM) method to assess changes in the operative times across the case sequence.
Results: Among the 281 patients who received breast reconstruction surgeries, a total of 104 consecutive data were recorded and eligible. Both groups had higher rates of postoperative complications including bleeding, nipple-areolar complex (NAC) ischemia, skin ischemia, infection and longer drainage duration during the phrase 1 compared to the phrase 2. Notably, in terms of the most severe postoperative complications, implant expose and loss, both groups exhibited higher rates during the phrase 1. Breast-Q scores for group 1 in phases 1 and 2 were 66 and 84, respectively, while for group 2, they were 67 and 80. As compared with surgeons in group 2, well-trained surgeons in group 1 were more accessible for stable learning curve with fewer training patients (18 patients) and relatively lower rate of postoperative complications (p > 0.05).
Conclusion: The estimated learning curve for RSEM-IPI was achieved after 18 cases in the well-trained surgeon group. The endoscopic training and assistance were critical to master the breast endoscopic surgeries for breast surgeons.
Keywords: breast cancer reconstruction, learning curve, reverse-sequence, endoscopic mastectomy
Introduction
Breast cancer has become the second most common malignant tumor in humans.1,2 The incidence of breast cancer continues to rise globally and in China.1,2 With the advancement of research, the 5-year survival rate for breast cancer patients has increased by nearly 10% over the past decade.2,3 Among these treatments, surgery remains a crucial method for curing early-stage breast cancer patients.4,5 Over the past century, surgical techniques for breast cancer have undergone revolutionary changes, becoming more precise, minimally invasive, and less damaging.5,6
Early-stage breast cancer patients may not be suitable for breast-conserving surgery and may face the dilemma of mastectomy. The choice of breast reconstruction surgery poses a challenge for all breast surgeons. Autologous reconstruction is time-consuming, labor-intensive associated with significant trauma and long-time recovery. Although its acceptance has increased in recent years, its clinical application remains limited due to the complexity of the procedure.7 Prosthetic reconstruction is currently the mainstream choice, as it is relatively simple to perform, which has fewer complications and is widely accepted by clinicians.8,9 Prepectoral implant reconstruction is more widely used in clinical practice due to its superior cosmetic outcomes.8 Professor Zhenggui Du from West China Hospital of Sichuan University has modified the endoscopic mastectomy + immediate prosthetic implantation technique by a reverse-sequence method for breast removal.8 This technique, known as the reverse-sequence endoscopic nipple-sparing mastectomy with immediate prepectoral implant reconstruction (RSEM-IPI), has gained widespread acceptance due to its scarless approach on the breast.
Breast endoscopic surgery has been developed over a decade, but RSEM-IPI procedure has recently been promoted in China.8,10 Our research team has been actively engaged in related explorations and has accumulated a certain level of technical expertise. We aimed to construct the learning curve of RSEM-IPI by analyzing previous data, thereby assisting more breast surgeons in achieving rapid growth, mastering this technique swiftly, reducing postoperative complications, and comparing the advantages and disadvantages of RSEM-IPI with other breast surgical treatments.
Materials and Methods
Patients and Groups
We retrospectively analyzed all patients with early-stage breast cancer in the comprehensive breast care center, the second affiliated hospital of Xi’an jiaotong university. Between January 2023 and February 2024, 104 patients with early-stage breast cancer performed the reverse-sequence endoscopic nipple-sparing mastectomy with immediate prepectoral implant reconstruction, who were divided into two groups, group 1 and group 2. Group 1 was Yang Zhao and Shuai Lin’s group, including 53 patients, as well as group 2 was other surgeons’ group, including 51 patients. The surgeons and assistants in group 1 completed 3-month endoscopic training of breast cancer surgery and 6-month laparoscopic assistance in our hospital and West China hospital. On the other hand, the surgeons and assistants in group 2 were not assigned to complete the endoscopic training and laparoscopic assistance. All patients signed the operation consents. Besides, all surgeons and assistants in each group had completed more than 300 traditional operations of breast cancer. The therapeutic strategies of patients with breast cancer were drawn up according the national comprehensive cancer network (NCCN) guideline for breast cancer (https://www.nccn.org/).
Clinical Parameters and Files
One hundred and four patients with early-stage breast cancer in group 1 and group 2 were eligible for our study. All clinical parameters of 104 breast cancer patients were recorded in our center. The clinical parameters included age, gender, T status, lymph node status, hormone receptor status, Her-2 status, neoadjuvant/adjuvant chemotherapy and radiotherapy. As we did the learning curve analysis, the post- and intra-operative parameters including bleeding volume, drainage duration, nipple-areolar/skin ischemia, infection, implant expose and implant loss were involved in our study. In addition, Breast-Q questionnaire was completed to acquire the cosmetic Q score11,12 at the postoperative 3 month. We characterized the operation time as the single parameter to establish learning curve. According to learning curve, different phases were divided for learning RSEM-IPI. Operative time was characterized as the timing of RSEM and implant placement.
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were made up according to the guideline of breast cancer reconstruction of China.13 Inclusion criteria: 1. Female; 2. Invasive breast cancer or breast carcinoma in situ; 3. Contraindications or refusion of breast-conserving surgeries; 4. Thickness of subcutaneous tissue was acceptable for RSEM-IPI, sub-areolar biopsy confirmed as tumor-free and negative; 5. Signed consent form; 6. Clinicopathological data were available; 7. Breast ptosis grade 1–2.14 The indications of RSEM-IPI were referred to Zhenggui Du’s paper.8
Exclusion criteria: 1. Metastatic breast cancer; 2. No accomplishment of R0 resection, skin invasion or satellite nodules; 3. Severe underlying diseases or severe cardiopulmonary dysfunction leading to the inability to tolerate general anesthesia; 4. Clinicopathological data was missed or unavailable; 5. Breast ptosis grade 3.14
Operative Team and Technique
The surgeons and assistants in group 1 and group 2 cooperated together for 1 year or longer. The breast surgery nurses team had been built for 2 years, who were able to understand the concept of breast reconstruction and do a favor to finish the reconstruction surgery. The operations were performed according to the guideline of Zhenggui Du’s team.8,10 In brief, the incision of axillary fossa skin was designed and applied, 4–5 cm, to sentinel lymph node biopsy or axillary lymph node dissection, where the disposable surgitractor for breast cancer was fixed on the incision. The flow rate and pressure were facilitated as 15 L/min and 12 mmHg, respectively. Then, the mammary gland was freed by retromammary space between mammary gland and pectoralis major, and subcutaneous tissue between skin and mammary gland. The implant (Mentor, USA) was put into the prepectoral space, and the Fowler’s or semi-upright position was intra-operatively used for the cosmic outcome of implant. The operation times were recorded (min). The implants in this study were provided from Mentor 311 and 321 series. TiLoop mesh (PFM, Germany) was selectively used for patients with prebreast cancer receiving postoperative radiation.
Postoperative Follow-up and Oncological Outcomes
Patients were scheduled for follow-up visits every 3 months for the first 2 years, then every 6 months for a further 3 years, and every year thereafter. Patients were requested to complete the self-administered Breast-Q questionnaires at 3 months after surgery to acquire the satisfaction degree for the cosmetic outcome of implant-based reconstruction.
Cumulative Sum (CUSUM) Analysis and Fitting Curve Equation
CUSUM analysis was a statistical technique applied to surgical procedures for the quantitative estimation of learning curve, which was the running total of differences between the individual data points and the average of all data points. In the present study, we referred to the RSEM-IPI operative time as the parameter for CUSUM. Cases were arranged chronologically from the earliest case to the latest case. CUSUM was defined using the following equation: CUSUMn=Operation timen-Operation timeaverage+CUSUMn-1.15,16 According to the CUSUM process, the learning curve can be represented intuitively while detecting consistent changes in the operative time. The fitting curve equations of group 1 and group 2 were established in the software of Excel.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for Social Sciences, version 25.0 (SPSS, Chicago, USA). Continuous variables are expressed as means or medians and were compared using ANOVA and t tests, according to the normality of data and the homogeneity of variance test. Categorical variables are expressed as proportions and were compared using the Chi-square and Fisher’s exact tests. In this study, the learning curve was analyzed using the CUSUM methods. Two-sided P values < 0.05 were considered as significant.
Results
Study Flow Chart and Patients’ Characteristics
As shown in Figure 1, the flow chart of this study was constructed. We retrospectively analyzed all patients with breast cancer performing immediate breast reconstruction in the comprehensive breast care center of the second affiliated hospital of Xi’an jiaotong university from January 2023 to February 2024. One hundred and four patients with early-stage breast cancer were eligible for our study (RSEM-IPI), who were divided into two groups, group 1 (Yang Zhao and Shuai Lin’ group for 53) and group 2 (Weili Min’s group for 51). The clinicopathological characters of the patients in group 1 and group 2 were shown in Table S1. Accordingly, the similar distribution of the different clinicopathological parameters were observed between group 1 and group 2.
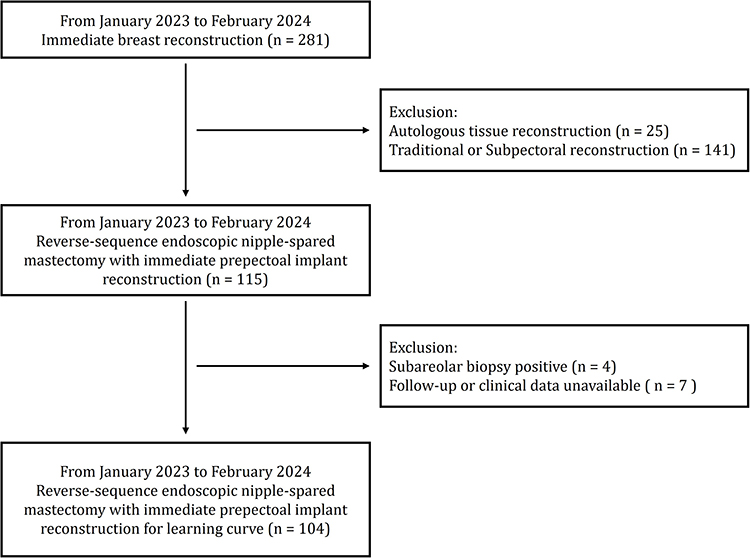 |
Figure 1 Flow chart of study for learning curve analysis. |
Surgical Technique and Process of RSEM-IPI
All surgeons in group 1 and group 2 had the ability to perform a variety of breast cancer surgeries, including mastectomy, breast-conserving surgery, sentinel lymph node biopsy and axillary lymph node dissection. The surgeons in group 1 were assigned to achieve the endoscopic training and assistance (Figure 2), but the surgeons in group 2 not.
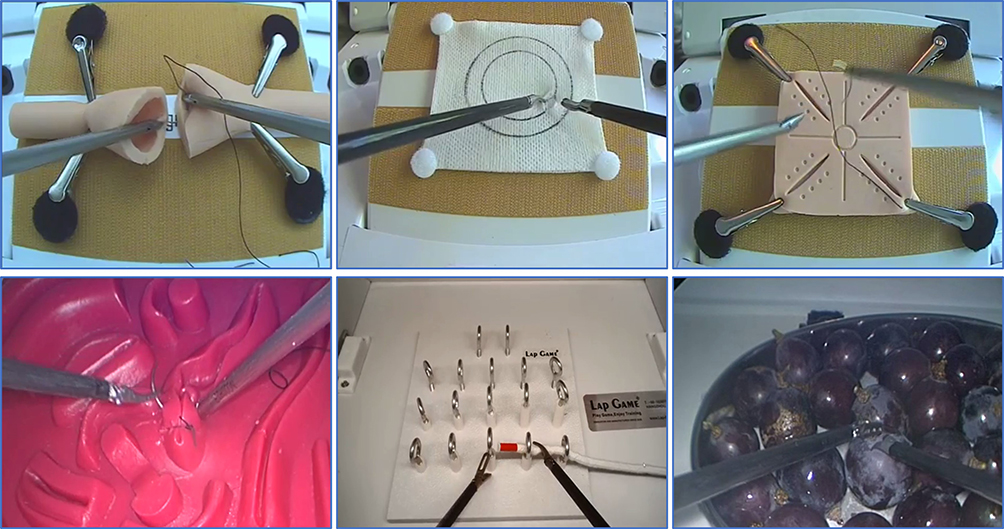 |
Figure 2 Endoscopic training. |
The operative procedures and notions were referred to Zhenggui Du’s instructions.8,10 During the RSEM-IPI, we fixed and located trocars in the axillary incision (Figure 3A). We initially freed the mammary gland in the retromammary space. Then, the mammary gland was completely removed through the subcutaneous tissue layer (Figure 3B and C). RSEM-IPI was able to provide an opportunity to create the aesthetic outcome with the non-wounded breast skin.
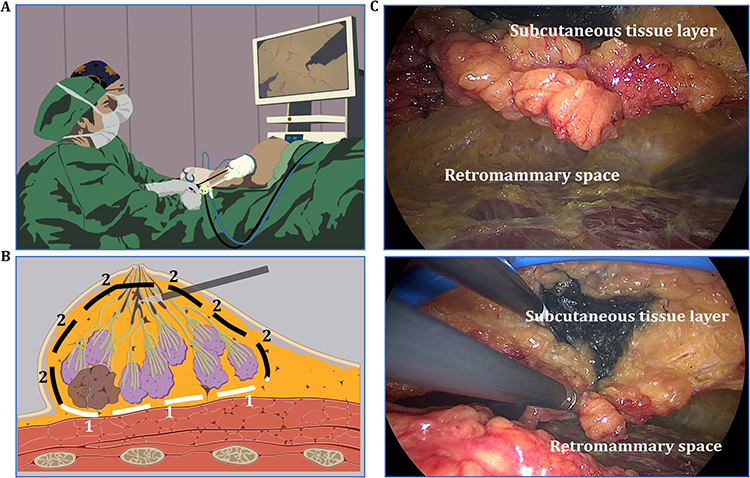 |
Figure 3 RSEM-IPI. (A) Surgical techniques of RSEM-IPI. (B) Schematic diagram of RSEM-IPI. The dashed lines delineated the extent of the resected breast tissue. “1” indicates the white dashed boundary at the base of the gland, while “2” denotes the black dashed boundary on the epidermal side of the gland. (C) Subcutaneous tissue layer and retromammary space showed during surgery. |
Learning Curve Analysis of RSEM-IPI
All 104 eligible patients with early-stage breast cancer underwent RSEM-IPI in the group 1 and group 2, and the consecutive data were recorded. In the cohort of group 2, 2 patients did not complete RSEM-IPI, while performed the traditional mastectomy with the immediate implant reconstruction. We defined the operative time as the single variable for CUSUM analysis. The operative time from the patients from group 1 and group 2 are shown in Figure 4A and B. According to the operative time from group 1 and group 2, we established the learning curves for group 1 and group 2, by which the curve fitting equations for group 1 and group 2 were conceived for group 1: y = −1.1112x2 + 50.454x + 332.4 and group 2: y = −1.9335x2 + 95.7x - 0.0773. We divided the learning curves of group 1 and group 2 into two phrases, phrase 1 (learning phrase) and phrase 2 (mastering phrase) (Figure 4A and B). According to the learning curve of group 1, case 1–18 represented phrase 1, as well as case 19–53 indicated phrase 2. In the group 2, case 1–25 represented phrase 1, while case 26–49 indicated phrase 2. Hence, surgeons in the group 2 needed more cases to access phrase 2. It indicated that endoscopic training and assistance was dominant to promote surgeons’ ability to complete RSEM-IPI.
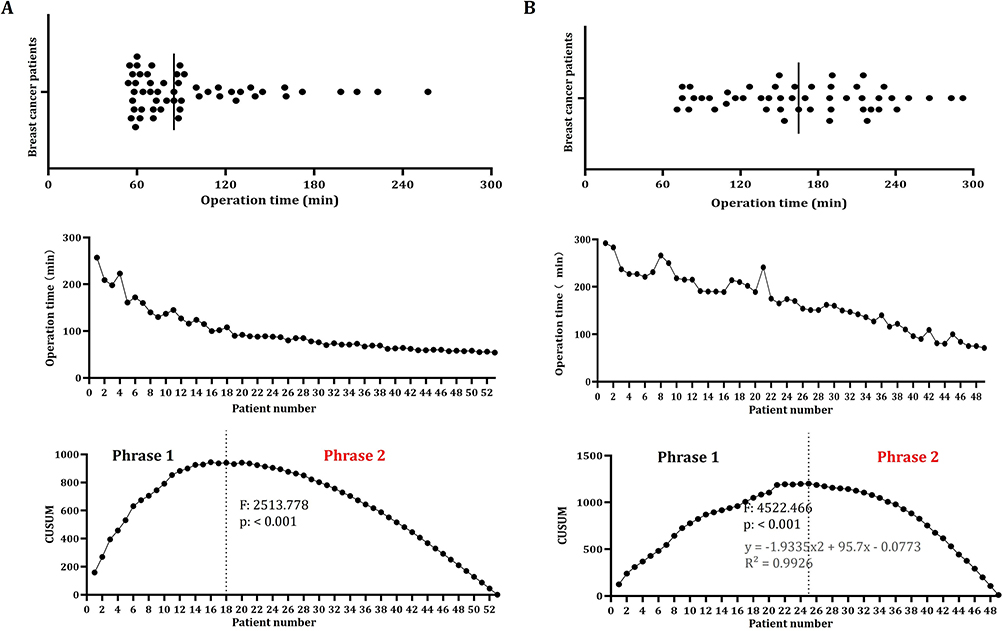 |
Figure 4 Learning curves of RSEM-IPI in group 1 (A) and group 2 (B) according the operative time. |
Postoperative Outcomes and Complications in the Different Learning Phrases
Through comparison, we found that both groups had higher rates of postoperative complications including bleeding, nipple-areolar complex (NAC) ischemia, skin ischemia, infection, drainage duration during the phrase 1 compared to the phrase 2 (Table S2). Notably, in terms of the most severe postoperative complications, implant expose and loss, both groups exhibited higher rates during the phrase 1 (Table S2). It indicated that the proficiency could only be achieved through the accumulation of case experience during the learning process. Intriguingly, we observed that during the phrase 1, the postoperative complication rate in group 1 was lower than that in group 2, further emphasizing the necessity of comprehensive training and laparoscopic-assisted practice, whereas our data showed no significant differences between the both groups. It might be due to the relatively small number of cases included. We planned to further expand our sample size for analysis.
Aesthetic Outcomes After RSEM-IPI
The evaluation of the cosmetic outcomes of RSEM-PI was a crucial component of the overall surgical assessment. We employed the Chinese version of the Breast-Q scale to assess the cosmetic effects in surgical patients. Preliminary observations revealed that, despite the use of Tiloop mesh, the impact of radiotherapy on cosmetic outcomes remained destructive (Figure 5A and B). To illustrate the cosmetic finale of the surgery and to exclude the influence of radiotherapy, we chose to apply the Breast-Q scale at the post-surgery 3 months before the initiation of radiotherapy. We utilized the Breast-Q template specifically designed for breast reconstruction, focusing on breast satisfaction after surgery. According to our observations, the cosmetic scores in both groups during Phase 1 were significantly lower than those in Phase 2 (P < 0.001, Figure 6). The average Breast-Q scores for group 1 in phases 1 and 2 were 66 and 84, respectively. While for group 2, they were 67 and 80 (Figure 6). These findings further validated the rationality of our learning curve.
 |
Figure 5 Aesthetic outcomes for patients (patient 1 (A) and patient 2 (B)) receiving RSEM-IPI after radiation. The arrow-pointed region served as the comparative area for evaluating the effects of radiotherapy versus non-radiotherapy on breast aesthetic outcomes. |
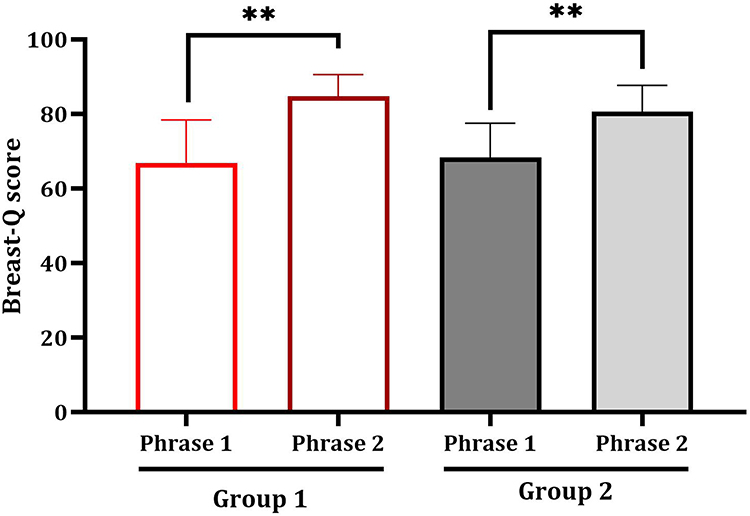 |
Figure 6 Breast-Q scores for phrases 1 and 2 in the groups 1 and 2. **p < 0.01. |
Discussion
The treatment modalities for breast cancer are constantly evolving, with drugs being updated and treatment models innovated.4,8,17 However, it is undeniable that surgery remains a method for curing early-stage breast cancer.18,19 Surgical approaches for breast cancer are also continuously changing, with breast-conserving surgery and sentinel lymph node biopsy as representative examples. These surgical methods have become more refined and diverse, placing higher demands on breast surgeons. The breast is a symbolic organ for women, and breast surgery, to varying degrees, affects women’s psychological and physiological health.3,11 In clinical practices of breast surgeons, there is indeed a subset of early-stage breast cancer patients who cannot undergo breast-conserving surgery and face the dilemma of mastectomy. Breast reconstruction is an inevitable choice for these patients. The first choice is whether to perform immediate reconstruction or delayed reconstruction. Based on current clinical data, immediate reconstruction should be the preferred option due to fewer complications, lower costs, and better cosmetic outcomes.20 On the other hand, the debate between autologous reconstruction and implant-based reconstruction persists.7,21 Autologous reconstruction is more surgically challenging, costly, and has a slower recovery, but it offers better long-term results and is less affected by radiotherapy. In contrast, implant-based reconstruction is more affected by radiotherapy and has slightly inferior long-term results compared to autologous reconstruction, but it is less surgically challenging, less costly, and has a prompt recovery. Implant-based reconstruction remains mainstream in breast cancer reconstruction surgery. Implant-based immediate reconstruction was more commonly performed subpectorally, but the subpectoral space is artificially created and restricted, and the implant is significantly affected by the pectoralis major muscle leading to pronounced capsular contracture after radiotherapy.22,23 Therefore, prepectoral implant-based immediate surgery recently has begun to emerge as the mainstream.
The placement of the implant in the prepectoral space avoids limiting impaired muscle function, muscle spasms, postoperative pain, and the dreaded animation deformity.24 Additional surgery is needed to modify the animation deformity but converting the submuscular or dual plane implant to prepectoral reconstruction. Endoscopic breast cancer surgery has been widely reported by Jiang Jun’s team who have made outstanding contributions in this field.25 Through the lipolysis method, axillary lymph node dissection can be successfully performed. However, mastectomy remains challenging. The team led by Zhenggui Du from West China Hospital proposed the reverse sequence method for breast cancer resection combined with immediate prosthetic implantation.8 The RSEM-IPI surgery was used in clinical practice for about a decade, and the application of laparoscopy in breast reconstruction was limited by a lack of experience. Prepectoral surgery, where the prosthesis is covered by the skin, increases the risk of failure, but the risk could be mitigated by improving surgical techniques. The learning curve is a prerequisite for mastering any new surgical procedure and represents the inevitable process through which the surgeon progresses from inexperience to proficiency. The learning curve was constructed using the CUSUM method, and our study selected operative time as the single variate to build the learning curve. Based on our team’s observations, 18 cases of RSEM-IPI surgery were generally sufficient to meet the learning process of surgeons, enabling them to master this technique proficiently. By comparing the surgeons in group 2, we found that the thorough laparoscopic training and preparatory work are essential prerequisites for performing RSEM-IPI surgery, effectively reducing postoperative complications, particularly for implant expose or loss. Our results also reaffirmed the reality of the learning curve, where the incidence of complications was higher during the learning phase. Specifically, the complication rates in both groups during the learning phase (Phrase 1) were higher than those in the proficient phase (Phrase 2).
For breast reconstruction surgery, aesthetic satisfaction is of paramount importance. The Breast-Q scale is the most widely used aesthetic satisfaction scale among breast plastic surgeons worldwide.26,27 In our study, we employed the aesthetic satisfaction scale of the breast reconstruction module to evaluate postoperative aesthetic satisfaction. Our team also incorporated breast aesthetics as a crucial component in assessing the learning curve. We observed that during the phrase 1, the breast aesthetic scores were significantly lower than those in the phrase 2, indicating that surgical outcomes can be improved through learning. Our findings suggested that with sufficient practice, this surgical technique could be mastered and effectively applied in clinical settings, providing valuable insights and assistance for surgeons aspiring to perform this procedure. However, the limited number of cases in this study might have influenced the results. We expected to observe our findings in studies with larger sample sizes and longer follow-up period.
Conclusion
RSEM-IPI surgery has been increasingly accepted by more breast surgeons. Our research findings will encourage more breast surgeons to standardize their learning and practice of RSEM-IPI, thereby making RSEI-IPI surgery more standardized.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. The procedures of this study were approved by the ethics committee of the second affiliated hospital of Xi’an jiaotong university (2024YS096). We obtained consent from the participants to access their medical records.
Consent for Publication
All authors consent for publication. Consent forms have been signed.
Acknowledgment
A lot of thanks for Weili Min who provided the data of group 2. A lot of thanks for Rongqiang Zhang who provided the favors of the statistical analysis for those data in the study. A lot of thanks for AI software ReadPaper for translation from Chinese to English.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by Hospital Funding (2020YJ(ZYTS)433); SCI funding (SCI00368); National Natural Science Foundation of China (No. 81872390).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng RS, Chen R, Han BF, et al. Cancer incidence and mortality in China, 2022. Zhonghua Zhong Liu Za Zhi. 2024;46(3):221–231. doi:10.3760/cma.j.cn112152-20240119-00035 Polish
2. Lan B, Li Q, Ma F, Xu B. The road toward breast cancer single-disease quality control in China. Cancer Innov. 2023;2(5):319–322. doi:10.1002/cai2.93
3. Lei S, Zheng R, Zhang S, et al. Breast cancer incidence and mortality in women in China: temporal trends and projections to 2030. Cancer Biol Med. 2021. doi:10.20892/j.issn.2095-3941.2020.0523
4. Toi M, Kinoshita T, Benson JR, et al. Non-surgical ablation for breast cancer: an emerging therapeutic option. Lancet Oncol. 2024;25(3):e114–e125. doi:10.1016/S1470-2045(23)00615-0
5. Gentilini OD, Botteri E, Sangalli C, et al. Sentinel lymph node biopsy vs no axillary surgery in patients with small breast cancer and negative results on ultrasonography of axillary lymph nodes: the sound randomized clinical trial. JAMA Oncol. 2023;9(11):1557–1564. doi:10.1001/jamaoncol.2023.3759
6. Pantiora E, Tasoulis MK, Valachis A, et al. Evolution and refinement of magnetically guided sentinel lymph node detection in breast cancer: meta-analysis. Br J Surg. 2023;110(4):410–419. doi:10.1093/bjs/znac426
7. Malekpour M, Malekpour F, Wang HT. Breast reconstruction: review of current autologous and implant-based techniques and long-term oncologic outcome. World J Clin Cases. 2023;11(10):2201–2212. doi:10.12998/wjcc.v11.i10.2201
8. Zhou J, Xie Y, Liang F, et al. A novel technique of reverse-sequence endoscopic nipple-sparing mastectomy with direct-to-implant breast reconstruction: medium-term oncological safety outcomes and feasibility of 24-h discharge for breast cancer patients. Int J Surg. 2024;110(4):2243–2252. doi:10.1097/JS9.0000000000001134
9. Tellarini A, Bascialla E, Paganini F, et al. Breast reconstruction with TiLOOP(R) Bra: another arrow in plastic surgeons’ quiver? J Plast Reconstr Aesthet Surg. 2024;97:89–114. doi:10.1016/j.bjps.2024.07.060
10. Chung K, Xie Y, Liang F, et al. Reverse-sequence endoscopic nipple-sparing mastectomy with immediate implant-based breast reconstruction: an improvement of conventional minimal access breast surgery. Front Oncol. 2024;14:1366877. doi:10.3389/fonc.2024.1366877
11. Gallo L, Chu JJ, Shamsunder MG, et al. Best practices for BREAST-Q research: a systematic review of study methodology. Plast Reconstr Surg. 2022;150(3):526e–535e. doi:10.1097/PRS.0000000000009401
12. Li L, Yang B, Li H, et al. Chinese multicentre prospective registry of breast cancer patient-reported outcome-reconstruction and oncoplastic cohort (PRO-ROC): a study protocol. BMJ Open. 2019;9(12):e032945. doi:10.1136/bmjopen-2019-032945
13. Guideline of breast cancer from the society of breast cancer china anti-cancer association (2024). J China Oncology. 2023;33(12):1092–1186. doi:10.19401/j.cnki.1007-3639.2023.12.004
14. See MH, Yip KC, Teh MS, et al. Classification and assessment techniques of breast ptosis: a systematic review. J Plast Reconstr Aesthet Surg. 2023;83:380–395. doi:10.1016/j.bjps.2023.04.003
15. Zhang L, Hu C, Qin Q, et al. Learning process analysis of robotic lateral pelvic lymph node dissection for local advanced rectal cancer: the CUSUM curve of 78 consecutive patients. Surg Today. 2024;54(3):220–230. doi:10.1007/s00595-023-02725-6
16. Yu J, Rao S, Lin Z, Pan Z, Zheng X, Wang Z. The learning curve of endoscopic thyroid surgery for papillary thyroid microcarcinoma: CUSUM analysis of a single surgeon’s experience. Surg Endosc. 2019;33(4):1284–1289. doi:10.1007/s00464-018-6410-y
17. Zheng LW, Liu CC, Yu KD. Phase separations in oncogenesis, tumor progressions and metastasis: a glance from hallmarks of cancer. J Hematol Oncol. 2023;16(1):123. doi:10.1186/s13045-023-01522-5
18. Rocco N, Rispoli C, Moja L, et al. Different types of implants for reconstructive breast surgery. Cochrane Database Syst Rev. 2016;2016(5):CD010895. doi:10.1002/14651858.CD010895.pub2
19. Cicero Urban MR. Oncoplastic and Reconstructive Breast Surgery. Springer; 2013.
20. Yoon AP, Qi J, Brown DL, et al. Outcomes of immediate versus delayed breast reconstruction: results of a multicenter prospective study. Breast. 2018;37:72–79. doi:10.1016/j.breast.2017.10.009
21. Naoum GE, Salama L, Niemierko A, et al. Single stage direct-to-implant breast reconstruction has lower complication rates than tissue expander and implant and comparable rates to autologous reconstruction in patients receiving postmastectomy radiation. Int J Radiat Oncol Biol Phys. 2020;106(3):514–524. doi:10.1016/j.ijrobp.2019.11.008
22. Ostapenko E, Nixdorf L, Devyatko Y, Exner R, Wimmer K, Fitzal F. Prepectoral versus subpectoral implant-based breast reconstruction: a systemic review and meta-analysis. Ann Surg Oncol. 2023;30(1):126–136. doi:10.1245/s10434-022-12567-0
23. Hung YC, McCarthy JT, Park BC, et al. Comparison of complication rates between subpectoral vs prepectoral techniques in prosthetic breast reconstruction. Aesthet Surg J. 2023;43(11):1285–1292. doi:10.1093/asj/sjad145
24. Fusario D, Casella D. Postoperative complications following prepectoral versus partial subpectoral implant-based breast reconstruction using ADM: a systematic review and meta-analysis. Aesthetic Plast Surg. 2024;48(1):13–14. doi:10.1007/s00266-023-03370-7
25. Du J, Liang Q, Qi X, et al. Endoscopic nipple sparing mastectomy with immediate implant-based reconstruction versus breast conserving surgery: a long-term study. Sci Rep. 2017;7:45636. doi:10.1038/srep45636
26. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, Cano SJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):345–353. doi:10.1097/PRS.0b013e3181aee807
27. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, Cano SJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):354. doi:10.1097/PRS.0b013e3181aee81e
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.