")
Back to Journals » International Journal of Women's Health » Volume 15
The Knowledge and Determinants of Sexual Health and Sexual Transmitted Infections Among Women in Saudi Arabia: A Nationwide Survey
Authors AlNujaidi HY , AlSaif AK, Saleem ALAnsary NF, Althumiri NA, BinDhim NF
Received 6 August 2023
Accepted for publication 30 October 2023
Published 11 November 2023 Volume 2023:15 Pages 1745—1756
DOI https://doi.org/10.2147/IJWH.S434179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Heba Yaagoub AlNujaidi,1 Atheer Kalid AlSaif,1 Naof Faiz Saleem ALAnsary,1 Nora A Althumiri,2 Nasser F BinDhim2
1Department of Public Health, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Scientific Department, Sharik Association for Health Research, Riyadh, Saudi Arabia
Correspondence: Heba Yaagoub AlNujaidi, Email [email protected]
Background: Sexual health is a necessary part of any society because it significantly influences the quality of life. Women’s knowledge regarding STIs and safe sex practices in Saudi Arabia has not been thoroughly investigated; therefore, this study aims to investigate and measure the knowledge and the determinants of sexual health and STIs among women in Saudi Arabia.
Methods: This study is a nationwide cross-sectional survey conducted through phone interviews in Saudi Arabia in 2021. This study included 1334 female participants aged 18 years or older.
Results: The study’s results collectively show that women in Saudi Arabia have limited knowledge of sexual health and STIs. The primary causes are the lack of knowledge of different STIs-communicability, symptoms, and an overall lack of technical proficiency in the subject. The study analyzed factors associated with participants’ knowledge of sexual health and sexually transmitted infections. Significant associations were found between knowledge and age, region, educational level, and family income. In the multivariable analysis, participants aged 20– 29 had higher knowledge compared to those aged > 60. Participants in the Eastern region had higher knowledge than those in the Southern region. Participants with less than a bachelor’s degree had lower knowledge than those with a bachelor’s degree or higher. Participants earning an average of 16,000 SAR to 19,999 SAR had higher knowledge than those with unstable monthly income.
Conclusion: The study found that women’s understanding of sexual health and STIs in Saudi Arabia is low due to a lack of knowledge and awareness. Knowledge levels were correlated with educational levels; therefore, targeted health promotion initiatives are needed to increase understanding, particularly regarding condom use for HIV and STI prevention.
Keywords: women’s health, STI, knowledge, sexual health, Saudi Arabia
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Fikri has been published for this article.
Introduction
Sexual health is a necessary part of any society because it significantly influences the quality of life. The WHO defines sexual health as “a state of physical, emotional, mental and social well-being related to sexuality; it is not merely the absence of disease, dysfunction or infirmity”.1 One of the critical indicators of sexual health is the individual ability to engage in safe sexual experiences that are characterized as being free of enforcement, discrimination, and violence.
Engaging in safe sexual experiences reduces the risks of sexually transmitted infections. Sexually transmitted infections (STIs), also known as Sexually Transmitted Diseases (STDs), “are caused by bacteria, viruses or parasites that are transmitted through unprotected sex (vaginal, anal, or oral) and skin-to-skin genital contact”.2 STIs can be passed on from one individual to another during the experience of unprotected sex.
The global spread of STIs is a major public health concern, particularly in developing countries. Although most STIs can be treated, they can lead to serious health complications if left untreated.3 A late diagnosis or inadequate treatment of sexually transmitted illnesses can result in serious complications such as premature mortality, infertility, and ectopic pregnancy. Therefore, knowledge of safe sexual practices is valuable to personal and public health, hence, the importance of addressing it.4 Nowadays, STIs have a significant impact on sexual and reproductive health globally. The WHO reported that more than 376 million people are at risk of contracting STIs.5 STIs encompass many diseases and conditions, put together from a global perspective, burden healthcare systems financially and socially.6
Addressing sexually transmitted infections (STIs) is still considered offensive in Saudi Arabia, where cultural norms pose a serious obstacle to freely discussing such private issues without fear of repercussions and shaming. In the case of Saudi Arabia, it has been posited that adults lack the needed knowledge and education that would help them protect themselves against the transmission of STIs. The diminished knowledge may very much result from the attitude towards the subject and the heightened sensitivity by which Saudi adults approach such topics.
Remarkably, data on sexually transmitted diseases among women in Saudi Arabia and females in other Islamic nations is considered limited.7,8 Also, this particular informational shortage has been confirmed by a systematic review conducted by Alomair et al, discussing the knowledge and attitudes of Muslim women worldwide toward sexually transmitted infections.7 Most published papers examining Saudi women’s sexual health were mainly focused on university students. The researcher of the review posited that Saudi women lack sufficient sexual health knowledge, and their negative attitudes concerning sexually transmitted infections (STIs) created barriers to seeking sexual health information and guidance.
Furthermore,9 Albanghali and Othman conducted a study among university students in Abha, Saudi Arabia, in which a lack of knowledge of STDs and a need for educational programs have been reported.9 Besides, Balbeesi & Mohizea investigated the knowledge of STIs among Saudi women in 2015. They found that they were more knowledgeable about HIV/AIDS and the modes of transmission than other STIs. The knowledge of STI symptoms was higher among younger, more educated, and more affluent females.10
Demographic factors such as the level of education and attitudes towards the use of condoms significantly impact the sexual health of most Saudi adults. According to Filemban and his collogues, educational level is substantially associated with the spread of sexually transmitted infections (STIs).11 This study supports previous research findings by demonstrating that individuals with little or no education are more likely to contract STIs.
Adequate education is required to dispel myths regarding STIs, such as the common misconceptions concerning Acquired Immune Deficiency Syndrome (AIDS). Therefore, health practitioners must identify more effective ways to educate adults about STI prevention, especially regarding protected sexual practices.
Sex education helps adults make educated health decisions by influencing their behavior and increasing their understanding of STDs. Furthermore, sex education enhances awareness of STI manifestations and symptoms, ultimately leading to better detection and earlier medical interventions.12 Therefore, local public health authorities may find it helpful to disseminate sex education materials in ways that are easy to understand, and that may not be found offensive or insensitive by the targeted audience or the public on a larger scale.
Among the notable and validated tools previously used in researching data related to sexual health and STIs include interviews, observation, and focus groups. Ivanova et al used in-depth interviews to gather detailed information regarding sexual and reproductive health (SRH).13 This method’s disadvantages include potential time and resource intensiveness, subjectivity, limited generalizability, social desirability bias, and the complexity of the data analysis.14 Similarly, Svenkerud & Isachsen used face-to-face interviews to question sexually active women’s socio-demographic characteristics and STI knowledge.15
In their studies, Khajehei et al and Zin et al used questionnaires to determine the participants’ knowledge of STIs.16,17 Also, Chukwu et al utilized self-constructed questionnaires to survey 280 medical students at the University of Maiduguri, Borno State.18 Such researchers suffer low response rates, potential social desirability bias, inflexibility in adapting to unexpected replies, language and cultural barriers, incomplete or inaccurate responses, and the impact of poorly worded questions associated with using questionnaires.19
As highlighted previously, women’s knowledge regarding STIs and safe sex practices in Saudi Arabia has not been thoroughly investigated. One study conducted among medical students reported that participants had proper attitudes toward dealing with STIs, which could be explained as due to their knowledge as medical students.6 Previously published studies are limited to specific sample surveys. Therefore, this study aims to investigate and measure the knowledge of sexual health and STIs among women in Saudi Arabia. This study has two major objectives: 1. To measure the level of knowledge of safe sex practices and STIs among women in Saudi Arabia. 2. To outline the associations between sociodemographic factors and the level of knowledge.
Methods
Research Design
This study is a nationwide cross-sectional survey conducted through phone interviews in Saudi Arabia in 2021.
Sampling and Sample Size
A proportional quota sampling technique was employed to acquire an equal distribution of participants stratified by age and gender across the 13 regions of Saudi Arabia. Based on the median age of Saudi adults (36 years) according to the Saudi General Authority for Statistics, two age groups (18–36 and 37+) were adopted, leading to a sample of 26 strata. The data collection system used, ZdataCloud®, integrated eligibility, and sampling modules to control the sample distribution. The SDHNS sample size was calculated based on a medium effect size of 0.25. Participants were selected to empower the sample to compare between quota groups, with an 80% power and a 95% confidence level. Thus, each quota (age /region quota) required 50 participants with a total sample of 1300 participants.
Participant Recruitment
Participant recruitment was limited to Arabic-speaking females, Saudi nationals, and residents aged 18 years and older, generated via random phone number lists provided by the Sharik Association for Research and Studies. Participants were contacted by phone up to three times. If a potential participant did not respond to any of the three calls, a new potential participant’s phone number was generated, given that the substitute participant demonstrates similar demographics (age group, gender, and region of residence). This process was repeated until the targeted quota was fulfilled.
Variables and Outcome Measures
The collected data included sociodemographic information of participants (age, educational level, marital status, and income). The region of Saudi Arabia was added as a variable due to its valuable insights and contribution to a comprehensive understanding of knowledge of sexual health. Sexual health behaviors and outcomes can vary across different regions due to various factors such as cultural norms, socioeconomic conditions, and access to healthcare services. Also, the outcome of the study will help policymakers to make targeted interventions based on each region. Knowledge was assessed through 5 questions pertinent to types, transmission, symptoms, causes, prevention, and cure of STIs, in addition to knowledge of safe sex practices.
Linguistic validation of the survey questions ensured that the questions and answers were understandable enough to generate the intended results. A focus group of 10 participants was asked to discuss and answer the survey questions, and an updated version was tested again with another focus group. Afterward, the electronic version of the survey was developed on the ZDataCloud, and a pilot test with 30 to 50 participants was interviewed by phone to ensure the survey’s accuracy, quality, and data integrity. Per the pilot study results and feedback from the researchers and interviewers, the survey questions were edited further, and an improved version was developed. This process was repeated every time the survey questions were updated and edited.
All questions had to be answered for the responses to be successfully submitted to the database. All data were coded and stored on the ZdataCloud database [12].
Statistical Analysis
The data was analyzed using SPSS software. Frequency and percentage were used for presenting categorical data. Knowledge score was calculated using the sum function, and the cut-off points for categorizing participants as knowledgeable and low in knowledge were calculated using 75 percentiles. The association of knowledge with participants’ demographic characteristics was calculated using bivariate analysis (chi-square). Multivariable analysis using logistic regression was used to determine the determinants of sexual health and sexually transmitted diseases among women in Saudi Arabia.
Ethical Considerations
The Sharik Association for Health Research Ethics Committee approved this research project (Approval IRB number 01–2022.) in alignment with the National Research Ethics Regulations. Participants’ consent was obtained verbally during the phone interview and was documented on the data collection system. The research complies with the Declaration of Helsinki.
Results
Participant Characteristics
A total of 1660 women were contacted through phone in 2021, 1334 women agreed to participate in the research during the three weeks of data collection (response rate 80.36). As shown in Table 1, Most of the study participants were Saudi nationals (98.4%). More than half of them were between the ages of 20–39 years old (58%). Most of the participants were from the Northern and Southern regions of Saudi Arabia (30.9% and 30.9%, respectively). Regarding marital status, a slightly higher percentage of participants fell in the Married category (55.5%). Regarding education, 54.4% of the participants had a bachelor’s degree or higher. Around 28% of participants had an average family income ranging between 6000 SAR and 10,999 SAR.
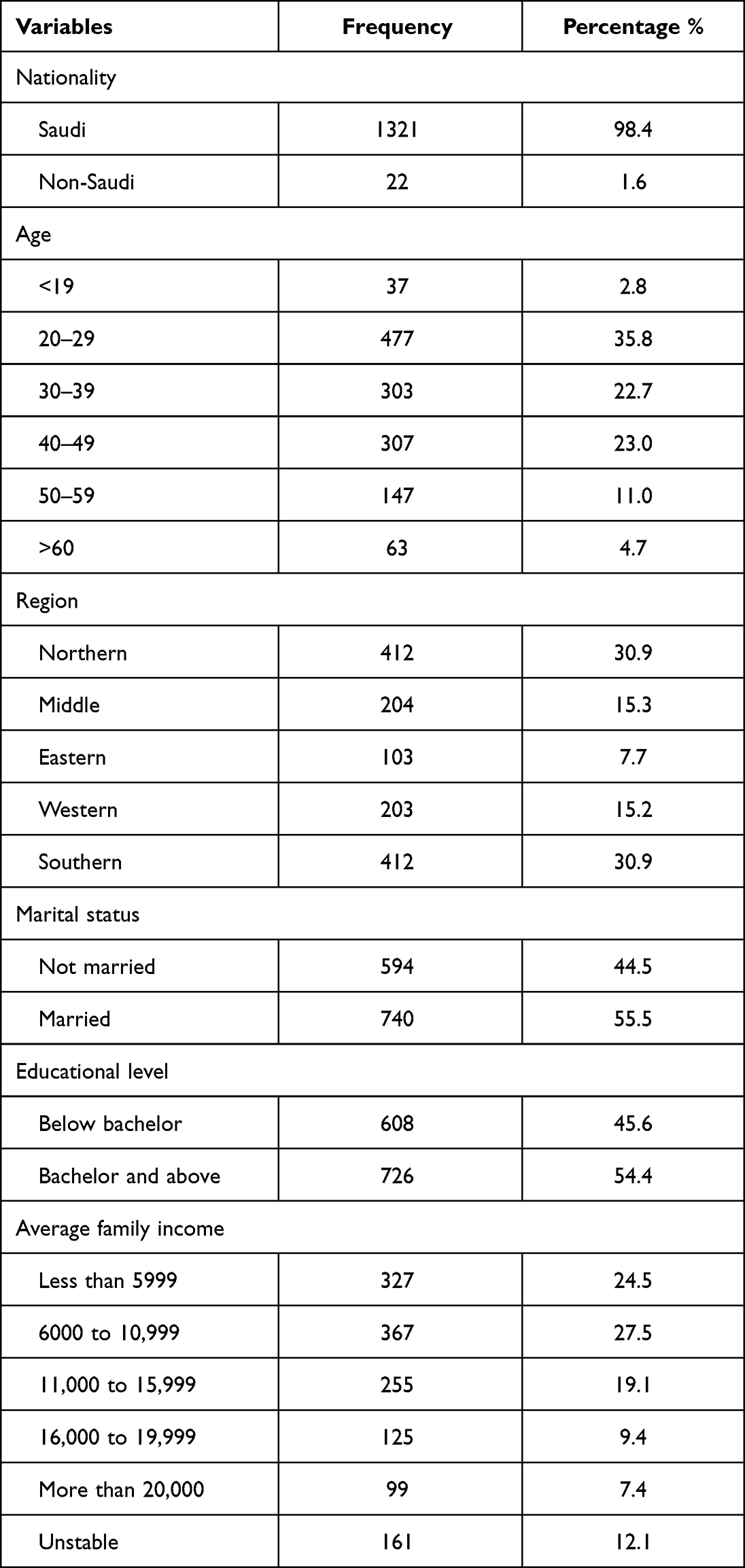 |
Table 1 Demographic Characteristics of Study Participants |
Knowledge of Participants Towards Sexual Health and Sexually Transmitted Diseases
This domain assessed knowledge of the types, transmission, symptoms, causes, prevention, and cure of STIs. As shown in Table 2, most of the participants were knowledgeable of HIV (77.5%), Syphilis (62.4%), Gonorrhea (43.9%), and Genital herpes (42.1%) as STIs. On the other hand, a majority of the participants were not aware that Chlamydia (15.6%), Pubic lice and Scabies (22.4%), Genital warts (23.9%), Papillomavirus infection (26.1%), Genital ulcer (26.5%), Trichomoniasis (27.5%), Chancroid (29.6%) were types of STIs. A significant percentage of participants (84%) knew that STIs were transmittable and that treating the infected individual, as well as the partner, was necessary (92.8%).
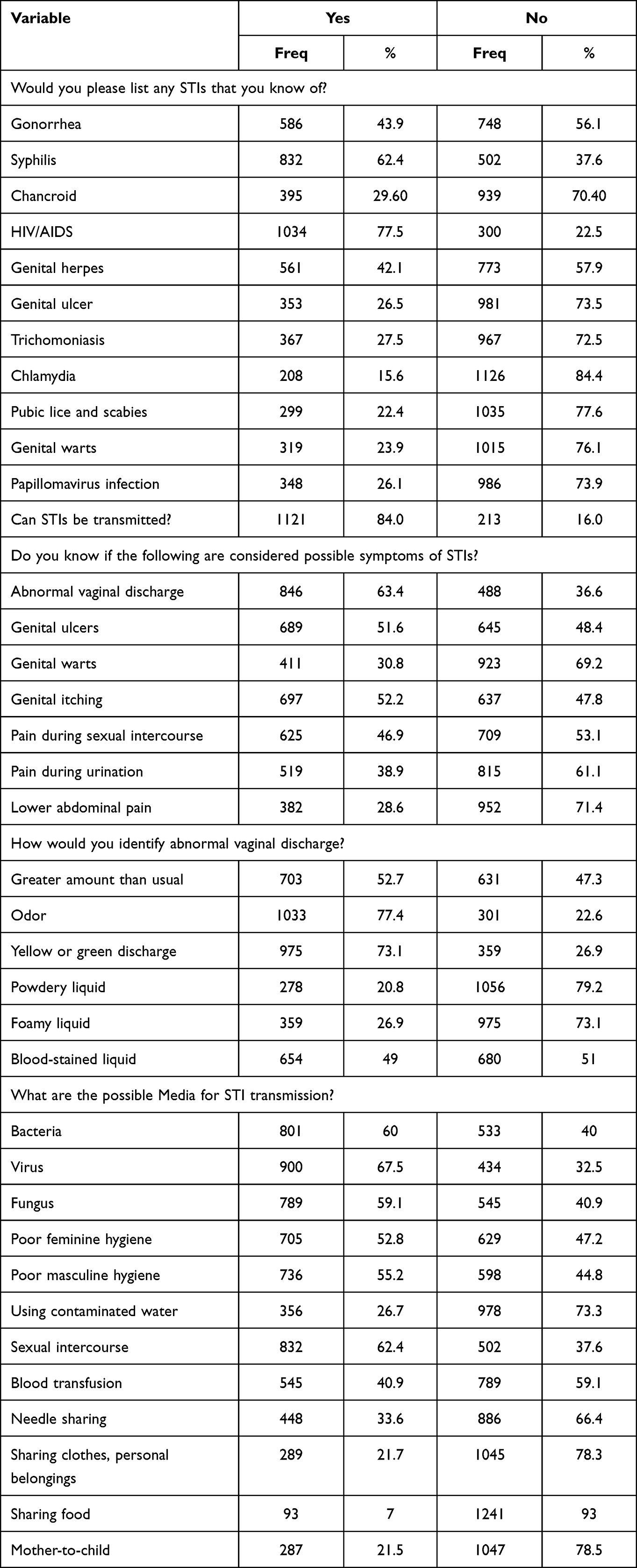 |
Table 2 Frequency Distribution of Participants’ Response to Knowledge of Sexual Health and Sexually Transmitted Diseases |
Regarding the symptoms of STIs, more than half of the participants recognized abnormal vaginal discharge (63.4%), genital ulcers (51.6%), and genital itching (52.2%) as key STI symptoms. Almost half of the participants recognized pain during sexual intercourse as a key symptom (46.9%), and less than half recognized genital warts, pain during urination, and lower abdominal pain as key symptoms (30.8%, 38.9%, 28.6%, respectively). Furthermore, most participants failed to identify vaginal discharge presenting powdery or foamy liquid as an abnormality (20.8%, and 26.9%, respectively). However, more than half of the participants recognized excessive vaginal discharge, odorous vaginal discharge, and green or yellow discharge as abnormal (52.7%, 77.4%, and 73.1%, respectively).
A sweeping majority of participants did not recognize meal sharing as a possible mode for STI transmission (93%). Mother-to-child transmission through sharing clothes and personal belongings was also unidentified by 78% and 78.3% of participants, respectively. On the other hand, most participants recognized that viruses, sexual intercourse, and fungus were possible media for STI transmission. Most participants (73.6%) believed that some types of STIs could be cured.
Participants’ knowledge of safe sex practices was measured through five questions. The level of knowledge of safe sex practices was generally acceptable, except for the use of condoms as a preventive measure for STI/HIV transmission, which was correctly stated by only 42.4% of the participants.
The Knowledge Scoring
The calculation of the knowledge score ranged between (0–44). The cut-off points for categorizing participants as knowledgeable and low in knowledge were calculated using 75 percentiles. Low-knowledge participants had a score below 28, whereas knowledgeable participants had a score of 28 and above.
Factors Associated with Participants’ Knowledge Level of Sexual Health and Sexually Transmitted Infections
Participants’, region, educational level, and family income showed significant associations among the variables examined in the bi-variate analysis. Variables with P-value <0.05 were considered for the multivariable logistic analysis, as shown in Table 3. Age were also added due to it practical significant. In the multivariable logistic analysis, participants aged between 20 and 29 had 2.09 times higher knowledge than those aged >60 (CI 1.03–4.23). Participants in the Eastern Region had 1.93 times higher knowledge than those in the Southern Region (CI 1.23–3.04). In terms of education, participants with less than a bachelor’s degree had 0.65 times lower knowledge than those with a bachelor’s degree and above (CI 0.51–0.84). Regarding income, participants with an average of 16,000 SAR to 19,999 SAR had 2.51 times higher knowledge than participants with unstable monthly income (CI 1.48–4.26), as shown in Table 4.
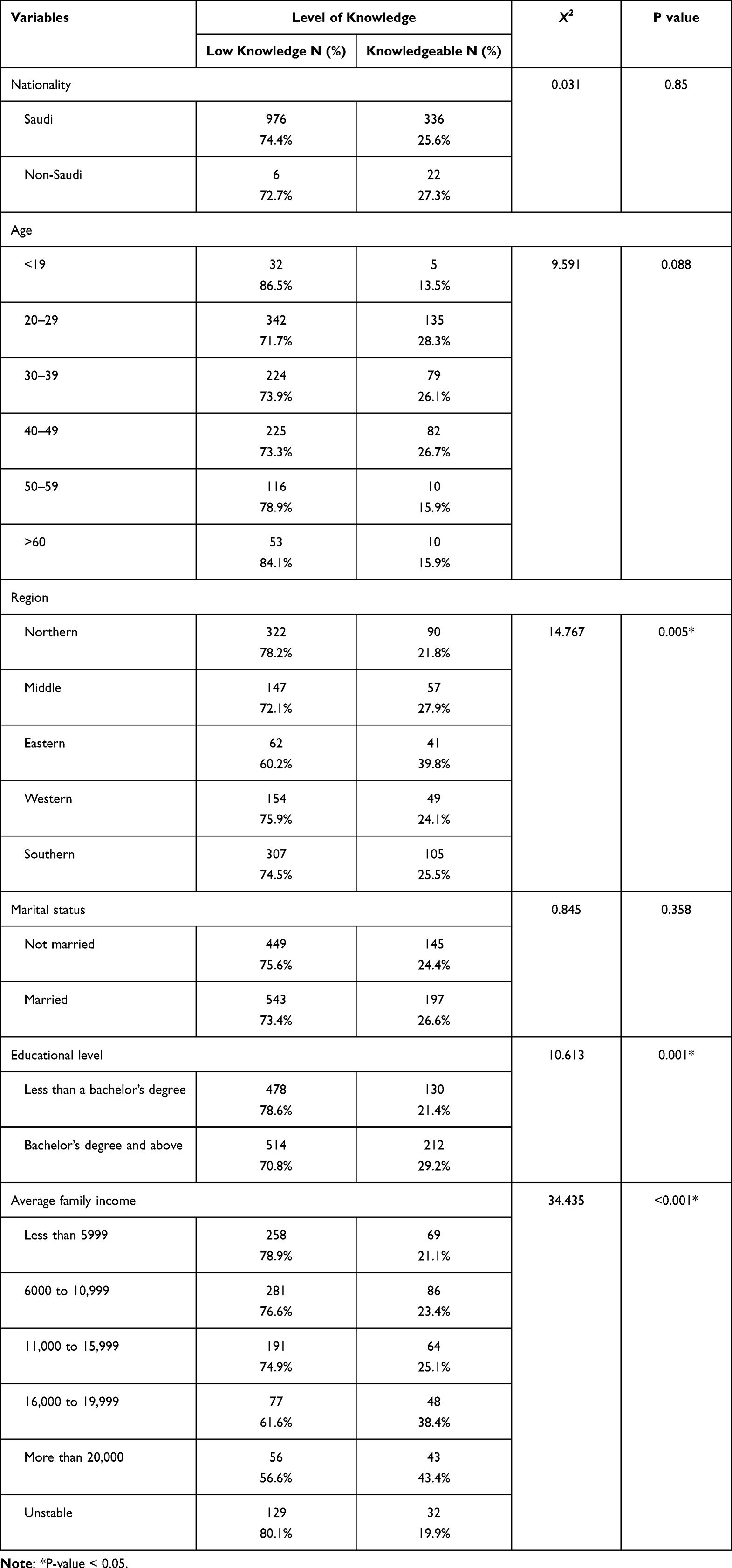 |
Table 3 Association of Knowledge with Participants’ Demographic Characteristics |
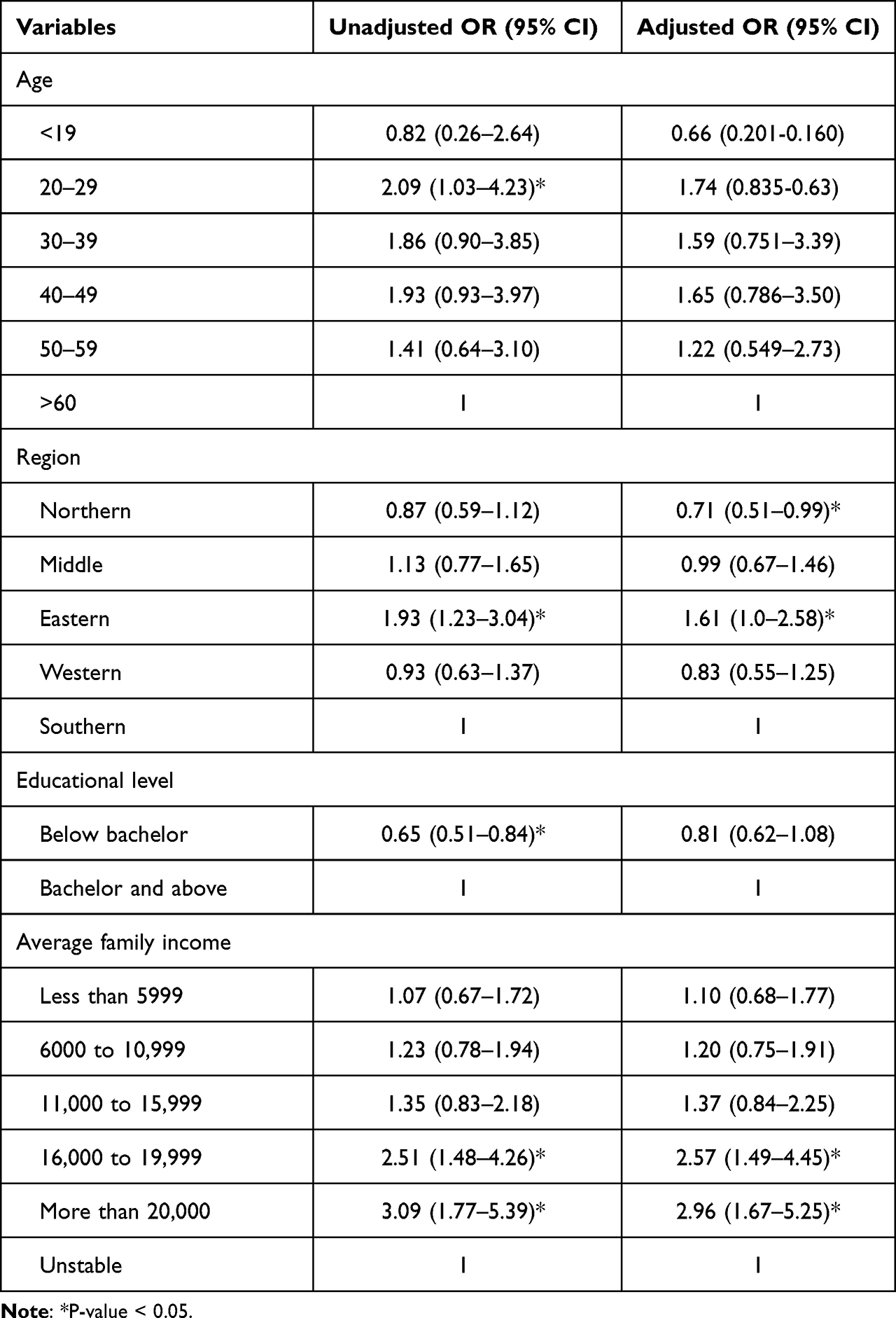 |
Table 4 Determinants of Sexual Health and Sexually Transmitted Diseases Among Women in Saudi Arabia |
Discussion
The findings of this study on the knowledge and determinants of sexual health and sexually transmitted diseases among women in Saudi Arabia suggested that only a quarter of the respondents (25.6%) were considered knowledgeable. Although the overall level of knowledge was considerably low, a significant proportion of this lack of knowledge is referred to the lack of “technical” knowledge pertinent to the types of STIs (only 2 STIs were correctly identified by more than half of the participants), and the causes and modes of transmission, where only 7 out of 12 were correctly identified by more than half of the participants. The poor knowledge of the role needle sharing plays in STI transmission (33.6%), has been confirmed by another study titled Sexually Transmitted Infections in Saudi Arabia,20 in which the author posits that health promotion in terms of blood-borne infection prevention is not sufficiently carried out in the conservative Saudi society, as much as it may be in other countries around the world. Regarding STI symptoms, 4 out of 7 symptoms were correctly identified by more than half of the participants. Similarly, a systematic review based on eighteen studies of 13 Muslim countries confirmed the findings of this study in terms of the poor knowledge of STI signs and symptoms, which may be due to the diminished openness in offering and receiving information pertaining to sexual practices.7,21
On the other hand, a sweeping majority understood the importance of treating partners (92.8%) and were aware that cures are available for STIs (73.6%), and more importantly, most of the participants demonstrated knowledge of 4 out of 5 safe sex practices. The role of condom use in the prevention of STIs and HIV scored the lowest level of knowledge among the five sex-safe practices, a finding which once more has been confirmed by Madani, where the lack of promotion regarding safe sex practices was associated with conservatism that characterizes the Saudi culture.20 This was also confirmed by a recent study by Alsubaie, (2020); it was found that 64.3% of the study participants had poor knowledge of HIV and STIs.22
The results of this study also revealed that participants with lower levels of education had less knowledge of sexually transmitted diseases compared to college degree holders (21.4% compared to 29.2%). This association between the level of education and knowledge of STIs is mirrored in another study by,11 demonstrating the prevalence of STIs among less or non-educated individuals. Synthesis of the findings of both studies confirms that less educated individuals constitute a high-risk group, since STIs are more prevalent among them. Identifying high-risk groups is one of the main opportunities presented by this study to introduce calibrated and focused health promotion programs.
Moreover, the findings of this study revealed that the lowest knowledge score for safe sex practices was attributed to the role of condom use in preventing HIV and STIs (42.4%). This deficiency is particularly worrying from a public health perspective, especially given that other studies have confirmed that STIs are higher among non-condom users.11 According to WHO: Global Strategy for the Prevention and Control of Sexually Transmitted Infection: 2006–2015: Breaking the Chain of Transmission, “condom use is considered the single, most efficient, available means to reduce the sexual transmission of both HIV and STI”. Hence, focusing health promotion programs on the advantages of condom use and how such use is effective in reducing HIV and STI contraction should be a focus for public health officials, especially among high-risk groups.
Another finding in this study is the diminished level of knowledge of sexually transmitted diseases among unmarried women (75.6%).23 This contrast in the level of knowledge associated with the female’s marital status has been confirmed by another study conducted among women residing in North rural Vietnam.24 Those findings support calibrated public health efforts in identifying high-risk groups.
Significant associations were found between knowledge and age, region, educational level, and family income. In the multivariable analysis, participants aged 20–29 had higher knowledge compared to those aged >60. Participants in the Eastern Region had higher knowledge than those in the Southern Region. Participants with less than a bachelor’s degree had lower knowledge than those with a bachelor’s degree or higher. Participants earning an average of 16,000 to 19,999 SR had higher knowledge than those with unstable monthly income.
Conclusion
In conclusion, this study provides valuable information on the knowledge and determinants of sexual health and STDs among women in Saudi Arabia. One of the main strengths of this study, which could also be viewed from a different perspective as a limitation, is the fact that the study focuses on identifying the level of participants’ knowledge. This is a strength because it enables pinpointing the shortages and gaps in knowledge in terms of different aspects pertinent to sexual health. However, an ensuant limitation may be the lack of deep focus on attitudes and practices. Hence, further studies are needed to address this particular limitation. Another main strength of this research is the usability of the findings in creating targeted health promotion campaigns that are aligned with the clearly identified gaps in knowledge. A future study focused on male knowledge, attitudes, and practices as pertinent to sexual health may be helpful in terms of creating a reference point for comparing and contrasting with the female population in Saudi Arabia.
The study’s findings indicate that women’s general understanding of sexual health and STDs in Saudi Arabia is quite low. The main causes appear to be a lack of knowledge and awareness about the different types of STIs, the means of transmission, and the identification of symptoms. However, many of the participants demonstrated knowledge of the importance of treating partners, the existence of cures, and safe sex practices. Using condoms in STI and HIV prevention was found to have the lowest knowledge score. Knowledge levels were shown to be correlated with educational levels and marital status. These findings demonstrate the necessity for calibrated and targeted health promotion initiatives, particularly those aimed at high-risk populations. Regarding preventive measures and health promotion efforts, public health officials need to focus on raising awareness regarding safe sex practices, especially the role of condom use in reducing HIV and STI transmission.
Funding
This work was funded by Informed Decision-Making IDM - Saudi Arabia [01082023].
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Sexual health; 2006. Available from: https://www.who.int/westernpacific/health-topics/sexual-health.
2. IAMAT. Saudi Arabia: sexually Transmitted Infections | IAMAT; 2020. Available from: https://www.iamat.org/country/saudi-arabia/risk/sexually-transmitted-infections.
3. Avert. Sexually transmitted infections (STI). Avert; 2020. Available from: https://www.avert.org/sex-stis/sexually-transmitted-infections.
4. Workowski K, Bolan G Sexually transmitted diseases treatment guidelines; 2015. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htm.
5. World Health Organization. Sexually transmitted infections (STIs); 2019. Available from:
6. Abuabat A, Alfarhan A, Alahmari R, et al. Knowledge and attitudes of sexually transmitted infections among medical students in Riyadh, Saudi Arabia. Int J Med Dev Ctries. 2020:1. doi:10.24911/IJMDC.51-1588598905
7. Alomair N, Alageel S, Davies N, Bailey JV. Sexually transmitted infection knowledge and attitudes among Muslim women worldwide: a systematic review. Sex Reprod Health Matt. 2020;28(1):1731296. doi:10.1080/26410397.2020.1731296
8. El-Tholoth HS, Alqahtani FD, Aljabri AA, et al. Knowledge and attitude about sexually transmitted diseases among youth in Saudi Arabia. Urol Ann. 2018;10(2):198. doi:10.4103/UA.UA_14_17
9. Albanghali MA, Othman BA. A cross-sectional study on the knowledge of sexually transmitted diseases among young adults living in Albaha, Saudi Arabia. Int J Environ Res Public Health. 2020;17(6):1872. doi:10.3390/ijerph17061872
10. Balbeesi A, Mohizea S. Knowledge and misconceptions of Saudi women about sexually transmitted infections. J Egypt Public Health Assoc. 2017;92(4):235–239. doi:10.21608/EPX.2018.22045
11. Filemban SM, Yasein YA, Abdalla MHH, Al-Hakeem R, Al-Tawfiq JA, Memish ZA. Prevalence and behavioral risk factors for STIs/HIV among attendees of the Ministry of Health hospitals in Saudi Arabia. J Infect Dev Ctries. 2015;9(04):402–408. doi:10.3855/jidc.5964
12. Raheel H, Mahmood MA, BinSaeed A. Sexual practices of young educated men: implications for further research and health education in Kingdom of Saudi Arabia (KSA). J Public Health Oxf Engl. 2013;35(1):21–26. doi:10.1093/pubmed/fds055
13. Ivanova O, Rai M, Mlahagwa W, et al. A cross-sectional mixed-methods study of sexual and reproductive health knowledge, experiences and access to services among refugee adolescent girls in the Nakivale refugee settlement, Uganda. Reprod Health. 2019;16(1):35. doi:10.1186/s12978-019-0698-5
14. Amiri P, Asghari G, Sadrosadat H, et al. Psychometric properties of a developed questionnaire to assess knowledge, attitude and practice regarding vitamin D (D-KAP-38). Nutrients. 2019;9(5):471. doi:10.3390/nu9050471
15. Svenkerud BA, Isachsen K Knowledge of sexually transmitted infections among women attending primary health care clinics in Moshi, Tanzania; 2011.
16. Khajehei M, Ziyadlou S, Ghanizadeh A. Knowledge of and attitudes towards sexual and reproductive health in adults in Shiraz: a need for further education. East Mediterr Health J. 2013;19(12):982–989. doi:10.26719/2013.19.12.982
17. Zin NM, Ishak I, Manoharan K. Knowledge, attitude and practice towards sexually transmitted diseases amongst the inmates of women shelters homes at Klang Valley. BMC Public Health. 2019;19(Suppl 4):639. doi:10.1186/s12889-019-6863-5
18. Chukwu EO, Iornengen EM, Fiase TM, Chia T, Haruna H, Hamina D Knowledge and practice of safe sex among students of College | 15878; 2017. Available from: https://www.interesjournals.org/abstract/knowledge-and-practice-of-safe-sex-among-students-of-college-of-medical-sciences-university-of-maiduguri-borno-state-nig-15878.html.
19. Afolayan MS, Oniyinde OA. Interviews and questionnaires as legal research instruments. J Law Policy Glob. 2019;83:51.
20. Madani TA. Sexually transmitted infections in Saudi Arabia. BMC Infect Dis. 2006;6(1):3. doi:10.1186/1471-2334-6-3
21. Memish ZA, Filemban SM, Al-Hakeem RF, Hassan MH, Al-Tawfiq JA. Sexually transmitted infections case notification rates in the Kingdom of Saudi Arabia, 2005–2012. J Infect Dev Ctries. 2016;10(8):884–887. doi:10.3855/jidc.7020
22. Alsubaie ASR. Examining HIV and STIs related knowledge among male adolescents in Saudi Arabia. Open AIDS J. 2020;14(1):27–34. doi:10.2174/1874613602014010027
23. Lewis DA, Latif AS, Ndowa F. WHO global strategy for the prevention and control of sexually transmitted infections: time for action. Sex Transm Infect. 2007;83(7):508. doi:10.1136/sti.2007.028142
24. Lan PT, Lundborg CS, Mogren I, Phuc HD, Chuc NTK. Lack of knowledge about sexually transmitted infections among women in North rural Vietnam. BMC Infect Dis. 2009;9(1):85. doi:10.1186/1471-2334-9-85
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.