Back to Journals » Journal of Inflammation Research » Volume 19
The Joint Effect of C-Reactive Protein and Fibrinogen in Predicting Intracranial Hypertension of Cerebral Venous Sinus Thrombosis Patients
Authors Xu Y, Yan J, Lu M, Huang Z, Ni J, Zhang X
Received 7 August 2025
Accepted for publication 27 January 2026
Published 7 February 2026 Volume 2026:19 554496
DOI https://doi.org/10.2147/JIR.S554496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dharmappa Krishnappa
Yingying Xu,1,* Jiahui Yan,1,* Manli Lu,1 Zhichao Huang,1 Jianqiang Ni,2 Xia Zhang1
1Department of Neurology and Clinical Research Center of Neurological Disease, the Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Department of Neurology, the First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Zhang, Department of Neurology and Clinical Research Center of Neurological Disease, the Second Affiliated Hospital of Soochow University, No. 1055, Sanxiang Road, Suzhou, Jiangsu, 215004, People’s Republic of China, Tel +86 512 67784786, Email [email protected] Jianqiang Ni, Department of Neurology, the First Affiliated Hospital of Soochow University, No. 899, Pinghai Road, Suzhou, Jiangsu, 215031, People’s Republic of China, Tel +86 512 67780327, Email [email protected]
Purpose: Intracranial hypertension is the most common symptom of cerebral venous sinus thrombosis. Recent studies have indicated that both the coagulation and inflammation systems play roles in the occurrence and development of cerebral venous sinus thrombosis. Therefore, this study aimed to explore the individual and combined effects of coagulation-related biomarker [fibrinogen (FIB)] and inflammation-related biomarker [C-reactive Protein (CRP)] in predicting intracranial hypertension.
Patients and Methods: We retrospectively and consecutively included 157 cerebral venous sinus thrombosis patients, who were divided into four groups according to the cut-offs of CRP and FIB by the receiver operating characteristics curves: low CRP low FIB, high CRP low FIB, low CRP high FIB and high CRP high FIB. Logistic regression models were used to compute the odds ratios and 95% confidence intervals for intracranial hypertension across the four subgroups.
Results: Cerebral venous sinus thrombosis patients with intracranial hypertension had much higher CRP and FIB levels than those without intracranial hypertension did (all P< 0.05). After adjusted by gender, age, modified Rankin scale, duration, headache, seizure, smoking, history of thrombosis and other risk factors, white blood cell, systemic immune-inflammation index and estimated glomerular filtration rate, patients in high CRP high FIB group were 5.286 (95% CI: 2.04– 13.701, P=0.001) times more frequent to experience intracranial hypertension than those in low CRP low FIB group did. The addition of CRP and FIB to the basic model significantly improved discriminatory power for intracranial hypertension, as area under the curve increased from 0.692 (95% CI: 0.609– 0.775, P< 0.001) to 0.767 (95% CI: 0.692– 0.843, P< 0.001).
Conclusion: Higher levels of both CRP and FIB are associated with an increased risk of intracranial hypertension following cerebral venous sinus thrombosis. The combination of CRP and FIB has a better predictive ability for intracranial hypertension in patients with cerebral venous sinus thrombosis than either CRP or FIB alone.
Keywords: inflammation biomarker, coagulation factor, cerebrovascular disease, joint effect
Introduction
Cerebral venous sinus thrombosis (CVST) is a special cerebrovascular disease caused by thrombosis of the dural sinuses and/or intracranial veins, with an estimated annual incidence of 1.3 to 3.16 cases per 100,000 adults.1,2 CVST is a rare yet potentially life-threatening cerebrovascular disorder, characterized by four distinct clinical phenotypes that correlate closely with the location and extent of venous sinus occlusion-an association critical for timely clinical recognition and early intervention. The most prevalent phenotype is isolated intracranial hypertension (IH), typically secondary to occlusion of major cerebrospinal fluid (CSF)-resorbing sinuses. Hallmark features include persistent headache, papilledema, and elevated opening pressure on lumbar puncture, with the notable absence of focal neurological deficits. By contrast, focal neurological syndrome arises from impaired regional venous drainage, manifesting as corresponding focal deficits (eg, hemiparesis) often accompanied by headache or seizures. Diffuse encephalopathy, a life-threatening subtype induced by extensive multi-sinus occlusion, is defined by altered consciousness and carries a high risk of cerebral herniation. Finally, cavernous sinus syndrome represents a rare, location-specific phenotype, presenting with a triad of ophthalmoplegia, trigeminal nerve dysfunction, and proptosis. Among these, IH is the most common symptom, which affected 28% to 83% of selected CVST patients.3–5 IH leads to headache, emesis, and permanent visual impairment, obviously aggravating the condition of CVST patients.3 Thus, the prompt identification of IH seems important. Nowadays, lumbar puncture remains the most common-used method for measurement of the open pressure of CSF to detect IH, which can be challenged by the use of anticoagulants and disease severity with invasiveness.6 Therefore, rapid and noninvasive assessment of IH is urgently needed to facilitate early identification and timely intervention of high-risk CVST patients for better prognosis.
CVST could be caused by infection or nonspecific inflammation of the head and face or other sites or non-inflammatory factors such as hypercoagulability. The association of inflammation biomarkers with diagnosis, severity, and poor prognosis of CVST has already been reported, especially C-reactive protein (CRP). Increased baseline CRP level was reported to be associated with unfavorable functional outcome at day 90 of CVST patients.7 Fibrinogen (FIB) is a coagulation factor in plasma, which has been revealed to be closely related to inflammation reaction.8 Pathological FIB elevation demonstrates a hypercoagulable state with the increased possibility of thrombosis. Previous reports have shown that a high level of FIB was strongly correlated with CVST progression and severity.9 Meng et al showed 73.5% of CVST patients had FIB elevation and the sensitivity and specificity of FIB for diagnosis of CVST were 73.5% and 83.9%, respectively.8 Zhang et al explored the dynamic changes of CRP and FIB in 82 patients with progressive cerebral infarction and 186 with non-progressive disease. Results showed that in the progressive group, CRP levels peaked on day 3 then declined but remained significantly higher than in the non-progressive group (P<0.01), while FIB levels were consistently elevated on days 3, 7 and 14 (P<0.01), indicating dynamic monitoring of these biomarkers may facilitate early identification and timely treatment of progressive ischemic strokes.10 A prospective study demonstrated that elevated FIB levels show a trend towards association with poor prognosis in ischemic cerebrovascular disease and their impact on prognosis may be indirectly mediated through the correlation with CRP.11 However, their single or joint effect on IH of CVST patients has not been explored yet. For traumatic brain injury (TBI) patients, both CRP and FIB have been identified as a robust indicator of IH.12 Thus, the present study aimed to investigate the single and joint effect of CRP and FIB in predicting IH of CVST patients.
Materials and Methods
Study Design and Participants
Patients with a first episode of CVST from the Department of Neurology at the First and Second Affiliated Hospital of Soochow University between January 2011 and June 2024 (Figure 1) were retrospectively and consecutively enrolled. Those aged >14 years with a confirmed diagnosis of CVST by magnetic resonance imaging (MRI) combined with magnetic resonance venography (MRV), computed tomography venography (CTV) or digital subtraction angiography (DSA), following established diagnostic criteria were included.13 Lumbar puncture and all laboratory tests were done before any treatment and valid information was available. Prior to lumbar puncture, written informed consent was obtained from each patient or their legal guardians. Participants without complete data of CRP, FIB and lumbar puncture were excluded. Moreover, those with inflammatory diseases like pneumonia were ineligible. All enrolled patients signed written informed consent. This study involved a mixture of adult and minor participants, and for minors, consent was obtained from the parents/legal guardians. The study protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Soochow University, China (JD-HG-2024-027) and conducted in accordance with the Declaration of Helsinki. The data that support the findings of this study are available from the corresponding author upon reasonable request.
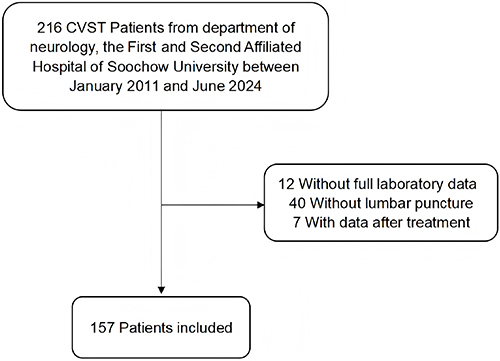 |
Figure 1 Patients’ flow chart. |
Data Acquisition and Outcome Assessment
Data of all participants were standardly collected including demographic characteristics, symptoms, disease duration, risk factors of CVST such as history of stroke and venous thrombosis disease, medication history (antiplatelet drugs, anticoagulation drugs, estrogen-progesterone, puerperium, oral contraceptives), sex-specific factors (pregnancy), hereditary thrombophilia factors (protein C, S, or antithrombin III deficiency). Intracranial pressure (ICP) was presented by the open pressure of CSF through lumbar puncture. The patient was positioned in the left lateral decubitus with flexed knees, hips, and neck, hands clasped around the knees to draw them tightly against the abdomen. The primary puncture site was the intersection of the bilateral iliac crest line and posterior midline, preferring the L3-L4 interspinous space (adjustable to adjacent spaces based on body habitus). After successful puncture, the stylet was slowly withdrawn, a manometer attached, and the patient instructed to extend both lower extremities.5 CSF pressure was recorded once the manometer fluid level stabilized with slight respiratory fluctuations. An ICP of higher than 250 mmH2O was defined as IH.14
Blood samples were collected within 24 hours of hospital admission before any treatment. CRP was measured by the Mindray CRP-M100 specific protein immune analyzer (Mindray CRP-M100, Shenzhen, China) using immunity transmission turbidity. FIB was measured with Sysmex CA-1500 automatic coagulation analyzer (Sysmex CA-1500, Tokyo, Japan) by the von Clauss method. The estimated glomerular filtration rate (eGFR) was calculated by applying the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation with an adjusted coefficient of 1.1 for Chinese populations: 141 *min (CR/к, 1) a *max (CR/к, 1)-1.209*0.993Age*1.018[if female]*1.1, к is 0.7 for females and 0.9 for males, а is −0.329 for females and −0.411 for males, min indicates the minimum of CR/к or 1, and max indicates the maximum of CR/к or 1.15
Statistical Analysis
All patients were divided into two groups according to ICP: CVST with normal ICP (CVST-IH) and CVST with IH (CVST+IH). The Shapiro–Wilk test was used to test normality of continuous variables. The baseline characteristics of continuous variables were presented as medians with interquartile ranges (IQRs) and were compared using Mann–Whitney U-test or Kruskal–Wallis test. The categorical variables were expressed as a percentage, and compared using Chi-square test. We further examined the single and joint effect of CRP and FIB. Receiver operating characteristic (ROC) curve analysis was employed to evaluate FIB and CRP as predictors of intracranial hypertension in patients with CVST. The area under the curve (AUC) and corresponding 95% confidence intervals (CIs) were calculated to quantify predictive performance. Given the clinical imperative to minimize both false-negative and false-positive results, the maximum Youden’s Index method was prioritized for determining the optimal cut-off values, as it achieves a balanced trade-off between sensitivity and specificity. The optimal cut-off values were identified as 5.55 g/L for CRP and 3.44 mg/L for FIB. The patients were categorized into four groups: low CRP and low FIB (LCLF), high CRP and low FIB (HCLF), low CRP and high FIB (LCHF), and high CRP and high FIB (HCHF). Logistic regression models were used to compute the odds ratios (ORs) and 95% CIs of IH. Gender, age, modified rankin scale (mRS), duration, headache, seizure, smoking, history of thrombosis and others, white blood cell (WBC), Systemic Immune-Inflammation Index (SII), and eGFR were included in the multivariable-adjusted model. ROC curve analysis was used to evaluate the predictive ability of CRP and FIB for IH in CVST patients.
All P values were 2-tailed, and a significance level of 0.05 was used. Statistical analysis was conducted using SPSS 26.0 statistical software (IBM Corp., NY)).
Results
Clinical Characteristics Between CVT Patients with and without IH
A total of 157 patients (78 men and 79 women) were finally analyzed with a median age of 37 years (IQR, 27–48) and disease duration from the onset was 7 days (IQR, 4–17). The median baseline mRS score was 2 (IQR, 2–3). And the median baseline CSF pressure was 220 mmH2O (IQR, 140–280). Sixty-one patients (38.9%) had IH. One hundred and twenty-one patients (77%) complained of headache and 17 patients (10.8%) had seizures. In addition, 20 patients (12.7%) had a history of thrombosis and 18 patients (11.4%) had other risk factors. Among them, age, disease duration, headache/epilepsy incidence, comorbid risk factors, smoking history, and medication history were comparable between the two groups. The proportion of male and the mRS were higher in CVST+IH group (all P<0.05). Patients in CVST+IH group had much higher CRP and FIB levels than those in CVST-IH group did (all P<0.05) (Table 1). However, the number of WBC, lymphocyte, monocye, neutrophils, SII, and eGFR between the two groups showed no significant difference (all P>0.05) (Table 1).
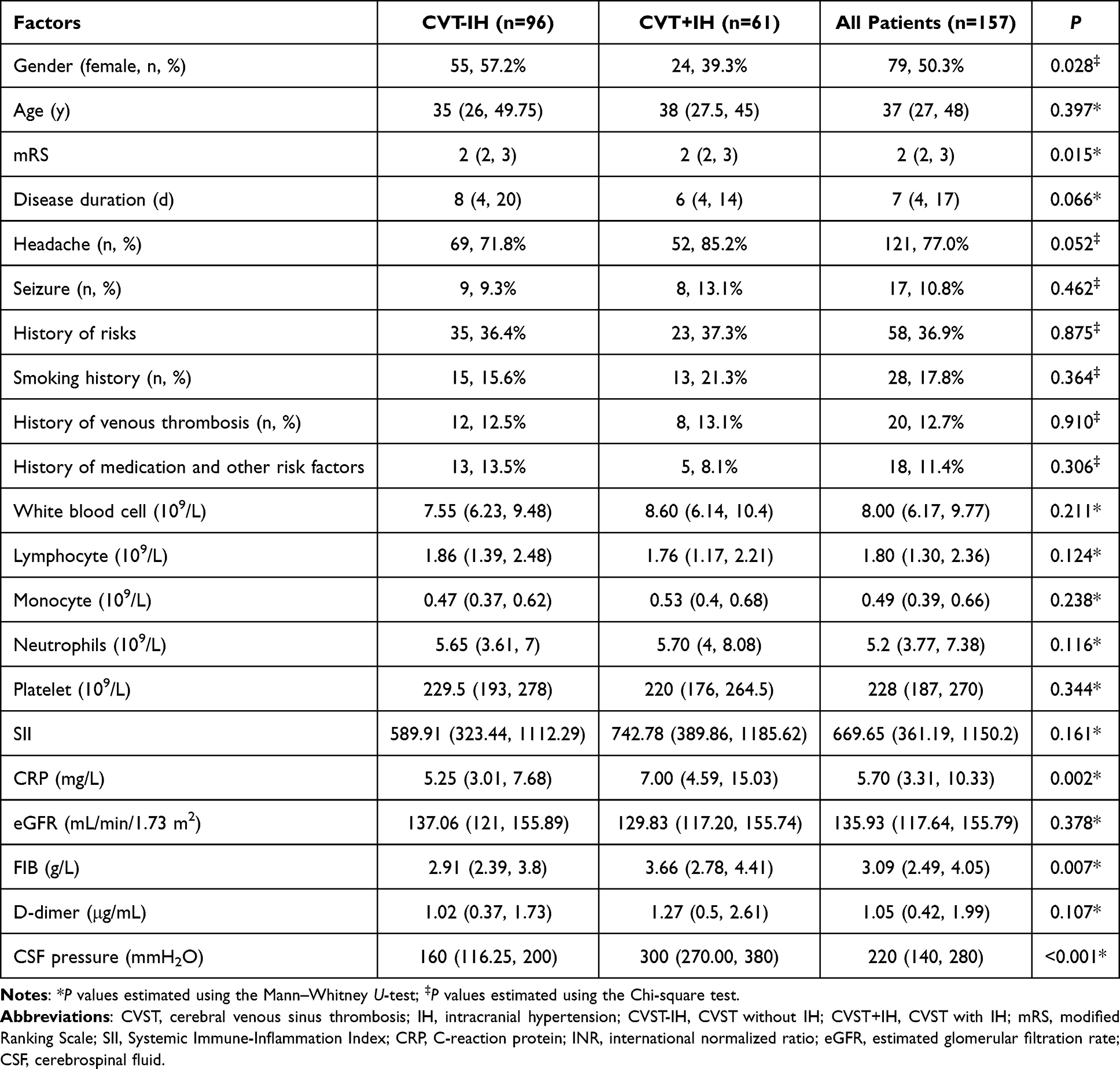 |
Table 1 Demographic Variables and Clinical Assessments Between CVST Patients with and Without IH |
Independently Predictive Significance for IH: Role of CRP and FIB
After adjusting for gender, age, mRS, duration, headache, seizure, smoking, history of thrombosis and other risk factors, WBC, SII, eGFR, both high CRP and FIB levels were associated with IH. The multivariable adjusted OR of CRP for IH was 1.334 (95% CI: 1–1.778, P=0.002) and FIB was 1.334 (95% CI: 1–1.778, P=0.050), respectively (Table 2). Patients with CRP>5.55mg/L or FIB>3.44g/L were more likely to experience IH with sensitivity and specificity of 68.9% and 59.4%, or 59.0% and 69.8%, respectively (Figure 2).
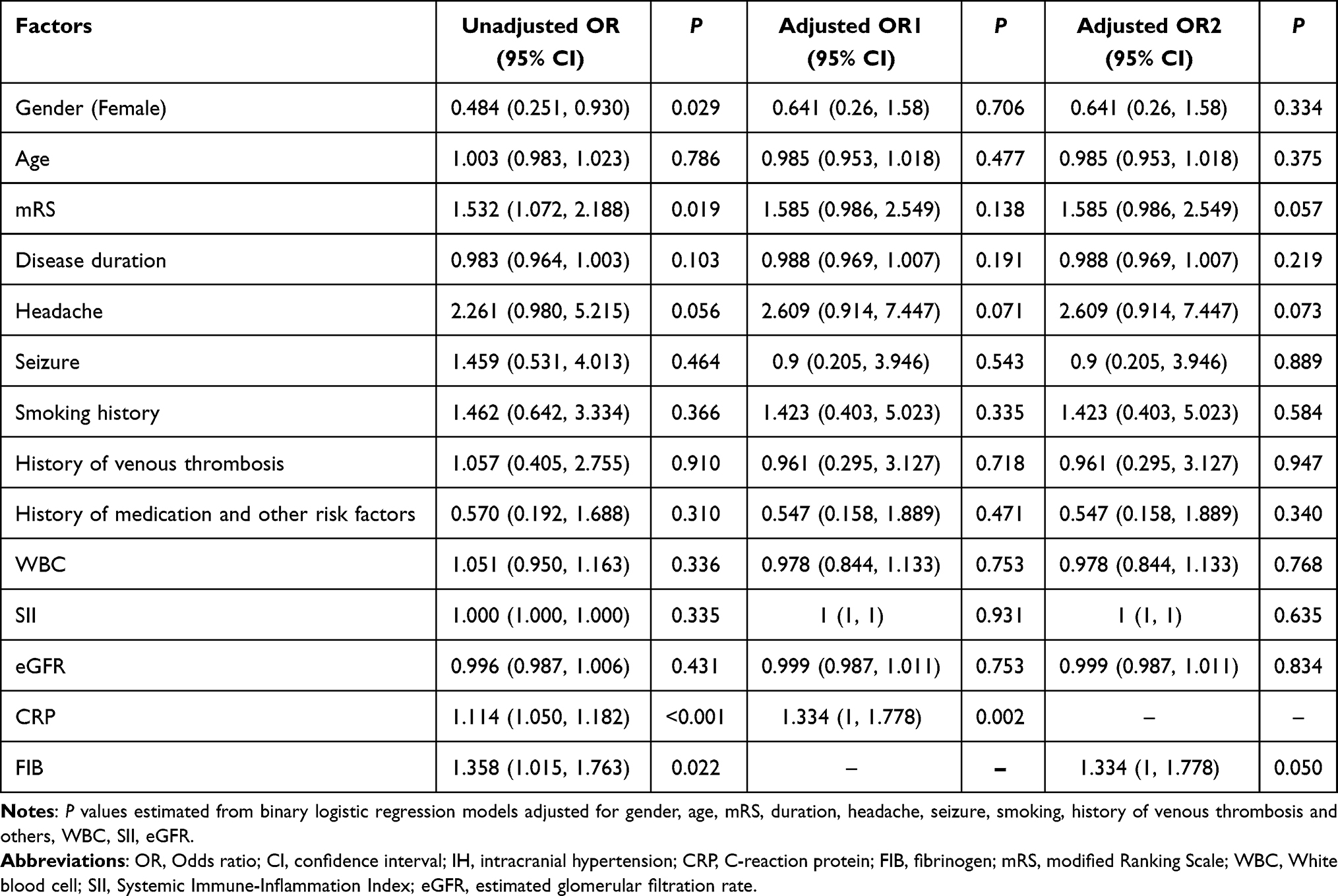 |
Table 2 ORs and 95% CIs for IH According to CRP and FIB Separately |
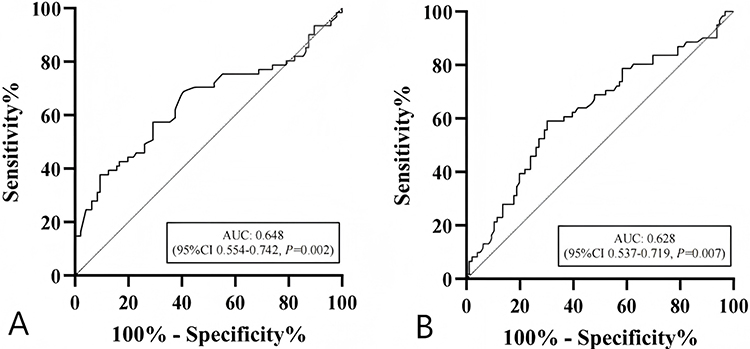 |
Figure 2 Cut-off value of biomarkers: (A) CRP; (B) FIB. Abbreviations: AUC, area under curve; CRP, C-reaction protein; FIB, fibrinogen. |
The Combined Predictive Ability of CRP and FIB for IH
We further assessed the joint predictive value of CRP and FIB for IH. Patients were categorized into four groups according to the cutoffs of CRP and FIB by ROC curves: LCLF, HCLF, LCHF and HCHF groups. Table 3 shows the baseline characteristics of four groups. Compared with patients in LCLF group, those in HCHF group were more likely to have higher monocyte, neutrophils, CRP, FIB and have higher CSF pressure.
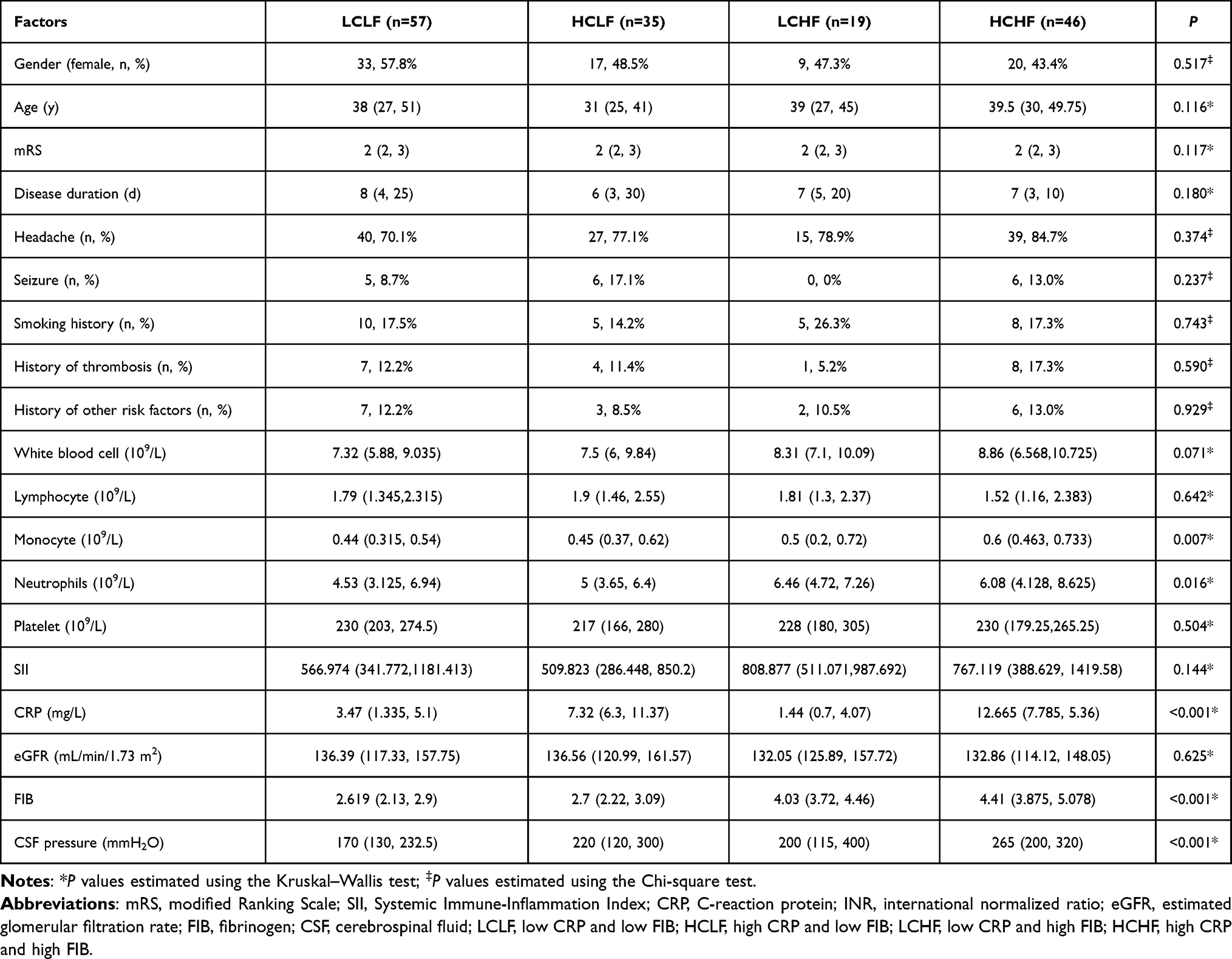 |
Table 3 Demographic Variables and Clinical Assessments According to the Combination of CRP and FIB |
After adjusted by gender, age, mRS, duration, headache, seizure, smoking, history of thrombosis and other risk factors, WBC, SII, and eGFR, patients in HCHF group were 5.286 (95% CI:2.04–13.701, P=0.001) times more frequent to experience IH than those in LCLF group did (Table 4). Patients in HCHF group had the highest risk of IH. The addition of CRP and FIB to the basic model significantly improved discriminatory power for IH, as AUC increased from 0.692 (95% CI: 0.609–0.775, P<0.001) to 0.767 (95% CI: 0.692–0.843, P<0.001) (Figure 3).
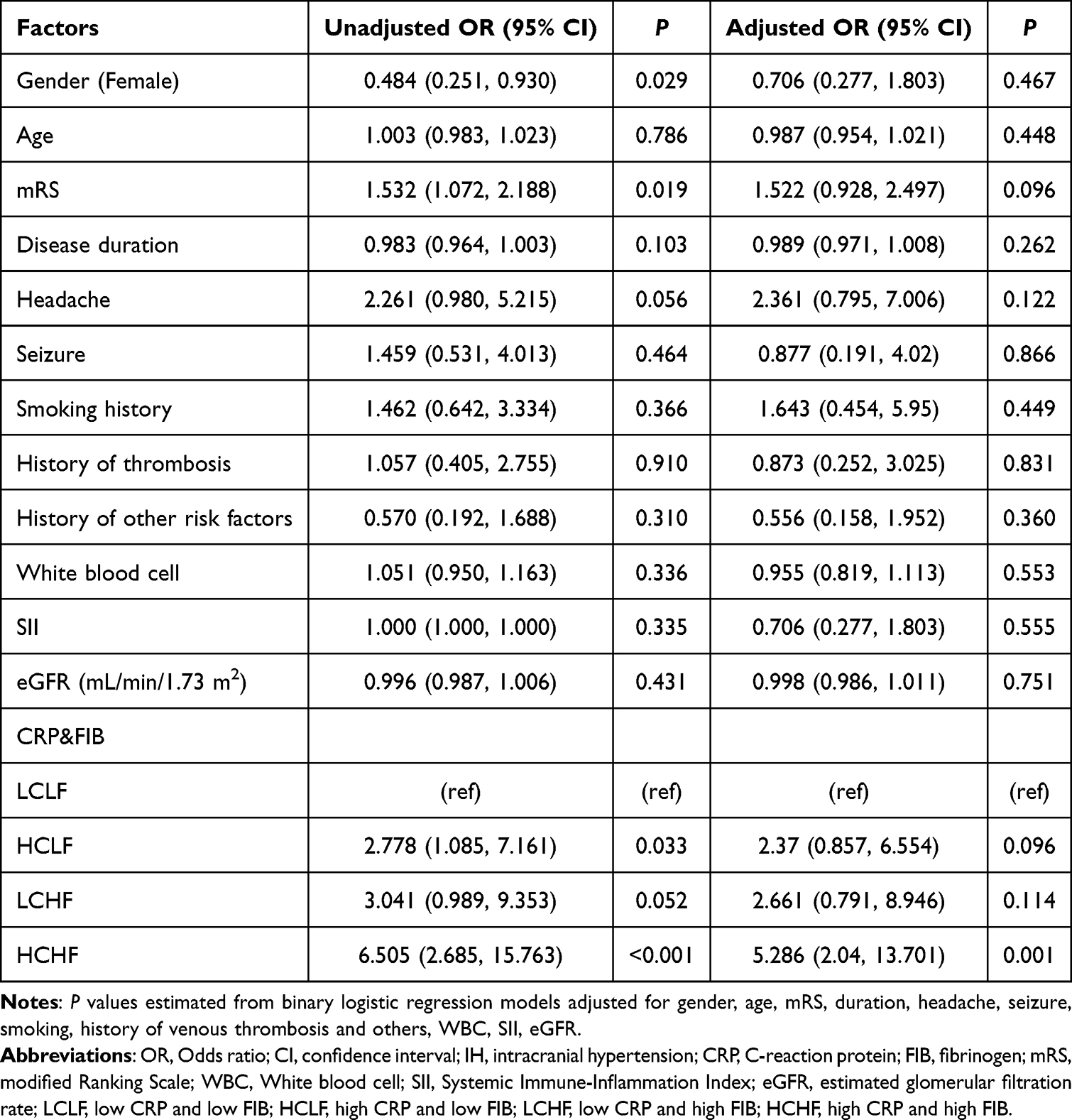 |
Table 4 ORs and 95% CIs for IH According to the Combination of CRP and FIB |
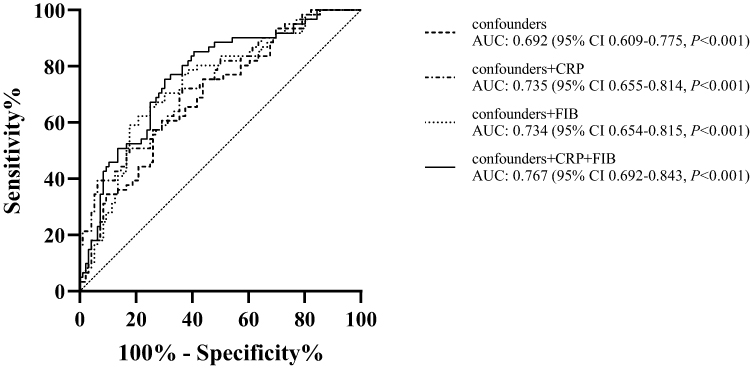 |
Figure 3 ROC curves of IH by confounders, CRP, and FIB. Logistic confounding factors: gender, age, mRS, duration, headache, seizure, smoking, history of thrombosis and other risk factors, WBC, SII, eGFR. Abbreviations: ROC, receiver operating characteristic; AUC, area under curve; CRP, C-reaction protein; FIB, fibrinogen; WBC, White blood cell; SII, Systemic Immune-Inflammation Index; eGFR, estimated glomerular filtration rate. |
Discussion
The present study demonstrated for the first time the prognostic role of CRP and FIB, especially their joint effect, in IH of CVST patients. For CVST patients, CRP >5.55mg/L and FIB>3.44g/L were associated with the increased risk of IH. Furthermore, CVST patients with both high CRP and FIB levels had the highest risk for IH, which was 5.286-fold in the HCHF group compared with that in LCLF group. Following analysis showed our model with good predictive ability, which indicated the combination of CRP and FIB could enhance the predictive value for IH of CVST patients. The notable quantitative improvement in prognostic metrics (the model’s AUC increased from 0.692 to 0.767, P<0.001) after incorporating CRP and FIB into the multivariate regression analysis, and the enhanced clinical utility for risk stratification in CVST patients. While we acknowledge that biomarker value overlap is an inherent limitation of this observational study, attributable to the substantial heterogeneity of CVST patients in etiology, disease severity, and comorbidities, the observed statistical differences can still inform clinical practice by optimizing admission risk stratification, guiding individualized treatment de-escalation for borderline-risk patients, and enabling evidence-based prognostic counseling. The findings provide a rapid, convenient and noninvasive way to monitor ICP, facilitating early identification of IH and prompt treatment of high-risk CVST patients to improve their outcomes. This model should serve as an adjunct clinical tool rather than a standalone decision-making criterion, and future prospective studies with larger sample sizes and standardized data collection are needed to further validate its clinical utility.
Inflammatory cells were detected throughout all brain specimens of animal models of acute liver failure (ALF) with increased ICP.16 Hannah et al demonstrated that the glucagon-like peptide-1 receptor agonist exendin-4 was able to reduce ICP in a rat model of hydrocephalus, which might be partly due to its anti-inflammatory effects.17 Moreover, a rabbit model of cerebral venous infarction showed that FIB increased as ICP gradient increased.18 All the data implied that both inflammation and coagulation systems might contribute to the formation of IH through animal models, which has not been extensively explored in CVST, especially in CVST patients.
CRP is a kind of acute-phase response protein synthesized and secreted by liver under certain pathological conditions, sensitively reflecting the activation of inflammatory response in the body. CRP can activate monocytes, promote tissue factor secretion, and initiate coagulation activation, which then promote the synthesis of coagulation factors and accelerate the formation of thrombosis.19 Inflammatory biomarkers associated with diagnosis, severity, and poor prognosis of CVST have been reported.19–21 A multicenter prospective observational study conducted in Portugal with 62 patients, demonstrated that elevated inflammatory biomarkers such as neutrophil to lymphocyte ratio and interleukin-6 were independently predictive factors for poor prognosis of CVST patients. Moreover, three inflammatory biomarkers, including CRP, were evaluated as predictors of evolution.21 A hospital-based CVST study found that higher CRP, measured on the first day of admission, was associated with both hospital fatality and poor outcome.22 However, there have been few studies on the association between CRP and IH in CVST patients. For TBI patients, CRP has been indicated as an indicator of IH,12 which is consistent with our study. In the etiology of idiopathic intracranial hypertension (IH), the contribution of inflammatory mechanisms and changes in cytokine levels have been proposed.23,24 We hypothesized that inflammatory factor could also affect ICP in a similar way. Additionally, a retrospective study showed both CRP and ICP were significantly decreased after patients were treated with glucocorticoid and anticoagulation, indicating a possible interaction between IH and inflammatory reaction in CVST.25
Pathological elevation of FIB implicates a hypercoagulable and inflammatory state with increased possibility of thrombosis.8,26 The most common location of thrombosis for CVST patients with IH is superior sagittal and transverse sinuses.27 Impaired cerebral venous drainage and abnormal CSF absorption act as the two most important pathogenesis of IH. Therefore, FIB might play a vital role in the formation of IH of CVST patients. The diagnostic sensitivity and specificity of FIB for CVST were 73.5–77.5% and 60–83.9%, respectively.9 Kiyohira et al showed that low FIB levels were associated with ICP elevation in patients with severe acute subdural hematoma (ASDH), indicating a possible correlation between FIB levels and ICP.28 However, it has not been extensively explored in CVST patients. In the multivariate regression analysis, the unadjusted OR of FIB was associated with a statistically significant P-value of 0.022, whereas the P-value for the adjusted OR was 0.05. The conventional threshold for statistical significance (P<0.05) is an arbitrarily defined criterion. A P-value of 0.05 is considered “marginally significant”, indicating a weak trend of statistical association rather than no association at all. In exploratory studies, variables should not be arbitrarily excluded solely based on P≥0.05, especially when there is a clear biological mechanism supporting the variable. And the 95% CI was (1, 1.778), which excluded the null value of 1 at its lower bound, suggesting a potential trend of association between exposure factors and outcomes. Patients with FIB>3.44 g/L were more likely to experience IH, which was consistent with the animal study.18
Increasing evidence points to extensive cross-talk between inflammation and coagulation systems, whereby inflammation leads not only to activation of coagulation, but coagulation also considerably affects inflammatory activity, especially in thrombotic diseases.26 Coagulation factors (such as thrombin) or anticoagulant proteins (such as activated protein C) may activate specific cell receptors on mononuclear cells or endothelial cells, which may affect, for example, cytokine production or inflammatory cell apoptosis.29 We previously reported combined prognostic significance of WBC and D-dimer on in-hospital outcomes of acute ischemic stroke (AIS) patients, indicating the cross-talk between inflammation and coagulation in the pathogenesis of AIS.30 Billoir et al also found that both C-reactive protein and D-dimer could help predict bad prognosis in CVST.20 In the present study, we first found the combination of CRP and FIB could better predict IH in CVST, which implied both systems contributed to its occurrence with synergistic effect.
The mRS score was higher in IH of CVST patients, which is readily understandable. Notably, the IH group had a higher proportion of male patients. Anatomical studies have demonstrated that males exhibit thicker skulls and relatively narrower intracranial venous sinus lumens, with the average diameter of the transverse sinus in males being 8–12% smaller than that in females. The cerebral blood flow increases more substantially with elevations in body mass index (BMI). When thrombosis occurs, these narrow lumens are more prone to obstruction, leading to an acute increase in venous return resistance. This, in turn, induces cerebral congestion and edema, which ultimately compress the CSF circulation pathway and result in elevated intracranial pressure. Additionally, males are more likely to present with unilateral transverse sinus hypoplasia. If thrombosis develops in the contralateral (healthy) transverse sinus, the absence of effective collateral circulation compensation precipitates the rapid progression of venous return impairment to overt intracranial hypertension.31
The strength of our study included being the first study to explore the joint effect of CRP and FIB on IH of CVST patients, providing a useful and convenient tool for the timely identification of high-risk patients, facilitating appropriate treatment, which is also noninvasive compared to lumbar puncture. However, there are still some potential limitations that merit considerations. First, the study participants were from two centers in China, which may limit the generalizability of our findings. Secondly, a proportion of patients were excluded due to a lack of CRP and FIB data, which may lead to selection bias. Thirdly, data on alcohol consumption in this study were derived from medical record review. However, detailed records of drinking status (eg, alcohol intake, drinking frequency, exposure duration) were lacking in the medical records of some patients, with only 21.5% of patients having clear documentation of their drinking history. Due to insufficient data completeness, standardized classification (eg, light/excessive drinking) and statistical analysis were not feasible, so this variable was not included in the study. Finally, a longer follow-up period might be needed to comprehensively understand the correlation of the crosstalk between inflammation and coagulation systems and the pathogenesis of CVST. In the future, a multicenter study with a larger sample-size, longer follow-up period and broader range of inflammatory and coagulation biomarkers will help deepen our understanding of pathogenesis of IH of CVST.
Conclusion
In conclusion, higher CRP and FIB levels were both associated with increased risk of IH subsequent to CVST. The combination of high CRP and FIB levels could better predict IH of CVST patients than CRP and FIB levels alone.
Data Sharing Statement
The data that support the findings of this study are available on request from Xia Zhang, one of the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Soochow University. The patients/participants provided their written informed consent to participate in this study.
Funding
This work was supported by Suzhou Scientific and Technological Projects of Medical Innovation and Application Research(SKY202317); Jiangsu Provincial Medical Key Discipline(ZDXK202217);Chinese Cardiovascular Association-Natural lipid-lowering drugs fund(2023-CCA-NLD-339).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Alghamdi SR, Cho A, Lam J, Al-Saadi T. Cerebral venous sinus thrombosis in closed head injury: systematic review and meta-analysis. J Clin Neurosci. 2022;98:254–11. doi:10.1016/j.jocn.2022.01.027
2. Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791–1798. doi:10.1056/NEJMra042354
3. Ranjan R, Ken-Dror G, Sharma P. Pathophysiology, diagnosis and management of cerebral venous thrombosis: a comprehensive review. Medicine. 2023;102(48):e36366. doi:10.1097/MD.0000000000036366
4. Duman T, Uluduz D, Midi I, et al. A multicenter study of 1144 patients with cerebral venous thrombosis: the VENOST study. J Stroke Cerebrovasc Dis. 2017;26(8):1848–1857. doi:10.1016/j.jstrokecerebrovasdis.2017.04.020
5. Canhao P, Abreu LF, Ferro JM, et al. Safety of lumbar puncture in patients with cerebral venous thrombosis. Eur J Neurol. 2013;20(7):1075–1080. doi:10.1111/ene.12136
6. Schuchardt F, Demerath T, Lutzen N, et al. Risk factors for the development of secondary intracranial hypertension in acute cerebral venous thrombosis. Neuroradiology. 2023;65(3):463–477. doi:10.1007/s00234-022-03091-9
7. Silvis SM, de Sousa DA, Ferro JM, Coutinho JM. Cerebral venous thrombosis. Nat Rev Neurol. 2017;13(9):555–565. doi:10.1038/nrneurol.2017.104
8. Meng R, Wang X, Hussain M, et al. Evaluation of plasma D-dimer plus fibrinogen in predicting acute CVST. Int J Stroke. 2014;9(2):166–173. doi:10.1111/ijs.12034
9. Pathak A, Singh VK, Kumar A, Mishra VN, Joshi D, Chaurasia RN. Predictive value of combination of D-dimer and fibrinogen in diagnosing acute CVST. Ann Neurosci. 2021;28(3–4):156–161. doi:10.1177/09727531211063138
10. Zang RS, Zhang H, Xu Y, et al. Serum C-reactive protein, fibrinogen and D-dimer in patients with progressive cerebral infarction. Transl Neurosci. 2016;7(1):84–88. doi:10.1515/tnsci-2016-0013
11. Di Napoli M, Papa F, Bocola V. Prognostic influence of increased C-reactive protein and fibrinogen levels in ischemic stroke. Stroke. 2001;32(1):133–138. doi:10.1161/01.str.32.1.133
12. Hergenroeder G, Redell JB, Moore AN, et al. Identification of serum biomarkers in brain-injured adults: potential for predicting elevated intracranial pressure. J Neurotrauma. 2008;25(2):79–93. doi:10.1089/neu.2007.0386
13. Saposnik G, Bushnell C, Coutinho JM, et al. Diagnosis and management of cerebral venous thrombosis: a scientific statement from the American heart association. Stroke. 2024;55(3):e77–e90. doi:10.1161/STR.0000000000000456
14. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
15. Ma YC, Zuo L, Chen JH, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17(10):2937–2944. doi:10.1681/ASN.2006040368
16. Kristiansen RG, Lindal S, Myreng K, Revhaug A, Ytrebo LM, Rose CF. Neuropathological changes in the brain of pigs with acute liver failure. Scand J Gastroenterol. 2010;45(7–8):935–943. doi:10.3109/00365521003675047
17. Botfield HF, Uldall MS, Westgate CSJ, et al. A glucagon-like peptide-1 receptor agonist reduces intracranial pressure in a rat model of hydrocephalus. Sci Transl Med. 2017;9(404). doi:10.1126/scitranslmed.aan0972
18. Wang W, Lin C, Hong J, Wang S, Gu J. Effects of increased intracranial pressure gradient on cerebral venous infarction in rabbits. World Neurosurg. 2018;120:e161–e168. doi:10.1016/j.wneu.2018.07.264
19. Wang L, Duan J, Bian T, et al. Inflammation is correlated with severity and outcome of cerebral venous thrombosis. J Neuroinflammation. 2018;15(1):329. doi:10.1186/s12974-018-1369-0
20. Billoir P, Siguret V, Fron EM, et al. C-reactive protein and D-dimer in cerebral vein thrombosis: relation to clinical and imaging characteristics as well as outcomes in a French cohort study. Res Pract Thromb Haemost. 2023;7(3):100130. doi:10.1016/j.rpth.2023.100130
21. Aguiar de Sousa D, Pereira-Santos MC, Serra-Caetano A, et al. Blood biomarkers associated with inflammation predict poor prognosis in cerebral venous thrombosis:: a multicenter prospective observational study. Eur J Neurol. 2021;28(1):202–208. doi:10.1111/ene.14526
22. Shakibajahromi B, Haghighi AB, Salehi A, et al. Clinical and radiological characteristics and predictors of outcome of cerebral venous sinus thrombosis, a hospital-based study. Acta Neurol Belg. 2020;120(4):845–852. doi:10.1007/s13760-018-1009-6
23. Fahmy EM, Rashed LA, Mostafa RH, Ismail RS. Role of tumor necrosis factor-alpha in the pathophysiology of idiopathic intracranial hypertension. Acta Neurol Scand. 2021;144(5):509–516. doi:10.1111/ane.13482
24. Sinclair AJ, Ball AK, Burdon MA, et al. Exploring the pathogenesis of IIH: an inflammatory perspective. J Neuroimmunol. 2008;201-202:212–220. doi:10.1016/j.jneuroim.2008.06.029
25. Shuyuan H, Kaiyuan Z, Yaqin G, Jingkai L, Chen Z, Xunming J. Exploration of glucocorticoid combined with anticoagulation in acute / subacute severe cerebral venous thrombosis. Journal of Capital Medical University. 2023;44:280–288.
26. Levi M, van der Poll T, Buller HR. Bidirectional relation between inflammation and coagulation. Circulation. 2004;109(22):2698–2704. doi:10.1161/01.CIR.0000131660.51520.9A
27. Wei H, Jiang H, Zhou Y, Liu L, Zhou C, Ji X. Intracranial hypertension after cerebral venous thrombosis-Risk factors and outcomes. CNS Neurosci Ther. 2023;29(9):2540–2547. doi:10.1111/cns.14194
28. Kiyohira M, Suehiro E, Fujiyama Y, Suzuki M. Predictive factors of intracranial pressure elevation in patients with severe acute subdural hematoma. No Shinkei Geka. 2019;47(7):753–760. doi:10.11477/mf.1436204019
29. Dziedzic T. Systemic inflammation as a therapeutic target in acute ischemic stroke. Expert Rev Neurother. 2015;15(5):523–531. doi:10.1586/14737175.2015.1035712
30. Peng D, Huang Y, Wang Y, et al. Combined prognostic significance of white blood cell count and D-dimer on in-hospital outcomes of acute ischemic stroke. Nutr Metab Cardiovasc Dis. 2023;33(1):177–184. doi:10.1016/j.numecd.2022.10.008
31. Ozcan TA, Meral H, Ozben S, et al. Cerebral venous sinus thrombosis: gender differences in ten years experience. Dusunen Adam J Psychiatr Neurol Sci. 2013;26(3):281–285. doi:10.5350/DAJPN2013260307
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.