Back to Journals » Clinical Ophthalmology » Volume 20
The JFC Method: A Proof-of-Concept Report on the Surgical Technique and Initial Feasibility of a Novel Flanged-Cord Temporary Occlusion for Non-Valved Glaucoma Drainage Devices
Authors Numa S ![]() , Suda K
, Suda K ![]() , Miyake M, Nakano E, Mori Y, Morino K, Tsujikawa A
, Miyake M, Nakano E, Mori Y, Morino K, Tsujikawa A ![]()
Received 3 December 2025
Accepted for publication 16 April 2026
Published 22 May 2026 Volume 2026:20 586326
DOI https://doi.org/10.2147/OPTH.S586326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
JFC Method for Non-Valved Glaucoma Drainage – Video S1 [586326]
Views: 59
Shogo Numa, Kenji Suda, Masahiro Miyake, Eri Nakano, Yuki Mori, Kazuya Morino, Akitaka Tsujikawa
Department of Ophthalmology and Visual Sciences, Kyoto University Graduate School of Medicine, Kyoto, Japan
Correspondence: Shogo Numa, Department of Ophthalmology and Visual Sciences, Kyoto University Graduate School of Medicine, Kyoto, Japan, Tel +81-75-751-3248, Fax +81-75-752-0933, Email [email protected]
Purpose: To describe the design and initial proof-of-concept of the Japanese Flanged Cord (JFC) method, a novel technique for temporary intraluminal occlusion of non-valved glaucoma drainage devices (GDDs) to prevent postoperative hypotony.
Patients and Methods: This technical report describes a new occlusion method utilizing a 5– 0 polyvinylidene fluoride (PVDF) or polypropylene monofilament suture. A terminal flange is created on the suture using thermal cautery, functioning as an intraluminal plug. This flanged cord is inserted into the GDD tube to block aqueous flow without tube ligation. The external end is secured subconjunctivally for later removal. The clinical feasibility of this technique was evaluated in a single patient with refractory glaucoma undergoing Ahmed ClearPath (New World Medical Inc. CA, USA), implantation.
Results: In this index case, the JFC method provided secure, watertight occlusion of the GDD tube. The intraluminal obturation mechanism eliminated the need for external ligation, thereby avoiding potential tube damage such as kinking or laceration. Postoperatively, intraocular pressure was well-controlled without hypotony. The cord was removed atraumatically at the slit lamp at the surgeon’s discretion, establishing flow without complications.
Conclusion: The JFC method demonstrated initial clinical feasibility as a potential alternative to traditional external ligation techniques. By avoiding external compression and offering surgeon-controlled flow initiation, this technique may address key limitations of current non-valved GDD surgery. However, as these findings are based on a single-case report, further studies in larger cohorts are strictly required to validate its safety and long-term efficacy.
Keywords: glaucoma drainage device, hypotony, surgical technique, tube occlusion, baerveldt, ahmed clearpath
Introduction
Glaucoma drainage devices (GDDs) are a cornerstone in the management of refractory glaucoma.1 Non-valved GDDs, such as the Baerveldt Glaucoma Implant (Johnson & Johnson Vision, Santa Ana, CA, USA) and Ahmed ClearPath (New World Medical Inc., CA, USA), are particularly effective for achieving low long-term intraocular pressure (IOP)2 but require temporary tube occlusion to prevent immediate postoperative hypotony and its vision-threatening sequelae.3 This occlusion allows for the formation of a flow-regulating fibrous capsule around the endplate over four to six weeks.3
The current gold standard for temporary occlusion involves external ligation of the tube using an absorbable suture, typically 7–0 or 8–0 polyglactin (Vicryl (Ethicon, Inc., Raritan, NJ, USA)).4 While widely adopted, this technique has inherent drawbacks. First, the degradation rate of polyglactin is variable and influenced by ocular inflammation, leading to unpredictable timing of tube opening.5 Premature dissolution can result in hypotony maculopathy or choroidal detachment. Indeed, large-scale clinical trials have highlighted the prevalence of such issues; for instance, the Tube Versus Trabeculectomy (TVT) Study and the Ahmed Versus Baerveldt (AVB) Study reported that early postoperative complications such as shallow or flat anterior chamber and choroidal effusion occur in approximately 10% to 14% of patients receiving non-valved implants.6,7 Furthermore, because glaucoma drainage devices are primarily indicated for refractory cases or following failed trabeculectomy, they are frequently employed in patients with advanced disease. In such vulnerable eyes, these postoperative complications are not merely transient events but pose a critical risk of further severe and irreversible visual impairment. Delayed dissolution, on the other hand, may necessitate laser suture lysis, an additional procedure that requires a clear view of the tube and specialized equipment.8 Furthermore, alternative internal occlusion methods using intraluminal stents (eg, 3–0 nylon or polypropylene sutures) have been described. However, these “ripcord” techniques often still require an external anchoring suture to prevent leakage around the stent, which reintroduces the risk of tube compression.9 Most critically, any technique involving external tightening poses a risk of mechanical damage to the silicone tube. Tight ligatures can cause permanent kinking of the tube lumen, potentially compromising long-term filtration efficacy even after the suture has dissolved.10 Furthermore, while the precise incidence of intraoperative tube damage is likely underreported—as such occurrences often necessitate immediate device replacement and thus rarely appear in published clinical data—it is a recognized, albeit rare, complication. Reports exist of silicone tubes being inadvertently damaged or transected during the application of ligature sutures across various devices, including the Baerveldt glaucoma implant. Such accidents may require specialized interventions, such as the use of a tube extender or novel reinsertion techniques, to salvage the surgical procedure.11,12
In this study, we describe the design and surgical implementation of a novel technique, the Japanese Flanged Cord (JFC) method. We evaluated the initial feasibility and safety of this method, which shifts the paradigm from external compression to intraluminal obturation, aiming to provide a safer and more predictable means of managing early postoperative aqueous flow.
Materials and Methods
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board and Ethics Committee of Kyoto University Graduate School of Medicine (Approval No. R625). This technical report is designed as a proof-of-concept study to evaluate the initial feasibility and safety of the JFC method in a single patient. While this single-patient design inherently limits the generalizability of the findings and involves potential selection bias, it allows for a detailed, stepwise assessment of the novel technique’s surgical performance. Written informed consent was obtained from the patient for the publication of this report and any accompanying images and video.
In addition to standard instruments for long-tube shunt surgery, the JFC method necessitates some other materials; a 5–0 PVDF or polypropylene suture (eg, CROWNJUN Asflex Suture, KONO SEISAKUSHO Co., Ltd., Chiba, Japan; or PROLENE, Ethicon US LLC, Somerville, NJ, USA), a thermal cautery device (eg, Accu-Temp Variable Low Temp Cautery, BVI Medical, Inc., Waltham, MA, USA), and a 1 mL or 2.5 mL syringe are also required. (Figure 1)
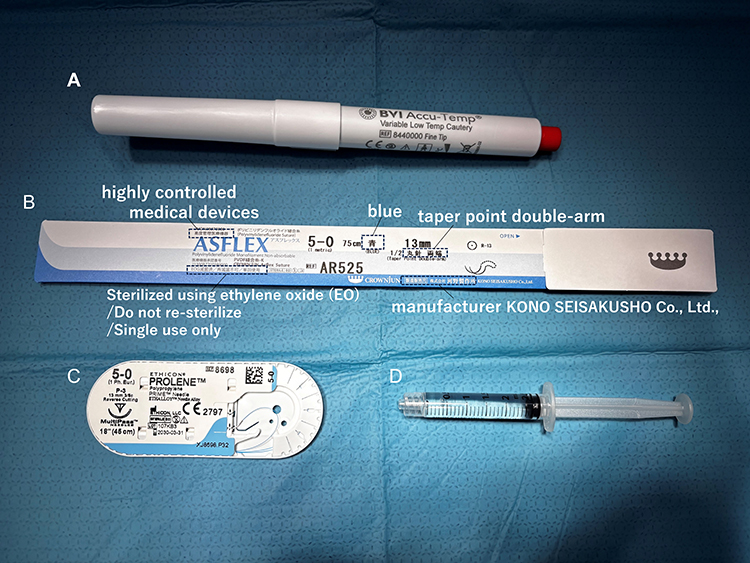 |
Figure 1 Materials required for the JFC method. (A) A thermal cautery device (Accu-Temp Variable Low Temp Cautery; BVI Medical, Inc., Waltham, MA, USA), commonly used for intrascleral intraocular lens fixation. (B) A 5–0 polyvinylidene fluoride (PVDF) suture (CROWNJUN Asflex Suture; KONO SEISAKUSHO Co., Ltd., Chiba, Japan). (C) A 5–0 polypropylene suture (PROLENE; Ethicon US LLC, Somerville, NJ, USA), which serves as a suitable alternative to PVDF. (D) A 2.5 mL syringe filled with balanced salt solution, used to prevent air entrapment within the GDD tube during priming. Syringes of other volumes (eg, 1 mL or 5 mL) are also acceptable. |
The 5–0 suture size was specifically selected for its optimal intraluminal fit (as detailed in the Discussion). For a non-valved GDD, the following preparation is performed before suturing the implant’s plate to the sclera. (See Benchtop Video S1 performing on the Ahmed ClearPath model 350)
1) Flange Creation: From the posterior end of the GDD tube (plate side), the 5–0 PVDF suture is passed from its non-needled end and externalized through the anterior tip of the tube. The tip of the externalized suture is approached with a thermal cautery to create a flange. It is crucial not to make direct contact with the cautery tip, similar to the Yamane technique for IOL scleral fixation,13 to ensure a proper flange shape. Direct contact will cause the suture to melt irregularly rather than forming a proper flange. (Figure 2)
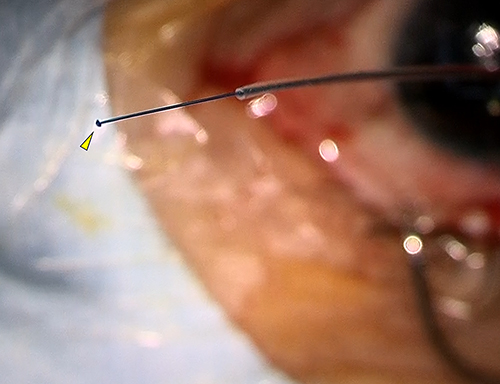 |
Figure 2 Preparation of the flanged cord. A 5–0 PVDF suture is threaded through the Ahmed ClearPath tube from the posterior end, and the suture tip exiting the anterior end is formed into a flange using a thermal cautery.(yellow arrowhead). |
2) Implant Priming: A syringe filled with balanced salt solution (BSS) is prepared. With the flanged tip of the suture and the anterior tip of the implant tube inserted into the nozzle of this syringe, the suture is slowly withdrawn from the posterior end. Withdrawing the suture while inside the nozzle allows the tube’s lumen to be filled with the solution, preventing air entrapment. This priming step is thought to be crucial to ensure immediate filtration upon later removal of the cord.
3) Occlusion Verification: As the flanged suture is withdrawn to position the flange at the desired location (specifically, for the Ahmed ClearPath, the suture holes on the plate serve as a convenient landmark for the author), the flange of 5–0 PVDF suture provides an ideal occlusion for the GDD tube (inner diameter approx. 300 μm). While there is minimal resistance when pulling the suture, the occlusion is secure and does not dislodge even under significant manual pressure. (Figure 3)
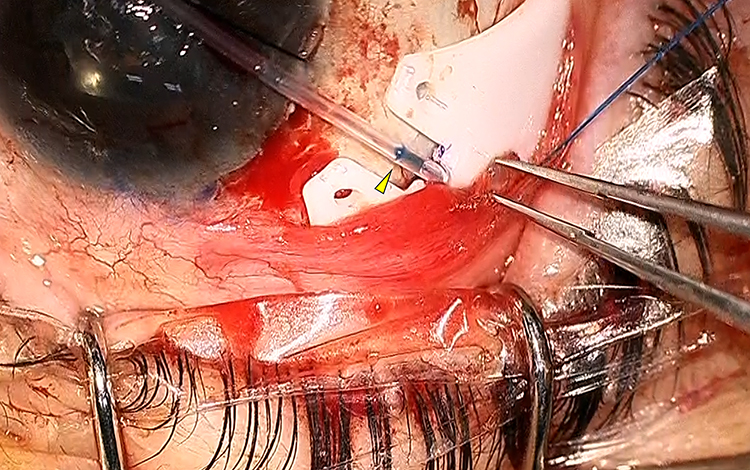 |
Figure 3 Intraoperative view of the intraluminal occlusion. The Ahmed ClearPath tube is effectively occluded by the flanged 5–0 PVDF suture. The flange is positioned at the level of the suture hole (yellow arrowhead). |
4) Implantation: The surgery proceeds with a conjunctival incision and dissection of Tenon’s capsule tailored to the size of the GDD, followed by implant fixation and tube insertion. For tube placement and to prevent exposure, rather than creating a scleral flap or utilizing a preserved scleral patch, the author prefers a scleral tunnel technique reported by Tanito M et al.14
5) Venting Slits (Sherwood Slits): Prior to insertion into the anterior chamber, venting slits (Sherwood slits) are created anterior to the occlusion point to allow for a controlled amount of aqueous filtration during the early postoperative period while the main lumen is occluded. Using 8–0 or 9–0 suture needle, fenestrations are made through the tube wall. This step is essential to prevent early postoperative IOP spikes, as the JFC method provides complete occlusion of the main lumen.
6) Externalization: After the tube is inserted into the anterior chamber or ciliary sulcus (posterior chamber) or pars plana (vitreous cavity), the external portion of the 5–0 suture is passed through the scleral tunnel and externalized near the limbus, leaving a small portion exposed subconjunctivally or transconjunctivally to facilitate easy removal one to two months postoperatively. (Figure 4) This externalization method mimics the technique described by Mieno H et al for PreserFlo MicroShunt implantation, in which a 10–0 nylon suture is minimally exposed at the corneal limbus; reference to their study is recommended.15 However, unlike Mieno’s technique, the stent suture used here is thicker. Therefore, a key step is to slightly widen the fornix side of the scleral tunnel with the bevel of the 5–0 PVDF needle (or the bevel of a 25G needle) to prevent the flange from catching during removal. Figure 4 shows the intraoperative view at the final stage of the procedure, immediately before conjunctival closure
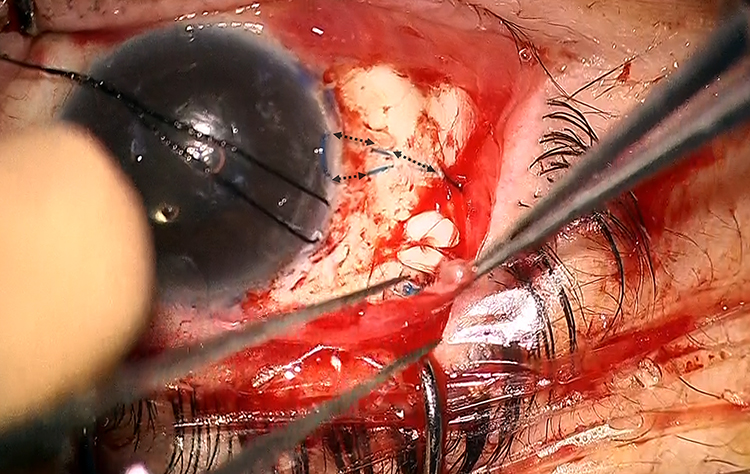 |
Figure 4 Intraoperative view immediately prior to conjunctival closure. The black dotted arrows indicate the extent of the ripcord placed within the scleral tunnel. The suture is exposed at the limbus to facilitate easy removal 4 to 8 weeks postoperatively. |
Results
The JFC method was successfully implemented in the index case. Preoperatively, the intraocular pressure (IOP) was 36 mmHg under 4 types of glaucoma medications. Intraoperatively, the flanged 5–0 PVDF suture provided immediate and watertight occlusion of the Ahmed ClearPath tube. The intraluminal plug withstood physiological and supraphysiological irrigation pressures without dislodgement. The preparation time for the JFC assembly was only several minutes.
Postoperatively, the patient was managed with a standard regimen of 0.5% Moxifloxacin and 0.1% betamethasone eye drops four times daily. On the first postoperative day, the IOP was 17 mmHg, and the anterior chamber remained deep and stable, equivalent to the preoperative state, with no signs of hyphema, fibrin, or significant intraocular inflammation. During the follow-up period, the IOP remained stable at 15 mmHg on day 3, 22 mmHg at 1 week, and 19 mmHg at 4 weeks postoperatively. Postoperative hypotony was not observed during the early postoperative period, confirming the efficacy of the intraluminal occlusion. The anterior chamber remained deep and stable Throughout the follow-up period, the conjunctiva covering the externalized 5–0 suture exhibited only mild focal injection, with no evidence of suture-related erosion, exposure, or infection. At 4 weeks postoperatively, after encapsulation of the plate was presumed, the externalized suture was easily removed at the slit lamp under topical anesthesia without complications. The flange passed smoothly through the widened scleral tunnel tract. Following removal, IOP reduction was achieved; from 19mmHg to 9–12mmHg confirming the patency of the tube. While these findings demonstrate the successful surgical implementation and initial feasibility of the JFC method in this specific case, they should be interpreted as a preliminary proof-of-concept rather than a definitive clinical validation.
Discussion
The management of early aqueous outflow in non-valved GDDs represents a critical challenge in glaucoma surgery. The JFC method addresses the fundamental limitations inherent in current flow-restriction techniques by eliminating external compressive forces on the GDD tube.
Conventional methods, including absorbable suture ligation and ripcord techniques, rely on circumferentially constricting the silicone tube.4 This mechanism creates iatrogenic risks such as tube laceration, kinking, and permanent luminal distortion, which can compromise the long-term function of the device. By utilizing an intraluminal plug, the JFC method may offer a potential improvement in procedural safety by avoiding external compression. Furthermore, the JFC method offers a high degree of predictability and control. Unlike the unpredictable hydrolysis of polyglactin sutures,5 the JFC method provides the surgeon with precise temporal control over the initiation of flow, similar to ripcord techniques,7 but without the antecedent risks of a compressive ligature.
The choice of suture material is pivotal to the success of this technique. We utilized PVDF (polyvinylidene fluoride) sutures, which are widely used in vascular surgery and recently popularized in ophthalmic surgery for intrascleral IOL fixation, which often use IOLs whose haptics are made of PVDF.9 PVDF possesses superior resistance to biodegradation compared to polypropylene, ensuring that the flange remains mechanically stable and does not become brittle or fracture during the indwelling period.16,17 This stability is crucial for ensuring smooth, atraumatic removal of the cord weeks or months after surgery.
Suture diameter is defined by the United States Pharmacopeia (USP) standards: 4–0 sutures range from 150 to 199 μm, 5–0 from 100 to 149 μm, and 6–0 from 70 to 99 μm. In this benchtop study, we evaluated CROWNJUN Asflex Sutures (PVDF; KONO SEISAKUSHO Co., Ltd., Chiba, Japan) and PROLENE sutures (polypropylene; Ethicon US LLC, Somerville, NJ, USA). We created flanges on 4–0, 5–0, and 6–0 sutures and assessed their occlusion efficacy and withdrawal resistance within the Ahmed ClearPath, which has an intraluminal diameter of approximately 300 μm. Our trials indicated that for both PVDF and polypropylene, the flanged 5–0 sutures provided adequate occlusion while allowing for smooth withdrawal without excessive resistance. Furthermore, we performed benchtop evaluations using multiple units of both the Ahmed ClearPath and the Baerveldt glaucoma implant to assess the stability of the intraluminal plug. In these trials, the flanged cord remained securely in place and did not dislodge once, even when subjected to high manual irrigation pressures. While these benchtop results are encouraging, the potential for dislodgement in a dynamic clinical environment cannot be entirely dismissed, and these findings must be viewed as a preliminary proof-of-concept. Biomechanical studies regarding the intrascleral fixation of intraocular lens(IOL), such as those by Kronschläger et al and Romero et al, reported a flange diameter expansion of approximately 2.2 to 3.0 times the original caliber of the PVDF IOL haptics following thermal cauterization.18,19 Although caution is required as the forming process may differ between sutures and haptics despite using the same PVDF material, extrapolating these findings to the current procedure suggests that the use of 5–0 or 4–0 PVDF sutures is considered optimal. However, even among sutures of the same material and USP classification, subtle variations in diameter may occur within the standardized ranges depending on the manufacturer. Therefore, we recommend that surgeons verify the compatibility of the specific sutures and non-valved glaucoma drainage devices (GDDs) used at their respective institutions prior to clinical application.
In addition to its safety profile, the JFC method offers a significant economic advantage. It utilizes standard, readily available surgical consumables (a 5–0 suture and a cautery device) without the need for expensive, specialized intraluminal stents or complex valved devices. This cost-effectiveness makes it a potentially attractive option for healthcare systems with limited resources.
The conceptual basis of this method is adapted from the well-established Yamane technique for sutureless intrascleral IOL fixation.9 The familiarity of many surgeons with creating a terminal flange using thermal cautery may facilitate a shorter learning curve and wider adoption.
This study represents a pilot technical report with short-term follow-up, therefore has several limitations. While the initial experience demonstrates excellent feasibility and safety, further prospective studies with a larger sample size are warranted to validate the long-term efficacy and safety profile in a broader patient population. Potential complications specific to this method, such as inadvertent cord dislodgement, infection, patient discomfort, corneal epithelial complications, or chronic inflammatory reactions, require further investigation. Furthermore, while our initial results are promising, the impact of an indwelling intraluminal cord on long-term tube patency and the potential for late-onset luminal changes remain unknown. Moreover, the clinical success of this technique relies heavily on the patient’s ability to cooperate with postoperative procedures. While the cord can typically be removed under topical anesthesia at the slit lamp, the JFC method may be contraindicated in patients for whom slit-lamp manipulation is difficult, such as those with advanced dementia or Down syndrome. In such cases, the inability to safely remove the flanged cord under local anesthesia would pose a significant challenge, potentially requiring a return to the operating room for removal under monitored anesthesia care. Therefore, careful patient selection is paramount to ensure the advantages of this surgeon-controlled initiation of flow are realized.
Conclusion
The JFC method is a novel, feasible technique for temporary occlusion of non-valved GDDs. However, as this is an early-stage, single-case feasibility study, our findings primarily demonstrate the potential of this non-compressive, intraluminal plug to eliminate iatrogenic tube damage while providing predictable, surgeon-controlled initiation of aqueous flow. While this approach shows promise in improving the safety profile of non-valved GDD surgery, broader claims regarding its safety and efficacy require further validation in larger cohorts with longer follow-up.
Data Sharing Statement
The data used in this study are available from the corresponding author upon reasonable request.
Ethics Approval
All research and measurements complied with the principles of the Declaration of Helsinki after receiving approval from the Kyoto University Graduate School and Faculty of Medicine Ethics Committee.
Acknowledgments
This study received no funding from any funding agency. The authors declare no personal or financial conflict of interest related to this study.
Funding
This research did not receive support from any funding agency.
Disclosure
Dr Shogo Numa reports personal fees and/or non-financial support from JFC Sales Plan Co., Ltd., Kono Seisakusho Co., Ltd, during the conduct of the study. Dr Kenji Suda reports grants and/or non-financial support from Nipro, Alcon; personal fees from Santen, Kowa, Senju, and Otsuka, outside the submitted work. Dr Yuki Mori reports personal fees from Santen Pharmaceutical, Kowa Company, Senju Pharmaceutical, and Novartis Pharma, outside the submitted work. Dr Akitaka Tsujikawa reports grants and/or personal fees from Canon, Findex, Santen Pharmaceutical, Sumitomo Pharma, Astellas Pharma, Otsuka Pharmaceutical, Senju Pharmaceutical, Alcon Japan, Wakamoto Pharmaceutical, Chugai Pharmaceutical, Rhoto Nitten, HOYA, Boehringer Ingelheim, Bayer Yakuhin, MSD, Kyowa Kirin, Janssen Pharmaceutical, Bayer, Novartis Pharma, AMO Japan, Kowa Pharmaceutical, Rhoto Pharmaceutical, and Johnson & Johnson, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Tsai JC, Johnson CC, Kammer JA, Dietrich MS. The Ahmed shunt versus the Baerveldt shunt for refractory glaucoma II: longer-term outcomes from a single surgeon. Ophthalmology. 2006;113(6):913–8. doi:10.1016/j.ophtha.2006.02.029
2. Budenz DL, Barton K, Feuer WJ, et al. Treatment outcomes in the Ahmed Baerveldt comparison study: five-year results. Ophthalmology. 2015;122(2):308–316. doi:10.1016/j.ophtha.2014.08.043
3. Christakis PG, Kalenak JW, Tsai JC, et al. The Ahmed versus Baerveldt study: five-year treatment outcomes. Ophthalmology. 2016;123(10):2093–2102. doi:10.1016/j.ophtha.2016.06.035
4. SooHoo JR, Smith M, Pantcheva M, et al. Complications of glaucoma drainage devices. Curr Opin Ophthalmol. 2014;25(2):148–155. doi:10.1097/ICU.0000000000000034
5. Ishida K, Kanno M, Hori N, et al. Baerveldt glaucoma implant: comparison of the absorbable and nonabsorbable suture ligation methods. J Glaucoma. 2016;25(2):177–182. doi:10.1097/IJG.0000000000000076
6. Christakis PG, Kalenak JW, Zurakowski D, et al. The Ahmed Versus Baerveldt study: one-year treatment outcomes. Ophthalmology. 2011;118(11):2180–2189. doi:10.1016/j.ophtha.2011.05.004
7. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. doi:10.1016/j.ajo.2011.10.024
8. Grover DS, Fellman RL, Fantes F, et al. Nonabsorbable tube ligatures with postoperative laser suture lysis for nonvalved glaucoma drainage devices. J Glaucoma. 2010;19(5):346–348. doi:10.1097/IJG.0b013e3181e07a14
9. El Chehab H, De Smedt S, De Keyser M, et al. One-year outcomes following internal ligation suture removal after Baerveldt tube surgery for refractory glaucoma. J Curr Glaucoma Pract. 2022;16(2):72–77.
10. Esfandiari H, Kurji K, Su D, et al. A novel technique to salvage a kinked Baerveldt Tube. J Glaucoma. 2020;29(5):e43–e45.
11. Mungale S, Dave P. A novel simplified method for managing inadvertent tube cut during aurolab aqueous drainage implant surgery for refractory glaucoma. Indian J Ophthalmol. 2019;67(5):694–696. doi:10.4103/ijo.IJO_1708_18
12. Sarkisian SR, Netland PA. Tube extender for revision of glaucoma drainage implants. J Glaucoma. 2007;16(7):637–639. doi:10.1097/IJG.0b013e3180640f6c
13. Yamane S, Sato S, Maruyama-Inoue M, et al. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136–1142. doi:10.1016/j.ophtha.2017.03.036
14. Tanito M, Ikeda Y, Asaoka R. A novel scleral tunnel technique for preventing tube exposure in Ahmed Glaucoma valve implantation. Cureus. 2024;16(4):e58499. doi:10.7759/cureus.58499
15. Mieno H, Mori K, Yoshii K, et al. Risk factors and protective strategies for hypotony following preserflo microshunt implantation. Sci Rep. 2025;15(1):8344. doi:10.1038/s41598-025-92879-9
16. Guidoin R, Rao Y, Marois Y, et al. Polyvinylidene fluoride vascular sutures: an investigation of their in vitro and in vivo stability. Cardiovasc Eng. 1996;1(3):117–125.
17. Wada A, Kubota H, Hatanaka H, et al. Comparison of mechanical properties of polyvinylidene fluoride and polypropylene monofilament sutures used for flexor tendon repair. J Hand Surg Br. 2001;26(4):341–345. doi:10.1054/jhsb.2000.0508
18. Kronschläger M, Blouin S, Zeilinger J, et al. Comparison of flange creation in three-piece intraocular lenses between high- and low-temperature cautery. BMC Ophthalmol. 2025;25(1):592. doi:10.1186/s12886-025-04428-7
19. Ma KK, Yuan A, Sharifi S, et al. A biomechanical study of flanged intrascleral haptic fixation of three-piece intraocular lenses. Am J Ophthalmol. 2021;227:45–52. doi:10.1016/j.ajo.2021.02.021
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.