Back to Journals » OncoTargets and Therapy » Volume 9
The interleukin-18 gene promoter -607 A/C polymorphism contributes to non-small-cell lung cancer risk in a Chinese population
Authors Jia Y, Zang A, Jiao S, Chen S, Yan F
Received 31 October 2015
Accepted for publication 2 February 2016
Published 21 March 2016 Volume 2016:9 Pages 1715—1719
DOI https://doi.org/10.2147/OTT.S99581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Min Li
Youchao Jia,1,2 Aimin Zang,2 Shunchang Jiao,1 Sumei Chen,1 Fu Yan1
1Department of Medical Oncology, General Hospital of Chinese PLA, Beijing, 2Department of Oncology, Affiliated Hospital of Hebei University, Hebei, People’s Republic of China
Abstract: The purpose of the present study was to determine the relationship between interleukin-18 (IL-18) -607 A/C polymorphism and the risk of non-small-cell lung cancer (NSCLC) and its impact on the serum IL-18 level. The genotyping of IL-18 -607 A/C polymorphism was detected by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). The results showed that the AA/AC genotype distribution in NSCLC patients was significantly higher than that of healthy controls (P=0.02). However, no significant differences were found between the two subgroups when stratified by clinical characteristics. Furthermore, serum IL-18 levels were found to be significantly higher in the NSCLC patients than in the controls (P=0.01) as detected by enzyme-linked immunosorbent assay analysis. There was no correlation between serum IL-18 levels and different genotypes. In conclusion, these findings suggest that IL-18 -607 A/C polymorphism increases the risk of NSCLC in the Chinese population, and this polymorphism could not functionally affect the IL-18 levels.
Keywords: IL-18, polymorphism, NSCLC
Introduction
Lung cancer is the leading cause of human cancer deaths worldwide. Most patients with lung cancer are diagnosed with an advanced, unresectable disease and have a poor prognosis. Non-small-cell lung cancer (NSCLC) accounts for more than 80% of all lung cancer cases. The overall 5-year survival rate of patients with lung cancer is less than 16%.1 The etiology of the lung cancer, to date, is still unknown. It is accepted that the pathogenesis of lung cancer is multifactorial, and the genetic background may be one of the critical etiologic factors.
Interleukin-18 (IL-18), an 18-kDa cytokine, belongs to the interleukin-1 superfamily.2 It has been reported that IL-18 has both anticancer and procancer effects on lung cancer.3–5 IL-18 has pleiotropic efficacy in activating natural killer cell cytotoxic effect and enhancing Th1 immune response, mainly by stimulating the expression of interferon-γ and tumor necrosis factor-α and consequently causing the elimination of tumor cells in vivo.6,7 It has been proposed that IL-18 modulates the immune system for attacking cancer cells through the suppression of tumor growth and angiogenesis in ovarian cancer, inhibition of breast cancer cell proliferation, potential invasion, and enhancement of cytotoxic effects on colon carcinoma cells.8–10 Furthermore, increased levels of IL-18 have been reported in head and neck squamous cell and hepatocellular carcinoma; esophageal, gastric, ovarian, colon, skin cancer; and myeloid leukemia cells.11–14
The IL-18 gene is located on chromosome 11q22.2-q22.3. The single nucleotide polymorphic (SNP) position of -607A/C (rs1946518) has confirmed the impact on IL-18 activity and expression in tissues.6,15 To date, numerous studies have explored the role of IL-18 SNPs in diseases, such as rheumatoid arthritis,16 type 1 diabetes,17 immune thrombocytopenia,18 and several cancers,19–22 including lung cancer.23 In this study, we investigated the role of IL-18 gene promoter polymorphism -607A/C in NSCLC occurrence and progress in order to provide data for screening high-risk Han Chinese individuals.
Materials and methods
Subjects
A total of 500 patients and 500 healthy controls were recruited in this study for the determination of genotyping of the IL-18 -607 A/C polymorphism. Serum IL-18 levels were determined in 90 NSCLC patients and 30 controls. The diagnosis of NSCLC was established by histopathological examination of biopsy or resected tissue specimens. An inclusion criterion was that NSCLC was confirmed by histology. The exclusion criteria were that clinical staging was indistinct and cases lacked specific clinical data. The healthy controls were from the health examination center. The study was approved by the hospital-based Ethics Committee of the General Hospital of Chinese PLA, Beijing, People’s Republic of China. Written informed consent was obtained from all of the subjects.
Genotyping
Peripheral blood samples were collected in vacuum tubes with 5% ethylenediaminetetraacetic acid (EDTA). Genomic DNA was extracted using DNA purification kit (Tiangen Biotech, Beijing, People’s Republic of China) according to the manufacturer’s instruction. The genotyping of the IL-18 -607 A/C polymorphism was performed by polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP). The forward primer 5′-CTTTGCTATCATTCCAGGAA-3′ and the reverse primer 5′-TAACCTCATTCAGGACTTCC-3′ were used for PCR analysis. The 20 μL PCR mixture contained 50–150 ng of genomic DNA and 10 μL 2× PCR mix (Tiangen Biotech). For PCR amplification, an initial denaturation at 95°C for 5 minutes was performed followed by 36 cycles at 95°C for 30 seconds, 64°C for 50 seconds, 72°C for 20 seconds, and a final extension at 72°C for 10 minutes. MseI (New England Biolabs, Beverly, MA, USA) was used to detect this A–C transition. The IL-18 CC genotype was expected to show three DNA bands at the positions of 199 bp, 73 bp, and 29 bp, whereas the AA genotype was expected to show three bands (101/98 bp, 73 bp and 29 bp), and the heterozygote was expected to have four bands (199 bp, 101/98 bp, 73 bp, and 29 bp). To confirm the genotyping results, 20% PCR-amplified DNA samples were examined by DNA sequence, and the results were 100% concordant.
ELISA assay for serum IL-18 levels
Serum samples were collected from all the subjects. The blood samples were collected into serum tubes with an accelerating agent for serum separation and kept at a room temperature for 30 minutes before centrifugation for 20 minutes at a minimum of 1,500× g. Serum was then isolated and stored at -80°C until further use.
Serum IL-18 levels were measured by enzyme-linked immunosorbent assay (ELISA) kits (NeoBioscience Technology Co., Ltd, Shenzhen, People’s Republic of China) according to the manufacturer’s instructions.
Statistical analysis
The statistical analysis was performed using SPSS statistical software version 18.0 (SPSS Inc., Chicago, IL, USA). The genotype distribution and genotype frequencies were analyzed by chi-square test. The results are presented as mean ± standard deviation (SD). The data were analyzed by the nonparametric Mann–Whitney U-test. P-values <0.05 were considered to be statistically significant.
Results
The demographic and clinical characteristics of the subjects including NSCLC patients and healthy controls are shown in Table 1. Most of the NSCLC patients had squamous cell carcinoma (52.2%) and adenocarcinoma (47.8%). A total of 23.6% patients had NSCLC stage I+II and 76.4% had stage III+V.
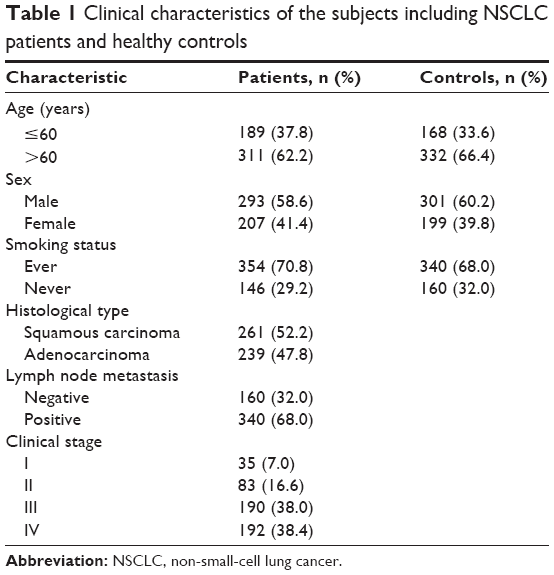 | Table 1 Clinical characteristics of the subjects including NSCLC patients and healthy controls |
In this study, the genotype and allele frequency of IL-18 -607 A/C polymorphism were detected for the first time in Chinese NSCLC patients and controls. The results showed that the AA/AC genotype distribution in the NSCLC patients was significantly higher than that of the controls (P=0.02), and a significant difference (P<0.07) was observed between the homozygous AA and CC genotypes (Table 2).
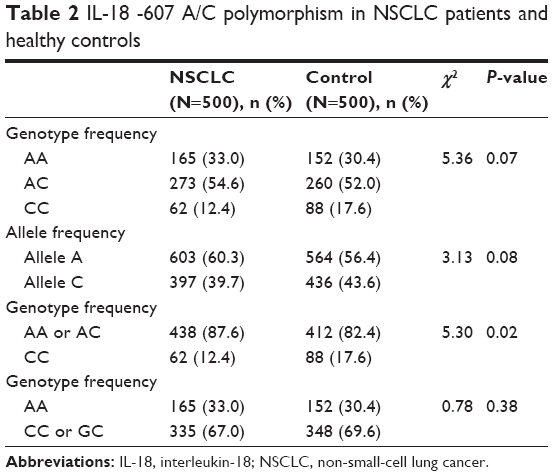 | Table 2 IL-18 -607 A/C polymorphism in NSCLC patients and healthy controls |
To verify the association between the IL-18 -607 A/C polymorphism and clinical characteristic features, we performed stratified analyses for combined genotypes – AA genotype versus AC + CC genotype and CC genotype versus AC + AA genotype – in NSCLC patients according to age at admission, sex, smoking status, histological type, lymph node metastasis, and clinical stage. Unfortunately, no significant differences were found (Table 3).
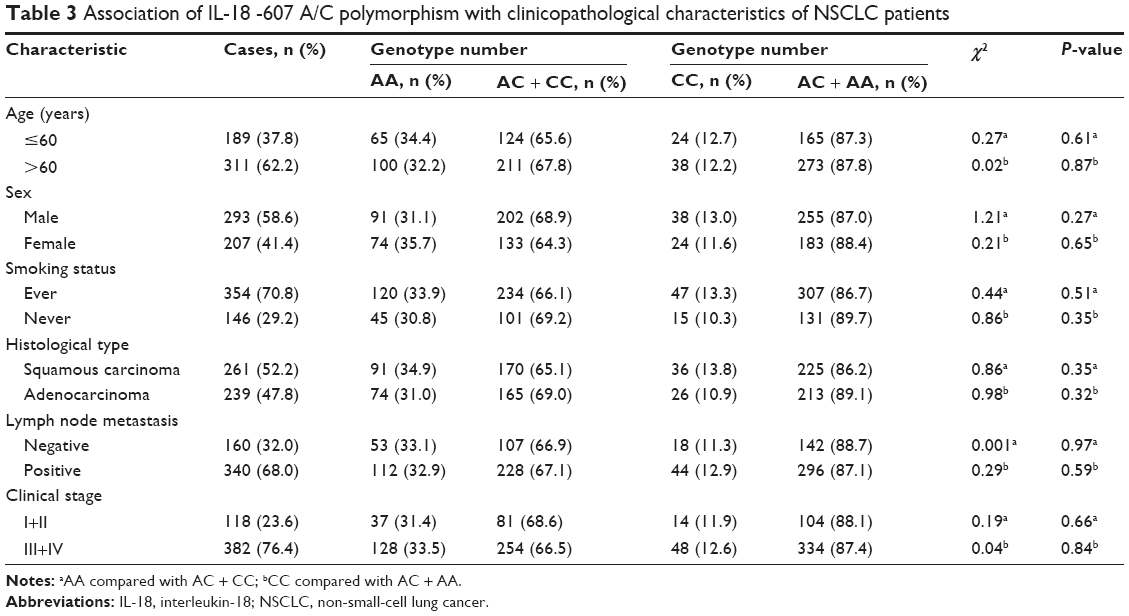 | Table 3 Association of IL-18 -607 A/C polymorphism with clinicopathological characteristics of NSCLC patients |
The serum IL-18 levels were determined using ELISA. The results demonstrated that the IL-18 expression was significantly increased in NSCLC patients compared with the controls (P=0.01) (as shown in Figure 1). According to the genotype distribution, the 90 NSCLC patients were divided into three subgroups: 30 patients with AA genotype, 40 with AC, and 20 with CC. No association was found between serum IL-18 levels and different genotypes (as shown in Figure 2).
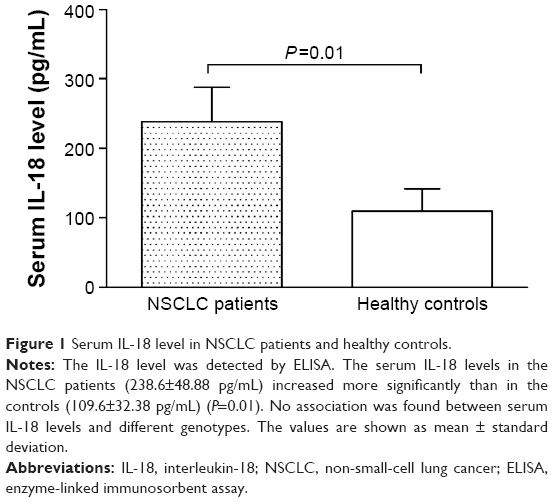 | Figure 1 Serum IL-18 level in NSCLC patients and healthy controls. |
 | Figure 2 Serum IL-18 level in different genotypes of NSCLC patients. |
Discussion
Lung cancer is the most common malignancy worldwide, and the pathogenesis of this disease is still unclear. In recent years, the important role played by genetic predisposition in lung cancer has promoted substantial interest. IL-18 is a pleiotropic proinflammatory cytokine. This is the first report that describes a comprehensive assessment of the relationship between IL-18 -607 A/C polymorphism and NSCLC risk and whether this polymorphism influences its occurrence in the Chinese Han population.
In this study, the PCR–RFLP method was used to detect IL-18 gene -607A/C, and an ELISA kit was used to determine serum IL-18 levels. The results showed that the AA/AC genotype distribution in the NSCLC patients was significantly higher than that in the controls (P=0.02). Furthermore, stratified analyses for combined genotypes, AA genotype versus AC + CC genotype and CC genotype versus AC + AA genotype, were performed in NSCLC patients according to age at admission, sex, smoking status, histological type, lymph node metastasis, and clinical stage. However, no significant differences were found, implying that the IL-18 expression increased significantly in NSCLC patients (P=0.01) regardless of their clinical characteristics. According to the genotype distribution, no association was found between serum IL-18 levels and different genotypes, which is inconsistent with a previous report,23 possibly because of the different ethnic population.
In conclusion, the current study demonstrates the important role of IL-18 -607 A/C polymorphism in increasing the risk of NSCLC in the Chinese population, but this SNP could not functionally affect the IL-18 levels. Thus, further studies are needed in a larger and ethnically different population to confirm this genetic influence on lung cancer.
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
Dinarello CA. IL-18: a TH1-inducing, proinflammatory cytokine and new member of the IL-1 family. J Allergy Clin Immunol. 1999;103(1 Pt 1):11–24. | ||
Tian H, Shi G, Yang G, et al. Cellular immunotherapy using irradiated lung cancer cell vaccine co-expressing GM-CSF and IL-18 can induce significant antitumor effects. BMC Cancer. 2014;14:48. | ||
Naumnik W, Naumnik B, Niewiarowska K, Ossolinska M, Chyczewska E. Angiogenic axis angiopoietin-1 and angiopoietin-2/Tie-2 in non-small cell lung cancer: a bronchoalveolar lavage and serum study. Adv Exp Med Biol. 2013;788:341–348. | ||
Rovina N, Hillas G, Dima E, et al. VEGF and IL-18 in induced sputum of lung cancer patients. Cytokine. 2011;54(3):277–281. | ||
Kalina U, Ballas K, Koyama N, et al. Genomic organization and regulation of the human interleukin-18 gene. Scand J Immunol. 2000;52(6):525–530. | ||
Marshall DJ, Rudnick KA, McCarthy SG, et al. Interleukin-18 enhances Th1 immunity and tumor protection of a DNA vaccine. Vaccine. 2006;24(3):244–253. | ||
Wang ZY, Gaggero A, Rubartelli A, et al. Expression of interleukin-18 in human ovarian carcinoma and normal ovarian epithelium: evidence for defective processing in tumor cells. Int J Cancer. 2002;98(6):873–878. | ||
Nicolini A, Carpi A, Rossi G. Cytokines in breast cancer. Cytokine Growth Factor Rev. 2006;17(5):325–337. | ||
Pages F, Berger A, Henglein B, et al. Modulation of interleukin-18 expression in human colon carcinoma: consequences for tumor immune surveillance. Int J Cancer. 1999;84(3):326–330. | ||
Wen Z, Ouyang Q, Chen D, Su X. [Interleukin 18 expression in colon cancer and adenoma]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2003;34(2):262–264. Chinese. | ||
Ye ZB, Ma T, Li H, Jin XL, Xu HM. Expression and significance of intratumoral interleukin-12 and interleukin-18 in human gastric carcinoma. World J Gastroenterol. 2007;13(11):1747–1751. | ||
Lebel-Binay S, Thiounn N, De Pinieux G, et al. IL-18 is produced by prostate cancer cells and secreted in response to interferons. Int J Cancer. 2003;106(6):827–835. | ||
Park H, Byun D, Kim TS, et al. Enhanced IL-18 expression in common skin tumors. Immunol Lett. 2001;79(3):215–219. | ||
Giedraitis V, He B, Huang WX, Hillert J. Cloning and mutation analysis of the human IL-18 promoter: a possible role of polymorphisms in expression regulation. J Neuroimmunol. 2001;112(1–2):146–152. | ||
Gracie JA, Koyama N, Murdoch J, et al. Disease association of two distinct interleukin-18 promoter polymorphisms in Caucasian rheumatoid arthritis patients. Genes Immun. 2005;6(3):211–216. | ||
Mojtahedi Z, Naeimi S, Farjadian S, Omrani GR, Ghaderi A. Association of IL-18 promoter polymorphisms with predisposition to type 1 diabetes. Diabet Med. 2006;23(3):235–239. | ||
Zhao H, Zhang Y, Xiao G, Wu N, Xu J, Fang Z. Interleukin-18 gene promoter- -607 A/C polymorphism and the risk of immune thrombocytopenia. Autoimmunity. 2014;47(7):478–481. | ||
Tsai HT, Hsin CH, Hsieh YH, et al. Impact of interleukin-18 polymorphisms -607A/C and -137G/C on oral cancer occurrence and clinical progression. PloS One. 2013;8(12):e83572. | ||
Taheri M, Hashemi M, Eskandari-Nasab E, et al. Association of -607 C/A polymorphism of IL-18 gene (rs1946518) with breast cancer risk in Zahedan, Southeast Iran. Prague Med Rep. 2012;113(3):217–222. | ||
Liu JM, Liu JN, Wei MT, et al. Effect of IL-18 gene promoter polymorphisms on prostate cancer occurrence and prognosis in Han Chinese population. Genet Mol Res. 2013;12(1):820–829. | ||
Nikiteas N, Yannopoulos A, Chatzitheofylaktou A, Tsigris C. Heterozygosity for interleukin-18 -607 A/C polymorphism is associated with risk for colorectal cancer. Anticancer Res. 2007;27(6B):3849–3853. | ||
Farjadfar A, Mojtahedi Z, Ghayumi MA, Erfani N, Haghshenas MR, Ghaderi A. Interleukin-18 promoter polymorphism is associated with lung cancer: a case-control study. Acta Oncol. 2009;48(7):971–976. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.