Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
The Influence of Age and Experience on Safety Climate Perceptions Among Healthcare Staff in Operating, Interventional Radiology, and Hybrid Operating Rooms: A Cross-Sectional Study
Authors Rhodin J, Erestam S ![]() , Bazzi M, Milton J, Strömberg S, Pettersson M
, Bazzi M, Milton J, Strömberg S, Pettersson M
Received 29 August 2025
Accepted for publication 20 December 2025
Published 17 January 2026 Volume 2026:19 538494
DOI https://doi.org/10.2147/JMDH.S538494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Johanna Rhodin,1,2 Sofia Erestam,1,2 May Bazzi,1,2 Jenny Milton,2,3 Sofia Strömberg,4,5 Monica Pettersson2
1Department of Hybrid and Interventional Procedures, Vascular Unit, Sahlgrenska University Hospital, Gothenburg, Sweden; 2Institute of Health and Care Science, University of Gothenburg, Gothenburg, Sweden; 3Department of Acute Medicine and Geriatrics, Sahlgrenska University Hospital, Gothenburg, Sweden; 4Institute of Medicine, Department of Molecular and Clinical Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 5Department of Vascular Surgery, Sahlgrenska University Hospital, Gothenburg, Sweden
Correspondence: Monica Pettersson, Institute of Health and Care science, University of Gothenburg, Box 457, Gothenburg, 405 30, Sweden, Tel +46 31786 60 45, Email [email protected]
Introduction: Patient safety is a critical priority in high-risk environments like operating rooms, interventional radiology rooms, and hybrid operating rooms, where complex procedures and multidisciplinary teams are involved.
Purpose: This study explores healthcare staff perceptions of safety climate across the operating, interventional, and hybrid operating rooms, aiming to identify areas for improvement to promote a safer, more collaborative environment.
Patients and Methods: A cross-sectional study was conducted using a modified Swedish version of the Safety Attitudes Questionnaire - Operating Room. Participants included physicians, nurses, and nurse assistants from the Operating, Interventional Radiology, and Hybrid Operating Room at a Swedish university hospital. Differences in safety climate perceptions were analyzed across professional groups and based on demographics including age and length of experience.
Results: Among 180 healthcare staff members (44.8% response rate), no significant differences in safety attitudes were found between professional groups or multidisciplinary teams. Significant differences were observed across age groups in the domains of teamwork climate (p = 0.035), job satisfaction (p = 0.015), and perception of management (p = 0.021). Differences were also found across experience groups for working conditions (p = 0.029), stress recognition (p = 0.041), and perception of management (p = 0.046). Qualitative analysis highlighted the importance of staff retention, effective communication, and continuous professional development in improving patient safety.
Conclusion: Safety climate perceptions vary significantly with age and experience rather than professional role. These findings highlight the importance of fostering inclusive team dynamics that integrate diverse experience levels and implementing targeted strategies focused on staff retention, communication, and education to strengthen the overall safety climate.
Keywords: healthcare staff, multidisciplinary team, patient safety, safety climate, safety attitudes questionnaire
Introduction
Medical advancements continue to progress, leading to a growing demand for more advanced care and additional examinations, due to the aging population and longer life expectancy.1 Patient safety is a central priority in healthcare, especially in high-risk environments like operating rooms (OR),2 Interventional radiology (IR) rooms,3 and hybrid operating rooms (Hybrid OR).4,5 These environments involve complex, invasive procedures often requiring the use of multidisciplinary teams and advanced technologies.6 As healthcare settings become more complex and technically demanding, they are being exploited for a wider range of procedures across various patient groups.7 It has been shown that the risk of harm is higher for patients undergoing more complex procedures.8,9 Many adverse events in these settings are linked to factors such as poor communication,10,11 organizational issues,12 and teamwork failure,6,13 problems that could be prevented.14
In recent years, IR has grown as a field in healthcare.15 Minimally invasive procedures can often replace surgery or be part of an open procedure. These treatments are less traumatic for patients though they do not require large incisions, leading to less pain and shorter recovery time.16 If complication occurs during minimally invasive procedures, the patient treatment may need to be converted to open surgery.17 A hybrid OR combines traditional surgery and IR in one space. This setup reduces the need for risky patient transfers and may improve patient safety.4,18,19
A strong safety culture and positive climate are essential for reducing risks and improving patient safety.5,20 Safety culture refers to the shared values, beliefs, and attitudes toward safety in the organization.21 Safety climate is shaped by healthcare staff perceptions of the organization´s safety guidelines and procedures. Both safety culture and climate affect healthcare staff behave daily, such as following protocols, communicating concerns, and reporting errors.22,23
In high-risk environments like OR, IR and Hybrid OR, positive safety attitudes among healthcare staff lead to better teamwork,24 open communication,12 and adherence to safety protocols, which ultimately improve patient outcomes.22
The operation and interventional radiology sectors are continuously evolving, and integrating these activities has led to the emergence of hybrid environments.25 Hybrid operating rooms offer clinical advantages, they also bring professionals from distinct disciplines such as surgery, anesthesia, and interventional radiology. These groups often differ in work routines, communication patterns, and safety priorities, which may influence how safety climate is perceived in these integrated environments. Understanding their dynamics is important to identify potential variations and areas for improvement in patient safety culture. Although safety climate has been studied in both operating room and interventional radiology settings,26,27 research focusing on hybrid operating room remain limited. This study aims to explore safety climate perceptions among healthcare staff working in Operating Rooms, Interventional Radiology, and Hybrid Operating Room settings, by identifying potential differences and contributing factors that may influence patient safety. These findings aim to inform targeted interventions that could improve the overall safety climate across these critical teams in healthcare settings.
Methods
Study Design and Setting
This study used a cross-sectional questionnaire to explore the safety attitudes of healthcare staff at a university hospital in Sweden. The questionnaire was sent to healthcare staff working in the OR, IR room, and hybrid OR.
The Safety Attitudes Questionnaire – Operating Room
The Safety Attitudes Questionnaire (SAQ) is a tool used to assess the safety attitudes of healthcare staff and understand the safety climate within healthcare organizations.22 The study used the Swedish translated Safety Attitudes Questionnaire – Operating Room (SAQ-OR) version to measure the safety climate.28 To ensure inclusion of healthcare staff working in the interventional radiology department, questions originally referring only to OR were modified to OR/IR room.29 The modified SAQ-OR consists of 71 questions, divided into four parts: Part 1 (Question 1–57): Items about the patient safety climate, Part 2 (Question 58–66): Items about how healthcare staff experience the quality of teamwork and communication between different healthcare staff groups, Part 3 (Question 67): An open question, asking respondents to list their top three recommendations for improving patient safety in the OR/IR room, Part 4 (Question 68–71): Demographic questions asking about the respondent´s age, job title, graduation year, and typical work shifts. Thirty of the items are divided into six key domains: Safety Climate (seven items), Teamwork climate (six items), Job Satisfaction (five items), Working Conditions (four items), Stress Recognition (four items), and Perception of Management (four items), (Table 1).
 |
Table 1 SAQ-OR Domains, Definitions, and Example Items22 |
To interpret the data, each response was converted from a modified Likert Scale (1=Strongly Disagree, 2=Disagree Slightly, 3=Neutral, 4=Agree Slightly, 5=Agree Strongly, and 6=Not Applicable) to a 100-point scale, where 100 is the most desirable score. The values were assigned as follows: 0=Strongly Disagree, 25=Disagree slightly, 50=Neutral, 75=Agree Slightly, 100=Agree Strongly, and Missing Value=Not Applicable. For two items (Question 12 and 24), the scores were reversed, meaning that a lower score on these questions indicated a more positive attitude. We then averaged the scores for each group, producing a final score between 0 and 100. A score ≥ 75 were considered positive. Any missing data or responses marked as “Not Applicable” were treated as missing and were excluded from the analysis.22,30
Participants
The target population for this study included healthcare staff working in the IR room, OR, or hybrid OR at a university hospital in Sweden. Participants represented a range of professional roles including anesthesiologists, surgeons, cardiologists, interventional radiologists, anesthesia nurses, operating room nurses, radiographers, registered nurses, and nurse assistants. Healthcare staff working in other areas of the hospital (not in patient care) were excluded from the study. Additionally, responses from participants who chose not to complete any of the questions, yet submitted the form, were excluded.
Participants were categorized into four main groups based on profession, multidisciplinary team, age and length of experience. The profession groups included: Physicians (anesthesiologists, surgeons, cardiologist, interventional radiologist), Registered Nurses (anesthesia nurses, operating room nurses, registered radiographers and non-specialized registered nurses), and Nurse Assistant. The multidisciplinary profession group consisted of: Anesthesia (anesthesiologists, and anesthesia nurses), Operation (surgeons, operating room nurses and nurse assistants), and Interventional Radiology (cardiologist, interventional radiologist, radiographers and registered nurses).
Participants were grouped by age: 20–39 years, 40–49 years, 50–59 years, and 60–69. Length of experience was categorized into six groups: less than 2 years, 3–5years, 6–9 years, 10–19 years, 20–39 years and more than 40 years to explore differences in safety attitudes. These categories were used to explore potential differences in safety attitudes across different groups.
Data Collection
Data were collected between June and October 2022. Healthcare staff were verbally informed at a meeting prior to the distribution of the questionnaire. Study information, along with a link to the questionnaire were emailed to the healthcare staff, and two reminder emails were sent to encourage participation.
The questionnaire was completed electronically via the Esmaker platform and took 10–15 minutes to finish. Participants were encouraged to complete the questionnaire during their work shift.
Data Analysis
The responses were exported from Esmaker into Microsoft Excel (Version 2408) and then transferred to IBM SPSS Statistics (Version: 28.0.1.1) for statistical analysis.
To assess the internal consistency of the questionnaire, Cronbach´s alpha was calculated for each domain. The following criteria were used to interpret Cronbach´s alpha: a value of ≥ 0.9 indicated excellent reliability, between 0.8 and 0.9 indicates good reliability, between 0.7 and 0.8 indicates acceptable reliability, between 0.6 and 0.7 indicates questionable, and between 0.5 and 0.6 indicates poor reliability.31,32 Shapiro–Wilk test was used to check for normal distribution. Data was not normally distributed, hence the Kruskal–Wallis test and post hoc pairwise comparisons to explore differences between groups. A significance level of p < 0.05 was applied for all statistical tests.
Question 67, the recommendation for improving patient safety, was analyzed using a summative content analysis approach.33 The responses were categorized into three groups: the Anesthesia group, the operation group, and the IR group. These groups were created to explore potential differences in the reactions between the different teams. The analysis involved reviewing the textual data to understand the content and identify relevant statements to patient safety. These statements were coded and grouped into categories based on the similarities. The frequency of each category was counted to see the most common recommendation for improving patient safety. The categories were analyzed to draw meaningful conclusions according to the summative approach.33 The first author (J.R) primarily performed the analysis with support from coauthors (S.E., M.B., J.M., and M.P) for refinement and credibility.34
Ethical Considerations
This study explores healthcare staffs’ safety attitudes in a hospital setting and were conducted in accordance with the principles outlined in the Helsinki Declaration.35 Participants received written information detailing the purpose of the study and were informed that data collection would be anonymous and handled confidentially. Before answering the questionnaire participants agreed to take part in the study, and at the end of the questionnaire, there was a statement confirming that by completing it, participants gave their consent to participate. The Swedish Ethical Review Authority had no ethical objections to the research project (Ref. No. 2021–06399-01).
Results
Questionnaires (n=402) were sent out via Email to healthcare staff. A total of n=180 healthcare staff completed the questionnaire, resulting in a response rate of 44.8%. Table 2 presents the internal consistency of Cronbach´s alpha, which present acceptable values 0.70–0.9032 in five out of the six domains.
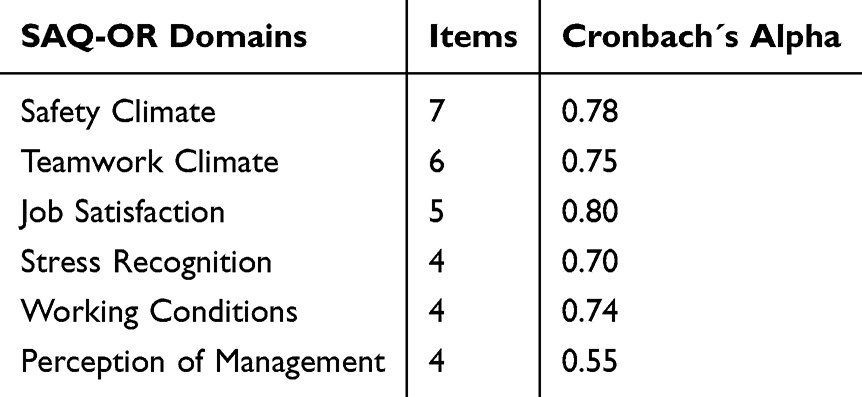 |
Table 2 Internal Consistency for Safety Attitudes Questionnaire – Operating Room |
The results indicated no statistically significant differences between professional groups or between multidisciplinary groups when analyzed separately. Significant differences were found across age groups in the following domains of teamwork climate (p=0.035), job satisfaction (p=0.015), and perception of management (p=0.021). Significant differences were observed across length of experience groups in the working conditions (p=0.029), stress recognition (p=0.041), and perception of management (p=0.046) domains Table 3.
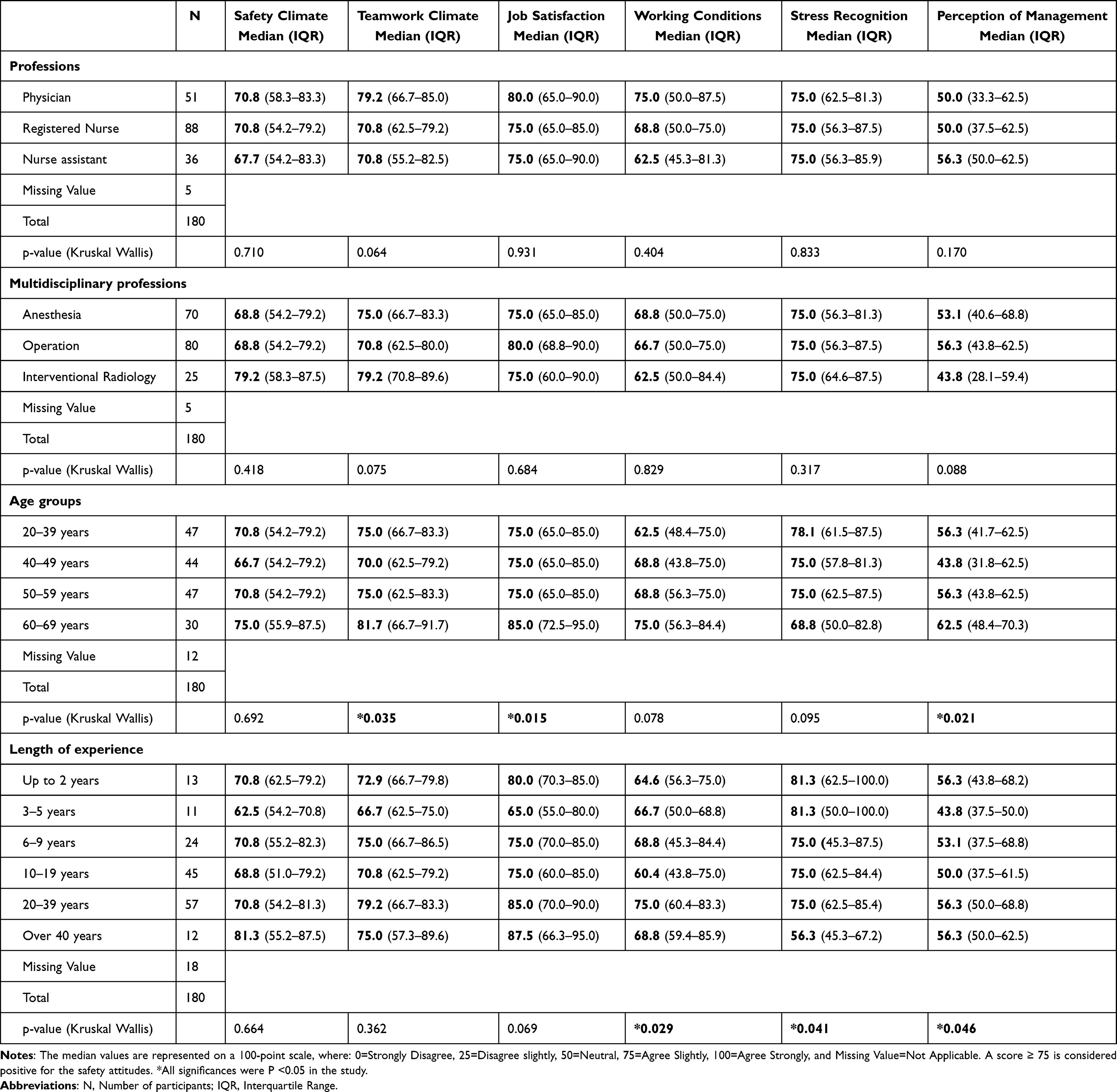 |
Table 3 Differences in SAQ-OR Factor Median Scores by Professions, Multidisciplinary Professions, Age Groups, and Length of Experience |
In the teamwork climate domain, significant differences were found between the age groups 20–39 years and 60–69 years (p=0.049), 40–49 years and 60–69 years (p=0.004), and 50–59 years and 60–69 years (p=0.040). Within the job satisfaction domain, significant differences were observed between 20–39 years and 60–69 years (p=0.015), 40–49 years and 60–69 years (p=0.002), and 50–59 years and 60–69 years (p=0.034). Within the perception of management domain, significant differences were noted between the age groups 40–49 years and 60 years (p=0.002).
In terms of length of experience, pairwise comparisons revealed significant difference in the working condition between the groups 10–19 years and 20–39 years of experience (p=0.002). For the stress recognition domain, significant differences were found between the groups <2 years and >40 years (p=0.02), 3–5 years and >40 years (p=0.016), 6–9 years and >40 (p=0.031), 10–19 years and >40 years (p=0.006), and 20–39 years and >40 years (0.014).
In the Perception of management domain, significant differences were observed between the groups 3–5 years and >40 (p=0.047), 3–5 years and 20–39 years (p=0.008), and 10–19 years and 20–39 years (p=0.014).
Of the 180 healthcare staff who completed the questionnaire, 117 responded to the open question, resulting in a response rate of 65%. Healthcare staffs’ recommendations for improving patient safety (question 67) revealed nine key items, Figure 1. The most common recommendation for improving patient safety were the retention of healthcare staff, the importance of effective communication, and competence and continuous education.
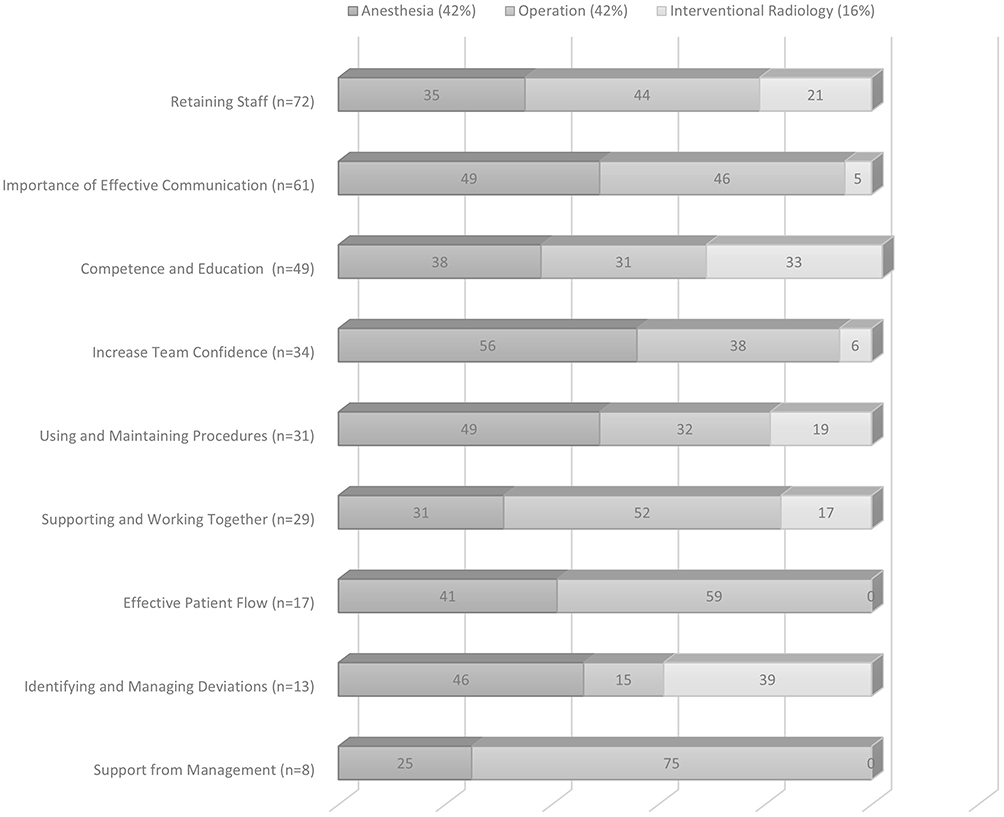 |
Figure 1 Top three recommendations for improving patient safety. N = number of responses. Values in the bar chart represent percentages. |
Discussion
This study aimed to explore the safety climate perception among healthcare staff in operating, intervention and hybrid settings, revealing several important findings. The analysis revealed differences in safety climate between younger and older healthcare staff, particularly in areas such as teamwork, job satisfaction, and management perception. These results highlight the importance of age-based perspectives in shaping team dynamics. No significant differences were found between the responses from different professional groups (physician, nurse, radiographers, and nurse assistant) or between the multidisciplinary teams (Anesthesia, Operation, and IR). This is different from previous studies, which have shown differences across professional groups where physicians often rate teamwork and collaboration higher in contrast to nurses.36–38
Working experience and older age has been associated with healthcare staffs’ attitudes toward patient safety.39,40 In this study significant differences were found across age groups. Healthcare staff aged 60 years and older reported higher satisfaction with teamwork compared to those aged 59 years or younger. This finding may suggest that experience and age contribute to a more positive perception of teamwork, which can influence attitudes toward safety and overall job satisfaction. Job satisfaction was higher among healthcare staff over the age of 60, which aligns with findings that healthcare staff who have worked longer in a specific unit or hospital report higher levels of job satisfaction,41,42 potentially reflecting a sense of fulfillment and stability in their roles. Healthcare staff can be influenced by their job satisfaction and their view of management within the healthcare setting.43
The perception of management varied across different levels of work experience. Healthcare staff with 3–5 years of experience and those with 20–39 years or more than 40 years of experience, reported a more positive view of management. Less experienced healthcare staff tend to have idealistic perceptions, focusing on support and mentorship from management,43 which is consistent with findings in the study where healthcare staff with 3–5 years of work experience expressed greater satisfaction of management. Notably the perception of management domain showed a Cronbach’s alpha of 0.55, indicating poor reliability.32
Regarding stress recognition, healthcare staff with less than 40 years of experience reported a greater impact from stressors such as fatigue and workload, while those with more than 40 years of experience were less affected. However, other studies have also shown that older healthcare staff tend to report higher levels of stress recognition.39 This domain of stress recognition may be subject to misunderstanding, as there is a possibility that respondents are evaluating their personal stress levels rather than assessing the work environment. This could potentially lead to misleading results.44 The relationship between stress, job satisfaction, and safety perceptions highlights the human aspect of these findings. More experienced staff may handle stress more effectively, leading to greater job satisfaction and a stronger sense of safety within teams.
In the summative analysis, anesthesia, operation, and IR teams all emphasized the importance of retaining healthcare staff to improve patient safety. Working with reduced healthcare staff can create a stressful work environment, leading to staff overloaded with responsibilities. This overload can result in fewer tasks being completed or delays in operations, as the overall efficiency and performance of the team.45 Previous study has highlighted the significant impact of healthcare staff turnover, particularly among nurses and physicians.46 The healthcare system faces challenges in recruiting younger generations of workers, who thinks nursing is an unattractive profession due to low salaries and limited job status.47 Physicians and nurses are leaving the medical field due to insufficient training opportunities and salary relative to their work conditions.48,49
These findings align with the quantitative results, where less experienced staff reported higher stress recognition and lower job satisfaction. This suggests that stress and workload may contribute to retention issues and reinforce the need to continuous education, mentorship and supportive leadership, recommendations that were strongly emphasized in the qualitative responses. These results highlight that supportive management, mentorship, and continuous learning opportunities can help reduce stress, strengthen staff well-being, and enhance patient safety. Promoting interprofessional learning and mutual understanding of each profession’s roles, for example through job shadowing, may further improve communication and collaboration within teams. The integration of Interventional Radiology into the operating environment may also affect safety culture. IR teams have traditionally worked more independently, and adapting to multidisciplinary collaboration requires shared communication practices and mutual understanding.50
This study suggests that prioritizing effective communication can significantly improve patient safety, a finding supported by research51 highlighting the importance of collaboration and clear communication within well-coordinated healthcare teams. Communication errors pose a risk to patient safety, often due to delayed information sharing or missing details. These issues can lead to inefficiencies among healthcare staff, create tension within the teams, and ultimately delay the care process.10,52 Therefore, it is crucial to ensure that incidents or errors are reported through deviation reporting, as this allows healthcare staff to learn from each other and improve practices, ultimately reducing risk of patient harm.5,53
Strengths and Limitations
This study’s strengths lie in its multidisciplinary approach, which includes input from various healthcare staff. By incorporating a diverse range of professionals, the study provides comprehensive view of the perspectives and experiences across the healthcare staff. Participants were divided into length of experience and age group, allowing for more granular analysis of potential differences in healthcare staff perspectives. Despite its strengths, this study has limitations. The missing data were not imputed, which could have influenced the results.28 Furthermore, the response rate was relatively low, which may have impacted the generalizability of the findings.
Conclusion
This study found differences in healthcare staff´s perception of teamwork, job satisfaction, and management across age groups and years of experience. Healthcare staff provided valuable recommendations for improving patient safety, with a strong focus on staff retention, effective communication, and continuous education. These findings highlight the importance of incorporating diverse age groups and levels of experiences within multidisciplinary teams to improve the safety climate and overall team dynamics. Future initiatives could include implementing structured mentorship programs that pair experienced and younger staff to enhance communication and job satisfaction, as well as developing targeted strategies to support staff retention and continuous education. Such interventions could strengthen collaboration and contribute to a more sustainable and positive safety climate. Further research across different institutions, both nationally and internationally, is recommended to explore how local practices and organizational cultures may influence safety climate perceptions.
Abbreviations
IR, Interventional Radiology; IQR, Interquartile Range; OR, Operating Room; SAQ, Safety Attitude Questionnaire; SAQ-OR, Safety Attitudes Questionnaire -Operating Room.
Acknowledgments
We kindly would like to thank all participants in the study who took their time to answer the questionnaires. We would also like to thank Magnus Pettersson for his essential help with the statistical analysis in this study. A PhD fellowship was received by J.R. and granted by the Department of Hybrid and Interventional procedures, Vascular Unit, Sahlgrenska University Hospital, Gothenburg, Sweden, and the Institute of Health and Care Sciences, University of Gothenburg.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Van den Heede K, Bouckaert N, Van de Voorde C. The impact of an ageing population on the required hospital capacity: results from forecast analysis on administrative data. Eur Geriatr Med. 2019;10(5):697–11. doi:10.1007/s41999-019-00219-8
2. Alfredsdottir H, Bjornsdottir K. Nursing and patient safety in the operating room. J Adv Nurs. 2008;61(1):29–37. doi:10.1111/j.1365-2648.2007.04462.x
3. Wallin A, Bazzi M, Ringdal M, Ahlberg K, Lundén M. Radiographers’ perception of patient safety culture in radiology. Radiography. 2023;29(3):610–616. doi:10.1016/j.radi.2023.04.005
4. Jin H, Lu L, Liu J, Cui M. A systematic review on the application of the hybrid operating room in surgery: experiences and challenges. Updates Surg. 2022;74(2):403–415. doi:10.1007/s13304-021-00989-6
5. World Health Organisation. Global patient safety action plan 2021-2030 - towards eliminating avoidableharm in health care. 2021.
6. Boet S, Burns JK, Brehaut J, et al. Analyzing interprofessional teamwork in the operating room: an exploratory observational study using conventional and alternative approaches. J Interprof Care. 2023;37(5):715–724. doi:10.1080/13561820.2023.2171373
7. Zegers M, de Bruijne MC, de Keizer B, et al. The incidence, root-causes, and outcomes of adverse events in surgical units: implication for potential prevention strategies. Patient Saf Surg. 2011;5(1):13. doi:10.1186/1754-9493-5-13
8. Mavros MN, Bohnen JD, Ramly EP, et al. Intraoperative adverse events: risk adjustment for procedure complexity and presence of adhesions is crucial. J Am Coll Surg. 2015;221(2):345–353. doi:10.1016/j.jamcollsurg.2015.03.045
9. Hanssen I, Smith Jacobsen IL, Skråmm SH. Non-technical skills in operating room nursing: ethical aspects. Nurs Ethics. 2020;27(5):1364–1372. doi:10.1177/0969733020914376
10. Gillespie BM, Chaboyer W, Fairweather N. Interruptions and miscommunications in surgery: an observational study. Aorn J. 2012;95(5):576–590. doi:10.1016/j.aorn.2012.02.012
11. Bazzi M, Bergbom I, Hellström M, Fridh I, Ahlberg K, Lundgren SM. Team composition and staff roles in a hybrid operating room: a prospective study using video observations. Nurs Open. 2019;6(3):1245–1253. doi:10.1002/nop2.327
12. Arad D, Finkelstein A, Rozenblum R, Magnezi R. Patient safety and staff psychological safety: a mixed methods study on aspects of teamwork in the operating room. Front Public Health. 2022;10:1060473. doi:10.3389/fpubh.2022.1060473
13. Mazzocco K, Petitti DB, Fong KT, et al. Surgical team behaviors and patient outcomes. Am J Surg. 2009;197(5):678–685. doi:10.1016/j.amjsurg.2008.03.002
14. Christian CK, Gustafson ML, Roth EM, et al. A prospective study of patient safety in the operating room. Surgery. 2006;139(2):159–173. doi:10.1016/j.surg.2005.07.037
15. Brock KK, Chen SR, Sheth RA, Siewerdsen JH. Imaging in interventional radiology: 2043 and beyond. Radiology. 2023;308(1):e230146. doi:10.1148/radiol.230146
16. Tonutti M, Elson DS, Yang GZ, Darzi AW, Sodergren MH. The role of technology in minimally invasive surgery: state of the art, recent developments and future directions. Postgrad Med J. 2017;93(1097):159–167. doi:10.1136/postgradmedj-2016-134311
17. Sabharwal T, Fotiadis N, Adam A. Modern trends in interventional radiology. Br Med Bull. 2007;81-82(1):167–182. doi:10.1093/bmb/ldm006
18. Kpodonu J, Raney A. The cardiovascular hybrid room a key component for hybrid interventions and image guided surgery in the emerging specialty of cardiovascular hybrid surgery. Interact Cardiovasc Thorac Surg. 2009;9(4):688–692. doi:10.1510/icvts.2009.209429
19. Drevets P, Chung JM, Schampaert S, Schroeder C. Hybrid operating room: one-stop-shop for diagnosis, staging, and treatment. Innovations. 2019;14(5):463–467. doi:10.1177/1556984519863800
20. Alanazi FK, Sim J, Lapkin S. Systematic review: nurses’ safety attitudes and their impact on patient outcomes in acute-care hospitals. Nurs Open. 2022;9(1):30–43. doi:10.1002/nop2.1063
21. Sammer CE, Lykens K, Singh KP, Mains DA, Lackan NA. What is patient safety culture? A review of the literature. J Nurs Scholarsh. 2010;42(2):156–165. doi:10.1111/j.1547-5069.2009.01330.x
22. Sexton JB, Helmreich RL, Neilands TB, et al. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6(1):44. doi:10.1186/1472-6963-6-44
23. Skråmm SH, Smith Jacobsen IL, Hanssen I. Communication as a non-technical skill in the operating room: a qualitative study. Nurs Open. 2021;8(4):1822–1828. doi:10.1002/nop2.830
24. Weller J, Boyd M, Cumin D. Teams, tribes and patient safety: overcoming barriers to effective teamwork in healthcare. Postgrad Med J. 2014;90(1061):149–154. doi:10.1136/postgradmedj-2012-131168
25. ten Cate G, Fosse E, Hol PK, et al. Integrating surgery and radiology in one suite: a multicenter study. J Vasc Surg. 2004;40(3):494–499. doi:10.1016/j.jvs.2004.06.005
26. Bjällmark A, Persson V, Karlsson B, Bazzi M. Exploring attitudes toward safety climate: a cross-sectional study among interventional radiology team members using the Safety Attitudes Questionnaire (SAQ). Discover Health Syst. 2024;3(1):16. doi:10.1007/s44250-024-00081-x
27. Göras C, Unbeck M, Nilsson U, Ehrenberg A. Interprofessional team assessments of the patient safety climate in Swedish operating rooms: a cross-sectional survey. BMJ open. 2017;7(9):e015607. doi:10.1136/bmjopen-2016-015607
28. Göras C, Wallentin FY, Nilsson U, Ehrenberg A. Swedish translation and psychometric testing of the safety attitudes questionnaire (operating room version). BMC Health Serv Res. 2013;13(1):104. doi:10.1186/1472-6963-13-104
29. Erestam S, Haglind E, Bock D, Andersson AE, Angenete E. Changes in safety climate and teamwork in the operating room after implementation of a revised WHO checklist: a prospective interventional study. Patient Saf Surg. 2017;11(1):4. doi:10.1186/s13037-017-0120-6
30. Sexton JB, Makary MA, Tersigni AR, et al. Teamwork in the operating room: frontline perspectives among hospitals and operating room personnel. Anesthesiology. 2006;105(5):877–884. doi:10.1097/00000542-200611000-00006
31. Bland JM, Altman DG. Cronbach’s alpha. BMJ. 1997;314(7080):572. doi:10.1136/bmj.314.7080.572
32. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
33. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
34. Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J Occup Ther. 1991;45(3):214–222. doi:10.5014/ajot.45.3.214
35. (WMA) WMA. Declaration of Helsinki: ethical principles for medical research involving human subjects. 2024. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki/.
36. Flin R, Yule S, McKenzie L, Paterson-Brown S, Maran N. Attitudes to teamwork and safety in the operating theatre. Surgeon. 2006;4(3):145–151. doi:10.1016/s1479-666x(06)80084-3
37. Makary MA, Sexton JB, Freischlag JA, et al. Operating room teamwork among physicians and nurses: teamwork in the eye of the beholder. J Am Coll Surg. 2006;202(5):746–752. doi:10.1016/j.jamcollsurg.2006.01.017
38. Mills P, Neily J, Dunn E. Teamwork and communication in surgical teams: implications for patient safety. J Am Coll Surg. 2008;206(1):107–112. doi:10.1016/j.jamcollsurg.2007.06.281
39. Nyberg A, Olofsson B, Fagerdahl A, Haney M, Otten V. Longer work experience and age associated with safety attitudes in operating room nurses: an online cross-sectional study. BMJ Open Qual. 2024;13(1):e002182. doi:10.1136/bmjoq-2022-002182
40. Danielsson M, Nilsen P, Rutberg H, Årestedt K. A national study of patient safety culture in hospitals in Sweden. J Patient Saf. 2019;15(4):328–333. doi:10.1097/pts.0000000000000369
41. Hayes B, Bonner A, Pryor J. Factors contributing to nurse job satisfaction in the acute hospital setting: a review of recent literature. J Nurs Manag. 2010;18(7):804–814. doi:10.1111/j.1365-2834.2010.01131.x
42. Voltmer E, Rosta J, Köslich-Strumann S, Goetz K. Job satisfaction and work stress among physicians in Norway and Germany-A cross-sectional study. PLoS One. 2024;19(1):e0296703
43. Moya D, Guilabert M, Manzanera R, et al. Differences in perception of healthcare management between patients and professionals. Int J Environ Res Public Health. 2023;20(5):3842. doi:10.3390/ijerph20053842
44. Taylor JA, Pandian R. A dissonant scale: stress recognition in the SAQ. BMC Res Notes. 2013;6(1):302. doi:10.1186/1756-0500-6-302
45. Eklöf M, Törner M, Pousette A. Organizational and social-psychological conditions in healthcare and their importance for patient and staff safety. A critical incident study among doctors and nurses. Saf Sci. 2014;70:211–221. doi:10.1016/j.ssci.2014.06.007
46. De Vries N, Lavreysen O, Boone A, et al. Retaining healthcare workers: a systematic review of strategies for sustaining power in the workplace. Healthcare. 2023;11(13). doi:10.3390/healthcare11131887
47. Wu LT, Low MM, Tan KK, Lopez V, Liaw SY. Why not nursing? A systematic review of factors influencing career choice among healthcare students. Int Nurs Rev. 2015;62(4):547–562. doi:10.1111/inr.12220
48. Kabbash I, El-Sallamy R, Zayed H, Alkhyate I, Omar A, Abdo S. The brain drain: why medical students and young physicians want to leave Egypt. East Mediterr Health J. 2021;27(11):1102–1108. doi:10.26719/emhj.21.050
49. Marufu TC, Collins A, Vargas L, Gillespie L, Almghairbi D. Factors influencing retention among hospital nurses: systematic review. Br J Nurs. 2021;30(5):302–308. doi:10.12968/bjon.2021.30.5.302
50. Bazzi M. Patients and Staff in the hybrid operating room. Experiences Challenges. 2019.
51. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004;13 Suppl 1(Suppl 1):i85–90. doi:10.1136/qhc.13.suppl_1.i85
52. Lingard L, Espin S, Whyte S, et al. Communication failures in the operating room: an observational classification of recurrent types and effects. Qual Saf Health Care. 2004;13(5):330–334. doi:10.1136/qhc.13.5.330
53. Kim M. The effectiveness of error reporting promoting strategy on nurse’s attitude, patient safety culture, intention to report and reporting rate. J Korean Acad Nurs. 2010;40(2):172–181. doi:10.4040/jkan.2010.40.2.172
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.