")
Back to Journals » Journal of Healthcare Leadership » Volume 14
The Impact of Total Automaton on the Clinical Laboratory Workforce: A Case Study
Authors Al Naam YA, Elsafi S , Al Jahdali MH, Al Shaman RS, Al-Qurouni BH, Al Zahrani EM
Received 15 February 2022
Accepted for publication 15 April 2022
Published 9 May 2022 Volume 2022:14 Pages 55—62
DOI https://doi.org/10.2147/JHL.S362614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Yaser A Al Naam,1 Salah Elsafi,1 Majed H Al Jahdali,2 Randa S Al Shaman,3 Bader H Al-Qurouni,4 Eidan M Al Zahrani5
1Clinical Laboratory Sciences Department, Prince Sultan Military Colleges of Health Sciences, Dhahran, Saudi Arabia; 2Human Resources Directorate, Prince Sultan Military Colleges of Health Sciences, Dhahran, Saudi Arabia; 3Department of Medical Laboratory, King Salman Armed Forces Hospital, Tabuk, Saudi Arabia; 4Department of Medical Laboratory, King Fahad Military Medical Complex, Dhahran, Saudi Arabia; 5Prince Sultan Military Colleges of Health Sciences, Dhahran, Saudi Arabia
Correspondence: Salah Elsafi, Clinical Laboratory Sciences Department, Prince Sultan Military Colleges of Health Sciences, P.O. Box 33048, Dhahran, 31448, Saudi Arabia, Email [email protected]; [email protected]
Background: There has been a significant concern that total automation can decrease the need for laboratory personnel at all levels. The objective of this study was to investigate the impact of total laboratory automation on the clinical laboratory workforce.
Methods: A one-year data including the demographical features of laboratory workforce and technical productivity of laboratory tests were provided by two medical laboratory departments of similar profile and different equipment setup; one adopting a total automation system and the other utilizing discrete analysis system. The technical productivities of the two laboratories were compared and statistically tested.
Results: A similar technical productivity per single laboratory worker was noted in the hematology section in each of the two sites with no significant difference (average odd radio = 0.9, p = 0.79). However, with total automation, the number of tests performed per single worker has increased to an average of 1.4 and 3.7 times with total automation in the clinical chemistry and serology sections, respectively (p ≤ 0.001).
Conclusion: Total laboratory automation improves the productivity of the laboratory, leading to a decreased laboratory workforce. The laboratory workload has increased steadily therefore, the existing laboratory workforce, in the absence of automation, could not have been able to maintain the current volume of service. Adoption of automation reduces repetitive manual labor, thereby allowing the redefinition of the job roles of the laboratory workforce. TLA is ideal for laboratories that suffer from workforce shortages or managing high volume testing with less staff.
Keywords: laboratory automation, workforce, demography, productivity, Saudi Arabia
Introduction
The introduction of electronics, robotics, and highly advanced technical methodologies has led to the expansion of clinical laboratory automation. Automation is one of the greatest breakthrough in the recent history of the diagnostics laboratory sciences. Laboratory automation began in the 1950s and has progressed throughout the decades to reduce the turnaround times in laboratory testing and eliminate the human errors.1 By replacing the repetitive and laborious manual processes involved in laboratory testing, automation has reduced the overall errors and allowed laboratory technicians to focus more time and energy on quality assurance.2
Laboratory automation has been achieved using many types of instruments and equipment. Each automation system is chosen for individual laboratories based on their workflow and demand. One type of machine that improves laboratory automation is the automated analyzer. These machines generally measure various chemical and biological characteristics with minimal human assistance. Automated analyzers are classified into continuous flow, which function by analyzing a continuously flowing stream of the sample through processes such as filtration and the introduction of reagents. They may also measure characteristics sequentially.3 Another form of laboratory automation is the discrete analyzer, which allows for the rapid analysis of liquid samples kept in discrete cells throughout the analytic process.4
Automation can also be applied to all the steps used to perform through manual assays, including specimen procurement, reagent delivery, reaction step, measurement phase, and data analysis.5 A total laboratory automation (TLA) means that a track system connects all aspects of the laboratory process, including the preanalytic, analytic, and postanalytic phases. The major steps designed by manufacturers to mimic the manual techniques are specimen processing, reagent measurement and delivery, chemical reaction phase, measurement phase, signal processing, and data handling.6 TLA may be variably effective at reducing turnaround time while simultaneously increasing laboratory productivity.7–12 The evolution of automated core facilities has been delivered successfully in both clinical chemistry and hematology.10,13,14 Although TLA has gained widespread traction in several diagnostic lines, especially clinical chemistry, immunochemistry, and hematology, its application in diagnostic microbiology and histology has proceeded much more slowly, with several activities requiring a considerable manual burden.
Although TLA has resulted in an expanded profitability, enhanced workflow, reduced time cycle, and improved quality and safety, it is not without potential concerns. These include higher initial costs, higher risk of downtime, psychological dependence of laboratory technologists, and disruption of staff trained in specific technologies.15 The TLA market is growing at a compound annual growth rate of 6.6% over the next 5 years.16 Despite the expansion of TLA, the clinical laboratory workforce continues to play a vital role in the health care system. Members of this workforce provide essential information concerning the prevention, diagnosis, and management of health and disease. However, there is great concern, following the adoption of TLA, regarding the quality and quantity of laboratory professionals entering the workforce.
Typically, the workforce of a clinical laboratory includes pathologists, laboratory scientists, phlebotomists, and laboratory technologists and technicians. Laboratory technologists and technicians represent the two largest groups of within this workforce. Laboratory technologists have completed a bachelor’s degree in an accredited education program specific to clinical laboratory sciences. They have also fulfilled the required laboratory experience specified by a certifying agency.17 They are trained to perform a wide range of complex chemical and biological laboratory assays on tissues, blood, and other body fluids. Laboratory technicians have completed a diploma degree or equivalent. These members of the laboratory workforce usually perform less complex tasks under the supervision of a technologist/scientist.
There has been a significant concern that total automation can decrease the need for personnel in the laboratory and alter the skill sets required for laboratory personnel at all levels.15 However, another concern within the laboratory medicine sector is the growing shortage of clinical laboratory workers, which is expected to worsen over the next decade. Among the factors contributing to this shortage are the growing demand for laboratorians, the decline in the number of fresh graduates as a result of the decreasing number of clinical laboratory sciences programs, and the retirement of the aging laboratory workforce.18,19
The Saudi Ministry of Health has reported 13,152 employed laboratorians who have performed 174,225,388 different laboratory tests in 2019.20 The Saudi Commission for health Specialties estimated the number of medical laboratory specialists in 2017 was 14,487. It has been estimated that 28,200 medical laboratory specialists will be needed in the year 2027. According to the same report, the total number of students expected to graduate between 2018 and 2022 is 1306 enrolled in the Bachelor of Medical Laboratory programs.21
TLA is a new trend for improving the management of high clinical laboratory workloads, but there is scant literature to support its wide adoption in Saudi Arabia. Most previous reports on TLA have dealt with the reduction of cost and turnaround time.22–24 Although its effect on productivity, cost reduction and enhanced quality of service has been studied,25 very little data is available regarding its impact on the laboratory workforce. Such data is greatly required to evaluate the return on investment of total laboratory automation. Thus, the primary objective of this study is to investigate the impact of TLA on the clinical laboratory workforce in Saudi Arabia.
Methods
The Ethics Review Board of Prince Sultan Military College of Health Sciences, Dhahran approved this study (IRB Number IRB-2021-CLS-50). Two medical laboratory departments participated in this study. The first one is the Medical Laboratory Department of King Salman Armed Forces Hospital (KSAFH), Tabuk. This department has recently adopted a total automation system in three sections, clinical chemistry, hematology, and serology. These consisted of continuous flow analysis using Atellica® Solution for clinical chemistry, Sysmex XN-1000™ for hematology, and Abbott Alinity i for serology. The other department is the Medical Laboratory Department of King Fahad Military Medical Complex (KFMMC), Dhahran. This department uses discrete analysis, an automated methodology in which samples are held in separate containers to be assayed. Both laboratories belong to a tertiary care military hospital with similar case mix of patients with a total of 400 beds each.
Data provided by both centers included the number of laboratory employees in each section, as well as their ages, genders, nationalities, education, and years of experience. Data also include the total number of laboratory tests performed in each section between September 2020 and August 2021. Both centers were instructed to unbundle the various test profiles when counting the tests in the clinical chemistry, hematology and serology sections. Technical productivity was calculated by dividing the number of tests performed by the total number of paid full-time employees or equivalents.26 We calculated the productivity ratios, defined as testing volumes per full-time equivalent. The number of tests per employee per month in each of the three sections of the two laboratories was calculated.
Data Analysis
Data were analyzed using t-test by using the SPSS version 20 (SPSS Inc., Chicago, IL, USA). We also calculated the odds ratios (OR) and the respective 95% confidence interval and the P values for the comparison of the productivities between the two sites. The odds ratios were calculated by comparing the number of laboratory tests performed by a single worker in each section in both sites. We used KFMMC site, without total automation, as the reference and calculated odds ratios and p-values compared to this one. We used 5% (p < 0.05) as a level of significance.
Results
Table 1 shows the characteristics of the laboratory workforce of the two sites in the selected sections of the laboratory. There were 36 laboratory workers at the three sections of the KSAFH. The mean age of laboratory workers was 33.5 years, mean total experience of 7 years, and 69.4% have completed a bachelor’s degree. The other site of KFMMC consisted of 64 laboratory workers of a more or less similar age, qualifications, and length of experience. There was a notable difference in the ratio of male to female laboratory workers between the two sites. Males constituted 80.6% of all laboratory workers at the KSAFH site, while constituting only 42.9% of the total laboratory workforce at the KFMMC site. More Saudi citizens were represented in the KSAFH site (80.6%) compared to that of KFMMC (60.7%).
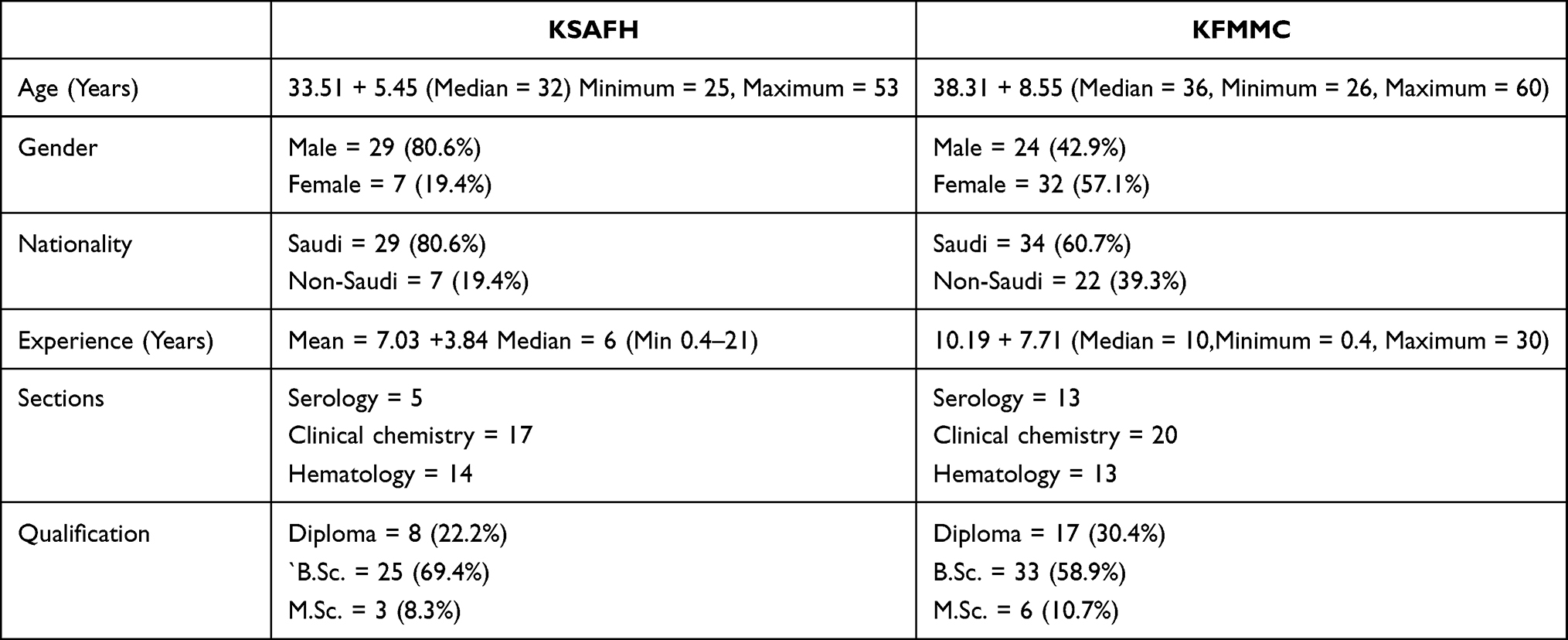 |
Table 1 Demographical Data of the Workforce of the Two Sites |
Table 2 represents the total number of laboratory tests performed at each of the three sections in both sites along with the number of laboratory workers. The odds ratios, 95% confidence intervals, and p values are shown. The results indicated a similar work productivity by a single laboratory worker in the hematology section in each of the two sites with no significant difference (average odd radio = 0.9, p = 0.79). However, the number of tests performed by a single worker has increased to an average of 1.4 and 3.7 times at the KSAFH site compared to KFMMC site in the clinical chemistry and serology sections respectively.
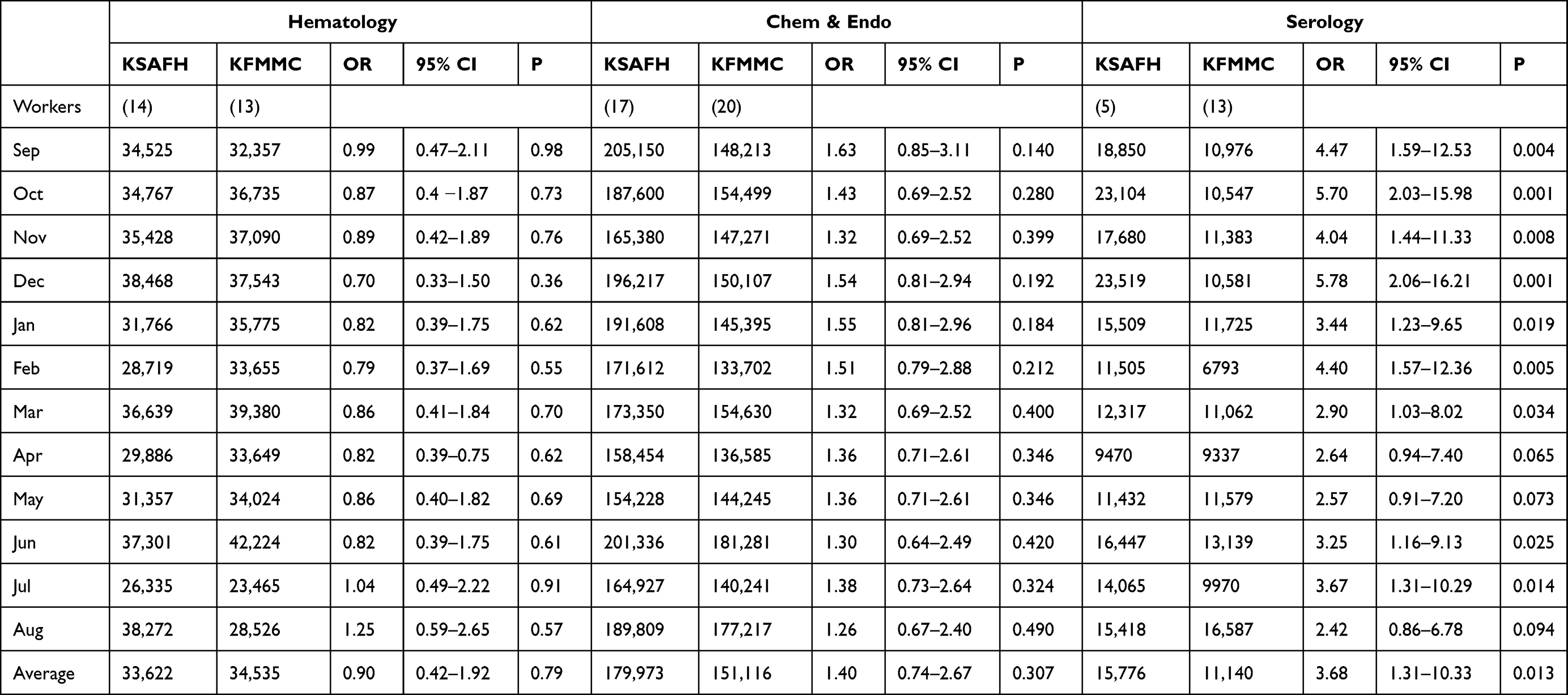 |
Table 2 Total Number of Laboratory Test Performed at Each of the Three Sections in Both Sites with the Odds Ratios, The 95% Confidence Intervals, and p values. The Number of Laboratory Workers in Each Section of the Two Sites in Parenthesis |
Table 3 shows a comparison between the average laboratory tests performed in the three sections of the two sites. Large difference in the average productivity of a single worker in the serology and clinical chemistry sections of KSAFH laboratory compared to those of KFMMC (p ≤ 0.001).
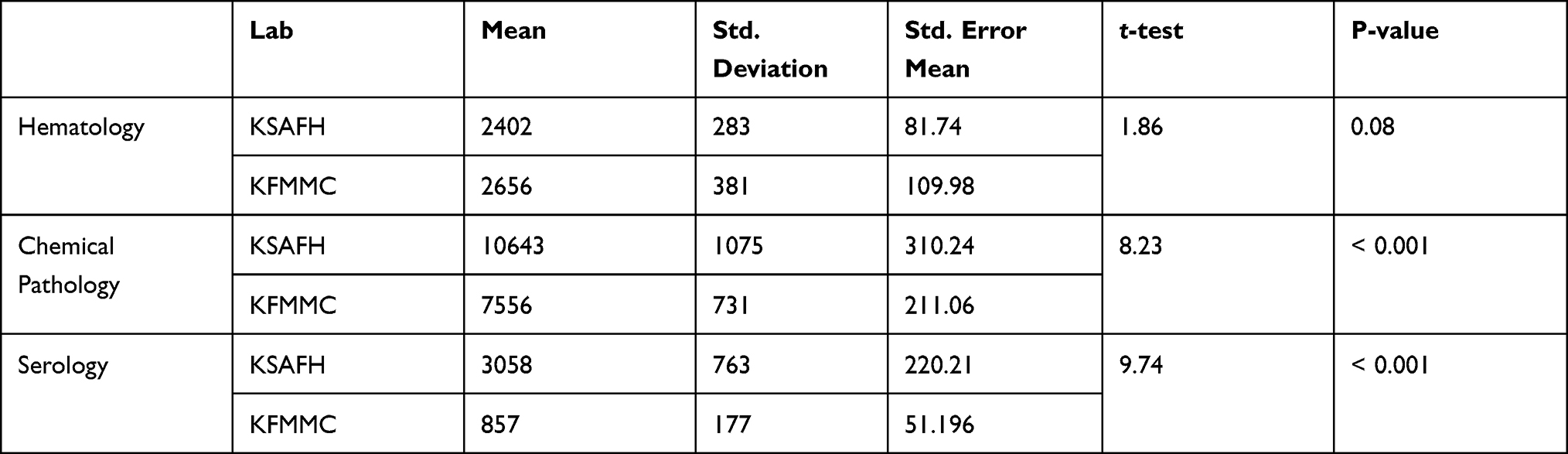 |
Table 3 Average Monthly Number of Tests Performed by a Single Worker in Each Section of the Two Sites |
Discussion
We compared the productivity of two laboratories of similar workforce characteristics and laboratory test profiles while utilizing different testing systems. KSAFH laboratory has adopted a total automation system in three sections consisting of continuous flow analysis while the KFMMC laboratory utilizes discrete analysis. Both laboratories belong to the Armed Forces Medical Services of the Ministry of Defense for the Kingdom of Saudi Arabia. The laboratory workforce at both sites consisted of various individuals with similar qualifications and years of experience.
We calculated the productivity ratios, defined as testing volumes per full-time worker.26,27 The total number of laboratory tests performed at each of the three sections in both sites were used in this study. The number of laboratory tests performed by a single worker in each section were compared and statistically analyzed. The results indicated similar productivity by a single laboratory worker in the hematology section in each of the two sites with no significant difference (average odd radio = 0.9, P = 0.79). However, the number of tests performed by a single worker has increased to an average of 1.4 and 3.7 times at the KSAFH site as compared to the KFMMC site in the clinical chemistry and serology sections, respectively. In other study, the productivity increased by 58.2% as measured by tests/employee, and 82% as measured by specimens per employee.25
Productivity varied widely among the various laboratory departments within both site and among different sections participating in this study. Many other studies have used the testing volume as a measurement of the productivity ratio.27 Despite standardization of testing profiles in both study sites, there was wide variation in the average productivity in the serology and clinical chemistry sections. This variation has been noted before and indicates opportunities to improve staff productivity in many facilities.28
Without TLA, more staff is needed to conduct the increasing number of tests. However, with TLA, the productivity of the laboratory is enhanced, leading to a reduction in staff. In another study, the assumed productivity increased by 16.2% in the presence of TLA, resulting in decreased laboratory workforce.22
A previous study in Saudi Arabia indicated that staffing cost was reduced and less staff was required with the adoption of TLA.23 It has been clearly demonstrated that implementing TLA results in less staff, reduced operating costs, and more rapid testing.29
A previous findings showed that core lab and computerization have almost the same impact on the workforce reduction by 35% and 30% respectively, and modular robotics the least impact with 17%.24
Over the last ten years, laboratory workload has increased steadily against a fairly constant headcount, estimated as a compound annual growth rate of 5%.2 Therefore, the existing laboratory workforce, in the absence of automation, could not have been able to maintain current standards of service. Automation aims to contain the ever-increasing workload challenge, reduce errors, and enhance laboratory performance while managing a limited labor force. Total automation also reduces the possibility of human errors that arise from repetitive and laborious procedures undertaken by the laboratory personnel. While TLA has resulted in less full-time staff, it has also uncovered the need for changes in staff skills. Adoption of automation reduces the mundane and repetitive manual labor, thereby minimizing human error and allowing the redefinition of the job roles of the laboratory workforce. With greater automation, laboratory employees can move towards value-added activities, such as quality control and quality assurance. TLA can also facilitate the expansion of the laboratory repertoire to include tests performed via state-of-the-art but labor-intensive platforms.
Laboratory automation can be a resource that increases productivity and improves work scheduling while providing new opportunities to re-skill, and develop all laboratory personnel.30 Automation results in increased efficiency, but requires changes to laboratory infrastructure and a shift in workforce training requirements. TLA may reduce the laboratory manual workforce needed for managing high volume testing and produce lower staff congestion within the laboratory. This is especially true for auxiliary and technical staff.13,23 The major benefits of laboratory automation are reduction of medical errors, reduced specimen sample volume, increased accuracy and precision, improved safety for laboratory staff, faster turnaround time of results, and partially alleviating the impending shortage of skilled laboratory staff.
It has been reported that retirement rates for the clinical laboratory workforce exceeded the number of graduates.31 TLA may be ideal for laboratories that suffer from workforce shortages,31–33 However, automation has increasingly found a way into the good clinical, laboratory, and manufacturing practices (GxP) regulated laboratories following the increasing demands on the throughput, traceability, and reproducibility.34 The adoption of TLA model is currently incorporating several diagnostic lines such as clinical chemistry, immunochemistry, hematology, and coagulation). However, different settings might be encountered in other sections of the laboratory such as histology and microbiology that requires more manual work.
Several challenges need to be addressed before lab automation can reach its full prospective. Automation will also require changes to laboratory infrastructure and a shift in workforce training requirements. Retraining and continuing medical laboratory education opportunities are required enable the workforce to acquire the necessary skills on artificial intelligence and laboratory informatics. Systematically analyzing and reviewing the impact of TLA on the laboratory workforce would be of great value.
Although the current study has made relatively simple adjustments for the differences between laboratories, such as their testing volume and their type of workload, more other differences in the test mix or differences in human resource policies were not considered. In spite of these limitations, we believe the data from this study provide a useful reference point for the impact of total automatons on the clinical laboratory workforce.
Conclusion
Total laboratory automation improves the productivity of the laboratory, leading to a decreased laboratory workforce. Adoption of automation reduces repetitive manual labor, thereby allowing the redefinition of the job roles of the laboratory workforce. However, TLA also presents some potential problems pertaining to the laboratory workforce such as decreased number of laboratorians, human psychological dependence, and reconsideration of training needs. The laboratory workload has increased significantly therefore, the existing laboratory workforce, in the absence of automation, could not have been able to maintain the current volume of service. TLA is ideal for laboratories that suffer from workforce shortages or managing high volume testing with less staff.
Ethical Approval
This study obtained ethical approval from the IRB at Prince Sultan Military College of Health Sciences (Ref. No. IRB-2021-CLS-050) dated 21st August, 2021.
Acknowledgment
The authors would like to thank the Medical Laboratory Departments of KSAFH and KFMMC for generously providing the data. Thanks are also due to Mrs. Huda Olan and Dr. Arifi Waked of the English Department of PSMCHS for proofreading the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest.
References
1. Olsen K. The first 110 years of laboratory automation: technologies, applications, and the creative scientist. J Lab Autom. 2012;17(6):469–480. doi:10.1177/2211068212455631
2. Yeo CP, Ng WY. Automation and productivity in the clinical laboratory: experience of a tertiary healthcare facility. Singapore Med J. 2018;59(11):597–601. doi:10.11622/smedj.2018136
3. Bezerra MA, Lemos VA, de Oliveira DM, et al., Automation of continuous flow analysis systems – a review. Microchem J. 2020;155:104731. doi:10.1016/j.microc.2020.104731
4. Rifai N, Horvath AR, Wittwer CT, Charles D, Jonathan R, Carl TW, Editors. Automation in the Clinical Laboratory February. In Book: Tietz Textbook of Clinical Chemistry and Molecular Diagnostics Edition: 6 Chapter: 26. Publisher: Elsevier; 2017.
5. Armbruster DA, Overcash DR, Reyes J. Clinical chemistry laboratory automation in the 21st century - Amat Victoria curam (Victory loves careful preparation). Clin Biochem Rev. 2014;35(3):143–153.
6. Turgeon ML. Linné & Ringsrud’s Clinical Laboratory Science: Concepts, Procedures, and Clinical Applications. Elsevier; 2016.
7. Seaberg RS, Stallone RO, Statland BE. The role of TLAin a consolidated laboratory network. Clin Chem. 2000;46:751–756. doi:10.1093/clinchem/46.5.751
8. Angeletti S, De Cesaris M, Hart JG, et al. Laboratory automation and intra-laboratory turnaround time: experience at the University hospital campus bio-medico of Rome. J Lab Autom. 2015;20(6):652–658. doi:10.1177/2211068214566458
9. Ialongo C, Porzio O, Giambini I, Bernardini S. Total automation for the core laboratory: improving the turnaround time helps to reduce the volume of ordered STAT tests. J Lab Autom. 2016;21(3):451–458. doi:10.1177/2211068215581488
10. Lou AH, Elnenaei MO, Sadek I, Thompson S, Crocker BD, Nassar B. Evaluation of the impact of a total automation system in a large core laboratory on turnaround time. Clin Biochem. 2016;49(16–17):1254–1258. doi:10.1016/j.clinbiochem.2016.08.018
11. Chung HJ, Song YK, Hwang SH, Lee DH, Sugiura T. Experimental fusion of different versions of the total laboratory automation system and improvement of laboratory turnaround time. J Clin Lab Anal. 2018;32:e22400. doi:10.1002/jcla.22400
12. Yu HE, Lanzoni H, Steffen T, et al. Improving laboratory processes with total laboratory automation. Lab Med. 2019;50:96–102. doi:10.1093/labmed/lmy031
13. Archetti C, Montanelli A, Finazzi D, Caimi L, Garrafa E. Clinical laboratory automation: a case study. J Public Health Res. 2017;6(1):881. doi:10.4081/jphr.2017.881
14. Hawker CD. Nonanalytic Laboratory Automation: a quarter century of progress. Clin Chem. 2017;63(6):1074–1082. doi:10.1373/clinchem.2017.272047
15. Lippi G, Da Rin G. Advantages and limitations of total laboratory automation: a personal overview. Clin Chem Lab Med. 2019;57(6):802–811. doi:10.1515/cclm-2018-1323
16. Total Lab Automation Market. Growth, Trends, and Forecasts (2020–2025). Mordor Intelligence; 2020:120.
17. Brown K, Fenn JP, Fong K, et al. ASCP board of certification survey of medical laboratory science education programs. Lab Med. 2019;50(4):e70- e74. doi:10.1093/labmed/lmz019
18. Garcia E, Kundu I, Kelly M, Soles R. The American Society for Clinical Pathology 2020 vacancy survey of medical laboratories in the United States. Am J Clin Pathol. 2021;aqab197. doi:10.1093/ajcp/aqab197
19. Cortelyou-Ward K, Ramirez B, Rotarius T. The laboratory workforce shortage: a managerial perspective. Health Care Manag. 2011;30(2):148–155. doi:10.1097/HCM.0b013e318216f5df
20. Ministry of Health. Annual Statistical Book. Riyadh, Saudi Arabia: Ministry of Health; 2017.
21. Saudi Commission for Health Specialties. The reality of the Saudi health workforce during the next ten years 2018–2027. Riyadh Saudi Arabia: SCFHS; 2017.
22. Kim K, Lee SG, Kim TH, Lee SG. Economic evaluation of total laboratory automation in the clinical laboratory of a tertiary care hospital. Ann Lab Med. 2022;42(1):89–95. doi:10.3343/alm.2022.42.1.89
23. Ellison TL, Alharbi M, Alkaf M, et al. Implementation of total laboratory automation at a tertiary care hospital in Saudi Arabia: effect on turnaround time and cost efficiency. Ann Saudi Med. 2018;38(5):352–357. doi:10.5144/0256-4947.2018.352
24. Dadoun R. Impact on human resources: core laboratory versus laboratory information system versus modular robotics. Clin Leadersh Manage Rev. 1998;12(4):248–255.
25. Sarkozi L, Simson E, Ramanathan L. The effects of total laboratory automation on the management of a clinical chemistry laboratory Retrospective analysis of 36 years. Clinica Chimica Acta. 2003;329(1–2):89–94. doi:10.1016/S0009-8981(03)00020-2
26. Young DS. Laboratory automation: smart strategies and practical applications. Clin Chem. 2000;46(5):740–745. doi:10.1093/clinchem/46.5.740
27. Novis DA, Coulter SN, Blond B, Perrotta P, Talbert ML. Technical Staffing Ratios: a Summary of 3 College of American Pathologists Q-Probes Studies. Arch Pathol Lab Med. 2021. doi:10.5858/arpa.2020-0760-CP
28. Valenstein PN, Souers R, Wilkinson DS. College of American Pathologists. Staffing benchmarks for clinical laboratories: a College of American Pathologists Q-probes study of staffing at 151 institutions. Arch Pathol Lab Med. 2005;129(4):467–473. doi:10.5858/2005-129-467-SBFCLA
29. Dogether MA, Muallem YA, Househ M, Saddik B, Khalifa M. The impact of automating laboratory request forms on the quality of healthcare services. J Infect Public Health. 2016;9(6):749–756. doi:10.1016/j.jiph.2016.09.003
30. Halloran KJ. Laboratory automation: changing the role of the technical professional. J Autom Chem. 1993;15(1):13–17. doi:10.1155/S1463924693000045
31. Garcia E, Kundu I, Kelly M, Soles R. The American Society for clinical pathology’s 2018 vacancy survey of medical laboratories in the United States. Am J Clin Pathol. 2019;152(2):155–168. doi:10.1093/ajcp/aqz046
32. Chapman SE, Lindler V, Ward-Cook K. An assessment of critical issues facing the clinical laboratory workforce. Clin Leadersh Manage Rev. 2005;19(1):E4.
33. La Porta AD, Bowden AS, Barr S. Workflow improvement and impact of the new Beckman Coulter LH 1500 high throughput automated hematology workcell. Lab Hematol. 2004;10(2):95–101. doi:10.1532/LH96.04022
34. Gröschl M. Introducing automation to a regulated laboratory - an experience report. Bioanalysis. 2020;12(10):643–647. doi:10.4155/bio-2020-0118
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.