")
Back to Journals » Patient Preference and Adherence » Volume 13
The impact of short message services and personal consultation by pharmacy students on medication adherence and blood pressure control: study protocol for a cluster randomized trial
Authors Zhai P, Li Q, Gillani AH, Hayat K , Shi L, Wang S, Peng F, Xu S, Du Q, Cao Z, Morisky DE , Fang Y
Received 11 December 2018
Accepted for publication 13 March 2019
Published 30 April 2019 Volume 2019:13 Pages 627—636
DOI https://doi.org/10.2147/PPA.S197858
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Naifeng Liu
Panpan Zhai,1–3 Qian Li,1–3 Ali Hassan Gillani,4 Khezar Hayat,1–3,5 Li Shi,1–3 Siyi Wang,1–3 Fei Peng,1–3 Sen Xu,1–3 Qianqian Du,1–3 Zeyu Cao,1–3 Donald E Morisky,6 Yu Fang1–3
1Department of Pharmacy Administration and Clinical Pharmacy, School of Pharmacy, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2Center for Drug Safety and Policy Research, Xi’an, People’s Republic of China; 3Shaanxi Center for Health Reform and Development Research, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 4Department of Pharmacy, Yusra Institute of Pharmaceutical Sciences, Islamabad, Pakistan; 5Institute of Pharmaceutical Sciences, University of Veternary and Animal Sciences, Lahore, Pakistan; 6Department of Community Health Sciences, UCLA Fielding School of Public Health, Los Angeles, CA 90095-1772, USA
Purpose: Hypertension prevalence is mounting at a great pace in the People’s Republic of China and poses a serious threat to health care systems. Medication nonadherence is one of the key factors in controlling high blood pressure. Our study uses two-arm cluster randomized controlled trial to investigate whether personal consultation by postgraduate pharmacy students and short message services (SMS) is effective in improving medication adherence and blood pressure control.
Patients and methods: The trial will involve 384 treated patients in 8 community health care centers (CHCs). The 8 CHCs will be randomly assigned to intervention and control group in a ratio of 1:1. Patients in the intervention group will receive a personal consultation which identifies the barriers to medication adherence and SMS reminders which will be sent at 3-day intervals while patients in the control group will receive standard pharmaceutical care. Personal consultation by pharmacy students will be delivered at months 0 and 3. SMS messages will include educational information about normal blood pressure, complications of hypertension, salt intake, healthy diet, smoking cessation, regular exercise, weight control, antihypertensive medication schedule and treatment. Both groups will be followed for 6 months in order to compare their medication adherence and blood pressure at months 0, 3 and 6. The primary clinical outcome is the change in mean blood pressure and medication adherence measured at baseline, months 3 and 6. Secondary outcome is the proportion of patients reaching controlled blood pressure at months 3 and 6.
Discussion: Pharmacy students led consultation will be conducted in the process of physical examination and SMS reminders which is at low cost, may be a feasible way to address the high prevalence of hypertension in the People’s Republic of China.
Keywords: medication adherence, hypertension, blood pressure, SMS reminders, personal consultation, community health care centers
Introduction
Hypertension, one of the most common non-communicable diseases, accounts for more than 26% of the world’s adult population and the prevalence increases with age.1 Globally, hypertension is also one of the leading causes of premature death, with 7.1 million people dying every year from high blood pressure-related diseases.2 For every 20 mmHg lower systolic blood pressure (SBP) or 10 mmHg lower diastolic blood pressure (DBP), the risk of a cardiovascular event is reduced by about 50%.3 Therefore, blood pressure control is the entry point for prevention and treatment of cardiovascular disease.
According to the 2017 “National Guidelines for the Prevention and Treatment of Hypertension in Primary Settings”,4 it is estimated that the number of hypertensive patients in the People's Republic of China has reached 270 million. Complications of hypertension, such as stroke, fundus disease, heart and kidney disease, increase the risk of disability and mortality which have posed immense financial burden on health care systems in the People's Republic of China. Adherence to a medication regimen can be defined simply as the extent to which patients take medications as prescribed by their health care providers.5 Hypertension, a chronic disease, requires long-term adherence to medications to reduce complications.6 However, approximately 20–50% of patients with chronic illnesses are reported to be non-adherent to their medications, a situation that compromises treatment effectiveness.7–9
Globally, the mobile phone has become the preferred tool for communication and access to information bringing together communication.10 As of December 2018, about 1.57 billion mobile phone subscriptions had been registered in the People's Republic of China.11 Short message services (SMS) has low cost, easy and wide coverage, and the potential for individualized instant delivery.12 Furthermore, studies have confirmed the effectiveness of SMS reminders on improving medication adherence and it could be an effective tool to overcome poor medication adherence.13–15 SMS has been used in several diseases, such as HIV,16 diabetes mellitus17 and allergic rhinitis,18 but there are limited studies on its use in hypertensive patients. As a matter of fact, a meta-analysis evaluating the effectiveness of text messaging only included one hypertension study.19 Similarly, in the People's Republic of China, most studies focused on patients with coronary artery disease,20 HIV21 and mental health problems.22 Studies about the effect of SMS reminders on hypertensive patients are needed to fill in the gap.
Pharmacists play a pivotal role in health care systems and have a direct impact on improving the value of medication treatment through frequent interaction with patients.23,24 Studies have shown that pharmacists are beneficial in improving medication adherence among patients with hypertension.25–29 However, health care systems are lacking in pharmacists and they are prone to sub-health status due to work stress, overload of work and lack of sleep. The questions remain, however, as to whether pharmacists can do these interventions effectively in busy community practices.30 Moreover, interventions by pharmacists cannot be widely used due to high pharmacist’s cost and time constraints.31 The value of pharmacy students consultation has been approved in different clinical settings.32–34 Pharmacy students and residents conducting discharge counseling program on heart failure readmission, 89% of patients receiving the program had better understanding of medications.32 A study33 examined the impact of 5-min counseling program led by pharmacy students among 198 participants to improve knowledge about influenza and vaccines and it showed that a targeted consultation can increase vaccination rates and change public views. American and Kenyan pharmacy students successfully provide clinical pharmacy consultations in a resource-constrained, acute-care practice setting and it suggests pharmacy students have an important role in providing improved pharmacy service, reducing medication errors and cost.34 Literature showed the potential influence of student interventions on medication adherence is lacking.30
The purpose of this study is to investigate whether mobile health interventions by pharmacy students are feasible in improving patient medication adherence and lowering their blood pressure in 6 months. If the intervention is effective, we can provide intervention models to government departments and help them to develop education guidelines for patients to improve their medication adherence and reduce their chances of having hypertension-related complications.
Methods
Study design
It is a 6-month, intention-to-treat, two-arm cluster randomized controlled trial to assess the effectiveness of SMS reminders and health consultation in addition to standard pharmaceutical care compared to standard pharmaceutical care only. This study used a stratified proportional sampling approach and is designed according to SPIRIT 2013 Statement (Standard Protocol Items: Recommendations for Interventional Trials).35
According to the GDP per capita of Xi’an city, Shaanxi Province in 2017 (Statistical data from the Statistical Yearbook of Shaanxi Province in 2017), the districts in Xi’an were divided into three categories: high, medium and low social economic development level. In each category, one district was selected randomly as the representative district, and the results selected are: Yanta district, Xincheng district and Lintong district. According to the number of permanent residents, the proportion of population in Yanta district, Xincheng district and Lintong district is about 4:2:2, so four community health care centers (CHCs) in Yanta district, two CHCs in Xincheng district and two CHCs in Lintong district were selected accordingly and they are comparable in regional characteristics. Eight CHCs will be randomized into two parallel groups in a 1:1 allocation ratio. In Yanta district, two CHCs will be selected, based on computer-generated random numbers, as intervention group and the other two will be serving as the control group. In Xincheng and Lintong districts, one CHC will be randomly selected as intervention group and the other one will be in the control group. The sampling process will ensure the generalizability of our trial results and reflect the real-world population with hypertension who are the target of our intervention, so our intervention could be used in a larger scale.
Study settings
The study will be conducted at 8 public CHCs in Xi’an, Shaanxi, the People's Republic of China. The CHCs provide a full range of primary care services. We selected CHCs within the walking distance of communities and each CHC manages approximately 2,000 patients with chronic diseases. Patients with hypertension are managed by nurses and physicians and they will be followed up four times a year by nurses through telephone, face-to-face communication or family visit. The nurses will ask patients about their medication regimen, side effects, lifestyle modifications, blood pressure and weight control. Patients who attend the CHCs for physical examination or medication treatment in the outpatient clinic will be approached for participation in the study.
Study participants
We will enroll those patients who meet the trial eligibility criteria: aged over 18 years; diagnosed with hypertension by physicians; prescribed at least one high blood pressure medication; with a SBP <220 mm Hg and a DBP <120 mm Hg at enrollment; have resident health record at CHC; signed informed consent form. Eligible patients are attending the CHCs, residing in the trial area; having access to mobile phone and can read SMS text messages.
Patients who are suffering from dementia, depression, serious heart, lung and kidney diseases; pregnant or in their lactation period; illiterate or cannot clearly express themselves or refused to participate in the study will be excluded. The inclusion and exclusion criteria will enable us to avoid selection bias and ensure the external validity of our study. All participants will be provided written informed consent to ensure their understanding of the trial.
Control group
Patients in the control group will receive standard pharmaceutical care according to “Guidelines for Good Pharmacy Practice”36 (GPP). The China Non-prescription Medicines Association recommended the first edition of “Guidelines for Good Pharmacy Practice” as a standard for pharmacy practice.37 According to the GPP, traditionally, the mission of pharmacy practice in the People's Republic of China is to provide medications and other health care products and services. However, in recent years the term “pharmaceutical care” has established itself as a philosophy of practice, with the patient and the community as the primary beneficiaries of the pharmacist’s actions. GPP guidelines are based on the pharmaceutical care given by pharmacists. Similar to other countries, in the People's Republic of China, pharmaceutical care is a patient-centered, outcomes-oriented pharmacy practice that requires the pharmacist to work in concert with the patient and the patient’s other health care providers to promote health, to prevent disease, and to assess, monitor, initiate, and modify medication use to assure that drug therapy regimens are safe and effective. The goal of pharmaceutical care is to optimize the patient’s health-related quality of life, and achieve positive clinical outcomes, within realistic economic expenditures. Patients in the control group will also receive a welcome SMS at the time of recruitment to confirm their enrollment in the trial and end-of-trial message.
Intervention group
The intervention group will receive a welcome SMS, end-of-trial message and standard pharmaceutical care with additional interventions. The intervention consists of two parts: personal consultation by pharmacy students at baseline and 3 months from the baseline study and SMS reminders at 3-day intervals. According to previous study, half of the patients occasionally forgot to take their medication.38 If forgetting is the primary reason for non-adherence, we will recommend patients to place their medication nearby a toothbrush or hygiene kit as a reminder. For individuals who forget to bring their medication along when traveling, we will suggest them to place their medications in a pill container, a purse or hygiene kit.39
The content of SMS is developed based on previous literature10,40,41 which aim to improve treatment adherence and clinical outcomes through SMS-based interventions and “National Guidelines for the Prevention and Treatment of Hypertension in Primary Settings”.4 SMS reminders will be developed by principal investigator, pharmacists, nurses and will be reviewed by a cardiologist in a tertiary hospital. The content of SMS includes three parts: hypertension-related knowledge, suggestions of lifestyle modifications and advice of overcoming barriers to medication adherence which is in accordance with the recommendations of our national guideline. Messages are designed to motivate medication-taking behaviors and to improve patient understanding of hypertension-related knowledge, medication regimen and medication adherence. SMS messages will include educational information about normal blood pressure, complications of hypertension, salt intake, healthy diet, smoking cessation, regular exercise, weight control, antihypertensive medication schedule and treatment. All the messages will be sent in the morning at 7 am when patients are supposed to take their medications. All SMS messages will be delivered automatically by an open access website run by a third-party company (Alibaba Cloud, Alibaba Cloud Computing Co. Ltd. Hangzhou, People's Republic of China).
Procedures
The baseline study will be conducted by pharmacy students. To reach target sample size, patients will be recruited when they are in the process of physical examination or outpatient clinic by medical staff. Informed consent will be taken from all enrolled hypertensive patients who meet the inclusion criteria. After this, Morisky Medication Adherence Scale-8 (MMAS-8) and paper-based questionnaires will be administered to patients both in the intervention group and control group. The MMAS-8 questionnaire will be done by using the Morisky Widget online (Morisky Widget, MMAS Research LLC, Las Vegas, NV, USA) on mobile tablets. The widget will give us scores and answers immediately which will allow us to identify the reasons of medication non-adherence and facilitate immediate feedback to patients. For hypertensive patients, who are unfamiliar with tablets, interviewers will read the questions to patients and type in their answers. Then, the paper-based questionnaires including patient’s demographics, clinical conditions, medication complexity, side effects, behavior and patient’s knowledge will be administered to patients. The knowledge part consists of 7 statements, each requesting patients to answer with “yes”, “no”, or “not aware”. Each correct answer will be coded as 1 point, and incorrect answer or unaware of the question will be coded as zero so the maximum score is 7. The higher the score, the higher the knowledge about hypertension. The design of questionnaire was based on previous literature42–45 and 2017 “National Guidelines for the Prevention and Treatment of Hypertension in Primary Settings”.4
After that, pharmacy students who are certificated by the MMAS research group will give a personal consultation to hypertensive patients in intervention group based on their responses to the MMAS-8 questions and questionnaires. The personal consultation will last about 5 mins to identify patients’ barriers to medication adherence and provide suggestions to overcome their barriers such as forgetfulness, side effects and negative beliefs. The whole process will last about 20 mins and patients will have the opportunity to ask questions during the consultation. During the intervention period, patients in the intervention group will also receive SMS reminders at 3-day intervals while patients in the control group will only receive a welcome SMS and end-of-trial SMS.
At month 3, hypertensive patients who complete baseline survey will be invited to the CHCs or will be interviewed on telephone by trained interviewers to finish the MMAS-8 in two groups. For patients in the intervention group, they will receive another personal consultation which will last for 5 mins. For patients, who are too busy to go to the CHCs or answer their phones, medical staff and pharmacy students will go to their communities to finish the follow-up study. At months 0, 3 and 6, patients will undergo assessments on medication adherence and blood pressure both in the control and intervention groups. For blood pressure measurement, patients will be measured by blinded nurses using the calibrated upper-arm electronic sphygmomanometer (OMRON HEM-7200, OMRON Corporation, Dalian). The study design is shown in Figure 1.
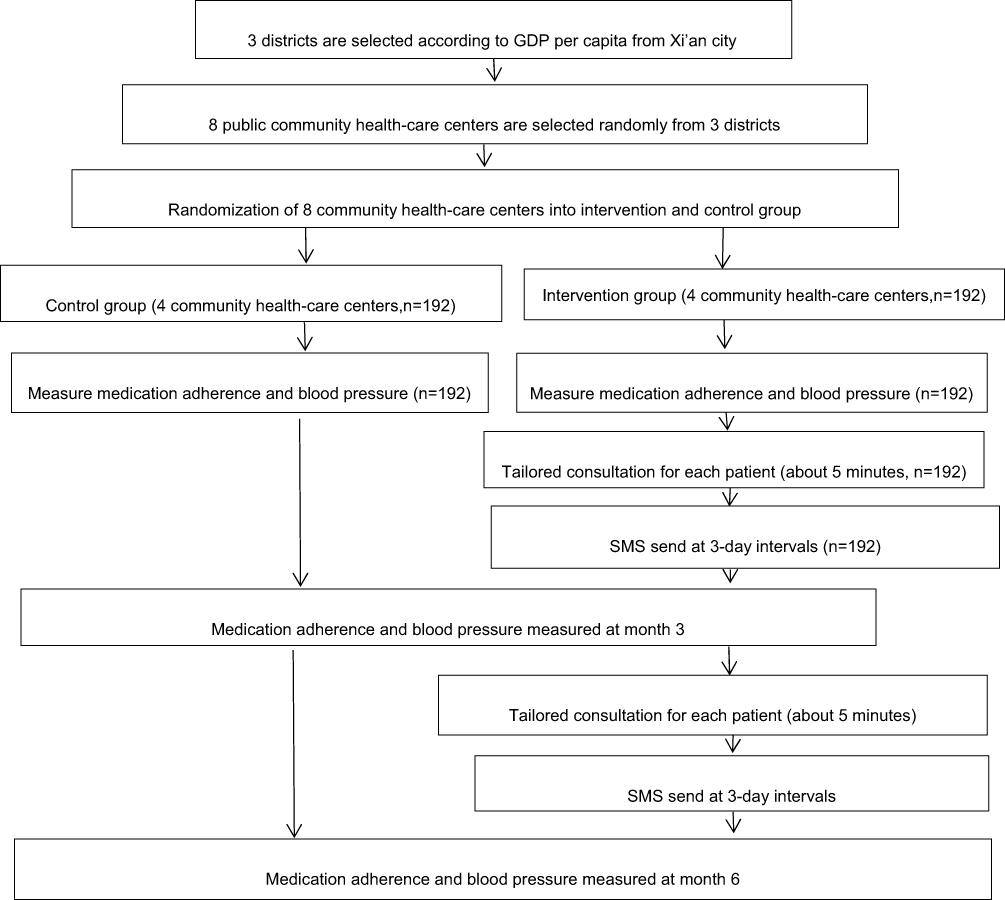 | Figure 1 Study design. |
Outcomes
The primary outcome is change in blood pressure and medication adherence from baseline to months 3 and 6. Patients without drinking, smoking or consuming coffee or tea within 30 mins before the measurement will be measured by medical staff using certified and regularly calibrated upper-arm electronic sphygmomanometer according to the standard guideline. There will be two measurements taken 5 mins apart46 and blood pressure will be the average of the two measurements.4 If the difference between two measurements is 5 mmHg or more, the third time measurement will be taken, and the final blood pressure will be the average of two closest measurements.4 Medication adherence is measured by MMAS-8 with a total score range 0–8.47 Response answers are dichotomous (yes/no) for the first seven questions and a 5-point Likert response for the last item. Low adherence and medium adherence are defined as having <6 and 6 to <8, respectively. High adherence is defined as getting 8 in the test. It is widely used with good reliability (Cronbach’s α=0.83) and validity. The MMAS-8 demonstrated good internal consistency (Cronbach’s α = 0.77) and test–retest reliability in Chinese population.48
The secondary outcome is the proportion of people having controlled blood pressure at months 3 and 6. Hypertension control is defined as having a SBP <140 mmHg and a DBP <90 mmHg for hypertensive patients without diabetes or chronic kidney diseases or a SBP <150 mmHg and a DBP <90 mmHg for hypertensive patients aged over 80 years old49 or a SBP <130 mmHg and a DBP <80 mmHg for patients with diabetes or chronic kidney disease.25
Sample size
The study is based on the comparison of blood pressure between control group and intervention group at baseline and at month 6. Based on a previous study,50 a 5 mmHg decrease in SBP can reduce the risk of having stroke and coronary heart diseases. According to earlier study,51 we used the standard deviation of SBP (14.1 mm Hg) to calculate the sample size. The intended sample size is 384, allowing for 15% loss to follow-up, with 90% power and 5% (two-sided) level of significance.
Data analysis
At baseline study, Shapiro–Wilk test will be used to check whether the data are normally distributed. We will compare the difference between two groups on patient demographics, medication adherence, systolic and diastolic blood pressure using chi-square test or independent-samples t-test or Mann–Whitney test. Continuous variables will be reported as mean with standard deviation for normal data or medians with inter-quartile ranges for non-normal data. Categorical data will be presented as frequencies and percentages. Logistic regression will be performed using medication adherence and blood pressure as outcome variables to analyze the potential factors affecting them.
We will analyze the primary outcome using mix-effect model on repeated data collected at 3 and 6 months. Since repeated observations are measured within each subject, mixed models will be used to test intervention effects while taking into account within-subjects correlation. As for the secondary outcome, blood pressure control will be analyzed using mixed-effect logistic regression models. Intention-to-treat analysis will be used where all participants remain in the allocated group irrespective of their adherence with the protocol.41 After the study, data will be entered on a double-entry basis by research assistants to ensure the quality of data and then the statistician will receive anonymous data at the end of the trial.
All data analysis will be analyzed using SPSS 18.0 and P<0.05 is considered to be significant.
Morisky Widget & Morisky medication adherence protocol training
The Morisky Widget & Morisky Medication Adherence Protocol Training for pharmacy students was conducted over 2 days (20–21 July 2018) by Professor Morisky and his colleagues in the MMAS research group. Professors, lecturers and pharmacy students in their master and PhD degree attended the training course. The training included 3 sessions: interactive discussion, Morisky Training Test and Morisky Widget. On the first day, the training included demonstration and discussion on the proper use of MMAS-8 and students were asked to finish Morisky Training Evaluation test after the training. Only those students who answered 80% of questions in the evaluation correctly were qualified for the second day’s training. On the second day, the qualified students observed role playing based on responses to the Morisky Widget to identify problems with medication adherence, like forgetfulness and conducted two simulated conversations with each other. The students checked the overall score, intentional and unintentional score to conduct personal consultation.
The role-playing process was evaluated by Professor Morisky. General and individual feedback was given to students after the evaluation. A total of 8 professors, lecturers and students were certificated by the MMAS research group and Professor Morisky. In total, 3 pharmacy students in their second or third years of the master curriculum were qualified by MMAS research group. To avoid inter-student variations, only one pharmacy student will deliver consultation and conduct all intervention sessions at baseline throughout the study.52
Ethical statement
Ethical approval for the study was obtained from the Research Ethics Committee of Health Science Center, Xi’an Jiaotong University (No.2018531). During the investigation, the investigator will explain the purpose and related content of the survey to participants and obtain patients’ informed consent. The study will be conducted in accordance with the Declaration of Helsinki. All the data will be stored in a password protected file and can only be accessed by statistician in the study.
Discussion
This study is designed to answer whether personal consultation by pharmacy students and SMS reminders in addition to standard pharmaceutical care is effective in improving patient medication adherence and blood pressure control. We will assess the efficacy and acceptability of consultation and integrating different aspects of clinical care through an open-source online platform.
Personal consultation by pharmacy students will alleviate the problem of shortage of clinical pharmacists in the People's Republic of China and SMS is widely used and at low cost which can be integrated into clinical care. According to a meta-analysis53 about text message intervention, it showed that daily reminders may lead to response fatigue and possible intrusion and showed smaller effects than interventions that messaged several times a week or weekly. In order to deliver as much as information and avoid response fatigue, we chose 3-day intervals to send messages. A feasible and preliminarily effective intervention in this study could lead to clinical trials conducted in a larger scale to benefit more patients and reduce hypertension-related morbidity and mortality.
Moreover, most of the intervention studies in the People's Republic of China focus on patient medication adherence rather than their blood pressure control. Little is known about the blood pressure control after intervention. However, in our study, we will collect data at months 0, 3 and 6 to check whether our intervention is effective to reduce patient blood pressure and we will use real-time adherence and blood pressure measurements to provide immediate feedback to patients which will help them to understand the importance of being adherent to their medication regimens. SMS reminders and pharmacy students-lead consultation are low-cost approaches and can be easily integrated into daily practice. We will send messages via a third-party website which is highly available and affordable in community settings. Through the intervention, medical staff participating in the study will realize the importance of medication adherence for addressing chronic disease management in communities.
Our study has several limitations. First of all, medication adherence is measured by patient self-report and may overestimate their medication adherence. However, MMAS-8 has high validity and reliability and is widely used in measuring medication adherence.47 Self-reported measures could be simple, inexpensive, and straightforward and therefore can be conveniently administered in research and clinical practice settings.54 Second, due to our time cost, response burden and fund limitation, only one city will be investigated and could not be extended to the whole province, but the sample is rather representative. Third, the study will last for 6 months; therefore, we will be unable to determine the effect of medication adherence on longer term outcomes, including hypertension-related stroke, myocardial infarction, acute coronary syndrome, heart failure, hospitalization, ER visits, morbidity and mortality. But the study is not designed to detect the effect of medication adherence and blood pressure on other clinical outcomes such as the occurrence of stroke and heart disease. Additionally, we will implement our study to a larger scale if the intervention is effective in lowering patient blood pressure to address the limitation and we will explore other intervention methods such as telephone calls and mobile phone applications to make sure the sustainability of our study in future studies. Finally, SMS may be less effective in patients with low education level or live in the remote areas. But we exclude patients who are illiterate, and we will send messages in Chinese understood by patients with low education background and we will tell patients to read their messages sent by Xi’an Jiaotong University during the consultation. Furthermore, SMS is the most accessible and inexpensive way to remind patients to take their medicine and educate them about self-care management knowledge.
The study addresses the challenge of high prevalence of hypertension and low medication adherence to long-term treatment. SMS reminders and consultation may be an effective way to improve medication adherence and manage blood pressure in community settings.
Ethics approval and consent to participate
Ethical approval was obtained from the Research Ethics Committee of Health Science Center, Xi’an Jiaotong University. Written informed consent will be obtained from patients before enrolling in this study and patients are free to withdraw throughout the study.
Acknowledgments
The MMAS (8-item) content, name and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from Donald E. Morisky, ScD, ScM, MSPH, 14725 NE 20th St Bellevue, WA 98007, USA; [email protected]. We are grateful for the patients, nurses, physicians for taking part in this trial. The trial is funded by “Natural Science Foundation of China” and was approved by the Xi’an Jiaotong University’s Research Ethics Committee. The authors are solely responsible for the study design, field study, data analysis and draft the manuscript and the final protocol.
Author contributions
This is a collaborative research, each of the listed people provided important intellectual contribution to study design. PPZ drafted the protocol. PPZ, QL, AHG and KH drafted the final manuscript while DEM and YF revised the final protocol. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Dr Morisky is the developer/owner of the copyrighted and trademarked protected Morisky Medication Adherence Scale and sells MMAS licenses and consulting services through MMAS Research LLC, 14725 NE 20th St., Bellevue, Washington 98007. Dr Morisky also reports personal fees from MMAS Research LLC, during the conduct of the study; receives personal fees from MMAS Reasearch, LLC, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217–223. doi:10.1016/S0140-6736(05)17741-1
2. Guilbert JJ. The world health report 2002 – reducing risks, promoting healthy life. Educ Health (Abingdon). 2003;16(2):230.
3. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R;
4.
5. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
6. Krousel-Wood M, Thomas S, Muntner P, Morisky D. Medication adherence: a key factor in achieving blood pressure control and good clinical outcomes in hypertensive patients. Curr Opin Cardiol. 2004;19(4):357–362.
7. Butler RJ, Davis TK, Johnson WG, Gardner HH. Effects of nonadherence with prescription drugs among older adults. Am J Manag Care. 2011;17(2):153–160.
8. MacLaughlin EJ, Raehl CL, Treadway AK, Sterling TL, Zoller DP, Bond CA. Assessing medication adherence in the elderly: which tools to use in clinical practice? Drugs Aging. 2005;22(3):231–255. doi:10.2165/00002512-200522030-00005
9. Foreman KF, Stockl KM, Le LB, et al. Impact of a text messaging pilot program on patient medication adherence. Clin Ther. 2012;34(5):1084–1091. doi:10.1016/j.clinthera.2012.04.007
10. Bobrow K, Brennan T, Springer D, et al. Efficacy of a text messaging (SMS) based intervention for adults with hypertension: protocol for the StAR (SMS Text-message Adherence suppoRt trial) randomised controlled trial. BMC Public Health. 2014;14:28. doi:10.1186/1471-2458-14-28
11.
12. Ruan Y, Xiao X, Chen J, Li X, Williams AB, Wang H. Acceptability and efficacy of interactive short message service intervention in improving HIV medication adherence in Chinese antiretroviral treatment-naive individuals. Patient Prefer Adherence. 2017;11:221–228. doi:10.2147/PPA.S120003
13. Schroeder K, Fahey T, Ebrahim S. How can we improve adherence to blood pressure-lowering medication in ambulatory care? Systematic review of randomized controlled trials. Arch Intern Med. 2004;164(7):722–732. doi:10.1001/archinte.164.7.722
14. Varleta P, Acevedo M, Akel C, et al. Mobile phone text messaging improves antihypertensive drug adherence in the community. J Clin Hypertens (Greenwich). 2017;19(12):1276–1284. doi:10.1111/jch.13098
15. Leon N, Surender R, Bobrow K, Muller J, Farmer A. Improving treatment adherence for blood pressure lowering via mobile phone SMS-messages in South Africa: a qualitative evaluation of the SMS-text Adherence SuppoRt (StAR) trial. BMC Fam Pract. 2015;16:80. doi:10.1186/s12875-015-0289-7
16. Lester RT, Ritvo P, Mills EJ, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–1845. doi:10.1016/S0140-6736(10)61997-6
17. Vervloet M, van Dijk L, Santen-Reestman J, et al. SMS reminders improve adherence to oral medication in type 2 diabetes patients who are real time electronically monitored. Int J Med Inform. 2012;81(9):594–604. doi:10.1016/j.ijmedinf.2012.05.005
18. Wang K, Wang C, Xi L, et al. A randomized controlled trial to assess adherence to allergic rhinitis treatment following a daily short message service (SMS) via the mobile phone. Int Arch Allergy Immunol. 2014;163(1):51–58. doi:10.1159/000356317
19. Thakkar J, Kurup R, Laba T-L, et al. Mobile telephone text messaging for medication adherence in chronic disease: a meta-analysis. JAMA Intern Med. 2016;176(3):340–349. doi:10.1001/jamainternmed.2015.7667
20. Fang R, Li X. Electronic messaging support service programs improve adherence to lipid-lowering therapy among outpatients with coronary artery disease: an exploratory randomised control study. J Clin Nurs. 2016;25(5–6):664–671. doi:10.1111/jocn.12988
21. Guo Y, Xu Z, Qiao J, et al. Development and feasibility testing of an mHealth (Text Message and WeChat) intervention to improve the medication adherence and quality of life of people living with HIV in China: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2018;6(9):e10274. doi:10.2196/10274
22. Kannisto KA, Korhonen J, Adams CE, Koivunen MH, Vahlberg T, Valimaki MA. Factors associated with dropout during recruitment and follow-up periods of a mHealth-based randomized controlled trial for mobile.net to encourage treatment adherence for people with serious mental health problems. J Med Internet Res. 2017;19(2):e46. doi:10.2196/jmir.6417
23. Santschi V, Chiolero A, Colosimo AL, et al. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. J Am Heart Assoc. 2014;3(2):e000718. doi:10.1161/JAHA.114.000844
24. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169(21):1996–2002. doi:10.1001/archinternmed.2009.358
25. Morgado M, Rolo S, Castelo-Branco M. Pharmacist intervention program to enhance hypertension control: a randomised controlled trial. Int J Clin Pharm. 2011;33(1):132–140. doi:10.1007/s11096-010-9474-x
26. Fikri-Benbrahim N, Faus MJ, Martinez-Martinez F, Sabater-Hernandez D. Impact of a community pharmacists‘ hypertension-care service on medication adherence. The AFenPA study. Res Social Adm Pharm. 2013;9(6):797–805. doi:10.1016/j.sapharm.2012.12.006
27. Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication adherence and persistence, blood pressure, and low-density lipoprotein cholesterol: a randomized controlled trial. JAMA. 2006;296(21):2563–2571. doi:10.1001/jama.296.21.joc60162
28. Lau R, Stewart K, McNamara KP, et al. Evaluation of a community pharmacy-based intervention for improving patient adherence to antihypertensives: a randomised controlled trial. BMC Health Serv Res. 2010;10:34. doi:10.1186/1472-6963-10-302
29. Svarstad BL, Kotchen JM, Shireman TI, et al. Improving refill adherence and hypertension control in black patients: Wisconsin TEAM trial. J Am Pharm Assoc (2003). 2013;53(5):520–529. doi:10.1331/JAPhA.2013.12246
30. Abughosh S, Wang X, Serna O, et al. A motivational interviewing intervention by pharmacy students to improve medication adherence. J Manag Care Spec Pharm. 2017;23(5):549–560. doi:10.18553/jmcp.2017.23.5.549
31. Odegard PS, Carpinito G, Christensen DB. Medication adherence program: adherence challenges and interventions in type 2 diabetes. J Am Pharm Assoc (2003). 2013;53(3):267–272. doi:10.1331/JAPhA.2013.12065
32. Szkiladz A, Carey K, Ackerbauer K, Heelon M, Friderici J, Kopcza K. Impact of pharmacy student and resident-led discharge counseling on heart failure patients. J Pharm Pract. 2013;26(6):574–579. doi:10.1177/0897190013491768
33. Chou TI, Lash DB, Malcolm B, et al. Effects of a student pharmacist consultation on patient knowledge and attitudes about vaccines. J Am Pharm Assoc (2003). 2014;54(2):130–137. doi:10.1331/JAPhA.2014.13114
34. Pastakia SD, Vincent WR
35. Chan A-W, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
36.
37. Yang SM. Chinese Pharmaceutical Law and Regulations.
38. Haugbolle LS, Sorensen EW, Henriksen HH. Medication- and illness-related factual knowledge, perceptions and behaviour in angina pectoris patients. Patient Educ Couns. 2002;47(4):281–289.
39. Morisky DE, DiMatteo MR. Improving the measurement of self-reported medication nonadherence: response to authors. J Clin Epidemiol. 2011;64(3):
40. Haramiova Z, Stasko M, Hulin M, Tesar T, Kuzelova M, Morisky DM. The effectiveness of daily SMS reminders in pharmaceutical care of older adults on improving patients‘ adherence to antihypertensive medication (SPPA): study protocol for a randomized controlled trial. Trials. 2017;18(1):334. doi:10.1186/s13063-017-2063-8
41. Bobrow K, Farmer AJ, Springer D, et al. Mobile phone text messages to support treatment adherence in adults with high blood pressure (SMS-Text Adherence Support [StAR]): a single-blind, randomized trial. Circulation. 2016;133(6):592–600. doi:10.1161/CIRCULATIONAHA.115.017530
42. Gu J, Zhang X-J, Wang T-H, Zhang Y, Chen Q. Hypertension knowledge, awareness, and self-management behaviors affect hypertension control: a community-based study in Xuhui District, Shanghai, China. Cardiology. 2014;127(2):96–104. doi:10.1159/000355576
43. Berlowitz DR, Foy CG, Kazis LE, et al. Effect of intensive blood-pressure treatment on patient-reported outcomes. N Engl J Med. 2017;377(8):733–744. doi:10.1056/NEJMoa1611179
44. Bilal M, Haseeb A, Lashkerwala SS, et al. Knowledge, awareness and self-care practices of hypertension among cardiac hypertensive patients. Glob J Health Sci. 2015;8(2):9–19. doi:10.5539/gjhs.v8n2p9
45. Xu B, Xu Z, Xu X, Cai Q, Xu Y. Prevalence, awareness, treatment, and control of hypertension among residents in Guangdong Province, China, 2004 to 2007. Circ Cardiovasc Qual Outcomes. 2013;6(2):217–222. doi:10.1161/CIRCOUTCOMES.111.000062
46. Siu AL;
47. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich). 2008;10(5):348–354.
48. Yan J, You L-M, Yang Q, et al. Translation and validation of a Chinese version of the 8-item Morisky medication adherence scale in myocardial infarction patients. J Eval Clin Pract. 2014;20(4):311–317. doi:10.1111/jep.12125
49. Lu J, Lu Y, Wang X, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet. 2017;390(10112):2549–2558. doi:10.1016/S0140-6736(17)32478-9
50. Collins R, Peto R, MacMahon S, et al. Blood pressure, stroke, and coronary heart disease. Part 2, short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335(8693):827–838.
51. Liu Z, Chen S, Zhang G, Lin A. Mobile phone-based lifestyle intervention for reducing overall cardiovascular disease risk in Guangzhou, China: a pilot study. Int J Environ Res Public Health. 2015;12(12):15993–16004. doi:10.3390/ijerph121215037
52. Wong MC, Liu KQ, Wang HH, et al. Effectiveness of a pharmacist-led drug counseling on enhancing antihypertensive adherence and blood pressure control: a randomized controlled trial. J Clin Pharmacol. 2013;53(7):753–761. doi:10.1002/jcph.101
53. Finitsis DJ, Pellowski JA, Johnson BT. Text message intervention designs to promote adherence to antiretroviral therapy (ART): a meta-analysis of randomized controlled trials. PLoS One. 2014;9(2):e88166. doi:10.1371/journal.pone.0088166
54. Pednekar PP, Agh T, Malmenas M, et al. Methods for measuring multiple medication adherence: a systematic review-report of the ISPOR Medication Adherence and Persistence Special Interest Group. Value Health. 2019;22(2):139–156. doi:10.1016/j.jval.2018.08.006
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.