Back to Journals » Journal of Inflammation Research » Volume 19
The Impact of Obesity on Airway Inflammation, Lung Function and Biologic Treatment in Asthma: A Narrative Review
Authors Hadžić B, Vasbinder EC, Lek RM, Castro Cabezas M, Braunstahl GJ ![]()
Received 9 March 2026
Accepted for publication 9 May 2026
Published 5 June 2026 Volume 2026:19 554138
DOI https://doi.org/10.2147/JIR.S554138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Benjamin Hadžić,1 Erwin C Vasbinder,1 Rob M Lek,1 Manuel Castro Cabezas,2,3 Gert-Jan Braunstahl4,5
1Department of Hospital Pharmacy, Franciscus Gasthuis & Vlietland, Rotterdam, The Netherlands; 2Department of Internal Medicine, Franciscus Gasthuis & Vlietland, Rotterdam, The Netherlands; 3Julius Clinical, Zeist, The Netherlands; 4Department of Pulmonology, Franciscus Gasthuis & Vlietland, Rotterdam, The Netherlands; 5Department of Pulmonology, Erasmus MC, Rotterdam, The Netherlands
Correspondence: Benjamin Hadžić, Department of Hospital Pharmacy, Franciscus Gasthuis En Vlietland, Kleiweg 500, Rotterdam, 3045 PM, The Netherlands, Email [email protected]
Abstract: Obesity and asthma are two chronic conditions with increasing global prevalence. The interplay between obesity and asthma has created a distinct “obese asthma phenotype” characterized by increased disease severity, poorer symptom control and altered treatment response. This phenotype is driven by complex interactions between mechanical factors, chronic low-grade systemic inflammation and metabolic dysfunction. Since the last decades biologics are used to treat patients with severe asthma. These therapies act on specific inflammatory pathways, so it is plausible that obesity-related metabolic and inflammatory alterations may alter their effectiveness. Obese patients can have both type-2 high and type-2 low (T2-low) endotypes, although there seems to be a shift towards T2-low asthma, with increased airway neutrophils and altered cytokine profiles. Current biologics targeting several cytokines demonstrate varying results in treatment efficacy in obese asthma patients, whereas tezepelumab shows the most benefit. Several mechanisms have been proposed for reduced efficacy of biologics in this population through mechanisms involving pharmacokinetics/dynamics, inflammatory and immunologic pathways. Obese patients frequently exhibit persistent symptoms despite treatment, suggesting incomplete disease control. Understanding the relationship of obesity and asthma is critical in determining optimal management and requires integrated strategies addressing both airway inflammation and metabolic dysfunction. Several emerging therapies, like glucagon-like peptide-1 receptor agonists (GLP-1) show promise through mechanisms extending beyond weight reduction. Future research priorities include trials in obese populations to optimize biologic dosing, improved biomarker research and develop precision medicine treatments to transform this complex interplay of conditions into a manageable multisystem disease. This review aims to assess current evidence regarding the link between asthma and obesity, biologic responsiveness in this population and to explore potential mechanisms, clinical implications, new therapeutic possibilities and areas for future research.
Keywords: adiposity, efficacy, pharmacokinetics, immunology
Introduction
Asthma and obesity have been recognized as a disease burden for centuries. Hippocrates mentioned the effects of obesity over 2000 years ago and he also introduced the term “asthma”.1–3 Even though the interplay between obesity and respiratory problems was not yet established until 1956, there is historic evidence of physicians treating asthmatic patients with a stricter diet.3,4 These early observations underscore a long-standing awareness of the potential link between metabolic status and respiratory health. Although the conceptualization of asthma and obesity has evolved substantially since antiquity, these insights highlight that the coexistence of these conditions is far from a modern phenomenon.
Nowadays asthma and obesity are two chronic conditions with increasing global prevalence over the past decades. Around 262 million people were affected by asthma in 2019, while the estimate for obesity prevalence is 890 million globally, and is predicted to keep growing.5–7 Asthma prevalence in adults in the United States is 7,1% in lean individuals versus 11,1% in obese individuals.8 Even more, the prevalence of obesity has increased more in subjects with asthma than in those without.9 The parallel increase of these conditions presents a growing clinical challenge as excess adiposity may influence asthma severity, symptom control and response to pharmacotherapy in a bi-directional multifactorial fashion through mechanical, immunologic and inflammatory pathways.8,10–12
Epidemiological data suggest that individuals with obesity often experience more severe or difficult-to-control asthma, highlighting the importance of understanding disease mechanisms in this subgroup.13,14 Obesity is a well-established modifier of disease expression and treatment response across multiple chronic conditions, including type 2 diabetes mellitus (DMII), cardiovascular disease, non-alcoholic steatohepatitis, and the metabolic syndrome.15,16 Shared pathophysiological mechanisms, such as chronic low-grade systemic inflammation, altered adipokine signaling and immune dysregulation, suggest that obesity may similarly influence respiratory disease.17–19 The recognition of an “obese asthma phenotype” has emerged from this understanding, characterized by increased disease severity, poorer symptom control and reduced responsiveness to conventional therapy.18,20
Asthma management has undergone substantial evolution. Historically, treatment relied on bronchodilators and corticosteroids, but the past two decades we have seen the emergence of biologic therapies targeting specific inflammatory pathways, including immunoglobulin E (IgE), interleukin (IL)-5, IL-4/13 and thymic stromal lymphopoietin (TSLP).3,20–23 These agents have significantly improved outcomes in selected patients with severe asthma. However, pivotal clinical trials frequently underrepresent individuals with obesity as shown by Akenroye et al, raising the question whether excess adiposity may modify therapeutic efficacy.24
Since biologic therapies act on specific inflammatory pathways, it is plausible that obesity-related metabolic and inflammatory alterations may alter their effectiveness, as shown in several studies in asthma, but also in inflammatory bowel diseases (IBD).18,25
Obesity and Airway Inflammation
Asthma is a chronic inflammatory airway disease that is predominantly characterized by type 2 (T2) inflammation, which is present in over 80% of patients. In contrast, asthma associated with obesity is more frequently characterized by a non–type 2, type 1 (T1) and T-helper 17 (Th17)–skewed endotype, diverging from the classical eosinophilic phenotype.26 Consistent with this observation, sputum eosinophils and fractional exhaled nitric oxide (FeNO) are generally lower in obese asthma patients than in non-obese asthma patients.27 However, some studies have reported higher numbers of eosinophils in sputum and submucosa in subsets of obese asthma patients.28,29 This could probably be related to severity asthma and/or class of obesity, as discussed further on.
Importantly, blood eosinophil counts appear to perform poorly as a biomarker of airway type 2 inflammation in morbidly obese patients. Peters et al demonstrated a strong modifying effect of body mass index (BMI) on the relationship between blood eosinophil counts and sputum type 2 cytokine gene expression (T2GM) While blood eosinophil levels correlated well with sputum T2GM in patients with a BMI < 40 kg/m2, this association progressively weakened with increasing BMI and was minimal in morbid obesity.30 In contrast, sputum neutrophils were positively associated with BMI and have been shown to decrease following dietary weight-loss intervention.31,32
Eosinophils are increasingly recognized as regulators of metabolic homeostasis in adipose tissue, with roles in adipokine secretion and inflammation, suggesting relevance for obesity-related asthma.33 Adipose tissue eosinophils exhibit distinct transcriptional and functional properties compared with airway eosinophils, which are known to promote airway hyperresponsiveness through neural mechanisms, such as altered sensory signaling, autonomic imbalance or release of neuropeptides.20 These observations underscore the importance of anatomical context and highlight that blood eosinophil counts alone do not adequately reflect tissue-specific eosinophil contributions to asthma pathophysiology.
Interleukin-17 (IL-17) has been associated with corticosteroid resistance by altering the balance between glucocorticoid receptor (GR) isoforms, with dysregulated GR-α and GR-β expression in adipocytes.34 Adipocytes obtained from obese patients cultured in vitro in the presence of IL-17A for 48 hours showed a decrease in GRα/GRβ ratio as compared to adipocytes from lean subjects where GR-α/GR-β ratio was increased following IL-17A and IL-17F stimulation. In addition, IL-17–driven cytokine signaling contributes to the amplification of pro-inflammatory mediator production in obesity. Consistent with these observations, a negative association was demonstrated between BMI and the GR-α/GR-β ratio in the serum of patients with asthma.34 So obesity leads to increased IL-17 signaling that may induce corticosteroid resistance.
Airway hyperresponsiveness (AHR) in obesity has been linked to the expansion of CCR6⁺ type 3 innate lymphoid cells (ILC3s) in bronchoalveolar lavage (BAL) fluid in obese murine models, supporting the existence of an alternative T2-low inflammatory pathway.35 In line with these findings, recent human data indicate increased activation and pulmonary recruitment of total ILCs and ILC3s in obese asthma patients. Moreover, asthma severity has been associated with elevated numbers of activated ILC subsets, particularly Cluster of Differentiation (CD)69+, CD161⁺ total ILCs, ILC2s, and ILC3s.36
Visceral adipose tissue (VAT) accumulation in obesity creates a hypoxic microenvironment that promotes differentiation of adipose tissue macrophages (ATMs) toward a pro-inflammatory phenotype. This results in increased secretion of mediators such as interleukin-6 (IL-6) and leptin, which are linked to T-helper 1 (Th1)-mediated immune responses.37 While abdominal circumference rather than overall VAT macrophage burden was found to be most strongly associated with asthma outcomes, obese asthmatic patients exhibited a higher proportion of pro-inflammatory macrophages (M1) ATMs compared with obese non-asthmatic controls. Furthermore, the VAT M1:M2 macrophage ratio was negatively associated with FEV1 (% predicted).38 Therefore, visceral inflammation with increased pro-inflammatory M1 occurs in obese asthma and may be a determinant of systemic inflammation and asthma severity.
Macrophage infiltration of VAT has also been associated with increased leptin and reduced adiponectin expression independent of BMI.39 Airway epithelial cells express receptors for both adipokines, and airway reactivity has been shown to correlate with visceral fat–derived leptin expression.39 These immunometabolic effects are mediated, at least in part, by insulin resistance and dyslipidemia, hallmark features of obesity.40
Obesity may further promote airway dysfunction through increased oxidative stress driven by adipokine imbalance. Elevated leptin levels have shown to induce airway smooth muscle contraction, an effect potentiated by epithelial injury or allergen sensitization.41 Conversely, adiponectin appears to exert protective effects on human bronchial epithelial cells against mechanical and oxidative injury.42 In experimental models of obese asthma, markers of oxidative stress, including 4-hydroxynonenal (4-HNE), isoprostanes, and hydrogen peroxide, were significantly higher in high-fat diet–fed mice than in controls.43 In human studies, plasma 8-isoprostane concentrations were significantly higher in obese children than in lean controls, further supporting a role for systemic oxidative stress in obesity-related asthma.44
In summary, asthma is usually linked to type 2 inflammation, but obesity-related asthma often shows a T2-low, type 1–skewed inflammatory profile with lower FeNO, sputum eosinophils, and less reliable blood eosinophil biomarkers. Higher BMI is connected to neutrophilic airway inflammation, increased ILC3 cells, and greater airway hyperresponsiveness. A type 3 (T3) inflammation in obese patients is also proposed, which is mediated by domain-like receptor protein 3 (NLRP3), Th 17 cells and type 17 cytotoxic (tc17) cells.18 Visceral fat–related immunometabolic disturbance, adipokine imbalance, and oxidative stress likely worsen lung function and asthma severity in obese individuals.
Obesity and Lung Function
Obesity influences asthma through the combined effects of altered respiratory mechanics and obesity-related immunometabolic dysregulation. The accumulation of subcutaneous adipose tissue along the chest wall and visceral fat within the abdomen restricts diaphragmatic excursion and chest wall expansion, resulting in reduced lung compliance and a predominantly restrictive ventilatory pattern.10 These effects are most pronounced in functional residual capacity (FRC) and expiratory reserve volume (ERV), while total lung capacity (TLC) is only modestly affected.10,45–47 During dynamic lung function testing, both forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) are reduced, whereas the FEV1/FVC ratio is generally preserved,10,47 except in individuals with concomitant metabolic syndrome, underscoring the contribution of systemic metabolic dysfunction.48
Given that dynamic hyperinflation with air trapping is already present in up to 81% of non-obese asthma patients,49 obesity is expected to further exacerbate air trapping and small airway dysfunction, particularly due to breathing at chronically low lung volumes.10,46,50 These mechanical effects may amplify airflow limitation and contribute to increased disease severity. Although oxygen saturation may be reduced in obese patients with asthma, particularly in the supine position, diffusion capacity is typically preserved or increased.51,52 Therefore, hypoxemia is more likely attributable to restrictive lung mechanics and ventilation perfusion mismatch resulting from compression of the dependent lower lung regions.53,54
Exercise capacity is reduced in obese asthma patients reflected by a decreased six-minute walking distance (6MWD) and Maximum Volume O2 (VO2max) compared to non-obese asthma patients.55 High intensity interval training (HIIT) resulted in greater improvement of cardiopulmonary fitness (VO2max) and a greater reduction of body fat mass compared to traditional exercise.56 HIIT also provided sustained improvements in asthma control, body composition and exercise capacity in obese asthmatics that were not optimally controlled.46
Importantly, the impact of obesity on lung function is not adequately captured by BMI alone but is strongly influenced by body fat distribution. Elevated visceral to subcutaneous fat area ratio (EV) measured on computed tomography (CT) was associated with decreased airway lumen diameter and a lower FEV1.57 Individuals with predominant abdominal (android or “apple-shaped”) adiposity have a higher prevalence of asthma than those with predominantly gluteofemoral (gynoid or “pear-shaped”) fat distribution.58–60 This association appears particularly pronounced in women, as bronchial provocation studies have demonstrated greater airway hyperresponsiveness and delayed post-challenge recovery in obese women than in men.50,60
Several mechanisms may underlie obesity-related airway hyperresponsiveness. Breathing at low lung volumes is associated with enhanced bronchial hyperresponsiveness, potentially due to reduced outward tethering forces exerted by the lung parenchyma on the airways and increased airway smooth muscle shortening.61,62 In addition, closure of peripheral airways during tidal breathing near closing volume, especially in the supine position, leads to airflow limitation and increased peripheral airway resistance.53 Collectively, these mechanical alterations render the lung more susceptible to airway narrowing, creating a functional state that resembles asthma through obesity-related chest wall compression.
These biomechanical changes closely interact with obesity-related immunometabolic dysregulation. Expansion of visceral adipose tissue promotes a pro-inflammatory state with M1 macrophage activation and increased leptin and IL-6 production, driving Th1-skewed inflammation, insulin resistance, and impaired lung function.38–40 Adipokine imbalance further aggravates airway dysfunction, as leptin increases airway smooth muscle contractility while reduced adiponectin weakens epithelial protection;41,42 together with obesity-related oxidative stress43,44 and low lung volume breathing,53,63 this promotes small airway instability and airway hyperresponsiveness characteristic of obesity-related asthma.
Obesity and Asthma Mutual Influence on Disease Burden
Both, overdiagnosis and underdiagnosis of asthma occur in individuals with morbid obesity. In this population, symptom-based diagnosis alone is unreliable, and objective pulmonary function testing is essential to establish or refute the diagnosis of asthma.48 Indeed, approximately one-third of both obese and non-obese individuals with physician-diagnosed asthma do not have asthma when assessed objectively using bronchial provocation or reversibility testing.64,65 Notably, health-related quality-of-life scores do not differ significantly between subjects with and without demonstrable bronchial hyperresponsiveness, underscoring the limited specificity of symptoms alone in this context.65
Conversely, asthma may also remain unrecognised in obese individuals despite the presence of respiratory symptoms. The reasons for underdiagnosis are likely multifactorial. One explanation is symptom misperception at the patient level, whereby dyspnoea and exercise intolerance are attributed to excess body weight rather than to an underlying respiratory disorder, reducing the likelihood of seeking medical attention.66 Alternatively, diagnostic misattribution may occur at the physician level, with respiratory complaints being ascribed primarily to obesity rather than prompting objective evaluation for asthma.48
Beyond diagnostic challenges, obesity is increasingly recognised as a major disease modifier in asthma. Multiple studies have demonstrated that higher BMI is independently associated with poorer symptomatic control and impaired quality of life. In adult outpatient cohorts, increasing BMI correlates with higher Asthma Control Questionnaire (ACQ) scores and lower Asthma Quality of Life Questionnaire (AQLQ) scores, even after adjustment for age, sex and conventional markers of asthma severity, indicating a greater disease burden in obese compared with lean patients.67 These observations are supported by clinical and epidemiological data showing that obesity adversely affects asthma control across phenotypes, mediated by altered lung mechanics, systemic low-grade inflammation and reduced responsiveness to standard therapies.68,69
In terms of healthcare utilisation, obese individuals with asthma experience more acute exacerbations, emergency department visits and hospital admissions. Importantly, these adverse outcomes appear to improve following substantial weight loss, eg after bariatric surgery, suggesting a causal contribution of adiposity to exacerbation risk and acute care use.70 Meta-analytic data further indicate that obese adults with asthma require higher doses of inhaled corticosteroids, short-acting β2-agonists and systemic corticosteroids than their normal-weight counterparts.71
In addition to its clinical burden, obesity-related asthma is associated with substantial socioeconomic consequences, in which this association may be bi-directional. Several cohort studies have shown that obese individuals with asthma experience higher rates of work absenteeism and activity limitation compared with normal-weight asthmatics. Increased BMI is independently associated with a greater number of missed workdays, reduced work productivity and higher likelihood of work disability, reflecting both poorer asthma control and the additive impact of obesity-related comorbidities.67,72 In paediatric populations, obesity similarly amplifies asthma-related school absenteeism, with obese children with asthma missing more school days and reporting greater functional impairment than their lean peers, independent of asthma severity.73–75
From a health economic perspective, obesity substantially increases the direct and indirect costs of asthma. Obese patients with asthma incur higher healthcare expenditures driven by increased medication use, more frequent physician visits, emergency department presentations and hospitalisations.68,70,75 Indirect costs, including productivity loss due to absenteeism and presenteeism, further contribute to the societal burden. Importantly, obesity-related asthma has been identified as a key contributor to the overall economic burden of asthma at the population level, accounting for a disproportionate share of costs relative to prevalence.76 Interventions that result in sustained weight loss have been associated with reductions in healthcare utilisation, medication requirements and work productivity loss, underscoring the potential societal and economic benefits of targeting obesity as a modifiable trait in asthma management.70
Obesity and Treatment Response
Pharmacokinetics and Pharmacodynamics in Obesity
It is well known that obesity can influence many areas of pharmacokinetics (PK) and pharmacodynamics (PD), which makes it challenging to predict how a drug will behave. It has been shown that certain drugs have different levels in people with obesity, while others that share similar traits remain unaffected.77 In the following section the basic principles of general drug PK/PD will be briefly described, focusing on how obesity affects the absorption, distribution, metabolism and excretion (ADME) processes.
Absorption: Oral
Obesity influences PK in several ways. Obese people have a higher median gastric pH than lean people.77,78 Also, the lowest pH measured seems more variable in obese people than in lean people. It is well established that gastric pH can influence bioavailability and thus absorption of several drugs, for example in tyrosine kinase inhibitors (TKI). There is contradictory evidence that gastrointestinal motility and gastric emptying is either increased, not affected or decreased. Increased gastrointestinal motility and emptying could cause lower absorption of oral drugs that are absorbed from the stomach because of less time for solubilization. A similar effect on the gallbladder could explain an enhanced absorption of lipophilic molecules due to improved solubilization in the alkaline bile environment, after oral intake.77,78 These factors may play a role in the absorption of oral drugs used in obesity-related asthma, as will be mentioned later on.
Absorption: Subcutaneous
Subcutaneously administered large molecule drugs, like biologics, are absorbed slowly into the circulation through the lymphatic system, reaching peak plasma concentrations several days after injection.79
There are roughly two different types of distribution of excess adipose tissue in obese patients: gynoid and android obesity. Gynoid obesity manifests as increased subcutaneous fat, juxtaposed to increased visceral fat for android obesity.10 Visceral fat is connected to metabolic syndrome, and this has been linked to asthma.39 Gynoid obesity might interfere more with absorption of subcutaneous injections in general, because of a larger subcutaneous skin layer from which drug depots are released more slowly than from leaner skin tissue. Gouju et al describe a very limited effect of obesity on absorption of subcutaneous and transdermal applied medication. Although lower values for area under the curve (AUC) were found, efficacy was comparable. These changes in PK are most likely to be influenced by an increase of volume of distribution (Vd) and clearance (Cl).78
Distribution
Obesity can affect drug disposition, but no single variable adequately describes the PK changes for all drugs. Alterations in volume of distribution (Vd) are specific to each drug and rely on factors such as proportional fat mass (FM), tissue blood flow, and protein binding. These variables are determined by the physicochemical properties of the drug, including molecular size, degree of ionization, lipid solubility, and permeability across biological membranes.80
In obesity, most excess weight is gained as FM and this is stored in adipose tissue. With this weight gain the proportions of the body are altered. Lean body weight (LBW) increases only slightly compared to FM.78 The accumulation of FM in adipose tissue therefore lowers the proportional aqueous compartment. Theoretically, Vd should therefore increase namely for lipophilic molecules. For some drugs, such as benzodiazepines this has been observed in research, in which is shown that an increased Vd lead to less clearance and subsequent prolonged half lives.77,78 However, Smit et al have shown that this is not always the case as propofol and digoxin do not have an increased Vd in obese subjects, because of accumulation in different organs like the heart and liver, instead of FM.77
Metabolism/Elimination
In obesity there are often abnormalities in the liver. Obesity can cause liver injury, which can reduce the total clearance capacity of the liver.80 However, obesity can also cause an increased liver blood flow through an increased cardiac output.77 Thus, if clearance is mainly affected by liver blood flow, elimination is enhanced. However, if clearance is mainly affected by intrinsic metabolizing capacity, then elimination could be decreased because of hepatic impairment.77
In general, small drug metabolism consists of two phases: Phase I and Phase II. Enzymes of the cytochrome P450 (CYP) family play an important role in phase I metabolism, mainly modifying the drug by oxidation. Phase II metabolism consists of conjugation reactions, mainly via glucuronidation and sulfation.77,78 Glucuronidation and sulfation are increased, while CYP3A4 activity is reduced in obese people.77,80 For drugs that are metabolized by CYP3A4 no changes have been seen in humans. Most likely, clearance of these drugs depends more on liver blood flow than on CYP enzymes. In large molecules, such as biologics, different metabolizing steps are undertaken, as will be discussed later on.
Many drugs are eliminated by the kidneys. It is not completely understood how obesity affects kidney function. Obese subjects most likely exhibit higher total CL, however CL does not linearly increase with total body weight (TBW).80
Corticosteroid Efficacy in Obese Patients
It is well known that obese patients are less responsive to corticosteroids, as mentioned in earlier sections. Since corticosteroids are lipophilic substances one might expect that they will accumulate in adipose tissue. However, obese people have higher baseline cortisol levels than normal weight individuals.81 It is also possible that low grade inflammation lowers the threshold for action by corticosteroids. This might counteract the distribution of corticosteroids towards adipose tissue. Therefore, a decreased response to treatment with corticosteroids is seen in obese asthma patients.21,71,82 Corticosteroids are partially metabolized by CYP3A4. Chronic low-grade inflammation due to obesity causes a downregulation of CYP3A4. However, this is usually only clinically relevant in cases of morbid obesity. However, also asthma patients with a lower degree of obesity have decreased efficacy of corticosteroids.10,21,71 It is possible that IL-17 mediated dysregulation of GR-α and GR-β, as mentioned earlier, explains the unresponsiveness of obese asthmatics to corticosteroids.34
Potential Mechanisms for Reduced Biologic Efficacy
The effects of obesity on the pharmacodynamics and kinetics of drugs in general, as previously discussed, are important to consider regarding the potential mechanisms for reduced biologic efficacy in obese asthmatic patients. Reduced biologic efficacy in obese patients has already been shown in other indications like IBD,25 but also recently in severe asthma by Gonem et al.83
Several mechanisms have been proposed. The pharmacokinetic mechanisms contributing to the diminished effectiveness of biologic therapies in obese patients with asthma are not yet fully elucidated. Current consensus suggests that pharmacokinetic alterations alone are unlikely to fully account for reduced biologic efficacy in this group. Nevertheless, several plausible pharmacokinetic mechanisms have been proposed, as shown in Figure 1.
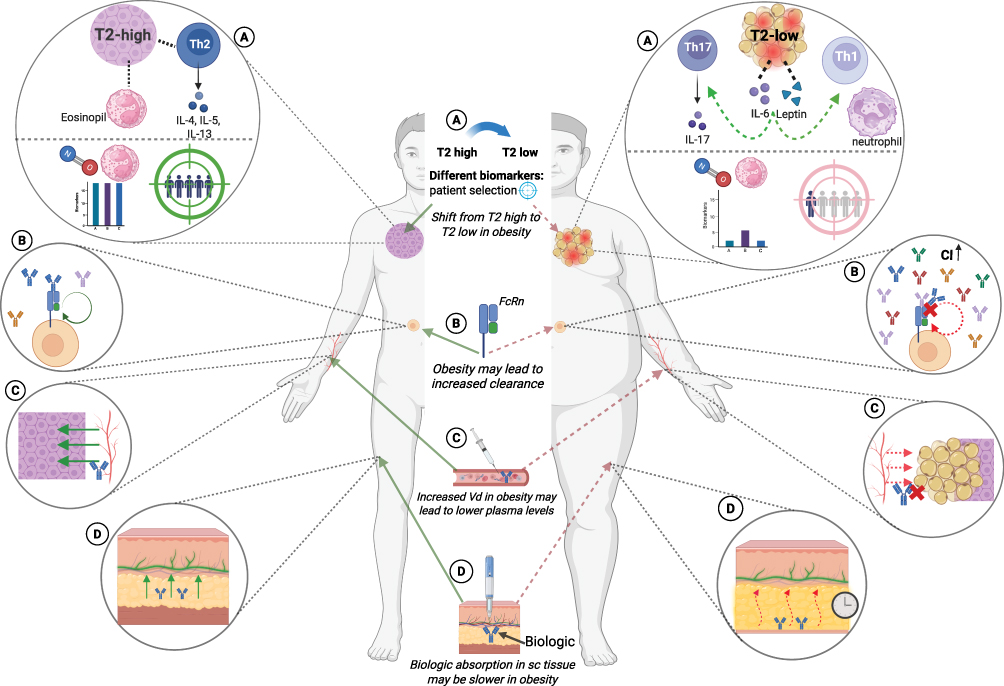 |
Figure 1 Possible mechanisms for reduced efficacy of biologics in obese asthma patients (A-D). FIGURE MADE WITH BIORENDER.COM. (A) Chronic low grade inflammation and altered immune cell function may lead to reduced biologic drug concentrations at target sites and modify immune responses. Elevated levels of IL-6 and other adipokines, like leptin, that are associated with obesity may modulate immune responses and cause a shift away from T2 -high toward a T2-low inflammatory profile, characterized by increased neutrophilic rather than eosinophilic inflammation pathway. Also, because of the heterogeneity of obesity, there is variable expression of biomarkers such as blood eosinophils and FeNO. This complicates patient selection and monitoring for biologic therapy. (B) Biologics are protected of clearance via neonatal fc receptor (FcRn). In obese patients there is accumulation of several forms of IgG in adipose tissue, which may lead to saturated FcRn’s. This may lead to more clearance of biologics and consequently a reduced drug exposure. (C) Increased body mass and adiposity may theoretically increase the Vd of mAbs possibly resulting in lower plasma peak levels. Despite being engineered for high-affinity binding to target tissue sites, which could imply large apparent Vd in obese patients, mAbs generally do not exhibit extensive tissue distribution in practice. Clinical evidence for this mechanism is limited. Given the molecular size of biologics and their limited distribution in adipose tissue, this mechanism is not most plausible. (D) Because of their large size, biologics are mostly absorbed slowly through lymphatic transport. Obesity increases subcutaneous tissue thickness and alters tissue composition. This may lead to slower and less predictable absorption. Precipitation and catabolism may also play a role in diminished efficacy. |
First, increased body mass and adiposity may theoretically increase the volume of distribution of monoclonal antibodies (mAbs), potentially resulting in lower peak and trough serum concentrations when fixed dosing regimens are used. Despite being engineered for high-affinity binding to target tissue sites, which could imply large apparent volumes of distribution, mAbs generally do not exhibit extensive tissue distribution in practice.79 This theoretical effect may be particularly relevant for biologics administered independently of body weight, such as, mepolizumab, benralizumab, dupilumab and tezepelumab, and could theoretically lead to subtherapeutic tissue exposure in individuals with high BMI. However, clinical evidence for this mechanism is limited and inconsistent. Moreover, pharmacokinetic studies indicate that bodyweight significantly affects both CL and Vd.79 Nevertheless, most pharmacokinetic studies indicate that different mAbs show a lot of similarities in their pharmacokinetic profile.84 Therefore, it may be possible that mAbs maintain relatively stable serum concentrations across BMI categories, possibly due to their large molecular size and limited distribution into adipose tissue.
Secondly, obesity increases subcutaneous tissue mass and alters tissue composition, which can slow and reduce the absorption of drugs administered by subcutaneous or intramuscular injection. Slower and less predictable absorption from subcutaneous injections may result in lower and more variable serum concentrations, potentially impacting therapeutic efficacy.78,85 Local absorption of mAbs is further affected by precipitation and catabolism at the injection site, which can decrease the amount of active drug entering systemic circulation.85 Because of their large size, mAbs are mainly absorbed slowly through lymphatic transport, a process that can be further slowed in obesity due to changes in tissue composition.85–87
Third, obesity-related insulin resistance and metabolic syndrome may affect monoclonal antibody clearance through alterations in the recycling mechanism of neonatal Fc receptor (FcRn).88 The accumulation of immunoglobulin G (IgG) in adipose tissue observed in obese patients can potentially alter the clearance of biologics, by increasing tissue-specific IgG accumulation and competition for neonatal FcRn-mediated recycling. In obesity, IgG levels in adipose tissue are markedly elevated, up to 16-fold above plasma levels, due to enhanced FcRn-mediated uptake.88–90 This may consequently saturate FcRn, which is responsible for protecting IgG and IgG-based biologics from lysosomal degradation and prolonging their half-life.88–90 When FcRn is saturated, mAbs may undergo increased catabolism, leading to higher clearance and reduced systemic exposure. Nonetheless, robust clinical data supporting a significant role for this mechanism in asthma are currently lacking.
Despite substantial advances in elucidating the pharmacokinetics of mAbs and the factors that influence them, numerous questions remain unresolved. These include data on subcutaneous bioavailability, the precise role of FcRn receptors in mediating efficacy and the influence of molecular characteristics as well as their complex interrelationships.91 Overall, while pharmacokinetic changes, such as increased Vd and potential alterations in CL, are biologically plausible, the diminished efficacy of biologic therapies in obese patients with asthma is more likely due to alternative mechanisms rather than significant pharmacokinetic abnormalities.20,92–94
The most plausible mechanism may not be of pharmacokinetic nature. Specifically, obesity is associated not only with changes in drug absorption, distribution, and metabolism, but also with chronic low-grade inflammation and altered immune cell function, as previously discussed. Obesity can thereby potentially reduce biologic drug concentrations at target sites and modify immune responses, which may influence the pharmacodynamic rather than pharmacokinetic effects of biologic therapies.18,20,92 Elevated levels of circulating IL-6 and other adipokines, like leptin, that are associated with obesity may modulate immune responses in asthma by promoting a shift away from type 2 high (Th2/eosinophilic) inflammation toward non-type 2, T2-low, (Th1/Th17/neutrophilic) inflammatory profile, characterized by increased neutrophilic rather than eosinophilic inflammation pathways.93,95–98 This immune remodeling is characterized by increased systemic and airway neutrophilia, monocyte and macrophage activation, and Th1 polarization, which can potentially attenuate the efficacy of biologics, as most currently approved biologics target T2-high pathways (eg, IL-5, IgE). However, this represents an indirect effect, rather than a true pharmacokinetic mechanism, these biologics may be less suitable in obese asthma phenotypes, leading to reduced efficacy. Also, this heterogeneity of obese asthma with its variable expression of biomarkers such as blood eosinophils and FeNO and confounding of lung function parameters may also complicate patient selection and monitoring for biologic therapy.99,100 Traditional biomarkers used for diagnosis and treatment effect may not accurately reflect airway inflammation in obese patients. Therefore, several new biomarkers or targets are being considered in this population, like, IL-6 and IL-33.99
Evidence for Biologic Drug Efficacy in Obese Asthma Patients
While these theoretical considerations suggest multiple mechanisms by which obesity may influence biologic treatment response, their clinical relevance ultimately depends on whether such effects are observed in patient outcomes. The following section therefore examines the available clinical evidence on the efficacy per biologic. Table 1 provides a summary of these findings.
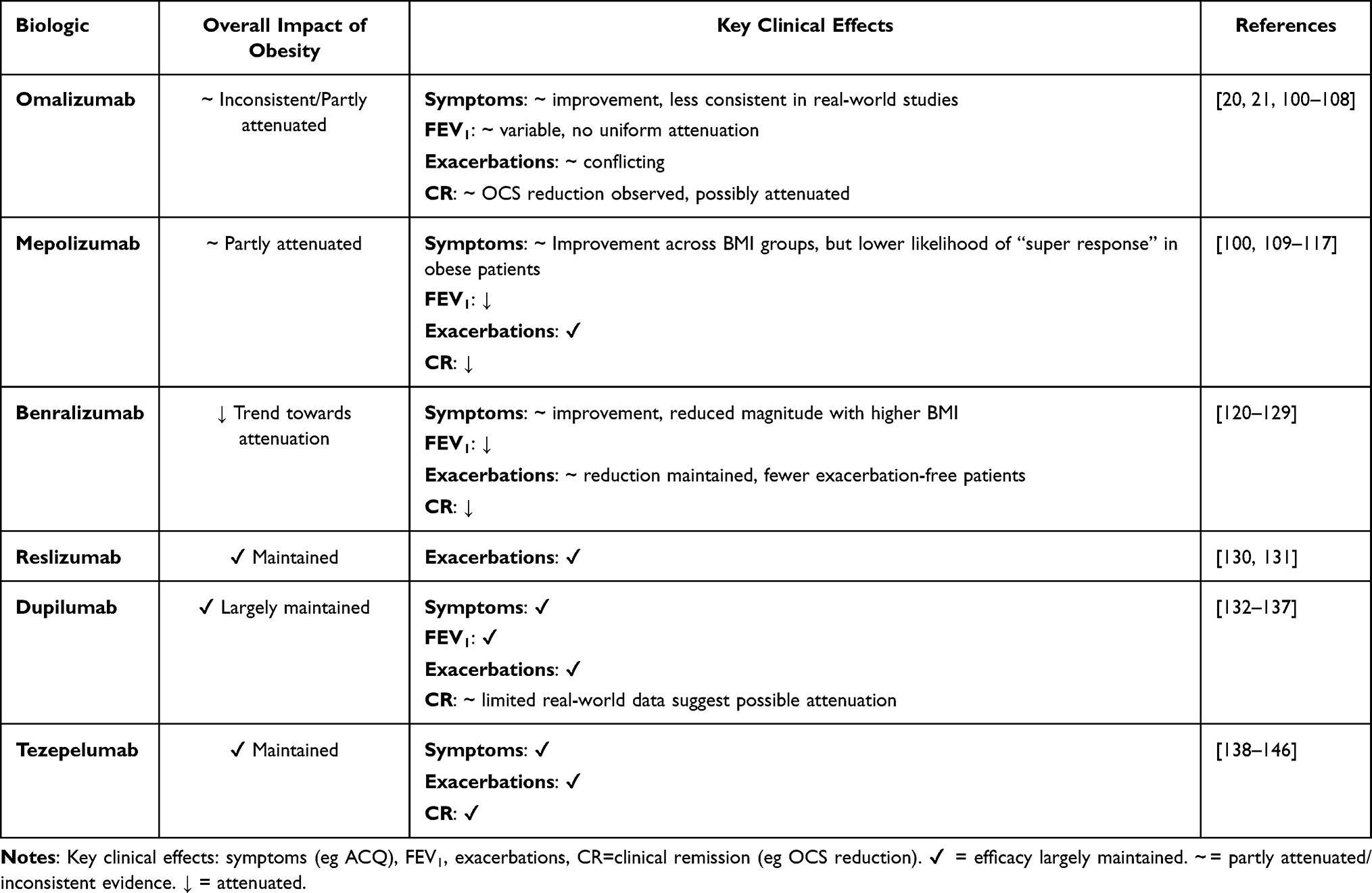 |
Table 1 Overview of the Impact of Obesity on the Efficacy of Asthma Biologics |
Omalizumab
Omalizumab was the first biologic registered for treating patients with severe asthma. It exerts its effects by targeting IgE and prohibits binding to mast cells and basophils.94 As the first asthma biologic, omalizumab has the most extensive evidence about its effects in patients with obesity-related asthma. Also, omalizumab is unique in its dosing, namely via weight-based dosing and IgE serum levels.94
Geng et al found that omalizumab improves lung function, symptom scores, reduces exacerbations, and lowers corticosteroid use in adults with moderate-to-severe allergic asthma, regardless of BMI Notably, obese patients experienced a greater placebo-adjusted reduction in exacerbation rates than normal-weight and overweight (BMI 25–30 kg/m2) groups.101 While increasing BMI showed minor, non-significant improvements in asthma symptoms and quality of life,101 these results align with Oliveira et al, who found significant benefits in lung function, fewer exacerbations, and reduced corticosteroid use with omalizumab in obese patients.102 Similarly, Özden et al reported omalizumab improved asthma control in this group.100
In contrast, some observational studies report little or no improvement in asthma control and exacerbation reduction with higher BMI, and some find no significant differences in response based on BMI.20,21,103 Also, Sposato et al found that obesity was associated with a 3x higher risk of exacerbations and a lower asthma control compared to non-obese patients after more than one year of omalizumab treatment and concluded that obesity reduced omalizumab efficacy.104 Similarly, Gibson et al, reported that obese patients were significantly less likely to be classified as responders than non-obese patients though among those who did respond, the magnitude of effect was similar between groups.105 Several other studies also reported that a higher BMI was associated with lower exacerbation reduction or less improvement in asthma control.106–108 The evidence regarding the efficacy of omalizumab in obese patients therefore is contradictory and warrants further study.
Mepolizumab
Mepolizumab, a biologic for severe eosinophilic asthma that targets IL-5, has shown heterogeneous results on efficacy in obese versus non-obese patients. Some studies find reduced effectiveness in obese individuals, while others report no significant impact of BMI on treatment response.
A meta-analysis of MENSA109 and MUSCA110 trials found that mepolizumab reduced exacerbations by 49–62% across all BMI categories compared to placebo, despite overlapping confidence intervals. Significant FEV1 improvements occurred in normal and overweight groups, but not in the obese group. Blood eosinophil reductions were slightly lower in higher BMI groups. Improvements in baseline ACQ-5 scores were consistent across BMI. Albers et al concluded that fixed-dose of 100 mg sc regimen was effective regardless of body weight or BMI.111
Several real-world observational studies have reported more pronounced BMI-related differences in treatment response. One study found that BMI ≥30 kg/m2 was associated with a poorer ACQ-5 response to mepolizumab (p=0.043) as “super-responders” (upper 25% of ACQ-5 responders) had significantly lower BMI than those in lower quartiles.112 Another study reported that super-responders had a significantly lower BMI and were significantly less likely to have a history of obesity.113 Da Cunha Fonseca et al observed no significant differences between obese and non-obese patients for most variables, except FVC% predicted, which improved more in non-obese individuals. Both groups showed notable reductions in exacerbations and better asthma control.114 Özden et al found that mepolizumab increased FEV1 more in non-obese than obese patients, although both groups showed similar gains in asthma control and fewer exacerbations.100 Regarding clinical remission, Thomas et al reported that the odds of achieving clinical remission decreased by 59% for patients with obesity.115
Some studies report no significant BMI-related differences in mepolizumab response. A meta-analysis by Gibson et al found similar exacerbation rates and ACQ-5 scores in obese and non-obese groups, though only non-obese individuals showed significant FEV1 improvement.116 Another study reported that mepolizumab reduced exacerbation rates by 47–77% across comorbidity subgroups including obesity, with comparable clinical improvements regardless of obesity status.117 Two other observational studies similarly found no difference in response to mepolizumab by BMI category.118,119 Although meta-analyses have thoroughly examined data related to mepolizumab, the impact of obesity on its efficacy remains inconclusive.
Benralizumab
Benralizumab is another biologic that targets IL-5, but in a slightly different fashion than mepolizumab and reslizumab. Benralizumab exerts its effect by binding to the alpha subunit of the IL-5 receptor, instead of targeting IL-5 as a ligand.94 The evidence regarding benralizumab efficacy in obese versus non-obese patients with severe asthma presents conflicting findings, with some studies demonstrating reduced effectiveness in patients with higher BMI while others report consistent benefits across all weight categories.
In a post-hoc pooled analysis of the SIROCCO120 and CALIMA121 trials, FitzGerald et al found that there were no significant differences in exacerbation rates or FEV1 improvements among benralizumab patients with BMI ≥35 kg/m2, compared to placebo, suggesting impaired efficacy in this severely obese subgroup.122 Similarly, Trudo et al found that benralizumab reduced asthma exacerbations and improved lung function for all BMI groups, though benefits were less marked in individuals with obesity.123
Observational studies have shown inconsistent findings on BMI’s effect on benralizumab response, but some suggest higher BMI doubles the risk of a poor outcome.124 Another study found that obesity impaired the beneficial effects of benralizumab in patients with severe eosinophilic asthma. A significantly higher proportion of non-obese patients remained completely exacerbation-free compared to those with obesity and morbid obesity, suggesting more efficacy in non-obese patients.125 Similarly, findings from the XALOC-1 real-world study showed lower BMI was associated with achieving clinical remission in patients using benralizumab.126 Also, Penz et al found that lower BMI at baseline was associated with clinical remission criteria at week 56 in the XALOC-2 prospective real-world study.127
In contrast, Menzella et al found that severe annual exacerbation rates decreased considerably across all BMI groups, though the trend suggested diminishing efficacy with increased BMI, the authors concluded that in their Italian real world setting the efficacy of benralizumab was unaffected by obesity.128 Also, Kroes et al found no statistically significant difference in BMI between responders and non-responders to benralizumab in the Dutch RAPSODI registry.129 Overall, the current evidence highlights a trend toward diminished benralizumab efficacy with increasing BMI, though the magnitude and clinical significance of this effect vary across studies. Further prospective studies are needed to fully elucidate the effect of obesity on the efficacy of benralizumab.
Reslizumab
Reslizumab is the final anti-IL-5 biologic registered for severe asthma, to be covered in this review. The evidence regarding reslizumab’s efficacy in obese patients is limited but suggests benefits across all BMI categories.
In a post-hoc analysis, Nair et al found that both BMI groups (BMI <25 and BMI ≥25) experienced similar reductions in asthma exacerbations with reslizumab, with no significant difference between groups.130 Reslizumab is unique among anti-IL-5 biologics for its weight-based dosing, which may explain its consistent efficacy across different BMI groups. One study found that weight-adjusted intravenous reslizumab was more effective than fixed-dose mepolizumab in reducing airway eosinophilia, indicating that pharmacokinetic differences related to bioavailability could drive variable responses to fixed-dose biologics in obese patients.131
Dupilumab
Dupilumab is the only biologic for severe asthma which exerts its effect by blocking the IL-4 receptor, thereby inhibiting the signaling of both IL-4 and IL-13. In contrast to the other biologics, dupilumab is also registered for a wide array of other indications like eczema, chronic obstructive pulmonary disease (COPD) and chronic rhinosinusitis with nasal polyps (CRSwNP).
The evidence regarding dupilumab efficacy in obese versus non-obese patients with severe asthma largely suggests consistent benefits across BMI categories, although some real-world data indicate potential attenuation in obese patients.
Two post-hoc analyses of the Phase 3 LIBERTY Asthma QUEST132 trial found no significant difference in dupilumab treatment response per BMI category. Busse et al reported similar decreases in annualized asthma exacerbation rates after 52 weeks across BMI groups, as well as similar improvements in FEV1.133 These findings were confirmed by the other post-hoc analyses, in which similar reductions in exacerbation rates and FEV1 improvements were shown with dupilumab across BMI categories for both the 200 mg and 300 mg dosing regimens.134,135 Consistent with these findings in severe asthma patients, another study demonstrated that the efficacy of dupilumab in patients with CRSwNP is not affected by BMI, further supporting the notion that dupilumab efficacy is maintained across different body weights.136
However, one real-world study suggests a more nuanced picture. Quarato et al followed 20 adults with severe eosinophilic asthma on dupilumab for 24 months and found that obesity was associated with significantly decreased odds of achieving clinical remission.137 Given the small sample and unadjusted results, this study should be interpreted with caution.
In summary, while randomized controlled trial data consistently demonstrate that dupilumab effectively reduces exacerbations and improves lung function regardless of BMI, some, albeit limited, real-world evidence suggests that obesity may impair the likelihood of achieving clinical remission. Further long-term studies are needed to clarify the impact of obesity on sustained dupilumab response and whether dose optimization strategies could improve outcomes in obese patients.
Tezepelumab
Approved since 2021, tezepelumab is the newest addition to the severe asthma arsenal.103 It works in a distinctly different way compared to other biologics, ie tezepelumab binds upstream of the cascade, to TSLP and thereby prevents further downstream signaling via IL-4, IL-5, IL-13 involving several other signaling pathways, that play a role in T2-high and also in T2-low asthma.103 Tezepelumab is the only biologic, to date, with shown benefit for patients with severe asthma involving T2-low pathways.103
In a post-hoc pooled analysis of the phase 2b PATHWAY138 and phase 3 NAVIGATOR trials,139 Corren et al found similar, statistically significant reductions in exacerbations and exacerbation-related hospitalizations after 52 weeks of treatment across BMI groups.140 Another post-hoc analysis of NAVIGATOR confirmed these findings, by demonstrating similar reductions in asthma exacerbations across all BMI categories.141 Two additional studies confirmed that tezepelumab was effective in lowering the annualized rate of asthma exacerbations, independent of baseline BMI.142,143
Pharmacokinetic analyses may provide mechanistic support for these clinical findings. Zheng et al demonstrated that while body weight was the most influential covariate on tezepelumab exposure, no significant differences in efficacy or safety were observed across body weight groups in patients receiving the fixed 210 mg sc dose. The authors concluded that the fixed-dose regimen is appropriate for all eligible patients regardless of body weight, as the dose appears to be on the plateau of the exposure-response curve.144
Emerging real-world data support these trial findings. Two real world studies present results in line with the above-mentioned clinical findings. One study analyzed data from 142 patients (60% obese) treated with tezepelumab, finding no significant differences in treatment responses between obese and non-obese groups. After 12 months, both groups experienced substantial reductions in exacerbation frequency, with similar rates of treatment discontinuation due to adverse effects or lack of efficacy.145 Worth mentioning, 34,5% of patients in this cohort were T2-low, a population that may be particularly enriched among obese asthmatics and for whom tezepelumab offers a unique therapeutic option.145 Finally, another study included 129 severe asthma (82 were obese) patients and showed that tezepelumab treatment, irrespective of BMI, was associated with significant reduction in exacerbation rate, improvement asthma control, and even reduction of daily dose of oral corticosteroids.146
Conclusively, tezepelumab demonstrates consistent efficacy across all BMI categories in both randomized controlled trials (RCT’s) and emerging real-world studies. This distinguishes tezepelumab from other biologics where obesity has been associated with attenuated responses and may make it a particularly appealing possibility for obese patients with severe asthma, especially those T2-low asthma, who may not qualify for or respond optimally to other biologic therapies. Tezepelumab is a relatively new biologic, further real-world evidence will emerge in the future, which will give us more evidence regarding the effects of obesity on its efficacy.
Discussion
Cross-Disease Mechanisms
Anti-Inflammatory and Metabolic Effects of Biologics
Biologics aimed at T2-high inflammation have shown effectiveness, particularly in reducing exacerbation rates among obese individuals with severe asthma. Notably, the underlying mechanisms involve processes that surpass conventional anti-inflammatory pathways. Tezepelumab is unique among asthma biologics for blocking TSLP to reduce inflammation. It shows broad efficacy in severe asthma by suppressing T2 cytokines (IL-4, IL-5, IL-13) and may affect mast cell and airway smooth muscle activation, which could benefit T2-low asthma and other inflammatory diseases. While TSLP is involved in conditions like CRSwNP, COPD, and chronic spontaneous urticaria, tezepelumab is currently approved only for asthma and CRSwNP.147 Direct metabolic effects of biologics have not yet been investigated, in contrast to indirect metabolic effects. Thus, while anti-TSLP biologics have broad anti-inflammatory effects and potential utility in other inflammatory diseases, their metabolic benefits remain currently unproven.
Reducing Corticosteroid Burden
Although biologics show no direct impact on metabolic outcomes, they may have an indirect effect.148 Corticosteroids, both oral and inhaled, are widely associated with metabolic issues such as DMII, osteoporosis, and weight gain.149 It has been shown that the use of biologics can reduce oral corticosteroid (OCS) use in asthmatic patients.150,151 Regarding ICS use, the SHAMAL study by Jackson et al demonstrated that patients with severe asthma controlled on benralizumab could achieve significant reductions in ICS therapy while maintaining asthma control:152 92% of patients successfully reduced their high-dose ICS and 91% remained exacerbation-free during tapering.152 This finding is particularly relevant for obese asthmatics, who often require higher corticosteroid doses but demonstrate reduced responsiveness.153 Although metabolic outcomes were not measured, theoretically, reduced corticosteroid use may improve metabolism and promote weight loss.
Improving Exercise Capacity
While data on exercise capacity specifically in obese asthmatics receiving biologics remain limited, preliminary evidence suggests potential benefits. A pilot study examining physical activity levels in severe asthma patients found that omalizumab and mepolizumab therapy significantly improved daily physical activity compared to conventional therapy.154 Enhanced functional capacity can be especially significant in cases of obesity-related asthma, as increased mechanical load and physical deconditioning further exacerbate respiratory constraints.
Translational Opportunities: Novel Therapeutic Approaches
Repurposing Metabolic Medication
Repurposing existing medication for new indications is not a novel phenomenon and is widely seen as a durable part of pharmaceutical innovation.155 The interplay of asthma and metabolic dysfunction has given rise to novel therapeutic possibilities.
In a large cohort study, metformin, widely used in type 2 diabetes treatment, demonstrated approximately 30% reduction in asthma attacks in patients with concurrent diabetes and asthma, with effects independent of glycemic control or weight loss.156 Also, other studies found benefits of metformin in asthmatic patients, owing its effects most probably to anti-inflammatory mechanisms, as shown in in murine models.20,156 Remarkably, the addition of GLP-1 receptor agonists (GLP-1RA) to metformin provided an additional 40% reduction in asthma attacks.156
GLP-1RA, initially registered for DMII and more recently for obesity, especially show promising results in obesity-related asthma through multiple mechanisms beyond just bodyweight reduction. Pre-clinical, clinical and observational studies demonstrate that GLP-1RAs reduce airway inflammation and hyperresponsiveness, through various metabolic and anti-inflammatory mechanisms, particularly in disease processes with metabolic dysregulation.18,157 A retrospective study in patients with DMII and asthma, GLP-1RA users experienced fewer asthma exacerbations than users of other antidiabetic medications, with differences persisting after adjusting for BMI.157 These emerging findings suggest GLP-1Ras, administered mostly via sc route but also orally, may represent a novel treatment for asthma associated with metabolic dysfunction, potentially addressing both T2-high and T2-low phenotypes.
Novel Emerging Therapeutic Targets
The convergence of asthma, obesity, and metabolic disorders creates opportunities for integrated therapeutic approaches, not only for repurposing drugs, but also for new targets.
In addition to repurposing GLP-1RAs and metformin, new therapeutic targets are emerging, such as IL-6. Drugs both new and established, like tocilizumab, are under investigation. Other targets include IL-17, IL-23, IL-1-Beta, IL-33 and its receptor, as well as TNF-alpha. Arginine metabolites, including GLP1-arginine advanced glycation end products (AGE), nitro-fatty acids and mitochondrial antioxidants are also being explored, with ongoing clinical trials focused on their potential. Several promising targets are currently under investigation and close to registration, eg itepekimab and astegolimab, both affecting IL-33.22,23,158
For T2-low asthma, which is frequently associated with obesity and metabolic syndrome, NLRP3 inflammasome inhibitors show promise. Small molecule NLRP3 inhibitors have demonstrated efficacy in reducing neutrophilic airway inflammation and airway hyperresponsiveness in preclinical models. These agents may address the steroid-resistant, neutrophilic inflammation characteristic of obesity-related asthma.18,20,22,159 Also, imatinib, a TKI, is currently under investigation in T2-low asthma patients.22
Other therapies are also under scrutiny in this population, like allergen immunotherapy, probiotics, but also bariatric surgery, which has shown to reduce asthma medication, for at least 60 months after surgery.18,160 But also emerging weight-loss drugs, similar to GLP-1RA, that work like di- or triagonists eg tirzepatide, may have huge impact on this population.18,20
Pharmacologic Drug Delivery Innovations
The choice between systemic and inhaled delivery carries important implications. While current biologics require subcutaneous or intravenous administration, which may be altered in obese patients, inhaled formulations like ecleralimab, the first inhaled anti-TSLP antibody, may offer improved tissue penetration and reduced systemic adverse events.103 Ecleralimab significantly attenuated allergen-induced bronchoconstriction and airway inflammation in mild atopic asthma. This approach offers potential advantages of direct lung targeting with reduced systemic exposure, though efficacy in obesity-related asthma requires investigation.161 Another state of the art formulation is the formulation of the drug lunsekimig, with NANOBODY technology and bispecific inhibition of TSLP and IL-13, which promises enhanced efficacy through improved tissue penetration.162
Limitations of Current Evidence
The current evidence for biologics in severe asthma patients with obesity suffers from several limitations. Most data derive from retrospective analyses or post-hoc subgroup analyses of clinical trials, with obese patients not principally considered in trial design.20,24 Real-world studies and registry data provide valuable insights but lack the rigor of prospective trials.83 Sample sizes in obesity-specific analyses remain small and heterogeneous, limiting generalizability.
Standardized metabolic endpoints are notably absent from asthma trials. Studies rarely incorporate measures of insulin resistance, adipokine profiles, or metabolic syndrome components, hampering our understanding of how metabolic dysfunction modulates biologic efficacy. Future research should elucidate cellular and metabolic functions in the obesity-asthma relationship to optimize treatment selection. Head-to-head comparisons of biologics and biomarker driven research in patients eligible for multiple agents are needed to guide personalized therapy.
Conclusion
Obesity and asthma comorbidity create a difficult-to-treat phenotype, driven by complex interactions between systemic inflammation, mechanical factors of adiposity, and metabolic dysfunction. These factors complicate disease management, with unresolved questions about disease drivers and the impact of weight loss. While losing weight can help, it is often hindered by asthma symptoms.
Biologics such as dupilumab and especially tezepelumab show potential in treating asthma in obese patients, but more studies tailored to obese patients are needed to optimise dosing and delivery. Obesity-induced changes in pharmacokinetics, pharmacodynamics and immune function may affect efficacy of biologics and require dedicated research.
Future trials should assess both respiratory and metabolic outcomes; GLP-1RA drugs illustrate this approach. This therapeutic duality hints at deeper mechanistic connections awaiting further investigation. But also emerging new targets and pharmaceutical formulations currently being investigated will hopefully be of great value in this population.
The path forward requires abandoning separate approaches that treat asthma and obesity as isolated entities. Precision medicine should guide therapy selection, integrating immunologic and metabolic profiles to tailor interventions for each patient type. Managing obesity-related asthma requires unified strategies addressing both airway and metabolic issues, improved biomarker research and personalized biologic treatments to transform this complex condition into a manageable multisystem disease.
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analysed in this study.
Author Contributions
Benjamin Hadžić: Conceptualization, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review and editing. Erwin Vasbinder: Conceptualization, Writing – review and editing. Rob Lek: Investigation, Writing – original draft. Manuel Castro Cabezas: Conceptualization, Writing – review and editing. Gert-Jan Braunstahl Conceptualization, Investigation, Supervision, Writing – original draft, Writing – review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
Erwin Vasbinder: received grants from AstraZeneca and Pfizer. Gert-Jan Braunstahl:- received grants and other payments from AstraZeneca, GSK, Novartis, Sanofi, personal fees from ALK Abello, and served as Vice-chairman NVALT asthma section, as Secretary on the ERS task force Allergy and Immunology and on the Scientific advisory board Longfords. The authors have no other conflicts of interest to declare.
References
1. Haslam D, Rigby N. A long look at obesity. Lancet. 2010;376(9735):85–20. doi:10.1016/S0140-6736(10)61065-3
2. Cserháti E. The history of bronchial asthma from the ancient times till the Middle Ages. Acta Physiol Hung. 2004;91(3–4):243–261. doi:10.1556/APhysiol.91.2004.3-4.8
3. Diamant Z, Boot JD, Virchow JC. Summing up 100 years of asthma. Respir Med. 2007;101(3):378–388. doi:10.1016/j.rmed.2006.12.004
4. Eknoyan G. A history of obesity, or how what was good became ugly and then bad. Adv Chronic Kidney Dis. 2006;13(4):421–427. doi:10.1053/j.ackd.2006.07.002
5. WHO. Obesity and overweight. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
6. Institute RK. Asthma: prevalence (from 18 years). Federal Health Reporting. 2025. Available from: https://gbe.rki.de.
7. Pate CA, Zahran HS. The Status of Asthma in the United States. Prev Chronic Dis. 2024;21:E53. doi:10.5888/pcd21.240005
8. Peters U, Dixon AE, Forno E. Obesity and asthma. J Allergy Clin Immunol. 2018;141(4):1169–1179. doi:10.1016/j.jaci.2018.02.004
9. Ford ES, Mannino DM. Time trends in obesity among adults with asthma in the United States: findings from three national surveys. J Asthma. 2005;42(2):91–95.
10. Dixon AE, Peters U. The effect of obesity on lung function. Expert Rev Respir Med. 2018;12(9):755–767. doi:10.1080/17476348.2018.1506331
11. Mohan A, Grace J, Wang BR, Lugogo N. The Effects of Obesity in Asthma. Curr Allergy Asthma Rep. 2019;19(10):49. doi:10.1007/s11882-019-0877-z
12. Sutherland ER. Linking obesity and asthma. Ann N Y Acad Sci. 2014;1311:31–41. doi:10.1111/nyas.12357
13. Luthe SK, Hirayama A, Goto T, Faridi MK, Camargo Jr CA, Hasegawa K. Association Between Obesity and Acute Severity Among Patients Hospitalized for Asthma Exacerbation. J Allergy Clin Immunol Pract. 2018;6(6):1936–1941. doi:10.1016/j.jaip.2018.02.001
14. Bal C, Pohl W, Milger K, et al. Characterization of Obesity in Severe Asthma in the German Asthma Net. J Allergy Clin Immunol Pract. 2023;11(11):3417–3424. doi:10.1016/j.jaip.2023.06.049
15. Lam BCC, Lim AYL, Chan SL, Yum MPS, Koh NSY, Finkelstein EA. The impact of obesity: a narrative review. Singapore Med J. 2023;64(3):163–171. doi:10.4103/singaporemedj.SMJ-2022-232
16. Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13(3):221–262. doi:10.1016/S2213-8587(24)00316-4
17. Sharma V, Cowan DC. Obesity, Inflammation, and Severe Asthma: an Update. Curr Allergy Asthma Rep. 2021;21(12):46. doi:10.1007/s11882-021-01024-9
18. Li W, Marx N, Yang Q, Fang D, Zhang Y. Obesity: next game changer of allergic airway diseases? Clin Transl Med. 2025;15(5):e70316. doi:10.1002/ctm2.70316
19. Mohanan S, Tapp H, McWilliams A, Dulin M. Obesity and asthma: pathophysiology and implications for diagnosis and management in primary care. Exp Biol Med (Maywood). 2014;239(11):1531–1540. doi:10.1177/1535370214525302
20. Althoff MD, Gaietto K, Holguin F, Forno E. Obesity-related Asthma: a Pathobiology-based Overview of Existing and Emerging Treatment Approaches. Am J Respir Crit Care Med. 2024;210(10):1186–1200. doi:10.1164/rccm.202406-1166SO
21. Pilkington A, Buragamadagu B, Johnston RA. Weighted Breaths: exploring Biologic and Non-Biologic Therapies for Co-Existing Asthma and Obesity. Curr Allergy Asthma Rep. 2024;24(7):381–393. doi:10.1007/s11882-024-01153-x
22. Niessen NM, Fricker M, McDonald VM, Gibson PG. T2-low: what do we know?: past, present, and future of biologic therapies in noneosinophilic asthma. Ann Allergy Asthma Immunol. 2022;129(2):150–159. doi:10.1016/j.anai.2022.04.020
23. Howell I, Howell A, Pavord ID. Type 2 inflammation and biological therapies in asthma: targeted medicine taking flight. J Exp Med. 2023;220(7):8. doi:10.1084/jem.20221212
24. Akenroye A, Keet C. Underrepresentation of blacks, smokers, and obese patients in studies of monoclonal antibodies for asthma. J Allergy Clin Immunol Pract. 2020;8(2):739–741e6. doi:10.1016/j.jaip.2019.08.023
25. Bassi M, Singh S. Impact of Obesity on Response to Biologic Therapies in Patients with Inflammatory Bowel Diseases. BioDrugs. 2022;36(2):197–203. doi:10.1007/s40259-022-00522-0
26. Ricciardolo FLM, Sprio AE, Baroso A, et al. Characterization of T2-Low and T2-High Asthma Phenotypes in Real-Life. Biomedicines. 2021;9(11):1684. doi:10.3390/biomedicines9111684
27. van Veen IH, Ten Brinke A, Sterk PJ, Rabe KF, Bel EH. Airway inflammation in obese and nonobese patients with difficult-to-treat asthma. Allergy. 2008;63(5):570–574. doi:10.1111/j.1398-9995.2007.01597.x
28. Desai D, Newby C, Symon FA, et al. Elevated sputum interleukin-5 and submucosal eosinophilia in obese individuals with severe asthma. Am J Respir Crit Care Med. 2013;188(6):657–663. doi:10.1164/rccm.201208-1470OC
29. Mahender H, Amarnath R, Vadivelu S. A comparative study evaluating C-reactive protein, sputum eosinophils and forced expiratory volume in one second in obese and nonobese asthmatics. Adv Respir Med. 2020;88(5):394–399. doi:10.5603/ARM.a2020.0155
30. Peters MC, Kerr S, Dunican EM, et al. Refractory airway type 2 inflammation in a large subgroup of asthmatic patients treated with inhaled corticosteroids. J Allergy Clin Immunol. 2019;143(1):104–113e14. doi:10.1016/j.jaci.2017.12.1009
31. Scott HA, Gibson PG, Garg ML, et al. Dietary restriction and exercise improve airway inflammation and clinical outcomes in overweight and obese asthma: a randomized trial. Clin Exp Allergy. 2013;43(1):36–49. doi:10.1111/cea.12004
32. Wood LG, Baines KJ, Fu J, Scott HA, Gibson PG. The neutrophilic inflammatory phenotype is associated with systemic inflammation in asthma. Chest. 2012;142(1):86–93. doi:10.1378/chest.11-1838
33. Rosenberg HF, Dyer KD, Foster PS. Eosinophils: changing perspectives in health and disease. Nat Rev Immunol. 2013;13(1):9–22. doi:10.1038/nri3341
34. Al Heialy S, Gaudet M, Ramakrishnan RK, et al. Contribution of IL-17 in Steroid Hyporesponsiveness in Obese Asthmatics Through Dysregulation of Glucocorticoid Receptors alpha and beta. Front Immunol. 2020;11:1724. doi:10.3389/fimmu.2020.01724
35. Kim HY, Lee HJ, Chang YJ, et al. Interleukin-17-producing innate lymphoid cells and the NLRP3 inflammasome facilitate obesity-associated airway hyperreactivity. Nat Med. 2014;20(1):54–61. doi:10.1038/nm.3423
36. Celebi Sozener Z, Cevhertas L, Satitsuksanoa P, et al. Innate lymphoid cell subsets in obese asthma patients: difference in activated cells in peripheral blood and their relationship to disease severity. Allergy. 2022;77(9):2835–2839. doi:10.1111/all.15378
37. Turk Y, Witte JA, van Huisstede A, et al. Visceral adipose tissue: a relevant inflammatory compartment in obesity-related asthma? Clin Exp Allergy. 2023;53(12):1295–1297. doi:10.1111/cea.14395
38. Periyalil HA, Wood LG, Wright TA, et al. Obese asthmatics are characterized by altered adipose tissue macrophage activation. Clin Exp Allergy. 2018;48(6):641–649. doi:10.1111/cea.13109
39. Sideleva O, Suratt BT, Black KE, et al. Obesity and asthma: an inflammatory disease of adipose tissue not the airway. Am J Respir Crit Care Med. 2012;186(7):598–605. doi:10.1164/rccm.201203-0573OC
40. Rastogi D. Pediatric obesity-related asthma: a prototype of pediatric severe non-T2 asthma. Pediatr Pulmonol. 2020;55(3):809–817. doi:10.1002/ppul.24600
41. Magzoub A, Al-Ayed M, Shaikh IA, Habeeb MS, Al-Shaibary K, Shalayel M. Leptin induces a contracting effect on Guinea pig tracheal smooth muscle via the Ob-R receptor mechanism: novel evidence. Can J Physiol Pharmacol. 2020;98(11):810–817. doi:10.1139/cjpp-2019-0605
42. Zhu XL, Qin XQ, Xiang Y, Tan YR, Qu XP, Liu HJ. Adipokine adiponectin is a potential protector to human bronchial epithelial cell for regulating proliferation, wound repair and apoptosis: comparison with leptin and resistin. Peptides. 2013;40:34–41. doi:10.1016/j.peptides.2012.11.017
43. Kleniewska P, Pawliczak R. Does Oxidative Stress Along with Dysbiosis Participate in the Pathogenesis of Asthma in the Obese? Cell Biochem Biophys. 2023;81(1):117–126. doi:10.1007/s12013-022-01114-z
44. Araki S, Dobashi K, Yamamoto Y, Asayama K, Kusuhara K. Increased plasma isoprostane is associated with visceral fat, high molecular weight adiponectin, and metabolic complications in obese children. Eur J Pediatr. 2010;169(8):965–970. doi:10.1007/s00431-010-1157-z
45. Dixon AE, Poynter ME, Garrow OJ, Kaminsky DA, Tharp WG, Bates JHT. Peripheral Airway Dysfunction in Obesity and Obese Asthma. Chest. 2023;163(4):753–762. doi:10.1016/j.chest.2022.12.030
46. Turk Y, Theel W, van Huisstede A, et al. Short-term and long-term effect of a high-intensity pulmonary rehabilitation programme in obese patients with asthma: a randomised controlled trial. Eur Respir J. 2020;56(1):7. doi:10.1183/13993003.01820-2019
47. van Huisstede A, Rudolphus A, Castro Cabezas M, et al. Effect of bariatric surgery on asthma control, lung function and bronchial and systemic inflammation in morbidly obese subjects with asthma. Thorax. 2015;70(7):659–667. doi:10.1136/thoraxjnl-2014-206712
48. van Huisstede A, Castro Cabezas M, van de Geijn GJ, et al. Underdiagnosis and overdiagnosis of asthma in the morbidly obese. Respir Med. 2013;107(9):1356–1364. doi:10.1016/j.rmed.2013.05.007
49. van der Meer AN, de Jong K, Hoekstra-Kuik A, Bel EH, Ten Brinke A. Dynamic hyperinflation impairs daily life activity in asthma. Eur Respir J. 2019;53(4):6. doi:10.1183/13993003.01500-2018
50. de Vreede CC, Witte JA, Kappen JH, Braunstahl GJ. Recovery after histamine challenge test: effect of gender and body mass index. J Appl Physiol. 2023;135(2):300–301. doi:10.1152/japplphysiol.00319.2023
51. Saydain G, Beck KC, Decker PA, Cowl CT, Scanlon PD. Clinical significance of elevated diffusing capacity. Chest. 2004;125(2):446–452. doi:10.1378/chest.125.2.446
52. Rabec C, Janssens JP, Murphy PB. Ventilation in the obese: physiological insights and management. Eur Respir Rev. 2025;34(176):5. doi:10.1183/16000617.0190-2024
53. Pankow W, Podszus T, Gutheil T, Penzel T, Peter J, Von Wichert P. Expiratory flow limitation and intrinsic positive end-expiratory pressure in obesity. J Appl Physiol. 1998;85(4):1236–1243. doi:10.1152/jappl.1998.85.4.1236
54. Rivas E, Arismendi E, Agusti A, et al. Ventilation/Perfusion distribution abnormalities in morbidly obese subjects before and after bariatric surgery. Chest. 2015;147(4):1127–1134. doi:10.1378/chest.14-1749
55. Turk Y, van Huisstede A, Franssen FME, et al. Effect of an Outpatient Pulmonary Rehabilitation Program on Exercise Tolerance and Asthma Control in Obese Asthma Patients. J Cardiopulm Rehabil Prev. 2017;37(3):214–222. doi:10.1097/HCR.0000000000000249
56. Turk Y, Theel W, Kasteleyn MJ, et al. High intensity training in obesity: a Meta-analysis. Obes Sci Pract. 2017;3(3):258–271. doi:10.1002/osp4.109
57. Yang MS, Choi S, Choi Y, Jin KN. Association Between Airway Parameters and Abdominal Fat Measured via Computed Tomography in Asthmatic Patients. Allergy Asthma Immunol Res. 2018;10(5):503–515. doi:10.4168/aair.2018.10.5.503
58. Chan R, Lipworth B. Clinical impact of obesity on oscillometry lung mechanics in adults with asthma. Ann Allergy Asthma Immunol. 2023;131(3):338–342e3. doi:10.1016/j.anai.2023.05.014
59. Genchi VA, Rossi E, Lauriola C, et al. Adipose Tissue Dysfunction and Obesity-Related Male Hypogonadism. Int J Mol Sci. 2022;23(15):8194. doi:10.3390/ijms23158194
60. Kisiel MA, Arnfelt O, Lindberg E, et al. Association between abdominal and general obesity and respiratory symptoms, asthma and COPD. Results from the RHINE study. Respir Med. 2023;211:107213. doi:10.1016/j.rmed.2023.107213
61. Orfanos S, Jude J, Deeney BT, et al. Obesity increases airway smooth muscle responses to contractile agonists. Am J Physiol Lung Cell Mol Physiol. 2018;315(5):L673–L681. doi:10.1152/ajplung.00459.2017
62. Xu S, Karmacharya N, Cao G, et al. Obesity elicits a unique metabolomic signature in human airway smooth muscle cells. Am J Physiol Lung Cell Mol Physiol. 2022;323(3):L297–L307. doi:10.1152/ajplung.00132.2022
63. Fairbank NJ, Connolly SC, Mackinnon JD, Wehry K, Deng L, Maksym GN. Airway smooth muscle cell tone amplifies contractile function in the presence of chronic cyclic strain. Am J Physiol Lung Cell Mol Physiol. 2008;295(3):L479–88. doi:10.1152/ajplung.00421.2007
64. Aaron SD, Vandemheen KL, Boulet LP, et al. Overdiagnosis of asthma in obese and nonobese adults. CMAJ. 2008;179(11):1121–1131. doi:10.1503/cmaj.081332
65. Scott S, Currie J, Albert P, Calverley P, Wilding JPH. Risk of misdiagnosis, health-related quality of life, and BMI in patients who are overweight with doctor-diagnosed asthma. Chest. 2012;141(3):616–624. doi:10.1378/chest.11-0948
66. van Schayck CP, van Der Heijden FM, van Den Boom G, Tirimanna PR, van Herwaarden CL. Underdiagnosis of asthma: is the doctor or the patient to blame? The DIMCA project. Thorax. 2000;55(7):562–565. doi:10.1136/thorax.55.7.562
67. Lavoie KL, Bacon SL, Labrecque M, Cartier A, Ditto B. Higher BMI is associated with worse asthma control and quality of life but not asthma severity. Respir Med. 2006;100(4):648–657. doi:10.1016/j.rmed.2005.08.001
68. Maalej S, Yaacoub Z, Fakhfekh R, Yaalaoui S, Kheder AB, Drira I. Association of obesity with asthma severity, control and quality of life. Tanaffos. 2012;11(1):38–43.
69. Sutherland ER, Goleva E, Strand M, Beuther DA, Leung DY. Body mass and glucocorticoid response in asthma. Am J Respir Crit Care Med. 2008;178(7):682–687. doi:10.1164/rccm.200801-076OC
70. Greiner B, Elenwo C, Hartwell M. Increased serum cotinine and obesity negatively impact asthma exacerbations and hospitalizations: a cross-sectional analysis of NHANES. J Clin Transl Sci. 2023;7(1):e10. doi:10.1017/cts.2022.509
71. Thompson CA, Eslick SR, Berthon BS, Wood LG. Asthma medication use in obese and healthy weight asthma: systematic review/meta-analysis. Eur Respir J. 2021;57(3):4. doi:10.1183/13993003.00612-2020
72. Taylor B, Mannino D, Brown C, Crocker D, Twum-Baah N, Holguin F. Body mass index and asthma severity in the National Asthma Survey. Thorax. 2008;63(1):14–20. doi:10.1136/thx.2007.082784
73. Fletcher JM, Green JC, Neidell MJ. Long term effects of childhood asthma on adult health. J Health Econ. 2010;29(3):377–387. doi:10.1016/j.jhealeco.2010.03.007
74. Halfon N, Larson K, Slusser W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad Pediatr. 2013;13(1):6–13. doi:10.1016/j.acap.2012.10.007
75. Manion AB, Velsor-Friedrich B. Quality of Life and Health Outcomes in Overweight and Non-Overweight Children With Asthma. J Pediatr Health Care. 2017;31(1):37–45. doi:10.1016/j.pedhc.2016.01.005
76. Nguyen HV, Nadkarni NV, Sankari U, Mital S, Lye WK, Tan NC. Association between asthma control and asthma cost: results from a longitudinal study in a primary care setting. Respirology. 2017;22(3):454–459. doi:10.1111/resp.12930
77. Smit C, De Hoogd S, Bruggemann RJM, Knibbe CAJ. Obesity and drug pharmacology: a review of the influence of obesity on pharmacokinetic and pharmacodynamic parameters. Expert Opin Drug Metab Toxicol. 2018;14(3):275–285. doi:10.1080/17425255.2018.1440287
78. Gouju J, Legeay S. Pharmacokinetics of obese adults: not only an increase in weight. Biomed Pharmacother. 2023;166:115281. doi:10.1016/j.biopha.2023.115281
79. Keizer RJ, Huitema AD, Schellens JH, Beijnen JH. Clinical pharmacokinetics of therapeutic monoclonal antibodies. Clin Pharmacokinet. 2010;49(8):493–507. doi:10.2165/11531280-000000000-00000
80. Hanley MJ, Abernethy DR, Greenblatt DJ. Effect of obesity on the pharmacokinetics of drugs in humans. Clin Pharmacokinet. 2010;49(2):71–87. doi:10.2165/11318100-000000000-00000
81. Milsap RL, Plaisance KI, Jusko WJ. Prednisolone disposition in obese men. Clin Pharmacol Ther. 1984;36(6):824–831. doi:10.1038/clpt.1984.263
82. To M, To Y. Corticosteroid insensitivity in obese asthma: potential mechanisms and therapeutic perspectives. Front Allergy. 2025;6:1719900. doi:10.3389/falgy.2025.1719900
83. Gonem S, Redmond C, Busby J, et al. Effects of Obesity on Response to Asthma Biologic Treatment: longitudinal Data From the United Kingdom Severe Asthma Registry. J Allergy Clin Immunol Pract. 2025;13(11):3002–3010. doi:10.1016/j.jaip.2025.07.041
84. Dirks NL, Meibohm B. Population pharmacokinetics of therapeutic monoclonal antibodies. Clin Pharmacokinet. 2010;49(10):633–659. doi:10.2165/11535960-000000000-00000
85. Erstad BL, Barletta JF. Implications of obesity for drug administration and absorption from subcutaneous and intramuscular injections: a primer. Am J Health Syst Pharm. 2022;79(15):1236–1244. doi:10.1093/ajhp/zxac058
86. de Lucio M, Leng Y, Wang H, Vlachos PP, Gomez H. Modeling drug transport and absorption in subcutaneous injection of monoclonal antibodies: impact of tissue deformation, devices, and physiology. Int J Pharm. 2024;661:124446. doi:10.1016/j.ijpharm.2024.124446
87. Richter WF, Jacobsen B. Subcutaneous absorption of biotherapeutics: knowns and unknowns. Drug Metab Dispos. 2014;42(11):1881–1889. doi:10.1124/dmd.114.059238
88. Kim S, Kim J, Lee HL, Kim MS. Temporal dynamics of IgG-mediated immunometabolic dysfunction: from acute obesity to chronic aging. Front Immunol. 2025;16:1661391. doi:10.3389/fimmu.2025.1661391
89. Yu L, Yang YX, Gong Z, et al. FcRn-dependent IgG accumulation in adipose tissue unmasks obesity pathophysiology. Cell Metab. 2025;37(3):656–672e7. doi:10.1016/j.cmet.2024.11.001
90. Bussel JB, Cines DB, Blumberg RS. Neonatal Fc Receptor - Biology and Therapeutics. N Engl J Med. 2025;392(16):1621–1635. doi:10.1056/NEJMra2312718
91. Matera MG, Calzetta L, Rogliani P, Cazzola M. Monoclonal antibodies for severe asthma: pharmacokinetic profiles. Respir Med. 2019;153:3–13. doi:10.1016/j.rmed.2019.05.005
92. Guerrero SC, Panettieri Jr RA, Rastogi D. Mechanistic Links Between Obesity and Airway Pathobiology Inform Therapies for Obesity-Related Asthma. Paediatr Drugs. 2023;25(3):283–299. doi:10.1007/s40272-022-00554-7
93. Scott HA, Ng SH, McLoughlin RF, et al. Effect of obesity on airway and systemic inflammation in adults with asthma: a systematic review and meta-analysis. Thorax. 2023;78(10):957–965. doi:10.1136/thorax-2022-219268
94. Brusselle GG, Koppelman GH. Biologic Therapies for Severe Asthma. N Engl J Med. 2022;386(2):157–171. doi:10.1056/NEJMra2032506
95. Peters MC, McGrath KW, Hawkins GA, et al. Plasma interleukin-6 concentrations, metabolic dysfunction, and asthma severity: a cross-sectional analysis of two cohorts. Lancet Respir Med. 2016;4(7):574–584. doi:10.1016/S2213-2600(16)30048-0
96. Reyes-Angel J, Kaviany P, Rastogi D, Forno E. Obesity-related asthma in children and adolescents. Lancet Child Adolesc Health. 2022;6(10):713–724. doi:10.1016/S2352-4642(22)00185-7
97. Witte A, Turk Y, Braunstahl GJ. Obesity-related asthma: new insights leading to a different approach. Curr Opin Pulm Med. 2024;30(3):294–302. doi:10.1097/MCP.0000000000001073
98. Weare-Regales N, Carr T, Holguin F, Tibbitt CA, Lockey RF. Obesity and hormonal influences on asthma: mechanisms, management challenges, and emerging therapeutic strategies. J Allergy Clin Immunol. 2024;154(6):1355–1368. doi:10.1016/j.jaci.2024.09.018
99. Grace J, Mohan A, Lugogo NL. Obesity and adult asthma: diagnostic and management challenges. Curr Opin Pulm Med. 2019;25(1):44–50. doi:10.1097/MCP.0000000000000531
100. Ozden S, Tepetam FM, Orcen C, Yakut T. The phenotypic heterogeneity of obese and nonobese patients with severe asthma and comparison of omalizumab–mepolizumab treatment efficiency in these patients. Medicine. 2023;102(43):e35247. doi:10.1097/MD.0000000000035247
101. Geng B, Dixon AE, Ko J, et al. Impact of body mass index on omalizumab response in adults with moderate-to-severe allergic asthma. Ann Allergy Asthma Immunol. 2022;128(5):553–560. doi:10.1016/j.anai.2022.01.025
102. Oliveira MJ, Vieira M, Coutinho D, et al. Severe asthma in obese patients: improvement of lung function after treatment with omalizumab. Pulmonology. 2019;25(1):15–20. doi:10.1016/j.pulmoe.2018.01.005
103. Garg D, Que LG, Ingram JL. Effects of biological therapies on patients with Type-2 high asthma and comorbid obesity. Front Pharmacol. 2024;14:1315540. doi:10.3389/fphar.2023.1315540
104. Sposato B, Scalese M, Milanese M, et al. Factors reducing omalizumab response in severe asthma. Eur J Intern Med. 2018;52:78–85. doi:10.1016/j.ejim.2018.01.026
105. Gibson PG, Reddel H, McDonald VM, et al. Effectiveness and response predictors of omalizumab in a severe allergic asthma population with a high prevalence of comorbidities: the Australian Xolair Registry. Intern Med J. 2016;46(9):1054–1062. doi:10.1111/imj.13166
106. Gu C, Upchurch K, Mamaril-Davis J, et al. Obesity influences the outcomes of anti-IgE (omalizumab) therapy of asthma. Clin Exp Allergy. 2020;50(10):1196–1199. doi:10.1111/cea.13696
107. Huang WC, Fu PK, Chan MC, et al. Predictors of a Minimal Clinically Important Difference Following Omalizumab Treatment in Adult Patients With Severe Allergic Asthma. Front Med Lausanne. 2021;8:762318. doi:10.3389/fmed.2021.762318
108. Novelli F, Latorre M, Vergura L, et al. Asthma control in severe asthmatics under treatment with omalizumab: a cross-sectional observational study in Italy. Pulm Pharmacol Ther. 2015;31:123–129. doi:10.1016/j.pupt.2014.09.007
109. Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. doi:10.1056/NEJMoa1403290
110. Chupp GL, Bradford ES, Albers FC, et al. Efficacy of mepolizumab add-on therapy on health-related quality of life and markers of asthma control in severe eosinophilic asthma (MUSCA): a randomised, double-blind, placebo-controlled, parallel-group, multicentre, phase 3b trial. Lancet Respir Med. 2017;5(5):390–400. doi:10.1016/S2213-2600(17)30125-X
111. Albers FC, Papi A, Taille C, et al. Mepolizumab reduces exacerbations in patients with severe eosinophilic asthma, irrespective of body weight/body mass index: meta-analysis of MENSA and MUSCA. Respir Res. 2019;20(1):169. doi:10.1186/s12931-019-1134-7
112. Harvey ES, Langton D, Katelaris C, et al. Mepolizumab effectiveness and identification of super-responders in severe asthma. Eur Respir J. 2020;55(5):3. doi:10.1183/13993003.02420-2019
113. Fong WCG, Azim A, Knight D, et al. Real-world Omalizumab and Mepolizumab treated difficult asthma phenotypes and their clinical outcomes. Clin Exp Allergy. 2021;51(8):1019–1032. doi:10.1111/cea.13882
114. Da Cunha Fonseca A, Machado D, Pascoal I, Franco I, Lima R. Severe asthma in obese patients: what to expect with Mepolizumab? Eur Respir J. 2022;60(suppl 66):3216. doi:10.1183/13993003.congress-2022.3216
115. Thomas D, McDonald VM, Stevens S, et al. Biologics (mepolizumab and omalizumab) induced remission in severe asthma patients. Allergy. 2024;79(2):384–392. doi:10.1111/all.15867
116. Gibson PG, Prazma CM, Chupp GL, et al. Mepolizumab improves clinical outcomes in patients with severe asthma and comorbid conditions. Respir Res. 2021;22(1):171. doi:10.1186/s12931-021-01746-4
117. Kritikos V, Harvey ES, Stevens S, et al. Comorbidities Modify the Phenotype but Not the Treatment Effectiveness to Mepolizumab in Severe Eosinophilic Asthma. J Allergy Clin Immunol Pract. 2023;11(3):885–895e13. doi:10.1016/j.jaip.2022.12.004
118. Crimi C, Campisi R, Cacopardo G, et al. Real-life effectiveness of mepolizumab in patients with severe refractory eosinophilic asthma and multiple comorbidities. World Allergy Organ J. 2020;13(9):100462. doi:10.1016/j.waojou.2020.100462
119. Casale T, Molfino NA, Silver J, et al. Real-world effectiveness of mepolizumab in patients with severe asthma and associated comorbidities. Ann Allergy Asthma Immunol. 2021;127(3):354–362e2. doi:10.1016/j.anai.2021.05.021
120. Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting beta(2)-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2115–2127. doi:10.1016/S0140-6736(16)31324-1
121. FitzGerald JM, Bleecker ER, Nair P, et al. Benralizumab, an anti-interleukin-5 receptor alpha monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2128–2141. doi:10.1016/S0140-6736(16)31322-8
122. FitzGerald JM, Bleecker ER, Menzies-Gow A, et al. Predictors of enhanced response with benralizumab for patients with severe asthma: pooled analysis of the SIROCCO and CALIMA studies. Lancet Respir Med. 2018;6(1):51–64. doi:10.1016/S2213-2600(17)30344-2
123. Trudo F, Hirsch I, Gopalan G, Martin U. Impact of Body Mass Index on Efficacy of Benralizumab in Patients with Severe, Uncontrolled Eosinophilic Asthma: pooled Analysis of the SIROCCO and CALIMA Trials. A101 MECHANISMS and CLINICAL FEATURES of SEVERE ASTHMA. 2018;2018:A2490–A2490.
124. Al-Ahmad M, Ali A, Maher A. Factors influencing poor response to type 2 targeted therapies in severe asthma: a retrospective cohort study. BMC Pulm Med. 2023;23(1):490. doi:10.1186/s12890-023-02786-w
125. Nanzer A, Burhan H, Menzies-Gow A, et al. P207 The influence of obesity on the clinical outcome of benralizumab treatment in severe eosinophilic asthma a subgroup analysis from the BPAP study. Thorax. 2022;77(Suppl 1):A192–A193. doi:10.1136/thorax-2022-BTSabstracts.341
126. Louis R, Lommatzsch M, Jackson DJ, et al. Advancing Remission in Severe Asthma With Benralizumab: latest Findings, Current Perspectives and Future Direction. Clin Exp Allergy. 2025;55(7):521–531. doi:10.1111/cea.70083
127. Penz E, Rothe T, Dupont L, et al. Early and Sustained Asthma Control and Remission in Real-World Patients With Severe Eosinophilic Asthma Treated With Benralizumab: XALOC-2. Clin Exp Allergy. 2025;2025:70162. doi:10.1111/cea.70162
128. Menzella F, Aliani M, Altieri E, et al. Real-life impact of weight in severe eosinophilic asthma patients treated with benralizumab. Eur Respir J. 2021;58(suppl 65):PA3735. doi:10.1183/13993003.congress-2021.PA3735
129. Kroes JA, de Jong K, Hashimoto S, et al. Clinical response to benralizumab can be predicted by combining clinical outcomes at 3 months with baseline characteristics. ERJ Open Res. 2023;9(2):3. doi:10.1183/23120541.00559-2022
130. Nair P, Bardin P, Humbert M, et al. Efficacy of Intravenous Reslizumab in Oral Corticosteroid-Dependent Asthma. J Allergy Clin Immunol Pract. 2020;8(2):555–564. doi:10.1016/j.jaip.2019.09.036
131. Mukherjee M, Aleman Paramo F, Kjarsgaard M, et al. Weight-adjusted Intravenous Reslizumab in Severe Asthma with Inadequate Response to Fixed-Dose Subcutaneous Mepolizumab. Am J Respir Crit Care Med. 2018;197(1):38–46. doi:10.1164/rccm.201707-1323OC
132. Busse WW, Maspero JF, Rabe KF, et al. Liberty Asthma QUEST: phase 3 Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study to Evaluate Dupilumab Efficacy/Safety in Patients with Uncontrolled, Moderate-to-Severe Asthma. Adv Ther. 2018;35(5):737–748. doi:10.1007/s12325-018-0702-4
133. Busse WW, Paggiaro P, Munoz X, et al. Impact of baseline patient characteristics on dupilumab efficacy in type 2 asthma. Eur Respir J. 2021;58(4):2. doi:10.1183/13993003.04605-2020
134. Bourdin A, Virchow JC, Papi A, et al. Dupilumab efficacy in subgroups of type 2 asthma with high-dose inhaled corticosteroids at baseline. Respir Med. 2022;202:106938. doi:10.1016/j.rmed.2022.106938
135. Korn S, Busse WW, Echave-Sustaeta JM, et al. Dupilimab Efficacy in Patients with Uncontrolled, Moderate-to-Severe Asthma by Body Mass Index. Eur Respir J. 2019;54(suppl 63):PA2753. doi:10.1183/13993003.congress-2019.PA2753
136. Seong Cho BT, Cohen N. Dupilumab improves objective, subjective, and health-related quality of life outcomes in chronic rhinosinusitis with nasal polyps (CRSwNP), regardless of BMI ≥30 kg/m2 or weight ≥90 kg: post-hoc analysis of the SINUS-24 and SINUS-52 studies. J Allergy Clin Immunol. 2022;149(2):AB143. doi:10.1016/j.jaci.2021.12.483
137. Quarato CMI, Tondo P, Lacedonia D, et al. Clinical Remission in Patients Affected by Severe Eosinophilic Asthma on Dupilumab Therapy: a Long-Term Real-Life Study. J Clin Med. 2024;13(1):291. doi:10.3390/jcm13010291
138. Corren J, Parnes JR, Wang L, et al. Tezepelumab in Adults with Uncontrolled Asthma. N Engl J Med. 2017;377(10):936–946. doi:10.1056/NEJMoa1704064
139. Menzies-Gow A, Colice G, Griffiths JM, et al. NAVIGATOR: a phase 3 multicentre, randomized, double-blind, placebo-controlled, parallel-group trial to evaluate the efficacy and safety of tezepelumab in adults and adolescents with severe, uncontrolled asthma. Respir Res. 2020;21(1):266. doi:10.1186/s12931-020-01526-6
140. Corren J, Menzies-Gow A, Chupp G, et al. Efficacy of Tezepelumab in Severe, Uncontrolled Asthma: pooled Analysis of the PATHWAY and NAVIGATOR Clinical Trials. Am J Respir Crit Care Med. 2023;208(1):13–24. doi:10.1164/rccm.202210-2005OC
141. Carr TF, Moore WC, Kraft M, et al. Efficacy of Tezepelumab in Patients with Severe, Uncontrolled Asthma Across Multiple Clinically Relevant Subgroups in the NAVIGATOR Study. Adv Ther. 2024;41(7):2978–2990. doi:10.1007/s12325-024-02889-8
142. Ambrose C, Colice G, Salapa K, Parnes J, Corren J. S138 Effect of tezepelumab on exacerbations in patients with severe, uncontrolled asthma, according to baseline body mass index: results from the Phase 2b PATHWAY study. Thorax. 2021;76(Suppl 1):A83. doi:10.1136/thorax-2020-BTSabstracts.143
143. Geoffrey Chupp NL, Michael W. Long-Term Efficacy Of Tezepelumab In Patients With Severe, Uncontrolled Asthma By Baseline Body Mass Index. Allergy and Airway. 2023;164(4):A9–A14. doi:10.1016/j.chest.2023.07.075
144. Zheng Y, Abuqayyas L, Quartino A, et al. Population Pharmacokinetic Modeling and Exposure-Efficacy and Body Weight-Response Analyses for Tezepelumab in Patients With Severe, Uncontrolled Asthma. J Clin Pharmacol. 2024;64(8):908–921. doi:10.1002/jcph.2433
145. Ajayi C, Khan S, Drew M, et al. P205 Real world outcomes of Tezepelumab in obese and non-obese severe asthmatics. Thorax. 2025;80(Suppl 2):A272–A274. doi:10.1136/thorax-2025-BTSabstracts.386
146. Aslam S, Bagheri. Real-World Study: impact Of Bmi In Tezepelumab Treated Severe Asthma Patients. Chest J. 2025;168(4):A5454–A5456. doi:10.1016/j.chest.2025.07.3054
147. Bagnasco D, De Ferrari L, Bondi B, et al. Thymic Stromal Lymphopoietin and Tezepelumab in Airway Diseases: from Physiological Role to Target Therapy. Int J Mol Sci. 2024;25(11):5972. doi:10.3390/ijms25115972
148. Matera MG, Page C, Calzetta L, Rogliani P, Cazzola M. Pharmacological interactions between asthma and T2DM therapies: clinical and metabolic implications. Expert Opin Drug Metab Toxicol. 2026;1–15. doi:10.1080/17425255.2026.2632668
149. von Bulow A, Hansen S, Sandin P, et al. Use of High-Dose Inhaled Corticosteroids and Risk of Corticosteroid-Related Adverse Events in Asthma Findings From the NORDSTAR Cohort. J Allergy Clin Immunol Pract. 2025;13(7):1609–1619e5. doi:10.1016/j.jaip.2025.01.023
150. Bel EH, Wenzel SE, Thompson PJ, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014;371(13):1189–1197. doi:10.1056/NEJMoa1403291
151. Nair P, Wenzel S, Rabe KF, et al. Oral Glucocorticoid-Sparing Effect of Benralizumab in Severe Asthma. N Engl J Med. 2017;376(25):2448–2458. doi:10.1056/NEJMoa1703501
152. Jackson DJ, Heaney LG, Humbert M, et al. Reduction of daily maintenance inhaled corticosteroids in patients with severe eosinophilic asthma treated with benralizumab (SHAMAL): a randomised, multicentre, open-label, Phase 4 study. Lancet. 2024;403(10423):271–281. doi:10.1016/S0140-6736(23)02284-5
153. Hudler AC, Diaz IRR, Sharma S, Holguin F. Gaps and Future Directions in Clinical Research on Obesity-Related Asthma. Pulm Ther. 2023;9(3):309–327. doi:10.1007/s41030-023-00230-2
154. Carpagnano GE, Sessa F, Scioscia G, et al. Physical Activity as a New Tool to Evaluate the Response to Omalizumab and Mepolizumab in Severe Asthmatic Patients: a Pilot Study. Front Pharmacol. 2019;10:1630. doi:10.3389/fphar.2019.01630
155. Akodad S, Niu X, Secades B, Stevens H. Impact of drug repurposing between 1985 and 2024 on pharmaceutical innovation. Commun Med. 2026;2026:1. doi:10.1038/s43856-025-01344-1
156. Lee B, Man KKC, Wong E, et al. Antidiabetic Medication and Asthma Attacks. JAMA Intern Med. 2025;185(1):16–25. doi:10.1001/jamainternmed.2024.5982
157. Foer D, Beeler PE, Cui J, Karlson EW, Bates DW, Cahill KN. Asthma Exacerbations in Patients with Type 2 Diabetes and Asthma on Glucagon-like Peptide-1 Receptor Agonists. Am J Respir Crit Care Med. 2021;203(7):831–840. doi:10.1164/rccm.202004-0993OC
158. Gomez DR, Swartzman I, Linderholm A, et al. State of the Art Review: glucagon-Like Peptide-1 in Obesity-Related Asthma. Lung. 2025;203(1):108. doi:10.1007/s00408-025-00861-z
159. Włodarczyk S, Matshaba. Mechanisms behind corticosteroid resistance in obesity-induced airway inflammation – a review. J Med Sci. 2024;93(3):e1034. doi:10.20883/medical.e1034
160. Smith BM, Fitzsimmons AJ, Kovacs AJ, Grover BT, Pfeiffer JD. Impact of Bariatric Surgery on Asthma Severity and Medication Use. Obes Surg. 2024;34(8):2814–2819. doi:10.1007/s11695-024-07074-y
161. Gauvreau GM, Hohlfeld JM, FitzGerald JM, et al. Inhaled anti-TSLP antibody fragment, ecleralimab, blocks responses to allergen in mild asthma. Eur Respir J. 2023;61(3):1. doi:10.1183/13993003.01193-2022
162. Deiteren A, Bontinck L, Conickx G, et al. A first-in-human, single and multiple dose study of lunsekimig, a novel anti-TSLP/anti-IL-13 NANOBODY(R) compound, in healthy volunteers. Clin Transl Sci. 2024;17(6):e13864. doi:10.1111/cts.13864
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.