Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
The Impact of Information and Communication Technology on Doctors’ and Registered Nurses’ Working Conditions and Clinical Work – A Cross-Sectional Study in a Norwegian Hospital
Authors Kirchhoff JW ![]() , Marks A, Helgesen AK
, Marks A, Helgesen AK ![]() , Andersen KL, Andreassen HM, Grøndahl VA
, Andersen KL, Andreassen HM, Grøndahl VA ![]()
Received 2 July 2021
Accepted for publication 28 September 2021
Published 21 October 2021 Volume 2021:14 Pages 2941—2949
DOI https://doi.org/10.2147/JMDH.S327669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jörg W Kirchhoff,1 Abigail Marks,2 Ann Karin Helgesen,1 Kirsti Lauvli Andersen,1 Hilde Marie Andreassen,1 Vigdis Abrahamsen Grøndahl1
1Faculty of Health, Welfare and Organisation, Østfold University College, Halden, Norway; 2Author Affiliations Newcastle University Business School, Newcastle University, Newcastle Upon Tyne, UK
Correspondence: Jörg W Kirchhoff
Faculty of Health, Welfare and Organisation, Østfold University College, Halden, Norway
Tel +47 47 69 60 86 99
Email [email protected]
Purpose: Previous studies indicate that the introduction of information and communication technology (ICT) in health care organizations impairs health care professional’s working conditions and diminishes job discretion. Most of these studies, however, were designed to explore the influence of ICT exclusively on a single group of health care professionals and thereby did not consider the influence of the same technology on other groups of health care professionals. The aim of this article is to explore the influence of a fully integrated ICT system on both doctors and registered nurses within the same working environment: a high-tech hospital.
Methods: This is a cross-sectional study conducted in a high-tech Norwegian hospital. Data were collected in 2016. In total, 264 registered nurses and 172 doctors responded to a questionnaire on their working conditions and experiences with ICT in clinical work. Descriptive statistics, compare means, cross-tables, Chi-square and bivariate correlation analysis were used to analyze the data. Statistical significance was set at p < 0.05.
Results: The findings revealed differences in doctors’ and registered nurses’ working conditions. Registered nurses reported a statistically significant higher workload and better job content than doctors. There was no difference in job discretion between doctors and registered nurses. Both occupational groups experienced that the ICT system impairs patient contact and the quality of health services. We found statistically significant correlations between registered nurses’ and doctors’ experiences with ICT in clinical work and working conditions, whereof the strongest correlation was related to job discretion in clinical work.
Conclusion: This study concludes that the impact of ICT on doctors’ and registered nurses’ working conditions in a hospital depends on the experiences of ICT in clinical work. In consequence, it is recommended to involve doctors and registered nurses in the implementation of ICT in hospitals.
Keywords: health care professionals, information and communication technology, job discretion, job content, working conditions
Introduction
Initially introduced to support administrative functions, information and communication technology (ICT) is increasingly adopted to support clinical activities in health care organizations. In particular, ICT is implemented for the purpose of electronic medical records (EMR), which integrate information from the pharmacy, radiology and laboratory, thereby providing access to information that presents a comprehensive picture of a patient’s health, treatment and background.1 ICT has thus become increasingly integral to many work processes within health care organizations and is found to improve health care services, reduce the use of antibiotics and make work easier.2–4
Nevertheless, despite of the beneficial outcomes related to ICT and health care services for patients,5 the extensive integration of ICT within healthcare has also impaired health care professionals’ working conditions, especially for doctors and registered nurses. Petrakaki and Kornelakis6 for example, find that the introduction of an EMR system increased the standardization of work tasks executed by doctors and registered nurses, thereby delimiting health care professionals’ job discretion. Existing research regarding the influence of ICT on doctors and registered nurses working conditions indicates that the existence of ICT in day-to-day work frequently restricts health care professionals’ autonomy,6–8 increases their workload,9,10 facilitates surveillance11 and negatively impacts their relationships with other professional groups and patients.12–14
Expert knowledge held by occupational groups, however, may moderate the negative impact of ICT on health care professionals’ working conditions. Based on expert knowledge, professionals obtain a legal status from society that provides jurisdiction and the privilege of job discretion and self-governance within their field of expertise.15,16 Self-governance then provides the ability for professionals to not only regulate their own work but also develop their own training programs, which are subject to collegial control and an opportunity to control occupational groups when entering their field of expertise.15,17,18 Differences in expert knowledge and discretionary power therefore place doctors at the top of a professional hierarchy when compared to other medically-based health care occupations.19,20 Spyridonidis and Calnan21 found that medical expertise enables doctors to resist standards in ICT, whereas registered nurses find themselves controlled by standards based on medical algorithms that were integrated in ICT.22
In sum, the literature indicates disparate outcomes of ICT on doctors' and registered nurses' working conditions. Most of these studies, however, were designed to explore exclusively the influence of ICT on a single group of health care professionals and did not consider the influence of the same technology on both groups simultaneously. The aim of this study is thus to further the knowledge regarding the influence of ICT on doctors' and registered nurses' working conditions by exploring the impact of a fully integrated EMR system on both groups of health care professionals in a Norwegian hospital. Furthermore, we survey doctors’ and registered nurses’ experiences of ICT in clinical work and the interrelationship between their experience and working conditions.
Materials and Methods
Design
The data presented are based on a cross-sectional study in a high-tech hospital that explores and compares the influence of a complete and integrated ICT system on doctors’ and nurses’ working conditions.
Setting
The study was carried out in a hospital categorized as a medium to large hospital by Norwegian standards that provides specialized health care services to approximately 290,000 people. Due to a relocation to a new building, the hospital implemented a fully integrated electronic patient record (EPR) system. The EPR system is the prominent eHealth system in Norway, introduced in most hospitals across Norway and has more than 80,000 daily users, connecting both doctors and registered nurses to the same ICT system in hospitals. The new system involves the complete assimilation of patient health information into electronic medical records, the introduction of a computerized provider’s order entry system and electronic requests for the examination and treatment of patients. Consequently, all health care professionals involved in the provision of health care services to patients at the hospital can register and access all information about patients within the hospital’s ICT system.
Furthermore, electronic whiteboards displaying information from the ICT system regarding inpatients’ clinical status and treatment are utilized to ensure coordination and assist in the logistics of inpatients. The ICT system also includes an arrangement for message alerts using smart phones. This is for the purpose of facilitating easy and fast communication across health care professionals and clinical units. Using mobile solutions, such as tablets and smart phones, allows health professionals to have access to real time information.
All doctors and registered nurses were engaged in the provision of specialized health care services to patients and highly dependent on the ICT system in their day-to day work, although in different ways. Due to the authority given by the Health Personnel Act in Norway, doctors are accountable for all medical decisions, eg, the diagnosis and treatment of patients. Hence, doctors depend highly on the information about patients’ clinical status and outcomes of treatment provided by the ICT system, resulting in an ICT system that favors medical information about patients’ lab results, medication, clinical data and the like. Registered nurses, who are foremost responsible for supporting doctors in their work, are accordingly appointed to obtain and register information about patients’ clinical status and outcomes of treatment in the ICT system. Additionally, registered nurses are also responsible for hospital patients’ nursing care. The enhanced implementation of ICT thereby comprises an extensive reorganization of health care professionals’ work within the hospital.
Participants and Procedure
All doctors and registered nurses, engaged in the provision of health care services to patients at the somatic wards of the hospital were invited to participate in a survey by responding to a questionnaire. The questionnaire was distributed via their work email over a period of two weeks in the autumn of 2016, one year after the relocation and introduction of a fully integrated ICT system. The response rate among registered nurses was 45% (n=264), and among the doctors it was 56% (n=172).
Data Collection – The Questionnaire
The questionnaire included questions regarding the health care professionals’ background, working conditions, and how they experienced the use of ICT at work. Questions on health care professionals’ working conditions were presented as statements and adopted from a questionnaire developed by Statistics Norway, as well as based on the job demand - job decision model from Karasek.23 The questionnaire included statements related to job discretion (“I decide how to execute my job” and “I decide whether the quality of my work is sufficient”); workload (“I have found my job increasingly stressful in recent years” and “I have the opportunity to take a break when I need it”); and job content (“My job provides me an opportunity for professional development” and “I feel that I get to use my professional competence to the fullest”). Doctors and registered nurses also responded to a specific question on the influence of ICT with respect to job discretion (“I find that ICT solutions inhibit the exercise of my clinical judgment in patient care”).
In addition, we explored the health care professionals’ experiences in utilizing ICT when providing health care services to patients by asking them to respond to the following statements: “I experience that new ICT solutions free up more time for patient contact” and “I experience that the quality of health care services is positively affected with new ICT solutions”. Both statements were used to compute an index-variable (alpha 0.81), ie “Experience with ICT in clinical work”. All questions were measured by utilizing a five‐point Likert scale ranging from “totally disagree” (1) to “totally agree” (5).
Statistical Analyses
The data was analyzed using IBM SPSS Statistics v27. Descriptive statistics were generated to ascertain the socio-demographic characteristics of the health care professionals, their working conditions and their experience of ICT at work. Compare Means were utilized in the analysis of doctors’ and registered nurses’ working conditions and how they experienced the use of ICT at work. Cross-tables, Chi-square and bivariate correlation analysis were used to explore any interrelationships between the socio-demographic characteristics of doctors and registered nurses, their working conditions, and experience with ICT in clinical work. Kendall’s tau was used to measure the association between the variables in bivariate correlation.24 Statistical significance was set at p < 0.05.
Results
Table 1 displays the socio-demographic characteristics of the doctors and registered nurses in the study and reveals that the statistics (Chi-square test) on registered nurses differ significantly from doctors with respect to gender (p < 0.001), age (p < 0.001), percentage of full-time employment (p < 0.001) and years of employment at the hospital (p < 0.022). Registered nurses, in this study, were predominantly women (90%), 18 to 44 years old (74%) and part-time employed (60%) at the hospital. Hence, differences in socio-demographic characteristics were taken into account in our analysis.
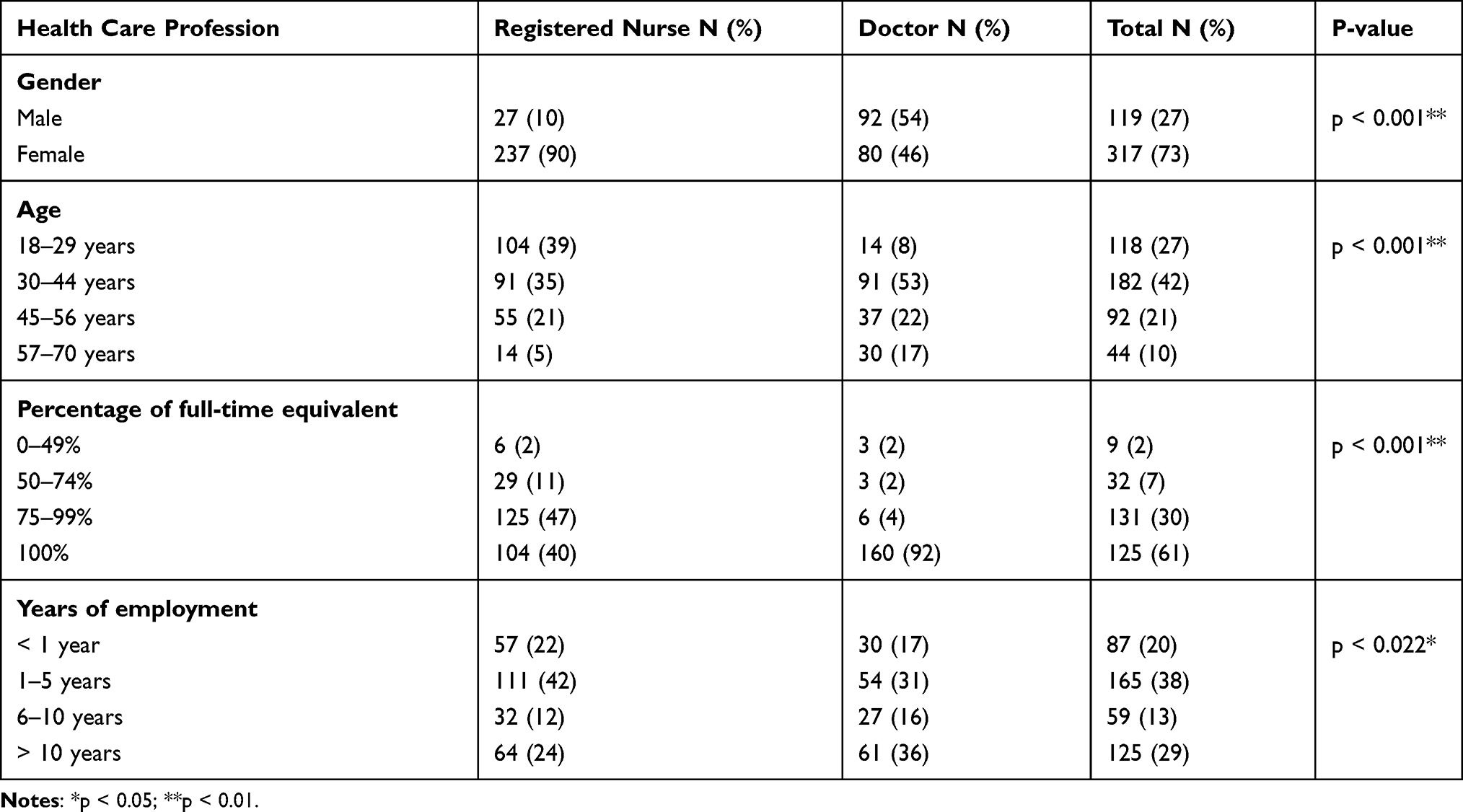 |
Table 1 Descriptive Statistics. Doctors (N=172) and Registered Nurses (N=264) |
In Table 2, mean, standard deviation and P-values for the Chi-square tests in doctors’ and registered nurses’ responses regarding how they experience their working conditions and the use of ICT in the provision of health care services are shown. In the examination of correlations between doctors’ and registered nurses’ socio-demographic characteristics and the findings presented in Table 2, we find no statistically significant interrelationships for doctors.
 |
Table 2 Doctors’ (N=172) and Registered Nurses’ (N=264) Working Conditions and Experience with ICT in Clinical Work a |
However, differences in registered nurses’ socio-demographic characteristics correlate significantly with their working conditions and experiences with ICT in clinical work. Registered nurses who have been employed at the hospital for more than six years report less job discretion (p < 0.031), find their job increasingly more stressful (p < 0.009) and were less likely to agree that their job gave them an opportunity for professional development (p < 0.001). In relation to their experience with ICT in clinical work, registered nurses with more than six years of employment at the hospital are more likely than their colleagues to disagree that ICT frees up time for patients (p < 0.046).
Table 2 displays no statistically significant differences in doctors’ and registered nurses’ perception of job discretion. Nevertheless, both doctors and registered nurses slightly agree on that ICT inhibits their job discretion, and registered nurses agree significantly more than doctors that job discretion is inhibited by ICT in clinical work (p < 0.048). Furthermore, Table 2 displays statistically significant differences between doctors and registered nurses with respect to workload, job content and experience with ICT in clinical work. Registered nurses disagree significantly more than doctors about needing the opportunity to take a break (p < 0.001) and agree significant more about having a job with an opportunity to develop professionally (p < 0.002) and exercise professional competence (p < 0.001). In addition, Table 2 displays that doctors and registered nurses experienced a negative impact of ICT on clinical work (mean < 3), and that registered nurses disagree significantly less than doctors that ICT positively affects the quality of health care services (p < 0.045).
Table 3 shows the correlation coefficient (Kendall’s tau) between doctors’ and registered nurses’ experience with ICT in clinical work and various aspects of their working conditions.
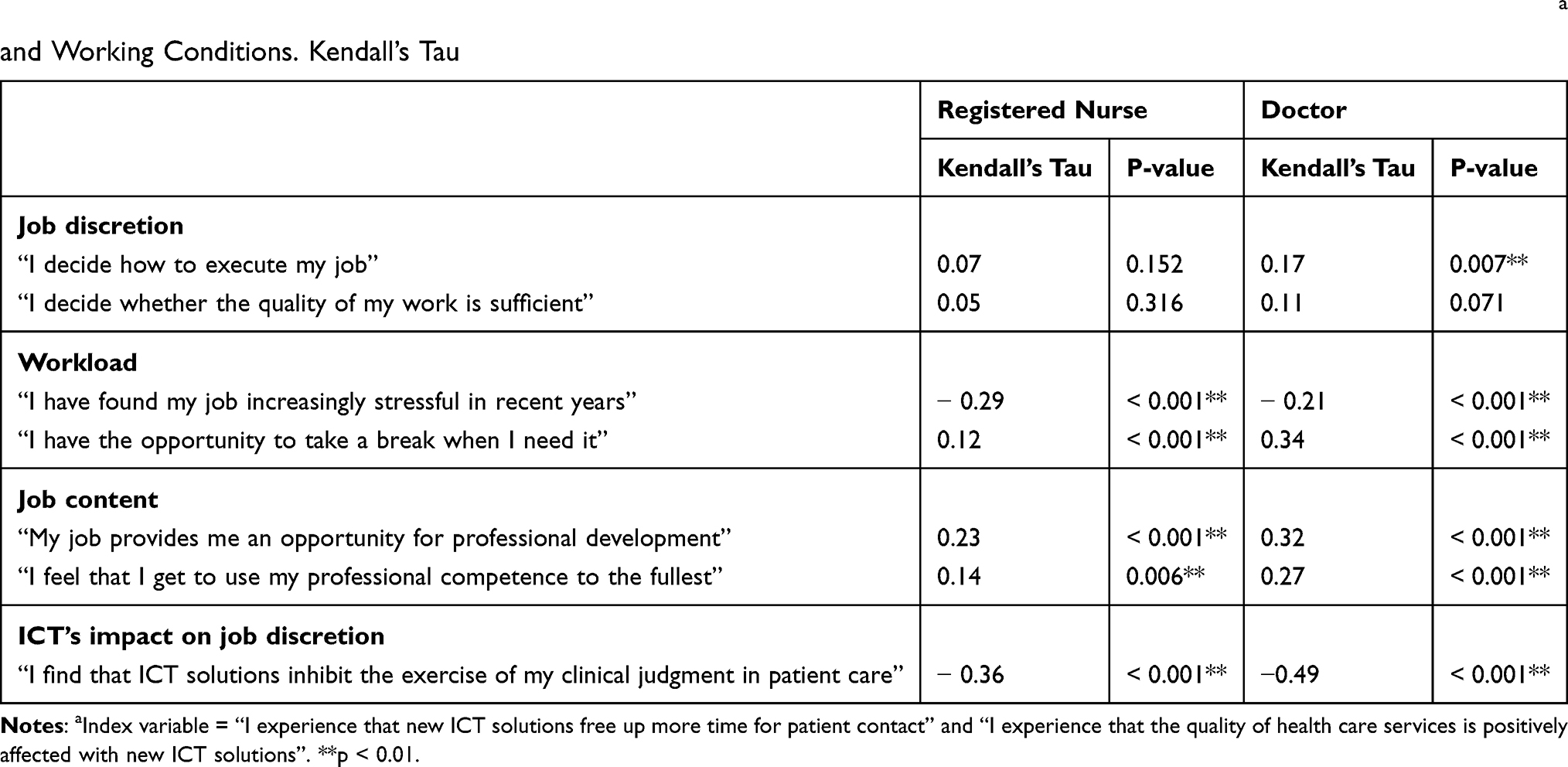 |
Table 3 Bivariate Correlation Between Registered Nurses’ (N=264) and Doctors’ (N=172) “Experience with ICT in Clinical Work” a and Working Conditions. Kendall’s Tau |
Apart from the two statements related to job discretion, Table 3 displays statistically significant correlations between registered nurses’ experience with ICT in clinical work and workload (p < 0.001), opportunities to develop professionally (p < 0.001) and exercise professional competence (p < 0.006), and ICT’s impact on job discretion (p < 0.001). There is a medium strong negative correlation between registered nurses’ experience with ICT and ICT’s impact on job discretion (Kendall’s tau – 0.36). Nevertheless, most of the correlation coefficients between registered nurses’ experience with ICT and working conditions are poor (Kendall’s tau < 0.3). In contrast to registered nurses, the associations between doctor’s experience with ICT in clinical work and working conditions appear to be stronger, and there is a statistically significant negative yet strong correlation with ICT’s impact on doctors’ job discretion in clinical work (Kendall’s tau - 0.49).
Discussion
The findings presented illustrate differences in the working conditions among doctors and registered nurses in a hospital with a fully integrated ICT system. Registered nurses in our study, for example, perceived a higher workload and simultaneously found that their job facilitated professional development, whereas doctors perceived a better opportunity to take breaks, but to a lesser degree identified job content that supported professional development. Nevertheless, despite identifying statistically significant differences in doctors’ and registered nurses’ working conditions, the extent of the differences between these two groups of health care professionals is relatively small.17 These findings are in accordance with work life reports carried out by Statistics Norway displaying that there are relatively minor differences in working conditions in Norway among employees with higher education, and this coincides with Fagerstrom, Tuvesson,13 indicating that the utilization of ICT in a Nordic context differs from other countries where the introduction of ICT impairs registered nurses’ working conditions to a high degree.6,10,11
In addition, we found that doctors and registered nurses have predominantly negative experiences with ICT in clinical work. They experienced that ICT neither freed up more time for patient contact nor enhanced the quality of health care services for patients, and actually inhibited health care professionals’ job discretion. The latter coincides with other research, highlighting the impact of an increased utilization of ICT on health care professionals’ job discretion in clinical work.21,25,26 Furthermore, the strong associations between doctors’ and registered nurses’ experience with ICT in clinical work and the impact of ICT on job discretion, presented in Table 3, indicate no negative attitude toward ICT in general, but rather question the importance of whether ICT is supportive. These findings confirm that both doctors’ and registered nurses’ assessment of the integration of ICT in health care organizations is based on the relevance of the information provided by ICT systems and the number of work tasks related to the maintenance of the ICT system.27–30 In our study, obstructing health care professionals in clinical work by preventing them from having patient contact is found to be most important in their perception of ICT in the hospital. This is in contrast to previous findings, where no significant change in time spent on patients is found.31 Therefore, although it provides relevant and important information to support health care professionals in clinical work,13 attention needs to be given to changes in workload when utilizing ICT in health care organizations to prevent health care professionals’ resistance toward ICT.6,32
Finally, we found statistically significant associations between health care professionals’ working conditions and their experience with ICT in clinical work, where these associations appear to be stronger for doctors than registered nurses. These findings confirm our discussion above, ie, that an increased utilization of ICT in health care organizations needs to fit health care professionals’ work processes and constitute working conditions that support clinical work. Morquin,32 for example, reveals that doctors’ “legitimate” resistance toward the use of ICT foremost relates to the influence of ICT solutions on medical decision-making processes and job discretion in clinical work. The relatively strong negative association between doctors’ experience with ICT in clinical work and the impact of ICT on job discretion in our study indicate a decrease in decentralized authority due to the ICT system, thereby impairing the organizational preconditions for doctors’ work.33 The literature on ICT in clinical work demonstrates that changes in job discretion predominantly relate to the standardizations of work processes.9,11,25,34 There are, however, disparate outcomes in the consequences of the standardization of work processes. On one hand, standardization is found to increase the number of routinized work tasks, organizational control of health care professionals and threaten the logic of care.11,22,35 Then again, the standardization of work also simplifies the complexity of patients’ needs, improves work routines and enhances the quality of health care services.9,36,37 Hence, the outcomes of incorporating ICT into health care organizations appear not to be related to the technology itself but to the choices and processes involved when integrating ICT into health care professionals’ clinical work.38
Methodological Considerations
The population of doctors and registered nurses in our study covers health care professionals from one case, ie, a high-tech hospital. Consequently, the findings presented are not representative for the whole population of doctors and registered nurses utilizing a fully integrated ICT system in clinical work.39 In addition, we have to consider that the questionnaire was sent to doctors and registered nurses at all wards without differentiating between them. For instance is it likely that doctors and registered nurses encounter differences in workload across hospital wards. This study thus provides foremost a general picture of the impact of the ICT system on doctors and registered nurses’ clinical work from one case. Nevertheless, completing a cross-sectional study in a case that constitutes the same environment for doctors’ and registered nurses’ clinical work provides valuable insights into how the same technology influences different groups of health care professionals.
The two groups of respondents in this study, ie doctors and registered nurses, differ significantly on all socio-demographic characteristics. In consequence, these differences were considered when analyzing interrelationships between ICT and health care professionals’ working conditions and experiences with ICT. Among registered nurses we found statistically significant correlations between some of the socio-demographic characteristics and the influence of ICT on their working conditions and experience with ICT; however, we found no correlation for doctors. Due to a relatively small number of doctors with similar characteristics as nurses, we cannot exclude that these socio-demographic characteristics are relevant for doctors’ perceptions of ICT in clinical work, and this should therefore be investigated in forthcoming studies.
In our study, we used questions developed by Statistics Norway to study doctors and registered nurses working conditions. The number of questions related to the different aspects that constitute health care professionals working conditions, however, are relatively limited. On the other hand, the questions included are used in national surveys on employees working conditions on a regular basis, and, therefore considered to be reliable. In addition, other aspects that could explain doctors' and registered nurses’ perception of the ICT system in clinical work at the hospital are not included. Previous studies have for example found that attitude toward ICT and contextual factors are important and could provide further insights when integrating ICT in clinical work.40–42
Conclusion
ICT has become increasingly integral to many work processes within health care organizations, and in this study we illuminate the influence of the same ICT system on doctors and registered nurses working conditions in a hospital. We find statistically significant yet minor differences in the working conditions among doctors and registered nurses in the hospital. In addition, both occupational groups experienced a negative impact of ICT on clinical work, including an impairment in contact with patients, the quality of health care services and job discretion in clinical work. Furthermore, we find that doctors and registered nurses experience with ICT in clinical work correlated with their working conditions, and that doctors’ experiences with ICT have a stronger effect on the working conditions than for the nurses. This study, therefore, concludes that the impact of ICT on doctors and registered nurses working conditions in a hospital depend on the experiences of ICT in clinical work.
The finding that doctors and registered nurses working conditions correlate with their experiences with ICT in clinical work indicate a possibility to prevent the negative outcomes when introducing and utilizing ICT in a hospital. For example, involving doctors and registered nurses during the implementation of an ICT system, developing an ICT system that balances work tasks related to clinical work and the maintenance of the ICT system, supports doctors and registered nurses decision-making processes and constitutes sufficient authority to sustain job discretion in clinical work, are aspects that could improve doctors and registered nurses’ experiences with ICT and reduce the negative impact of ICT on working conditions.
Ethical Considerations and Approval
The study was conducted in accordance with the principles of the Declaration of Helsinki.43 All health care professionals were given written information stating the purpose of the study and that the data would be handled confidentially. Informed consent to participate was considered given when the respondent returned a completed questionnaire. The study was approved by the Norwegian Social Science Data services (reference number 44034).
Acknowledgments
The authors are grateful to all doctors and registered nurses who participated and shared their experiences in utilizing a new ICT system in clinical work and the influence of the ICT system on their working conditions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arvanitis S, Loukis EN. Investigating the effects of ICT on innovation and performance of European hospitals: an exploratory study. Eur J Health Economics. 2016;17(4):403–418. doi:10.1007/s10198-015-0686-9
2. Ayaad O, Alloubani A, Abu Alhajaa E, et al. The role of electronic medical records in improving the quality of health care services: comparative study. Int J Med Inform. 2019;127:63–67. doi:10.1016/j.ijmedinf.2019.04.014
3. Seibert K, Domhoff D, Huter K, et al. Application of digital technologies in nursing practice: results of a mixed methods study on nurses’ experiences, needs and perspectives. Zeitschrift Fur Evidenz Fortbildung Und Qualitaet Im Gesundheitswesen. 2020;158:94–106. doi:10.1016/j.zefq.2020.10.010
4. Park YT, Kim D, Park RW, et al. Association between Full Electronic Medical Record System Adoption and Drug Use: antibiotics and Polypharmacy. Healthc Inform Res. 2020;26:68–77. doi:10.4258/hir.2020.26.1.68
5. Kearns M, Kavanagh A, Curran M, Collier D. ICT supporting clinicians and patients – the key facilitator of integrated care. Int J Integr Care. 2017;17(5):413. doi:10.5334/ijic.3732
6. Petrakaki D, Kornelakis A. ‘We can only request what’s in our protocol’: technology and work autonomy in healthcare. New Tech Work Employ. 2016;31(3):223–237. doi:10.1111/ntwe.12072
7. Hong JY, Ivory CH, VanHouten CB, et al. Disappearing expertise in clinical automation: barcode medication administration and nurse autonomy. J Am Med Informatics Assoc. 2021;28:232–238. doi:10.1093/jamia/ocaa135
8. Bansler JP. Challenges in user-driven optimization of EHR: a case study of a large Epic implementation in Denmark. Int J Med Inform. 2021;148. doi:10.1016/j.ijmedinf.2021.104394
9. Cheraghi-Sohi S, Calnan M. Discretion or discretions? Delineating professional discretion: the case of English medical practice. Soc Sci Med. 2013;96:52–59. doi:10.1016/j.socscimed.2013.07.011
10. Moore EC, Tolley CL, Bates DW, et al. A systematic review of the impact of health information technology on nurses’ time. J Am Med Informatics Assoc. 2020;27(5):798–807. doi:10.1093/jamia/ocz231
11. Timmons S. A failed panopticon: surveillance of nursing practice via new technology. New Tech Work Employ. 2003;18(2):143–153. doi:10.1111/1468-005X.00116
12. Dean S, Lewis J, Ferguson C. Editorial: is technology responsible for nurses losing touch? J Clin Nurs. 2017;26(5–6):583–585. doi:10.1111/jocn.13470
13. Fagerstrom C, Tuvesson H, Axelsson L, Nilsson L. The role of ICT in nursing practice: an integrative literature review of the Swedish context. Scand J Caring Sci. 2017;31(3):434–448. doi:10.1111/scs.12370
14. Dupret K. Working around technologies—invisible professionalism? New Tech Work Employ. 2017;32:174–187. doi:10.1111/ntwe.12093
15. Abbott A. The System of Professions: An Essay on the Division of Expert Labor. Chicago: University of Chicago Press; 1988.
16. Freidson E. Professionalism: The Third Logic. Cambridge: Polity Press; 2001.
17. McLaughlin J, Webster A. Rationalising knowledge: IT systems, professional identities and power. Sociological Rev. 1998;46(4):781–802. doi:10.1111/1467-954X.00140
18. Evetts J. Professionalism: value and ideology. Current Sociology. 2013;61(5–6):778–796. doi:10.1177/0011392113479316
19. Currie G, Croft C. Examining hybrid nurse managers as a case of identity transition in healthcare: developing a balanced research agenda. Work Employment Soc. 2015;29(5):855–865. doi:10.1177/0950017015572581
20. Molleman E, Rink F. The antecedents and consequences of a strong professional identity among medical specialists. Social Theory & Health. 2015;13(1):46–61. doi:10.1057/sth.2014.16
21. Spyridonidis D, Calnan M. Are new forms of professionalism emerging in medicine? The case of the implementation of NICE guidelines. Health Sociology Rev. 2011;20(4):394–409. doi:10.5172/hesr.2011.20.4.394
22. Russell B, Trusson C, De S. The ambiguities of ‘managed professionalism’: working in and with IT. In: Wilkinson A, Hislop D, Coupland C, editors. Perspectives on Contemporary Professional Work: Challenges and Experiences. Cheltenham, UK: Edward Elgar Publishing; 2016:361.
23. Karasek RA
24. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
25. Petrakaki D, Klecun E, Cornford T. Changes in healthcare professional work afforded by technology: the introduction of a national electronic patient record in an English hospital. Organization. 2016;23(2):206. doi:10.1177/1350508414545907
26. Kent B, Redley B, Wickramasinghe N, et al. Exploring nurses’ reactions to a novel technology to support acute health care delivery. J Clin Nurs. 2015;24(15–16):2340–2351. doi:10.1111/jocn.12881
27. Ketikidis P, Dimitrovski T, Lazuras L, Bath P. Acceptance of health information technology in health professionals: an application of the revised technology acceptance model. Health Informatics J. 2012;18(2):124–134. doi:10.1177/1460458211435425
28. Chow SK, Chin WY, Lee HY, Leung HC, Tang FH. Nurses’ perceptions and attitudes towards computerisation in a private hospital. J Clin Nurs. 2012;21(11‐12):1685–1696. doi:10.1111/j.1365-2702.2011.03905.x
29. Anthony DL, Stablein T. Privacy in practice: professional discourse about information control in health care. J Health Organ Manag. 2016;30(2):207–226. doi:10.1108/JHOM-12-2014-0220
30. Gastaldi L, Radaelli G, Lettieri E, et al. Professionals’ use of ICT in hospitals: the interplay between institutional and rational factors. Int J Tech Management. 2019;80:85–106. doi:10.1504/ijtm.2019.099768
31. Westbrook JI, Li L, Georgiou A, Paoloni R, Cullen J. Impact of an electronic medication management system on hospital doctors’ and nurses’ work: a controlled pre-post, time and motion study. J Am Med Inform Assoc. 2013;20(6):1150–1158. doi:10.1136/amiajnl-2012-001414
32. Morquin D. Legitimate resistance without technophobia: analysis of electronic medical records impacts on the medical profession. Rev Med Interne. 2020;41(9):617–621. doi:10.1016/j.revmed.2020.03.011
33. Mintzberg H, Quinn JB, Ghoshal S. The Strategy Process. London: Prentice Hall; 1995:
34. Russell B. Professional call centres, professional workers and the paradox of the algorithm: the case of telenursing. Work Employ Soc. 2012;26:195–210. doi:10.1177/0950017011433155
35. Plumb JJ, Hains I, Parr MJ, Milliss D, Herkes R, Westbrook JI. Technology meets tradition: the perceived impact of the introduction of information and communication technology on ward rounds in the intensive care unit. Int J Med Inform. 2017;105:49–58. doi:10.1016/j.ijmedinf.2017.04.004
36. Højlund H, Villadsen K. Technologies in caregiving: professionals’ strategies for engaging with new technology. New Tech Work Employ. 2020;35:178–194. doi:10.1111/ntwe.12161
37. De Meester K, Das T, Hellemans K, et al. Impact of a standardized nurse observation protocol including MEWS after Intensive Care Unit discharge. Resuscitation. 2013;84(2):184–188. doi:10.1016/j.resuscitation.2012.06.017
38. Berg M. Patient care information systems and health care work: a sociotechnical approach. Int J Med Inform. 1999;55(2):87–101. doi:10.1016/S1386-5056(99)00011-8
39. Bryman A. Social Research Methods.
40. Thapa S, Nielsen JB, Aldahmash AM, et al. Willingness to use digital health tools in patient care among health care professionals and students at a University Hospital in Saudi Arabia: quantitative cross-sectional survey. JMIR Med Educ. 2021;7:e18590–e18590. doi:10.2196/18590
41. Asemahagn MA. Health professionals’ Challenge in using ICTs to manage their Patients: the case of Hospitals in Addis Ababa, Ethiopia. Online J Nursing Informatics. 2016;20:4.
42. Parthasarathy R, Steinbach T, Knight J, et al. Framework to Enhance Nurses’ Use of EMR. Hosp Top. 2018;96:85–93. doi:10.1080/00185868.2018.1488545
43. Millum J, Wendler D, Emanuel EJ. The 50th Anniversary of the Declaration of Helsinki: progress but Many Remaining Challenges. JAMA. 2013;310(20):2143–2144. doi:10.1001/jama.2013.281632
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.