Back to Journals » Clinical Ophthalmology » Volume 14
The Impact of Image Registration for Ablation Orientation on Clinical Outcomes After Wavefront-Optimized Refractive Surgery in Eyes with Myopia and Astigmatism
Authors Brunson PB, Mann PM II, Mann PM, Potvin R ![]()
Received 7 September 2020
Accepted for publication 29 October 2020
Published 17 November 2020 Volume 2020:14 Pages 3983—3990
DOI https://doi.org/10.2147/OPTH.S280818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Phillip B Brunson,1 Paul M Mann II,1 Paul Michael Mann,1 Richard Potvin2
1Mann Eye Institute and Laser Centers, Houston, TX, USA; 2Science in Vision, Bend, OR, USA
Correspondence: Phillip B Brunson
Mann Eye Institute and Laser Centers, 5115 Main Street, Suite #300, Houston, TX 77002, USA
Email [email protected]
Purpose: To compare the clinical outcomes from laser refractive surgery performed with the same laser with and without incorporating iris registration technology to compensate for ocular cyclotorsion.
Design: Single-site, two-arm, retrospective chart review.
Methods: Clinical outcomes at a single site after wavefront-optimized LASIK using the Wavelight excimer laser with and without the Vario imaging system for iris registration (IR) were evaluated. Eligible subjects were those that received on-label wavefront-optimized treatment of myopia with astigmatism > 1.5 D. Measures of interest were the amount of residual refractive cylinder after surgery, the refractive error, and the best-corrected (BCVA) and uncorrected (UCVA) visual acuities, with a target follow-up of around 90 days.
Results: A total of 112 eligible eyes that were treated with IR and 126 similar eyes treated without IR (NO IR) were included. The refractive sphere and spherical equivalent refractions were statistically significantly different between groups (p < 0.05), but the mean differences were < 0.1 D in both cases. Refractive cylinder averaged around 0.12 D and was not statistically significantly different between groups. The number of eyes with residual cylinder > 0.50 D was higher in the NO IR group vs the IR group (6% vs 1%, respectively, p = 0.04). The mean logMAR UCVA and BCVA were statistically significantly better in the IR group, with a difference of 1.5 letters for UCVA and 1.0 letters for BCVA (p < 0.001 for both). Significantly more eyes in the IR group had a UCVA (p = 0.01) and a BCVA of 20/15 or better (p = 0.003). Overall, 96% of eyes in the IR group and 91% of eyes in the NO IR group had uncorrected visual acuity of 20/20 or better.
Conclusion: Iris registration with the VARIO imaging device demonstrably reduced the overall variability in clinical outcomes.
Keywords: LASIK, laser refractive surgery, cyclotorsion, iris registration, astigmatism, VARIO
Plain Language Summary
Laser refractive surgery is a very common procedure for people interested in reducing their need for glasses or contact lenses. Modern results are excellent, with most patients obtaining 20/20 or better vision after surgery. Refractive surgery can correct far-sightedness and near-sightedness, and can also correct astigmatism, an optical error that causes blurriness at all distances. Astigmatism results when the curvature of the front of the eye is not a sphere, but more like a football, where the curvature from end to end is not as pronounced as around the diameter. There is, therefore, an orientation (or axis) to this astigmatism.
When we lie down, our eyes rotate a bit, which means any measurement of an astigmatism axis when one is sitting up (for instance, when vision is tested) will change slightly when one lies down (for instance, when having laser refractive surgery). The difference varies between people but is usually 3–5 degrees. The current study was designed to see if “iris registration”, a method of adjusting the laser treatment to account for this rotation, could improve overall outcomes. Subjects in our study had excellent results, but the iris registration group had slightly better results, and slightly less overall variability.
Introduction
Laser vision correction (LVC) is collectively one of the most common elective eye procedures performed worldwide. It consists of three general types including photorefractive keratectomy (PRK), laser in situ keratomileusis (LASIK), and small incision lenticule extraction (SMILE). In all three procedures, proper alignment of preoperative measurements, particularly the axis of refractive astigmatism, to corneal position during surgery is needed for accurate and precise excimer ablation.1 Misalignment of the planned ablation pattern can impact postoperative visual outcomes, especially with wavefront and topography-guided procedures, or in eyes with moderate to high astigmatism.
The alignment of the ablation pattern based on preoperative refractive measurements during surgery is most affected by ocular cyclotorsion and pupil decentration. Cyclotorsion commonly occurs when patients move from an upright position (typical for preoperative measurements) to a supine position during surgery. Patient eyes can rotate by up to 14 degrees when supine during LVC, though the average is 2–3 degrees.2,3 In addition to cyclotorsion from moving to a supine position, patient eyes may also exhibit intraoperative cyclotorsion during the LVC procedure. Eye rotations of up to 13.5 degrees have been reported to occur intraoperatively.3,4 The pupil center can be in different positions under different illumination conditions, and pupil decentration has also been reported to occur intraoperatively.5
Manual compensation for corneal cyclotorsion can be performed by marking the sclera at the slit lamp while the patient is upright and overlapping those marks with the microscope reticle at the time of surgery when the patient is supine.6 This method results in good refractive outcomes, but is prone to human error due to variability in marking and the width of the actual mark. Iris registration (IR) offers the potential for much better alignment. It works by capturing an image of unique iris details and using these details for iris recognition and cyclotorsion identification while the patient is supine.7
The Wavelight® Topolyzer™ Vario imaging device (Alcon Laboratories, Inc., Fort Worth, TX) utilizes iris registration for wavefront-optimized LASIK treatments. It also allows for centration of the laser ablation at the corneal apex versus the center of the pupil. The use of the Vario device in LASIK and PRK has resulted in excellent clinical outcomes to date.7,8 However, there are currently no studies that directly compare outcomes with and without the use of Vario. The purpose of the present study was to evaluate the clinical outcomes from refractive surgery performed with the same laser with and without incorporating the Vario imaging device.
Methods
This study was a retrospective chart review, comprising a two-arm study of clinical outcomes at a single site after wavefront-optimized LASIK using the Wavelight excimer laser with and without the Vario imaging system. The study was approved by an institutional review board (Salus IRB, Austin, TX, USA) with a waiver of informed consent; the extracted chart data were de-identified. The study was conducted in compliance with International Harmonization (ICH) guidelines, Good Clinical Practice (GCP), and the tenets of the Declaration of Helsinki. There was no clinical intervention, so there was no requirement to register the study with any clinical trial registry.
Using an alpha of 0.05 and a beta (power) of 0.8, it was determined that a two-sided test of two proportions would require 99 eyes in each group to reliably confirm a presumed difference of 10% (88% vs 98%). The intent was to collect data from a minimum of 100 eyes treated using VARIO (iris registration or IR group) and 100 eyes treated without (NO IR group). The imaging in the IR group allowed for compensation of cyclotorsion and centration of the ablation pattern at the corneal apex. The NO IR group had no cyclotorsion compensation and the ablation pattern was centered on the pupil. Since this was a retrospective study, dropout was not expected.
Eligible subjects were those that received on-label wavefront-optimized treatment of myopia with astigmatism using the Wavelight Laser (Alcon Laboratories, Inc., Fort Worth, TX, USA), with or without the Vario imaging system. Subjects were excluded if they had clinically-significant ocular pathology other than residual refractive error, a history of previous refractive surgery, myopia greater than 8.00 D, cylinder that was less than 1.50 D or greater than 6.00 D, abnormal topographies, calculated residual stromal bed thickness less than 250 microns, or suboptimal surgical outcomes that were not related to the method of treatment.
The primary measure of interest was the amount of residual refractive cylinder present after surgery, reported as both a mean value and the number/percentage of eyes with postoperative refractive cylinder >0.50 D. Secondary measures included the spherical equivalent refractive error, and the best-corrected and uncorrected visual acuities (BCVA and UCVA, respectively).
Manual and electronic data records were used to identify eyes that fit the inclusion and exclusion criteria above. De-identified data from the preoperative examination and examinations in the 1-month to 6-month month postoperative period were extracted from these clinical records. The postoperative exam selected for analysis for any eye was the one closest to 90 days after surgery. Preoperative data included age, sex, and preoperative refractive error. Postoperative data included the follow-up time, the postoperative best-corrected and uncorrected distance visual acuities and the manifest refraction. Visual acuities were converted to the equivalent log of the minimum angle of resolution (logMAR) notation for statistical analysis.
Statistical analyses were performed using Statistica 12 (TIBCO Software Inc., Palo Alto, CA, USA). An analysis of variance (ANOVA) was used for parametric comparisons and the Chi-squared test was used for non-parametric comparisons. In all cases, p ≤ 0.05 was considered significant.
Results
A chart review identified 112 eyes that were treated with IR, and 126 similar eyes were identified for inclusion in the NO IR group. Table 1 shows the relevant demographics, preoperative refractive status and the time of follow-up. As can be seen, the two groups were well matched, with a statistically significant difference in only one of the variables reported. The BCVA in the NO IR group was marginally better than in the IR group, but the difference was clinically negligible (half a logMAR letter, or 1/10 of a logMAR line). Outcomes for the majority of eyes in both groups (>80%) were reported between 30 and 120 days postoperative, with data from all eyes limited to between 3 weeks and 6 months. There were no adverse events identified and no safety concerns in the data set extracted.
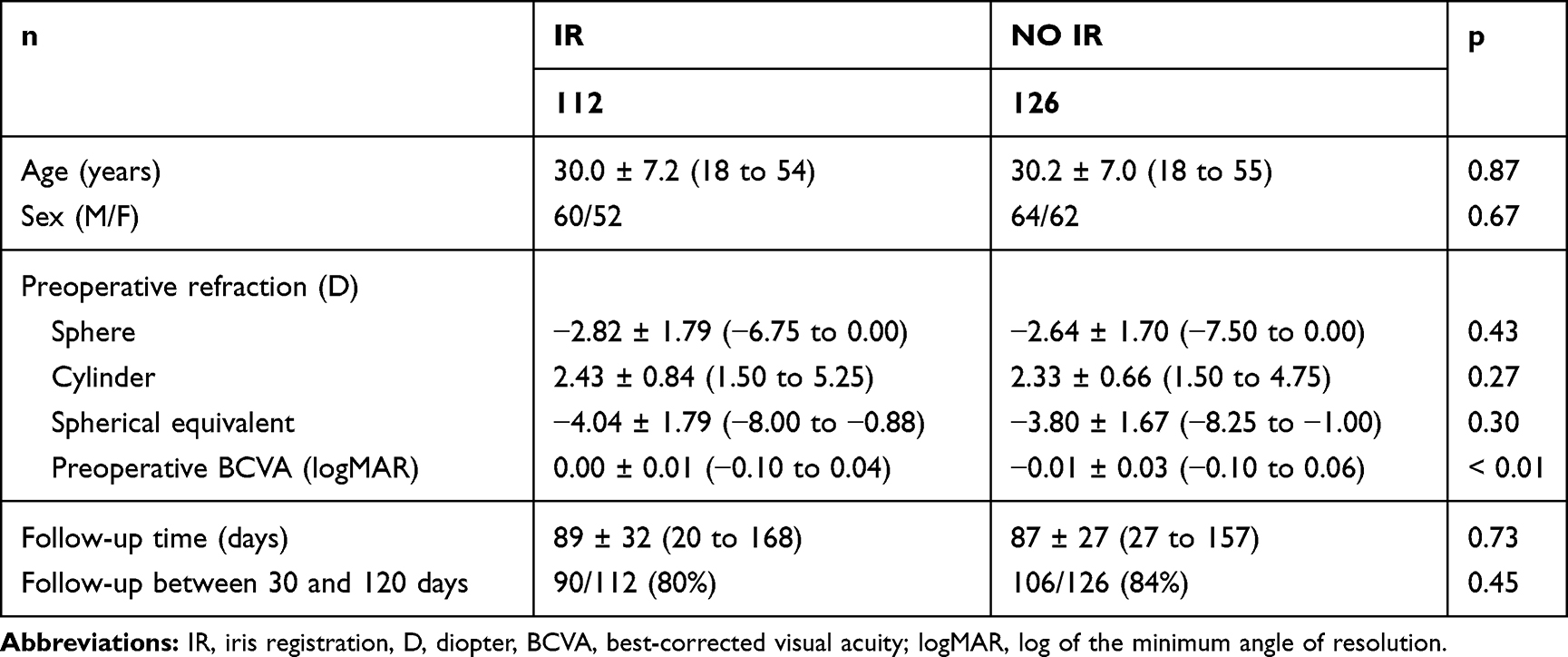 |
Table 1 Demographics, Preoperative Refractive Status and Follow-Up Time |
Table 2 contains the summary refractive and visual acuity data for the two groups. The refractive sphere and spherical equivalent refractions were statistically significantly different, but the mean differences were <0.1 D in both cases. This is likely to be clinically insignificant. Refractive cylinder was not statistically significantly different between the two groups, averaging around 0.125 D for both groups. However, Figure 1 shows the distribution of residual refractive cylinder. A chi-squared test showed that the number of eyes with a residual cylinder >0.50 D was higher in the NO IR group than in the IR group (6% vs 1%, respectively, p = 0.04). Note that 75% of eyes in the IR group and 73% of eyes in the NO IR group had no residual cylinder after surgery. Given this, a detailed vector analysis of results was not deemed necessary.
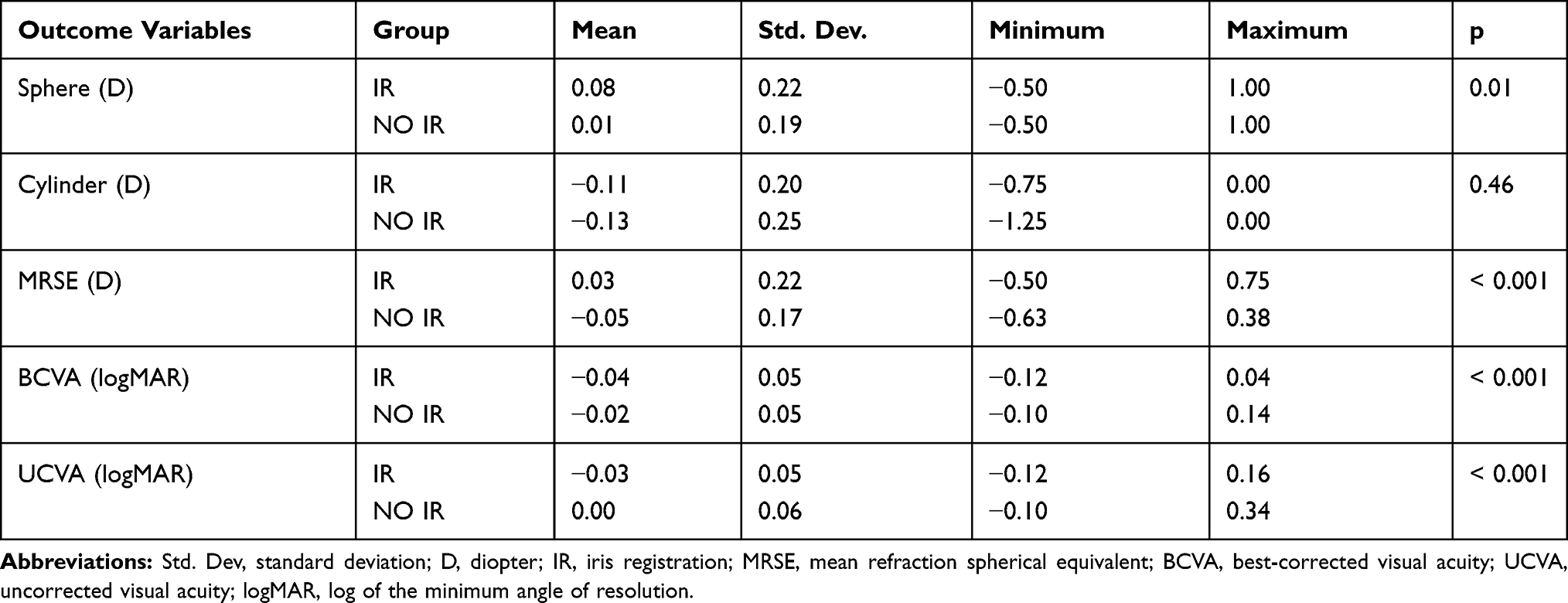 |
Table 2 Clinical Outcomes (n = 112 IR, 126 NO IR) |
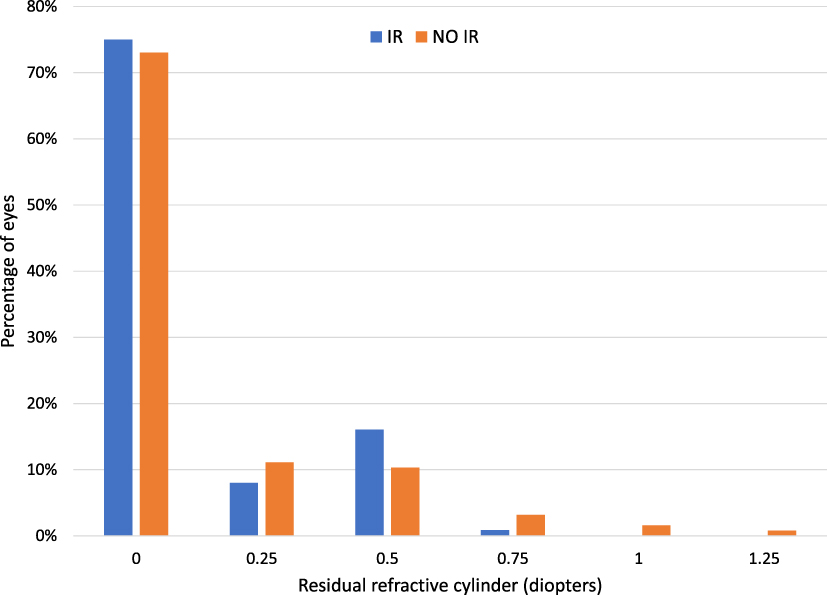 |
Figure 1 Residual refractive cylinder distribution by group. |
The mean logMAR UCVA and BCVA were statistically significantly better in the IR group, but the differences were minor (1.5 letters for UCVA, 1.0 letters for BCVA). Figures 2 and 3 show the distribution of UCVA and BCVA by group, to the nearest line of Snellen acuity. Significantly more eyes in the IR group had a UCVA of 20/15 or better (41% vs 25%, p = 0.01) and a BCVA of 20/15 or better (47% to 29%, p = 0.003). While more eyes in the NO IR group had UCVA of 20/25 or worse, the difference was not statistically significant (p = 0.07). Overall acuities were excellent, with 100% of eyes in the IR group and 97% of eyes in the NO IR group having 20/20 or better best corrected visual acuity; 96% of eyes in the IR group and 91% of eyes in the NO IR group had uncorrected visual acuity of 20/20 or better.
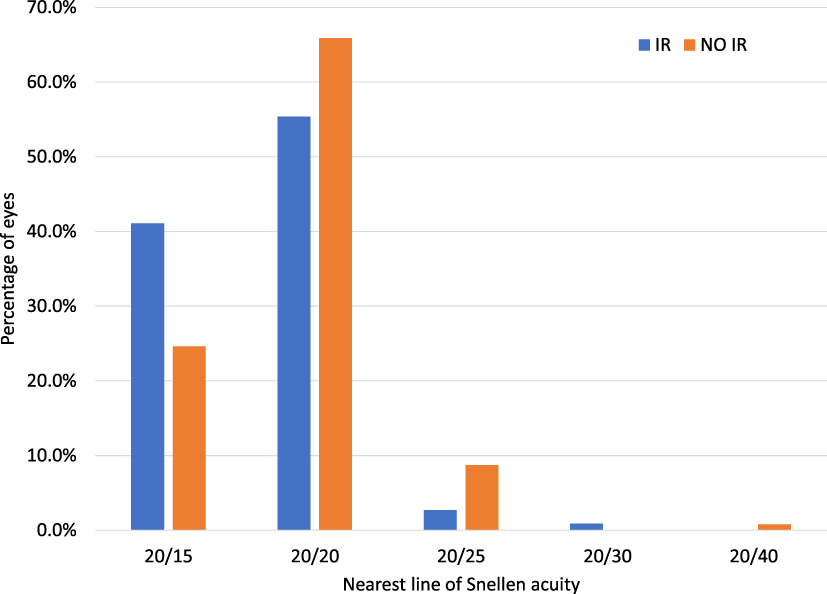 |
Figure 2 Uncorrected visual acuity by group. |
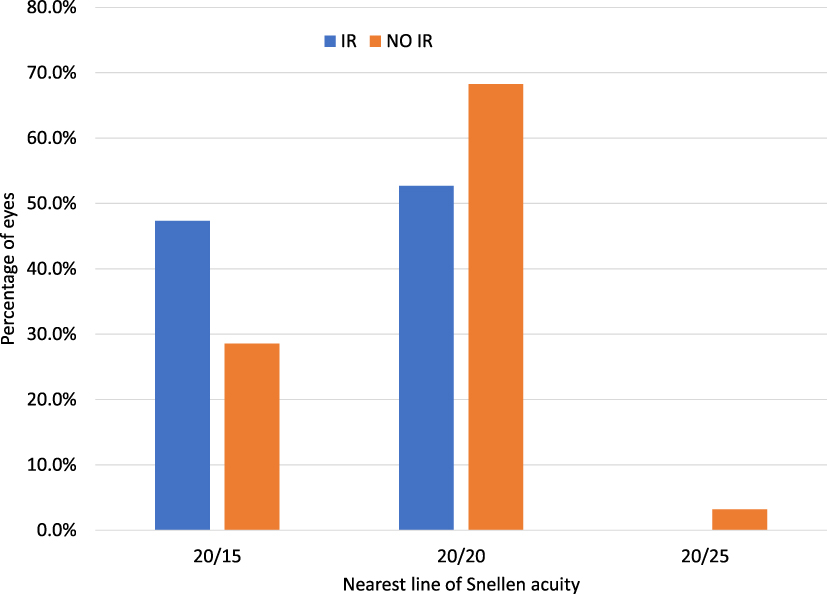 |
Figure 3 Best corrected visual acuity by group. |
Table 3 shows the difference between the preoperative BCVA and the postoperative UCVA and BCVA by group. Significantly more eyes in the IR group had a postoperative UCVA more than 1 line better than the preoperative BCVA (p < 0.002). Significantly more eyes in the NO IR group had a postoperative UCVA more than 1 line worse than the preoperative BCVA (p = 0.04). Significantly more eyes in the IR group had a BCVA increase of more than 1 line after surgery (p < 0.001). No eye in either group had a BCVA decrease of more than 1.5 lines after surgery.
 |
Table 3 Difference Between Preoperative BCVA and Postoperative UCVA and BCVA |
Discussion
To the best of our knowledge, this is the first study to directly compare clinical outcomes from refractive surgery performed with the same laser with and without the Vario imaging device. Overall, results were uniformly very good for both the IR and NO IR groups, but there is some indication that while mean results are similar, individual patient results may be incrementally better when IR is used. In particular, the IR group had a higher percentage of eyes with residual refractive cylinder ≤0.50 D and a higher percentage of eyes with both UCVA and BCVA of 20/15 or better. The IR group also had a higher number of eyes that showed a BCVA increase of more than one line. The better UCVA may be primarily a function of the slightly better correction of refractive cylinder, but that would not explain the relatively better BCVA. We speculate that it may be a function of the centration of the ablation pattern (corneal apex for IR, pupil center for NO IR), but there is no way to definitively prove this. Such an increase in BCVA has been noted in topography-guided laser refractive treatments in prior studies, though results here in both groups were slightly higher than reported in the past.9
Results evaluating the effects of iris registration with a different laser system have been variable. Khalifa et al10 investigated the effects of IR in LASIK patients using the VISX Star S4 (Johnson & Johnson Vision, Santa Ana, CA, USA). The authors reported that uncorrected visual acuity was higher in the group with IR, with 90% of patients 20/20 or better compared to 70% of patients in the non-IR group. The predictability of cylinder refraction was also higher in the group with IR, with 80% of patients having ≤0.5 D of postoperative astigmatism compare to 65% in the non-IR group. These differences are large, but the non-IR results appear significantly lower than those observed in the current study. Overall, results for both IR and NO IR appear better in the current study. Lee et al11 compared the clinical outcomes after laser epithelial keratomileusis (LASEK) using the VISX Star S4 with and without IR in a small group of patients. The authors reported no significant differences in refractive outcomes between the groups. Both groups had mean postoperative astigmatism higher than the IR and NO IR groups in this study. Uncorrected visual acuity was also better in the current study.
Arba-Mosquera and Arbelaez4 investigated the cyclotorsion compensation with the Schwind AMARIS laser system (Schwind, Kleinostheim, Germany). Postoperative astigmatism was ≤0.5 D in 88% of eyes. Again, results appear lower than observed with IR (99%) and NO IR (94%) in the current study. Pajic et al reported improvement with static and dynamic cyclotorsion tracking using the Technolas 217z100P™ laser system (Technolas, Munich, Germany), with improvements in the correction of astigmatism noted when cyclotorsion control was used.12
Wallerstein et al13 observed good visual outcomes following LASIK with the WaveLight EX500 laser and reported that postoperative astigmatism was ≤0.5 D in 93.7% of eyes. This is very similar to the NO IR results obtained in the current study, though Wallerstein was evaluating the topography-guided ablation pattern for the laser system. Faria-Correia et al7 also observed good visual outcomes with the same system, though postoperative astigmatism was ≤0.5 D in only 90% of eyes. Again, they were evaluating the topography-guided ablation pattern for the laser system. Similarly, the uncorrected and best-corrected visual acuities achieved with the wavefront-optimized ablation pattern used in the current study were similar to those obtained in the topography-guided ablation studies above.
There are limitations to the current study. It was a retrospective chart review, so there was no quality control of the postoperative evaluations. Refractive data may also not always be as carefully collected as with a prospective study, but this would be likely to be an effect seen in both groups, which means relative differences in the groups are likely to be reliable. In addition, standardized logMAR charts were not used, so testing at a 20/10 acuity level was not possible. Another limitation is that the effect of the VARIO imaging device is presumed to be primarily related to cyclotorsion control; with the available data we could not separate the possibly distinct effects of cyclotorsion control and centration; in the IR group the ablation was centered at the corneal apex, while in the NO IR group it was centered on the pupil center. Vector analysis of cylinder was also not conducted; the high percentage of eyes in both groups with no residual refractive cylinder suggested this would be of limited value. Finally, any comparisons with prior study results will be affected by differences in enrollment, refractive range, follow-up times and testing methodologies.
In summary, use of the VARIO imaging system demonstrably reduced the variability of outcomes in patients, with fewer outliers in both postoperative residual astigmatism and visual acuity results. While there were only nominal changes in the mean clinical outcome measures, the number of eyes with 20/15 or better uncorrected and best corrected visual acuity was higher in the IR group, and more eyes had a residual refractive cylinder ≤0.50 D.
Acknowledgments
Brad Hall, PhD of Sengi, aided in the preparation of this manuscript. Angelique Tarazona, BS, COMT from Mann Eye Institute and Laser Centers assisted with data extraction and data checking. This research was conducted with an investigator-initiated study grant from Alcon (IIT #51006443).
Disclosure
Dr Phillip B Brunson reports grants from Alcon, during the conduct of the study; a consultant for Novartis Pharmaceuticals, Eyevance Pharmaceuticals, and Allergan Pharmaceuticals, outside the submitted work. Dr Paul Michael Mann and Dr Paul M Mann II report grants from Alcon, during the conduct of the study. Dr Richard Potvin reports personal fees from Alcon and Carl Zeiss Meditec, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Tantayakom T, Lim JN, Purcell TL, Nalgirkar A, Cheng L, Schanzlin DJ. Visual outcomes after wavefront-guided laser in situ keratomileusis with and without iris registration. J Cataract Refract Surg. 2008;34(9):1532–1537. doi:10.1016/j.jcrs.2008.05.025
2. Chang J. Cyclotorsion during laser in situ keratomileusis. J Cataract Refract Surg. 2008;34(10):1720–1726. doi:10.1016/j.jcrs.2008.06.027
3. Febbraro J-L, Koch DD, Khan HN, Saad A, Gatinel D. Detection of static cyclotorsion and compensation for dynamic cyclotorsion in laser in situ keratomileusis. J Cataract Refract Surg. 2010;36(10):1718–1723. doi:10.1016/j.jcrs.2010.05.019
4. Arba-Mosquera S, Arbelaez M. Three-month clinical outcomes with static and dynamic cyclotorsion correction using the SCHWIND AMARIS. Cornea. 2011;30(9):951. doi:10.1097/ICO.0b013e318207eac2
5. Yang Y, Thompson K, Burns SA. Pupil location under mesopic, photopic, and pharmacologically dilated conditions. Invest Ophthalmol Vis Sci. 2002;43(7):2508–2512.
6. Shaikh NM, Manche EE. Laser in situ keratomileusis for myopia and compound myopic astigmatism using the Technolas 217 scanning-spot laser. J Cataract Refract Surg. 2002;28(3):485–490. doi:10.1016/S0886-3350(01)01287-1
7. Faria-Correia F, Ribeiro S, Monteiro T, Lopes BT, Salomao MQ, Ambrosio R. Topography-guided custom photorefractive keratectomy for myopia in primary eyes with the WaveLight EX500 platform. J Refract Surg. 2018;34(8):541–546. doi:10.3928/1081597X-20180705-03
8. Kanellopoulos AJ. Topography-guided LASIK versus small incision lenticule extraction (SMILE) for myopia and myopic astigmatism: A randomized, prospective, contralateral eye study. J Refract Surg. 2017;33(5):306–312. doi:10.3928/1081597X-20170221-01
9. Fares U, Otri AM, Al-Aqaba MA, Faraj L, Dua HS. Wavefront-optimized excimer laser in situ keratomileusis for myopia and myopic astigmatism: refractive outcomes and corneal densitometry. J Cataract Refract Surg. 2012;38(12):2131–2138.
10. Khalifa M, El-Kateb M, Shaheen MS. Iris registration in wavefront-guided LASIK to correct mixed astigmatism. J Cataract Refract Surg. 2009;35(3):433–437. doi:10.1016/j.jcrs.2008.11.039
11. Lee JJ, Kim MK, Wee WR. Effect of Iris registration on visual outcome in wavefront-guided LASEK for myopic astigmatism. Int Ophthalmol. 2018;38(2):513–525. doi:10.1007/s10792-017-0486-6
12. Pajic B, Cvejic Z, Mijatovic Z, Indjin D, Mueller J. Excimer Laser Surgery: biometrical Iris Eye Recognition with Cyclorotational Control Eye Tracker System. Sensors. 2017;17(6):1211.
13. Wallerstein A, Gauvin M, Cohen M. Effect of anterior corneal higher-order aberration ablation depth on primary topography-guided LASIK outcomes. J Refract Surg. 2019;35(12):754–762. doi:10.3928/1081597X-20191021-02
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.