Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Impact of Gut Microbiota on Chronic Obstructive Pulmonary Disease: A Dual-Sample Mendelian Randomization Study
Authors Niu N, Zhao J, Li H ![]() , Miao Y, Chen F, Liu J, Cao L
, Miao Y, Chen F, Liu J, Cao L ![]() , Ji T
, Ji T ![]() , Gao F, Xie S, Zhang Y
, Gao F, Xie S, Zhang Y
Received 11 December 2024
Accepted for publication 5 June 2025
Published 17 June 2025 Volume 2025:20 Pages 1983—1993
DOI https://doi.org/10.2147/COPD.S511383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Na Niu,1– 3,* Jian Zhao,4,* Haoxiang Li,1,3,* Yongen Miao,1,3,* Futao Chen,5 Junyong Liu,6 Limin Cao,5 Tuo Ji,7 Feng Gao,8 Shuanshuan Xie,1 Yunfeng Zhang9
1Department of Respiratory Medicine, Tenth People’s Hospital of Tongji University, Shanghai, People’s Republic of China; 2Department of Clinical Laboratory, Tenth People’s Hospital of Tongji University, Shanghai, People’s Republic of China; 3Tongji University School of Medicine, Shanghai, People’s Republic of China; 4Department of Emergency Department, Tenth People’s Hospital of Tongji University, Shanghai, People’s Republic of China; 5Department of Respiratory and Critical Care Medicine, The Second People’s Hospital of Lianyungang, Lianyungang, Jiangsu, People’s Republic of China; 6Department of Respiratory and Critical Care Medicine, Chenzhou No.1 People’s Hospital, Chenzhou, Hunan, People’s Republic of China; 7Department of Central Laboratory, The Second People’s Hospital of Lianyungang, Lianyungang, Jiangsu, People’s Republic of China; 8Department of Respiratory, Zhangjiagang Hospital Affiliated to Soochow University, Suzhou, Jiangsu, People’s Republic of China; 9Department of Pulmonary and Critical Care Medicine, Shanghai Putuo Liqun Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuanshuan Xie, Email [email protected] Yunfeng Zhang, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) is a major cause of global mortality and disability. Previous research suggests a relationship between gut microbiota and COPD, yet the causal link remains unclear. Hence, we conducted a dual-sample Mendelian randomization study to elucidate the impact of gut microbiota on COPD.
Methods: We utilized single-nucleotide polymorphisms (SNPs) as instrumental variables, and the Inverse Variance Weighted (IVW) method for primary analysis. We explored the causal linkage between gut microbiota species (Coprococcus2, Holdemanella, Allisonella, Anaerostipes, Lachnospiraceae UCG008, Lachnospiraceae UCG010, Prevotella9, Marvinbryantia, Ruminococcaceae UCG013) and COPD through the analysis of genome-wide association study (GWAS) data sourced from a Finnish database. Summary data for COPD (6,915 cases and 186,723 controls), Early onset COPD (3,508 cases and 212,197 controls), admission rate of COPD (9,113 cases and 212,292 controls), related infection of COPD (59,925 cases and 159,867 controls), respiratory dysfunction of COPD (1,031 cases and 186,723 controls), were from FinnGen consortium R7 GWAS.
Result: Our analysis revealed statistically significant correlations between several genera and COPD. Coprococcus2 exhibits a consistent protective role throughout the progression of COPD, evident in both typical COPD [OR=0.750, 95% CI (0.601– 0.937)], early-onset cases [OR=0.686, 95% CI (0.511– 0.920)], COPD-related hospitalizations [OR=0.724, 95% CI (0.575– 0.910)] and infections [OR=0.301, 95% CI (0.094– 0.961)]. Holdemanella manifests as a consistent risk factor in the COPD incidence [OR=1.211, 95% CI (1.063– 1.380)], early-onset COPD [OR=1.214, 95% CI (1.019– 1.446)], COPD hospitalization [OR=1.225, 95% CI (1.072– 1.401)] and respiratory impairment (OR:1.645, 95% CI: 1.198– 2.258). Allisonella demonstrates protective attributes in COPD occurrence [OR=0.884, 95% CI (0.794– 0.984)]. Genera such as Anaerostipes, Lachnospiraceae UCG008, Lachnospiraceae UCG010, and Prevotella9 show protective effects specifically in early-onset COPD. Marvinbryantia and Ruminococcaceae UCG013 are consistently identified as risk factors in onset of typical COPD.
Conclusion: Mendelian randomization studies confirm a causal link between gut microbiota and various COPD types and complications, offering new insights into the disease’s pathogenesis, prevention, and treatment.
Keywords: gut microbiota, Mendelian randomization analysis, chronic obstructive pulmonary disease, gut–lung axis
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic progressive inflammatory disease of the lungs affecting both large and small airways.1,2 COPD seriously influences the lives and health of people around the world, and has become a huge burden on the health of the world.3 The human body has a large number of microorganisms, including bacteria, fungi and parasites, and the gut is rich in the number and variety of microorganisms.4 Research has shown that gut flora interacts with the lungs to influence the development of lung disease. This phenomenon is known as the “gut-lung axis.”5,6 This interaction mainly focuses on immune regulation and inflammatory responses. Viral infection in the lungs may lead to impaired innate immune function and cause dysbiosis of the intestinal flora, thereby weakening the intestinal barrier function. Conversely, changes in the intestinal flora may not only affect the immune function of the lungs and intensify systemic inflammatory responses, but also increase the risk of superinfection.5 Many recent studies have revealed an association between gut flora and lung disease. Liu et al analyzed the correlation between genome sequencing results of fecal samples from 7115 patients and the incidence of asthma and COPD after 15 years, and found that gut flora, such as Escherichia, Enterococcus, Clostridium, Veillonella, is an important risk factor for asthma and COPD.7 Yu-Chi Chiu et al showed that Fusobacterium and Aerococcus were more abundant in severe COPD patients’ gut microbiota, according to 16S rRNA sequencing of the fecal microbiomes of patients with COPD.8 Bacterial genera are significantly reduced in the intestinal flora of patients with COPD, including the genera Bacteroides and Roseburia in the family Lachnospiraceae. Gut flora plays an important role in the development of COPD, and an increase or decrease in the abundance of certain specific bacteria may lead to the development or even aggravation of COPD. In summary, existing research has preliminarily demonstrated that patients with COPD exhibit reduced gut microbiota diversity and compositional imbalance, highlighting the potential involvement of the gut–lung axis in the onset and progression of the disease. However, most studies to date have been cross-sectional in nature, focusing primarily on the associations between microbial alterations and clinical features of COPD, while lacking in-depth analysis of causal relationships. Notably, there remains a significant gap in understanding whether the gut microbiota contributes to the development and exacerbation of COPD and its complications—such as disease progression, hospitalizations, and infections—through modulation of systemic inflammation, immune responses, or metabolic pathways. Moreover, current evidence supporting the efficacy of microbiota-targeted interventions in improving COPD outcomes remains limited. Therefore, further investigation of the gut–lung axis is warranted to better characterize gut microbial alterations in COPD patients and to elucidate the causal mechanisms underlying these changes. Such research is of great importance for developing early intervention strategies and novel therapeutic approaches for COPD and its associated complications.
Mendelian randomization (MR) analysis uses genetic variation as an instrumental variable to infer whether there is a causal relationship between risk factors and health outcomes.9 Mendelian randomization studies using randomly assigned genetic variants at conception are more rational and stable than other observational studies.10,11 The Mendelian randomization approach has been widely used to investigate potential causal relationships between the gut microbiota and a variety of diseases in multiple systems of the body, including neuropsychiatric disorders,12,13 autoimmune disorders,14 and metabolic disorders.15 This approach is effective in exploring causality between the factors of interest and outcomes. Concerning the relationship between the gut microbiota and COPD, a number of studies have confirmed a causal relationship between changes in certain gut microbiota and COPD.16,17 However, fewer studies have explored the causal relationship that exists between the gut microbiota and the onset and further progression of COPD. MR offers unique advantages in exploring the causal relationship between gut microbiota and COPD and its complications. On one hand, the composition of the gut microbiota is influenced by a variety of environmental and lifestyle factors, such as diet, medication use, and smoking, which are difficult to fully control for in traditional cohort studies due to potential confounding. On the other hand, as a chronic progressive disease, COPD itself may alter gut microbiota composition, thereby introducing the risk of reverse causality. MR, by employing genetic variants (eg, single nucleotide polymorphisms [SNPs] identified through genome-wide association studies) associated with specific gut microbial taxa as instrumental variables, can theoretically overcome these limitations. This approach provides more robust evidence for assessing the potential causal role of gut microbiota in the development and progression of COPD and its related complications. In this study, we performed two sample MR Analyses to explore potential causal relationships between gut microbiota and COPD development, infection exacerbation, and hospital admission. This study revealed a potential causal relationship between some gut bacteria and the development of COPD, and hoped to provide new treatment options for treating COPD and preventing infection exacerbations.
Materials and Methods
Study Design
The Mendelian Randomization is based on three key postulated conditions, as shown in Figure 1. The first point is the Associative Hypothesis, which means that genetic variations must be strongly associated with the exposure factors. The second hypothesis is the Independence Hypothesis, which asserts that genetic variations are independent of confounding factors. The third assumption is the Exclusivity Hypothesis, which means that genetic variations can only influence outcomes through exposure factors. (Figure 1).
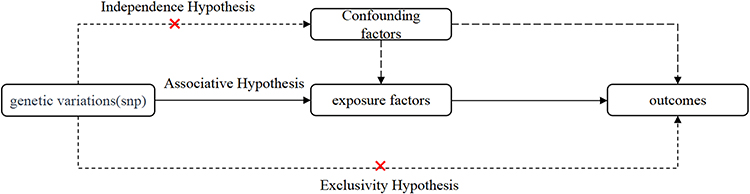 |
Figure 1 A classic designing process of Mendelian randomizations. The arrows in the DAGs depict causal relationships between two variables, indicating causality from the cause to the effect. If an “×” is present on an arrowed line, it signifies that a causal pathway is blocked. |
Data Sources
The research harnessed GWAS summary data from the MiBioGen database to study the gut microbiota, focusing on a comprehensive genetic analysis of 211 taxa. From this pool, 15 microbial taxa lacking specific species names were omitted. This left a refined categorization of six taxonomic groups at the level of 9 phyla, 16 classes, 20 orders, 31 families, and 119 genera. However, the study’s final analysis was conducted exclusively at the genus level. Detailed investigations were conducted on organisms such as (Coprococcus2, Holdemanella, Allisonella, Anaerostipes, Lachnospiraceae UCG008, Lachnospiraceae UCG010, Prevotella9 and so on), with SNPs having (P< 5e-5) used as instrumental variables.
GWAS summary data on COPD (6,915 cases and 186,723 controls), Early onset COPD which typically defined as diagnosis before the age of 50 with a smoking history of at least 10 years18,19 (3,508 cases and 212,197 controls), admission rate of COPD (9,113 cases and 212,292 controls), related infection of COPD (59,925 cases and 159,867 controls), respiratory dysfunction of COPD which was evaluated using the Nijmegen Questionnaire, a validated tool comprising 16 items, each rated on a scale from 0 to 4 and a total score exceeding 23 is indicative of clinically significant respiratory dysfunction20 (1,031 cases and 186,723 controls), were obtained from results of the GWAS on the FinnGen consortium R7. Detailed data on the involved cohorts, genotypes, endpoint definition, and association test in the FinnGen consortium are available on the FinnGen webpage.
Instrumental Variable Selection
The selection of instrumental variables involved the following criteria (1) Selection of Potential Instrumental Variables: SNPs associated with each genus were chosen if they met the locus-wide significance threshold (P < 1 × 10^-5). (2) Calculation of Linkage Disequilibrium: European samples data from the 1000 Genomes Project were used as a reference panel to compute linkage disequilibrium between SNPs. Among SNPs with an r^2 < 0.001 (using a clumping window size of 10,000 kb), only those with the lowest P-values were retained. (3) Exclusion of Low Minor Allele Frequency SNPs: SNPs with a minor allele frequency (MAF) ≤ 0.01 were excluded. (4) Treatment of Palindromic SNPs: In cases where palindromic SNPs were present, the alleles on the forward strand were inferred using allele frequency information.
The strength of these instrumental variables was assessed by calculating the F-statistic using the formula F = R’ × (N - 1 - K) / [(1 - R^2) × K], where R^2 represents the proportion of variance in the exposure explained by the genetic variants, N represents the sample size, and K represents the number of instruments. If the corresponding F-statistic was greater than 10, it was considered that there was no significant weak instrumental bias.
Mendelian Randomization Analysis
We employed four different methods for conducting MR analysis, which included the following: inverse variance weighted (IVW), multiplicative random effects (MR-Egger), weighted median, and weighted mode.
IVW, being the most commonly used and efficient method, was chosen as the primary analysis for this study. This choice was made because IVW provides the estimate with the highest statistical power, under the assumption that all SNPs used are valid instrumental variables. However, in cases where the assumption of no pleiotropy is violated, MR-Egger offers a more robust alternative. MR-Egger regression is a commonly used complementary method in MR studies, primarily employed to detect and correct for bias introduced by horizontal pleiotropy among genetic instrumental variables. Unlike the IVW method, MR-Egger allows for consistent estimation of causal effects under the less stringent InSIDE (Instrument Strength Independent of Direct Effect) assumption. It can assess the presence of directional pleiotropy, indicated by a non-zero average pleiotropic effect of the genetic variants.21 However, MR-Egger generally has lower statistical power than IVW and is more sensitive to outliers,22 potentially leading to unstable estimates. To examine the presence of pleiotropy and assess the robustness of our results, we conducted an MR-Egger intercept test. It is important to note that when multiple genetic variants influence the outcome through a shared confounding pathway, MR-Egger may be more susceptible to bias than the IVW method and may exhibit an increased Type I error rate.21,23 The weighted median, and weighted mode methods each have their respective strengths and limitations. Their applicability depends on the specific research question and the data available. To ensure the robustness of our findings, we also conducted supplementary analyses using these three methods.
Our sensitivity analysis was conducted to verify the stability and reliability of our research findings. In our MR analysis of all microbial communities, we utilized four MR methods, which included IVW, Weighted median, MR-Egger, and Simple Mode. Additionally, we also conducted tests for heterogeneity and horizontal pleiotropy to further ensure the stability of the results. Furthermore, we also employed Leave-One-Out cross-validation to assess the robustness of the instrumental variables for each genus. To reduce the risk of false-positive results, we applied false discovery rate (FDR) correction for multiple testing on associations with IVW-MR p values < 0.05.
All MR analyses were executed using R (version 4.1.2) with the R packages (TwoSampleMR and MRPRESSO).
Results
The Occurrence of COPD and Early Onset COPD
During the progression of COPD, the microbial community Coprococcus2 has shown a significant protective effect in the occurrence of both common COPD and early-onset COPD. Specifically, using the IVW method for analysis, the odds ratio (OR) for COPD incidence is 0.750 (95% CI: 0.601–0.937), and for early-onset COPD, the OR is 0.686 (95% CI: 0.511–0.920). On the other hand, the microbial genus Holdemanella has been identified as a risk factor in the development of both COPD and early-onset COPD, with corresponding OR values of 1.211 (95% CI: 1.063–1.380) and 1.214 (95% CI: 1.019–1.446). (Figures 2 and 3).
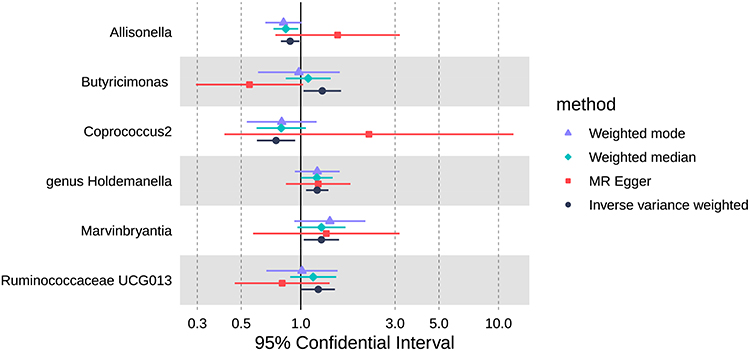 |
Figure 2 Forest plot of the causal effect of gut microbiota on the occurrence of COPD. in the analysis based on weighted mode methods, weighted median, multiplicative random effects (MR-Egger) and inverse variance weighted (IVW). |
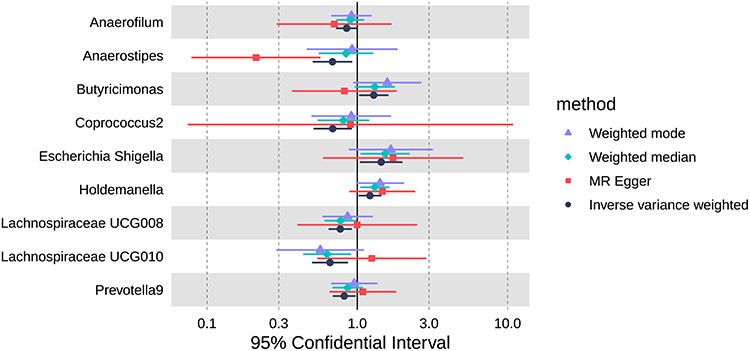 |
Figure 3 Forest plot of the causal effect of gut microbiota on the occurrence of early onset COPD in the analysis based on weighted mode methods, weighted median, multiplicative random effects (MR-Egger) and inverse variance weighted (IVW). |
Allisonella, exhibits a protective role in the development of COPD. The odds ratios (OR) from all four MR methods are less than 1, with the OR from the IVW method being 0.884 (95% CI: 0.794–0.984). Other genera, such as Anaerostipes, Lachnospiraceae UCG008, Lachnospiraceae UCG010, and Prevotella9, show protective effects in the context of early-onset COPD. Conversely, in the development of COPD, Marvinbryantia and Ruminococcaceae UCG013 are identified as risk factors. However, for some genera, although the IVW method results suggest risk, differences exist between the results obtained from other MR methods. Therefore, the stability of their outcomes requires further investigation.
COPD-Related Complications, Such as Admission Rate, Respiratory Dysfunction, and Infections
In the context of COPD-related hospitalization and infections, the microbial genus Coprococcus2 continues to exhibit a protective effect with OR values of 0.724 (95% CI: 0.575–0.910) and 0.301 (95% CI: 0.094–0.961) using the IVW method. However, caution is warranted regarding this conclusion, as the OR values from the MR Egger method significantly exceed 1. (Figures 4 and 5).
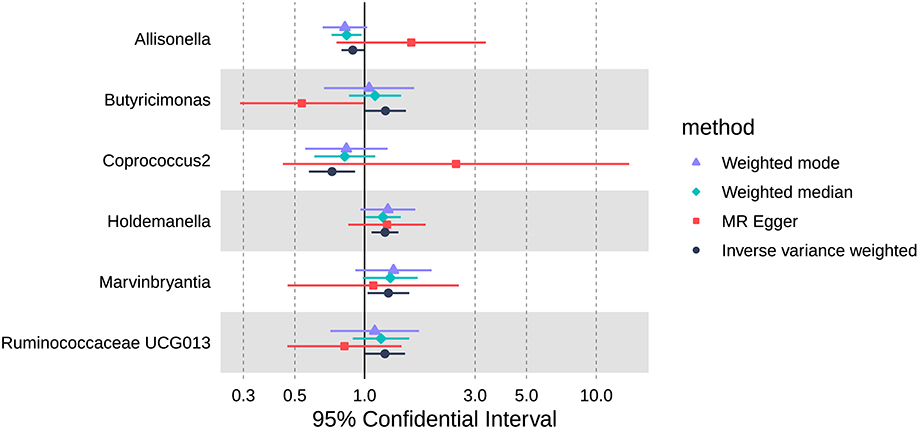 |
Figure 4 Forest plot of the causal effect of gut microbiota on the admission rate of COPD in the analysis based on weighted mode methods, weighted median, multiplicative random effects (MR-Egger) and inverse variance weighted (IVW). |
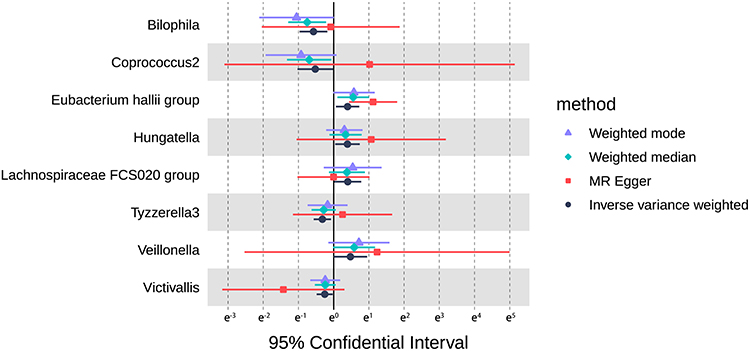 |
Figure 5 Forest plot of the causal effect of gut microbiota on the related infections of COPD in the analysis based on weighted mode methods, weighted median, multiplicative random effects (MR-Egger) and inverse variance weighted (IVW). |
On the other hand, for COPD hospitalization or respiratory impairment, the microbial genus Holdemanella consistently demonstrates a stable risk effect, with OR values of 1.225 (95% CI: 1.072–1.401) and 1.645 (95% CI: 1.198–2.258) using the IVW method. (Figures 4 and 6).
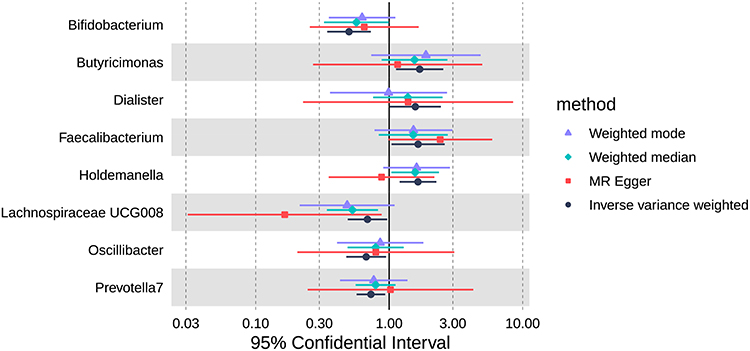 |
Figure 6 Forest plot of the causal effect of gut microbiota on the respiratory dysfunction in COPD in the analysis based on weighted mode methods, weighted median, multiplicative random effects (MR-Egger) and inverse variance weighted (IVW). |
Other genera, such as Allisonella, Marvinbryantia, and Ruminococcaceae UCG013, among others, each exhibit their respective protective or risk effects in relation to COPD-related hospitalization. Additionally, various other genera show significant impacts on respiratory impairment or infection. (Figures 4–6).
Sensitivity Analysis
We conduct sensitivity analysis to confirm the stability and reliability of the results obtained in our research. In the MR analysis of all microbial communities, we employed four MR methods, including IVW, Weighted Median, MR-Egger, and Simple Mode. Furthermore, we conducted examinations for heterogeneity and horizontal pleiotropy as an additional measure to ensure the stability of our findings. Despite demonstrating a protective effect against COPD in the IVW, Weighted Median, and Simple Mode methods, the protective effect of Coprococcus2 is not pronounced in the MR-Egger method. This may suggest that the MR-Egger method is more susceptible to the influence of weak instrument strength. The two bacterial groups, Holdemanella and Allisonella, consistently demonstrated results across all four MR methods, suggesting the stability of their effects in the development and early onset of COPD. Other genera, such as Anaerostipes and Lachnospiraceae UCG008, exhibited significant differences in their results across different MR methods. This could be attributed to the potential existence of non-linear causal relationships within these genera or the relatively weaker instrument strength of their instrumental variables. Besides, we employed the Leave-One-Out cross-validation method to assess the robustness of instrumental variables for each genus. Through the systematic process of individually excluding each instrumental variable and observing changes in the results, we observed that the majority of instrumental variables had a minimal impact on the stability of the outcomes. However, there were still a few instrumental variables that may have a significant impact on the results for certain genera.
Discussion
More and more studies are showing that interactions between gut bacteria and the lungs are closely related to COPD.6,24 Some clinical studies have collected feces from patients with COPD for gene sequencing to analyze the relationship between gut bacteria and COPD.25 However, most of them are cross-sectional studies in which the patients are already in a disease situation at the time of specimen collection, and it is not possible to determine a causal relationship between the changes in gut bacteria and COPD.7 Some other studies, analyzed the existence of an association between gut bacteria and COPD by MR study, however, these studies were mostly limited to the occurrence of COPD.17,26,27 To the best of our knowledge, we are the first large-scale comprehensive Mendelian randomization study designed to explore the causal relationship between the presence of specific gut bacteria and the occurrence, progression, and severity of COPD. Using MR study, the study reveals that some specific gut bacteria play a very important role in the occurrence and development of COPD. This will likely help in diagnosing COPD at an early stage, predicting the progression of the disease and providing important treatment targets.
In our study, we found that two flora had significant protective effects in the occurrence and development of COPD, among which Allisonella flora had a significant protective effect in the occurrence of COPD and early occurrence of COPD with good stability of the results. Coprococcus2 flora showed a significant protective effect in both common COPD and early occurrence COPD. However, Holdemanella flora showed risk factor in both occurrence and development of COPD with more stable results. In addition to this there were other flora that showed protective or risk factors.
In the present study, we found that Allisonella flora has a protective role in the development of COPD. Allisonella flora is a special genus of bacteria in the human gut, which can metabolize and produce histamine, inhibit intestinal microbial ectasia, and promote intestinal mucosal repair.17,28 A Mendelian randomization analysis in a previous study suggested a potential inverse causal relationship between the genus Allisonella and COPD, indicating that the presence of Allisonella may be associated with a reduced risk of developing COPD.17 Having Allisonella flora in normal proportions helps to maintain the stability of the intestinal microflora, maintains normal intestinal barrier function, and inhibits the onset and progression of COPD.29 However, in a study investigating gut microbiota characteristics across individuals with varying levels of systemic inflammation, Paula et al observed a significant increase in the relative abundance of the genus Allisonella among those with higher inflammatory indices.30 This finding suggests that Allisonella may play a potential role in the onset and progression of COPD by promoting inflammatory responses. These conflicting findings highlight the complexity of Allisonella’s role in COPD, suggesting that its effects may be context-dependent, potentially influenced by host genetics, microbial interactions, or environmental factors. These results indicate the possibility of targeting Allisonella as a novel therapeutic strategy for the prevention or treatment of COPD. However, current research on Allisonella remains limited, and the underlying mechanisms by which it may influence COPD development and progression require further investigation.
Coprococcus2 flora is an important member of the thick-walled bacterial phylum Trichoderma, an important genus of bacteria in the intestine. Most studies on Coprococcus2 intestinal flora have focused on neuropsychiatric disorders such as depression, Parkinson’s disease, and autism.31–33 However, in recent years, studies have also found that Coprococcus2 flora has a protective effect against COPD disease.17 In our study, Coprococcus2 flora showed significant protection in the development of both common COPD and early-onset COPD, as well as in COPD-associated hospitalizations and infections. It may be due to the fact that in the gastrointestinal tract C. faecalis is able to ferment carbohydrates and produce metabolites such as butyric and acetic acid, which inhibit the growth of harmful intestinal flora and maintain the stability of the intestinal flora. This finding may suggest that the genus Coprococcus2 represents a novel target for interventions aimed at preventing or treating the development and progression of COPD and its associated complications.
Holdemanella, a strictly anaerobic, Gram-positive bacterium belonging to the phylum Firmicutes, is predominantly found in the human gut but can also be detected in the gastrointestinal tracts of animals. Previous studies have indicated that Holdemanella may play a role in various diseases, including diabetes, cognitive impairment, and colorectal cancer.34–36 Du and Zhou et al identified Holdemanella as a potential risk factor for COPD,37,38 which is consistent with our findings. Notably, Holdemanella abundance was found to be negatively correlated with levels of propionate and isobutyrate, suggesting a possible pro-inflammatory role in the progression of COPD. However, the underlying mechanisms remain to be elucidated. Contrarily, some studies have reported a trend toward a protective effect of Holdemanella against COPD.39 Therefore, the precise role of Holdemanella in the onset and progression of COPD remains unclear, warranting further mechanistic investigations to clarify its functional impact.
Anaerostipes is a genus of anaerobic bacteria belonging to the phylum Firmicutes and the class Clostridia. Species within this genus are typically anaerobic and colonize the human gut, where they break down indigestible dietary fibers to produce short-chain fatty acids (SCFAs), such as acetate, propionate, and butyrate. These SCFAs play a crucial role in maintaining gut health by providing energy, preserving intestinal barrier function, and regulating immune responses.40 Studies have shown that Anaerostipes can prevent milk allergy in mice. Butyrate-producing anaerobic bacteria can facilitate the colonization and modulation of distinct resident microbiota, as well as regulate the host’s immune response to food antigens.41 This study suggests that Anaerostipes may exhibit a protective effect against early-onset COPD, potentially through the production of SCFAs that regulate immune responses and suppress inflammation. This implies that increasing the abundance of Anaerostipes, or supplementing with prebiotics or probiotics to enhance SCFA production, could help restore gut microbiome balance and reduce systemic inflammation, offering a potential therapeutic strategy for mitigating the onset of early-onset COPD.
Marvinbryantia is a relatively novel and less extensively studied genus of anaerobic gut bacteria, classified within the phylum Firmicutes, class Clostridia, order Clostridiales, and family Lachnospiraceae. Members of this genus are primarily identified in the gastrointestinal tracts of humans and animals, where they may play important roles in maintaining microbial homeostasis and contributing to the synthesis of key metabolic products. Several studies have identified associations between Marvinbryantia and various diseases, including Alzheimer’s disease, type 2 diabetes, diabetic nephropathy, and liver cirrhosis.42–45 Currently, research on the association between Marvinbryantia and COPD remains limited, and whether Marvinbryantia plays a role in the development of COPD is still unclear. However, some studies have reported a positive correlation between Marvinbryantia and pro-inflammatory cytokines.46 In line with our findings that Marvinbryantia may act as a risk factor for COPD development, this suggests that it could contribute to the progression of COPD through modulation of inflammatory responses.
In conclusion, our findings suggest that gut microbial genera such as Coprococcus2, Allisonella and Marvinbryantia hold promise as potential targets or biomarkers for COPD intervention. Modulating the gut microbiota through dietary strategies, prebiotics, or other microbiota-directed approaches could offer novel avenues for mitigating disease progression in COPD patients and may even contribute to the prevention of disease onset.
In our study, we applied FDR correction to control for the potential risk of false positives due to testing multiple genera. Although most associations did not reach statistical significance after correction, we observed consistent trends across different COPD outcomes for several genera. These trends are biologically plausible and have been reported in previous literature. Given that our study represents an exploratory Mendelian randomization analysis in the field of microbiome research where host-microbiota interactions are inherently complex, we believe these findings offer valuable insights and may inform future large-scale, multi-population studies.
We have several strengths in this study as follows. First, we used a two-sample Mendelian analysis to investigate the causal relationship that exists between gut microflora and COPD disease. Secondly, we investigated the causal associations that exist between gut flora and multiple outcomes of the onset and progression of common COPD and early-onset COPD. Traditional observational studies are susceptible to confounding factors and reverse causality, making the causal associations weak, but Mendelian analyses using an instrumental variable approach are more effective in deriving causal associations. In addition, we used GWAS database data for the study, which covers multiple populations and has a wider applicability of the results, and we used a combination of four analyses, IVW, Weighted median, Simple Mode, and MR-Egger, to make the results more stable.
However, several limitations of this study should be acknowledged. First, the population included in the underlying GWAS dataset was exclusively of European ancestry. Given potential genetic and gut microbiota differences across ethnic groups, the generalizability of our findings to non-European populations may be limited. Second, weak instrument bias in MR studies can lead to underestimation of causal effects and reduced statistical power. Finally, the proportion of variance in microbial exposure explained by genetic variants is relatively small, which may constrain the interpretability and clinical applicability of the observed causal estimates.
Conclusion
In conclusion, we systematically assessed the causal relationship that exists between the gut microbiota and COPD through two-sample MR analysis of data from the GWAS, identifying pathogenic and protective flora associated with the occurrence of common COPD and early-onset COPD and associated complications. This study provides genetic evidence supporting the causal role of gut microbiota in the pathogenesis of COPD, reinforcing the importance of the gut-lung axis in the development of chronic lung diseases. The identified microbial taxa may serve as potential targets for future COPD prediction, biomarker screening, and microbiota-based intervention strategies, such as probiotics or dietary fiber supplementation. However, despite the strengths of Mendelian randomization in mitigating confounding and reverse causality, this study is still limited by population heterogeneity and genetic pleiotropy, and further functional validation is needed to confirm these findings.
Overall, causal inference based on Mendelian randomization supports the gut microbiota as a crucial regulatory factor in COPD prevention and treatment, suggesting that modulating the gut microbiome may offer novel approaches for early intervention and personalized therapy for COPD.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the Putuo District Health and Wellness System, Shanghai (Approval No. 2024 tszb07). The requirement for informed consent was waived by the ethics committee, as all data used in the study were obtained from publicly available databases and were fully anonymized. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments.
Acknowledgments
The authors express their gratitude to all the participants and researchers for their participation in this MR study. The authors also appreciate the MiBioGen and UK Biobank consortia for releasing the GWAS summary statistics.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
No additional consent for publication is necessary as this study utilized de-identified patient data obtained from a public database and the use of these data complies with the terms and conditions of the database and the relevant ethical guidelines.
Funding
This paper was supported by the grant from Program for Research-oriented Physician of Shanghai Tenth People’s Hospital (No.2023YJXYSC007) and the Shanghai Putuo District Health Commission Clinical Specialty Program of Chronic Obstructive Pulmonary Disease (No.2024TSZB07).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Divo MJ, Cabrera C, Casanova C, et al. Comorbidity distribution, clinical expression and survival in COPD patients with different body mass index. Chronic Obstr Pulm Dis. 2014;1(2):229–238. doi:10.15326/jcopdf.1.2.2014.0117
2. Divo MJ, Martinez CH, Mannino DM. Ageing and the epidemiology of multimorbidity. Eur Respir J. 2014;44(4):1055–1068. doi:10.1183/09031936.00059814
3. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
4. Ifejika-Jones NL, Harun, Arun NH, et al. The interaction of aspiration pneumonia with demographic and cerebrovascular disease risk factors is predictive of discharge level of care in acute stroke patient. Am J Phys Med Rehabil. 2012;91(2):141–147. doi:10.1097/phm.0b013e31823caa8d
5. Budden KF, Gellatly SL, Wood DL, et al. Emerging pathogenic links between microbiota and the gut-lung axis. Nat Rev Microbiol. 2017;15(1):55–63. doi:10.1038/nrmicro.2016.142
6. Song W, Yue Y, Zhang Q. Imbalance of gut microbiota is involved in the development of chronic obstructive pulmonary disease: a review. Biomed Pharmacother. 2023;165:115150. doi:10.1016/j.biopha.2023.115150
7. Liu Y, Teo SM, Méric G, et al. The gut microbiome is a significant risk factor for future chronic lung disease. J Allergy Clin Immunol. 2023;151(4):943–952. doi:10.1016/j.jaci.2022.12.810
8. Chiu YC, Lee SW, Liu CW, et al. Comprehensive profiling of the gut microbiota in patients with chronic obstructive pulmonary disease of varying severity. PLoS One. 2021;16(4):e0249944. doi:10.1371/journal.pone.0249944
9. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–496. doi:10.1002/jrsm.1346
10. Au Yeung SL, Borges MC, Lawlor DA, Schooling CM. Impact of lung function on cardiovascular diseases and cardiovascular risk factors: a two sample bidirectional Mendelian randomisation study. Thorax. 2022;77(2):164–171. doi:10.1136/thoraxjnl-2020-215600
11. Ponsford MJ, Gkatzionis A, Walker VM, et al. Cardiometabolic traits, sepsis, and severe COVID-19: a Mendelian randomization investigation. Circulation. 2020;142(18):1791–1793. doi:10.1161/circulationaha.120.050753
12. Li P, Wang H, Guo L, et al. Association between gut microbiota and preeclampsia-eclampsia: a two-sample Mendelian randomization study. BMC Med. 2022;20(1):443. doi:10.1186/s12916-022-02657-x
13. Ni JJ, Xu Q, Yan SS, et al. Gut microbiota and psychiatric disorders: a two-sample Mendelian randomization study. Front Microbiol. 2021;12:737197. doi:10.3389/fmicb.2021.737197
14. Xu Q, Ni JJ, Han BX, et al. Causal relationship between gut microbiota and autoimmune diseases: a two-sample Mendelian randomization study. Front Immunol. 2021;12:746998. doi:10.3389/fimmu.2021.746998
15. Liu K, Zou J, Fan H, Hu H, You Z. Causal effects of gut microbiota on diabetic retinopathy: a Mendelian randomization study. Front Immunol. 2022;13:930318. doi:10.3389/fimmu.2022.930318
16. Shi H, Zhao T, Geng R, Sun L, Fan H. The associations between gut microbiota and chronic respiratory diseases: a Mendelian randomization study. Front Microbiol. 2023;14:1200937. doi:10.3389/fmicb.2023.1200937
17. Wei Y, Lu X, Liu C. Gut microbiota and chronic obstructive pulmonary disease: a Mendelian randomization study. Front Microbiol. 2023;14:1196751. doi:10.3389/fmicb.2023.1196751
18. Martinez FJ, Han MK, Allinson JP, et al. At the root: defining and halting progression of early chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(12):1540–1551. doi:10.1164/rccm.201710-2028PP
19. Soriano JB, Polverino F, Cosio BG. What is early COPD and why is it important? Eur Respir J. 2018;52(6):1801448. doi:10.1183/13993003.01448-2018
20. van Dixhoorn J, Duivenvoorden HJ. Efficacy of Nijmegen Questionnaire in recognition of the hyperventilation syndrome. J Psychosom Res. 1985;29(2):199–206. doi:10.1016/0022-3999(85)90042-x
21. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
22. Larsson SC, Butterworth AS, Burgess S. Mendelian randomization for cardiovascular diseases: principles and applications. Eur Heart J. 2023;44(47):4913–4924. doi:10.1093/eurheartj/ehad736
23. Burgess S, Thompson SG. Erratum to: interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):391–392. doi:10.1007/s10654-017-0276-5
24. Bowerman KL, Rehman SF, Vaughan A, et al. Disease-associated gut microbiome and metabolome changes in patients with chronic obstructive pulmonary disease. Nat Commun. 2020;11(1):5886. doi:10.1038/s41467-020-19701-0
25. Passos FC, Oliveira LMG, Jesus FR, et al. Beneficial bacteria in the gut microbiota may lead to improved metabolic and immunological status in chronic obstructive pulmonary disease. Med Sci. 12(3). doi:10.3390/medsci12030041
26. Du Y, Wang S, Zhou T, Zhao Z. Causal effects of gut microbiota and metabolites on chronic obstructive pulmonary disease: a bidirectional two sample Mendelian randomization study. Int J Chron Obstruct Pulmon Dis. 2024;19:2153–2167. doi:10.2147/copd.S472218
27. Li WJ, Yao C, Han L, Zhou JH, Pang RM. Causal relationship between gut microbiota and chronic obstructive pulmonary disease: a bidirectional two-sample Mendelian randomization study. Int J Chron Obstruct Pulmon Dis. 2024;19:1957–1969. doi:10.2147/copd.S464917
28. Garner MR, Flint JF, Russell JB. Allisonella histaminiformans gen. nov. sp. nov. A novel bacterium that produces histamine, utilizes histidine as its sole energy source, and could play a role in bovine and equine laminitis. Syst Appl Microbiol. 2002;25(4):498–506. doi:10.1078/07232020260517625
29. Binda C, Lopetuso LR, Rizzatti G, Gibiino G, Cennamo V, Gasbarrini A. Actinobacteria: a relevant minority for the maintenance of gut homeostasis. Dig Liver Dis. 2018;50(5):421–428. doi:10.1016/j.dld.2018.02.012
30. Aranaz P, Ramos-Lopez O, Cuevas-Sierra A, Martinez JA, Milagro FI, Riezu-Boj JI. A predictive regression model of the obesity-related inflammatory status based on gut microbiota composition. Int J Obes. 2021;45(10):2261–2268. doi:10.1038/s41366-021-00904-4
31. Guo D, Chen Q, Wang G, Li C. Causal relationship between gut microbiota and immune thrombocytopenia: a Mendelian randomization study of two samples. Front Microbiol. 2023;14:1190866. doi:10.3389/fmicb.2023.1190866
32. Liang Y, Zeng W, Hou T, et al. Gut microbiome and reproductive endocrine diseases: a Mendelian randomization study. Front Endocrinol. 2023;14:1164186. doi:10.3389/fendo.2023.1164186
33. Jin Q, Ren F, Dai D, Sun N, Qian Y, Song P. The causality between intestinal flora and allergic diseases: insights from a bi-directional two-sample Mendelian randomization analysis. Front Immunol. 2023;14:1121273. doi:10.3389/fimmu.2023.1121273
34. Xu YJ, He Y, Chen C, et al. Multiomics analysis revealed colorectal cancer pathogenesis. J Proteome Res. 2024;23(6):2100–2111. doi:10.1021/acs.jproteome.3c00894
35. Ning M, An L, Dong L, et al. Causal associations between gut microbiota, gut microbiota-derived metabolites, and alzheimer’s disease: a multivariable Mendelian randomization study. J Alzheimers Dis. 2024;100(1):229–237. doi:10.3233/jad-240082
36. Romaní-Pérez M, López-Almela I, Bullich-Vilarrubias C, et al. Holdemanella biformis improves glucose tolerance and regulates GLP-1 signaling in obese mice. FASEB j. 2021;35(7):e21734. doi:10.1096/fj.202100126R
37. Du Y, Li X, An Y, Song Y, Lu Y. Association of gut microbiota with sort-chain fatty acids and inflammatory cytokines in diabetic patients with cognitive impairment: a cross-sectional, non-controlled study. Front Nutr. 2022;9:930626. doi:10.3389/fnut.2022.930626
38. Zhou X, Shen S, Wang Z. Genetic evidence of bidirectional Mendelian randomization study on the causality between gut microbiome and respiratory diseases contributes to gut-lung axis. Sci Rep. 2024;14(1):25550. doi:10.1038/s41598-024-77273-1
39. Su Y, Zhang Y, Xu J. Genetic association and bidirectional Mendelian randomization for causality between gut microbiota and six lung diseases. Front Med. 2023;10:1279239. doi:10.3389/fmed.2023.1279239
40. Liu D, Xie LS, Lian S, et al. Anaerostipes hadrus, a butyrate-producing bacterium capable of metabolizing 5-fluorouracil. mSphere. 9(4):e0081623. doi:10.1128/msphere.00816-23
41. Hesser LA, Puente AA, Arnold J, et al. A synbiotic of Anaerostipes caccae and lactulose prevents and treats food allergy in mice. Cell Host Microbe. 2024;32(7):1163–1176.e6. doi:10.1016/j.chom.2024.05.019
42. Verhaar BJH, Hendriksen HMA, De leeuw FA, et al. Gut microbiota composition is related to AD pathology. Front Immunol. 2021;12:794519. doi:10.3389/fimmu.2021.794519
43. Chen Z, Radjabzadeh D, Chen L, et al. Association of insulin resistance and type 2 diabetes with gut microbial diversity: a microbiome-wide analysis from population studies. JAMA Netw Open. 2021;4(7):e2118811. doi:10.1001/jamanetworkopen.2021.18811
44. He G, Chen J, Hao W, Hu W. Causal effect of gut microbiota and diabetic nephropathy: a Mendelian randomization study. Diabetol Metab Syndr. 2024;16(1):89. doi:10.1186/s13098-024-01327-7
45. Yuan M, Hu X, Yao L, et al. Causal relationship between gut microbiota and liver cirrhosis: 16S rRNA sequencing and Mendelian randomization analyses. J Clin Transl Hepatol. 2024;12(2):123–133. doi:10.14218/jcth.2023.00259
46. Zhang Y, Chen L, Hu M, et al. Dietary type 2 resistant starch improves systemic inflammation and intestinal permeability by modulating microbiota and metabolites in aged mice on high-fat diet. Aging. 2020;12(10):9173–9187. doi:10.18632/aging.103187
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.