Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
The Impact of Comorbidities, EEG Abnormalities, and ASM Use as a Predicting Outcomes in Pediatric Status Epilepticus
Authors Chen D, Zhang Q, Miao H, Xu J, Li W ![]()
Received 26 May 2025
Accepted for publication 6 August 2025
Published 14 August 2025 Volume 2025:21 Pages 1689—1702
DOI https://doi.org/10.2147/NDT.S542918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Dongmei Chen,1 Qin Zhang,1 Hongjun Miao,1 Jin Xu,2 Wenjing Li2
1Emergency Department/Intensive Care Unit, Children’s Hospital of Nanjing Medical University, Nanjing, 210008, People’s Republic of China; 2Department of Pharmacy, Children’s Hospital of Nanjing Medical University, Nanjing, 210008, People’s Republic of China
Correspondence: Wenjing Li, Department of Pharmacy, Children’s Hospital of Nanjing Medical University, 72 Guangzhou Road, Nanjing, 210008, People’s Republic of China, Email [email protected]
Background: Pediatric patients admitted to the pediatric intensive care unit (PICU) often present with diverse clinical conditions that influence their prognosis. Identifying key prognostic factors is crucial for optimizing treatment strategies and improving patient outcomes.
Methods: A retrospective analysis was conducted on the clinical data of 203 pediatric patients with status epilepticus (SE) admitted to the PICU from January 2020 and December 2024. Based on result of the GOS score at 3 months after discharge, patients were categorized into the good prognosis group and the poor prognosis group. Perform statistical analysis on the data of two groups to identify risk factors associated with poor prognosis. The predictive value of the STEPSS and END-IT scoring systems was evaluated using ROC curve analysis.
Results: Among the 203 pediatric patients, the proportion of patients in the good prognosis group (68.5%) was significantly higher than that in the poor prognosis group (31.5%). The median hospital stay was longer in the poor prognosis group [11.0 (7.0, 16.0) days] compared to the good prognosis group [9.0 (7.0, 13.0) days]. The presence of comorbidities (79.7% vs 63.3%), abnormal EEG findings (98.0% vs 89.0%), and polypharmacy with ASMs (82.8% vs 31.7%) were significantly associated with poor prognosis. Logistic regression analysis indicated that the use of multiple ASMs was an independent risk factor for poor prognosis, with patients receiving two or more ASMs being 4.48 times more likely to have an unfavorable outcome (95% CI: 2.223– 9.029). The predictive value of the STEPSS and END-IT scoring systems was limited, with AUC values of 0.475 (P = 0.570) and 0.535 (P = 0.419), respectively.
Conclusion: Comorbidities, abnormal EEG findings, and increased ASM use are significant risk factors for poor prognosis in PICU patients with SE. ASM usage plays a crucial role in patient outcomes. Further research is needed to refine prognostic models and enhance clinical decision-making.
Keywords: antiepileptic drugs, EEG, END-IT, pediatric intensive care unit, prognosis, STEPSS
A Letter to the Editor has been published for this article.
Epilepsy is a common neurological disorder in clinical practice, characterized by sudden, transient abnormalities in brain function, such as loss of consciousness, abnormal muscle tone, sensory disturbances, and mental disorders. More than 50 million people worldwide suffer from epilepsy, with the prevalence in developed countries and developing countries being 5‰ and 7.2‰, respectively. In China, the prevalence of epilepsy ranges from 4‰ to 7‰, with a significantly higher incidence in males than females. Notably, more than 50% of cases first onset during childhood or adolescence.1
The pharmacological treatment of epilepsy follows the principle of monotherapy as the first-line approach, with the use of a single ASM at an adequate dosage and duration. With the proper and scientific use of ASMs (anti-seizure medication), most patients experience good symptom control, with an effective control rate of 70% to 80%. However, approximately 20% to 30% of patients, particularly children, experience drug-resistant epilepsy (DRE).2 DRE presents significant challenges due to its complex etiology, difficulties in pharmacological management, and poor prognosis, making it a major issue in pediatric neurological diseases.2–5
DRE often manifests as SE or refractory status epilepticus (RSE). SE is a time-sensitive neurological emergency, where prolonged seizure duration, whether in animal models or patients, is associated with increased treatment difficulty and poorer prognosis.6,7 Among SE patients, approximately 23–42% may progress to RSE or super-refractory status epilepticus (SRSE),8–10 conditions that are associated with a high mortality rate of up to 40%.11 In RSE patients, delayed initiation of anesthetic therapy significantly affects treatment outcomes.12 Therefore, early prognostic assessment in pediatric SE patients is crucial, allowing for the development of individualized treatment plans based on clinical presentation and electroencephalographic (EEG) findings. For patients with a high risk of drug resistance and a predisposition to developing DRE, early initiation of combination ASM therapy is recommended upon diagnosis.13
Moreover, several scoring systems are currently available for short-term prognostic evaluation in pediatric SE, including the Status Epilepticus in Pediatric Patients Severity Score (STEPSS), the tracheal intubation (END-IT) score, and the Glasgow Outcome Scale (GOS). The STESS assesses patient prognosis based on four factors: consciousness level, seizure type, history of previous seizures, and age. Subsequent studies have shown that STEPSS has a predictive value for poor outcomes.14 The END-IT score incorporates treatment factors and is currently used to predict post-discharge functional recovery in SE patients. Some studies suggest that the reliability of END-IT in predicting short-term poor outcomes in SE patients is limited. The Glasgow Outcome Scale (GOS) is commonly used for discharge assessment.
This study retrospectively analyzes the clinical data of pediatric patients diagnosed with SE, RSE, and SRSE who were admitted to the PICU of Children’s Hospital of Nanjing Medical University from January 2020 to December 2024. The study aims to analyze the risk factors affecting the prognosis of children with SE and compare the predictive value of the STEPSS and the END-IT score for adverse outcomes in pediatric SE patients, providing evidence for the development of optimized pharmacological treatment strategies for pediatric SE.
Materials and Methods
General Information
This study retrospectively analyzed the clinical data of pediatric patients diagnosed with SE, RSE, and SRSE who were admitted to the PICU of Children’s Hospital of Nanjing Medical University from January 2020 to December 2024. The study was approved by the Ethics Committee of Children’s Hospital of Nanjing Medical University, and informed consent from patients was waived.
SE is defined as either (1) a seizure lasting ≥5 minutes or (2) two or more seizures occurring without a return to baseline consciousness between episodes. In absence seizures, a duration of ≥10–15 minutes is required for SE diagnosis. Additionally, focal seizures with impaired awareness lasting ≥10 minutes can also be classified as SE.15,16
RSE is defined as persistent seizures despite the administration of two to three appropriately dosed ASMs, typically including a benzodiazepine followed by one or two additional ASMs, with electroencephalography (EEG) confirming ongoing epileptiform discharges.17,18
SRSE refers to seizures that continue despite treatment with two or more antiseizure medications beyond the RSE stage or recur upon medication withdrawal despite initial seizure control. SRSE often requires specialized treatment strategies.17,19
Inclusion and Exclusion Criteria
Inclusion Criteria
Patients diagnosed with SE, RSE, or SRSE according to the diagnostic criteria outlined in the 2022 Chinese Expert Consensus on the Diagnosis and Treatment of Pediatric Status Epilepticus.
Exclusion Criteria
(1) Patients older than 14 years;
(2) Patients with comorbid psychiatric disorders.
Methods
Data Collection
Clinical data were collected, including age, sex, etiologies, clinical presentation (level of consciousness, awareness, responsiveness, seizure activity, and muscle tone), diagnosis, length of hospital stay, administered medications, and findings from auxiliary examinations such as brain MRI and EEG monitoring, and cerebrospinal fluid (CSF) analysis.
Etiologies were classified according to the 2022 Chinese Expert Consensus on the Diagnosis and Treatment of Pediatric Status Epilepticus.
Clinical Scoring
All patients were assessed using the STEPSS and END-IT score. A 3-month follow-up was conducted after discharge, and patient outcomes were evaluated using the GOS score.
STEPSS Score
The STEPSS score is derived from the Status Epilepticus Severity Score (STESS) and serves as a simple bedside assessment tool for guiding treatment and prognosis. The score is based on four clinical parameters: age, history of prior seizures, seizure type, and level of consciousness. The total score ranges from 0 to 6, with lower scores indicating a lower risk of poor prognosis, whereas higher scores suggest an increased risk of adverse outcomes. In adult patients, a STESS score ≥3 has been shown to be a reliable predictor of unfavorable outcomes.20 However, the original STESS age criterion (0 points for <65 years; 2 points for ≥65 years) is not applicable to pediatric patients. Therefore, in STEPSS, the age criterion was modified to 2 points for <2 years and 0 points for ≥2 years, while the other scoring criteria remain unchanged. A STEPSS cutoff score of 3 has been identified for predicting poor prognosis, with a sensitivity of 93% and specificity of 81%.21 The scoring system is detailed in Table 1.
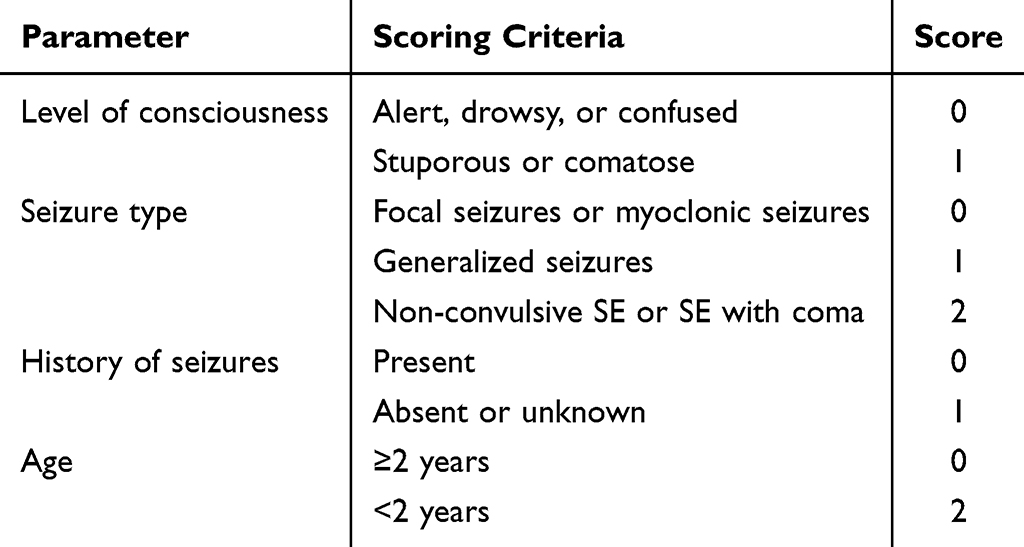 |
Table 1 STEPSS Score for Pediatric SE |
END-IT Score
The encephalitis, non-convulsive status epilepticus, diazepam resistance, imaging abnormalities, and END-IT score incorporates five key factors: presence of encephalitis, non-convulsive status epilepticus (NCSE), diazepam resistance, neuroimaging abnormalities, and the need for tracheal intubation. It is currently the only scoring system designed to predict functional recovery after hospital discharge in SE patients. Initially developed for long-term prognostic assessment in SE patients aged ≥12 years, the END-IT score ranges from 0 to 6, with a cutoff score of 3 for predicting poor outcomes.22 Some studies have extended its use to assess the short-term prognosis in pediatric SE patients, demonstrating good predictive value. For pediatric SE, a cutoff score of 2 has been identified for predicting poor prognosis, with a sensitivity of 73% and specificity of 94%.23 The scoring system is detailed in Table 2.
 |
Table 2 END-IT Score for Prognosis in Pediatric SE |
GOS Score
The GOS score is used to assess patient prognosis at 3 months post-onset or at the time of death. The scale consists of five levels: (1) Grade 5 (Good Recovery): The patient has mild or no sequelae, can resume normal social activities, and return to school; (2) Grade 4 (Moderate Disability): The patient has moderate sequelae but can live independently and work under supervision; (3) Grade 3 (Severe Disability): The patient has severe sequelae and is unable to live independently; (4) Grade 2 (Vegetative State): The patient exhibits minimal responses and lacks meaningful interaction with the environment; (5) Grade 1 (Death): The patient has died. A GOS score of 1 to 4 is classified as a poor prognosis, whereas a score of 5 indicates a favorable prognosis.
Statistical methods
Statistical analyses were performed using SPSS 26.0 software. Continuous variables following a normal distribution were expressed as mean ± standard deviation ( ), while categorical variables were presented as frequency and percentage [n (%)]. The t-test was used for comparisons between groups, and categorical data were analyzed using the χ²-test. For non-normally distributed data, the median and interquartile range [M (Q1, Q3)] were reported, and comparisons were conducted using non-parametric tests (rank-sum test). Binary logistic regression analysis was applied to identify risk factors for poor prognosis in children with SE. The predictive value of the prognostic scoring systems for short-term outcomes was assessed using the receiver operating characteristic (ROC) curve. A P-value < 0.05 was considered statistically significant.
), while categorical variables were presented as frequency and percentage [n (%)]. The t-test was used for comparisons between groups, and categorical data were analyzed using the χ²-test. For non-normally distributed data, the median and interquartile range [M (Q1, Q3)] were reported, and comparisons were conducted using non-parametric tests (rank-sum test). Binary logistic regression analysis was applied to identify risk factors for poor prognosis in children with SE. The predictive value of the prognostic scoring systems for short-term outcomes was assessed using the receiver operating characteristic (ROC) curve. A P-value < 0.05 was considered statistically significant.
Result
Characteristics
General characteristics
From January 2020 to December 2024, a total of 203 pediatric patients meeting the inclusion and exclusion criteria were admitted to the PICU of our hospital. The annual distribution was as follows: 44 cases in 2020, 50 cases in 2021, 25 cases in 2022, 44 cases in 2023, and 40 cases in 2024. Except for the lower number of cases in 2022, the number of admissions remained relatively stable across the other years.
During the follow-up period, only one patient among the 203 patients gave up treatment due to epidemic encephalitis B and died after discharge. Based on the result of the GOS score at 3 months after discharge, the 203 patients were classified into a good prognosis group (139 cases, 68.5%) and a poor prognosis group (64 cases, 31.5%). The proportion of patients in the good prognosis group was significantly higher than in the poor prognosis group, with a statistically significant difference observed across all years. The detailed results are presented in Table 3.
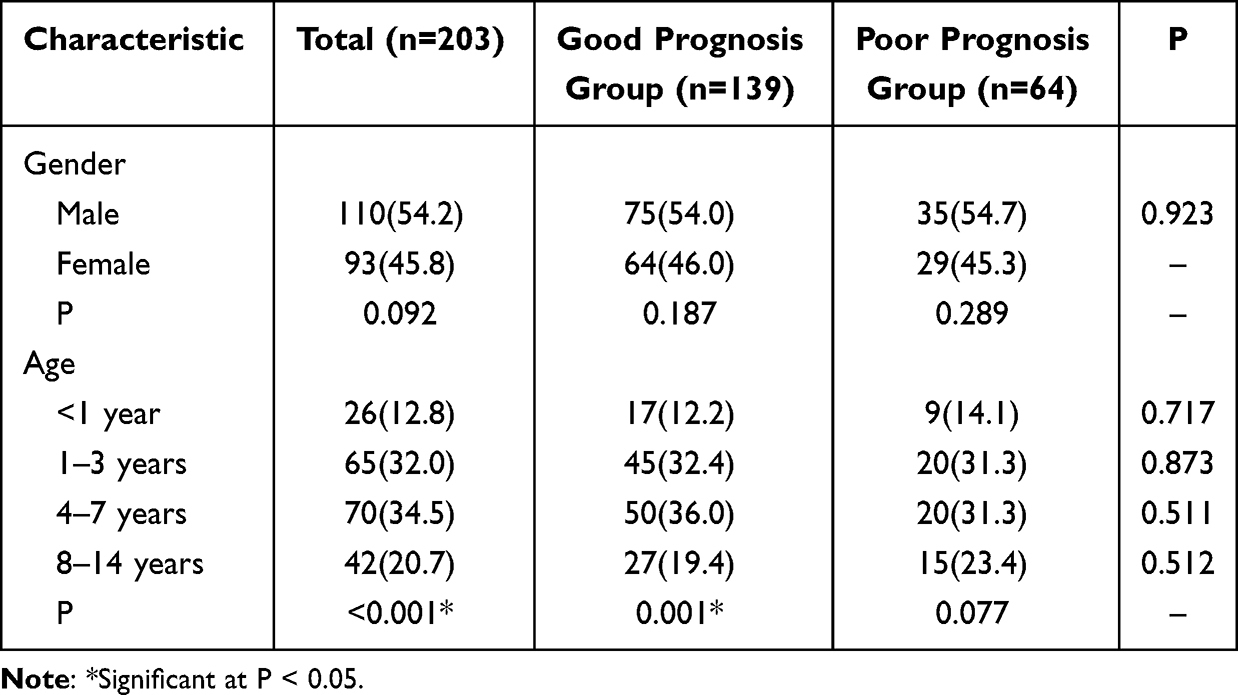 |
Table 3 General Characteristics of 203 Pediatric Patients, n (%) |
Gender Distribution
Among the 203 pediatric patients, 110 (54.2%) were male, including 75 cases (54.0%) in the good prognosis group and 35 cases (54.7%) in the poor prognosis group. The remaining 93 patients (45.8%) were female, with 64 cases (46.0%) in the good prognosis group and 29 cases (45.3%) in the poor prognosis group. There was no statistically significant difference in gender distribution between the two groups.
Except for the poor prognosis group in 2021 and 2024, where the proportion of female patients exceeded male patients, the male-to-female ratio remained higher in both groups across other years. Notably, the gender distribution in the poor prognosis group of 2023 showed a statistically significant difference.
Age Distribution
The median age of the 203 pediatric patients was [54.0 (22.0, 86.5)] months. In the good prognosis group, the median age was [54.0 (24.5, 85.5)] months, while in the poor prognosis group, it was [56.0 (19.8, 86.3)] months. There was no statistically significant difference in age distribution between the two groups.
The age distribution of the 203 patients showed that the largest proportion belonged to the 4–7 years age group, accounting for 34.5% of the total cases. This was followed closely by the 1–3 years group, which comprised 32.0% of the patients. The 8–14 years age group represented 20.7% of the cases, while the smallest proportion was observed in patients under 1 year of age, making up 12.8% of the total.
The age distribution in both the good prognosis and poor prognosis groups was consistent with the overall distribution, and no statistically significant differences were observed across age groups.
Clinical Data
Etiology Distribution
The 203 pediatric patients were categorized into primary epilepsy and epilepsy combined with other diseases based on etiology. The proportion of patients with epilepsy combined with other diseases (139 cases, 68.5%) was significantly higher than that of patients with primary epilepsy (64 cases, 31.5%), with a statistically significant difference (P < 0.05). The etiology distribution in both the good prognosis and poor prognosis groups was consistent with the overall distribution. However, the proportion of patients with primary epilepsy was significantly higher in the good prognosis group, while the proportion of patients with combined diseases was significantly higher in the poor prognosis group, and this difference was statistically significant (P < 0.05).
Seizure Type
The 203 pediatric patients were classified into generalized seizures and focal seizures based on the type of seizure. The proportion of patients with generalized seizures (126 cases, 62.1%) was significantly higher than those with focal seizures (77 cases, 37.9%), with a statistically significant difference (P < 0.05). The distribution of seizure types in both the good prognosis and poor prognosis groups was consistent with the overall distribution, and there was no statistically significant difference in seizure type distribution between the two groups.
History of Previous Seizures
The 203 pediatric patients were categorized based on whether they had a history of seizures. The proportion of patients with a history of seizures (140 cases, 69.0%) was significantly higher than those without a history of seizures (63 cases, 31.0%), with a statistically significant difference (P < 0.05). The history of seizures in both the good prognosis and poor prognosis groups was consistent with the overall distribution, and there was no statistically significant difference between the two groups regarding the history of seizures.
Presence of Encephalitis
Among the 203 pediatric patients, the proportion of those without encephalitis (178 cases, 87.7%) was significantly higher than those with encephalitis (25 cases, 12.3%), with a statistically significant difference (P < 0.05). The presence of encephalitis in both the good prognosis and poor prognosis groups was consistent with the overall situation, and there was no statistically significant difference between the two groups in terms of the presence of encephalitis.
Use of Mechanical Ventilation
Among the 203 pediatric patients, only 10 cases (4.9%) required mechanical ventilation during treatment. This included 5 cases (50.0%) in the good prognosis group and 5 cases (50.0%) in the poor prognosis group. The proportion of patients requiring mechanical ventilation was higher in the poor prognosis group (7.8%) compared to the good prognosis group (3.6%), but the difference was not statistically significant.
The distribution of mechanical ventilation use in the good and poor prognosis groups was consistent with the overall trend, and there was no statistically significant difference between the two groups regarding the need for mechanical ventilation.
The results of etiology, seizure type, history of previous seizures, the presence of encephalitis and the use of mechanical ventilation are presented in Table 4.
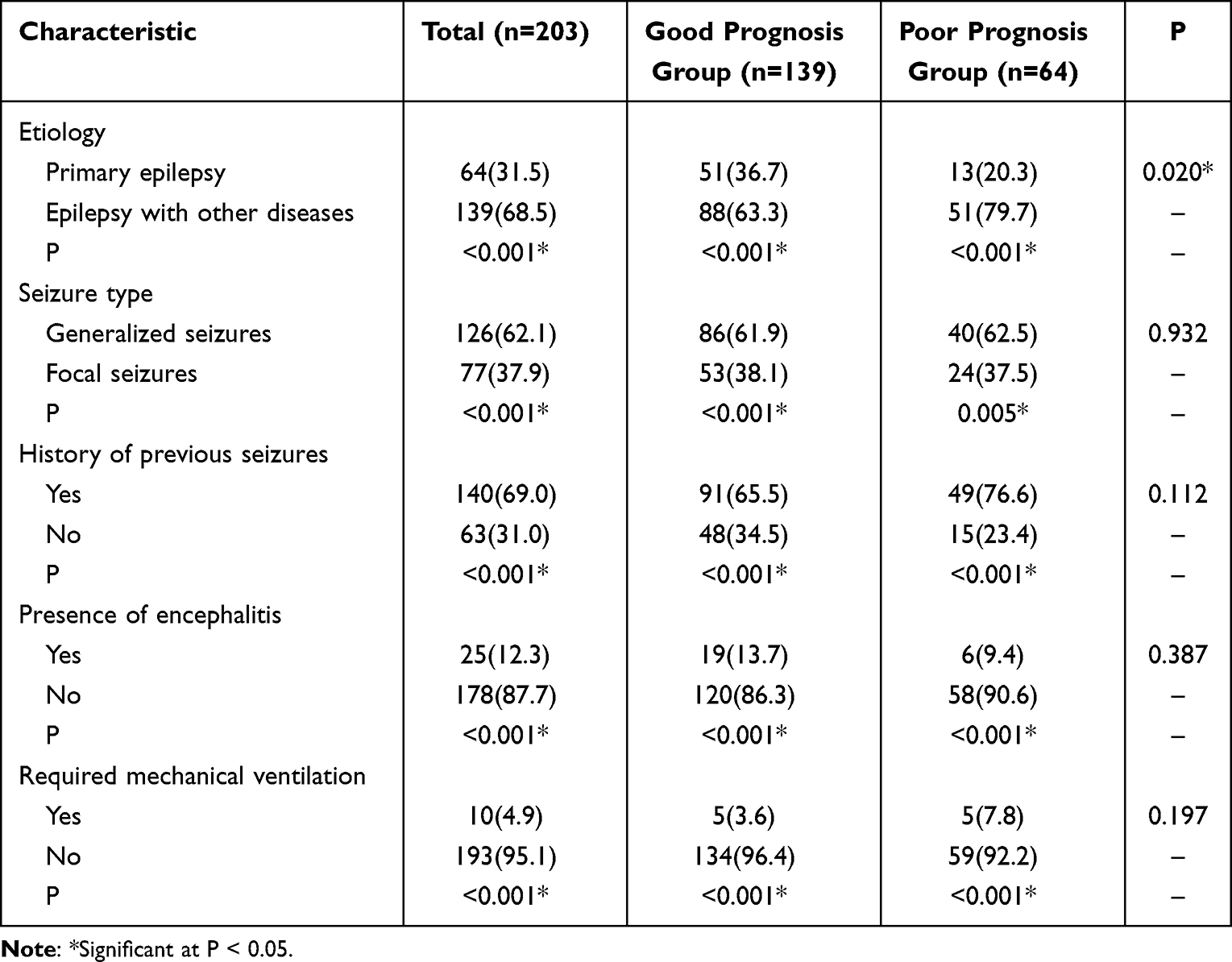 |
Table 4 Clinical Data of 203 Pediatric Patients, n (%) |
Length of Hospital Stay
The median length of hospital stay for the 203 pediatric patients was [10.0 (7.0, 14.0)] days. In the good prognosis group, the median hospital stay was [9.0 (7.0, 13.0)] days, while in the poor prognosis group, it was [11.0 (7.0, 16.0)] days. Although the average hospital stay was longer in the poor prognosis group compared to the good prognosis group, the difference was not statistically significant.
Imaging and Laboratory Examinations
The diagnosis of epilepsy relies not only on the clinical manifestations of patients, but also on. auxiliary examinations such as brain MRI and EEG and laboratory examinations. EEG is known as the gold standard for epilepsy diagnosis, to determine the type of epileptic seizures and epilepsy syndrome. The results are presented in Table 5.
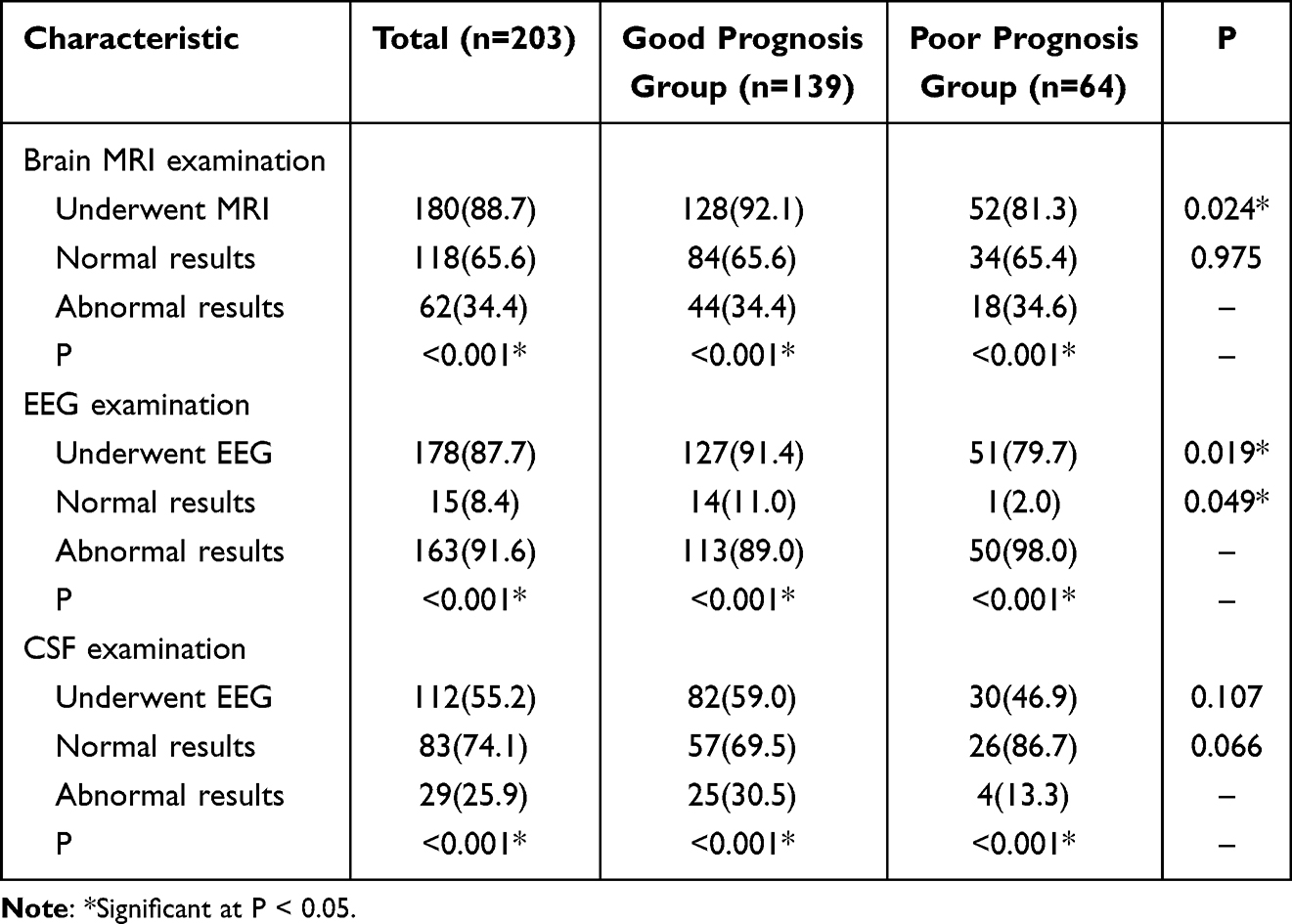 |
Table 5 Imaging and Laboratory Examination Results of 203 Pediatric Patients, n (%) |
Brain MRI Examination
Among the 203 pediatric patients, 180 (88.7%) underwent brain MRI, including 128 cases (71.1%) in the good prognosis group and 52 cases (28.9%) in the poor prognosis group. The proportion of patients who underwent MRI was significantly higher in the good prognosis group (92.1%) than in the poor prognosis group (81.3%), with a statistically significant difference.
Regarding MRI results, the proportion of patients with normal findings (65.6%) was significantly higher than those with abnormal findings (34.4%). The distribution of MRI results in the good prognosis and poor prognosis groups was consistent with the overall trend, and there was no statistically significant difference between the two groups in terms of normal versus abnormal findings.
EEG Examination
Among the 203 pediatric patients, 178 (87.7%) underwent EEG, including 127 cases (71.3%) in the good prognosis group and 51 cases (28.7%) in the poor prognosis group. The proportion of patients who underwent EEG was significantly higher in the good prognosis group (91.4%) than in the poor prognosis group (79.7%), with a statistically significant difference.
The proportion of patients with abnormal EEG findings (91.6%) was significantly higher than those with normal EEG findings (8.4%). Among them, the EEG of patients with epilepsy mostly showed focal spikes, sharp waves or slow waves, and the abnormal EEG wave was more obvious in patients with abnormal intracranial structure. However, the EEG of epilepsy status caused by intracranial infection and septic encephalopathy are common with focal or diffuse slow wave, and EEG degree of abnormality was positively correlated with the seriousness of disease and abnormalities of craniocerebral magnetic resonance. The distribution of EEG results in the good prognosis and poor prognosis groups was consistent with the overall trend. However, the proportion of patients with abnormal EEG findings was significantly higher in the poor prognosis group (98.0%) compared to the good prognosis group (89.0%), and this difference was statistically significant (P < 0.05), which is consistent with the conclusion that EEG is the gold standard for the diagnosis of epilepsy.
CSF Examination
Among the 203 pediatric patients, 112 (55.2%) underwent CSF examination, including 82 cases (73.2%) in the good prognosis group and 30 cases (26.8%) in the poor prognosis group. The proportion of patients who underwent CSF examination was higher in the good prognosis group (59.0%) than in the poor prognosis group (46.9%), but the difference was not statistically significant.
Regarding CSF results, the proportion of patients with normal findings (74.1%) was significantly higher than those with abnormal findings (25.9%). The distribution of CSF examination results in the good prognosis and poor prognosis groups was consistent with the overall trend, and there was no statistically significant difference between the two groups in terms of normal versus abnormal findings.
Types of Antiepileptic Drugs
For children with SE, first-line drugs such as diazepam or midazolam are preferred for intravenous infusion. When first-line drug treatment fails, second-line drugs such as sodium valproate or levetiracetam can be chosen for subsequent intravenous infusion. For the treatment of RSE, midazolam or propofol anesthesia is the preferred choice, and regardless of whether it is difficult to treat or not, second-line and third line drugs need to be prepared. The 203 pediatric patients were categorized based on the number of ASMs used during treatment into three groups: those receiving a single drug, those receiving two drugs, and those receiving three or more drugs. Among them, the majority of patients were treated with a single drug (106 cases, 52.2%), followed by those receiving three or more drugs (57 cases, 28.1%) and those receiving two drugs (40 cases, 19.7%), with a statistically significant difference (P < 0.05).
In the good prognosis group, the highest proportion of patients received a single drug (95 cases, 68.3%), followed by those receiving two drugs (24 cases, 17.3%) and those receiving three or more drugs (20 cases, 14.4%), with a statistically significant difference (P < 0.05). In contrast, in the poor prognosis group, the highest proportion of patients received three or more drugs (37 cases, 57.8%), followed by those receiving two drugs (16 cases, 25.0%) and those receiving a single drug (11 cases, 17.2%), with a statistically significant difference (P < 0.05). The proportion of patients receiving two or three or more drugs was significantly higher in the poor prognosis group compared to the good prognosis group, while the proportion of patients receiving a single drug was significantly higher in the good prognosis group than in the poor prognosis group. These differences were statistically significant (P < 0.05). The results are presented in Table 6.
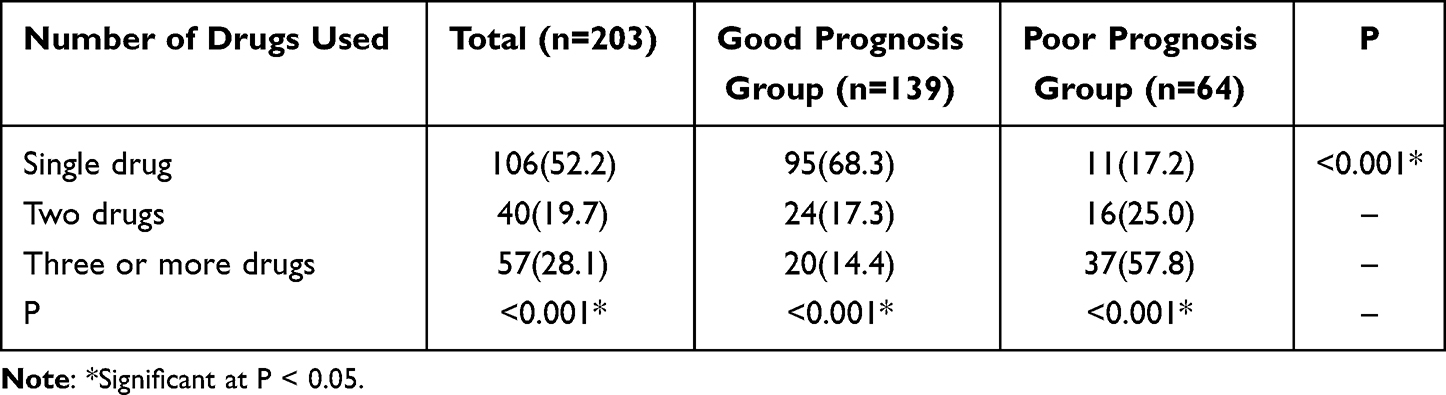 |
Table 6 Types of Antiepileptic Drugs Used in 203 Pediatric Patients, n (%) |
Prognostic Scores
The prognostic assessment included the STEPSS score and the END-IT score. The median STEPSS score for the 203 pediatric patients was [1.0 (1.0, 2.0)]. The median score was [1.0 (1.0, 2.0)] in the good prognosis group and [1.0 (1.0, 2.3)] in the poor prognosis group. There was no statistically significant difference in STESS scores between the two groups. The median END-IT score for the 203 pediatric patients was [1.0 (1.0, 2.0)]. The median score was [1.0 (1.0, 3.0)] in the good prognosis group and [1.0 (1.0, 2.0)] in the poor prognosis group. No statistically significant difference was observed in END-IT scores between the two groups.
Analysis of Prognostic Factors
Univariate Analysis
A univariate analysis was conducted on general characteristics, clinical data, medication usage, and prognostic scores between the two groups. The results showed that compared with the good prognosis group, the poor prognosis group had a significantly higher proportion of patients with comorbid diseases (P = 0.020) and abnormal EEG findings (P = 0.049). Additionally, the proportion of patients receiving two or more ASMs was significantly higher in the poor prognosis group (P < 0.001). Although the length of hospital stay was longer in the poor prognosis group, the difference was not statistically significant (P = 0.087).
Logistic Multivariate Analysis
A binary logistic regression analysis was performed, using prognostic outcomes as the dependent variable and the significant clinical indicators from the univariate analysis (presence of comorbid diseases, EEG findings, and medication usage) as independent variables. The forward stepwise LR method was applied to identify statistically significant predictors. The results indicated that the number of antiepileptic drugs used was a risk factor affecting prognosis. Compared with the good prognosis group, patients in the poor prognosis group were 4.48 times more likely to be treated with two or more ASMs than with a single drug, with a 95% confidence interval (CI) of 2.223–9.029. Detailed results are presented in Table 7.
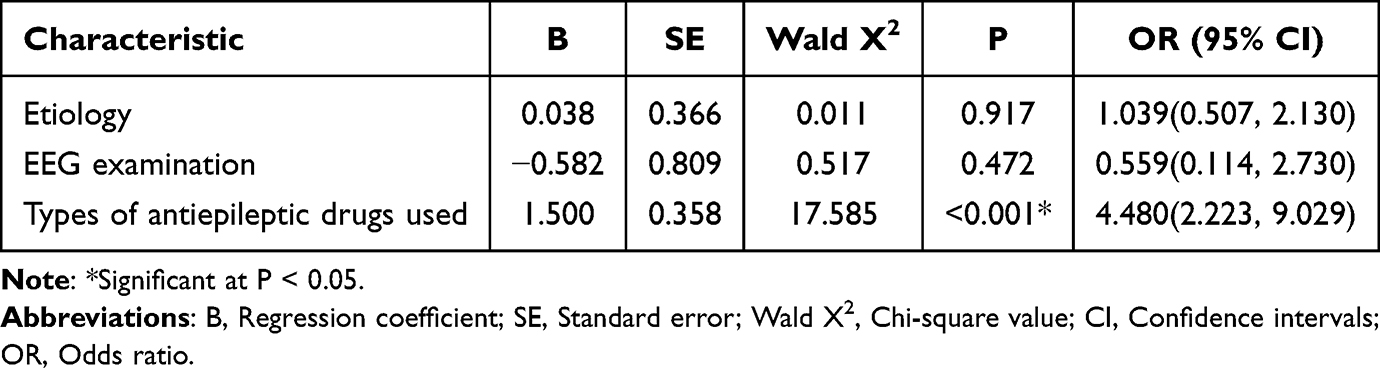 |
Table 7 Analysis of Risk Factors for Poor Prognosis in Pediatric Patients |
Comparison of the Prognostic Predictive Value of the STEPSS and END-IT Scoring Systems
ROC curves were plotted for STEPSS and END-IT scores to evaluate their predictive value for prognosis. The area under the curve (AUC) was 0.475 (P = 0.570) for STEPSS and 0.535 (P = 0.419) for END-IT, suggesting that both scoring systems have limited reference value in predicting prognosis. The ROC curve is shown in Figure 1.
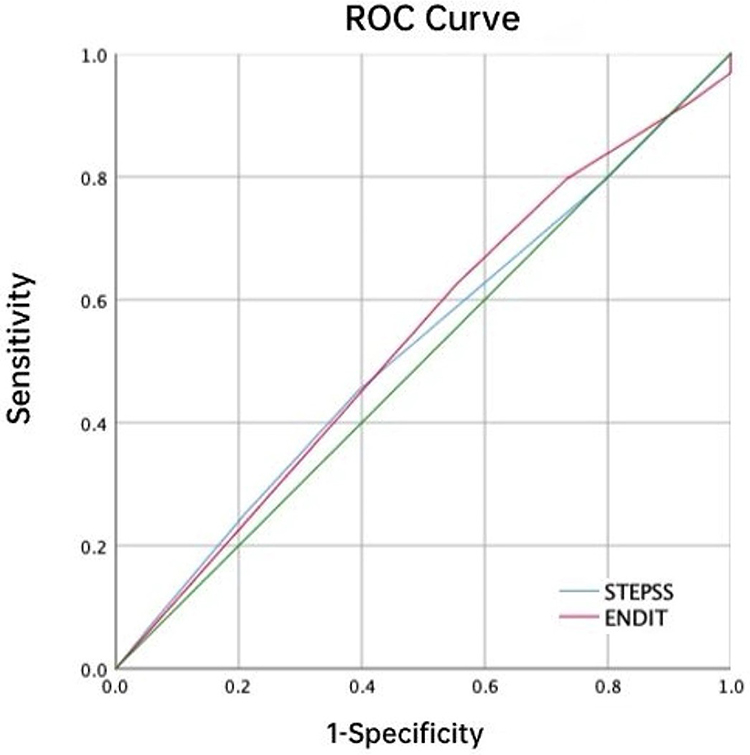 |
Figure 1 The ROC Curve of for STEPSS and END-IT scores. |
Discussion
Status epilepticus, one of the most critical conditions commonly encountered in PICU, affects approximately 3 to 42 per 100,000 children annually.24 The overall mortality rate of SE remains high, making early identification of risk factors for poor prognosis essential in reducing the rates of disability and mortality among affected patients.25 Several factors, including patient age, underlying etiology, seizure type, duration of convulsions, use of mechanical ventilation, imaging abnormalities, and developmental delays, have been associated with SE prognosis.26 Therefore, investigating prognostic factors for SE and utilizing them to predict unfavorable outcomes for early intervention is crucial for achieving prompt seizure control and improving treatment efficacy. In addition, this study introduces the STEPSS and END-IT scoring systems to assess their diagnostic value in predicting poor prognosis in pediatric SE patients.
A total of 203 pediatric patients with SE were included in this study, divided into good prognosis group and poor prognosis group. The demographic characteristics (age and gender distribution), clinical data, imaging and laboratory results, and the number of ASMs used were compared between the two groups to investigate the factors affecting the prognosis of children with SE, to evaluate the prognostic value of STEPSS and END-IT score. The results demonstrated that comorbidities, abnormal EEG findings, and the use of multiple ASMs were significantly associated with poor prognosis. Logistic regression analysis further identified the use of multiple ASMs as an independent risk factor for adverse outcomes, with patients receiving two or more ASMs being 4.48 times more likely to have a poor prognosis than other patients. Additionally, this study found that the STEPSS and END-IT scoring systems have limited predictive value for poor prognosis.
In DRE patients, comorbidities can lead to a deterioration in quality of life, exacerbate the severity of epilepsy, and worsen the prognosis of epilepsy.27 Some studies have demonstrated that patients diagnosed with a co-occurrence of epilepsy and psychiatric disorders are more likely to present refractory seizures and the probability of seizure remission after pharmacotherapy is reduced. The pathogenic mechanisms may include endocrine disorders, neuroinflammatory processes, neurotransmitter disturbances, and stress- triggered mechanisms.28 In our study, comorbidities were significantly associated with poor prognosis, which may be attributed to the fact that patients in the PICU often present with multiple underlying conditions, leading to more complex clinical scenarios. In children with epilepsy, the most prevalent comorbidities include attention-deficit hyperactivity disorder, mood and anxiety disorders, and autism spectrum disorder.29 In addition, although the number of children with comorbid mental illness is smaller than that of adults, the incidence of depression in adolescent children increases with the increase of children’s learning pressure,30 and for pediatric SE patients with depression may cause poor prognosis of the situation deserves the attention of clinicians.
Early diagnostic evaluations, including EEG monitoring, cranial CT or MRI, and cerebrospinal fluid examination, are crucial in guiding targeted therapy. Previous studies have identified younger age, abnormal brain MRI findings, and the need for endotracheal intubation as risk factors for poor prognosis in children with SE.31 Our findings further revealed that abnormal EEG results were significantly associated with poor prognosis. For PICU patients, bedside EEG monitoring may be beneficial, as seizure termination should not only be assessed clinically but also confirmed by the cessation of epileptic discharges on EEG. Continuous EEG monitoring has been shown to be valuable in assessing brain function prognosis in SE patients, and prolonged exposure to epileptic activity is associated with adverse neurobehavioral outcomes.32 Therefore, we recommend the routine implementation of bedside EEG monitoring in PICU patients with SE. When necessary, continuous bedside EEG should be considered as an adjunctive measure to guide treatment, minimize further brain injury, and improve long-term outcomes.33
ASMs are the most fundamental and primary treatment option for epilepsy, serving as the first-line therapy.13 Aggressive treatment has been recommended for SE, indeed the risk of poor prognosis and even death appears to be higher if treatment is delayed. Several studies evaluated the possible role of SE duration as an unfavorable prognostic factor. Longer duration appears to be associated with higher mortality. Evidence suggests that SE lasting more than 30 min is less likely to terminate spontaneously and is associated with a higher mortality than SE lasting less than 30 min.34 However, NORSE can be associated with significant recovery even after prolonged duration of SE. Meanwhile, studies have also confirmed that the development of epilepsy is associated with a higher number of ASM.35 Therefore, in children with SE, early and adequate administration of ASMs is critical. When initial treatment fails, timely initiation of combination therapy and early implementation of anesthetic protocols are essential to prevent RSE and improve patient outcomes.36 Our study supports this perspective, as the proportion of patients receiving polytherapy was significantly higher in the poor prognosis group. Furthermore, regression analysis also confirmed that the use of multiple ASMs is an independent risk factor for poor prognosis.
The STESS assesses patient prognosis based on four factors: consciousness level, seizure type, history of previous seizures, and age. It has been widely used in adults and has demonstrated significant clinical utility.20 In 2019, researchers adapted STESS for pediatric use by setting the age threshold at two years, defining it as the STEPSS score. They identified a cutoff score of 3 for predicting poor prognosis, with a sensitivity of 93% and specificity of 81%.21 Subsequent studies have further explored the predictive value of STEPSS for poor outcomes.14 However, in our study, STEPSS did not demonstrate a significant distinction between the two groups. The END-IT score incorporates treatment factors and is currently used to predict post-discharge functional recovery in SE patients. Kapoor et al applied this score to assess the short-term prognosis of pediatric SE patients in India, identifying a cutoff value of 2 points for predicting poor outcomes, with a sensitivity of 73% and a specificity of 94%.23 In China, studies have also evaluated the END-IT score for short-term prognosis in pediatric SE patients, reporting an AUC above 0.7 and a predictive cutoff value of 1.5 points. However, the sensitivity was only 76.0%, and the specificity did not reach 80%, resulting in a relatively low positive predictive value. These findings suggest that the reliability of END-IT in predicting short-term poor outcomes in SE patients is limited. Our study results align with this conclusion but differ from some previously published literature.22,23 Further research is needed to confirm the underlying reasons for these discrepancies. Furthermore, ROC curve analysis suggested that STEPSS and END-IT had limited prognostic value in predicting outcomes in pediatric SE patients. For patients with fewer comorbidities, the EMSE, STESS, and mSTESS scores may help to predict the prognosis of SE patients, and prospective trials should be conducted to evaluate their utility in patients with a higher number of comorbidities, as well as in pediatric patients.37 On the other hand, machine learning approaches can be attempted by deeply mining the data, combining multiple clinical and imaging factors, and improving the quality of life, to achieve personalized application of antiepileptic drugs and improve the prognosis of epilepsy patients.38
This study has several limitations: (1) All the patients included in this study were from the PICU of our hospital, which makes the results specific to this institution and potentially less generalizable to other hospitals or regions. A multicenter study with broader geographical representation would provide more robust findings; (2) The study cohort included patients with various underlying comorbidities, in addition to primary epilepsy, which may have influenced the outcomes. The diverse clinical conditions of PICU patients introduce heterogeneity that could potentially confound the interpretation of results; (3) The sample size of 203 patients may limit the statistical power of the study. To increase the reliability and validity of the findings, future research should include a larger cohort of patients to strengthen the conclusions; (4) This study primarily focused on the short-term prognosis of SE patients, and did not assess long-term outcomes or the dynamic changes in treatment response over time. Long-term follow-up would provide valuable insights into the enduring effects of interventions and the overall recovery trajectory; (5) The study did not record detailed information regarding the treatment process and its dynamic changes throughout the course of illness. A more detailed tracking of the treatment interventions, including drug adjustments, could provide a clearer picture of the factors influencing prognosis; (6) Given the limited predictive value of STEPSS and END-IT used in our study, future research may consider changing the scoring tools or using machine learning models for further investigation. Future studies addressing these limitations will be essential to better understand the complex nature of status epilepticus in children and to refine treatment and prognostic models for better outcomes.
Conclusion
In this study, we identified key clinical factors influencing the prognosis of children with SE admitted to the PICU. We found that comorbid conditions, EEG abnormalities, and the use of multiple ASMs were significantly associated with poor outcomes. Specifically, the use of two or more ASMs was an independent risk factor for unfavorable prognosis. Therefore, for SE patients, it is crucial to inquire about their medical history in detail, complete imaging examinations as soon as possible and formulate a suitable antiepileptic drug treatment regimen, especially the early initiation of combination medication. However, the STEPSS and END-IT scoring systems demonstrated limited predictive value in this cohort. Despite the promising results from clinical trials, further research with larger sample sizes, multi-center participation, long-term follow-up, and dynamic tracking of treatment protocols is required to refine prognosis predictions and enhance patient care. This study contributes to the understanding of SE in pediatric critical care and provides valuable insights into the factors influencing outcomes, while highlighting areas for further investigation to optimize treatment strategies for better long-term recovery.
Data Sharing Statement
No datasets were generated or analysed during the current study.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of Declaration of Helsinki, and approved by the Ethics Committee of Children’s Hospital of Nanjing Medical University. The need for written informed consent was waived by the Ethics Committee of Children’s Hospital of Nanjing Medical University due to the retrospective design of the study. Furthermore, the data sources were medical records filed by patients after discharge. The data collection did not interfere with patient diagnosis or treatment, and the study data did not contain identifiable personal information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Pharmacy Research Project of Tianqing Hospital of Jiangsu Pharmaceutical Association (Q202111).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Chang L, Wang XS. Advances in epidemiological studies on epilepsy in China. J Int Neurol Neurosurg. 2012;39(2):161–164.
2. Li JL, Cao J. Intractable epilepsy caused by SZT2 gene mutation in 2 children. J Clin Pediatr. 2019;37(4):288–291.
3. Wang CX, Yang ZQ, Yang ZY, et al. Temporal-parietal-occipital disconnection surgery for the treatment of drug-resistant epilepsy. Chin J Neurosurg. 2019;35(3):273–276.
4. Lei WJ, Pan J. Correlation analysis of Toll-like receptor 3 content in peripheral blood with electroencephalogram parameters and neurotransmitter content in children with intractable epilepsy. J Hainan Med Univ. 2019;25(4):284–287.
5. Xu XK, Li JL, Chen C, et al. Surgical treatment for intractable epilepsy in infants. J Clin Pediatr Surg. 2019;18(5):409–412.
6. Gaínza-Lein M, Sánchez Fernández I, Jackson M, et al. Association of time to treatment with short-term outcomes for pediatric patients with refractory convulsive status epilepticus. JAMA Neurol. 2018;75(4):410–418. doi:10.1001/jamaneurol.2017.4382
7. Eriksson K, Metsäranta P, Huhtala H, et al. Treatment delay and the risk of prolonged status epilepticus. Neurology. 2005;65(8):
8. Hirsch LJ, Gaspard N, van Baalen A, et al. Proposed consensus definitions for new‑onset refractory status epilepticus (NORSE), febrile infection‑related epilepsy syndrome (FIRES), and related conditions. Epilepsia. 2018;59(4):
9. Mayer SA, Claassen J, Lokin J, et al. Refractory status epilepticus: frequency, risk factors, and impact on outcome. Arch Neurol. 2002;59(2):
10. Kellinghaus C, Stögbauer F. Treatment of status epilepticus in a large community hospital. Epilepsy Behav. 2012;23(3):
11. Lowenstein DH, Bleck T, Macdonald RL. It’s time to revise the definition of status epilepticus. Epilepsia. 1999;40(1):
12. Su YY. Treatment strategies for refractory status epilepticus. Chin Neurol. 2015;48(3):161–163.
13. Chinese Society of Neurology, Chinese Society of Electroencephalography and Epilepsy. Chinese consensus for the anti‑seizure medications polytherapy. Chin J Neurol. 2024;57(2):108–117.
14. Zhang QQ, Liu LZ, Su J, et al. Analysis of the predictive value of serum Nesfatin-1 combined with the Status Epilepticus Severity Score in the short-term prognosis of children with status epilepticus. Chin J Appl Clin Pediatr. 2022;37(9):687–691.
15. Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus: report of the ILAE task force on classification of status epilepticus. Epilepsia. 2015;56(10):1515–1523. doi:10.1111/epi.13121
16. Samanta D, Garrity L, Arya R. Refractory and super-refractory status epilepticus. Indian Pediatr. 2020;57(3):239–253. doi:10.1007/s13312-020-1759-0
17. Wang XF, Li SC. Refractory Status Epilepticus: Diagnosis and Treatment. Singapore: Springer; 2017.
18. Dono F, Nucera B, Lanzone J, et al. Status epilepticus and COVID-19: a systematic review. Epilepsy Behav. 2021;118:107887. doi:10.1016/j.yebeh.2021.107887
19. Specchio N, Pietrafusa N. New-onset refractory status epilepticus and febrile infection-related epilepsy syndrome. Dev Med Child Neurol. 2020;62(8):897–905. doi:10.1111/dmcn.14553
20. Huang TH, Lai MC, Chen YS, et al. Status epilepticus mortality risk factors and a correlation survey with the newly modified STESS. Healthcare. 2021;9(11):1570. doi:10.3390/healthcare9111570
21. Sidharth SS, Jain P, Jain P, et al. Status epilepticus in pediatric patients severity score (STEPSS): a clinical score to predict the outcome of status epilepticus in children--a prospective cohort study. Seizure. 2019;71:328–332. doi:10.1016/j.seizure.2019.09.005
22. Gao Q, Ou-Yang TP, Sun XL, et al. Prediction of functional outcome in patients with convulsive status epilepticus: The END-IT score. Crit Care. 2016;25(20):46. doi:10.1186/s13054-016-1221-9
23. Kapoor D, Sidharth GD, Garg D, et al. Utility of the END-IT score to predict the outcome of childhood status epilepticus: A retrospective cohort study. Ann Indian Acad Neurol. 2021;24(3):390–395. doi:10.4103/aian.AIAN_1319_20
24. Zimmern V, Korff C. Status epilepticus in children. J Clin Neurophysiol. 2020;37(5):429–433. doi:10.1097/WNP.0000000000000657
25. Kannan L, Rathore C. Predicting the unpredictable: utility of outcome prediction scores in status epilepticus. Ann Indian Acad Neurol. 2021;24(3):313–314. doi:10.4103/aian.AIAN_220_21
26. Zhan Y, Hu Y. A QUIPS analysis of related factors of poor outcome in children with convulsive status epilepticus. J Epilepsy. 2021;7(2):112–121.
27. Mazarati A, Jones NC, Galanopoulou AS, et al. A companion to the preclinical common data elements on neurobehavioral comorbidities of epilepsy: a report of the TASK3 behavior working group of the ILAE/AES joint translational task force. Epilepsia Open. 2018;3:24–52. doi:10.1002/epi4.12236
28. Nogueira MH, Yasuda CL, Coan AC, et al. Concurrent mood and anxiety disorders are associated with pharmacoresistant seizures in patients with MTLE. Epilepsia. 2017;58:1268–1276. doi:10.1111/epi.13781
29. Hamiwka L, Jones JE, Salpekar J, et al. Child psychiatry. Epilepsy Behav. 2011;22(1):38–46. doi:10.1016/j.yebeh.2011.02.013
30. Xue CL, Zeng JX, Li WJ. Clinical characteristics and toxicological spectrum analysis of 493 cases of acute poisoning in children. BMC Emerg Med. 2024;24(1):181. doi:10.1186/s12873-024-01091-x
31. Chen ZZ, Jiang QN, Zhang XY, et al. Predictive values of the status epilepticus in pediatric patient severity score and END-IT score for short-term prognosis of children with status epilepticus. Chin J Appl Clin Pediatr. 2023;38(8):575–579.
32. Jin M, Sun SZ, Chen L, et al. Electroencephalogram characteristic and brain function prognosis in children with status epilepticus. J Clin Pediatr. 2020;38(3):161–165.
33. Zhao CG, Zhang LN. Application of continuous electroencephalography monitoring in patients with severe brain injuries. Chin J Pract Internal Med. 2019;39(12):1020–1025.
34. Leitinger M, Trinka E, Giovannini G, et al. Epidemiology of status epilepticus in adults: a population-based study on incidence, causes, and outcomes. Epilepsia. 2019;60(1):53–62. doi:10.1111/epi.14607
35. Sharath A, Ravindranadh CM, Ajay A, et al. New onset status epilepticus and its long-term outcome: a cohort study. Epilepsy Res. 2024;206:107442. doi:10.1016/j.eplepsyres.2024.107442
36. Shen KL, Zhu ZH, Qian SY, et al. Pediatric Specialist Standardized Training Textbook: Critical Care Medicine Volume. Beijing: People’s Medical Publishing House; 2018:82–83.
37. Yechoor N, Adeli A, Hafeez S. External validation of the epidemiology-based mortality score in status epilepticus in an American intensive care population. Epilepsy Res. 2018;148:32–36. doi:10.1016/j.eplepsyres.2018.10.001
38. Dong ZY, Yu Y, Yang Y, et al. The progress of the application of machine learning in epilepsy. Chin J Neurol. 2024;57(2):185–191.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.