Back to Journals » International Journal of Women's Health » Volume 18
The Impact of Cleavage and Blastocyst Stage Sequential Transfer on Clinical Pregnancy Outcomes of Frozen Embryo Transfer in Patients with Multiple Transplant Failures: A Retrospective Cohort Study
Authors Huang C ![]() , Liu J, Shen X, Mei J, Jiang Y, Zhang H, Kong N
, Liu J, Shen X, Mei J, Jiang Y, Zhang H, Kong N ![]()
Received 12 October 2025
Accepted for publication 27 February 2026
Published 8 March 2026 Volume 2026:18 573742
DOI https://doi.org/10.2147/IJWH.S573742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Chenyang Huang,1– 4,* Jingyu Liu,1– 4,* Xiaoyue Shen,1– 4 Jie Mei,1– 4 Yue Jiang,1– 4 Hui Zhang,1– 4 Na Kong1– 4
1Center for Reproductive Medicine and Obstetrics and Gynecology, Drum Tower Clinic Medical College of Nanjing Medical University, Nanjing, 210008, People’s Republic of China; 2Center for Reproductive Medicine and Obstetrics and Gynecology, Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School, Nanjing, 210008, People’s Republic of China; 3Center for Molecular Reproductive Medicine, Nanjing University, Nanjing, 210008, People’s Republic of China; 4State Key Laboratory of Reproductive Medicine and Offspring Health, Nanjing Medical University, Nanjing, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hui Zhang, Center for Reproductive Medicine and Obstetrics and Gynecology, Drum Tower Clinic Medical College of Nanjing Medical University, Nanjing, 210008, People’s Republic of China, Tel +8625-8310-6666-76208, Fax +8625-8310-7188, Email [email protected] Na Kong, Center for Reproductive Medicine and Obstetrics and Gynecology, Drum Tower Clinic Medical College of Nanjing Medical University, Nanjing, 210008, People’s Republic of China, Tel +8625-8310-6666-76208, Fax +8625-8310-7188, Email [email protected]
Background: To assess sequential embryo transfer’s impact on clinical outcomes in frozen embryo transfer (FET) cycles for patients with multiple transfer failures.
Methods: This retrospective cohort study encompasses 4,499 FET cycles involving double embryo transfers conducted at the Reproductive Medicine Center of Nanjing Drum Tower Hospital from 2020 to 2023. Group analyses were performed based on the type of transferred embryos (cleavage-stage embryos, blastocysts, and sequential embryo transfers) to assess the correlation between sequential transfers and clinical pregnancy rates, live birth rates, and multiple pregnancy rates. Subgroup analysis focused on patients with > 3 prior failures. Multivariate logistic regression adjusted for confounders.
Results: Sequential transfer did not improve clinical pregnancy (aOR = 0.94, 95% CI: 0.67– 1.32, p = 0.73) or live birth rates (aOR = 0.90, 95% CI: 0.65– 1.23, p = 0.49) versus blastocyst transfer, but significantly reduced multiple pregnancies (aOR = 0.50, 95% CI: 0.34– 0.75, p = 0.0008). Among patients with multiple failures, sequential transfer showed no significant association with clinical pregnancy (aOR = 0.57, 95% CI: 0.29– 1.11, p = 0.09) or live birth rates (aOR = 0.94, 95% CI: 0.49– 1.81, p = 0.85), yet significantly lowered multiple pregnancy odds (aOR = 0.30, 95% CI: 0.10– 0.90, p = 0.03).
Conclusion: Sequential embryo transfer does not enhance clinical pregnancy or live birth rates in FET cycles, regardless of prior failure history, but effectively reduces multiple pregnancy rates. For patients with > 3 embryo transfer failures, it yields live birth rates comparable to blastocyst transfer, representing a potentially advantageous option for this population.
Keywords: sequential embryo transfer, recurrent embryo transfer failure, frozen embryo transfer, live birth rate, multiple pregnancy rate
Background
Since 1978, assisted reproductive technology (ART) has made rapid advancements, benefiting many infertile couples.1 However, the current embryo implantation rate fluctuates between 25–50%,2–4 and many patients experience multiple embryo transfers without achieving their goal of childbirth. The repeated failures of embryo transfers impose psychological, physical, and financial stress on patients. This presents significant difficulties and challenges for clinicians and embryologists. Improving the clinical pregnancy outcomes for patients who have experienced multiple transfer failures poses a considerable challenge for both clinicians and embryologists.
Successful embryo implantation requires several essential conditions: high-quality embryos, a receptive endometrium, and good synchronization between the embryo and the endometrium.5 It is currently believed that abnormalities in endometrial receptivity are one of the main reasons for recurrent implantation failure (RIF).6 In vivo studies in mice have shown that embryos can induce improved endometrial receptivity.7 In recent years, sequential transfer protocols have gradually been applied to patients with recurrent transfer failures, where one cleavage-stage embryo is transferred first, followed by a blastocyst transfer after a certain interval. The first sequential transfer was performed by Abramovici et al in 1988, suggesting an increased probability of pregnancy.8 Some studies indicate that sequential embryo transfer does not improve clinical outcomes (live birth, miscarriages and multiple pregnancy) for RIF patients especially compared to blastocyst transfer,9–13 while other studies suggest that sequential embryo transfer may enhance clinical pregnancy and live birth rates compared to transfers on day 3 or day 5.14–16 Thus, the therapeutic effect of sequential embryo transfer remains controversial. Therefore, we conduct a retrospective study to analyze whether sequential transfer improves clinical pregnancy outcomes for patients with recurrent transfer failures at our reproductive medicine center.
Methods
Patients
This retrospective study included patients who underwent frozen-thawed embryo transfer (FET) at the Reproductive Medicine Center of Nanjing Drum Tower Hospital from January 2020 to July 2023. All patients received double embryo transfers and were categorized into three groups: those undergoing double cleavage-stage embryo transfer, those undergoing double blastocyst transfer and those undergoing sequential embryo transfer (Figure 1). The study encompassed all commonly utilized endometrial preparation protocols, including hormone replacement (HRT) cycles, modified natural cycles (mNC), mild stimulation cycles, and simple gonadotropin (Gn) cycles. Prior to initiating the FET cycle, all patients underwent a comprehensive preconception evaluation to identify and exclude any contraindications related to medication and pregnancy. The overall health status of the participants in this study was deemed normal. The exclusion criteria for this study were as follows: (1) self-administration of additional medications; (2) presence of hydrosalpinx, endometrial lesions, or abnormal uterine conditions (eg., uterine fibroids protruding into the uterine cavity, submucosal fibroids, or uterine adhesions); (3) moderate to severe endometriosis or adenomyosis; (4) patients with chromosomal karyotype abnormalities; and (5) patients who canceled the FET cycle for various reasons. All participants provided written informed consent for the utilization of their anonymized medical records for research purposes. This study received approval from the Ethics Committee of Nanjing Drum Towe Hospital (Approval No. 2021–384-01).
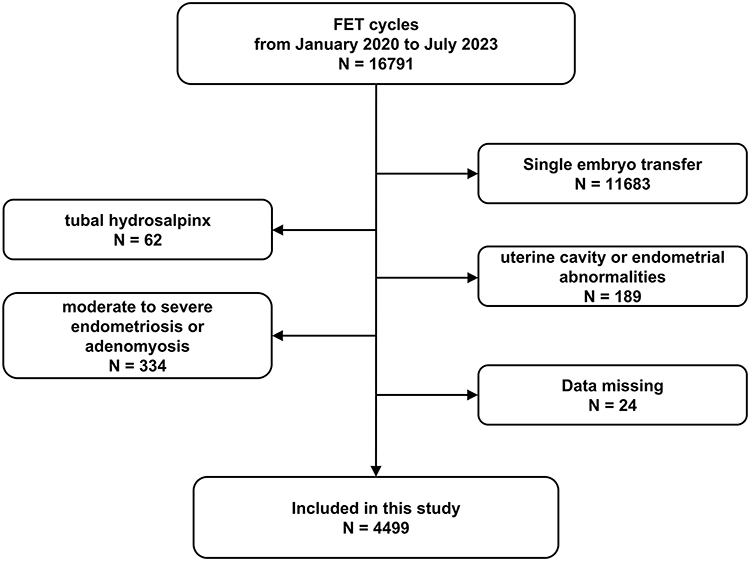 |
Figure 1 A flow chart of the inclusion and exclusion of patients. |
Endometrial Preparation and Thawed Embryo Transfer
The FET cycles for the patients in this study utilized several commonly employed endometrial preparation protocols at our center.
HRT: Patients commenced oral estradiol (Femoston, Abbott, USA) on the second day of their menstrual cycle, taking 2 mg three times daily for a duration of 14 days. Serum estradiol (E2) and progesterone (P) levels, along with endometrial thickness, were monitored throughout this period. At the appropriate time, oral estradiol was combined with dydrogesterone tablets (Femoston, 2 mg estradiol and 10 mg dydrogesterone, taken three times daily for 5 to 6 days), accompanied by a daily intramuscular injection of progesterone (60 mg) for 5 to 6 days to facilitate endometrial transformation. On the fifth day of this transformation, two cleavage-stage embryos were thawed and transferred. Alternatively, on the sixth day, two blastocysts were thawed and transferred. In cases of sequential transfer, one cleavage-stage embryo was thawed and transferred on the fifth day, followed by the thawing and transfer of one blastocyst two days later. Post-embryo transfer, patients continued with Femoston (2 mg estradiol and 10 mg dydrogesterone, three times daily) and a progesterone-releasing vaginal gel (90 mg daily) for luteal support.
mNC: Monitoring of serum E2, luteinizing hormone (LH), and P levels commenced on days 10 to 12 of the menstrual cycle, alongside ultrasound assessments of follicular development and endometrial growth. When the dominant follicle reached a diameter of at least 16 mm, human chorionic gonadotropin (hCG, Lizhu Pharmaceutical, 5000–10000 IU) was administered to induce ovulation. Dydrogesterone tablets (Duphaston, Abbott, 20 mg, taken twice daily for 4 to 6 days) were initiated the day following the hCG trigger to assist with endometrial transformation. Cleavage-stage embryos or blastocysts were thawed and transferred on the fifth and seventh days post-hCG trigger, respectively. Following embryo transfer, patients continued Duphaston (20 mg dydrogesterone, twice daily) for luteal support.
Mild-Stimulation Cycles: Beginning on the third day of the menstrual cycle, patients received ovulation induction medication (letrozole, 2.5 mg/day) for 5 consecutive days, with intermittent monitoring of serum E2, LH, and P levels, as well as ultrasound assessments of follicular and endometrial development. Based on follicular growth, human menopausal gonadotropin (HMG, Lizhu Pharmaceutical) was administered (75–300 IU/day). When the dominant follicle reached a diameter of at least 16 mm, hCG (5000–10000 IU) was utilized to induce ovulation. Dydrogesterone tablets (Duphaston, Abbott, 20 mg, taken twice daily for 4 to 6 days) were initiated the day after the hCG trigger to assist with endometrial transformation. Cleavage-stage embryos or blastocysts were thawed and transferred on the fifth and seventh days after the hCG trigger, respectively. Post-embryo transfer, patients continued Duphaston (20 mg dydrogesterone, twice daily) for luteal support.
Simple Gn Cycles: HMG injections began on the third day of the menstrual cycle at a starting dose of 75 IU/day, with subsequent adjustments to the HMG dosage (75–300 IU) based on the ovarian response, as indicated by changes in hormone levels and follicular development. The subsequent cycle arrangements mirrored those of the mild-stimulation protocol.
Twelve to fourteen days following embryo transfer, serum β-hCG levels were measured to ascertain biochemical pregnancy (> 20 IU/L). For patients with positive β-hCG results, transvaginal ultrasound was conducted 28 to 30 days post-embryo transfer to confirm clinical pregnancy and the number of implanted embryos. In cases of confirmed pregnancy, luteal support was maintained for an additional two months following transfer. Patients were continuously monitored for any abnormalities during the pregnancy.
Statistical Analysis
The primary outcome of this study was the live birth rate, while secondary outcomes included the clinical pregnancy rate, early miscarriage rate, and multiple pregnancy rate. Clinical pregnancy was defined as the presence of a gestational sac, while miscarriage occurring before 12 weeks of gestation was classified as early miscarriage. Live birth was defined as the delivery of at least one live newborn after 28 weeks of gestation, with the live birth rate calculated as the ratio of live birth cycles to the total number of embryo transfer cycles. The study population was stratified into three groups according to the embryo transfer methods employed: double cleavage-stage embryo transfer, blastocyst transfer, and sequential transfer. In the context of FET cycles, we evaluated the association between various transfer protocols and clinical pregnancy outcomes. A univariate analysis was first conducted to identify variables potentially associated with clinical pregnancy outcomes (Tables S1 and S2), which were selected as confounding variables requiring adjustment followed by a multivariable logistic regression analysis to assess the influence of sequential transfer on clinical outcomes within FET cycles. Additionally, subgroup analyses were performed to further elucidate the impact of the number of previous transfer failures on clinical pregnancy outcomes. Normality tests were conducted using the Kolmogorov–Smirnov test. For normally distributed variables, t-tests were utilized, while Mann–Whitney U-tests were applied to non-normally distributed variables. For categorical variables that met the criteria (theoretical frequency (T) > 5 and sample size (n) > 40), chi-square tests were performed. All variables were reported as mean ± standard deviation (SD). A two-sided α level of 0.05 was established for statistical significance. All statistical analyses were conducted using EmpowerStats (www.empowerstats.com, X&Y Solutions, Inc., Boston, MA) and R software version 3.6.0 (http://www.r-project.org).
Results
Characteristics of These 3 Groups According to Different Transferred Embryo Types
The study population was divided into three groups based on the type of embryo transfer: Group A, which received double cleavage-stage embryo transfers; Group B, which underwent double blastocyst transfers; and Group C, which experienced sequential embryo transfers (Table 1). Notably, couples in sequential embryo transfer Group exhibited a higher average age, a greater number of transfer cycles and thicker endometrium compared to those in double cleavage-stage embryo and blastocyst transfer Groups. Conversely, the Anti-Müllerian Hormone (AMH) levels in sequential embryo transfer Group were found to be lower. Double blastocyst transfer Group demonstrated the highest antral follicle count (AFC) and the lowest basal follicle-stimulating hormone (FSH) levels among the groups. There were no significant differences observed among the three groups concerning female body mass index (BMI), type of infertility, duration of infertility and endometrial preparation protocols. The clinical pregnancy rate in sequential embryo transfer Group was found to be higher than that in double cleavage-stage embryo transfer Group, yet lower than that in double blastocyst transfer Group, a trend that was also reflected in the live birth rates. The early miscarriage rate was similar in these three groups, while the multiple pregnancy rate was significantly lower in sequential embryo transfer Group compared to double cleavage-stage embryo and blastocyst transfer Groups.
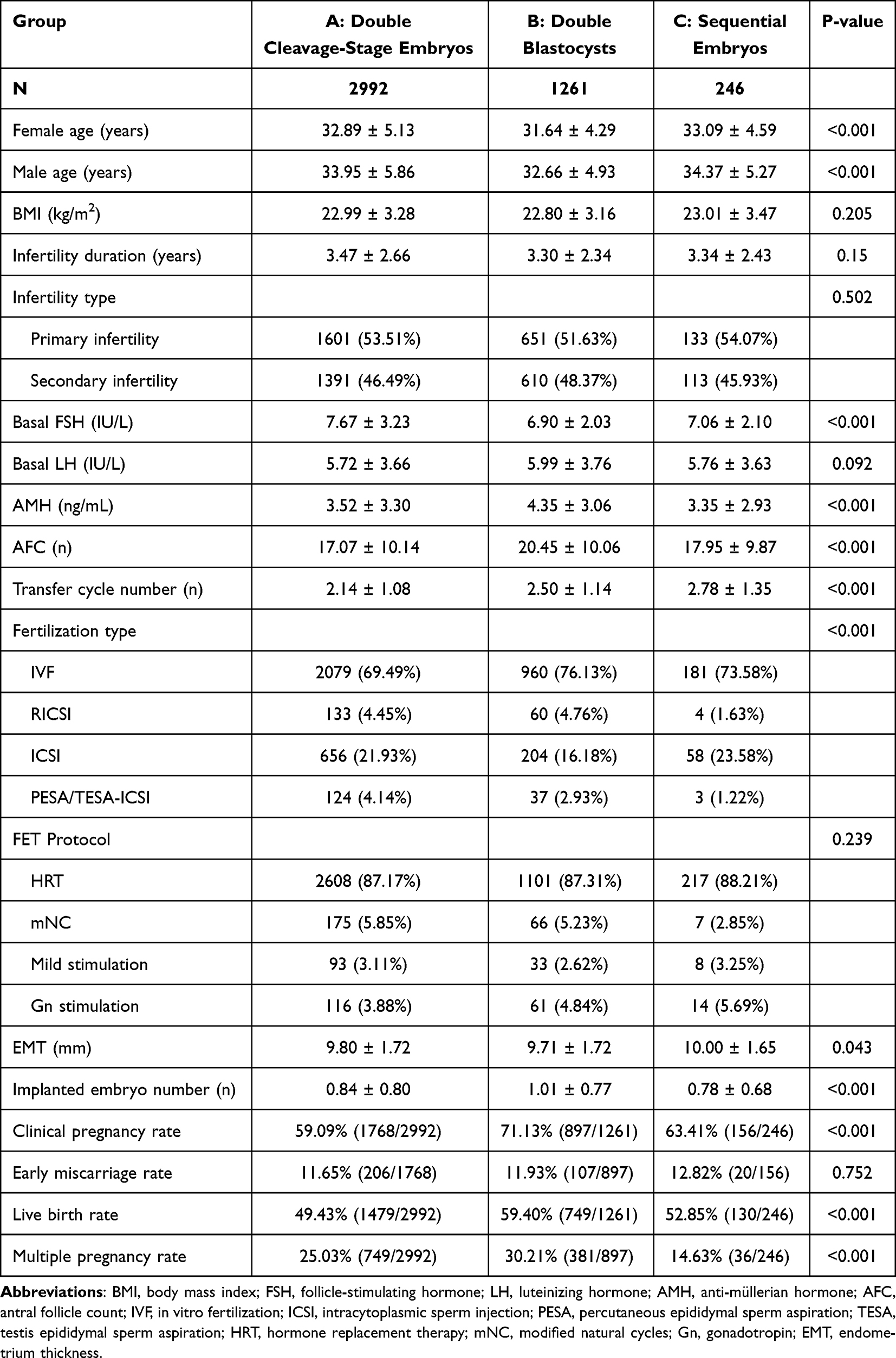 |
Table 1 Characteristics of FET Cycles According to Different Embryo Transfer Types |
Multivariate Regression Analysis for Clinical Outcomes Between Sequential Embryo Transfer and Double Blastocyst Transfer Groups
In this study, we aim to further investigate the differences between double blastocyst transfer and sequential embryo transfer. To facilitate this analysis, a preliminary univariate analysis was performed to identify potential confounding factors that may influence clinical pregnancy outcomes. Several variables were identified as confounders, including female age, male age, type of infertility, duration of infertility, baseline FSH, AMH, AFC, and the number of transfer cycles (Table S1). These variables were subsequently selected for adjustment in the multivariate regression analysis. The results indicate that sequential embryo transfer does not significantly adversely affect clinical pregnancy rates (Table 2, aRR = 0.983, 95% CI: 0.888–1.078, p = 0.358) or live birth rates (Table 2, aRR = 0.958, 95% CI: 0.842–1.078, p = 0.243). However, it is associated with a significant reduction in the likelihood of multiple pregnancies (Table 2, aOR = 0.505, 95% CI: 0.338–0.752, p < 0.001).
 |
Table 2 Multivariate Analysis for Sequential Embryos Transfer in FET Cycles Compared to Double Blastocysts Transfer Involved in the Clinical Pregnancy Rate, Live Birth Rate and Multiple Pregnancy Rate |
Characteristics of These 3 Subgroups Experienced Multiple Transfer Failures
Previous studies have indicated that sequential embryo transfer may enhance clinical pregnancy outcomes in patients experiencing recurrent implantation failure (RIF). In light of this, we performed additional subgroup analyses to investigate the impact of sequential embryo transfer on clinical pregnancy outcomes in patients with a history of more than three unsuccessful transfers. The patients were categorized into three groups based on the type of embryos transferred: Group D, which received double cleavage-stage embryo transfer; Group E, which underwent double blastocyst transfer; and Group F, which was assigned to sequential embryo transfer (Table 3). Notably, double blastocyst transfer Group exhibited the highest AFC and there were no statistically significant differences in other baseline characteristics among the three groups. The clinical pregnancy rate in sequential embryo transfer Group was found to be higher than that in double cleavage-stage embryo transfer Group, yet lower than that in double blastocyst transfer Group. Interestingly, the live birth rate in sequential embryo transfer Group was comparable to that in double blastocyst transfer Group, potentially due to a lower early miscarriage rate. Consistent with findings from all FET cycles, the multiple pregnancy rate in sequential embryo transfer Group was significantly lower than those in double cleavage-stage embryo and blastocyst transfer Groups.
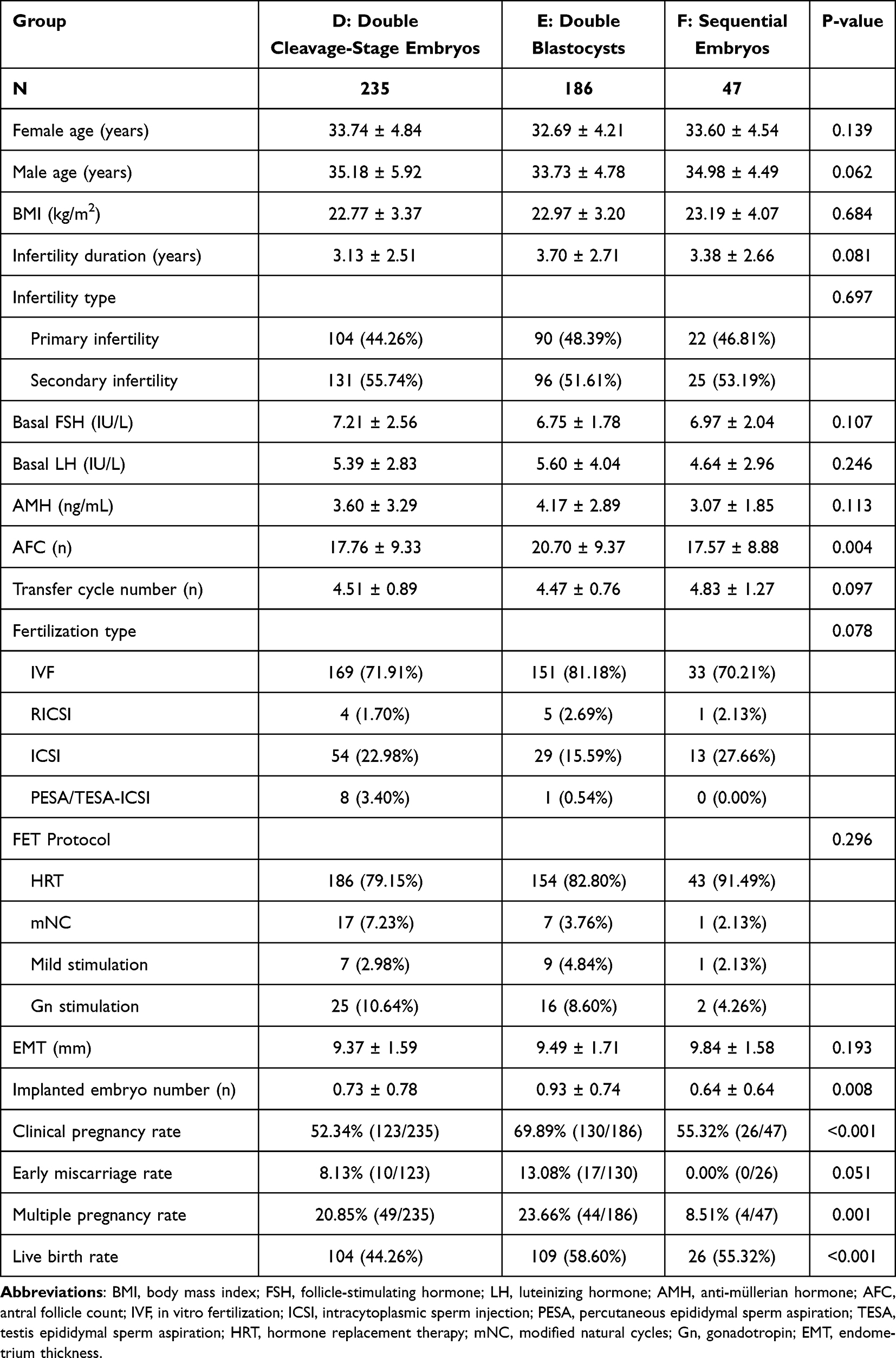 |
Table 3 Characteristics of FET Cycles with Previous Embryo Transfer Failures According to Different Embryo Transfer Types |
Multivariate Regression Analysis for Clinical Outcomes Between Sequential Embryo Transfer and Double Blastocyst Transfer Groups with Multiple Transfer Failures
In addition, we employed univariate analysis in conjunction with multivariate regression analysis to assess the impact of sequential embryo transfer on clinical pregnancy outcomes in patients with multiple failed transfers, relative to double blastocyst transfer. The univariate analysis identified several potential confounding factors that could influence clinical pregnancy outcomes, including female age and male age (Table S2). These factors were subsequently selected as adjustment variables for the multivariable regression analysis. The findings indicated that sequential embryo transfer did not demonstrate a significant association with clinical pregnancy rate (Table 4, aRR = 0.998, 95% CI: 0.967–1.029, p = 0.476) or live birth rate (Table 4, aRR = 0.999, 95% CI: 0.963–1.036, p = 0.499). However, it was found to significantly decrease the likelihood of multiple pregnancies (Table 4, aOR = 0.303, 95% CI: 0.103–0.895, p = 0.031).
 |
Table 4 Multivariate Analysis for Sequential Embryos Transfer in FET Cycles with Previous Transfer Failures Compared to Double Blastocysts Transfer Involved in the Clinical Pregnancy Rate, Live Birth Rate and Multiple Pregnancy Rate |
Discussion
Our retrospective study revealed that sequential embryo transfer does not significantly enhance clinical pregnancy rates or live birth rates among patients undergoing FET cycles. The clinical pregnancy rates associated with sequential embryo transfer were slightly higher than those observed with double cleavage-stage embryo transfer but lower than those seen with double blastocyst transfer. Furthermore, in patients with a history of multiple failed transfers, sequential embryo transfer also failed to improve clinical pregnancy rates, which remained significantly lower than those of patients undergoing double blastocyst transfer. Notably, however, the live birth rates in the sequential transfer group were comparable to those of the blastocyst transfer group. Additionally, we consistently observed that sequential embryo transfer significantly reduces the incidence of multiple pregnancies in FET patients, which may represent a key advantage of this approach.
Numerous studies have investigated sequential embryo transfer, with some suggesting that this approach can enhance clinical pregnancy outcomes for patients, which contrasts with our findings.15–19 The study results demonstrated that sequential embryo transfer significantly improved clinical pregnancy rates and ongoing pregnancy rates. Compared with blastocyst transfer, sequential embryo transfer did not achieve higher live birth rates. However, there were no statistically significant differences in multiple pregnancy rates or miscarriage rates. Notably, one study specifically examined fresh cycle transfer combined with thawed blastocyst transfer. In our centre, patients undergoing sequential embryo transfer typically experienced repeated transfer failures, and such individuals are generally not treated with the controlled hyperanovulation protocols that are acceptable for fresh embryo transfer. Furthermore, prospective study14 have suggested that sequential embryo transfer yields a higher clinical pregnancy rate than conventional day 5 FET. In this analysis, we observed that the clinical pregnancy rates for conventional FET patients were only 19% or 43%, whereas our clinical pregnancy rate for double blastocyst FET reached as high as 71.13%. This elevated clinical pregnancy rate may have obscured our ability to detect significant differences of sequential embryo transfer. Additionally, among patients who underwent more than three embryo transfer cycles in our study, the clinical pregnancy rate for double blastocyst FET remained as high as 69.89%, which does not correspond with the pregnancy probabilities typically associated with ESHRE recommended RIF patients (recommended threshold for the cumulative predicted chance of implantation to identify RIF for the purposes of initiating further investigation is 60%).20 Consequently, it is imperative to establish a personalized definition of RIF specific to our center. In future research, we can further investigate the potential benefits of sequential embryo transfer for populations that meet this tailored definition. Certainly, several studies have reported different findings that contrast with above results. A study indicates that women with poor ovarian response demonstrate higher clinical pregnancy rates and live birth rates when undergoing sequential embryo transfer compared to those receiving cleavage-stage embryo transfers, with no significant differences observed between sequential transfer and blastocyst transfer.21 Additionally, one study reported no statistically significant differences in clinical pregnancy rates and ongoing pregnancy rates among the sequential embryo transfer, blastocyst transfer, and cleavage-stage embryo transfer groups,9 although it noted a higher early miscarriage rate in the sequential transfer group. Another study suggests that sequential embryo transfer does not demonstrate better live birth rates or lower miscarriage rates compared to blastocyst transfer.13 Some studies even suggest that single and double blastocyst transfers exhibit higher implantation rates compared to sequential transfers.22 The results of our study align partially with these findings. We observed that the clinical pregnancy rates and live birth rates associated with sequential transfers in conventional FET cycles were lower than those for double blastocyst transfers. However, among patients with multiple failed transfers, the live birth rates for sequential transfers were comparable to those of double blastocyst transfers. In addition, the sequential transfer group is older than the other groups. This observation may represent a potential clinical advantage of the sequential transfer approach. We found that the early miscarriage rate for sequential transfers was lower, and there was a significant reduction in the rate of multiple pregnancies. In addition, we also compared sequential embryo transfer with double cleavage-stage embryo transfer. The results indicated that sequential embryo transfer could improve clinical pregnancy rates and reduce multiple pregnancy rates, but had no significant effect on live birth rates (Table S3). For patients with multiple transfer failures, sequential embryo transfer did not enhance clinical pregnancy rates or live birth rates, yet still significantly decreased multiple pregnancy rates (Table S4).
Currently, the clinical pregnancy rate for IVF typically ranges from 40% to 50%, with first IVF cycles achieving rates as high as 60%.23 Despite this, many patients continue to experience repeated failures of embryo transfer. Successful embryo implantation necessitates a synchronized interaction between a receptive endometrium and embryos with high developmental potential.5 Research indicates that approximately two-thirds of embryo transfer failures may be attributed to abnormalities in endometrial receptivity.24 Previous studies have demonstrated that co-culturing early embryos with endometrial epithelial cells can yield a blastocyst formation rate of 50.8% to 58.2%, along with favorable implantation rates, thereby enhancing pregnancy rates in IVF.25 Furthermore, some studies suggest that mechanical stimulation of the endometrium during the initial transfer may trigger the release of specific inflammatory factors, potentially facilitating the adhesion of subsequently transferred embryos.26–29 Additionally, given the uncertainty and individual variability concerning the timing and duration of the window of implantation (WOI), which may last several hours or days,30 transferring two embryos at different time points can improve the chances of aligning the embryos with a receptive endometrium, thereby increasing the likelihood of embryo implantation.31,32 Our findings demonstrate that sequential embryo transfer achieves a live birth rate comparable to that of double blastocyst transfer, while significantly reducing the incidence of multiple pregnancies. In line with previous theoretical studies, these observations suggest that the improved outcomes associated with sequential transfer may not be attributable solely to an increased number of embryos transferred. Instead, it is plausible that the initial transfer of a cleavage-stage embryo enhances endometrial receptivity and creates a more favorable uterine environment for subsequent blastocysts, thereby contributing to the improved clinical outcomes observed. This is merely a speculative explanation for such clinical phenomena. Further studies are warranted to validate this potential mechanism.
Multiple pregnancies have consistently been one of the primary complications associated with assisted reproductive technology (ART),33 adversely affecting outcomes for both mothers and newborns.34,35 Over the past two decades, efforts have been made to mitigate the risk of multiple pregnancies.33,36 However, for patients who have experienced multiple failed transfers, increasing the probability of pregnancy per transfer-by increasing the number of transferred embryos-remains particularly important, even if it occasionally raises the risk of multiple pregnancies. Based on the results of this study, sequential embryo transfer may represent a favorable option for patients who have undergone multiple transfer failures, as it ensures a high clinical pregnancy rate and live birth rate while effectively controlling the incidence of multiple pregnancies.
The current research has several limitations that should be acknowledged. Our study conducted further subgroup analyses based on previous embryo transfer cycles but did not provide a strict definition of RIF. Recent studies have consistently indicated that recurrent transfer failures may be more attributable to embryonic factors. After 3–5 rounds of euploid blastocyst transfers, the majority of patients achieve live birth (92.6–98.1%). Therefore, the proportion of patients with strictly defined RIF is approximately 5%.37,38 Because of the uncertainty in the definition of RIF, the inability to incorporate precise embryo scoring data and the patient’s previous pregnancy status, our study primarily focused on patients with multiple transfer failures. In future investigations, we plan to more precisely identify the characteristic RIF population within our center and analyze the effects of sequential transfer on this group. Additionally, due to constraints within our data management system, our study lacks certain baseline characteristics related to the oocyte retrieval cycles of patients, especially as embryo quality scores. The missing of this key variable increases the difficulty of controlling for the confounding factors and the results may be affected by this confounding factor. The timing of blastocyst transfers on different developmental days can significantly influence the clinical outcomes of IVF.39,40 Some studies indicate that there is no difference in pregnancy outcomes between day 5 and day 6 blastocysts in patients undergoing sequential embryo transfer, suggesting that sequential transfer may enhance the utilization rate of D6 blastocysts.41 This presents an avenue for further exploration. Our data analysis only adjusted for baseline variables without further examining partial effect modifiers, and the absence of interaction analysis also represents a limitation. Moreover, the primary limitation of this study is its retrospective design, which necessitates caution in applying these results to clinical practice. To better clarify the impact of sequential transfer on clinical pregnancy outcomes in FET, high-quality, large-scale randomized controlled trials are required. Such studies will aid in improving embryo utilization efficiency, enhancing implantation rates, and reducing the risk of multiple pregnancies.
Conclusion
In FET cycles, sequential embryo transfer does not improve clinical pregnancy rates or live birth rates but can significantly reduce the rate of multiple pregnancies. For patients who have experienced three or more failed embryo transfers, sequential embryo transfer achieves a live birth rate comparable to that of double blastocyst transfer, while substantially lowering the risk of multiple pregnancies. Therefore, for patients with multiple implantation failure, sequential embryo transfer may offer a more advantageous option, particularly in reducing the incidence of multiple pregnancies.
Abbreviations
FET, frozen-thawed embryo transfer; RIF, recurrent implantation failure; ART, Assisted Reproductive Technology; HRT, hormone replacement therapy; mNC, modified natural cycles, Gn, gonadotropin; hMG, human menopausal gonadotropin; PGT, preimplantation genetic testing; E2, estradiol; P, progesterone; β-hCG, β-human chorionic gonadotropin; SD, Standard Deviation; BMI, body mass index; FSH, follicle-stimulating hormone; LH, luteinizing hormone; AMH, anti-müllerian hormone; AFC, antral follicle count; IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; PESA, percutaneous epididymal sperm aspiration; TESA, testis epididymal sperm aspiration; EMT, endometrium thickness.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to the special requirements of our hospital and our reproductive medicine center for the disclosure of patients’ clinical data but are available from the corresponding author (Jun Xing) on reasonable request via E-mail.
Ethics Approval and Consent to Participate
This retrospective study received ethical approval from the ethics committee of Nanjing Drum Tower Hospital. All methods were carried out in accordance with relevant guidelines and regulations. Our study complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Fertility Research Program of Young and Middle-Aged Physicians-Clinical Research In 2022 and 2023 (Beijing Health Promotion Association, BJHPA-2022-SHZHYXZHQNYJ-LCH-002, BJHPA-2023-SZHYXZHQN-006), fundings for Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2021-LCYJ-MS-20), National Natural Science Foundation of China (82071646), Scientific research project of Jiangsu Province Association of Maternal and Child Health (No. FYX202203), Open project of the Affiliated Jiangning Hospital of Nanjing Medical University Immune Cell Transformation Research Center (JNYYZXKY202213) and Nanjing Drum Tower Hospital Medical Center Project (2022-YXZX-FC-03). There are no conflicts of interest.
Disclosure
Chenyang Huang and Jingyu Liu are co-first authors for this study. The authors declare that they have no competing interests in this work.
References
1. Fauser BC. Towards the global coverage of a unified registry of IVF outcomes. Reprod Biomed Online. 2019;38(2):133–12. doi:10.1016/j.rbmo.2018.12.001
2. De Geyter C, Calhaz-Jorge C, Kupka MS, et al. ART in Europe, 2014: results generated from European registries by ESHRE†. Hum Reprod. 2018;33(9):1586–1601. doi:10.1093/humrep/dey242
3. Huang C, Shen X, Yan Y, et al. The relationship between dominant follicle development and clinical outcomes of hormone replacement therapy-frozen embryo transfer: a retrospective clinical study. Front Endocrinol. 2023;14:1192696. doi:10.3389/fendo.2023.1192696
4. Mitri F, Nayot D, Casper RF, Bentov Y. Current tools for the optimization of embryo transfer technique for recurrent implantation failure. Minerva ginecologica. 2016;68(4):431–449.
5. Governini L, Luongo FP, Haxhiu A, Piomboni P, Luddi A. Main actors behind the endometrial receptivity and successful implantation. Tissue Cell. 2021;73:101656. doi:10.1016/j.tice.2021.101656
6. Craciunas L, Gallos I, Chu J, et al. Conventional and modern markers of endometrial receptivity: a systematic review and meta-analysis. Hum Reprod Update. 2019;25(2):202–223. doi:10.1093/humupd/dmy044
7. Wakuda K, Takakura K, Nakanishi K, et al. Embryo-dependent induction of embryo receptivity in the mouse endometrium. J Reprod Fertil. 1999;115(2):315–324. doi:10.1530/jrf.0.1150315
8. Abramovici H, Dirnfeld M, Weisman Z, et al. Pregnancies following the interval double-transfer technique in an in vitro fertilization-embryo transfer program. J in Vitro Fert Embryo Transf. 1988;5(3):175–176. doi:10.1007/BF01131183
9. Ji M, Zhang L, Fu X, Xie W, Wu X, Shu J. The outcomes of sequential embryo transfer in patients undergoing in vitro fertilization with frozen–thawed embryos: a retrospective study. J Obstet Gynaecol Res. 2022;48(10):2563–2570. doi:10.1111/jog.15369
10. Kyono K, Fukunaga N, Chiba S, et al. Two-step consecutive transfer of early embryos and blastocysts. Reprod Med Biol. 2003;2(3):133–137. doi:10.1046/j.1445-5781.2003.00031.x
11. Tehraninejad ES, Raisi E, Ghaleh FB, et al. The sequential embryo transfer compared to blastocyst embryo transfer in in vitro fertilization (IVF) cycle in patients with the three repeated consecutive IVF. A randomized controlled trial. Gynecol Endocrinol. 2019;35(11):955–959. doi:10.1080/09513590.2019.1613639
12. Zhao Q-H, Song Y-W, Chen J, et al. Embryo transfer strategies for women with recurrent implantation failure during the frozen-thawed embryo transfer cycles: sequential embryo transfer or double-blastocyst transfer? Curr Med Sci. 2024;44(1):212–222. doi:10.1007/s11596-024-2827-9
13. Shalma NM, Talaia AM, Abdelraouf MR, et al. Sequential embryo transfer efficacy in enhancing pregnancy outcomes: a systematic review and meta-analysis. J Assist Reprod Genet. 2025;42(7):2119–2140. doi:10.1007/s10815-025-03487-5
14. Arefi S, Ataei M, Maleki N, Yari N, Razi S, Amirajam S. Sequential (two-step) day 3/day 5 frozen-thawed embryo transfer: does it improve the pregnancy rate of patients suffering recurrent implantation failure? J Med Life. 2022;15(11):1365–1370. doi:10.25122/jml-2022-0041
15. Baradwan S, Alshahrani MS, Sabban H, et al. The effect of sequential embryo transfer on pregnancy outcomes in patients with recurrent implantation failure: a systematic review and meta-analysis of randomized controlled trials. Arch Gynecol Obstet. 2024;310(6):2767–2781. doi:10.1007/s00404-024-07764-z
16. Gao J, Li R, Liu P, Wang H, Long X. Live birth rate and perinatal outcomes following sequential embryo transfer in women with recurrent implantation failure undergoing frozen-thawed embryo transfer cycles. BMC Pregnancy Childbirth. 2025;25(1):433. doi:10.1186/s12884-025-07557-5
17. Wang Z, Liu F, Hu K, et al. One fresh cleavage-stage single embryo transfer (SET) plus one frozen-thawed blastocyst-stage SET or one fresh cleavage-stage double embryo transfer? A retrospective matched cohort study. Hum Reprod. 2024;39(12):2702–2710. doi:10.1093/humrep/deae245
18. Zhang J, Wang C, Zhang H, Zhou Y. Sequential cleavage and blastocyst embryo transfer and IVF outcomes: a systematic review. Reprod Biol Endocrinol. 2021;19(1):142. doi:10.1186/s12958-021-00824-y
19. Gao J, Yuan Y, Li J, et al. Sequential embryo transfer versus double cleavage-stage embryo or double blastocyst transfer in patients with recurrent implantation failure with frozen-thawed embryo transfer cycles: a cohort study. Front Endocrinol. 2023;14:1238251. doi:10.3389/fendo.2023.1238251
20. Failure EWGoRI, Cimadomo D, de Los Santos MJ, Griesinger G, et al. ESHRE good practice recommendations on recurrent implantation failure. Hum Reprod Open. 2023;2023(3):hoad023. doi:10.1093/hropen/hoad023
21. Hu Y-L, Wang Y, Geng L-H, et al. Effects of sequential cleavage and blastocyst embryo transfer on pregnancy outcomes in patients with poor ovarian response. J Reprod Immunol. 2023;155:103780. doi:10.1016/j.jri.2022.103780
22. Li Y, Zhang L, Yu P, Cai X, Li N, Ma B. The efficacy of sequential day 3 embryo and blastocyst transfer in patients with repeated implantation failure. Eur J Obstet Gynecol Reprod Biol. 2023;283:32–36. doi:10.1016/j.ejogrb.2023.01.005
23. Margalioth EJ, Ben-Chetrit A, Gal M, Eldar-Geva T. Investigation and treatment of repeated implantation failure following IVF-ET. Hum Reprod. 2006;21(12):3036–3043. doi:10.1093/humrep/del305
24. Achache H, Revel A. Endometrial receptivity markers, the journey to successful embryo implantation. Hum Reprod Update. 2006;12(6):731–746. doi:10.1093/humupd/dml004
25. Mercader A, Garcia-Velasco JA, Escudero E, Remohi J, Pellicer A, Simon C. Clinical experience and perinatal outcome of blastocyst transfer after coculture of human embryos with human endometrial epithelial cells: a 5-year follow-up study. Fertil Steril. 2003;80(5):1162–1168. doi:10.1016/S0015-0282(03)01178-6
26. Barash A, Dekel N, Fieldust S, Segal I, Schechtman E, Granot I. Local injury to the endometrium doubles the incidence of successful pregnancies in patients undergoing in vitro fertilization. Fertil Steril. 2003;79(6):1317–1322. doi:10.1016/S0015-0282(03)00345-5
27. Zhou L, Li R, Wang R, Huang H-X, Zhong K. Local injury to the endometrium in controlled ovarian hyperstimulation cycles improves implantation rates. Fertil Steril. 2008;89(5):1166–1176. doi:10.1016/j.fertnstert.2007.05.064
28. Gnainsky Y, Granot I, Aldo PB, et al. Local injury of the endometrium induces an inflammatory response that promotes successful implantation. Fertil Steril. 2010;94(6):2030–2036. doi:10.1016/j.fertnstert.2010.02.022
29. Fang C, Huang R, Li -T-T, Jia L, Li -L-L, Liang X-Y. Day-2 and day-3 sequential transfer improves pregnancy rate in patients with repeated IVF–embryo transfer failure: a retrospective case–control study. Reprod Biomed Online. 2013;26(1):30–35. doi:10.1016/j.rbmo.2012.10.004
30. Cha J, Sun X, Dey SK. Mechanisms of implantation: strategies for successful pregnancy. Nat Med. 2012;18(12):1754–1767. doi:10.1038/nm.3012
31. Almog B, Levin I, Wagman I, et al. Interval double transfer improves treatment success in patients with repeated IVF/ET failures. J Assist Reprod Genet. 2008;25(8):353–357. doi:10.1007/s10815-008-9237-y
32. Loutradis D, Drakakis P, Dallianidis K, et al. A double embryo transfer on days 2 and 4 or 5 improves pregnancy outcome in patients with good embryos but repeated failures in IVF or ICSI. Clin Exp Obstet Gynecol. 2004;31(1):63–66.
33. Kim HH, Matevossian K. Are two better than one? Two sequential transfers of a single embryo may be better than a double-embryo transfer. Fertil Steril. 2020;114(2):267–268. doi:10.1016/j.fertnstert.2020.04.064
34. Chambers GM, Hoang VP, Lee E, et al. Hospital costs of multiple-birth and singleton-birth children during the first 5 years of life and the role of assisted reproductive technology. JAMA Pediatr. 2014;168(11):1045–1053. doi:10.1001/jamapediatrics.2014.1357
35. Murray SR, Norman JE. Multiple pregnancies following assisted reproductive technologies – a happy consequence or double trouble? Semin Fetal Neonatal Med. 2014;19(4):222–227. doi:10.1016/j.siny.2014.03.001
36. Cutting R. Single embryo transfer for all. Best Pract Res Clin Obstet Gynaecol. 2018;53:30–37. doi:10.1016/j.bpobgyn.2018.07.001
37. Pirtea P, De Ziegler D, Tao X, et al. Rate of true recurrent implantation failure is low: results of three successive frozen euploid single embryo transfers. Fertil Steril. 2021;115(1):45–53. doi:10.1016/j.fertnstert.2020.07.002
38. Gill P, Ata B, Arnanz A, et al. Does recurrent implantation failure exist? Prevalence and outcomes of five consecutive euploid blastocyst transfers in 123 987 patients. Hum Reprod. 2024;39(5):974–980. doi:10.1093/humrep/deae040
39. Franasiak JM, Forman EJ, Patounakis G, et al. Investigating the impact of the timing of blastulation on implantation: management of embryo-endometrial synchrony improves outcomes. Hum Reprod Open. 2018;2018(4):hoy022. doi:10.1093/hropen/hoy022
40. Adolfsson E, Porath S, Andershed AN. External validation of a time-lapse mo a retrospective study comparing embryo evaluation using a morphokinetic model to standard morphology with live birth as endpoint. JBRA Assisted Reproduction. 2018;22(3):205–214. doi:10.5935/1518-0557.20180041
41. Li J, Ji J, Guo H, Wang F, Fu Y, Hu R. Stratified analysis of clinical pregnancy outcomes of sequential embryo transfer in frozen embryo transfer cycles based on different factors: a retrospective study. BMC Pregnancy Childbirth. 2023;23(1):806. doi:10.1186/s12884-023-06111-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gonadotropin Releasing Hormone Agonists Combined with Hormone Replacement Therapy Significantly Improves Reproductive Outcomes for Patients with Thin Endometrium and Intramural Fibroids in Frozen Embryo Transfer Cycles
Wei L, Tian B, Wang S, Xu S, Zhang C
Drug Design, Development and Therapy 2025, 19:173-183
Published Date: 10 January 2025