Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Impact of Case Management on Elderly Patients with Chronic Obstructive Pulmonary Disease
Authors Li N ![]() , Wang W, Lv Y, Li C, Mu X
, Wang W, Lv Y, Li C, Mu X
Received 15 January 2025
Accepted for publication 25 April 2025
Published 8 May 2025 Volume 2025:20 Pages 1407—1417
DOI https://doi.org/10.2147/COPD.S517564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Na Li,1 Wenjing Wang,2 Yinyin Lv,1 Caihong Li,1 Xiangdong Mu3
1Department of Nursing, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua Medicine, Tsinghua University, Beijing, People’s Republic of China; 2School of Nursing, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua Medicine, Tsinghua University, Beijing, People’s Republic of China
Correspondence: Xiangdong Mu, Department of Pulmonary and Critical Care Medicine, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua Medicine, Tsinghua University, Beijing, People’s Republic of China, Tel +86 15810981402, Email [email protected]
Purpose: This study aims to investigate the effects of case management on elderly patients with chronic obstructive pulmonary disease (COPD) and compare changes in pulmonary function indicators, quality of life, dyspnea, and inhaled medication adherence before and after case management.
Patients and Methods: A total of 199 elderly COPD patients were enrolled from Beijing Tsinghua Changgung Hospital between January 2020 and November 2023. We implemented case management programs including regular patient education, personalized interventions, continuous support systems, and timely feedback mechanisms, and subsequently collected patient data at 1, 3, 6, and 12 months after initiating case management.
Results: After one year of case management, pulmonary function indicators (FEV1/FVC, FEV1, FEV1%pred, MMEF75/25 and MMEF75/25%) in elderly patients with COPD showed significant improvement (P < 0.001). The CAT score decreased from 17.96± 6.57 (mean ± standard deviation) to 11.80± 6.50, and mMRC score decreased from 2.35± 0.66 to 1.14± 0.92 (p< 0.001). Additionally, 77.9% (155/199) of patients were able to maintain their use of the inhaler for 1 year.
Conclusion: This study confirmed the significant role of case management in improving respiratory function, quality of life, and dyspnea in elderly patients with COPD. These findings not only provide a valuable reference for clinicians and patients, but also provide a strong foundation for further optimization of management strategies for elderly patients with COPD.
Keywords: chronic obstructive pulmonary disease, case management, elderly patients, respiratory function, adherence for inhaled therapies
Introduction
Chronic obstructive pulmonary disease (COPD) is a global epidemic. The prevalence of COPD is high, with a global prevalence of 10.3%, and it increases with age.1,2 This high prevalence is particularly concerning among the elderly population, as aging significantly contributes to the progression and impact of the disease. According to the latest WHO data, COPD has become the fourth leading cause of death and the eighth leading cause of health in the world, putting a heavy burden on patients and society.3,4 With the aging population, the number of elderly patients with COPD will continue to rise.1 Therefore, the management of elderly patients with COPD has become a major challenge in the field of public health. Elderly patients with COPD face significant management difficulties and cost due to factors such as decreased physiological function, frequent complications, and low treatment compliance.5 At present, the management modes for this group are mainly divided into specialist management and self-management. Specialty management is limited by resources and time, making it difficult to achieve comprehensive and fine management, and self-management relies on the patient’s cognitive, belief, and behavior, making it difficult to maintain continuity.6
Case management is a patient-centered management model that emphasizes individuation and continuous support. It improves the quality of care and optimizes cost-effectiveness by integrating resources to meet the health needs of patients and their families. Case managers evaluate, coordinate, and plan services to improve the quality of care, reduce healthcare costs, and improve patient health. In recent years, the case management model has shown great potential in the field of disease management and has been successfully applied to care for patients with chronic diseases such as diabetes, infectious diseases such as AIDS, various cancer patients, and postoperative rehabilitation patients, and has achieved remarkable results.7–10 Therefore, this study applied the case management model to elderly COPD patients and explored the impact of case management on elderly COPD patients by comparing and analyzing changes in respiratory function indicators, quality of life, and medication compliance before and after case management. Through this study, we aim to reveal the value and potential benefits of case management in elderly patients with COPD, providing a useful reference for clinicians and patients. At the same time, we also hope that this study will promote further popularization and optimization of case management in elderly COPD patients, and make positive contributions to improving the health status and quality of life of elderly COPD patients.
Materials and Methods
General Information
A total of 199 patients with COPD who were admitted to Beijing Tsinghua Changgung Hospital from January 2020 to November 2023 were admitted in this study. The inclusion criteria were as follows: (1) patients must fulfill the diagnostic criteria for COPD with FEV1/FVC <0.70 after bronchodilator; (2) age ≥60 years old; (3) have normal language expression and comprehension abilities; (4) sign the informed consent and complete the assessment questionnaire voluntarily. Exclusion criteria: Patients with severe organ dysfunction, such as the heart, liver, and kidneys. This study was approved by the Hospital Ethics Committee (Ethics Approval Number: 24631-4-01).
Methods
The team consists of case managers (nurses with at least 10 years of experience in respiratory care), respiratory physicians, therapists, examination technicians, and head nurses. The case management process was developed through team discussions, as shown in Figure 1. Elderly patients with COPD confirmed by pulmonary function tests are referred to the case management clinic. Case managers collect patient information, evaluate patients’ quality of life and breathing difficulties, guide the use of inhaled medications, impart disease knowledge, develop personalized management plans, and coordinate medical resources. Specifically, education is delivered through regular patient meetings, covering COPD pathophysiology, symptom recognition, inhaler techniques, and self-management strategies. Case managers use visual aids, placebo devices, and step-by-step demonstrations to ensure patients understand and correctly apply their inhalers. Case managers actively engage with patients to gather basic information, assess the impact of symptoms on patients’ quality of life and degree of dyspnea, guide inhaled medication use, impart disease knowledge, develop personalized management plans, and coordinate medical resources. Patients are encouraged to attend weekly online patient meetings and activities to share disease-related knowledge, such as respiratory training guidance and practice, pulmonary rehabilitation strategies and precautions, inhaler correct operation demonstration, common error correction, stable patient experience sharing, acute phase coping strategies, etc. Each class lasts approximately one hour. Adherence to inhaled therapies, symptom control, and relief of dyspnea were assessed at 1, 3, 6, and 12 months through interviews, phone calls, WeChat, and online meetings. After 1 year of management and effective symptom control, the case has been resolved and continues to participate in popular science education and health sharing to enhance long-term management skills.
 |
Figure 1 Case management process flow chart. |
Observation Indicators
Respiratory Function
The respiratory function indices were evaluated using a pulmonary function tester (Model: MasterScreen) before and after implementing case management for patients. These indices measured Forced Expiratory Volume in One Second (FEV1), the percentage of FEV1 relative to the predicted value (FEV1%pred), the ratio of FEV1 to Forced Vital Capacity (FEV1/FVC), and the change rate of Maximum Mid-Expiratory Flow (MMEF) between 75% and 25% of vital capacity, expressed as MMEF75/25 and its percentage (MMEF75/25%).
Respiratory Function
Use the lung function tester (Model: MasterScreen) to assess the patient’s respiratory function, including forced expiratory volume (FEV1) in 1 second, the percentage of FEV1 relative to the predicted value (FEV1%pred), the ratio of FEV1 to forced vital capacity (FEV1/FVC), and the rate of change of maximum expiratory flow rate (MMEF) between 75% and 25% of vital capacity. Expressed as MMEF75/25 and its percentage (MMEF75/25%).
Chronic Obstructive Pulmonary Disease Assessment Test (CAT)
The CAT questionnaire was used to assess the effects of the disease on health status and quality of life in elderly patients with COPD. The CAT questionnaire consisted of eight items, each scored on a scale of 0 to 5 based on the severity of the impact, with a higher score indicating a greater impact of the disease on the patient.11
Revised Medical Research Council Dyspnea Scale (mMRC)
The mMRC scale was used to assess the severity of dyspnea. The mMRC scale is graded from 0 to 4, with higher scores indicating more severe dyspnea in patients.12
Test Of The Adherence to Inhalers (TAI)
The TAI questionnaire was used to assess patients’ adherence to inhaled drugs. The TAI questionnaire consisted of 10 items, all of which were scored using a 5-point Likert scale with lower scores indicating lower adherence to inhaled medications.13
Data Collection
The case manager collected general information and outcome indicators for this study. Data was collected at five time points: when patients received case management enrollment (T0), case management for 1 month (T1), 3 months (T2), 6 months (T3), and 1 year (T4). Basic data of patients was collected at T0. Respiratory function indicators were collected at T0 and T4. Inhaled drug compliance scores were recorded from T1 to T4. CAT scores and mMRC ratings were collected from T0 to T4. Basic data and lung function were collected on the spot in the hospital, and other questionnaires and scales were collected through interviews, phone calls, and WeChat.
Data Analysis
SPSS 25.0 software was used for statistical analysis. Categorical variables, such as age, sex, education, and medical history, were described in terms of frequency counts and percentages. Continuous variables, such as lung function index and scale scores, are expressed as mean ± standard deviation (SD). Paired-sample t-tests was used to compare the respiratory function index before and after case management. Changes in CAT, mMRC, and inhaler adherence scores over time were analyzed using repeated measures ANOVA. This statistical test was chosen because it allows for the comparison of measurements taken from the same participants at multiple time points, accounting for within-subject variability. As our study involved repeated assessments of the same participants over time, repeated measures ANOVA was the most appropriate method to assess the changes in these variables while controlling for individual differences. If no significant interaction between time and treatment factors is observed in the repeated measures ANOVA, the main effect test is used to assess the treatment effects. However, if a significant interaction between time and treatment factors is found, the Bonferroni correction method is applied for post-hoc analysis of individual effects. A significance level of α = 0.05 was used for all statistical tests.
Results
Basic Characteristics of Patients Included
A total of 199 participants participated in our study. Among them, 182 patients were aged 60–70 years and 70–80 years, accounting for 48.2% and 43.2%, respectively. The majority were male, accounting for 67.8% (135 cases). 33.2% of participants held a bachelor’s degree or higher. The vast majority (87.9%) used Medicare as a payment method. 82.9% of patients had a duration of disease of less than 5 years. Table 1 provides general information of the included patients.
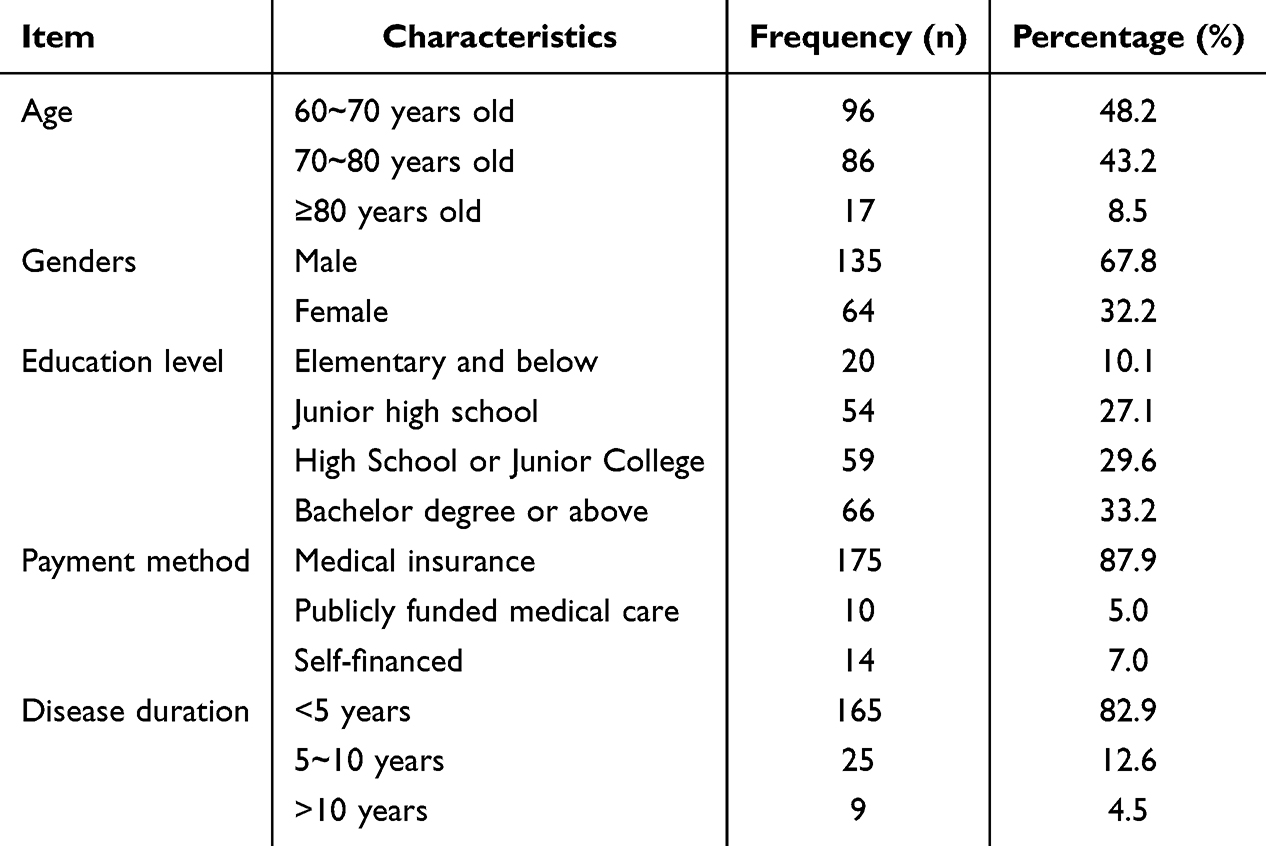 |
Table 1 General Information of the Included Patients (n=199) |
Comparison of Respiratory Function in Elderly COPD Patients Before and After Case Management
The results of a paired T-test showed that the pulmonary function indexes of elderly COPD patients improved before and after case management, with a statistically significant difference (P < 0.001). Table 2 shows the respiratory function indexes and paired T-test results of patients at T0 and T4, and the line chart is shown in Figure 2.
 |
Table 2 Comparison of Patients’ Respiratory Function Before and After Case Management |
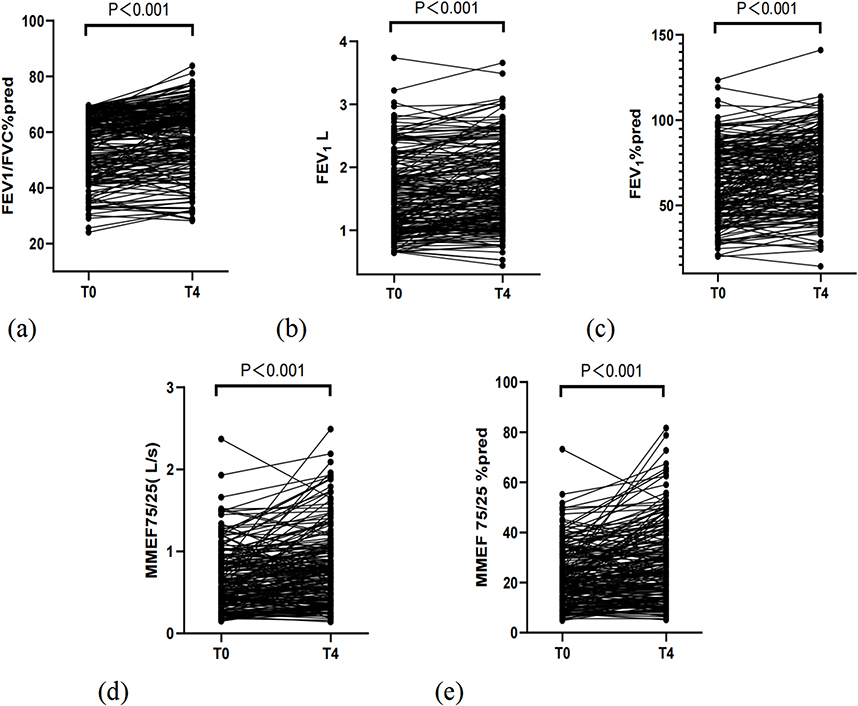 |
Figure 2 Changes in outcomes (a) FEV1/FVC%, (b) FEV1, (c) FEV1%pred, (d) MMEF75/25 (L/s), and (e) MMEF75/25 (%) before and after case management. |
Comparison of CAT Scores, mMRC Grades and TAI Scores in Elderly COPD Patients at Different Time Points of Case Management
In our study, the patient’s CAT score was 17.96±6.57 at the initial time point T0, but with the gradual implementation of case management measures, the score dropped significantly to 11.80±6.50 at the subsequent time point T1. The time points of T2 (10.73±6.66) and T3 (10.10±6.48) showed a continuous downward trend. By T4, the CAT score dropped further to 8.93±6.50. Repeated measurement ANOVA showed that CAT scores were significantly different at different time points (F=240.87, p<0.001). At the initial stage (T0), patients had a mean mMRC score of 2.35±0.66. As case management progressed, patients’ mMRC grades decreased significantly to 1.33±0.96 at T1 and remained stable at T2 (1.27±0.97) and T3 (1.29±0.98). By T4, the mMRC classification was further reduced to 1.14±0.92. Results of repeated measurement ANOVA showed that there were statistically significant differences in mMRC classification at each time point (F=109.77, p<0.001). A total of 199 patients were enrolled in our study, of which 1 patient stopped taking the drug in the first month, 9 patients stopped taking the drug in the third month, 22 patients stopped taking the drug in the sixth month, 12 patients stopped taking the drug within 1 year, and the remaining 155 patients continued taking the drug for 1 year. After 1 year of case management, 77.89% of elderly COPD patients adhered to inhaled medication. Repeated measurement ANOVA results showed no significant difference in patients’ adherence scores to inhaled medications over the case management period (F=1.656, p=0.179). Please refer to Table 3 and Figure 3 for details.
 |
Table 3 Comparison of CAT Scores, mMRC Grades and TAI Scores of Patients at Different Time Points of Case Management |
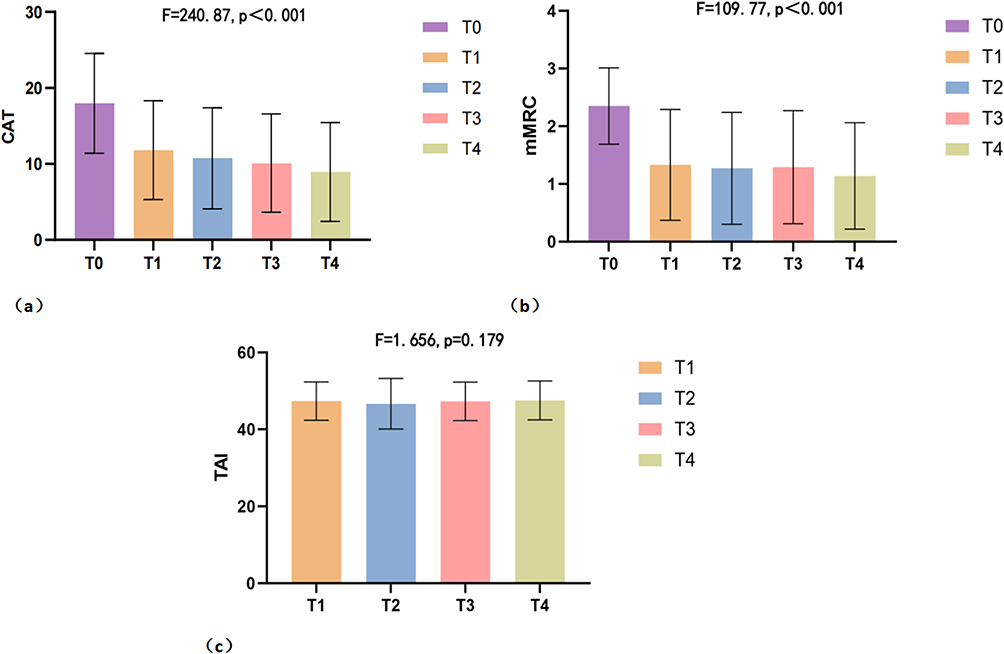 |
Figure 3 Comparison of (a) CAT scores, (b) mMRC grades and (c) TAI scores of patients at different time points of case management. |
Comparison of CAT Score, mMRC Grade and TAI Score of Elderly COPD Patients with Different Demographic Characteristics at Different Time Points of Case Management
We conducted repeated measurement ANOVA on CAT score, mMRC grade, and TAI score of elderly COPD patients with various demographic characteristics (age, gender, education level, and disease course), and the results showed that there were statistical differences in time effects among each group, as shown in Tables 4–7. Further results of the Bonferroni method showed that the mMRC grade of patients ≥80 years old was statistically different from that of the other two age groups (p=0.007, 0.025), and the mMRC grade of patients with disease course < 5 years was statistically different from that of patients with disease course 5–10 years (p=0.030). The remaining differences were not statistically significant.
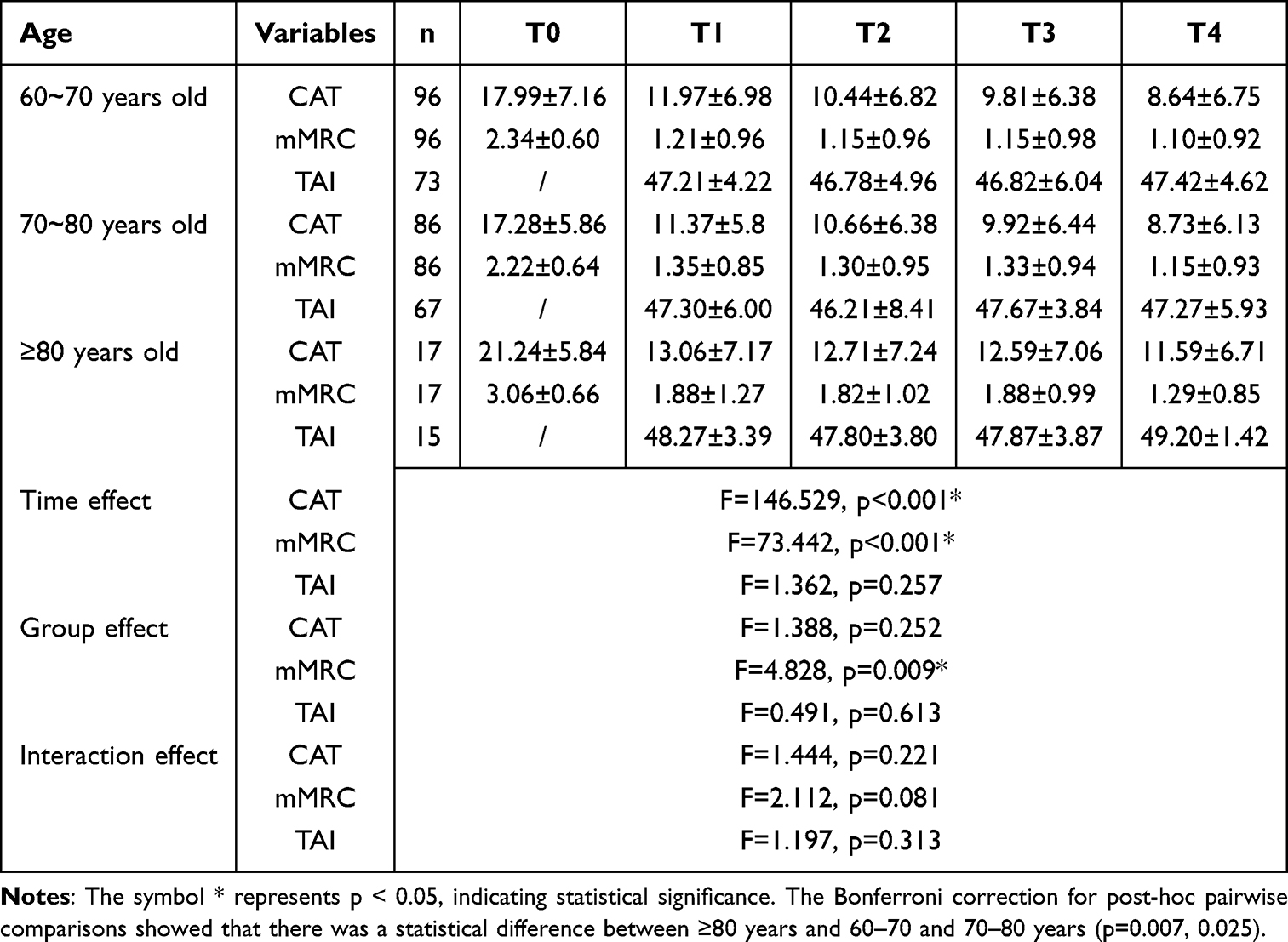 |
Table 4 Comparison of CAT Scores, mMRC Grades, and TAI Scores Among Patients of Different Ages |
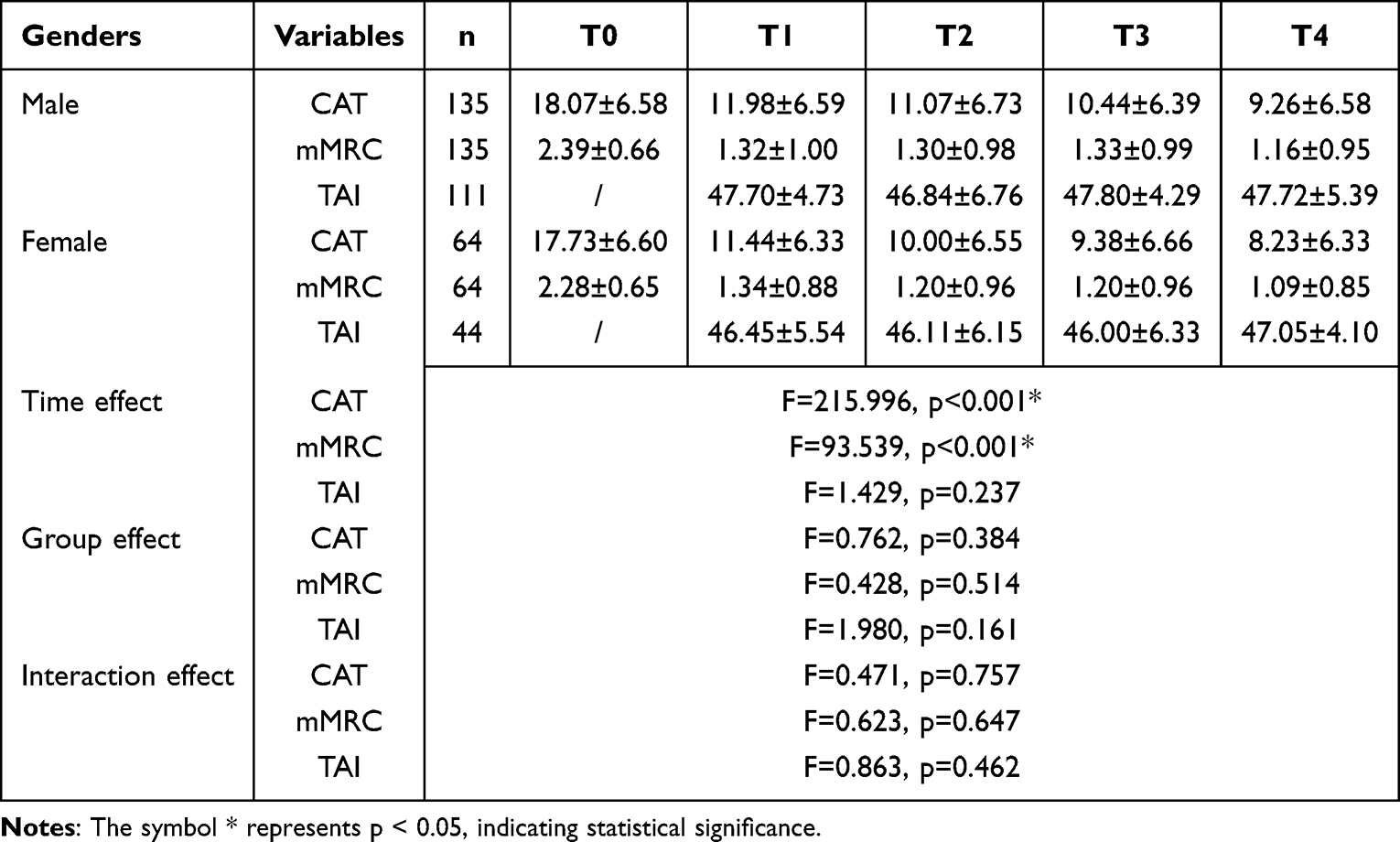 |
Table 5 Comparison of CAT Scores, mMRC Grades, and TAI Scores Among Patients of Different Genders |
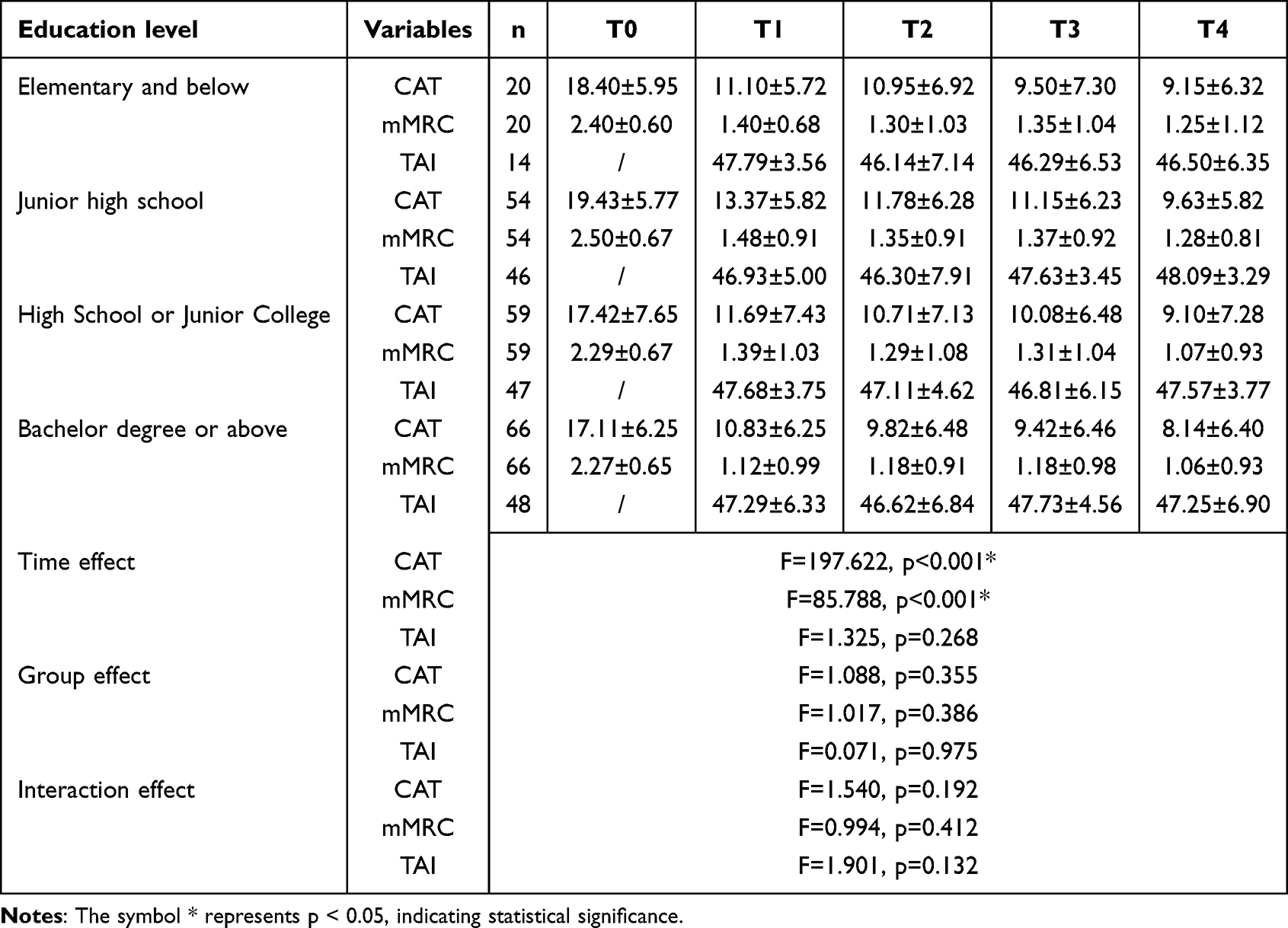 |
Table 6 Comparison of CAT Scores, mMRC Grades, and TAI Scores Among Patients of Different Education Level |
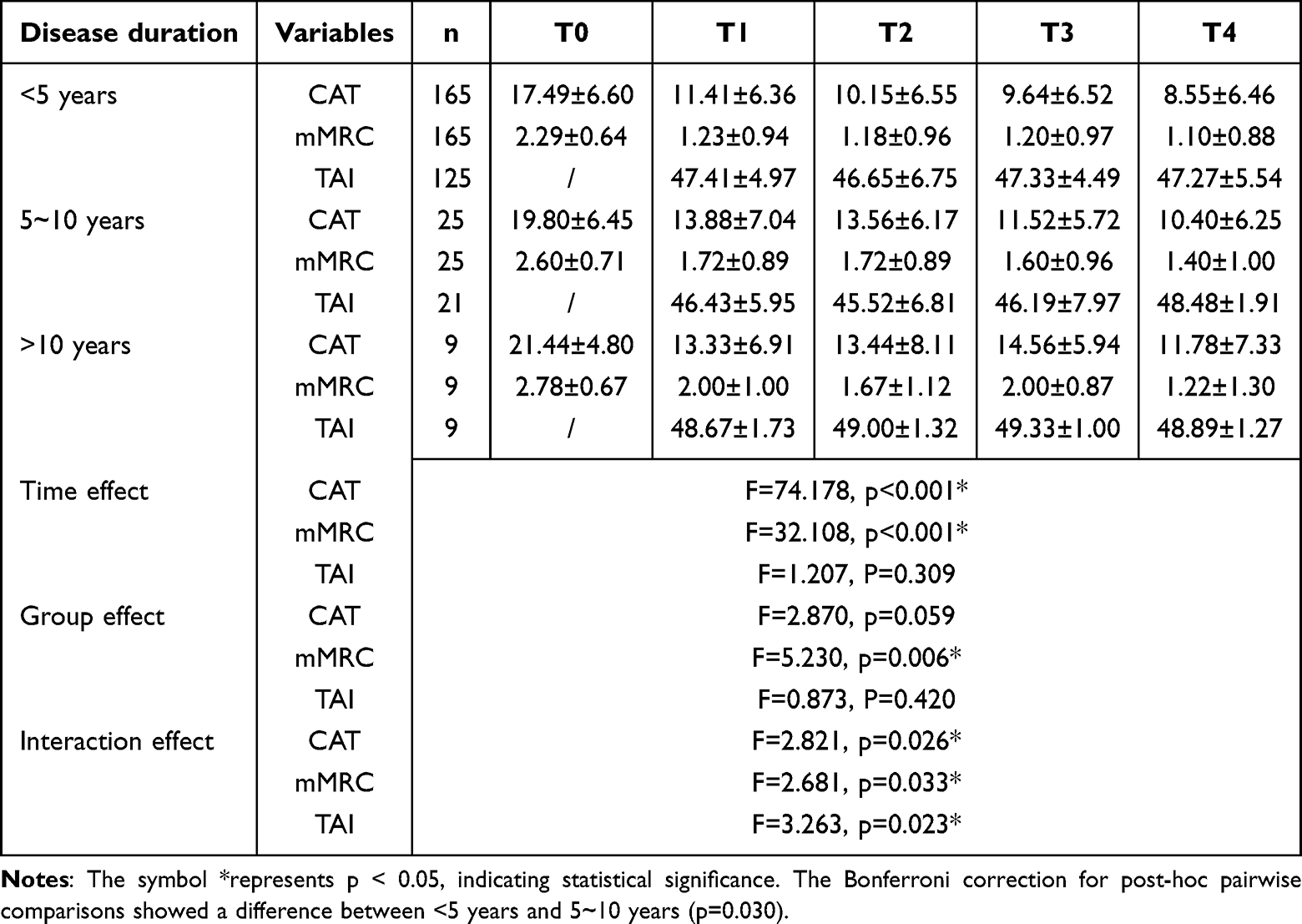 |
Table 7 Comparison of CAT Scores, mMRC Grades, and TAI Scores Among Patients of Different Disease Duration |
Discussion
The study showed that after case management, respiratory function, quality of life, and dyspnea were significantly improved in elderly patients with COPD. Health management is a cyclic and spiraling process that requires regular follow-up studies, evaluation of intervention effects, and adjustment of management programs to form a closed loop of health management.14 The case management implemented in our study emphasizes personalized health management to ensure that each patient has access to a treatment plan tailored to their specific situation and individual needs, which aligns with the philosophy of Songli and Choi.15,16 Songli15 emphasized the concept of precision medicine in the study and found that the precision nursing strategy based on a multidisciplinary collaborative model could effectively improve the lung function, mood, and quality of life of elderly patients undergoing thoracic surgery for lung cancer in a short period of time. Choi16 discovered that personalized education programs, including repetitive education and innovative educational approaches, are crucial in improving lung function, symptom control, asthma knowledge, and health-related quality of life in Korean adult asthmatic patients with poor adherence. Given that inhaled drugs are the first-line treatment for COPD,17 their central role in controlling symptoms, reducing the risk of acute exacerbations, and improving lung function and dyspnea should not be overlooked.18–21 In our study, we focused specifically on the training and education of patients on the proper use of inhaled drugs. In addition, the research of Langer and Hasanpour provides strong theoretical support for our guidance on breathing training.22,23 Langer22 found that eight weeks of home-based, partially supervised muscle training significantly improved patients’ dyspnea and exercise endurance. Similarly, Hasanpour’s study23 focused on breathing exercises such as inspiratory breathing, lip contraction breathing, and effective coughing, which led to a significant improvement in the FEV1/FVC ratio of patients post-intervention. In our weekly patient meetings, we instruct patients to perform standardized breathing exercises to improve their dyspnea levels.
Our study showed that 77.89% of elderly COPD patients were able to maintain their use of inhaled drugs during the one-year case management process, which was significantly higher than the results of previous studies.24 Inhaled drug noncompliance in COPD patients is a complex and multidimensional issue that involves patients’ personal beliefs, concerns about drug side effects, the complexity of treatment regiments, and socioeconomic factors.25,26 Studies have shown that patients often make errors when using inhaled drugs, in addition to non-compliance.27,28 In the case management process of our study, patients received continuous health guidance on inhaling drugs through regular follow-up to improve their medication knowledge and skills, which was the same as Tian’s study.29 Furthermore, in the case management process of this study, we provided inhalation trainers to patients with limited inhalation ability to help them practice inhalation anytime and anywhere in daily life and master inhalation methods more effectively, similar to the conclusion of Jansen’s study,30 which shows that the introduction of personalized reminder devices, such as smart inhalers, is an innovative and effective strategy to help patients establish good medication habits and ensure they can accurately control and manage the use of various inhalation devices. Although our study showed no significant difference in inhaled drug compliance after 1 year of case management, the TAI questionnaire stipulated that a score of > 45 indicated good inhalation compliance. In this study, in the stages of case management from T1 to T4, the average TAI score of elderly COPD patients remained above 45 points and did not decrease over time, which is still an exciting research result. Our study revealed that older COPD patients had more pronounced improvements in mMRC scores post - case management. This may stem from their higher treatment and management compliance. They more actively adhered to case managers’ guidance, leading to remarkable symptom alleviation. Even though body function may decline with age, it does not preclude them from achieving better subjective symptom outcomes through case management.
Based on the results of different subgroups, the case management model proposed in this study has a wide range of applicability. Specifically, the model achieved significant and consistent results across age levels, gender differences, and in older COPD patients with diverse educational backgrounds. This finding not only supports the effectiveness and universal applicability of this case management model, but also highlights its potential for application and promotion in a wider patient population.
Although our research has made some progress, there are several limitations that need to be addressed. The sample size of this study is limited, which may not fully reflect the overall population of elderly patients with COPD. To overcome this limitation, future studies should aim to include larger, more diverse samples from multiple healthcare settings to increase the generalizability of the findings. Furthermore, this study did not include a cost-benefit analysis of case management, which is crucial for evaluating the economic viability and sustainability of the approach. Future research should incorporate this analysis to provide a comprehensive understanding of the value of case management in COPD care. Another challenge is the potential challenges in implementing this model across different healthcare settings. These challenges include limited resources, a lack of specialized training for healthcare providers, and the variability in patient populations. To address these challenges, future research should focus on developing strategies to increase resource allocation, create targeted training programs for healthcare providers, and adapt the case management model to various clinical contexts.
Conclusion
Our study confirmed the significant effect of case management on improving respiratory function, quality of life, and alleviating dyspnea in elderly patients with COPD through the implementation of a case management model. These results provide feasible management options for clinical practice, particularly in improving patient health. Future research should explore the long-term effects of case management, as well as its feasibility in different healthcare settings. Additionally, studies should examine the specific obstacles to its implementation and ways to overcome them. From a policy perspective, integrating case management into routine care for COPD patients, particularly in elderly populations, could lead to better health outcomes and more efficient use of healthcare resources.
Ethics Approval and Consent to Participate
This study and the informed consent process were approved by the Ethics Review Committee of Beijing Tsinghua Changgung Hospital (24631-4-01). The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The analyses in Tables 4-7 are exploratory and were not pre-planned.
Funding
This research was funded by the Beijing Clinical Key Specialty (grant no.XKB2022B1002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Adeloye D, Song P, Zhu Y, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. World Health Organization. Chronic obstructive pulmonary disease. 2024.
4. Li H, Liang H, Wei L, et al. Health inequality in the global burden of chronic obstructive pulmonary disease: findings from the global burden of disease study 2019. Int J Chron Obstruct Pulmon Dis. 2022;17:1695–1702. doi:10.2147/COPD.S369120
5. Allen B, Aboussouan LS. Diagnostic and therapeutic challenges of chronic obstructive pulmonary disease in the elderly. Curr Opin Pulm Med. 2021;27(2):113–119. doi:10.1097/MCP.0000000000000750
6. Liu JC, Zheng HY, Li CF, et al. [The management model and development trend of chronic obstructive pulmonary disease]. Chin J Prev Contr Chron Dis. 2022;30(07):541–544. Corsican
7. Ji H, Chen R, Huang Y, et al. Effect of simulation education and case management on glycemic control in type 2 diabetes. Diabetes Metab Res Rev. 2019;35(3):e3112. doi:10.1002/dmrr.3112
8. Maria DS, Nyamathi A, Lightfoot M, et al. Results of a randomized wait-list controlled trial of CAYA: a nurse case management HIV prevention intervention for youth experiencing homelessness. AIDS Behav. 2024;29(2):613–625. doi:10.1007/s10461-024-04544-3
9. Zhou R, Xu CL. Application effect of case management nursing based on patient safety in patients with prostate cancer. World J Clin Cases. 2024;12(27):6070–6076. doi:10.12998/wjcc.v12.i27.6070
10. Jin H, Wu L, Huang P, et al. A study on the intervention effect of a case management model that breaks through spatiotemporal characteristics in home-based Phase II exercise rehabilitation post PCI. Front Cardiovasc Med. 2024;11:1412675. doi:10.3389/fcvm.2024.1412675
11. Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
12. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
13. Meng WW, Cui YN, Luo LJ, et al. Reliability and validity of the Chinese version of the test of the adherence to inhalers (TAI). Zhonghua Jie He He Hu Xi Za Zhi. 2022;45(5):423–430. doi:10.3760/cma.j.cn112147-20211108-00783
14. Guo JJ, Li XM, Yang YT. Research design and application practice of follow-up studies in health management. Chin J Health Manage. 2024;18(04):315–320.
15. Songli M, Xuyi W, Jie Y, et al. Application of precision nursing based on multidisciplinary collaboration model in older patients undergoing thoracoscopic surgery for lung cancer. J Sichuan Univ. 2023;54(5):1052–1057.
16. Choi JY, Cho Chung HI. Effect of an individualised education programme on asthma control, inhaler use skill, asthma knowledge and health-related quality of life among poorly compliant Korean adult patients with asthma. J Clin Nurs. 2011;20(1–2):119–126. doi:10.1111/j.1365-2702.2010.03420.x
17. Disease Gifcol. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021 REPORT). 2020.
18. Bourbeau J, Bhutani M, Hernandez P, et al. 2023 Canadian thoracic society guideline on pharmacotherapy in patients with stable COPD. Chest. 2023;164(5):1159–1183. doi:10.1016/j.chest.2023.08.014
19. Di Marco F, Santus P, Scichilone N, et al. Symptom variability and control in COPD: advantages of dual bronchodilation therapy. Respir Med. 2017;125:49–56. doi:10.1016/j.rmed.2017.03.001
20. Heo YA. Budesonide/glycopyrronium/formoterol: a review in COPD. Drugs. 2021;81(12):1411–1422. doi:10.1007/s40265-021-01562-6
21. Ozoglu Aytac S, Kilic SP, Ovayolu N. Effect of inhaler drug education on fatigue, dyspnea severity, and respiratory function tests in patients with COPD. Patient Educ Couns. 2020;103(4):709–716. doi:10.1016/j.pec.2019.11.003
22. Langer D, Ciavaglia C, Faisal A, et al. Inspiratory muscle training reduces diaphragm activation and dyspnea during exercise in COPD. J Appl Physiol. 2018;125(2):381–392. doi:10.1152/japplphysiol.01078.2017
23. Hasanpour Dehkordi A, Ebrahimi-Dehkordi S, Banitalebi-Dehkordi F, et al. The effect of teach-back training intervention of breathing exercise on the level of dyspnea, six-minutes walking test and FEV1/FVC ratio in patients with chronic obstructive pulmonary disease; a randomized controlled trial. Expert Rev Respir Med. 2021;15(1):161–169. doi:10.1080/17476348.2020.1822740
24. Restrepo RD, Alvarez MT, Wittnebel LD, et al. Medication adherence issues in patients treated for COPD. Int J Chron Obstruct Pulmon Dis. 2008;3(3):371–384. doi:10.2147/copd.s3036
25. Partridge MR, Dal negro RW, Olivieri D. Understanding patients with asthma and COPD: insights from a European study. Prim Care Respir J. 2011;20(3):315–323,317pfollowing323. doi:10.4104/pcrj.2011.00056
26. Woo S, Veliz P, Saint Arnault DM, et al. Development and preliminary psychometric evaluation of the COPD-related Stigma Scale. Heart Lung. 2023;61:22–28. doi:10.1016/j.hrtlng.2023.04.006
27. Sriram KB, Percival M. Suboptimal inhaler medication adherence and incorrect technique are common among chronic obstructive pulmonary disease patients. Chron Respir Dis. 2016;13(1):13–22. doi:10.1177/1479972315606313
28. Sanaullah T, Khan S, Masoom A, et al. Inhaler use technique in chronic obstructive pulmonary disease patients: errors, practices and barriers. Cureus. 2020;12(9):e10569. doi:10.7759/cureus.10569
29. Tian CY, Zhao J, Liu QY, et al. Application of telephone follow-up on COPD patients’ use of Spiriva. Chin J Mod Nurs. 2013;19(27):3339–3342.
30. Jansen EM, van de Hei SJ, Dierick BJH, et al. Global burden of medication non-adherence in chronic obstructive pulmonary disease (COPD) and asthma: a narrative review of the clinical and economic case for smart inhalers. J Thorac Dis. 2021;13(6):3846–3864. doi:10.21037/jtd-20-2360
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.