Back to Journals » Orthopedic Research and Reviews » Volume 18
The Impact of Bone Cement Distribution in Unilateral PVP on Therapeutic Outcomes of Vertebral Compression Fracture Repair
Authors Yusufu A, Yasin P, Haibier A ![]() , Ma Y
, Ma Y
Received 13 September 2025
Accepted for publication 24 November 2025
Published 8 June 2026 Volume 2026:18 567335
DOI https://doi.org/10.2147/ORR.S567335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Alimujiang Yusufu,1,2,* Parhat Yasin,1,2,* Abuduwupuer Haibier,1 Yuan Ma1,2
1Spine Surgery Department, Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 2Xinjiang Spine Surgery Institute, Urumqi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan Ma, Email [email protected]
Background: Osteoporotic vertebral compression fractures (OVCFs) are common in the elderly, severely impacting health and quality of life. Percutaneous vertebroplasty (PVP) is a primary treatment, with bone cement distribution being a key factor influencing its efficacy.
Objective: This study aimed to evaluate the impact of bone cement distribution patterns on clinical outcomes in unilateral PVP for OVCFs.
Methods: A total of 145 patients undergoing first-time unilateral PVP were retrospectively analyzed. Based on postoperative anteroposterior X-rays, patients were divided into three groups according to cement coverage: Group A (uniform distribution across three vertebral regions, n=57), Group B (covering > 1/2 to ≤ 2/3, n=51), and Group C (covering > 1/3 to ≤ 1/2, n=37). Primary outcomes (VAS, ODI, vertebral height recovery, refracture rate) and secondary outcomes were compared.
Results: At one-year follow-up, VAS scores were significantly lower in Groups A (2.12± 0.54) and B (2.16± 0.54) than in Group C (2.43± 0.50, P< 0.05). Vertebral height recovery was superior in Groups A and B compared to Group C (P< 0.05). The overall refracture rate was significantly lower in Group A (3.6%) than in Group C (18.9%, P< 0.05), with no significant difference from Group B (3.9%). Group A received a higher cement volume (4.95± 0.43 mL) than Groups B and C (P< 0.05).
Conclusion: Bone cement distribution crossing the vertebral midline is associated with better pain relief, improved vertebral height restoration, and a lower refracture rate after unilateral PVP. However, exceeding two-thirds vertebral coverage does not appear to be a critical factor for surgical efficacy.
Keywords: osteoporotic vertebral compression fractures, thoracolumbar vertebrae, percutaneous vertebroplasty, bone cement
Introduction
Osteoporotic vertebral compression fractures (OVCFs) are clinical manifestations secondary to osteoporosis.1 As one of the most severe fracture types, OVCFs account for approximately 50% of all osteoporotic fractures and has become the third most common fragile fracture in the world.2,3 This type of fracture is more common in the elderly, and may lead to chronic pain, motor dysfunction, spinal deformities, decreased quality of life and increased mortality. It not only seriously affects human health and quality of life, but also brings a heavy burden to families and society.4,5 While conservative management remains an option, it is often associated with prolonged pain, functional limitation, and risks of fracture progression or non-union, underscoring the need for effective surgical alternatives like percutaneous vertebroplasty (PVP).6
Percutaneous vertebroplasty(PVP) can instantly relieve pain and stabilize fractured vertebrae. It has high safety and reliable short-term efficacy. It has become the most commonly used treatment method for OVCFs in recent years.7,8 Polymethyl methacrylate bone cement is one of the most commonly used bone cements in clinical practice. It has good injection properties and mechanical properties. The safety and clinical effect of treating OVCFs have been widely recognized.9 Studies have proved that balanced filling of bone cement can effectively reduce vertebral fractures after PVP and improve recovery effect. However, how to ensure good bone cement distribution in PVP is still the focus of doctors.10
This study analyzed the clinical data of OVCFs patients diagnosed and treated at the Sixth Affiliated Hospital of Xinjiang Medical University from January 2022 to January 2024, and discussed the impact of bone cement distribution on the efficacy of unilateral PVP, so as to provide effective prevention and treatment measures to prevent postoperative vertebral fractures and improve surgical efficacy. To this end, we conducted a single-center retrospective cohort study of 145 patients who underwent unilateral PVP between January 2022 and June 2024, evaluating the association between cement distribution patterns (Group A, B, C) and key outcomes including pain relief (VAS at 12 months), vertebral height restoration, and refracture rates.
Materials and Methods
Case Selection
Inclusion criteria: ① Patients who underwent unilateral approach percutaneous vertebraption for the first time; ② Bone density examination confirmed osteoporosis, defined as a bone mineral density (BMD) T-score ≤ −2.5 standard deviations (SD) at the lumbar spine or hip, and MRI confirmed a fresh fracture consistent with osteoporotic changes; ③ Patients with BMD T-score > −2.5 SD (indicating normal bone mass or osteopenia); ④ Fresh compression fractures located in the thoracic or lumbar spine (T1-L5), with the number of fractured vertebrae ≤2.
Exclusion criteria: ① Patients with burst fractures (including thoracolumbar and other levels) or fractures caused by high-energy trauma. ② Patients with fractures associated with spinal canal compromise, spinal cord, or cauda equina nerve root injury. (This explicitly excludes cervical, sacral, and any other fracture types not meeting the inclusion criteria). ③ Patients with bone density showing normal or low bone mass. ④ Patients who cannot tolerate surgery such as coagulation abnormalities, mental history, liver and kidney dysfunction, etc. ⑤ Patients with metastatic tumors or other pathological fractures; ⑥ Patients allergic to bone cement.
This trial was conducted in the Department of Spinal Surgery, the Sixth Affiliated Hospital of Xinjiang Medical University from January 2022 to June 2024. There were 145 patients who chose to be admitted to the Sixth Affiliated Hospital of Xinjiang Medical University from January 2022 to January 2024 and received unilateral approach PVP for the first time, including 49 males and 96 females. The test complies with the Declaration of Helsinki. The test plan was reviewed by the Ethics Committee of the Sixth Affiliated Hospital of Xinjiang Medical University. Batch number: LFYLLSC20250710-01. All the trial subjects signed an informed consent form (see Figure 1 for case screening flow chart).
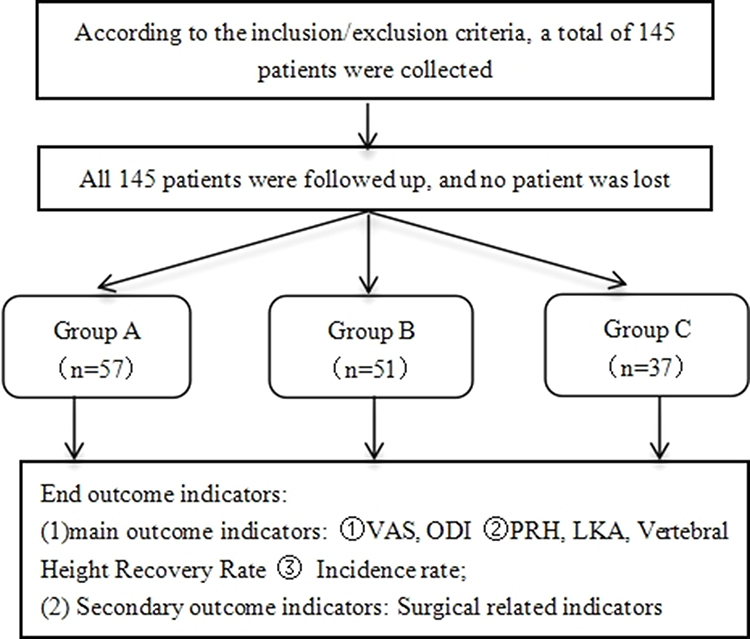 |
Figure 1 Flow chart of patient assignment. Notes: The vertebral body was divided into three regions A, B and C. Group I: the bone cement was evenly distributed in ABC region; Group II: the bone cement was distributed more than half but not more than two thirds of the vertebral body; Group III: the bone cement was distributed more than one third but not more than one half of the vertebral body (The yellow line divides the entire vertebral body into three equal parts, while the red line divides it into two equal parts.). |
Surgical Methods
Preoperative Preparation
All patients completed X-rays, CT and MRI examinations after admission to evaluate vertebral compression; routine blood C-reactive protein, liver and kidney function, and serum bone metabolism examinations were performed to evaluate the patient’s basic condition; bone density examinations were performed to evaluate the patient’s bone quality.
PVP Surgery Plan
The patient was prone to the position, with the chest and back and lower limbs raised, so that the chest and abdomen were suspended in the air. After the vertebrae was positioned in the vertebrae, he first gently pressed the vertebrae and used manual method to reduce the partial compression fracture. Conventional towel laying, local anesthesia, unilateral pedicle puncture, the entry point was selected at the lateral and superior aspect (the “10 o’clock” position on the left pedicle or the “2 o’clock” position on the right pedicle, conceptually) of the pedicle’s outer margin, after the puncture needle reaches the inner edge of the spinal canal root. In the lateral position of the fluoroscopic lateral position, it can be seen that the puncture needle reaches the posterior edge of the vertebrae and continues to enter the needle to reach 1/3 of the front of the vertebrae. Again, the correct position of the puncture needle is confirmed to be on the midline of the vertebra or just passed the midline of the vertebra. Pull out the puncture needle core and place the bone cement push rod to inject the bone cement that is in the “wire drawing stage” into the vertebra. The entire operation is monitored through the whole process to prevent the bone cement from leaking. At the end, first rotate the puncture needle and then pull it out to prevent the bone cement from being dragged. No suture incision is required, sterile dressing is bandaged, the patient’s vital signs are monitored to be smooth and then sent back to the ward.
Postoperative Treatment
After 8 hours of bed rest, you can wear a waist circumference and get out of bed to move, continue to treat anti-osteoporosis, take oral calcium carbonate D3 tablets, 600 mg each time, once a day; α-calciferol capsules, 0.25μg each, 1 to 2 times a day. Use 100mL of zoledronic acid injection once a year for 3 to 5 consecutive years. You can also intravenously inject salmon calcitonin 50IU each time, once a day for 1 consecutive month. The patient underwent X-ray and CT reexamination after surgery to clarify the distribution of bone cement and the recovery of the surgical vertebral body height.
Type of Bone Cement Distribution
Observe the distribution of bone cement based on the front X-ray film of the vertebral body, divide the vertebral body into three areas, type I (the bone cement is evenly distributed in the three areas), type II (the distribution range of bone cement exceeds one-half of the vertebral body, but not more than two-thirds), and type III (the bone cement only exceeds one-third of the vertebral body, but not more than one-half of the vertebral body), see Figure 2.
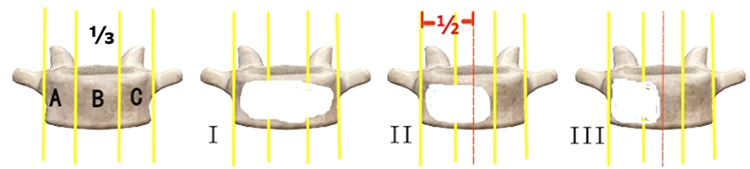 |
Figure 2 Type of bone cement distribution. Notes: A1 is the preoperative posterior edge of the vertebra; A2 is the preoperative height of the fractured vertebra; A3 is the preoperative anterior edge of the vertebra. B1 is the postoperative posterior edge of the vertebra; B2 is the postoperative restored height of the vertebra; B3 is the postoperative anterior edge of the vertebra. |
Refracture Evaluation
After percutaneous vertebratomy, the patient developed lumbar back pain and discomfort again. Physical examination showed positive percussion pain of spinal or spinous process. Through medical history, clinical manifestations and lumbar X-ray examination, it was suggested that the percussion plane vertebra had a compressive fracture, and the MRI examination showed that the fracture occurred again.
Observation Indicators
Collect basic information about patients before surgery, including gender, age, body mass index, time from injury to surgery, underlying diseases, VAS, ODI, PFH and LKA, etc.
The main outcome indicators include: postoperative VAS, ODI, PRH, LKA, vertebral height recovery rate, refracture occurrence and cement leakage rate. Among them, the measurement method of the local posterior kyphosis angle is: Line A is the parallel line of the upper end plate of the first vertebra above the fractured vertebra, Line B is the parallel line of the lower end plate of the first vertebra below the fractured vertebra, and LKA is the angle between A and B (see Figure 3). Recovery rate of vertebral height = (postoperative vertebral height - preoperative vertebral height)/primitive vertebral height.8 Secondary outcome indicators include: operation time, number of intraoperative fluoroscopy, Length of stays, amount of cement injection and total hospitalization cost.
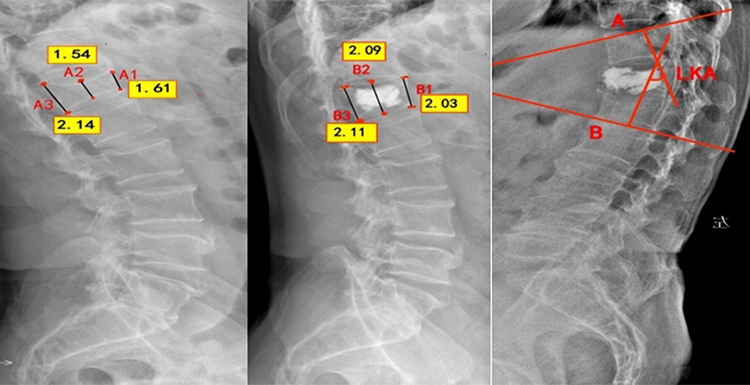 |
Figure 3 Measurement of imaging parameters after vertebroplasty. |
Statistical Analysis
SPSS26.0 software was used to conduct statistical analysis of the research data. The measurement data is expressed in  , and the count data is expressed in rate (%). According to the results of the normality test, if the normality distribution is met, the variance analysis is used for comparison between the three groups; if the normality distribution is not met, the Kruskal-wallisH test is used for comparison between the three groups. For post-hoc pairwise comparisons among the three groups following a significant ANOVA result, the Student-Newman-Keuls (SNK) q test was employed, as it is well-suited for identifying which specific group means differ after a significant omnibus test.
, and the count data is expressed in rate (%). According to the results of the normality test, if the normality distribution is met, the variance analysis is used for comparison between the three groups; if the normality distribution is not met, the Kruskal-wallisH test is used for comparison between the three groups. For post-hoc pairwise comparisons among the three groups following a significant ANOVA result, the Student-Newman-Keuls (SNK) q test was employed, as it is well-suited for identifying which specific group means differ after a significant omnibus test.
Results
General Information
There was no statistically significant difference in the general information of the two groups (P>0.05), suggesting that the two groups are comparable (Table 1). The follow-up time of the two groups was 12–20 months, and the average follow-up time was (14.145±1.863) months.
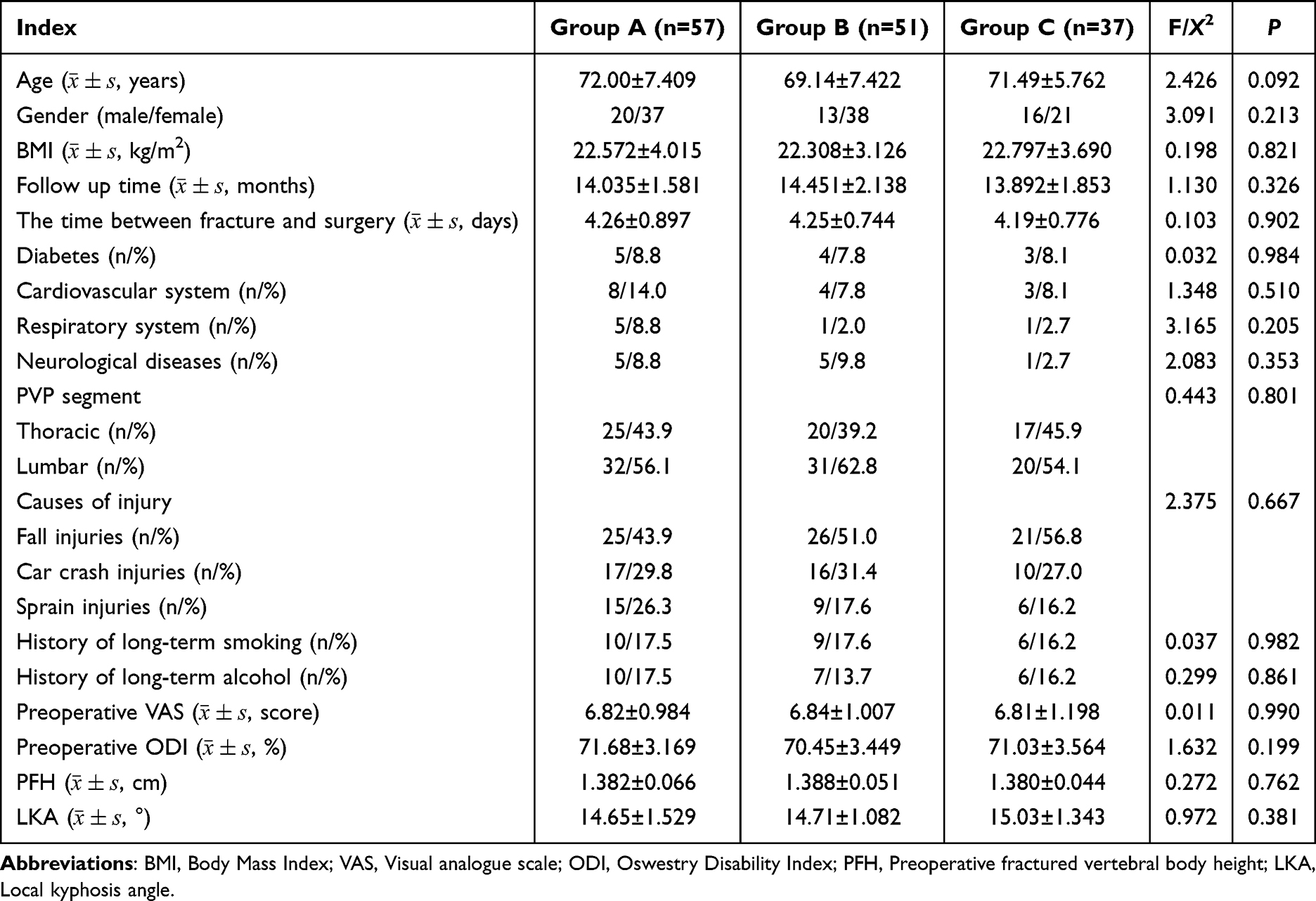 |
Table 1 Comparison of the Baseline Data |
Comparison of Main Outcome Indicators
Comparison Between Postoperative VAS and ODI
In terms of VAS scores of low back pain in 1 week after surgery, there was no difference between the three groups of patients (P>0.05); in terms of VAS scores of low back pain in 6 months after surgery, there was a significant difference between patients in group A compared with those in the other two groups (P<0.05), and group A had a smaller pain score. At the first anniversary of the operation, there was no significant difference between VAS scores of low back pain in group A and group B (P>0.05). However, groups A and B had smaller VAS scores compared with group C, and the difference was statistically significant (P<0.05). There was no significant difference in ODI scores of the three groups of patients after surgery (P>0.05). The specific situation is shown in Table 2 and Figure 4.
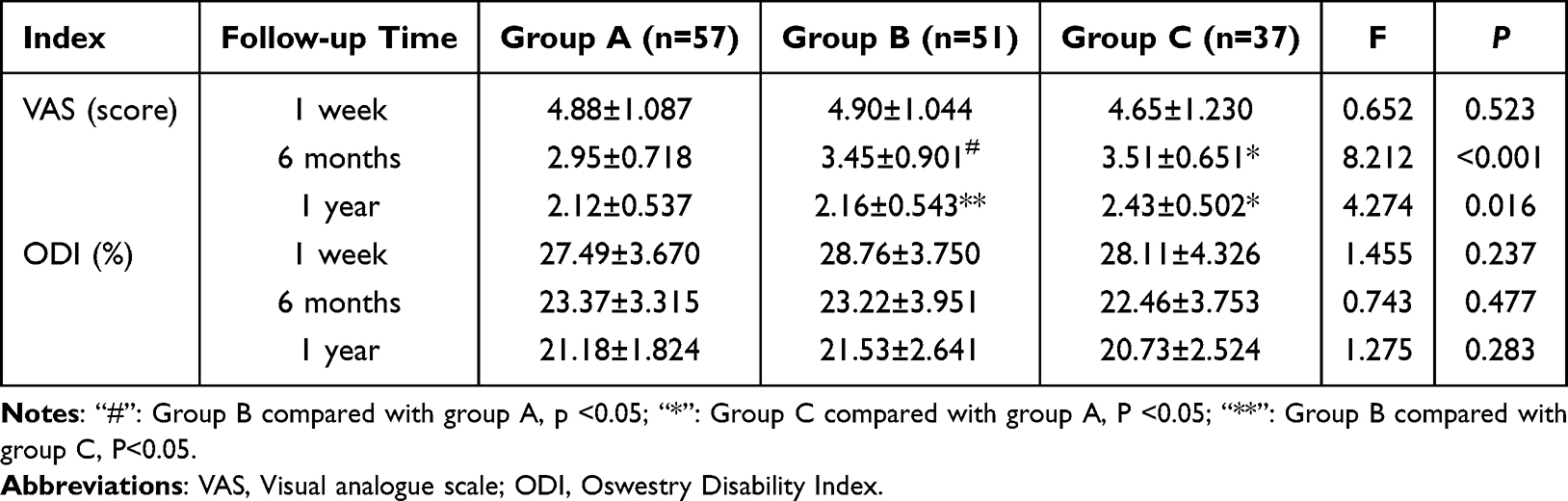 |
Table 2 Comparison of Postoperative VAS and ODI Scores in the Three Groups |
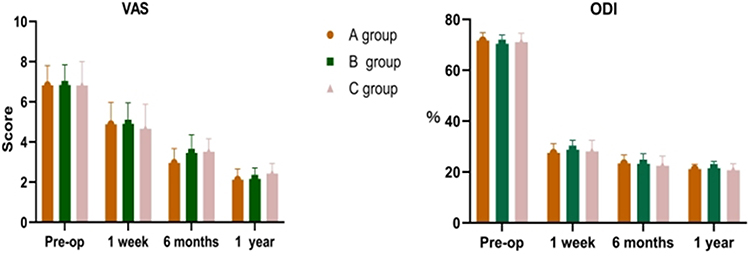 |
Figure 4 Comparison of VAS and ODI between the three groups. |
Comparison of Postoperative Imaging Indicators, Refractory Incidence and Bone Cement Leakage
By comparing the postoperative imaging data of patients after follow-up, it was found that patients in Group A and Group B had better vertebral height and vertebral height response rates (P=0.014) and lower overall fracture event rates (P= 0.020), with statistically significant differences; there was no significant difference in the remaining indicators of the three groups of patients (P > 0.05), see Table 3.
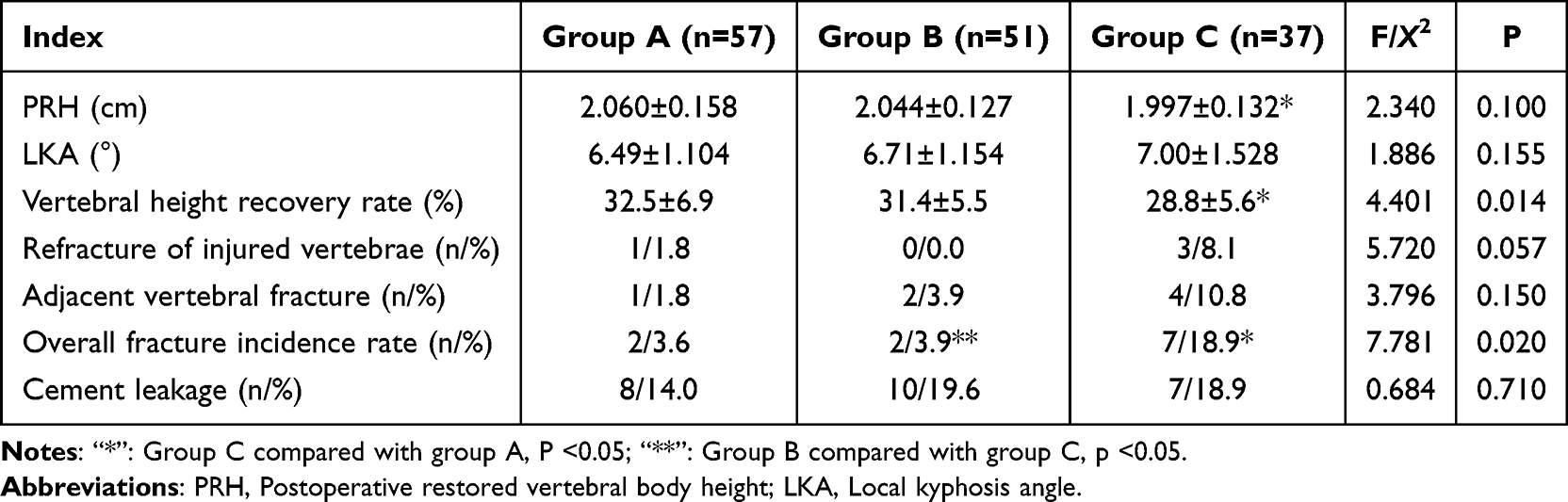 |
Table 3 Comparison of Imaging Data and Complications Among the Three Groups |
Comparison of Secondary Outcome Indicators
The amount of bone cement injection intraoperative in patients in Group A was significantly extraordinarily unnecessary for the other two groups, and the difference was statistically significant (P<0.001); the differences in the operation time, fluoroscopy, hospitalization days and hospitalization costs of the three groups were not statistically significant (P>0.05), see Table 4.
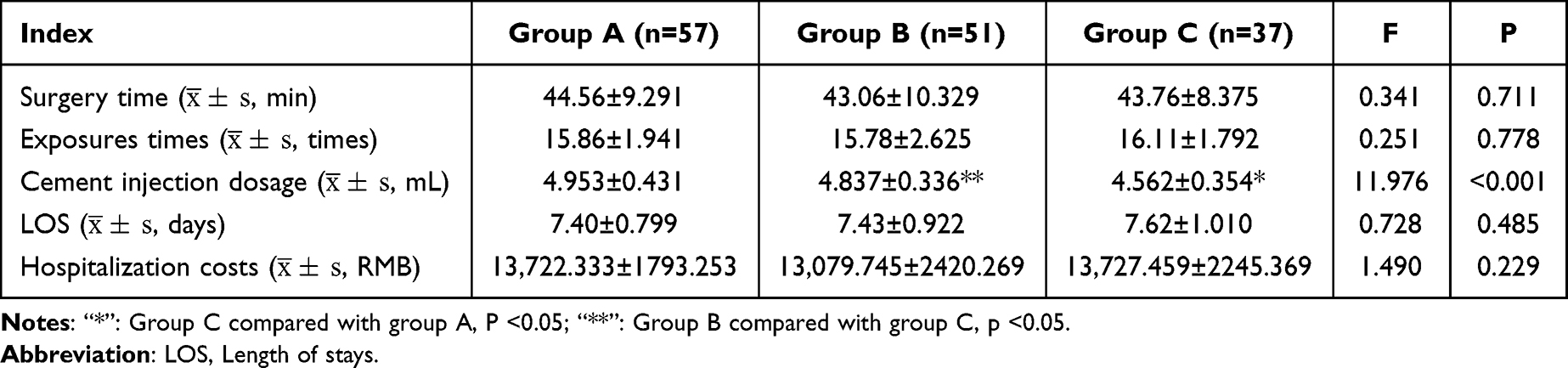 |
Table 4 Comparison of Secondary Outcome Indicators Between the Two Groups |
Discussion
As population aging intensifies, the incidence of OVCFs continues to rise.11 At present, the treatment of OVCFs is mainly surgical treatment. PVP can treat low-trauma OVCFs due to its high reliability and safety, and has now become one of the main surgical methods for this disease.12–14 PVP is a minimally invasive surgery in spinal surgery that minimizes surgical trauma, shorter surgery time, and can quickly relieve pain and recover quickly after surgery. This technology has been widely used since 1987 to treat vertebral compression fractures and vertebral bone destruction caused by osteoporosis, bone metastasis and invasive hemangioma.15,16 Studies have reported that different bone cement distributions may bring different surgical effects.17,18 The distribution pattern of bone cement has been studied by many researchers. Some literature reports that whether bone cement distribution exceeds the midline of the vertebral body has nothing to do with vertebral body strength, strengthening vertebral fracture and postoperative effect, but the current views are not consistent.19,20 Our study reveals a more nuanced picture. The discrepancy likely stems from how “midline crossing” is defined and evaluated. Previous studies often employed a binary classification (crossing vs not crossing). In contrast, our three-group grading system specifically differentiated between a uniform, bilateral distribution (Group A) and an asymmetric or limited distribution that merely passes the midline (Group B). Our findings indicate that the superior outcomes in Groups A and B are not solely due to crossing the midline per se, but are critically dependent on achieving a balanced and sufficient volumetric filling that restores biomechanical symmetry. A mere “touch” of cement across the midline, without adequate and even dispersion, may be insufficient to confer the biomechanical advantages. Therefore, our conclusions do not outright contradict but rather refine the previous understanding by emphasizing the qualitative aspect of cement distribution beyond a simple binary threshold.
At present, the optimal bone cement distribution cannot be determined. Therefore, this study explores the optimal bone cement distribution state for treating OVCFs by comparing three different distributions of bone cement. PVP surgery for elderly OVCFs can help relieve pain immediately after surgery. The reason is that after the cement is injected into the vertebrae, it can spread along the fracture site in a liquid state, playing an adhesion effect, making the fracture stable, and after solidification, it can increase the strength of the vertebrae, so that the vertebrae can withstand axial stress without further compression and deformation. At the same time, bone cement can produce thermal effects at the fracture site, and high temperature destroys the painful nerve endings of the fracture site, thereby achieving a good pain relief effect. Our study shows that patients in Group A were significantly better than patients in Group C at 6 months and 1 year after surgery, indicating that uniform bone cement distribution can reduce postoperative pain, improve patient quality of life, and improve patient satisfaction with surgery. Yu et al21 reported that evenly distributed bone cement state may cause less pain. Qi Zhenliang et al22 reported that when the bone cement filling exceeded the midline, the patients’ ODI and VAS scores improved significantly compared with preoperatively (P<0.01). In addition, some studies believe that injecting a larger amount of bone cement within a certain range can enable patients to obtain better pain relief and imaging indicators in the short term.23 There are also reports that when the amount of bone cement is injected is constant, the better the diffusion effect, the larger the volume, the greater the diffusion volume ratio of bone cement, and it is relatively better to relieve pain after surgery.24 In combination with our experimental results, patients in Group A had the largest amount of bone cement dose and uniform distribution of bone cement. Compared with Group C, patients in Group A had lower pain scores, vertebral height and vertebral height recovery rate.
Our results demonstrate a clear positive clinical effect associated with adequate cement distribution. Specifically, Patients in Groups A and B exhibited a statistically significant and clinically meaningful advantage over those in Group C, manifested as superior vertebral height restoration and a markedly lower overall refracture rate. The direction of this effect underscores that achieving cement distribution beyond the midline (as in Groups A & B) is a key determinant of better structural outcomes and long-term durability of the repair. Clinically, this translates to a reduced need for revision surgery, better maintenance of spinal alignment, and potentially a lower risk of chronic pain and disability for the patient. Previous research on bone cement has found that when the asymmetric distribution of bone cement (such as unilateral and uneven distribution) is found in the vertebral body, it will not only destroy the stress balance in the vertebral body, but also destroy the stress conduction trend of the spinal segment, which will lead to new spinal fractures or scoliosis after surgery.25,26 However, since unilateral PVP surgery has the characteristics of uneven distribution of bone cement on both sides of the vertebral body, it is relatively difficult to achieve bone cement exceeding the midline of the vertebral body and evenly distributed during surgery, which may increase the surgical time and increase the patient’s trauma; in addition, excessive distribution of bone cement may lead to excessive stability of the vertebral body, thereby affecting the physiological curvature and range of movement of the vertebral body. Additionally, if the cement touches the nerve root or spinal cord of the vertebral body, it may lead to nerve damage or other complications.
There are certain limitations in this trial: ① Due to the diversity of patients, medical conditions, surgical methods, research methods, follow-up time and other variable factors, the reliability of the above conclusions still needs to be confirmed by further prospective studies; ② The grouping method of this study is different from previous studies, which may lead to subjective deviations in the results; ③ This study is a single-center retrospective study. If you want to further study the correlation between the distribution of bone cement and the efficacy of surgery, large sample size and multi-center studies are required.
Conclusions
In this retrospective cohort study, a bone cement distribution that crossed the vertebral midline was associated with significantly lower long-term postoperative pain scores, better vertebral height recovery, and a reduced incidence of refractures compared to a distribution confined largely to the puncture side. However, the extent to which the cement filled the vertebral body (specifically, whether it exceeded two-thirds) did not show a significant association with the key clinical outcomes measured, suggesting that achieving midline crossing is more critical than maximizing the filler volume alone.
Abbreviations
OVCFs, Osteoporotic vertebral compression fracture; PVP, Percutaneous vertebroplasty; BMI, Body mass index; PFH, Preoperative fractured vertebral body height; PRH, Postoperative restored vertebral body height; LKA, Local kyphosis angle; ODI, Oswestry disability index; VAS, Visual analogue scale; LOS, length of stay.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of the Sixth Affiliated Hospital of Xinjiang Medical University; All patients gave informed consent.
Acknowledgments
The authors sincerely thank the entire staff of the Department of Spinal Surgery, the Sixth Affiliated Hospital of Xinjiang Medical University, for their assistance throughout the study.
Author Contributions
Alimujiang Yusufu and Paierhati Yasheng contributed equally to this work, as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Long Y, Yi W, Yang D. Advances in vertebral augmentation systems for osteoporotic vertebral compression fractures. Pain Res Manag. 2020;2020:3947368. doi:10.1155/2020/3947368
2. Li Y, Tian J, Ge M, et al. A worldwide bibliometric analysis of published literature on osteoporosis vertebral compression fracture. J Pain Res. 2022;15:2373–10. doi:10.2147/JPR.S375119
3. Yao K, Chen Y, Wang X, et al. Correlation analysis between residual pain after vertebral augmentation and the diffusion distribution of bone cement: a retrospective cohort study. Pain Res Manag. 2023;2023:1157611. doi:10.1155/2023/1157611
4. Xu Z, Hao D, Dong L, et al. Surgical options for symptomatic old osteoporotic vertebral compression fractures: a retrospective study of 238 cases. BMC Surg. 2021;21(1):22. doi:10.1186/s12893-020-01013-1
5. Johnston CB, Dagar M. Osteoporosis in Older Adults. Med Clin North Am. 2020;104(5):873–884. doi:10.1016/j.mcna.2020.06.004
6. Moldovan F. Bone cement implantation syndrome: a rare disaster following cemented hip arthroplasties-clinical considerations supported by case studies. J Pers Med. 2023;13(9):1381. PMID: 37763149; PMCID: PMC10532717. doi:10.3390/jpm13091381
7. Li X, Lu Y, Lin X. Refracture of osteoporotic vertebral body after treatment by balloon kyphoplasty: three cases report. Medicine. 2017;96(49):e8961. doi:10.1097/MD.0000000000008961
8. Abduwur H, Korkel K, Yusuf A, et al. Effects of unilateral percutaneous vertebroplasty cement distribution on the efficacy of vertebral compression fracture repair. Chin J Tissue Eng. 2025;29(10):2015–2022.
9. Wei Y, Baskaran N, Wang HY, et al. Study of polymethylmethacrylate/tricalcium silicate composite cement for orthopedic application. Biomed J. 2023;46(3):100540. doi:10.1016/j.bj.2022.05.005
10. Szkoda-Poliszuk K, Załuski R. A comparative biomechanical analysis of the impact of different configurations of pedicle-screw-based fixation in thoracolumbar compression fracture. Appl Bionics Biomech. 2022;2022:3817097. doi:10.1155/2022/3817097
11. Jianmin Y, Jianguo F, Nengfeng M, et al. Comparison of the efficacy of bilateral approach PVP and lateral hole injection combined with modified fluoroscopic unilateral approach PVP in the treatment of thoracolumbar osteoporotic fractures. BMC Surg. 2025;25(1):263. doi:10.1186/s12893-025-02985-8
12. Clark W, Bird P, Gonski P, et al. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2016;388(10052):1408–1416. doi:10.1016/S0140-6736(16)31341-1
13. Wang Y, Liu B, Sun Z, et al. Comparative efficacy of three minimally invasive procedures for Kümmell’s disease: a systematic review and network meta-analysis. Front Surg. 2022;9:893404. doi:10.3389/fsurg.2022.893404
14. Lv B, Ji P, Fan X, et al. Clinical efficacy of different bone cement distribution patterns in percutaneous kyphoplasty: a retrospective study. Pain Physician. 2020;23(4):E409–e16.
15. Bousson V, Guinebert S, Odri G, et al. Curved discography needle for percutaneous cervical spine vertebroplasty: a technical note. J Vasc Interv Radiol. 2020;31(4):686–689. doi:10.1016/j.jvir.2019.10.013
16. Zhou C, Huang S, Liao Y, et al. Correlation analysis of larger side bone cement volume/vertebral body volume ratio with adjacent vertebral compression fractures during vertebroplasty. Front Endocrinol. 2023;14:1072087. doi:10.3389/fendo.2023.1072087
17. Yuntao L, Haibier A, Kayierhan A, et al. Clinical effect analysis of unilateral percutaneous vertebral cement distribution in the repair of osteoporotic thoracolumbar vertebral compression fractures. BMC Surg. 2025;25(1):90. doi:10.1186/s12893-025-02820-0
18. Haibier A, Jie Y, Yusufu A, et al. Effect of different cement distribution on the clinical efficacy of vertebral compression fractures in unilateral percutaneous vertebroplasty. Eur Spine J. 2025;34(5):1673–1684. doi:10.1007/s00586-024-08630-x
19. Franc J, Lehmann P, Saliou G, et al. [Vertebroplasty: 10 years clinical and radiological follow-up]. J Neuroradiol. 2010;37(4):211–219. doi:10.1016/j.neurad.2009.10.004
20. Chen B, Xie D, Li Y, et al. Effect of unilateral PKP cement injection with midline distribution on stiffness of vertebral body on both sides in compression fracture. J Chin Spinal Cord Spinal Cord. 2011;21(2):118–121.
21. Yu D, Wang X, Kou D, et al. Clinical observation on bone cement distribution and residual low back pain after percutaneous vertebral body formation. Chin J Orthop Trauma. 2024;37(11):1075–1079.
22. Qi Z, Li W, Yu Y, et al. Comparison of efficacy of unilateral and bilateral percutaneous vertebral body formation for treatment of thoracolumbar osteoporotic compression fractures. J Cervical Lumbar Pain. 2016;37(6):501–503.
23. Wang M, Fu Z, Wang H, et al. Different bone cement doses for percutaneous vertebroplasty in the treatment of osteoporotic thoracolumbar compression fractures. J Spinal Surg. 2020;18(4):217–21,36.
24. Wang ZW, Wang GY, Liu DK, et al. Risk factors for residual back pain after PVP treatment for osteoporotic thoracolumbar compression fractures: a retrospective cohort study. World Neurosurg. 2023;180:e484–e93. doi:10.1016/j.wneu.2023.09.094
25. Haibier A, Yusufu A, Lin H, et al. Effect of different cement distribution in bilateral and unilateral Percutaneous vertebro plasty on the clinical efficacy of vertebral compression fractures. BMC Musculoskelet Disord. 2023;24(1):908. doi:10.1186/s12891-023-06997-4
26. Liebschner MA, Rosenberg WS, Keaveny TM. Effects of bone cement volume and distribution on vertebral stiffness after vertebroplasty. Spine. 2001;26(14):1547–1554. doi:10.1097/00007632-200107150-00009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.