Back to Journals » Integrated Pharmacy Research and Practice » Volume 15
The Impact of Bilingual Communities on the Effective Communication Process in Open-Circuit Pharmacies: A Quantitative Study to Overcome Language Barriers in Patient Care from Eastern Region of Romania
Authors Ferțu DI ![]() , Elisei AM, Stolerașu LI, Țigănașu A, Ștefan CS, Dinu AC
, Elisei AM, Stolerașu LI, Țigănașu A, Ștefan CS, Dinu AC ![]() , Matei MN, Nechita A, Lupoae M, Iacob A
, Matei MN, Nechita A, Lupoae M, Iacob A ![]()
Received 6 December 2025
Accepted for publication 14 April 2026
Published 15 May 2026 Volume 2026:15 583805
DOI https://doi.org/10.2147/IPRP.S583805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Walid Al-Qerem
Ionela Daniela Ferțu,1 Alina Mihaela Elisei,1 Lavinia Ioana Stolerașu,1 Andreea Țigănașu,1 Claudia Simona Ștefan,1 Adrian Ciprian Dinu,2,3 Mădălina Nicoleta Matei,2,3 Aurel Nechita,2,3 Mariana Lupoae,1 Ancuța Iacob1
1“Dunarea de Jos” University of Galati, Department of Pharmaceutical Science, Research Centre in the Medical-Pharmaceutical Field, Faculty of Medicine and Pharmacy, Galati, Romania; 2“Dunarea de Jos” University of Galati, Clinical Medical and Dental Medical Department, Research Centre in the Medical-Pharmaceutical Field, Faculty of Medicine and Pharmacy, Galati, Romania; 3“Sf. Ioan” Emergency Clinical Hospital for Children, Galati, Romania
Correspondence: Ancuța Iacob, “Dunarea de Jos” University of Galati, Faculty of Medicine and Pharmacy, Research Centre in the Medical-Pharmaceutical Field, Department of Pharmaceutical Science, Galati, Romania, Tel +40740072260, Email [email protected]
Background: Effective pharmacist-patient communication is essential for modern pharmaceutical services, relying heavily on optimized communication strategies that are essential for ensuring treatment adherence and overcoming the unique challenges of patient care in multilingual regions.
Purpose: This study investigates the perceptions, experiences, and strategies used by community pharmacists in Romania to overcome common communication barriers.
Methods: The research employed an observational, descriptive, cross-sectional study design, utilizing a self-administered online questionnaire. The data was collected through an anonymous online questionnaire (N=150) administered to patients in eastern Romania. Explicit digital informed consent was obtained. Data analysis involved descriptive statistics, t-tests for independent samples, and Spearman correlation coefficient.
Results: Results indicate the perception of significant barriers, notably differences in educational levels, the use of medical terminology, and time constraints. A negative and significant Spearman correlation (ρ = − 0.207, p < 0.001) was found between the perceived effectiveness of communication and the need for service improvement, confirming the detrimental impact of these difficulties on the quality of pharmaceutical services. Furthermore, the average self-assessment score of 2.59 for communication training suggests a predominantly negative perception of both university and continuing education in this area.
Conclusion: The conclusions highlight an urgent need to integrate culturally and linguistically adapted communication training into the education of community pharmacists. Future research should focus on developing and evaluating pilot educational programs and interventions specifically tailored for bilingual communities.
Keywords: communication, language barriers, pharmaceutical care, patient, pharmacist, minorities
Introduction
Effective communication in community pharmacies is essential for quality care and patient safety, going beyond simple information about medicines and becoming a process of personalized counselling.1,2 In linguistically and culturally diverse contexts, barriers often arise that impact treatment adherence and therapeutic outcomes.3 Figure 1 illustrates how language barriers influence the communication channel between the pharmacist and the patient.4 For example, Romania has four major ethnic communities: Romanian, Roma, and Hungarian, as well as Russian, especially in the context of the war taking place near the borders with Romania, which makes communication difficult in certain social contexts, such as tourist areas and during tourist seasons.
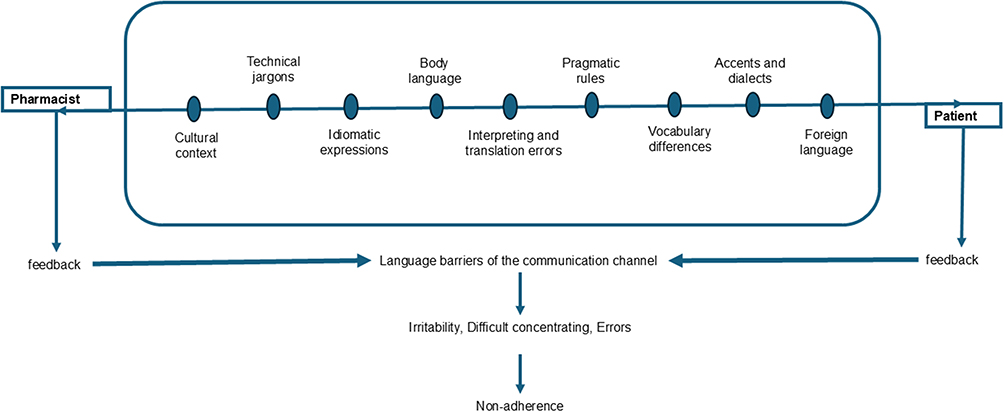 |
Figure 1 Types of language barriers that disrupt communication between patients and pharmacists. |
The literature emphasizes the importance of adapting language and checking patient understanding as part of two-way communication, highlighting the risks associated with poor communication, such as administration errors and reduced compliance.5,6 Recent studies have highlighted the influence of cultural values and norms on the perception of illness and the therapeutic relationship, showing how linguistic minorities face the risk of exclusion due to language barriers and inaccessible jargon.3,7 In multilingual communities, simply knowing the official language does not guarantee understanding of medical and pharmaceutical terminology, highlighting the need for adapted cultural and linguistic strategies.8,9
In both clinical and community pharmacies, a series of methods and techniques adapted and used to optimize the exchange of information between sender and receiver are essential. These action plans are called communication strategies, which, in the context of public health, are evaluated by the clarity of the medical information decoding process, transforming specialized language into an accessible and inclusive information vector.10 There is growing concern for strategies that reduce communication barriers in community pharmacies, such as simplifying language, avoiding jargon and using infographics tailored to the patient’s profile.11–13 Research shows that training pharmacists improves counselling and treatment adherence.14 However, few studies have specifically analyzed the challenges faced by minority communities in Romania in this context.
Given this gap in the literature, we considered it necessary to conduct research focused on strategies applicable in community pharmacies in bilingual regions of Romania, where Hungarian patients encounter specific difficulties in accessing pharmaceutical information. The choice of topic is motivated by clinical observations reported in the literature showing that language barriers reflect deep cultural differences, affecting trust and health behaviors, with direct implications for safety and equity in healthcare.13,15,16
From this perspective, our study makes an original contribution by focusing on the specific needs of a significant linguistic minority in Romania. The novelty of our research lies in the proposal and analysis of strategies adapted to the local context, which include not only the simplification of medical language, but also the integration of culturally relevant visual explanations, the use of bilingual information materials and the training of pharmacists in intercultural communication skills. Compared to other works that address the issue of language barriers in a general manner, our research highlights the particularities of Transylvanian regions with a large Hungarian population and explores how pharmaceutical practices can be adapted to respond to this diversity.17
There is also much discussion in the literature about the risk of oversimplifying language, which may trivialize professional discourse or reduce scientific accuracy.18,19 Our study proposes a balance between clarity and rigor through the development of careful paraphrasing techniques, continuous validation of patient understanding, and the contextualized use of relevant cultural examples. In addition, our research places particular emphasis on the concept of health literacy responsiveness, ie the ability of pharmacists to identify the patient’s level of health literacy and to adapt their communication continuously, avoiding assumptions based on appearances or perceived educational level.20
The working hypotheses of our study were built based on these realities and needs identified in practice and in literature. We started from the premise that linguistic and cultural barriers are significant factors limiting the effectiveness of pharmacistpatient communication from bilingual regions of Romania and that overcoming these barriers requires integrated strategies combining language simplification, the use of adapted visual aids and staff training in intercultural skills. We also assumed that the implementation of these strategies would lead to a significant improvement in the understanding of the message by patients from minority communities, increased adherence to treatment and strengthening of the therapeutic relationship based on mutual trust.
Therefore, our objectives included analyzing specific language barriers encountered in community pharmacies in regions with a significant Hungarian population, assessing the level of understanding of patients according to the communication strategies used, and developing practical recommendations for pharmaceutical staff. Our intention is to contribute to reducing health inequalities and promoting inclusive pharmaceutical practice that is capable of responding to the linguistic and cultural diversity of the communities served. In this way, our work aims not only to document a significant problem, but also to offer concrete and adaptable solutions with direct relevance to the contemporary Romanian healthcare context.
Materials and Methods
Study Design, Population, Setting and Ethical Consideration
Our study is observational, descriptive and cross-sectional, conducted through a self-administered questionnaire addressed to community pharmacists in bilingual regions of Romania. We used a quantitative method, through an online survey, chosen for its accessibility, rapid data collection and ease of analysis. The study used a non-probability convenience sampling technique. This approach was appropriate given the exploratory nature of the research and the geographical and professional specificity of the target population. To minimize selection bias, the survey was distributed through multiple professional platforms and social media groups dedicated to pharmacists in Romania, ensuring a broad reach within the bilingual regions of interest.
The instrument was an original questionnaire created in Google Forms and distributed on social networks and professional groups between 1 August and 30 October 2025 (three months), obtaining 150 voluntary responses from a convenience sample. The online method of submitting the questionnaire allowed for a single completion per user to eliminate the possibility of duplicate responses. Participants were selected based on specific eligibility and inclusion criteria: they had to be actively employed in community pharmacies, belong to a minority community, and give their informed consent to participate.
The study was classified as minimal risk, non-interventional, online questionnaire-based research and was conducted in accordance with the ethical principles of the Declaration of Helsinki. As the study was conducted online and guaranteed the complete anonymity of participants, the Digital Explicit Informed Consent method was used. When accessing the questionnaire link, participants were directed to a mandatory introductory page. This page served as an Information Sheet, detailing the purpose of the study, the participation procedure, the estimated duration, the minimal risks, the participant’s rights, and, crucially, the guarantees of confidentiality and complete anonymity. Access to the questionnaire was conditional upon checking a box that stated: “I have read and understood the above information and give my explicit consent to participate in this study”. Checking this box constituted formal proof of informed consent. It was clearly stated that participation was voluntary and that participants had the right to withdraw at any time by simply closing the browser page, without any consequences. The total anonymity of participants was ensured. This was achieved through the platform’s internal validation system, which requires a one-time sign-in without sharing the user’s identity or Email address with the researchers. No personally identifiable data (names, IP addresses, or Email addresses) were collected. All data collected is aggregated and presented exclusively in the form of statistical analyses. Although the study was classified as low risk and non-interventional, not requiring a formal reference number from a Research Ethics Committee (CEC/IRB), the researchers guarantee that they adhered to all fundamental ethical principles.
Description of the Questionnaire and Validation
The questionnaire was structured into 24 questions grouped into five major sections, as shown in Figure 2. Questions were formulated based on existing literature concerning language barriers and effective communication in pharmacy practice. The instrument was developed and administered in Romanian, as it is the official language of professional practice for all respondents. The draft was reviewed by three experts (two academic pharmacists and one specialist in communication) to ensure the relevance of terms such as complex medical and clinical terminology. A pilot test was conducted with 5 community pharmacists (not included in the final sample) to check for clarity and response time. Minor adjustments were made to the phrasing of “types of effective communication” strategies based on their feedback.
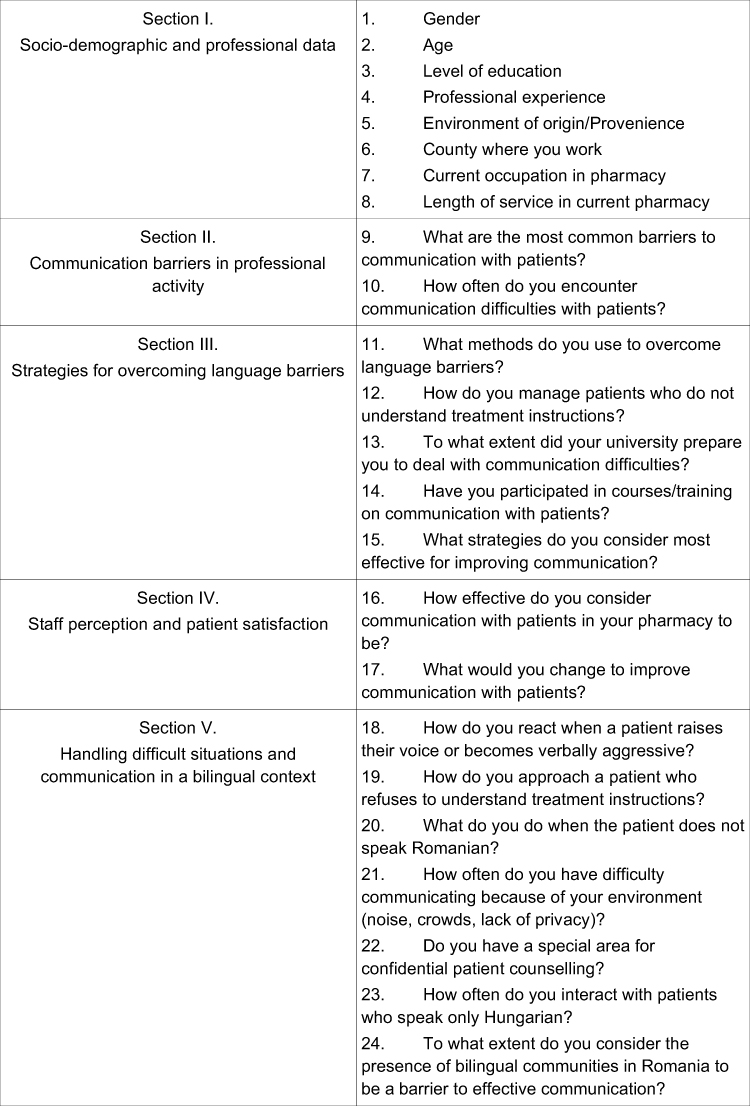 |
Figure 2 The sections of questionnaire. |
Closed-ended questions used for demographic data and frequency of communication difficulties. Specific answering options (Multiple Choice) used for identifying barriers and strategies. For these questions, multiple answers were allowed to capture the complexity of daily practice. Perceptions of training and effectiveness were measured using a 5-point Likert scale. The study was based on three hypotheses: H1 - community pharmacists perceive significant communication barriers in their relationship with patients, such as differences in educational level, medical terminology and the limited time allocated to each consultation; H2 - communication difficulties occur frequently in pharmaceutical practice and negatively influence the quality of services provided and the professional satisfaction of pharmacists; H3 - Most pharmacists consider that university training in patient communication is insufficient and that continuing education in this area is rarely available or inadequate.
Data Analysis
The data obtained from the questionnaire were entered and analyzed using SPSS version 26 and organized with Microsoft Excel. Prior to inferential analysis, the normality of the distribution of the analysed scores was assessed using the Shapiro–Wilk test. The independent-samples t-test was used to compare perceived communication barrier (Q16 and Q17) scores between pharmacists with ≤5 years of professional experience and those with more than 5 years of professional experience. Spearman’s rank correlation coefficient was used to examine the association between Q16 (perceived communication effectiveness) and a recoded improvement score derived from Q17 (perceived need for communication improvement). Q16 was measured on an ordinal scale reflecting pharmacists’ evaluation of communication effectiveness in their pharmacy (very effective to not effective at all). Responses to Q17, which assessed proposed measures for improving pharmacist–patient communication. Statistical significance was set at p < 0.05.
Results
General Characteristics of the Study Population – Demographic Data (Section I)
Table 1 shows a predominance of women among community pharmacists, which may positively influence communication style through empathy and openness. The age distribution highlights a young professional body, mostly under 44 years of age, suggesting flexibility and availability for continuing education. The high level of education reflects a solid foundation of professional training. Vary experience, ranging from newcomers to professionals with over 20 years of experience, ensures a balance between innovation and practical experience. The urban-rural distribution is relatively balanced, allowing for useful comparative observations between different environments. The dominance of Bacău county in the sample suggests a geographical concentration that may influence generalizability.
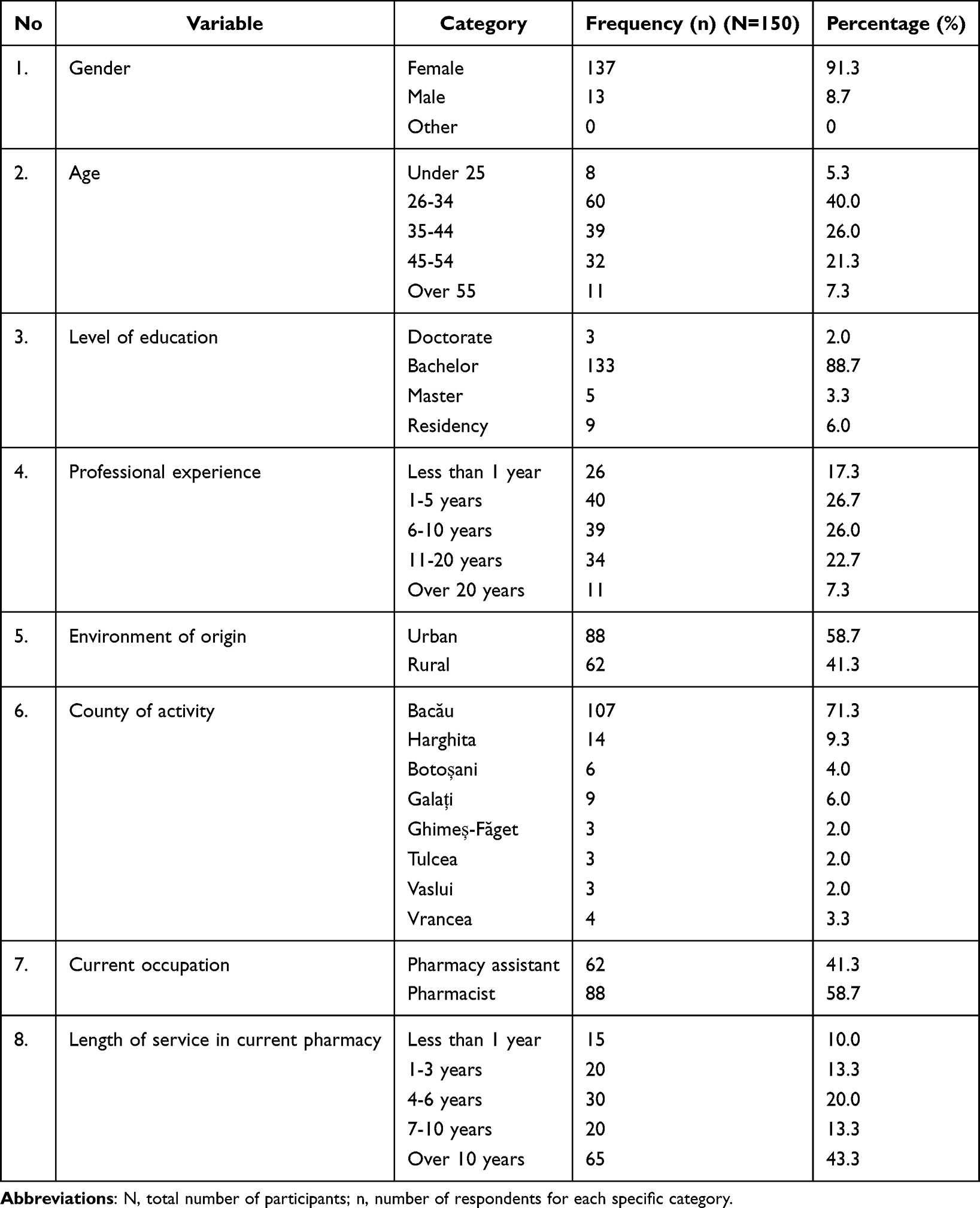 |
Table 1 Socio-Demographic Data of Participants (Section I) |
Perceived Communication Barriers (Section II)
Respondents reported multiple barriers that hinder communication with patients in daily pharmacy practice. When asked about the most common obstacles encountered, pharmacists mainly indicated the difficult attitude of the patient – for example, aggression or distrust (35.3% of responses), followed by an unfavorable working environment (busy or noisy pharmacy – 31.3%) and lack of time for counselling (17.3%). Language differences (patients who speak a language other than Romanian) were mentioned by 8.0% of respondents. In this study, language barriers are defined as the linguistic gap that occurs when the pharmacist and patient do not share a common primary language, leading to a breakdown in the encoding and decoding of medical messages.21 Similarly, the low level of health literacy among some patients (8.0%) directly impacts the understanding of complex medical and clinical terminology, which refers to the patient’s ability to decode specialized pharmacological terms and translate them into actionable health behaviors. These results, detailed in Table 2, confirm that language and educational barriers add to the already known problems related to patient behavior and time or environmental constraints, affecting the quality of the pharmacist-patient interaction. In addition to the nature of the barriers, the perceived frequency of communication difficulties was also assessed. We define communication difficulties as any internal or external interference—whether behavioral, environmental, or semantic—that disrupts the transmission of information and reduces the accuracy of the message during the pharmaceutical act.22 Most pharmacists (≈62%) reported that they “sometimes” encounter difficulties in communicating with patients, while 16% said that such problems occur “frequently” and only 2% “very frequently”. A percentage of 12% indicated that communication barriers occur “very rarely”, and 8% “rarely”.
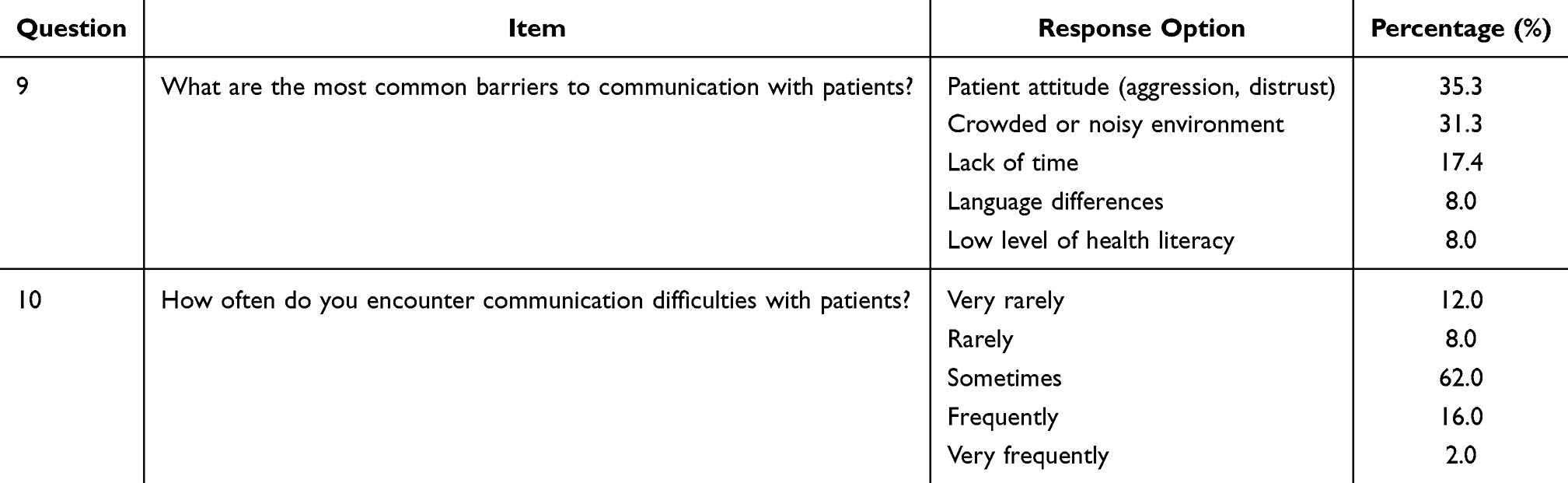 |
Table 2 Distribution of Responses Regarding the Frequency of Barriers and Difficulties Encountered in Communicating with Patients (Section II) |
The communication barriers identified confirm the challenges related to patient attitudes, working conditions and linguistic or literacy differences, highlighting the need for tailored training and organizational strategies in community pharmacies. These barriers are major and affect pharmacists’ ability to communicate effectively with patients, having a direct impact on the quality of care.
Strategies for Overcoming Barriers and Communication Training (Section III)
The third section of the questionnaire investigated how pharmacists try to overcome these barriers, as well as their perceived level of communication training. Respondents predominantly indicated the use of proactive strategies to facilitate patients’ understanding of messages. These strategies are classified as proactive because they represent a deliberate, pre-emptive effort by the pharmacist to ensure effective communication before a misunderstanding can occur.23 By simplifying medical terminology (80.7%) and avoiding technical jargon at the start of the interaction, the pharmacist acts as a “linguistic filter”, anticipating the patient’s potential decoding difficulties. This proactive stance is essential in bilingual contexts, as it shifts the responsibility of understanding from the patient to the professional, thereby reducing the risk of sub-optimal treatment adherence and potential medication errors. This adaptation is a deliberate strategy to guarantee understanding of complex medical and clinical terminology. Pharmacists reported that de-jargonizing involves breaking down pharmacodynamic concepts (eg, systemic effect or adverse reaction) into everyday analogies. By doing so, they bridge the gap between their high-level academic training and the patient’s health literacy, ensuring that the clinical essence of the prescription is not lost in translation. In addition, 12% resort to non-verbal language (gestures, facial expressions) to make themselves understood, and 4% use real-time translation apps on their phones. Only about 3% mentioned that they ask a colleague or a member of the patient’s family for help with translation, and 1.3% said they do not use any special methods to overcome language barriers.
Another practical question concerned how to handle situations where the patient does not understand the treatment instructions (for various reasons, such as difficult-to-understand terms or patient reluctance). These approaches represent different types of effective communication tailored to the patient’s specific needs. While 55.3% rely on verbal communication (repetition and paraphrasing), the use of written communication (15.3% through leaflets) and non-verbal communication (gestures) provides a multi-modal safety net. These diverse communication strategies are not used in isolation; rather, pharmacists often combine them to create a redundant information system that minimizes the risk of medication errors. The overwhelming majority of pharmacists – 55.3% – responded that in such cases they repeat the explanations using different words, patiently, until they are sure that the patient has understood correctly. Another 23.3% use concrete examples or analogies to illustrate the information, thus facilitating understanding. A percentage of 15.3% provide patients with written materials (leaflets, explanatory brochures) that they can consult at home, and 6% use the “teach-back” technique – they ask patients to repeat what they have understood from the explanations in order to check their level of comprehension and correct any misunderstandings. Although only 6% currently use the “teach-back” technique systematically, it was identified as the most robust method to guarantee understanding. By asking patients to explain the treatment in their own words, the pharmacist moves from a passive transmission of information to an active validation of comprehension. This shift is crucial for identifying “hidden” communication difficulties—where a patient might nod in agreement without actually grasping the complexity of the clinical instructions.
Also, this section included questions on pharmacists’ training in communication skills. Only 36% of respondents considered that, during their university studies, they had been prepared to a small extent to deal with communication difficulties with patients, while only 24.7% considered that they had been trained to a large extent and 13.3% to a very large extent. Another 13.3% self-assess their preparation as to a very small extent, and 12.7% remained neutral on this issue. These figures signal pharmacists’ dissatisfaction with their academic training in communication: most perceive that their university did not sufficiently develop these skills, suggesting a need to revise the university curriculum to include communication courses focused on patient relations. Table 3 presents the distribution of responses regarding the strategies used by pharmacists to overcome communication barriers, their approaches when patients do not understand treatment instructions, and their perceptions of communication training during university studies and professional practice. Even though pharmacists are trained during their university studies in pharmacology and medical treatment, their communication skills with patients are not sufficient. Therefore, the educational curriculum needs to be revised to include continuing education courses that develop pharmacists’ communication skills, given the diversity of patients and the complexity of the situations in which they are involved. The perceived insufficiency in university training is particularly evident in the lack of practical modules on how to translate complex medical and clinical terminology for laypeople or minority groups. Respondents suggested that while they possess the scientific knowledge, they lack the formal types of effective communication skills necessary to navigate high-pressure, bilingual contexts or resistant patient behaviors.
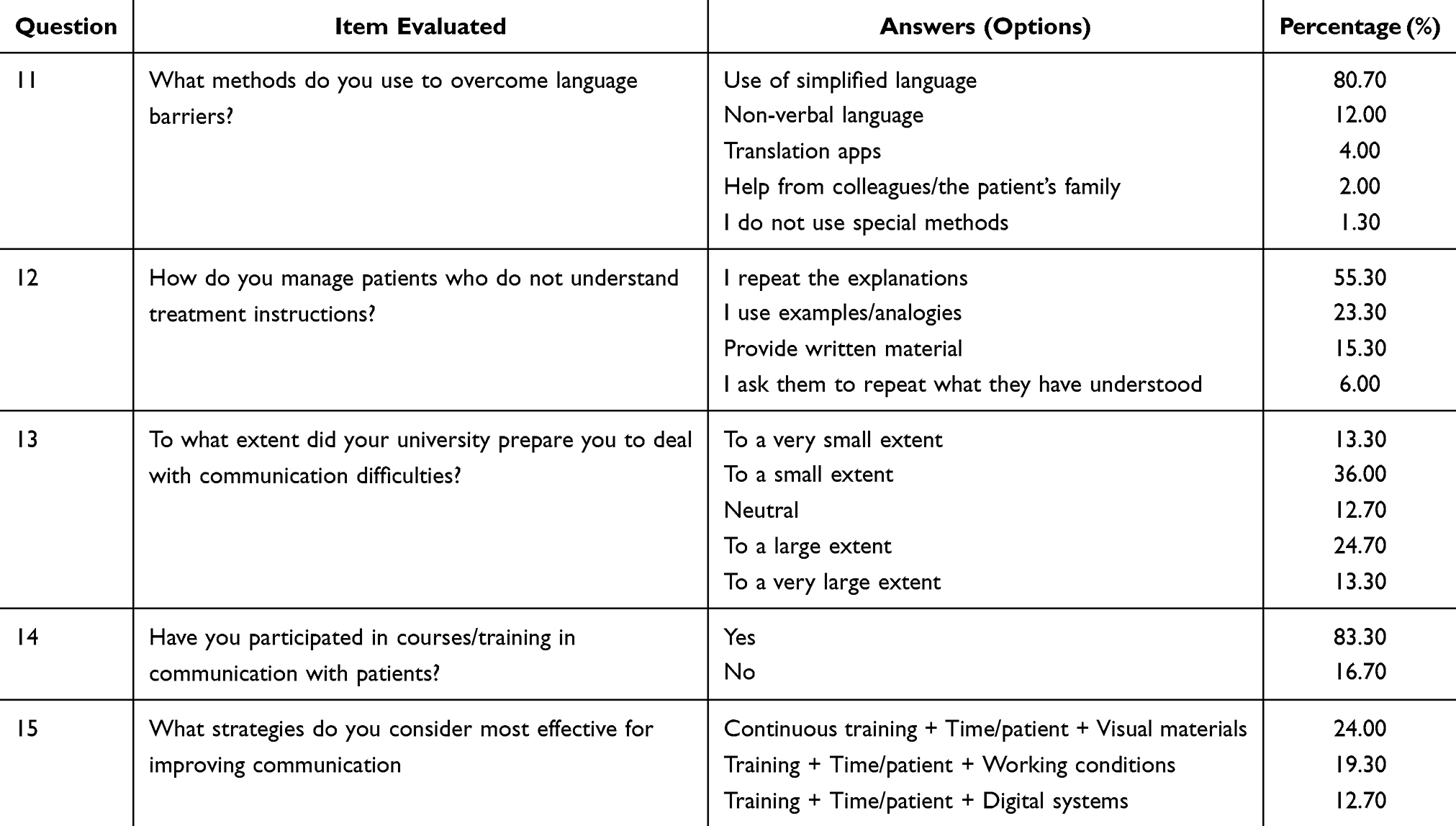 |
Table 3 Methods for Overcoming Communication Barriers and Communication Training (Section III) |
Perception of Communication Effectiveness and Needs for Improvement (Section IV)
In Section IV, participants were asked to rate how effective communication with patients is in their pharmacy and to indicate what they would change to improve it. For the purpose of this research, effective communication is understood as a bidirectional process where the intended message of the pharmacist is accurately received and understood by the patient, resulting in improved treatment adherence.24 This process encompasses various types of effective communication, including verbal (clarity of speech), non-verbal (body language and empathy), and written (clear instructions on prescriptions), all of which are essential for high-quality care.25 The assessment of communication effectiveness was generally optimistic: 60% of pharmacists consider communication in their own pharmacy to be “very effective”, and 24.6% consider it “effective”. The rest rated it as only “moderately effective” (12.7%) or even “not at all effective” (2.7%). In practice, almost 85% of respondents have a positive impression (effective or very effective) of their own communication with patients, which may indicate both confidence in their own abilities and the existence of well-established communication practices in most pharmacies. On the other hand, the small proportion (≈ 3%) who see communication as ineffective suggests that there are also specific problematic situations that require attention. Table 4 shows the complete distribution of of responses regarding pharmacists’ perceptions of communication effectiveness in their pharmacies, as well as the main measures they believe could improve pharmacist–patient communication.
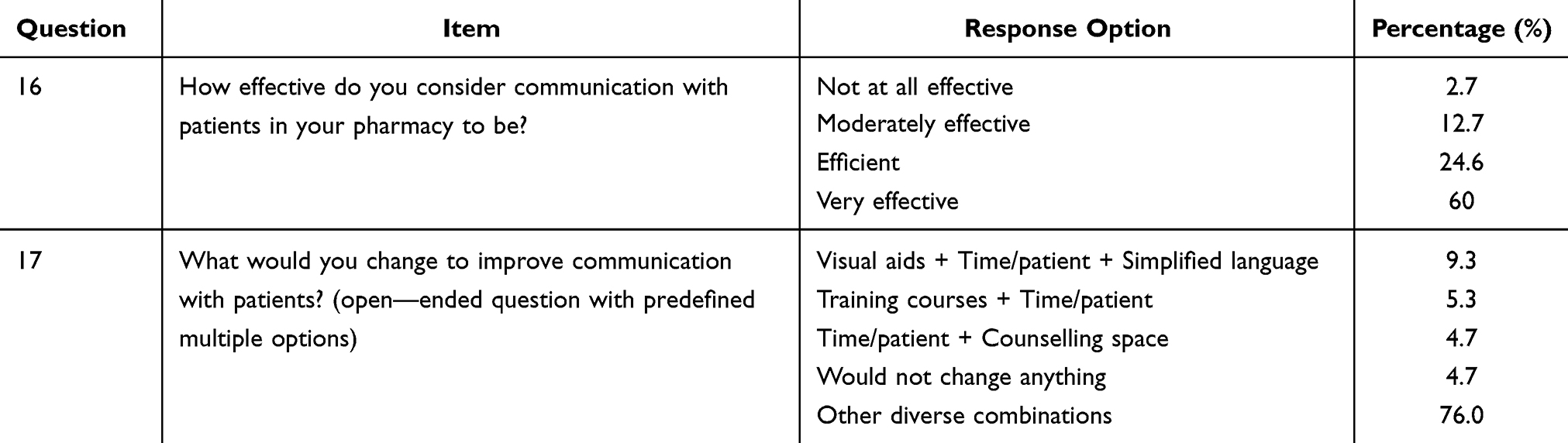 |
Table 4 Distribution of Respondents Regarding the Evaluation of the Communication Process and Ways to Improve It (Section IV) |
When asked what they would change to improve communication with patients, pharmacists provided a variety of answers, often ticking combinations of measures. The most common choice (9.3% of respondents) was a comprehensive approach: “I would introduce visual and written materials tailored to the patient’s level, allocate more time to each patient and reduce the use of complex medical language”. This combined option highlights the emphasis on simplifying and adapting information to the patient (through clear language and visual aids) coupled with the need for sufficient time for counselling. Other notable combinations included: “I would attend training courses and allocate more time per patient” (chosen by 5.3% of the sample) or “I would allocate more time per patient and create a space dedicated to confidential discussions” (4.7%). It should be noted that 4.7% of respondents said they would not change anything, considering the current method of communication to be already effective. These findings were further examined through correlation analysis, which explored the relationship between perceived communication effectiveness and the need for service improvement.
Practical Situations and Communication in a Bilingual Context (Section V)
The last section of the study explored pharmacists’ reactions in specific difficult situations (Table 5), as well as the specific challenges of communicating with patients from minority communities (Hungarians, Roma) or vulnerable patients (eg. those with depression). The results show that many pharmacists adopt a calm and conciliatory attitude when faced with a difficult patient. If a patient raises their voice or becomes verbally aggressive, 98% of pharmacists responded that they try to remain calm and reassure the patient, with only 2% calling for help from a colleague or superior in such situations. This almost unanimous response reflects the professionalism and self-control of pharmacists in tense situations, as they understand that escalating conflict is not beneficial.
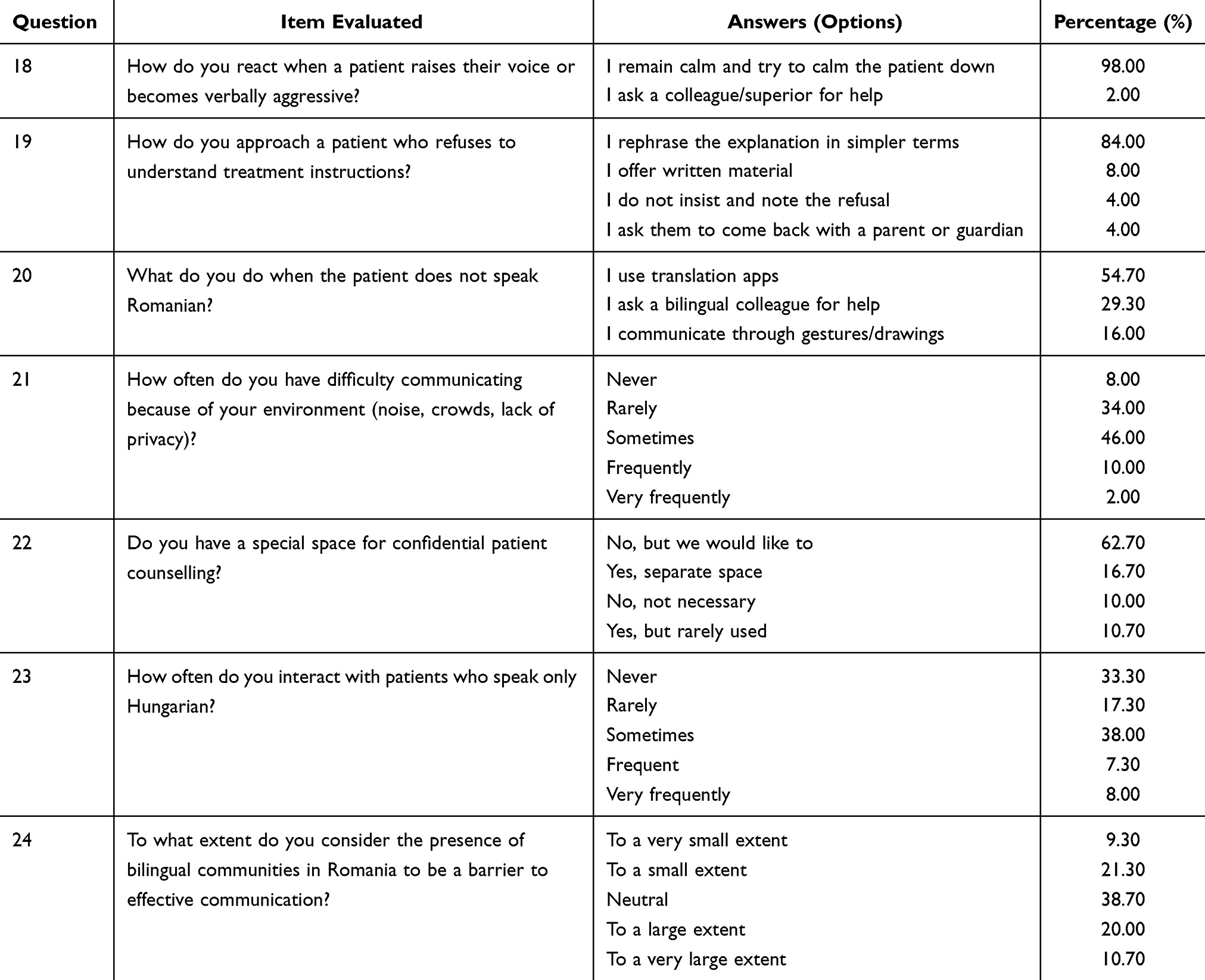 |
Table 5 Handling Difficult Situations and Communication in a Bilingual Context (Section V) |
In the case of a patient who simply does not want to understand or accept explanations about the administration of a medicine, pharmacists focus on clarification and documentation. 84% of respondents said that in such cases, they rephrase the explanation in a simpler way, trying a different communication approach to overcome the patient’s refusal. In addition to this main strategy, 8% provide the patient with written information (for them to reflect on later), and 4% either do not insist and note the refusal in the computer system (thus documenting the patient’s disagreement) or request the presence of a relative or carer who could help the patient better understand the message. These secondary options suggest that, although the pharmacist makes every effort to explain, sometimes it is necessary either to accept a disagreement (and record it in the patient’s file to protect the pharmacist) or to involve the family in the communication process.
Another challenge investigated was the lack of a common language between the pharmacist and the patient – a situation encountered especially in regions where linguistic minorities or foreign tourists live. The question “What do you do when the patient does not speak Romanian?” revealed that 54.7% of pharmacists use translation apps on their phone or computer to communicate with the patient on the spot. At the same time, 29.3% say they ask for help from a colleague who knows the language (eg. a colleague who speaks Hungarian or English, depending on the context), and 16% resort to non-verbal communication, gestures or drawings to understand the patient. It is remarkable that most pharmacists find a solution on the spot (technological, collegial or gestural) to overcome the language barrier, even in the absence of official translated materials – which reflects adaptability, but also the lack of a systematic framework for such situations.
An external factor often blamed for communication difficulties is the physical environment of the pharmacy. Pharmacists were asked, “How often do you experience communication difficulties due to the environment (noise, crowds, lack of privacy)?” Almost half (46%) responded that such problems occur “sometimes”, while 34% said “rarely”, 10% “frequently”, 2% “very frequently” and 8% said they “never” experience difficulties caused by the environment. Thus, about 1 in 8 pharmacists frequently (or very frequently) face communication barriers due to environmental conditions, and most experience them at least occasionally. Background noise and crowding reduce confidentiality and concentration in discussions with patients, which justifies the need for structural improvements, such as specially designed spaces for confidential counselling. In fact, when asked “Do you have a special space for confidential counselling with patients?”, only 16.7% of pharmacists answered “Yes, we have a separate space”, while another 10.7% said “Yes, but it is not used frequently”, and the vast majority do not have such a space (62.7% ticked “No, but we would like to have one”, indicating that they feel its absence, and 10.0% “No, and I don’t consider it necessary”). These data indicate that in over 70% of cases, counselling takes place at the counter, within earshot of others, although pharmacists are aware of the importance of privacy (the majority would like a dedicated space).
A central objective of the research was to understand communication in bilingual regions of Romania, particularly interaction with ethnic Hungarian and Roma patients who do not speak Romanian. When asked, “How often do you interact with patients who speak only Hungarian or Roma?”, responses varied substantially, highlighting regional differences. 33.3% of pharmacists said they “never” had such patients, while 28.0% encountered them “occasionally”, 17.3% “rarely”, 7.3% “frequently” and 8.0% “very frequently”. Six per cent ticked both “rarely, occasionally” (probably indicating an intermediate frequency). These results show that the experience of exposure to Hungarian/Roma-speaking patients varies greatly: approximately one third of pharmacists (probably those in areas without a Hungarian minority) do not encounter this situation at all, while for about 15% it is common (frequent or very frequent). However, more than half of respondents have encountered Hungarian/Roma-only patients at least rarely, which highlights the need for basic language training or Hungarian/Toma-language materials where necessary.
Moreover, when asked “To what extent do you consider the presence of bilingual communities in Romania to be a barrier to effective communication with patients?”, pharmacists gave mixed responses: 38.7% were neutral, probably considering that the issue did not apply in their pharmacies, while 20.0% considered the presence of bilingual communities to be “to a large extent” a barrier and 10.7% “to a very large extent”. At the opposite end of the scale, 21.3% saw this barrier as only “to a small extent” and 9.3% “to a very small extent”. In practice, ~30% of respondents strongly feel the language barrier, highlighting the need for local solutions (hiring bilingual staff, Hungarian language courses for pharmacists, availability of leaflets and displays in minority languages). However, the majority either do not face the problem directly or believe they can cope. The numerous neutral responses reflect a lack of firm opinion, possibly because some pharmacists do not have enough experience with bilingual patients to form an opinion.
Perceived Communication Barriers Among Community Pharmacists
Prior to conducting the independent-samples t-test, the normality of the communication barrier score distribution was assessed using the Shapiro–Wilk test. The results indicated that the distribution of the analysed scores did not significantly deviate from normality (p > 0.05), supporting the use of parametric statistical tests (Table 6). Since the normality assumption was satisfied, an independent-samples t-test was performed to compare perceived communication barrier scores between pharmacists with ≤5 years of professional experience and those with more than 5 years of professional experience.
 |
Table 6 Shapiro–Wilk Test for Normality of Communication Barrier Score |
An independent-samples t-test was conducted to examine differences in perceived communication barrier scores between groups of pharmacists according to professional experience. The analysis revealed a statistically significant difference (t = 5.178, p < 0.001), indicating that pharmacists’ perceptions of communication barriers vary significantly between the compared groups. These results support Hypothesis H1 (Community pharmacists perceive significant communication barriers in their relationship with patients, such as differences in educational level, medical terminology and the limited time allocated to each consultation) suggesting that community pharmacists perceive substantial communication barriers in their interactions with patients, including differences in educational level, the use of medical terminology, and limited consultation time (Table 7).
 |
Table 7 Results of the t-Test for Independent Samples on the Perception of Communication Barriers Among Community Pharmacists |
Relationship Between Communication Effectiveness and the Need for Service Improvement
Table 8 presents and confirm hypothesis H2: Communication difficulties occur frequently in pharmaceutical practice and negatively influence the quality of services provided and the professional satisfaction of pharmacists.
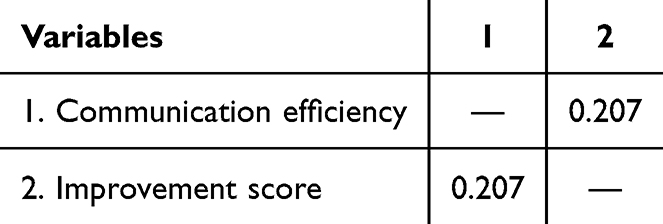 |
Table 8 Spearman Correlation Between Perceived Communication Effectiveness and Perceived Need for Improvement in Pharmaceutical Services |
Spearman’s rank correlation analysis was performed to assess the relationship between Q16 (perceived communication effectiveness) and the recoded improvement score derived from Q17, representing pharmacists’ perceived need for improving communication practices. The results revealed a weak but statistically significant negative correlation (ρ = −0.207, p < 0.001). This finding indicates that pharmacists who perceive communication with patients as less effective are more likely to consider that improvements in pharmaceutical services are necessary.
Perception of Communication Training Among Pharmacists
The mean score for perceived communication training was 2.59 (SD = 1.19) on a five-point scale, indicating a moderately negative evaluation of the adequacy of communication training received during university education. These findings support Hypothesis H3 (Most pharmacists consider that university training in patient communication is insufficient and that continuing education in this area is rarely available or inadequate), suggesting that many pharmacists perceive gaps in their formal training related to patient communication. The results highlight the need to strengthen communication skills training both during university education and through continuing professional development programmes (Table 9).
 |
Table 9 Descriptive Statistics on the Perception Score of Training in Pharmacist-Patient Communication |
Discussion
The results obtained highlight the importance of adapted communication in community pharmacies, especially when interacting with patients belonging to minority communities. The pharmacists interviewed report a high frequency of interactions with bilingual patients, noting difficulties such as lack of openness, vague expression of symptoms or refusal to engage in dialogue, issues that require specific strategies for empathetic and clear communication. To address these communication difficulties, pharmacists report using various types of effective communication, ranging from verbal strategies, such as simplifying language, repeating explanations, and checking understanding through interactive methods such as “teach-back”.26 The reported use of the “teach-back” method by pharmacists in our study is supported by a systematic review conducted by Ha Dinh et al, which analyzed 20 studies and found the technique to be effective in 19 out of 20 cases. Their findings demonstrate that teach-back significantly improves knowledge recall and retention, as well as objective health outcomes such as quality of life. This reinforces our argument that interactive verification of understanding is a superior proactive strategy compared to simple information delivery.27
In bilingual regions, the language barrier is perceived as a major obstacle to effective communication with patients from minority communities. Respondents indicate that, despite the use of translation apps or support from colleagues, linguistic differences limit the clarity of the message conveyed. Many consider the availability of information materials translated into Hungarian to be essential, emphasizing that a mere working knowledge of Romanian does not guarantee understanding of complex medical terminology. This suggests that even when language barriers are partially overcome, a secondary semantic barrier remains, where the technicality of the pharmaceutical act exceeds the patient’s health literacy. This phenomenon is well-documented in recent literature, which emphasizes that linguistic access does not guarantee conceptual understanding if the information is not aligned with the patient’s cognitive health literacy level.28–30
To address the identified language barriers, several systemic solutions are proposed. First, the integration of visual communication strategies, such as pharmaceutical pictograms, is essential to guarantee understanding when verbal fluency is lacking. Ros Dowse et al’s study showed that pictograms significantly improve medication adherence and understanding in populations with low literacy or language barriers by providing a universal symbolic language.31
Second, leveraging digital tools like QR-coded translated leaflets can bridge the gap in understanding of complex medical and clinical terminology.32 Recent evidence suggests that digital interventions and scannable information provide patients with on-demand, linguistically appropriate resources that enhance safety in outpatient care.33
Finally, fostering a “cultural mediation” approach—where pharmacists are trained in basic minority-language medical terms—transforms a potential communication difficulty into an opportunity for high-quality, equitable care.34 Training healthcare providers in culturally competent communication and basic minority-language terms has been shown to reduce health disparities and increase patient trust in multicultural settings.21 The pivotal role of the pharmacist as a “bridge” within fragmented healthcare systems is further validated by recent observational research conducted in Flanders, Belgium. Similar to our findings, the Belgian study highlights that pharmacists frequently employ adaptive communication practices to overcome the “dual logic” of retail pressure and clinical care. Specifically, their observation that pharmacy layout and staff composition (meso-level factors) dictate the quality of interaction aligns with the 31.3% of our respondents who identified environmental constraints as a primary obstacle. Furthermore, the necessity for systemic policy support and structured training—rather than relying solely on the pharmacist’s personal motivation—echoes our conclusion that university curricula must evolve to include intercultural competencies. By addressing these socio-economic and linguistic challenges through a proactive, “cultural mediation” approach, the community pharmacy transcends its traditional role, becoming a critical site for achieving health equity in multicultural and bilingual regions.34
Working conditions are an additional barrier, with pharmacists reporting difficulties caused by noise, crowding and lack of privacy for counselling. Our finding that 35.3% of pharmacists face patient aggression aligns with studies by Hilal İlbars et al, who noted that high-pressure environments in community pharmacies often lead to diminished patient trust.35 This lack of trust, combined with environmental stressors, complicates the delivery of the pharmaceutical act.
Furthermore, when addressing the linguistic gap, the choice of strategy reflects a specific professional culture. While some international literature suggests that digital translation tools are the primary solution for linguistic gaps, our results contradict this, showing that 80.7% of Romanian pharmacists still rely on manual simplified language.36 This suggests that in the local context, human-led proactive strategies are perceived as more reliable than current technological aids, possibly due to the need for immediate, empathetic rapport which a screen cannot yet replicate.
In this context, the use of dedicated spaces for confidential counselling and managerial support to optimize workflows.37 At the same time, although many have attended communication courses, there is a general perception that university training is insufficient to cope with the real challenges in community pharmacies.38
Our study confirms the need for a dynamic model of cultural competence in pharmaceutical communication, based on continuous learning and reflexivity. Recognizing cultural differences is not just about translating words, but also about adapting the content, form and tone of the message to the patient’s values and expectations. The results also suggest the importance of exploring the patient’s experiences narratively, actively listening to their history of illness, previous treatments and social barriers encountered. In Hungarian or Roma communities, the ability to express oneself in one’s mother tongue is not just a matter of clarity, but a gesture of cultural respect and a means of reducing anxiety related to interaction with the healthcare system.
Adapting communication in community pharmacies is not only a strategy for professional efficiency, but an ethical act.39 Achieving effective communication in these complex settings ensures that the therapeutic goals are aligned between the provider and the patient, directly impacting the quality of services provided and equity in access to healthcare. Pharmacists who develop empathic and intercultural communication skills can help reduce health disparities and strengthen patient trust in the pharmaceutical system, especially in bilingual regions where language and cultural barriers remain a significant challenge.40
In conclusion, the transition from simple interactions to effective communication requires both overcoming language barriers and translating concepts from complex medical terminology into accessible language.
Strengths and Limitations
This study is among the few to explore the specific intersection of medical terminology and bilingualism in Romanian community pharmacies. The use of a targeted sample in regions with significant minority populations (Hungarian and Roma) provides high ecological validity to the findings. The sample size (N=150) may limit the generalizability of the results to the entire national territory. Furthermore, the use of self-reported data may introduce social desirability bias, where pharmacists might over-report the use of proactive strategies like “teach-back”.
Implications for Practice and Research
Pharmacy managers should not only invest in translation apps but also in visual communication tools (pictograms) and private counseling areas to reduce the “noise” barrier identified by 31.3% of respondents. Future studies should employ mixed-methods, combining surveys with direct observation (shadowing) to see if the “simplified language” reported by pharmacists effectively translates into better patient adherence.
Conclusion
This study demonstrates that effective communication in community pharmacies, particularly in the bilingual and multicultural regions of Romania, is not merely a social skill but a critical clinical intervention. Our research identifies a clear hierarchy of challenges: while language barriers and crowded working conditions create the initial friction, a deeper secondary semantic barrier remains even when basic linguistic gaps are closed.
The findings confirm that pharmacists predominantly rely on human-led proactive strategies, such as the “teach-back” method and linguistic simplification, which are perceived as more effective and culturally resonant than current digital translation tools. However, the perceived insufficiency of university training and the significant impact of environmental factors (noise and lack of privacy) underscore that individual motivation is not enough.
To ensure medication safety and treatment adherence, especially for vulnerable groups, several systemic changes are required. First, the integration of visual communication aids (eg, pictograms) and translated QR-coded materials must be standardized to support low-health-literacy populations. Second, institutional policies must prioritize the creation of dedicated counseling spaces to mitigate the environmental barriers identified by 31.3% of our respondents.
In conclusion, transitioning from simple interaction to effective communication requires a transition from discretionary actions to a structured model of intercultural pharmaceutical care. This paper provides a framework for both educational reform in pharmacy curricula and for authorities to develop targeted training programs. Ultimately, fostering these skills is an ethical imperative that ensures equity, safety, and cultural respect, strengthening public trust in the healthcare system.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Michael E, Nurahmed A, Mihreteab H, et al. Patient-centered communication among pharmacy professionals working in hospitals and drug retail outlets in asmara, eritrea: knowledge, attitude, self-efficacy and barriers. IPRP. 2022;11:153–16. doi:10.2147/IPRP.S363931
2. Rusu A, Chereches MC, Popa C, Botezatu R, Lungu IA, Moldovan OL. Community pharmacist’s perspective regarding patient-centred communication in conjunction with pharmaceutical practice: a cross-sectional survey. Saudi Pharm J. 2022;30(9):1327–1344. doi:10.1016/j.jsps.2022.06.014
3. Al Shamsi H, Almutairi AG, Al Mashrafi S, Al Kalbani T. Implications of language barriers for healthcare: a systematic review. Oman Med J. 2020;35(2):e122. doi:10.5001/omj.2020.40
4. Buarqoub IAS. Language barriers to effective communication. Utopía y Praxis Latinoamericana. 2019;24(Esp.6):64–77.
5. Glinert LH. Communicative and discursive perspectives on the medication experience. Pharmacy. 2021;9(1):42. doi:10.3390/pharmacy9010042
6. Keller MS, Carrascoza-Bolanos J. Pharmacists, nurses, and physicians’ perspectives and use of formal and informal interpreters during medication management in the inpatient setting. Patient Educ Couns. 2023;108:107607. doi:10.1016/j.pec.2022.107607
7. Hayakawa S, Pan Y, Marian V. Language changes medical judgments and beliefs. Int J Bilingualism. 2022;26(1):104–121. doi:10.1177/13670069211022851
8. Jeong H, Lindemann S. Facilitating or compromising inclusion? Language policies at Swedish higher education institutions as workplaces. Multilingua. 2024;43(3):365–395. doi:10.1515/multi-2023-0077
9. Harrison R, Walton M, Chitkara U, et al. Beyond translation: engaging with culturally and linguistically diverse consumers. Health Expect. 2020;23(1):159–168. doi:10.1111/hex.12984
10. Shadrach I. Strategic communication: meaning, origin, principles, and practice. Commun Media Stud. 2023;593–607.
11. Filmer T, Ray R, Glass BD. Barriers and facilitators experienced by migrants and refugees when accessing pharmaceutical care: a scoping review. Res Soc Administrative Pharm. 2023;19(7):977–988. doi:10.1016/j.sapharm.2023.02.016
12. López-Pintor E, Gómez-Ramos A, Sanz-Valero J. Antibiotic infographics available on the internet: documentary quality, purpose, and appropriateness as educational tools on antimicrobial resistance. Antibiotics. 2023;12(3):462. doi:10.3390/antibiotics12030462
13. Tan R, Kawaja A, Ooi SP, Ng CJ. Communication barriers faced by pharmacists when managing patients with hypertension in a primary care team: a qualitative study. BMC Prim Care. 2024;25(1):100. doi:10.1186/s12875-024-02349-w
14. Sholihah S, Rahayu FP, Farhana L, Alshehri S, Alfian SD, Abdulah R. Pharmacist-led interventions to improve medication adherence among patients with multimorbidity: a scoping review. Patient Prefer Adherence. 2025;19:3589–3602. doi:10.2147/PPA.S542881
15. Al Mutairi F. Language barriers and their impact on effective communication in different fields. 2025. doi:10.13140/RG.2.2.29788.09607.
16. Krupić F, Krupić M, Sahra S, et al. Barriers to healthcare access and utilization among immigrants in host countries: a systematic review of qualitative and quantitative evidence. Cureus. 2026;18(2). doi:10.7759/cureus.104278
17. Worakittikul W, Mangdindam T, Ketkaew C, Naruetharadhol P. Breaking barriers: examining the impact of language on employee-driven innovation in European multinational subsidiaries in Thailand. Cogent Arts Humanities. 2025;12(1):2451492. doi:10.1080/23311983.2025.2451492
18. Peprah P, Lloyd J, Harris M. Responding to health literacy of refugees in Australian primary health care settings: a qualitative study of barriers and potential solutions. BMC Health Serv Res. 2024;24(1):757. doi:10.1186/s12913-024-11192-9
19. Pais C, Liu J, Voigt R, Gupta V, Wade E, Bayati M. Large language models for preventing medication direction errors in online pharmacies. Nat Med. 2024;30(6):1574–1582. doi:10.1038/s41591-024-02933-8
20. Marinkovic V, Odalovic M, Tadic I, Krajnovic D, Mandic I, Rogers HL. Person-centred care interventions in pharmaceutical care. In: Intelligent Systems for Sustainable Person-Centered Healthcare. Springer International Publishing Cham; 2022:53–68.
21. Organi ZK, Nazarenia M, Aghaee F. Understanding the challenges of language barriers in healthcare. Interdiscipl Stud Soc Law Politics. 2024;3(3):28–35. doi:10.61838/kman.isslp.3.3.5
22. Rojas-Ocaña MJ, Teresa-Morales C, Ramos-Pichardo JD, Araujo-Hernández M. Barriers and facilitators of communication in the medication reconciliation process during hospital discharge: primary healthcare professionals’ perspectives. Healthcare. 2023;11(10):1495. doi:10.3390/healthcare11101495
23. Delli RM, Kaur J, Lai PSM, Dumanig FP. Self-repair practices in pharmacist-patient interaction and their role in preventing misunderstanding and maintaining medication safety. Respectus Philologicus. 2022;41(46):53–66. doi:10.15388/RESPECTUS.2022.41.46.107
24. Adam B, Ibrahim K, Stevenson F, Leydon G. From theory to practice: a critical review and meta-framework for operationalising person-centredness, therapeutic alliance and empathy in pharmacist-led mental health consultations. Res Soc Administrative Pharm. 2026;22(4):509–529. doi:10.1016/j.sapharm.2025.12.012
25. Rehman U, Amjad Sohail D. Exploring the role of verbal and non-verbal communication skills of nursing in patients’ healing. JPEHSS. 2025;3(4):78–91. doi:10.63163/jpehss.v3i4.741
26. Sleiman AA, Richard EM, Gonzales-Portillo D, Tallman S, Gravina NE. Evaluation of teach-back and plain language acceptability during patient interactions. PEC Innov. 2026;8:100445. doi:10.1016/j.pecinn.2025.100445
27. Talevski J, Wong Shee A, Rasmussen B, Kemp G, Beauchamp A. Teach-back: a systematic review of implementation and impacts. PLoS One. 2020;15(4):e0231350. doi:10.1371/journal.pone.0231350
28. Ngoh L. Health literacy: a barrier to pharmacist-patient communication and medication adherence. J Am Pharm Assoc. 2009;49(5):e132–46. quize147. doi:10.1331/JAPhA.2009.07075
29. Ghaffari M, Bahrambeygi F, Mazar L, Rakhshanderou S. Reconceptualizing health literacy to end confusions: an umbrella review research. Health Sci Rep. 2025;9(1):e71657. doi:10.1002/hsr2.71657
30. Rüegg R. Health literacy: determinant of health or status indicator? 2022.
31. Dowse R, Okeyo S, Sikhondze S, Khumalo N. Pharmaceutical indication pictograms for low literacy viewers: health literacy and comprehension. Health SA. 2023;28:2192. doi:10.4102/hsag.v28i0.2192
32. Barry A, Granger S, Cunningham K, Potter M. QR code use for patient information leaflets: a sustainable, digital innovation. 2024. doi:10.13140/RG.2.2.13345.21601.
33. De Micco F, Di Palma G, Ferorelli D, et al. Artificial intelligence in healthcare: transforming patient safety with intelligent systems—A systematic review. Front Med. 2025;11. doi:10.3389/fmed.2024.1522554
34. Sente C, Foulon V, Kielmann K. Discretion at the margins: an observational study of community pharmacists’ adaptive practices in supporting migrant and ethnic minority health. Exploratory Res Clin Soc Pharm. 2026;22:100715. doi:10.1016/j.rcsop.2026.100715
35. Ilbars H, Terzioğlu Bebitoğlu B, Hidiroğlu S, Doğanç FB, Varol Y. The prevalence and impact of workplace violence in community pharmacies: a mixed-methods study. Turk J Med Sci. 2026;56(1):333–343. doi:10.55730/1300-0144.6167
36. Thonon F, Perrot S, Yergolkar AV, et al. Electronic tools to bridge the language gap in health care for people who have migrated: systematic review. J Med Internet Res. 2021;23(5):e25131. doi:10.2196/25131
37. Hattingh HL, Emmerton L, Ng Cheong Tin P, Green C. Utilization of community pharmacy space to enhance privacy: a qualitative study. Health Expect. 2016;19(5):1098–1110. doi:10.1111/hex.12401
38. Alshahrani SM. Perception and readiness of community pharmacists in delivering palliative care services in Saudi Arabia: a new role in the game. Front Pharmacol. 2025;16. doi:10.3389/fphar.2025.1646531
39. Esmalipour R, Larijani B, Mehrdad N, Ebadi A, Salari P. The ethical challenges in pharmacy practice in community Pharmacies: a qualitative study. Saudi Pharm J. 2021;29(12):1441–1448. doi:10.1016/j.jsps.2021.11.003
40. Shaw C, Khan G, Govind T, Robinson-Barella A. Implementing and delivering culturally centred pharmacy services tailored to ethnically minoritised populations: a qualitative systematic review and meta-ethnography. Health Expect. 2025;28(1):e70165. doi:10.1111/hex.70165
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.