")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
The Impact of Acne, Atopic Dermatitis, Skin Toxicities and Scars on Quality of Life and the Importance of a Holistic Treatment Approach
Authors Dreno B, Amici JM, Demessant-Flavigny AL , Wright C, Taieb C , Desai SR, Alexis A
Received 14 April 2021
Accepted for publication 15 May 2021
Published 14 June 2021 Volume 2021:14 Pages 623—632
DOI https://doi.org/10.2147/CCID.S315846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Brigitte Dreno,1 Jean Michel Amici,2 Ann Laure Demessant-Flavigny,3 Charlotte Wright,4 Charles Taieb,5 Seemal R Desai,6 Andrew Alexis7
1Dermatology Department, CHU Nantes, CIC 1413, CRCINA, Nantes University, Nantes, Pays de la Loire, France; 2Dermatology Department, Bordeaux University Hospital, Bordeaux, Nouvelle-Aquitaine, France; 3La Roche-Posay Dermatological Laboratoires, Levallois-Perret, France; 4Speak the Speech Consulting, Asnières-sur-Seine, Ile-de-France, France; 5Patients Priority Department, European Market Maintenance Assessment, Fontenay Sousbois, Ile-de-France, France; 6Department of Dermatology, The University of Texas Southwestern Medical Center & Innovative Dermatology, Dallas, TX, USA; 7Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai West, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Correspondence: Charles Taieb
Patients Priority Department, European Market Maintenance Assessment, Fontenay Sousbois, Ile-de-France, France
Tel +33 771772100
Email [email protected]
Abstract: Skin conditions such as acne, atopic dermatitis, skin toxicity from oncology treatment, and scars are among the most common health conditions and negatively impact quality of life (QoL). Yet the physician perception of this impact often varies greatly from the patient perception. This is important because patient illness perception is closely linked with seeking help and treatment adherence behaviors. The objective of this review is to better understand the impact of these four highly prevalent skin conditions on QoL including their health-related economic factors to improve treatment outcomes. The literature search included literature published on QoL with acne, atopic dermatitis, scars (from any cause) and skin toxicities on PubMed between 2015 and 2020. We found that patients with skin conditions have a much higher frequency of altered QoL and psychological distress than those without. Also, skin conditions negatively impact self-image and can cause feelings of isolation, loneliness, lower self-esteem, and lower body satisfaction. Additionally, physical discomfort adds to the psychological distress. These physical and psychological impacts are an enormous financial burden on patients, their families and society. We found evidence that holistic treatment including treating the skin condition itself, providing wider peer and psychological support as well as shared decision-making, therapeutic patient education and dermatologist involvement improves outcomes. Holistic history-taking, checklists, or the use of more formal QoL scoring tools can be incorporated into routine consultations to better assess patient well-being and provide clinicians with important information for adapting treatment to individual patient requirements. In conclusion, this review highlights the overall impact of skin conditions (including psychological and QoL impacts) and the importance of providing holistic care to optimize treatment outcomes. A comprehensive QoL screening tool would be useful to help provide patient-centered treatment.
Keywords: quality of life, acne, atopic dermatitis, scars, burns, skin toxicities
Plain Language Summary
Skin conditions are very common and affect many people around the world. Sadly, these conditions can reduce a patient’s quality of life and physicians often underestimate this impact. This review examines how skin conditions affect patients and how treatments can be tailored to ensure the best individual outcome.
We searched the PubMed online database of medical articles for information on quality of life and acne, eczema, side effects from cancer treatment affecting the skin and scars (from any cause).
The information found from this search revealed that these common skin conditions can cause mental health disorders such as depression, suicidal thoughts, and low self-esteem along with physical discomfort. Unfortunately, these conditions are costly for the patient, their family and society.
It was also found that by appreciating the full impact of the skin conditions, well-rounded patient-centered treatment starts with treating the skin condition itself and is followed by providing mental health support, education and shared decision-making. This gives the patient the best chance of an optimal treatment outcome.
Introduction
Skin conditions are among the most common health conditions affecting around 2 billion people1 and negatively impact quality of life (QoL). When considering disability-adjusted life years (DALYs), it was ranked as the fourth leading cause of non-fatal burden in 2013, directly following iron-deficiency anemia, tuberculosis and sense organ diseases and was the 18th leading cause of global DALYs.2
One of the most common skin conditions is acne, affecting approximately 85% of 11 to 30-year-olds3 with an estimated global prevalence of 9.4% making it the eighth most prevalent disease worldwide.4 Atopic dermatitis (AD) affects 20% of infants and adolescents and up to 3% of adults worldwide.5,6 However, this rate is increasing globally, particularly in developed nations, due to its links with increasing urbanization and industrialization.7
Skin toxicities from oncology treatments are highly prevalent and negatively impact QoL. Cancer has a vast global burden with over 18 million new cases in 2018 alone.8 Skin toxicity occurs in a third of patients on immune checkpoint inhibitors (immunotherapy)9,10 while the QoL impairment from skin toxicity appears unexpectedly more severe in patients treated with targeted therapy.10 Radiotherapy is associated with cutaneous adverse events such as radiodermatitis with up to 95% of patients developing moderate-to-severe skin reactions.11
Scars negatively impact QoL and have a considerably high prevalence globally. An estimated 100 million people per year in developed countries acquire scars from surgical procedures12 and approximately 6 million people suffer traumatic burns worldwide every year.13 It is estimated that three to four people per 1000 population in Europe are living with at least one scar.14
A physician’s perception of how these common skin conditions can impact their patient can vary greatly from the patient’s perception of their illness. For example, it has been suggested that it is more important to consider a patient’s perception of acne severity rather than physician-reported severity since acne patient perception is an indicator of body image satisfaction and self-confidence.15 Illness perception (IP) is defined as the cognitive and emotional representation of an illness or health threat held by an individual and is intimately linked with behaviors such as seeking help and treatment adherence.16 Nagpal et al. identified a direct relationship between IP and QoL meaning more information about IP and its impact on QoL will help clinicians identify and acknowledge patient perceptions and potentially positively impact patient wellbeing.17 Using QoL measures can improve clinician awareness of the patient’s perspective, the burden the patient and their family experiences18 as well as lesion severity are not necessarily correlated with impact on QoL.19 QoL impairment is such an important concept that Finlay proposed the new word “quimp” to mean QoL impairment and promote consideration of QoL into routine clinical practice.19,20
The objective of this review was to further understand the impact these skin conditions have on QoL and health related economic factors, and to identify treatment approaches to improve patient outcomes and well-being.
Materials and Methods
A current literature review was performed using PubMed with publications in English dated from 2015 to 2020. We searched “quality of life” with each skin condition using the terms “acne”, “atopic dermatitis”, “scars” and “skin toxicities”. For scars, we included any form of scar including burns, surgical scars, acne scars and keloid scars. Skin toxicities from oncology treatment included radiodermatitis and toxicities caused by systemic chemotherapy. Article abstracts were read initially. Papers were excluded if they did not include information on the impact of these skin conditions, QoL, QoL scoring tools, wider impact of the skin condition or treatment approaches to improve QoL. If the content was unclear, the full-text was read. Once included, each article was read completely and any data relating to the four skin conditions and search criteria were extracted onto a spreadsheet. Data were also extracted from any additional relevant articles identified during this process. Although this was not a systematic review, we endeavored to conduct the most thorough review possible considering we did not have access to Embase.
Health-Related Impact of Skin Conditions
Psychological
Patients with skin conditions have a much higher frequency of psychological distress and altered QoL than those without.21 Studies have demonstrated the levels of social, psychological and emotional problems and the impact on QoL reported by acne patients are as great as those reported by patients with chronic disabling asthma, epilepsy, diabetes, back pain, arthritis, or coronary heart disease.22–24 Similarly, people with AD have a lower QoL than other chronic conditions including heart disease, diabetes and high blood pressure with moderate and severe AD being associated with a dramatically lower QoL.25 In children, generalized AD has the second-largest impact on QoL following only cerebral palsy.26
Depression, anxiety, and suicidal ideation are more common in people with AD and acne than in the general population, even with mild to moderate disease,27–30 and acne is an independent risk factor for suicide.31,32 The greater the impact on QoL, the more severe the anxiety and depression.33,34 Adolescents are particularly at risk of these psychiatric disorders since they are more psychologically unstable and susceptible to appearance changes. If these disorders go undetected and untreated, the consequences can be severe.35
Most research on scarring focuses on severe scarring such as burns but there are few data on the psychological impact of scars from routine elective or aesthetic surgeries. Post-traumatic stress disorder (PTSD) has been found to occur commonly following severe burn injuries.36 In a large study of 438 patients in the Netherlands, 33% had severe PTSD one to two years post-burn.37 However, 10 years after a burn injury, QoL is, on average, comparable to the general population.38
Emotional
Skin conditions negatively impact self-image. Acne can cause feelings of isolation, loneliness, lower self-esteem, and lower body satisfaction.39 When comparing acne to other skin conditions, 20–30% of patients with psoriasis, AD, contact dermatitis or urticaria were withdrawn into themselves compared with more than 50% of people with acne.21 Burn survivors may experience feelings of shame, lack of confidence, low self-esteem, and avoidance of social situations while facial scars are associated with severe psychological, emotional, and social sequelae.40
When scarring (from any cause) is visible, patients may feel self-conscious and struggle with personal, work, and social relationships, and communication.41 Visible scars have the greatest impact on QoL while it appears that it is the presence of the scar rather than the severity which affects QoL.42 One study revealed that patients wished scars in both visible and nonvisible sites were less noticeable and 91% would value even a small improvement in scarring.43 Keloid and hypertrophic scars and chronic skin conditions have a similar impact on QoL due to internalized stigmatization, physical symptoms, and restricted mobility.41
Radiodermatitis has a wide-ranging impact on patients including changes to body image, clothing selection, ability to perform activities of daily living,44,45 lost work productivity, wound care costs, social isolation and affected QoL.46 Several studies in patients with gynecological cancers revealed dermatological adverse events impair functional, emotional, and physical well-being and significantly limit QoL, particularly because they persist long after completing chemotherapy.47–50
Emotional impacts can also include difficulties in sexual and conjugal life as reported by 10–20% of people with acne and sleep disturbances in 30–50% of acne patients.21
Physical
AD is associated with redness, flaking, bleeding, and chronic itching27 which is linked to mental distress and increased risk of suicidal ideation.51 Flares caused by triggers such as S. aureus, viral infections, food allergens, cosmetics and fragrance52–54 and exposure to environmental allergens such as pollens, dust mites, molds, cigarette smoke and animal dander55 not only exacerbate symptoms but are also linked to worse QoL scores.56
Scars, particularly burns, cause physical and psychosocial sequelae which negatively affect QoL and are one of the most influential causes of DALYs according to the WHO.38 Furthermore, acne marks and scars have been shown to significantly alter QoL regardless of age group.24 The physical and sensory changes alongside the burden of complete scar treatments mean the impact on QoL can be ongoing.57
Physical discomfort, perceived disfigurement and cosmetic dissatisfaction occur with radiation induced breast telangiectasias and are a constant reminder of the patient’s breast cancer.58 One study interviewed patients undergoing radiotherapy for breast cancer. 32% described itching, pain, and tenderness.46
The main forms of skin toxicity associated with immunotherapy are maculopapular rash and pruritus but psoriasis, acneiform rashes, autoimmune skin disease and sarcoidosis can also occur, all of which can profoundly diminish QoL and impact treatment adherence.9,10 Periungual inflammation and palmoplantar lesions from targeted therapy are accompanied by pain, and limited ability to perform self-care daily activities.59 Skin toxicities during oncology treatments can be so severe that treatment is significantly disrupted thus affecting both QoL and optimal anticancer treatment59 and limiting the use of specific treatment protocols.
Children
AD affects children in numerous ways including itching, pain, bleeding, dietary limitations, behavioral problems, crying, irritability, inattention/hyperactivity, anxiety, depression, and conduct disorders.26,60 46–60% of patients experience disturbed sleep which is a major factor impacting QoL.61 The significant impact of AD on sleep has possible long-term impacts on daytime functioning and may be more injurious at a young age during rapid brain development compared with similar levels of sleep disturbance in later childhood.62 However, AD in children impacts the wider family as well as the child. Parents of young children are particularly affected by sleep deprivation and the emotional distress of seeing their child suffer.63 23–75% of parents experience sleep disturbance and excessive tiredness.64,65 One study comparing AD and asthma found that mothers spent 78 minutes and fathers spent 90 minutes per night attending their child with AD while parents of children with asthma spent no time.63
Socioeconomic Impact of Altered QoL in Skin Conditions
The impact of skin conditions causes huge financial burdens on patients, their families and society. The direct costs include prescriptions, clinician visits and hospital costs while indirect costs include presenteeism (reduced productivity at work) and absenteeism (missing work).26
In 2015 in the USA, a conservative estimate of the annual burden of AD was $5.297 billion including $1.009 billion direct costs, $619 million in decreased productivity and $2.6 billion due to decreased QoL.26 These costs are likely underestimated since prevalence has increased since a study conducted in 2004.(Ref 26)
Missing school and reduced productivity are common with AD.66 One study found 12.2% of patients missed 1–2 days of work and 2.3% missed 3 or more days.25 Another study found 32% of patients believed AD impacted their school or work life and 14% felt it had hindered their career progression.66 In a 2019 study, an average of 7.1 work hours were missed in the previous seven days.56 Estimated mean productivity loss is almost 10% and mean presenteeism is 9.2%.67
Acne also has a large health economic impact with one study estimating that over the previous 30 days, 1.9 days of work and 1.7 days of school were missed due to acne recurrence. Extrapolating this data gives a better idea of the scale of this impact. For example, “Objectifs Peau” estimate there to be 3.3 million French citizens over 15 years of age affected by acne with 188,000 likely to experience acne recurrence, therefore resulting in 350,000 days lost due to acne recurrences.24
Evidence to Support a Holistic Treatment Approach
Treatment of the Condition
Holistic treatment starts with treating the skin condition itself. It has been shown that providing effective treatment for skin conditions improves QoL.15,35,42,58,68–72 During chemotherapy and radiotherapy treatments, detecting and treating any skin toxicities early is essential.73 Alongside treatments, focusing on techniques that patients already know including clothing choices, cleaning and emollients can help improve QoL.74 (See Table 1)
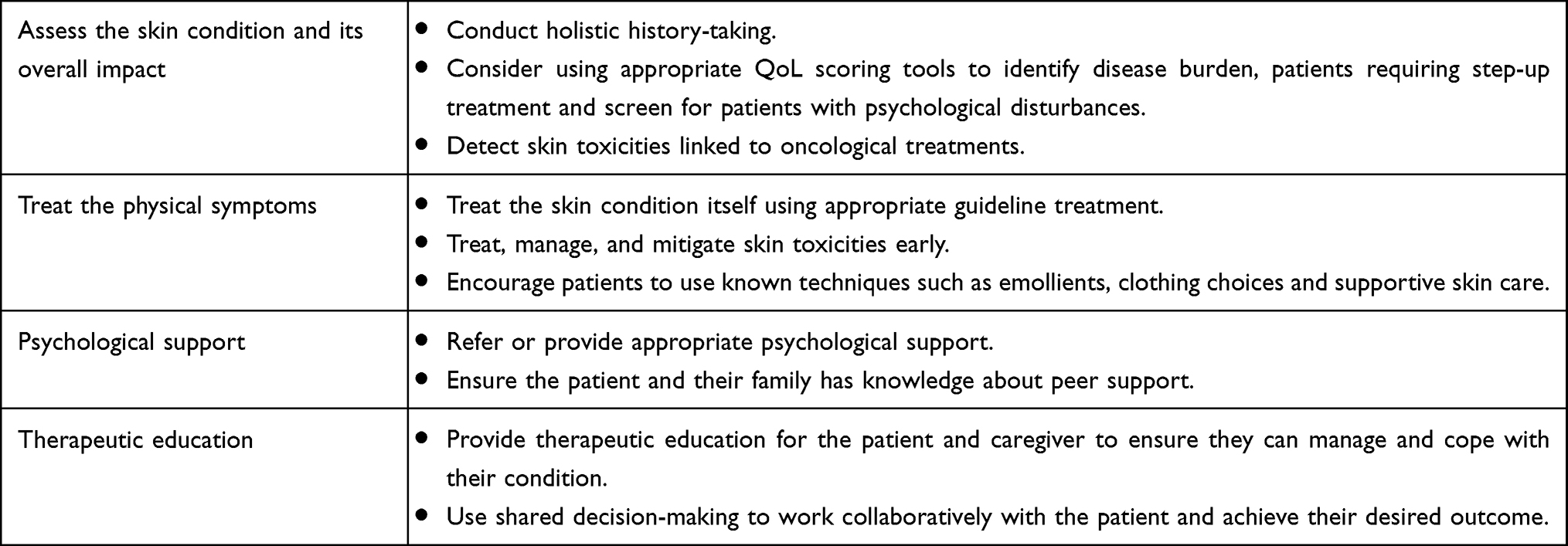 |
Table 1 A Holistic Treatment Approach |
Psychological Support
Unfortunately, current approaches to treatment are often limited to the physical symptoms of the skin conditions and do not sufficiently address the psychological ramifications. The psychological distress experienced by patients may be underestimated by health care providers,21 or conversely, resources to address recognized psychological effects of skin disorders may be lacking in many practice settings. Zuberbier et al. found that 74% of patients and caregivers reported that their physician had never discussed the emotional impact of their AD and 84% did not know support groups existed.66 In fact, over half of AD patients are not used to discussing their QoL with their physician with 22.4% of AD patients and 35.7% of other eczema patients feeling unsupported by their physician.74 One study found that 40% of specialist consultations did not discuss QoL.75
The relationship between acne and its psychiatric comorbidities is hugely disabling and ignoring this relationship during patient evaluations may result in under-treatment, poor adherence, and treatment dissatisfaction and contribute to an increased risk for anxiety, depression and impaired QoL in the future.31,39
A study by Brewin highlighted the serious neglect of psychosocial rehabilitation during burns treatment in the UK. It was suggested that psychological support was provided for profoundly disturbed patients when, in fact, routine screening for psychological distress should be performed for every patient.41
Adopting a multidisciplinary approach to the treatment of skin conditions including psychological support rather than focusing just on the dermatological aspects would be extremely beneficial.31 Ideally, symptoms and QoL should be evaluated to establish disease burden, identify patients needing step-up treatment and screen for any patients with psychological disturbances.25 While QoL may be indirectly assessed by clinicians (e.g. through history taking), validated assessment tools that are practical, efficient, and widely accepted in the community practice setting remain elusive.
Wider Support
Peer support has been shown to have a positive impact and provides hope to burn survivors.41 Families also need support and advice to help them normalize the scars, and understand scar permanence, outcome expectations, and how their loved one may change or respond following the burn injury.41 Burn survivors identified psychological support, wound care advice and treatment information, meeting other burn patients and learning acceptance and coping methods as the four areas of support they wanted.41 Family education has also been shown to influence QoL with AD.60
Educating society and decreasing stigma is essential and will help some factors affecting the psychological well-being of patients with skin conditions.74
Shared Decision-Making and Therapeutic Patient Education
When considering surgical scars, there is disparity between the patient’s and physician’s opinion on what is “acceptable”. In a UK study, 67% of women and 33% of men said they had concerns about a scar which the physician thought was “acceptable”.76 It has been shown that communication between patients and physicians, both before and after surgery, could be improved. Physicians report being aware of scarring being a concern for their patients and discussing this with them. They also reported attempting to prevent or improve scarring during surgery. However, over two-thirds of patients felt they were more concerned about scarring than the physician.43
This disparity between perceptions could be improved through shared decision-making (SDM) to improve treatment adherence and consequently improve QoL. This approach respects clinical evidence and the patient’s preference for specific treatment goals.77 It is defined as “an approach where clinicians and patients make decisions together, using the best available evidence”.78 This way, the physician and patient discuss the patient’s priorities for treatment and a management plan is created reflecting both the physician’s and the patient’s perspective. Physician’s use their professional judgement and work collaboratively with the patient to achieve the patient’s desired outcome.79 Using QoL measures may encourage patients to be involved in SDM.19
SDM is an important part of therapeutic patient education (TPE) which is a patient-centered process aiming to provide patients and caregivers with the skills needed to manage and cope with their condition. In all conditions, effective patient and caregiver therapeutic education is necessary and important and has been shown to improve outcomes such as severity, treatment adherence and QoL. When possible, TPE should ideally be multidisciplinary and use various methods and tools to transfer knowledge.80 QoL measures may enable personalized educational input to the patient by revealing specific issues.19
Dermatologist Involvement in Oncology Treatments
In the context of oncologic treatment, discussions about dermatologic side effects are often limited, as are proactive strategies to mitigate them. Timely access to supportive oncodermatology treatment during the immediate post-treatment transition period can be lacking, resulting in inadequate management of long-lasting skin toxicities.69
The emergence of novel cancer treatments and the longer life expectancy of cancer patients means skin toxicities will continue to expand. Dermatologists therefore have an increasingly important potential role in a multidisciplinary team managing or mitigating skin toxicities and helping to achieve optimal patient outcomes.81
There is increasing evidence demonstrating a relationship between dermatologist involvement for skin toxicities and improved QoL and outcomes.82,83 Involvement of dermatologists also reduces the number of patients unnecessarily discontinuing their anticancer treatment.82,83 More than 25% of referring physicians recommend discontinuing treatment when patients develop skin toxicities from targeted therapies compared with 4% of dermatologists.83 To ensure effective skin toxicity management some oncology clinics now have embedded dermatologists.81
QoL Scoring Tools
Assessing patient QoL provides important information for adapting treatment to each patient’s unique requirements84 and may help make clinical decisions more patient-centred.19 Assessing the patient’s perspective enables comprehensive interpretation of treatment efficacy and impact.57 QoL measures in pediatric consultations may enhance communication between children and their parents or carers and allow the parent to have a better understanding of the child’s perspective.85 Systematically assessing patient QoL can enhance the clinician-patient relationship and demonstrate that the clinician is aware of the QoL impact and cares about the patient’s preferred outcomes. It can also promote discussions about treatment satisfaction and preferences, and disease burden.19 QoL is already an essential component of many oncology treatment decisions86 and should become more integrated in dermatological treatments through the development of practical and efficient tools that are suitable for most practice settings.
QoL scoring tools are readily available, they are largely used in the clinical research setting or by select tertiary care centers. It is important to choose the appropriate tool for the assessment. Generic instruments are used to compare QoL impairment in the skin condition in question with nondermatological conditions. Conversely, dermatology-specific instruments can compare QoL across different skin disorders. These instruments can have better capacity for differentiation, be more sensitive to change and make it less likely to miss issues associated with the condition.87
Dermatology-specific instruments such as the Dermatology Life Quality Index (DLQI), the Dermatology Quality of Life Scales (DQOLS), and the Dermatology Specific Quality of Life (DSQL) are readily available. These have the advantage of assessing numerous domains impacted by a skin condition and provide information from patients with a wide spectrum of dermatological conditions.88 Disease-specific questionnaires are also available such as the Cardiff Acne Disability Index (CADI), Patient-Oriented Eczema Measure (POEM), and Brisbane Burn Scar Impact Profile (BBSIP). Many validated instruments are available assessing symptoms and QoL but do not comprehensively analyze all aspects of the condition.
Children, infant, and family-specific instruments include the Children’s Dermatology Life Quality Index (CDLQI), Infants’ Dermatitis Quality of Life Index (IDQoL)) Dermatitis Family Index (DFI), and the Childhood Atopic Dermatitis Impact Scale (CADIS).89 However, no QoL instrument for infants, children, and adolescents with AD can be highly recommended because none fulfil all required criteria.90
A systematic review was performed as part of the Global Research on the Impact of Dermatological Diseases (GRIDD) project analyzing 53 articles reporting on 36 different instruments. This review found that no single dermatology specific patient-reported outcome measure demonstrates sufficient evidence of adequate measurement properties to be recommended for use.91
The GRIDD project is currently developing a patient-impact measurement tool (called PRIDD) aiming to offer new perspectives on the lives of the millions of people living with skin conditions. It is hoped this new tool will address the issues with the existing tools such as the weaknesses in the DLQI.92
Conclusion
The QoL impact of skin conditions is an important consideration for therapeutic decision-making. Holistic history-taking, checklists, or the use of more formal QoL scoring tools can be incorporated into routine consultations to improve patient well-being. TPE and SDM are key components of a holistic treatment approach and can improve treatment outcomes as well as patient satisfaction.
For cancer patients, dermatologists can play a vital role in managing potential skin toxicities related to oncologic treatments and thereby reduce disruptions or premature treatment discontinuation due to cutaneous effects.
In conclusion, this review highlights the overall impact of skin conditions (including psychological and QoL impacts) and the importance of providing holistic care to optimize treatment outcomes. A comprehensive QoL screening tool would be useful to help provide patient-centered treatment.
Acknowledgments
The authors thank Amy Whereat of Speak the Speech Consulting for her contribution to conceptualization, editing and review of the manuscript.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This review was funded by La Roche-Posay Dermatological Laboratories. La Roche-Posay is a brand own by the L'Oreal group.
Disclosure
AL Demessant-Flavigny is an employee of L'Oreal, La Roche-Posay, France. Mrs Charlotte Wright reports personal fees for manuscript preparation from La Roche-Posay, during the conduct of the study. Dr. Seemal R. Desai reports personal fees from L’Oreal, outside the submitted work. Dr. Andrew Alexis reports grants and personal fees from Leo, Novartis, Almiral, during the conduct of the study; grants and personal fees from Leo, Novartis, Almirall, Bristol Myers Squibb, Amgen, Menlo, Galderma, Valeant/Bausch Health, Cara, Arcutis, Pfizer, SANOFI-Regeneron, Dermavant, Unilever, Beiersdorf, L’Oreal, Scientis, UCB, Foamix, Cassiopea, Janssen, Allergan, AbbVie, and Sol-Gel, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Hay RJ, Johns NE, Williams HC, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 2014;134(6):1527–1534. doi:10.1038/jid.2013.446
2. Karimkhani C, Dellavalle RP, Coffeng LE, et al. Global skin disease morbidity and mortality: an update from the global burden of disease study 2013. JAMA Dermatol. 2017;153(5):406–412. doi:10.1001/jamadermatol.2016.5538
3. Dreno B, Poli F. Epidemiology of acne. Dermatology. 2003;206(1):7–10. doi:10.1159/000067817
4. Tan JK, Bhate K. A global perspective on the epidemiology of acne. Br J Dermatol. 2015;172(Suppl 1):3–12. doi:10.1111/bjd.13462
5. Kowalska-Olędzka E, Czarnecka M, Baran A. Epidemiology of atopic dermatitis in Europe. J Drug Assess. 2019;8(1):126–128. doi:10.1080/21556660.2019.1619570
6. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66(Suppl 1):8–16. doi:10.1159/000370220
7. Hendricks AJ, Eichenfield LF, Shi VY. The impact of airborne pollution on atopic dermatitis: a literature review. Br J Dermatol. 2020;183(1):16–23. doi:10.1111/bjd.18781
8. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. doi:10.1002/ijc.31937
9. Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19(3):345–361. doi:10.1007/s40257-017-0336-3
10. Lacouture M, Sibaud V. Toxic side effects of targeted therapies and immunotherapies affecting the skin, oral mucosa, hair, and nails. Am J Clin Dermatol. 2018;19(Suppl 1):31–39. doi:10.1007/s40257-018-0384-3
11. Rosenthal A, Israilevich R, Moy R. Management of acute radiation dermatitis: a review of the literature and proposal for treatment algorithm. J Am Acad Dermatol. 2019;81(2):558–567. doi:10.1016/j.jaad.2019.02.047
12. Jourdan M, Madfes DC, Lima E, Tian Y, Seité S. Skin care management for medical and aesthetic procedures to prevent scarring. Clin Cosmet Investig Dermatol. 2019;12:799–804. doi:10.2147/CCID.S218134
13. Brusselaers N, Monstrey S, Vogelaers D, Hoste E, Blot S. Severe burn injury in Europe: a systematic review of the incidence, etiology, morbidity, and mortality. Crit Care. 2010;14(5):R188. doi:10.1186/cc9300
14. Jørgensen SF, Nygaard R, Posnett J. Meeting the challenges of wound care in Danish home care. J Wound Care. 2013;22(10):540–545. doi:10.12968/jowc.2013.22.10.540
15. Davern J, O’Donnell AT. Stigma predicts health-related quality of life impairment, psychological distress, and somatic symptoms in acne sufferers. PLoS One. 2018;13(9):e0205009. doi:10.1371/journal.pone.0205009
16. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
17. Nagpal N, Gordon-Elliott J, Lipner S. Comparison of quality of life and illness perception among patients with acne, eczema, and psoriasis. Dermatol Online J. 2019;25:5.
18. Basra MK, Sue-Ho R, Finlay AY. The family dermatology life quality index: measuring the secondary impact of skin disease. Br J Dermatol. 2007;156(3):528–538. doi:10.1111/j.1365-2133.2006.07617.x
19. Finlay AY, Salek MS, Abeni D, et al. Why quality of life measurement is important in dermatology clinical practice: an expert-based opinion statement by the EADV task force on quality of life. J Eur Acad Dermatol Venereol. 2017;31(3):424–431. doi:10.1111/jdv.13985
20. Finlay AY. Quimp: a word meaning “quality of life impairment”. Acta Derm Venereol. 2017;97(4):546–547. doi:10.2340/00015555-2650
21. Misery L, Taïeb C, Schollhammer M, et al. Psychological consequences of the most common dermatoses: data from the objectifs Peau study. Acta Derm Venereol. 2020;100(13):adv00175. doi:10.2340/00015555-3531
22. Mallon E, Newton JN, Klassen A, Stewart-Brown SL, Ryan TJ, Finlay AY. The quality of life in acne: a comparison with general medical conditions using generic questionnaires. Br J Dermatol. 1999;140(4):672–676. doi:10.1046/j.1365-2133.1999.02768.x
23. Cresce ND, Davis SA, Huang WW, Feldman SR. The quality of life impact of acne and rosacea compared to other major medical conditions. J Drugs Dermatol. 2014;13(6):692–697.
24. Dreno B, Bordet C, Seite S, Taieb C. Acne relapses: impact on quality of life and productivity. J Eur Acad Dermatol Venereol. 2019;33(5):937–943. doi:10.1111/jdv.15419
25. Silverberg JI, Gelfand JM, Margolis DJ, et al. Patient burden and quality of life in atopic dermatitis in US adults: a population-based cross-sectional study. Ann Allergy Asthma Immunol. 2018;121(3):340–347. doi:10.1016/j.anai.2018.07.006
26. Drucker AM, Wang AR, Li WQ, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the National Eczema association. J Invest Dermatol. 2017;137(1):26–30. doi:10.1016/j.jid.2016.07.012
27. Barrett A, Hahn-Pedersen J, Kragh N, Evans E, Gnanasakthy A. Patient-reported outcome measures in atopic dermatitis and chronic hand Eczema in adults. Patient. 2019;12(5):445–459. doi:10.1007/s40271-019-00373-y
28. Thomas DR. Psychosocial effects of acne. J Cutan Med Surg. 2004;8(Suppl 4):3–5. doi:10.1007/s10227-004-0752-x
29. Chren MM, Lasek RJ, Quinn LM, Mostow EN, Zyzanski SJ. Skindex, a quality-of-life measure for patients with skin disease: reliability, validity, and responsiveness. J Invest Dermatol. 1996;107(5):707–713. doi:10.1111/1523-1747.ep12365600
30. Hahm BJ, Min SU, Yoon MY, et al. Changes of psychiatric parameters and their relationships by oral isotretinoin in acne patients. J Dermatol. 2009;36(5):255–261. doi:10.1111/j.1346-8138.2009.00635.x
31. Cengiz GF, Gürel G. Difficulties in emotion regulation and quality of life in patients with acne. Qual Life Res. 2020;29(2):431–438. doi:10.1007/s11136-019-02318-2
32. Halvorsen JA, Stern RS, Dalgard F, Thoresen M, Bjertness E, Lien L. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study. J Invest Dermatol. 2011;131(2):363–370. doi:10.1038/jid.2010.264
33. Dalgard FJ, Gieler U, Tomas-Aragones L, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol. 2015;135(4):984–991. doi:10.1038/jid.2014.530
34. Yazici K, Baz K, Yazici AE, et al. Disease-specific quality of life is associated with anxiety and depression in patients with acne. J Eur Acad Dermatol Venereol. 2004;18(4):435–439. doi:10.1111/j.1468-3083.2004.00946.x
35. Erdoğan Y, Erturan İ, Aktepe E, Akyıldız A. Comparison of quality of life, depression, anxiety, suicide, social anxiety and obsessive-compulsive symptoms between adolescents with acne receiving isotretinoin and antibiotics: a prospective, non-randomised, open-label study. Paediatr Drugs. 2019;21(3):195–202. doi:10.1007/s40272-019-00340-y
36. McLean L, Chen R, Kwiet J, Streimer J, Vandervord J, Kornhaber R. A clinical update on posttraumatic stress disorder in burn injury survivors. Australas Psychiatry. 2017;25(4):348–350. doi:10.1177/1039856217700285
37. Taal LA, Faber AW. Posttraumatic stress and maladjustment among adult burn survivors 1–2 years postburn. Burns. 1998;24(4):285–292. doi:10.1016/S0305-4179(98)00030-8
38. Gojowy D, Kauke M, Ohmann T, Homann HH, Mannil L. Early and late-recorded predictors of health-related quality of life of burn patients on long-term follow-up. Burns. 2019;45(6):1300–1310. doi:10.1016/j.burns.2019.03.016
39. Gieler U, Gieler T, Kupfer JP. Acne and quality of life - impact and management. J Eur Acad Dermatol Venereol. 2015;29(Suppl 4):12–14. doi:10.1111/jdv.13191
40. Kant SB, Colla C, Van den Kerckhove E, Van der Hulst R, Piatkowski de Grzymala A. Satisfaction with facial appearance and quality of life after treatment of face scars with a transparent facial pressure mask. Facial Plast Surg. 2018;34(4):394–399. doi:10.1055/s-0038-1648249
41. Brewin MP, Homer SJ. The lived experience and quality of life with burn scarring-the results from a large-scale online survey. Burns. 2018;44(7):1801–1810. doi:10.1016/j.burns.2018.04.007
42. Limongelli P, Casalino G, Tolone S, et al. Quality of life and scar evolution after negative pressure or conventional therapy for wound dehiscence following post-bariatric abdominoplasty. Int Wound J. 2017;14(6):960–966. doi:10.1111/iwj.12739
43. Young VL, Hutchison J. Insights into patient and clinician concerns about scar appearance: semiquantitative structured surveys. Plast Reconstr Surg. 2009;124(1):256–265. doi:10.1097/PRS.0b013e3181a80747
44. Schnur JB, Ouellette SC, Bovbjerg DH, Montgomery GH. Breast cancer patients’ experience of external-beam radiotherapy. Qual Health Res. 2009;19(5):668–676. doi:10.1177/1049732309334097
45. Schnur JB, Ouellette SC, Dilorenzo TA, Green S, Montgomery GH. A qualitative analysis of acute skin toxicity among breast cancer radiotherapy patients. Psychooncology. 2011;20(3):260–268. doi:10.1002/pon.1734
46. Beamer LC, Grant M. Longitudinal trends in skin-related and global quality of life among women with breast radiodermatitis: a pilot study. Eur J Oncol Nurs. 2018;33:22–27. doi:10.1016/j.ejon.2018.01.008
47. Gandhi M, Oishi K, Zubal B, Lacouture ME. Unanticipated toxicities from anticancer therapies: survivors’ perspectives. Support Care Cancer. 2010;18(11):1461–1468. doi:10.1007/s00520-009-0769-1
48. Hackbarth M, Haas N, Fotopoulou C, Lichtenegger W, Sehouli J. Chemotherapy-induced dermatological toxicity: frequencies and impact on quality of life in women’s cancers. Results of a prospective study. Support Care Cancer. 2008;16(3):267–273. doi:10.1007/s00520-007-0318-8
49. Ra HS, Shin SJ, Kim JH, Lim H, Cho BC, Roh MR. The impact of dermatological toxicities of anti-cancer therapy on the dermatological quality of life of cancer patients. J Eur Acad Dermatol Venereol. 2013;27(1):e53–59. doi:10.1111/j.1468-3083.2012.04466.x
50. Sibaud V, Lebœuf NR, Roche H, et al. Dermatological adverse events with taxane chemotherapy. Eur J Dermatol. 2016;26(5):427–443. doi:10.1684/ejd.2016.2833
51. Halvorsen JA, Lien L, Dalgard F, Bjertness E, Stern RS. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134(7):1847–1854. doi:10.1038/jid.2014.70
52. Avena-Woods C. Overview of atopic dermatitis. Am J Manag Care. 2017;23(8 Suppl):S115–s123.
53. Silverberg NB. A practical overview of pediatric atopic dermatitis, part 2: triggers and grading. Cutis. 2016;97(5):326–329.
54. Geoghegan JA, Irvine AD, Foster TJ. Staphylococcus aureus and atopic dermatitis: a complex and evolving relationship. Trends Microbiol. 2018;26(6):484–497. doi:10.1016/j.tim.2017.11.008
55. Diseases NIoAaI. Eczema (atopic dermatitis) causes & strategies for prevention. 2020 [Updated June 30, 2016]. Available from: https://www.niaid.nih.gov/diseases-conditions/eczema-causes-prevention-strategies.
56. Wei W, Ghorayeb E, Andria M, et al. A real-world study evaluating adeQUacy of existing systemic treatments for patients with moderate-to-severe atopic dermatitis (QUEST-AD): baseline treatment patterns and unmet needs assessment. Ann Allergy Asthma Immunol. 2019;123(4):381–388.e382. doi:10.1016/j.anai.2019.07.008
57. Simons M, Kimble R, McPhail S, Tyack Z. The Brisbane Burn Scar impact profile (child and young person version) for measuring health-related quality of life in children with burn scars: a longitudinal cohort study of reliability, validity and responsiveness. Burns. 2019;45(7):1537–1552. doi:10.1016/j.burns.2019.07.012
58. Rossi AM, Blank NR, Nehal K, Dusza S, Lee EH. Effect of laser therapy on quality of life in patients with radiation-induced breast telangiectasias. Lasers Surg Med. 2018;50(4):284–290. doi:10.1002/lsm.22780
59. Lee J, Lim J, Park JS, et al. The impact of skin problems on the quality of life in patients treated with anticancer agents: a cross-sectional study. Cancer Res Treat. 2018;50(4):1186–1193. doi:10.4143/crt.2017.435
60. Rea CJ, Tran KD, Jorina M, Wenren LM, Hawryluk EB, Toomey SL. Associations of eczema severity and parent knowledge with child quality of life in a pediatric primary care population. Clin Pediatr. 2018;57(13):1506–1514. doi:10.1177/0009922818787295
61. Chang YS, Chiang BL. Mechanism of sleep disturbance in children with atopic dermatitis and the role of the circadian rhythm and melatonin. Int J Mol Sci. 2016;17(4):462. doi:10.3390/ijms17040462
62. Camfferman D, Kennedy JD, Gold M, Martin AJ, Lushington K. Eczema and sleep and its relationship to daytime functioning in children. Sleep Med Rev. 2010;14(6):359–369. doi:10.1016/j.smrv.2010.01.004
63. Moore K, David TJ, Murray CS, Child F, Arkwright PD. Effect of childhood eczema and asthma on parental sleep and well-being: a prospective comparative study. Br J Dermatol. 2006;154(3):514–518. doi:10.1111/j.1365-2133.2005.07082.x
64. Ricci G, Bendandi B, Bellini F, Patrizi A, Masi M. Atopic dermatitis: quality of life of young Italian children and their families and correlation with severity score. Pediatr Allergy Immunol. 2007;18(3):245–249. doi:10.1111/j.1399-3038.2006.00502.x
65. Ben-Gashir MA, Seed PT, Hay RJ. Are quality of family life and disease severity related in childhood atopic dermatitis? J Eur Acad Dermatol Venereol. 2002;16(5):455–462. doi:10.1046/j.1468-3083.2002.00495.x
66. Zuberbier T, Orlow SJ, Paller AS, et al. Patient perspectives on the management of atopic dermatitis. J Allergy Clin Immunol. 2006;118(1):226–232. doi:10.1016/j.jaci.2006.02.031
67. Haufe E, Abraham S, Heratizadeh A, et al. [Decreased professional performance and quality of life in patients with moderate-to-severe atopic eczema: results from the German atopic eczema registry TREATgermany]. Hautarzt. 2018;69(10):815–824. doi:10.1007/s00105-018-4261-z
68. Haruna F, Lipsett A, Marignol L. Topical management of acute radiation dermatitis in breast cancer patients: a systematic review and meta-analysis.. Anticancer Res. 2017;37(10):5343–5353. doi:10.21873/anticanres.11960
69. Dalenc F, Ribet V, Rossi AB, et al. Efficacy of a global supportive skin care programme with hydrotherapy after non-metastatic breast cancer treatment: a randomised, controlled study. Eur J Cancer Care. 2018;27(1):e12735. doi:10.1111/ecc.12735
70. Chernyshov PV, Tomas-Aragones L, Manolache L, et al. Which acne treatment has the best influence on health-related quality of life? Literature review by the European academy of dermatology and venereology task force on quality of life and patient oriented outcomes. J Eur Acad Dermatol Venereol. 2018;32(9):1410–1419. doi:10.1111/jdv.15048
71. Drost BH, van de Langenberg R, Manusama OR, et al. Dermatography (Medical Tattooing) for Scars and Skin Grafts in Head and Neck Patients to Improve Appearance and Quality of Life. JAMA Facial Plast Surg. 2017;19(1):16–22. doi:10.1001/jamafacial.2016.1084
72. Serra-Añó P, Inglés M, Bou-Catalá C, Iraola-Lliso A, Espí-López GV. Effectiveness of myofascial release after breast cancer surgery in women undergoing conservative surgery and radiotherapy: a randomized controlled trial. Support Care Cancer. 2019;27(7):2633–2641. doi:10.1007/s00520-018-4544-z
73. Urakawa R, Tarutani M, Kubota K, Uejima E. Hand foot syndrome has the strongest impact on QOL in skin toxicities of chemotherapy. J Cancer. 2019;10(20):4846–4851. doi:10.7150/jca.31059
74. Carvalho D, Aguiar P, Mendes-Bastos P, Palma-Carlos A, Freitas J, Ferrinho P. Quality of life and characterization of patients with atopic dermatitis in Portugal - QUADEP study. J Investig Allergol Clin Immunol. 2019. doi:10.18176/jiaci.0443
75. David SE, Ahmed Z, Salek MS, Finlay AY. Does enough quality of life-related discussion occur during dermatology outpatient consultations? Br J Dermatol. 2005;153(5):997–1000. doi:10.1111/j.1365-2133.2005.06876.x
76. Carr T, Harris D, James C. The Derriford Appearance Scale (DAS-59): a new scale to measure individual responses to living with problems of appearance. Br J Health Psychol. 2000;5(2):201–215. doi:10.1348/135910700168865
77. Den Ouden H, Vos RC, Rutten G. Effectiveness of shared goal setting and decision making to achieve treatment targets in type 2 diabetes patients: a cluster-randomized trial (OPTIMAL). Health Expect. 2017;20(5):1172–1180. doi:10.1111/hex.12563
78. Stiggelbout AM, Van der Weijden T, De Wit MP, et al. Shared decision making: really putting patients at the centre of healthcare. BMJ. 2012;344:e256. doi:10.1136/bmj.e256
79. Brown A. Implications of patient shared decision-making on wound care. Br J Community Nurs. 2013;18(Sup6):SS26. doi:10.12968/bjcn.2013.18.Sup6.S26
80. LeBovidge J, Borok J, Udkoff J, Yosipovitch G, Eichenfield LF. Atopic dermatitis: therapeutic care delivery: therapeutic education, shared decision-making, and access to care. Semin Cutan Med Surg. 2017;36(3):131–136. doi:10.12788/j.sder.2017.029
81. Kwong BY. Outcomes of embedding dermatologic care within oncology practices for patients with cancer. JAMA Dermatol. 2020;156(10):1051. doi:10.1001/jamadermatol.2020.1794
82. Chen ST, Molina GE, Lo JA, et al. Dermatology consultation reduces interruption of oncologic management among hospitalized patients with immune-related adverse events: a retrospective cohort study. J Am Acad Dermatol. 2020;82(4):994–996. doi:10.1016/j.jaad.2019.09.026
83. Naidoo J, Zhang J, Lipson EJ, et al. A multidisciplinary toxicity team for cancer immunotherapy-related adverse events. J Natl Compr Canc Netw. 2019;17(6):712–720. doi:10.6004/jnccn.2018.7268
84. Beamer LC, Grant GM. Skin-related quality of life among midwestern US community-based women with breast cancer experiencing radiodermatitis. Asia Pac J Oncol Nurs. 2019;6(1):50–56. doi:10.4103/apjon.apjon_40_18
85. Marinello E, Linder D, Spoto A, et al. Assessing the impact of atopic dermatitis on the patients’ parents with the visual instrument ‘Caregiver-PRISM’. Dermatology. 2016;232(4):490–495. doi:10.1159/000448030
86. Fuzissaki MA, Paiva CE, Oliveira MA, Lajolo Canto PP, Paiva Maia YC. The impact of radiodermatitis on breast cancer patients’ quality of life during radiotherapy: a prospective cohort study. J Pain Symptom Manage. 2019;58(1):92–99.e91. doi:10.1016/j.jpainsymman.2019.03.017
87. Chernyshov PV, Tomas-Aragones L, Manolache L, et al. Quality of life measurement in atopic dermatitis. Position paper of the European Academy of Dermatology and Venereology (EADV) Task Force on quality of life. J Eur Acad Dermatol Venereol. 2017;31(4):576–593. doi:10.1111/jdv.14058
88. Vakharia PP, Cella D, Silverberg JI. Patient-reported outcomes and quality of life measures in atopic dermatitis. Clin Dermatol. 2018;36(5):616–630. doi:10.1016/j.clindermatol.2018.05.011
89. Na CH, Chung J, Simpson EL. Quality of life and disease impact of atopic dermatitis and psoriasis on children and their families. Children. 2019;6:12. doi:10.3390/children6120133
90. Heinl D, Prinsen CAC, Sach T, et al. Measurement properties of quality-of-life measurement instruments for infants, children and adolescents with eczema: a systematic review. Br J Dermatol. 2017;176(4):878–889. doi:10.1111/bjd.14966
91. Pattinson RL, Trialonis-Suthakharan N, Gupta SG, et al. Patient-reported measures in dermatology: a systematic review. Eur Acad Dermatol Venereol. 2019.
92. Global Skin. About GRIDD. Available from: https://globalskin.org/research/gridd-about.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.