Back to Journals » Psychology Research and Behavior Management » Volume 15
The Hidden Factors Affecting Academic Performance Among Chinese Middle School Students: Traumatic Experience and Posttraumatic Stress Symptoms
Authors Zhou Y, Wang J, Zhou N, Zhan J, Sun L, Xing C, Liu N, Wang X ![]() , Liu W
, Liu W ![]()
Received 18 October 2021
Accepted for publication 15 December 2021
Published 11 January 2022 Volume 2022:15 Pages 111—121
DOI https://doi.org/10.2147/PRBM.S343452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Yaoguang Zhou,1,2,* Jing Wang,3,* Na Zhou,1,* Jingye Zhan,1,2,* Luna Sun,1,2 Chenqi Xing,1,2 Nianqi Liu,1,2 Xing Wang,4 Weizhi Liu1,2
1The Emotion & Cognition Lab, Faculty of Psychology and Mental Health, Naval Medical University, Shanghai, People’s Republic of China; 2Lab for Post-Traumatic Stress Disorder, Faculty of Psychology and Mental Health, Naval Medical University, Shanghai, People’s Republic of China; 3Department of Sports and Health, Shanghai Lixin University of Accounting and Finance, Shanghai, 201620, People’s Republic of China; 4Shanghai University of Sport, Shanghai, 200438, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weizhi Liu
The Emotion & Cognition Lab and Lab for Post-Traumatic Stress Disorder, Faculty of Psychology and Mental Health, Naval Medical University, 800 Xiangyin Road, Shanghai, 200433, People’s Republic of China
Tel/Fax +86-21-81871671
Email [email protected]
Xing Wang
Shanghai University of Sport, Shanghai, 200438, People’s Republic of China
Email [email protected]
Background and Purpose: The role of posttraumatic stress disorder (PTSD) in the path from traumatic exposure (TE) to academic performance (AP) is still not explicitly illustrated. The current study aimed to examine the moderator role of PTSD on the relationship between TE and AP, and then to investigate whether this moderator role is influenced by gender.
Participants and Methods: A sample of Chinese students (n=235) who had experienced the major earthquake of Wenchuan was chosen. PTSD and TE were measured by the Impact of Event Scale – Revised (IES-R) and an earthquake-related experience questionnaire, respectively. AP was collected from their up-to-date general examination. Data for 221 participants (53.4% female; mean age=14.03 years, SD=0.824) were finally included in the analysis. Parsimonious latent-variable interaction analysis and hierarchical regression analysis were adopted to examine the moderator role of PTSD.
Results: The average IES-R score was 27.57 (SD=13.265, range 0– 67). The average score for earthquake exposure was 5.86 (SD=2.069, range 1– 12). The results showed that both TE and the interaction term of PTSD*TE had significant negative correlations with AP, while PTSD was not associated with AP. Subsequent hierarchical regression analysis found that the relationship of the interaction term and AP was only significant in female students, and a simple slope plot showed a distinct pattern of the moderating effect of PTSD in both genders.
Conclusion: This study supported that PTSD moderated the connection between TE and AP in middle school students who had undergone a major earthquake trauma, which was influenced by gender. Students who experienced major trauma with drastic exposure history and manifested PTSD symptoms need specified intervention to avoid further deterioration in performance in school.
Keywords: trauma, posttraumatic stress disorder, academic performance, moderator, gender difference
Introduction
Suffering trauma, such as a natural disaster (eg, major earthquake), intrapersonal violence, and sexual assault, is a common phenomenon on a worldwide scale. According to a global mental health survey, seven-tenths of people had undergone a traumatic event, and one-third of people had been exposed to four or more traumatic events.1 As a result, those who experienced traumatic exposure (TE) had a lower quality of life under the influence of posttraumatic psychiatric problems.2 Studies have identified several negative psychological consequences in TE sufferers, including feelings of anger, fear, withdrawal, shock, guilt, confusion, nervousness, and distrust.3–5 On May 12, 2008, an earthquake with a magnitude of 8.0 on the Richter scale and a maximum intensity of over 10 at the epicenter occurred in the southwest of China and caused numerous deaths and injuries. The earthquake can be considered a major public traumatic event and provides the background to the current research.6
Posttraumatic stress disorder (PTSD) is a mental disorder that occurs after a traumatic event. The core symptoms of PTSD are intrusiveness of the traumatic event, avoidance of trauma-related stimuli, negative changes in cognition and emotion, and hypervigilance and overreaction.7 The 12-month prevalence of PTSD ranges from 0.2% to 3.8%, according to different social backgrounds and countries of residence.8 The lifetime prevalence of PTSD was estimated as 6.4% in a nationwide investigation in the USA.9 In China, the 12-month and lifetime PTSD prevalences were found to be 0.2% and 0.3%, respectively.10 After exposure to a major earthquake, there was a lack of decline in the prevalence rate of significant PTSD symptoms.7 The severity of PTSD correlates with other psychological and physical disorders, eg, over half of PTSD patients suffer from substance use disorders, and higher PTSD severity is related to poorer sleep status,9,11 ultimately leading to a reduced quality of life.12 In addition, PTSD can impair work performance in fields demanding a higher level of cognitive function, including decision making, attentional ability, and executive functions.13,14
Owing to the emphasis on education and expectations for their children, Chinese parents pay a lot of attention to their children’s school performance. Academic performance (AP) refers to one’s success and performance in school and can be measured by grade point averages (GPAs), which provide a reliable way to evaluate the general academic performance of a student15 and the competitiveness in education fulfillments for a country.16 Besides GPA, national standardized tests and total grade points of general examinations are also measurements of AP.17,18 A growing body of studies has investigated relevant factors in AP. For instance, AP may be affected by emotional intelligence, degree of effort, or lifestyle behaviors.18–20 It was also noted that girls perform better than boys on language courses, while boys outperform girls in math.21 In addition, recent research has demonstrated that physical and psychological health has significant associations with AP.17,22,23
The relationship among TE, PTSD, and AP has been widely discussed in previous research. TE has been proved to be negatively correlated with AP, which is reflected in examination scores (usually known as GPA) or adjustment to school.24–27 This effect may be mediated by psychological problems, such as anxiety, withdrawal, and aggressive behaviors, with gender differences.26 One possible mechanism is that a proportion of individuals who have been exposed to trauma suffer from PTSD, which can severely impair a person’s executive function.28 Regarding the relationship between PTSD and AP, some studies showed that students with higher self-reported PTSD symptoms were prone to having lower GPAs,29 students with lower AP had a higher prevalence of PTSD,30 and PTSD was associated with lower odds of achieving each of the educational milestones during the study period.31 Nevertheless, results from other studies found that the direct correlation between PTSD and AP was not significant.4,26 This difference can be attributed to the heterogeneity among studies, such as different study populations and social backgrounds. In addition, it could be further considered that the mediation role of effort regulation and academic locus of control may confound the relationship between PTSD and AP.4,32 Up to now, the role of PTSD in the path from TE to AP has still not been explicitly examined. The moderator role of PTSD on the relationship between a natural disaster and suicidal ideation was found in an investigation involving more than 2000 participants, which suggested that more severe PTSD symptoms impaired posttraumatic cognitive function33 and provided inspiration for the current study. Meanwhile, the majority of relevant studies focused on college students, with very few investigating middle school students. Furthermore, there was a lack of samples with the same type of major traumatic event, such as an earthquake, to control the heterogeneity in the type of trauma.
Hence, the current study was carried out to survey the TE, AP, and PTSD of middle school students who experienced a major earthquake in 2008. The hypothesis was that PTSD moderates the negative correlation between TE and AP. Considering that gender differences in the relationship among these three variables have been reported previously, and especially that more severe PTSD symptoms were prone to be reported in females,26,34 the current study further explored the effect of gender on the moderator role of PTSD.
Methods
Participants
All participants (n=235) were recruited from Mao County middle school, which was located in the severely damaged region of the M8.0 Wenchuan earthquake (41 km from the epicenter). Three grades were included: 130 of the students were in classes 6–8 of grade 7. And 73 students who were grade 8 came from classes 2 and 3. Considering that students of grade 9 had to prepare for their senior high school entrance examination, only 32 students from class 3 were recruited. Of the 235 participants, four were excluded because they reported that they had not experienced the major earthquake. Ten were removed because more than 50% of items were incomplete. Therefore, the final valid sample included 221 adolescents with an average age of 14.03 years (SD=0.824). In terms of gender, 118 (53.4%) were female and 103 (46.6%) were male. The majority of participants (197, 89.1%) reported as Qiang nationality, which is a minority ethnic group in China. Over half of students were from grade 7 (118, 53.4%), 72 were from grade 8, and 31 were from grade 9. The descriptions of the valid sample are presented in Table 1.
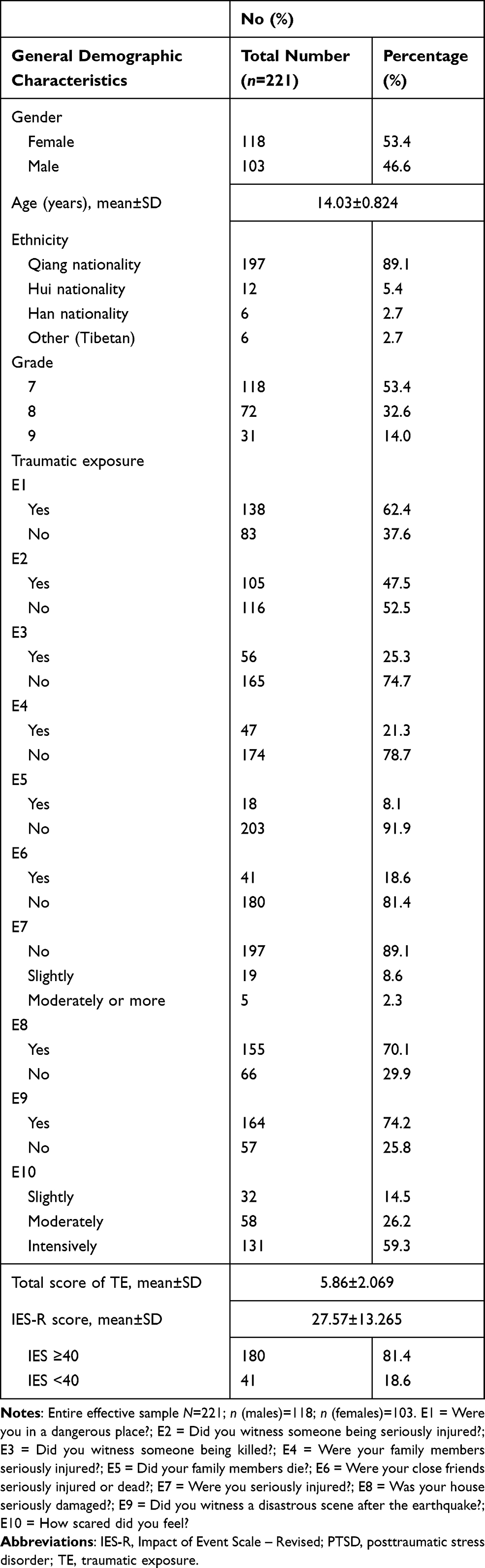 |
Table 1 Demographic Characteristics, TE, and PTSD of the Students |
Measurement
The demographic items on the questionnaire included gender, age, ethnicity, and grade.35
Impact of Event Scale – Revised (IES-R)
The Chinese version of the IES-R was adopted to evaluate the degree of PTSD.36–39 The IES-R consists of 22 items on posttraumatic symptoms, each in the form of a five-point scale: 0 indicates that the symptom occurs “not at all”; 1, “a little bit”; 2, “moderately”; 3, “quite a bit”; and 4, “extremely”. The total score ranges from 0 to 88. A critical score of 40 (total score) has been indicated to classify whether or not a student has clinically significant PTSD symptoms.40 IES-R measures are similar to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria for PTSD issued by the American Psychiatric Association, and have good psychometric properties.41,42 The IES-R subscales have high internal consistency, with Cronbach’s α ranging from 0.79 to 0.91, and test–retest reliability α ranging from 0.51 to 0.94. Furthermore, the Chinese version of IES-R has been demonstrated to have satisfactory psychometric properties.43 Cronbach’s α in the current sample was 0.885, suggesting high reliability.
Earthquake-Related Experience Questionnaire
A custom-designed earthquake-related experience questionnaire used in previous research was adapted to collect the data on the TE in the current study.2 This earthquake-related TE was made up of 10 incidents that could have occurred during or after the Wenchuan earthquake. The 10 earthquake-related incidents are shown as follows: Were you in a dangerous place (E1)?; Did you witness someone being seriously injured (E2)?; Did you witness someone being killed (E3)?; Were your family members seriously injured (E4)?; Did your family members die (E5)?; Were your close friends seriously injured or dead (E6)?; Were you seriously injured (E7)?; Was your house seriously damaged (E8)?; Did you witness a disastrous scene after the earthquake (E9)?; and How scared did you feel (E10)? E7 was estimated on a three-point Likert scale, ranging from 0 to 2: 0=not injured, 1=slightly injured, and 2=moderately injured or more. Question E10 estimated the intensity of horror related to the earthquake also measured on a three-point Likert scale, ranging from 1=slightly to 3=intensely. The remaining seven questions were coded into yes/no items, scoring 0 for no and 1 for yes. The sum of item scores reflects the exposure level of earthquake trauma.
Procedure
Academic Performance
The study protocol was approved by Ethics of Committee of the Naval Medical University. All procedures were conducted in accordance with the Declaration of Helsinki. The collection of academic performance came from an up-to-date general examination. The subjects in each grade were as follows: grade 7 included Chinese, Math, English, Politics, History, Geography, and Biology; grade 8 included Chinese, Math, English, Politics, History, Geography, Biology, and Physics; and grade 9 included Chinese, Math, English, Politics, History, Physics, and Chemistry. Since there were specified subjects in each grade and the total examination scores were different, the total score for each student was first calculated as a T score and then multiplied by 10 to obtain the final transformed score to make the AP in all students comparable. The raw and transformed AP scores for all students are presented in Table S1.
Measurement of IES-R and Earthquake TE
The test was performed by an expert interviewer, using the IES-R and earthquake experience questionnaire, 3 years after the Wenchuan earthquake. It took about 30 minutes to complete the measures, and every student completed the questionnaires without pay. All students were measured during their rest period (from 12 noon to 2 pm). Informed consent to participate in the study was obtained from the parents or guardians of the subjects prior to study commencement. To respect the students’ opinions and protect their interests, they all read the informed consent form before the study.
Statistical Analysis
The data were analyzed using SPSS software (version 21.0; IBM Corp, Armonk, NY, USA). No case reported more than 10% missing data, and missing values were replaced by multiple imputation using regression methods. The normality was tested by skewness and kurtosis for each variable. Variables (TE, PTSD measured by IES-R, and AP) showed a univariate normal distribution, with the skewness and kurtosis ranging from −1 to 1. Correlation coefficients were calculated to show the inter-correlations between variables. The moderator role of PTSD between TE and AP was tested using two techniques: 1) a parsimonious latent-variable interaction technique in the structural equation model (SEM) using AMOS 22;44 and 2) hierarchical regression analysis in SPSS. On the one hand, the parsimonious latent-variable interaction technique can include the measurement errors and indicators of the higher order factors. Ping suggested that the product of the sums of the relevant indicators be used as the sole indicator of the latent product. For example, x1, x2 and z1, z2 indicated two latent variables, X and Z, respectively. X and Z were hypothesized to interact in their effect on a third latent variable. The computed variable [(x1 + x2) * (z1 + z2)] could be used as the indicator of the latent product of interaction.44,45 In the current study, the indicators of TE are Eq1 and Eq2. Eq1 is the aggregated score of items related to events that happened to oneself (including E1, E7, E8, E9, and E10). Eq2 is the aggregated score of items related to events that happened to others (including E2, E3, E4, E5, and E6). And indicators of PTSD are P1, P2, and P3, which are the summed score of items for intrusion, avoidance, and hyperarousal, respectively. The computed variable [(Eq1 + Eq2) * (P1 + P2 + P3)] was used as the indicator of the latent product of the interaction term. On the other hand, hierarchical regression provided details for directly assessing the change in explanatory power between iterative steps. All variables were standardized to reduce the potential effects of multicollinearity.46 The technique of least squares was used, with the control variables entered as a block in step 1 (gender and grade), followed by the main effects in step 2 (PTSD and TE), and the interaction and moderators in step 3. The gender difference was tested in hierarchical regression by conducting subsequent regression analysis under subgroups of males and females.
Results
Severity of PTSD Symptoms, TE, and AP
As shown in Table 1, the average IES-R score was 27.57 (SD=13.265, range 0–67). According to the cut-off score of the IES-R (≥40), a total of 41 participants (18.6%) were screened as probable PTSD cases. The features of earthquake exposure are also presented in Table 1. The average score of earthquake exposure was 5.86 (SD=2.069, range 1–12). As AP was standardized in this sample, the mean and SD of AP were 500.00 and 10.00, respectively. Raw and transformed scores of AP for all students are presented in Table S1.
Outcomes of Correlation Analysis
The results of bivariate correlation analysis of gender, grade, TE, IES-R score, and AP showed that there were significant correlations between TE level and IES-R score (r=0.252, p<0.01), and between TE level and AP (r=−0.264, p<0.01). The correlation between IES-R score and AP was not significant (r=−0.093, p=0.166). The results are presented in Table 2.
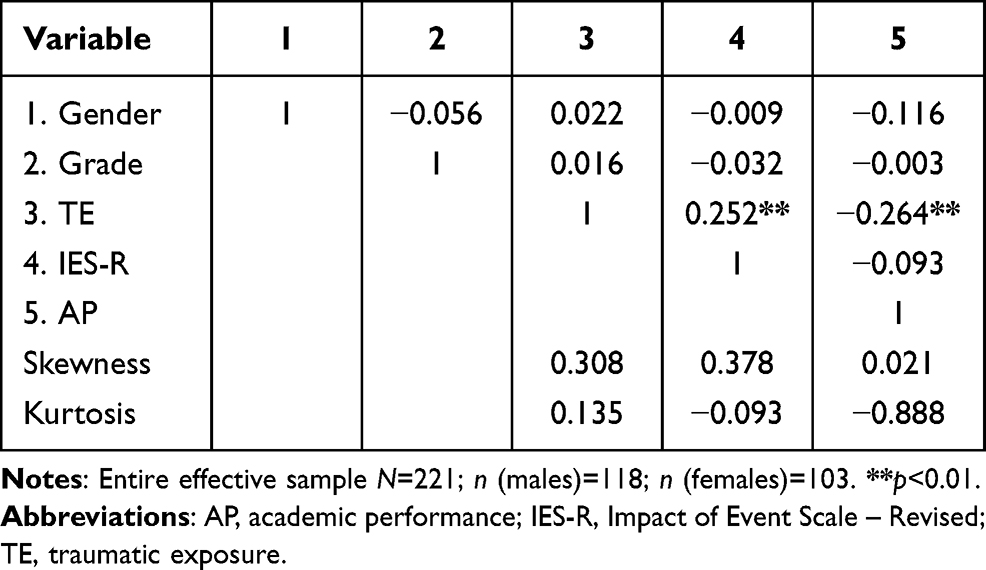 |
Table 2 Bivariate Correlation Analysis of Gender, Grade, TE, IES-R Score, and AP |
Outcomes of Parsimonious Latent-Variable Interaction Analysis
As shown in Table 3 and Figure 1, all latent variables had factor loading of more than 0.55 on the indicators, except for Eq2 (β=0.492, p<0.001), with a significant correlation (p<0.01). The results showed that TE had a significant negative correlation with AP (β=−0.431, p<0.01), and the correlation between PTSD and AP was not significant (β=0.099, p=0.332). The interaction term PTSD*TE was significantly correlated with AP (β=−0.305, p<0.01). The results of the model fit using the recommended index were: R2=0.24, CMIN=42.15, p=0.220, GFI=0.974, AGFI=0.938, CFI=0.991, RMSEA=0.020, and SRMR=0.050, suggesting a good model fit.47
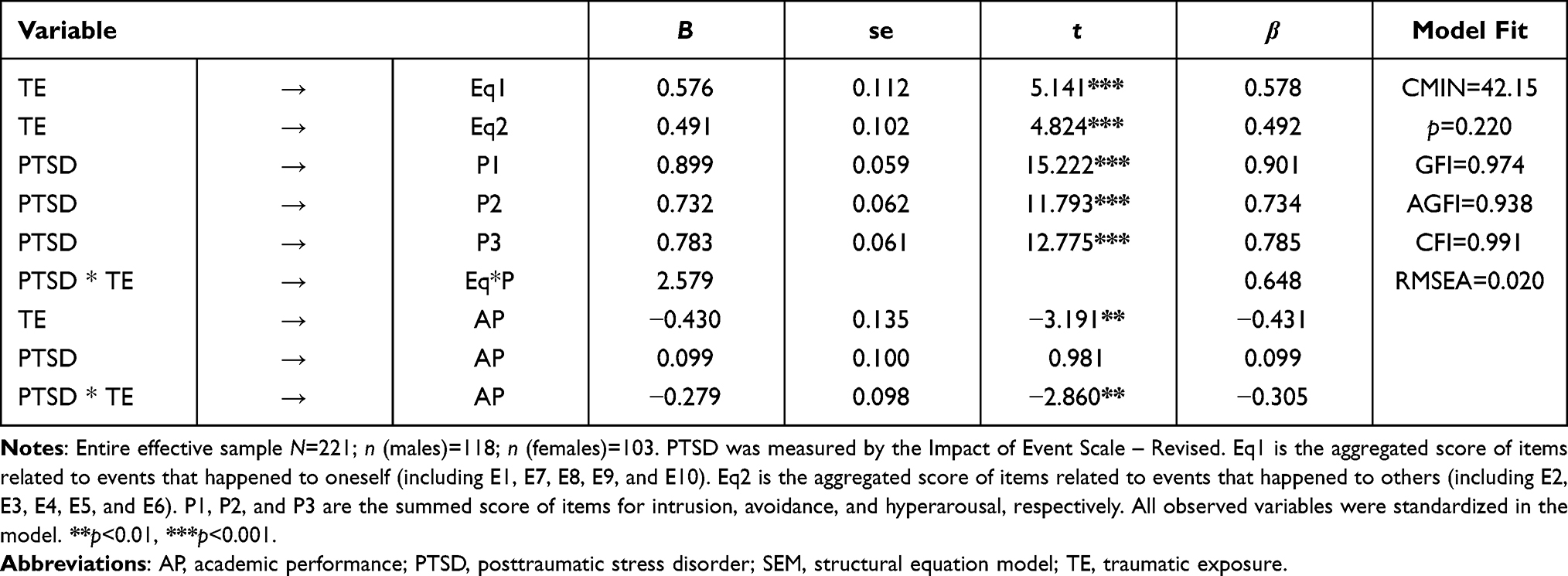 |
Table 3 Results of Parsimonious Latent-Variable Interaction Analysis in SEM to Test the Moderator Role of PTSD Between TE and AP |
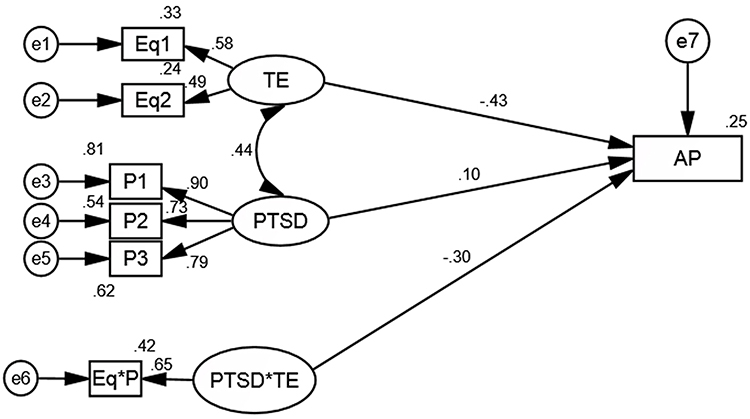 |
Figure 1 Moderator role of PTSD between TE and AP in SEM using parsimonious latent-variable interaction analysis. Abbreviations: AP, academic performance; PTSD, posttraumatic stress disorder; SEM, structural equation model; TE, traumatic exposure. Notes: PTSD was measured by the Impact of Event Scale – Revised. Eq1 is the aggregated score of items related to events that happened to oneself (including E1, E7, E8, E9, and E10). Eq2 is the aggregated score of items related to events that happened to others (including E2, E3, E4, E5, and E6). P1, P2, and P3 are the summed scores of items for intrusion, avoidance, and hyperarousal, respectively. All observed variables were standardized in the model. |
Outcomes of Hierarchical Regression Analysis
In step 1 (R2=0.014, F=1.500, p=0.225), two control variables were not significantly associated with AP (gender: β=−0.117, p=0.085; grade: β=−0.009, p=0.890). In step 2 (R2=0.083, F=4.868, p=0.001), the main effect of TE was significant (β=−0.254, p<0.001), while PTSD did not have a significant effect on AP (β=−0.031, p=0.649). In step 3 (R2=0.112, F=5.984, p<0.001), TE was still negatively associated with AP (β=−0.258, p<0.001), and the interaction term PTSD*TE also had a significant negative effect on AP (β=−0.201, p<0.01). PTSD was still not significantly correlated with AP (β=−0.018, p=0.782). Concerning gender differences in step 3 (female: R2=0.129, F=4.178, p<0.01; male: R2=0.119, F=3.297, p<0.05), the non-significant correlation between PTSD and AP were consistent in the subgroups of females and males (female: β=0.081, p=0.369; male: β=−0.136, p=0.178). TE in both subgroups was significantly associated with AP (female: β=−0.255, p<0.01; male: β=−0.252, p<0.05). PTSD*TE was only significantly correlated with AP in females (female: β=−0.244, p<0.01; male: β=−0.127, p=0.200). Concerning the model fit, R2 values were 0.112, 0.129, and 0.119 for the whole sample, females, and males, respectively, in step 3. See Table 4.
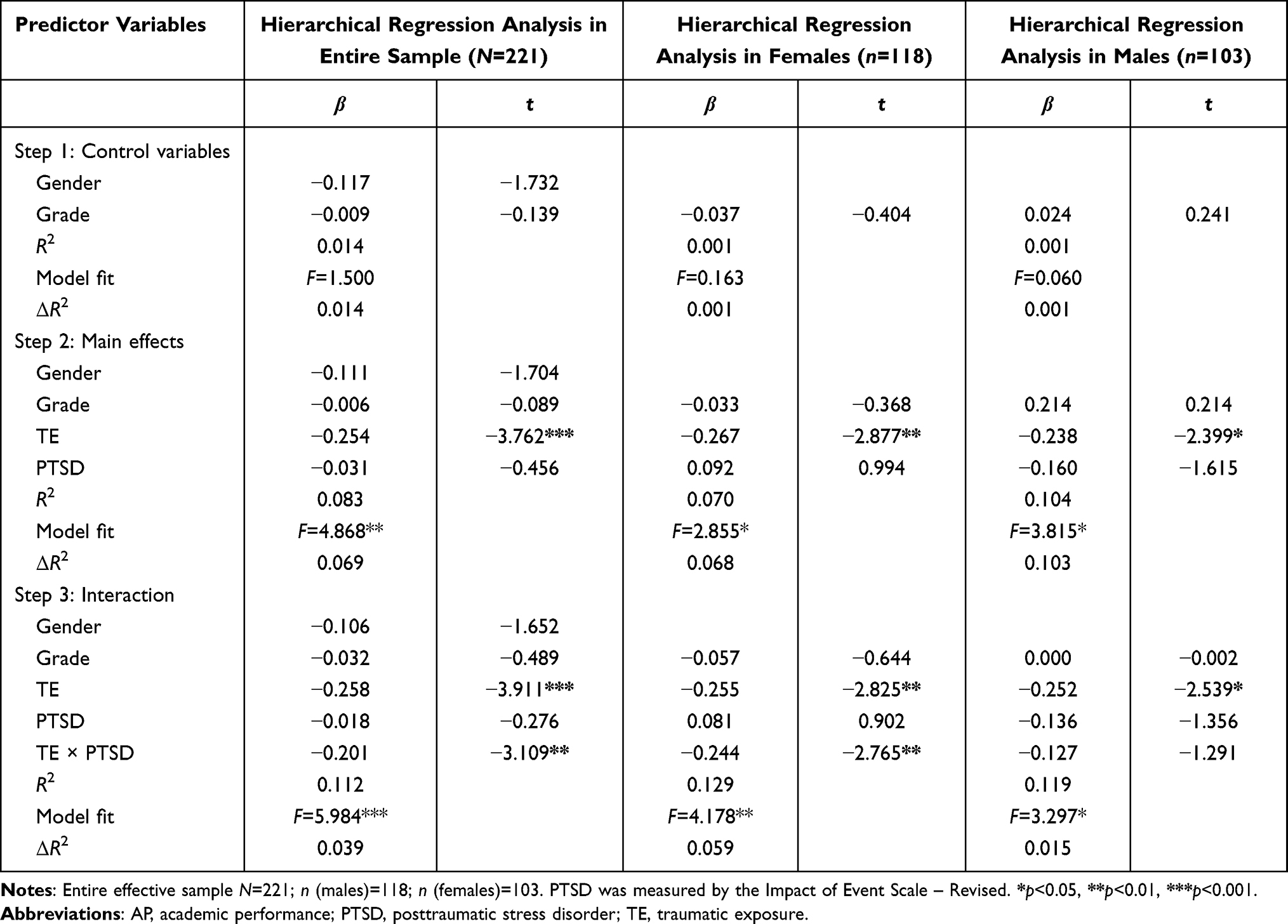 |
Table 4 Standardized Results of Hierarchical Regression Analysis Testing the Moderator Role of PTSD Between TE and AP, and Gender Differences on the Moderator Effect |
The simple slope interaction plot showing the moderating effect of PTSD is presented in Figure 2. For all participants, the simple slope for the low value of the moderator (−1 SD) was −0.018 (SE=0.088, t=−0.204, p=0.839), and for the high value of the moderator (+1 SD) was −0.406 (SE=0.091, t=−4.484, p<0.001). In females, the simple slope for the low value of the moderator (−1 SD) was −0.030 (SE=0.122, t=−0.245, p=0.807), and for the high value of the moderator (+1 SD) was −0.478 (SE=0.091, t=−3.903, p<0.001). In males, the simple slope for the low value of the moderator (−1 SD) was −0.122 (SE=0.134, t=−0.909, p=0.364), and for the high value of the moderator (+1 SD) was −0.378 (SE=0.148, t=−2.548, p<0.05).
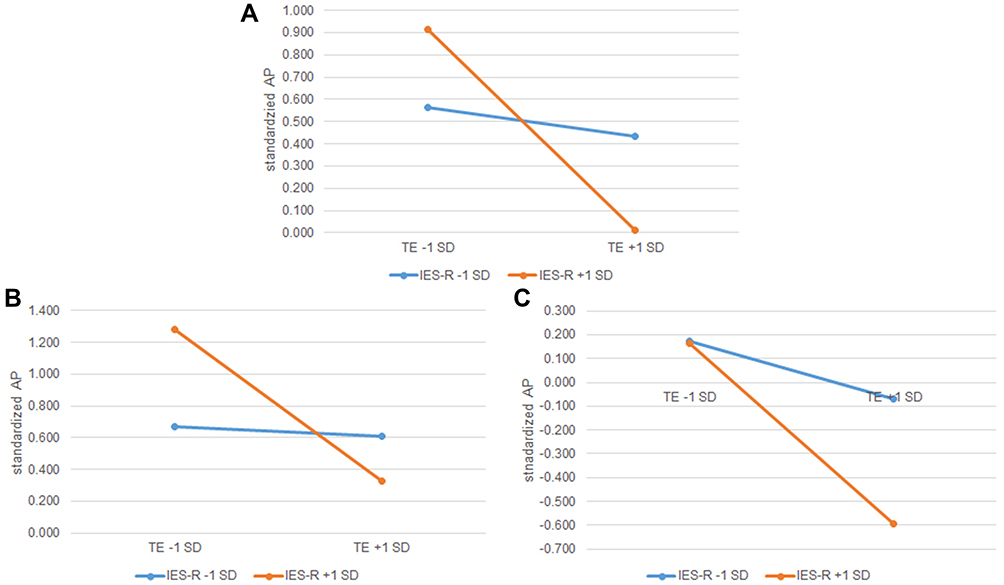 |
Figure 2 Slope plot of the moderating effect of PTSD on the relationship between TE and AP in (A) all participants, (B) females, and (C) males. Notes: AP, academic performance; IES-R, Impact of Event Scale – Revised; PTSD, posttraumatic stress disorder; TE, traumatic exposure. |
Discussion
The moderating effect of PTSD has been presented as the negative correlation between TE and AP, which was affected by gender (Figure 3), in a sample of middle school students who had undergone a major trauma, 3 years after the event. It could be further elaborated that the AP of individuals with slighter PTSD symptoms was less affected by the level of TE, while the AP of those with more severe PTSD symptoms declined more dramatically along with the increasing level of TE.
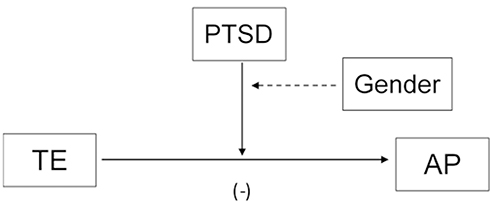 |
Figure 3 Influence of gender on the moderator role of PTSD between AP and TE. Notes: AP, academic performance; PTSD, posttraumatic stress disorder; TE, traumatic exposure. |
Students who had experienced trauma and showed less severe PTSD symptoms were expected to have stronger psychological resilience, which contributed to their adjustment to school and protected them from declining AP.24,48,49 For those with high PTSD scores, previous research in patients diagnosed with PTSD or individuals with observable PTSD symptoms (such as partial PTSD) found associations with functional impairments in brain regions related to attention (prefrontal cortex), memory (hippocampus), and regulation of emotions (amygdala).50 In addition, poorer performances on the spatial span forward subtest and execution time and accuracy in the Stroop test were found in a PTSD-positive group compared to healthy controls.13 Those dysfunctions directly worsened the performance in learning activity since they were intimately related to executive function, which was further exacerbated by a higher level of TE. TE was also closely related to executive function. It was reported that TE was associated with poorer performance on working memory, inhibition, auditory attention, and processing speed tasks in children.28 However, Cohodes et al did not find any significant correlations among TE, PTSD, and executive function, and pointed out that their relationships might be nuanced in children.51 Hence, detecting the moderator role of PTSD provided a new path for further investigation in this field.
Gender differences in the moderator role of PTSD were also observed in the current study. In female students with lower TE, those who reported more severe PTSD symptoms tended to achieve higher examination scores than those who did not. In the female subgroup with higher TE, students with more severe PTSD symptoms achieved lower AP than those with slighter symptoms. In the group of male students, the AP of students who reported a higher score for PTSD symptoms consistently had lower AP than those with lower PTSD scores. And when the level of TE increased, AP declined more drastically in the subgroup with more severe PTSD symptoms. This gender difference may mainly derived from the gender difference in AP, in that females tended to perform better than males.52,53 As a result, female middle school students with more severe PTSD symptoms may put more diligence into study than those with slighter PTSD symptoms as a coping method for posttraumatic psychological distress, such as intrusion.32 But for those who had experienced extremely disastrous traumatic scenes and had severe PTSD symptoms, their mental health state was too seriously disturbed to outperform those with slighter PTSD scores on learning activities. Worse still, this dysfunction might not be easily observed by teachers or parents because these children used engagement in study as a suppressor of their discomfort. Thus, it was difficult to offer them prompt and effective psychological intervention. Consistent with previous studies,4,26 PTSD and AP were not directly associated in the current study. The moderator role of PTSD identified from the results provided another possible explanation for this non-significant correlation. It can be inferred that students who have experienced major trauma with a drastic exposure history and manifest PTSD symptoms need specified intervention to avoid further impairment in AP, which is crucial for future development in adolescents.
Limitations of this article include the partial nature of the retrospective study, which may cause possible recall bias in TE, not using a PTSD interview scale to strengthen the validity, and the lack of a non-trauma control group to investigate the effects of major trauma on AP and PTSD. The results of moderator analysis were confounded by the large variance in the number of students from each grade, and the significance was affected by the relatively small sample size.
Conclusion
Under the influence of major trauma, the level of TE was negatively correlated with AP and PTSD in Chinese middle school students, 3 years after the traumatic event. Importantly, PTSD moderated the relationship between TE and AP, which was further influenced by gender. The students showing lower PTSD symptoms after trauma were unlikely to be affected by the level of TE on AP, while TE was more negatively correlated with AP in those with more severe PTSD symptoms. Thus, it could be inferred that having severe PTSD symptoms with a high level of TE was a robust indicator to predict poor AP in school. Children with this combination of problems should receive immediate help and effective intervention to prevent deterioration in their future development.
Acknowledgments
The authors would like to acknowledge the volunteers who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China (32071086).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Benjet C, Bromet E, Karam EG, et al. The epidemiology of traumatic event exposure worldwide: results from the World Mental Health Survey Consortium. Psychol Med. 2016;46(2):327–343. doi:10.1017/S0033291715001981
2. Hu T, Xu S, Liu W. A senior high school-based survey on the long-term impact of the Wenchuan earthquake on survivors’ quality of life: PTSD as a mediator. Psychiatry Res. 2018;270:310–316. doi:10.1016/j.psychres.2018.09.043
3. Artime TM, Buchholz KR, Jakupcak M. Mental health symptoms and treatment utilization among trauma-exposed college students. Psychol Trauma. 2019;11(3):274–282. doi:10.1037/tra0000376
4. Boyraz G, Granda R, Baker CN, Tidwell LL, Waits JB. Posttraumatic stress, effort regulation, and academic outcomes among college students: a longitudinal study. J Couns Psychol. 2016;63(4):475–486. doi:10.1037/cou0000102
5. Read JP, Ouimette P, White J, Colder C, Farrow S. Rates of DSM-IV-TR Trauma Exposure and Posttraumatic Stress Disorder Among Newly Matriculated College Students. Psychol Trauma. 2011;3(2):148–156. doi:10.1037/a0021260
6. Liang Y, Cheng J, Ruzek JI, Liu Z. Posttraumatic stress disorder following the 2008 Wenchuan earthquake: a 10-year systematic review among highly exposed populations in China. J Affect Disord. 2019;243:327–339. doi:10.1016/j.jad.2018.09.047
7. Zhou YG, Shang ZL, Zhang F, et al. PTSD: past, present and future implications for China. Chin J Traumatol. 2021;24(4):187–208. doi:10.1016/j.cjtee.2021.04.011
8. Karam EG, Friedman MJ, Hill ED, et al. Cumulative traumas and risk thresholds: 12-month PTSD in the World Mental Health (WMH) surveys. Depress Anxiety. 2014;31(2):130–142. doi:10.1002/da.22169
9. Pietrzak RH, Goldstein RB, Southwick SM, Grant BF. Prevalence and Axis I comorbidity of full and partial posttraumatic stress disorder in the United States: results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J Anxiety Disord. 2011;25(3):456–465. doi:10.1016/j.janxdis.2010.11.010
10. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/s2215-0366(18)30511-x
11. Wu L, Guo X, Shang Z, et al. China experience from COVID-19: mental health in mandatory quarantine zones urgently requires intervention. Psychol Trauma. 2020;12(S1):S3–S5. doi:10.1037/tra0000609
12. Pietrzak RH, Tsai J, Armour C, Mota N, Harpaz-Rotem I, Southwick SM. Functional significance of a novel 7-factor model of DSM-5 PTSD symptoms: results from the National Health and Resilience in Veterans study. J Affect Disord. 2015;174:522–526. doi:10.1016/j.jad.2014.12.007
13. Flaks MK, Malta SM, Almeida PP, et al. Attentional and executive functions are differentially affected by post-traumatic stress disorder and trauma. J Psychiatr Res. 2014;48(1):32–39. doi:10.1016/j.jpsychires.2013.10.009
14. Regehr C, LeBlanc VR. PTSD, Acute Stress, Performance and Decision-Making in Emergency Service Workers. J Am Acad Psychiatry Law. 2017;45(2):184–192.
15. Meece JL, Anderman EM, Anderman LH. Classroom goal structure, student motivation, and academic achievement. Ann Rev Psychol. 2006;57:487–503. doi:10.1146/annurev.psych.56.091103.070258
16. Donnelly JE, Hillman CH, Castelli D, et al. Physical activity, fitness, cognitive function, and academic achievement in children: a systematic review. Med Sci Sports Exerc. 2016;48(6):1197–1222. doi:10.1249/mss.0000000000000901
17. Muntaner-Mas A, Palou P, Vidal-Conti J, Esteban-Cornejo I, Mediation A. Analysis on the relationship of physical fitness components, obesity, and academic performance in children. J Pediatr. 2018;198:90–97.e4. doi:10.1016/j.jpeds.2018.02.068
18. Dumuid D, Olds T, Martin-Fernandez JA, Lewis LK, Cassidy L, Maher C. Academic performance and lifestyle behaviors in Australian school children: a cluster analysis. Health Educ Behav. 2017;44(6):918–927. doi:10.1177/1090198117699508
19. Wijekoon CN, Amaratunge H, de Silva Y, Senanayake S, Jayawardane P, Senarath U. Emotional intelligence and academic performance of medical undergraduates: a cross-sectional study in a selected university in Sri Lanka. BMC Med Educ. 2017;17(1):176. doi:10.1186/s12909-017-1018-9
20. Egeland J, Johansen SN, Ueland T. Do low-effort learning strategies mediate impaired memory in ADHD? J Learn Disabil. 2010;43(5):430–440. doi:10.1177/0022219409355473
21. Voyer D, Voyer SD. Gender differences in scholastic achievement: a meta-analysis. Psychol Bull. 2014;140(4):1174–1204. doi:10.1037/a0036620
22. Sijtsema JJ, Verboom CE, Penninx BW, Verhulst FC, Ormel J. Psychopathology and academic performance, social well-being, and social preference at school: the TRAILS study. Child Psychiatry Hum Dev. 2014;45(3):273–284. doi:10.1007/s10578-013-0399-1
23. Moreira de Sousa J, Moreira CA, Telles-Correia D. Anxiety, depression and academic performance: a study amongst Portuguese medical students versus non-medical students. Acta Med Port. 2018;31(9):454–462. doi:10.20344/amp.9996
24. Banyard VL, Cantor EN. Adjustment to college among trauma survivors: an exploratory study of resilience. J Coll Stud Dev. 2004;45(2):207–221. doi:10.1353/csd.2004.0017
25. Duncan RD. Childhood maltreatment and college drop-out rates: implications for child abuse researchers. J Interpers Violence. 2000;15(9):987–995. doi:10.1177/088626000015009005
26. Voisin DR, Neilands TB, Hunnicutt S. Mechanisms linking violence exposure and school engagement among african American adolescents: examining the roles of psychological problem behaviors and gender. Am J Orthopsychiatry. 2011;81(1):61–71. doi:10.1111/j.1939-0025.2010.01072.x
27. Nikulina V, Widom CS, Czaja S. The role of childhood neglect and childhood poverty in predicting mental health, academic achievement and crime in adulthood. Am J Community Psychol. 2011;48(3–4):309–321. doi:10.1007/s10464-010-9385-y
28. DePrince AP, Weinzierl KM, Combs MD. Executive function performance and trauma exposure in a community sample of children. Child Abuse Negl. 2009;33(6):353–361. doi:10.1016/j.chiabu.2008.08.002
29. Boyraz G, Horne SG, Owens AC, Armstrong AP. Academic achievement and college persistence of African American students with trauma exposure. J Couns Psychol. 2013;60(4):582–592. doi:10.1037/a0033672
30. Pereira JL, Guedes-Carneiro GM, Netto LR, et al. Types of trauma, posttraumatic stress disorder, and academic performance in a population of university students. J Nerv Ment Dis. 2018;206(7):507–512. doi:10.1097/NMD.0000000000000842
31. Vilaplana-Perez A, Sidorchuk A, Perez-Vigil A, et al. Assessment of posttraumatic stress disorder and educational achievement in Sweden. JAMA Netw Open. 2020;3(12):e2028477. doi:10.1001/jamanetworkopen.2020.28477
32. Boyraz G, Zhu Y, Waits JB. Avoidance coping and academic locus of control as mediators of the relationship between posttraumatic stress and academic achievement among first-year college students. Anxiety Stress Coping. 2019;32(5):545–558. doi:10.1080/10615806.2019.1638681
33. Brown LA, Fernandez CA, Kohn R, Saldivia S, Vicente B. Pre-disaster PTSD as a moderator of the relationship between natural disaster and suicidal ideation over time. J Affect Disord. 2018;230:7–14. doi:10.1016/j.jad.2017.12.096
34. Liu N, Zhang F, Wei C, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. 2020;287:112921. doi:10.1016/j.psychres.2020.112921
35. Liu Z, Zeng Z, Xiang Y, et al. A cross-sectional study on posttraumatic impact among Qiang women in Maoxian County 1 year after the Wenchuan Earthquake, China. Asia Pacific j Public Health. 2012;24(1):21–27. doi:10.1177/1010539510373945
36. Warsini S, Buettner P, Mills J, West C, Usher K. Psychometric evaluation of the Indonesian version of the Impact of Event Scale-Revised. J Psychiatr Ment Health Nurs. 2015;22(4):251–259. doi:10.1111/jpm.12194
37. Morina N, Ehring T, Priebe S. Diagnostic utility of the impact of event scale-revised in two samples of survivors of war. PLoS One. 2013;8(12):e83916. doi:10.1371/journal.pone.0083916
38. Christianson S, Marren J. The Impact of Event Scale - Revised (IES-R). Medsurg Nursing. 2012;21(5):321–322.
39. Coffey SF, Schumacher JA, Nosen E, et al. Trauma-focused exposure therapy for chronic posttraumatic stress disorder in alcohol and drug dependent patients: a randomized controlled trial. Psychol Addictive Behav. 2016;30(7):778–790. doi:10.1037/adb0000201
40. Bienvenu OJ, Williams JB, Yang A, Hopkins RO, Needham DM. Posttraumatic stress disorder in survivors of acute lung injury: evaluating the Impact of Event Scale-Revised. Chest. 2013;144(1):24–31. doi:10.1378/chest.12-0908
41. Battle DE. Diagnostic and Statistical Manual of Mental Disorders (DSM). CoDAS. 2013;25(2):191–192. doi:10.1590/s2317-17822013000200017
42. Liew TM, Feng L, Gao Q, Ng TP, Yap P. Diagnostic utility of Montreal Cognitive Assessment in the Fifth Edition of Diagnostic and Statistical Manual of Mental Disorders: major and mild neurocognitive disorders. J Am Med Dir Assoc. 2015;16(2):144–148. doi:10.1016/j.jamda.2014.07.021
43. Wu KK, Chan KS. The development of the Chinese version of Impact of Event Scale–Revised (CIES-R). Soc Psychiatry Psychiatr Epidemiol. 2003;38(2):94–98. doi:10.1007/s00127-003-0611-x
44. Ping R. A parsimonious estimating technique for interaction and quadratic latent variables. J Marketing Res. 1995;32:336. doi:10.2307/3151985
45. Cortina JM, Chen G, Dunlap WP. Testing Interaction Effects in LISREL: examination and Illustration of Available Procedures. Org Res Methods. 2001;4(4):324–360. doi:10.1177/109442810144002
46. Cohen J, Cohen P, West SG, Aiken LS. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences.
47. Jackson DL, Gillaspy JA, Purc-Stephenson R. Reporting practices in confirmatory factor analysis: an overview and some recommendations. Psychol Methods. 2009;14(1):6–23. doi:10.1037/a0014694
48. Horn SR, Feder A. Understanding Resilience and Preventing and Treating PTSD. Harv Rev Psychiatry. 2018;26(3):158–174. doi:10.1097/hrp.0000000000000194
49. Trigueros R, Padilla A, Aguilar-Parra JM, Mercader I, López-Liria R, Rocamora P. The Influence of Transformational Teacher Leadership on Academic Motivation and Resilience, Burnout and Academic Performance. Int J Environ Res Public Health. 2020;17(20):7687. doi:10.3390/ijerph17207687
50. Kunimatsu A, Yasaka K, Akai H, Kunimatsu N, Abe O. MRI findings in posttraumatic stress disorder. J Magnetic Resonance Imaging. 2020;52(2):380–396. doi:10.1002/jmri.26929
51. Cohodes EM, Chen SH, Lieberman AF, Bush NR. Examination of the associations between young children’s trauma exposure, trauma-symptomatology, and executive function. Child Abuse Negl. 2020;108:104635. doi:10.1016/j.chiabu.2020.104635
52. Lu Y, Shi X, Zhong S. Competitive experience and gender difference in risk preference, trust preference and academic performance: evidence from Gaokao in China. J Comp Econ. 2018;46(4):1388–1410. doi:10.1016/j.jce.2018.05.002
53. Sindhuja A, Nadiger V, Kisan R, Deshpande D. Gender differences in stress and academic performance in medical students. J Res Med Edu Ethics. 2014;4:46. doi:10.5958/j.2231-6728.4.1.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.