Back to Journals » International Journal of General Medicine » Volume 18
The Hidden Angles: Predictive Indices of Degenerative Spondylolisthesis at L4-5
Authors Tao Z, Li W, Wu M, Liu X, Xiong J, Yu J, Liu H
Received 28 April 2025
Accepted for publication 13 August 2025
Published 12 September 2025 Volume 2025:18 Pages 5395—5407
DOI https://doi.org/10.2147/IJGM.S537228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Zhiqiang Tao,1 Wenhua Li,2 Mingming Wu,3 Xinquan Liu,1 Jie Xiong,1 Jiangtao Yu,1 Huan Liu1
1Third Department of Spinal Surgery, Nanchang Hongdu Hospital of TCM, Nanchang, Jiangxi, 330006, People’s Republic of China; 2School of Physical Education and Health, Nanchang Institute of Science & Technology, Nanchang, Jiangxi, 330108, People’s Republic of China; 3Department of Spinal Surgery, Lushan People’s Hospital, Jiujiang, Jiangxi, 332800, People’s Republic of China
Correspondence: Huan Liu, Nanchang Hongdu Hospital of TCM, No. 1399, Diezihu Avenue, Honggutan District, Nanchang, Jiangxi, 330006, People’s Republic of China, Email [email protected]
Objective: To examine the relationship between facet joint orientation, alignment, degeneration, and degenerative spondylolisthesis (DS) at lumbar vertebra L4-5.
Methods: A retrospective study of 114 DS patients and 114 non-DS patients admitted to our hospital from May 2019 to April 2024. We compared facet joint angle (FJA), FJA difference, FJA asymmetry, L4 inclination angle (L4IA), Weishaupt classification, paraspinal muscle cross-sectional area (CSA), pedicle-facet angle (P-F angle), and P-F angle asymmetry between the two groups. We also analyzed FJA and slippage index changes across Weishaupt grades and their correlation using Pearson correlation. The predictive value of facet joint direction indices for DS at L4-5 was assessed using ROC curves.
Results: The DS group showed reduced FJA and FJA difference, increased left asymmetry, higher L4IA levels, and a greater proportion of grade II and III in Weishaupt classification compared to the non-DS group (P< 0.05). FJA decreased while the slippage index increased with more degeneration (P< 0.05). Weishaupt classification was negatively correlated with FJA (r=− 0.823, P< 0.001), but positively with the slippage index (r=0.756, P< 0.001). The P-F angle was significantly higher in the DS group (P< 0.05). Cut-off values for FJA, L4IA, and P-F angle were 42.57, 9.63, and 122.17, with AUC values of 0.893, 0.766, and 0.858, respectively, indicating predictive value for DS at L4-5.
Conclusion: The DS group had smaller FJA, larger L4IA and P-F angle, and more severe facet joint degeneration at L4-5, suggesting a strong link between DS at L4-5 and facet joint sagittalization, levelization, and degeneration.
Keywords: sagittalization of facet joint, levelization of facet joint, degeneration degree, degenerative spondylolisthesis at lumbar vertebra 4-5
Introduction
Lumbar spondylolisthesis refers to the forward movement or sliding of one vertebral body relative to the next, and is the main cause of lower back pain. According to the different causes of onset, it can be divided into degenerative, vertebral arch, traumatic, etc. Among them, degenerative spondylolisthesis (DS) is the most common type in clinical practice, with the incidence rate of about 6%. In individuals over 50 years old, the ratio of male to female is 1:2~1:6.1,2 The L4-5 segment is the most common site of DS, with a frequency about 9 times higher than adjacent segments. Patients with DS may experience lower back pain, neurogenic claudication, or radicular pain, which has a significant impact on their daily lives.3
The facet joints (FJ), as the only synovial joints of the spine, have received initial attention for the association between structural abnormalities and degenerative lumbar spondylolisthesis. During the disease, lumbar intervertebral space stenosis can lead to an increase in the load on small joints, causing changes in the morphology of the FT and articular surfaces. At the same time, it is accompanied by weakened muscle stabilization function, further exacerbating lumbar segmental instability and forming a vicious cycle of disease progression.4,5 In recent years, studies have found through imaging analysis that there is a correlation between the sagittal orientation of articular processes and lumbar spondylolisthesis, but the conclusion is still controversial. Most previous studies focused on the overall lumbar spine or L5/S1 segment, with relatively few specialized studies on anterior spondylolisthesis of the L4-5 segment.6,7 In addition, studies have shown8,9 that during the process of FJ degeneration, osteophyte formation may alter the mechanical distribution of the joint, leading to local stress concentration. Subchondral sclerosis reflects the degeneration of articular cartilage and reduces the joint’s buffering capacity. Narrowing of the joint space can limit the range of joint movement, further disrupting the stability of the lumbar spine. These degenerative changes are believed to be related to the progression of spondylolisthesis to some extent. However, there is still a lack of systematic exploration on the relationship between the degeneration degree of FJ and the progression of spondylolisthesis. It is particularly unclear whether it indirectly promotes spondylolisthesis by altering the local biomechanical environment (such as increasing the pre-spondylolisthesis torque). In clinical practice, the choice of treatment plan (conservative treatment or surgical intervention) for DS at L4-5 is highly dependent on imaging evaluation. However, the existing evaluation system mostly focuses on factors such as vertebral arch isthmus and intervertebral disc degeneration, and lacks comprehensive consideration of the direction and degeneration degree of FJ.10,11
In this study, the patients with DS at the L4-5 segment were included to explore the correlation between sagittalization, levelization, and the degenerative degree of FJ with DS at the L4-5 segment, aiming to provide a theoretical reference for the diagnosis and treatment of DS at the L4-5 segment.
Materials and Methods
Clinical Materials
Total of 114 cases of DS patients at L4-5 admitted in our hospital during May 2019 to April 2024 were retrospectively selected as the research objects as shown in Figure 1. Among them, there were 44 males and 70 females with an average age of (60.75 ± 8.10) years and an average body mass index (BMI) of (25.38 ± 2.90) kg/m2, including 59 cases of physical labor and 55 cases of non-physical labor occupations. Inclusion criteria: (1) All patients met the diagnostic guidelines for DS12 and were diagnosed with L4-5 segment vertebral spondylolisthesis through imaging. (2) The patient had been experiencing lower back pain for no less than 2 months. (3) The patient had complete clinical case data. (4) The patient had not undergone lumbar spine surgery in the past. Exclusion criteria: (1) Patients with lumbar spine deformities caused by congenital or acquired factors such as trauma or osteoporosis; (2) Patients with combined lumbar infection or lumbar tumors; (3) Patients with autoimmune diseases, such as infectious diseases or rheumatoid arthritis; (4) Patients with combined organic lesions of important organs. Besides, 114 cases of non-DS patients admitted to our hospital during the same period were chosen as the non-DS group. Among them, there were 41 males and 73 females with an average age of (61.46±9.36) years and an average BMI of (26.63±3.71) kg/m2, including 71 cases of physical labor and 43 cases of non-physical labor occupations. There was no significant difference in general data between the two groups (P>0.05).
 |
Figure 1 Patient Inclusion Process Diagram. |
Facet Joint Angle (FJA), L4 Inclination Angle (L4IA), and Pedicle-Facet Angle (P-F Angle)
FJA:13 The 64-slice spiral CT equipment was employed to scan the patient’s lumbar spine, with a scan layer thickness set at 1mm. After the scanning was completed, the image data were transmitted to Mimics medical imaging analysis software. In the software, the line connecting the two endpoints of FJ and the angle between the sagittal line (the perpendicular line passing through the center of the spinal canal and the line connecting the two lateral tangents of the vertebral body) were marked on the CT cross section, with the sagittal direction and the cross section parallel to the L4-5 intervertebral space as the head and tail sides, respectively. To ensure the accuracy of the measurement, the left and right FJ were measured by two experienced radiologists separately. If the difference between the two measurement results was greater than 5%, it should be re-measured. Finally, the average of the measurements by two radiologists was taken as the value for one side, and then the average of the left and right sides was taken as FJA.
L4IA:14 It was measured through lumbar X-ray anteroposterior and lateral radiographs. The patient was in a standard standing position, with the lumbar spine maintaining a natural physiological curvature. Image analysis software (the measurement tool included in the PACS system) was adopted, and the L4 vertebral endplate on the lateral radiograph was measured. A straight line was drawn along the vertebral endplate, and then the angle between the line and the horizontal plane was measured using software, which was the L4IA.
P-F angle:15 Image data obtained was scanned using 64-slice spiral CT. In Mimics software, the left and right lateral edge pedicle axis of the L4 spinal canal and the L4-5 facet joint gap were taken as the measurement objects. The angles between the left and right pedicle axes and the joint space of the facet joint were measured three times for each angle, and the average value was taken. Finally, the average values of the left and right sides were averaged again to obtain the P-F angle.
The asymmetry of FJA was the absolute value of the difference in FJA between the head and tail sides, which was used to measure the degree of difference in the angle of the FJ between the head and tail sides. The larger the value was, the more significant the angle changes of the facet joints in the head-tail direction were, which might affect the stability of the spinal segments.
The asymmetry of the P-F angle was the absolute value of the difference between the pedicle and FJA on both sides, reflecting the asymmetry of the connection angle between the left and right pedicle and FJ. The changes in P-F angle indicated an unbalanced state of stress on both sides of the lumbar spine, which was of great significance for evaluating the stability of the lumbar spine.
Cross sectional area (CSA) of paraspinal muscles: A 1.5T MRI device with a layer thickness of 3–5mm was adopted, and T1 weighted or T2 weighted imaging sequences were cooperated to locate the L4-5 segments. The scanning program was started to obtain cross-sectional images of the paraspinal muscles in the L4-5 segments. The paraspinal muscles (multifidus, erector spinae) was outlined in the software, and the CSA was calculated by the software automatically.
Slippage index: The patient maintained a standard standing or supine position and used X-ray equipment to take lateral images of the lumbar spine, keeping the centerline of the X-ray accurately aligned with the L4-5 segment. The PACS system was equipped with measurement tools. The posterior edge of the L5 vertebral body was taken as a reference to measure the vertical distance between the posterior lower edge of the L4 vertebral body and the posterior edge of the L5 vertebral body in the sagittal plane. This distance was the anterior displacement distance of the superior vertebral body (L4). The anterior posterior diameter of the L5 vertebral body was measured, which was the maximum distance from the anterior edge to the posterior edge of the L5 vertebral body. The value obtained by dividing the measured distance of anterior displacement of the superior vertebral body by the anterior-posterior diameter of the inferior vertebral body was the slippage index.
Degeneration Degree of FJ
According to the Weishaupt grading criteria,16 the degree of joint degeneration in patients was determined by observing CT images. The degeneration was divided into grade 0 (small joint space 2–4mm), grade I (small joint space less than 2mm, or/and small osteophyte or/and mild joint hyperplasia), grade II (small joint space less than 1mm, or/and moderate osteophyte or/and moderate joint hyperplasia or/and mild joint surface bone erosion), and grade III (small joint space less than 1mm, or/and large osteophyte or/and severe joint hyperplasia or/and moderate to severe joint surface bone erosion or/and subchondral cyst). In the judgment process, a senior radiologist made the initial judgment, followed by another spinal surgeon for review. If the two judgments were inconsistent, they would jointly discuss and determine the final grading.
Outcome Measures
The FJA at L4-5, FJA difference, FJA asymmetry, L4IA, Weishaupt classification, paraspinal muscle CSA, P-F angle, and P-F angle asymmetry were compared between the DS group and the non-DS group.
The changes of FJA and slippage index (Lateral displacement distance of upper vertebral body/anterior-posterior diameter of lower vertebral body in X-ray examination) in patients with different Weishaupt grades were compared. The correlation between Weishaupt grades with FJA and the slippage index was analyzed by Pearson correlation.
ROC was used to analyze the predictive value of sagittal and horizontal indexes of facet joint direction for DS at L4-5.
Statistical Analysis
Statistical analysis was conducted using SPSS 24.0. The measurement data that conformed to the normal distribution were represented by ( ± s). Independent sample t-test was employed for comparison between two groups, a single-factor multiple-sample mean comparison was adopted for comparison among multiple groups, and LSD-t test was further performed for pairwise comparison. The enumeration data were represented as [cases (%)], and the comparison between groups was conducted using the χ2 test. Rank sum test was used for comparison of grade data. Predict value was valued through ROC curve analysis. P<0.05 was considered as statistically significant.
± s). Independent sample t-test was employed for comparison between two groups, a single-factor multiple-sample mean comparison was adopted for comparison among multiple groups, and LSD-t test was further performed for pairwise comparison. The enumeration data were represented as [cases (%)], and the comparison between groups was conducted using the χ2 test. Rank sum test was used for comparison of grade data. Predict value was valued through ROC curve analysis. P<0.05 was considered as statistically significant.
Results
Comparison of FJA, FJA Difference and Asymmetry Between Two Groups of Patients in the L4-5 Segments
Compared with the non-DS group, DS group had reduced FJA and FJA difference in L4-5 segment and increased left asymmetry (P<0.05, Table 1). The axial CT images of typical cases showed that the articular surfaces of the L4-5 facet processed in the spondylolisthesis group were closer to the sagittal position, while those in the non-spondylolisthesis group were more inclined to the coronal position, which was consistent with the quantitative measurement results (Figure 2).
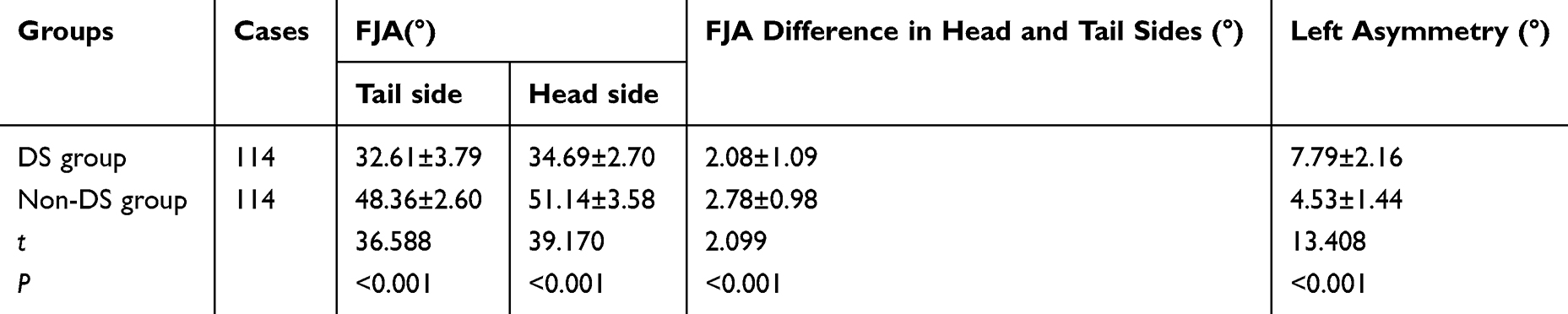 |
Table 1 Comparison of FJA, FJA Difference and Asymmetry Between Two Groups of Patients in the L4-5 Segments ( |

 |
Figure 2 Axial CT image of the facet joints of the L4-5 segment. |
Comparison of Other Parameters Between Two Groups of Patients
Compared with the non-DS group, DS group had increased level of L4IA, and largely increased proportion of gradeIIand III of Weishaupt classification (P<0.05). There was no significant difference in the CSA of the paraspinal muscles (multifidus and erector spinae) between the two groups (P>0.05, Table 2).
 |
Table 2 Comparison of Other Parameters Between Two Groups of Patients [Cases (%), ( |

Analysis of FJA and Slippage Index in Patients with Different Degrees of Degeneration
FJA gradually decreased and the slippage index gradually increased with increased degeneration degree (P<0.05). Compared with grade I patients, grade II patients showed a significant reduction in the levels of FJA on the tail and head sides, and a significant increase in the slippage index (P<0.05). Compared with grade II patients, grade III patients showed a significant reduction in the levels of FJA on the tail and head sides, and a significant increase in the slippage index (P<0.05, Table 3). Radiological comparison showed that the slip index of normal FJA (coronal predominant) patients was significantly lower than that of sagittal FJA patients, and the more severe the degree of degeneration, the more obvious the sagittal trend (Figure 3).
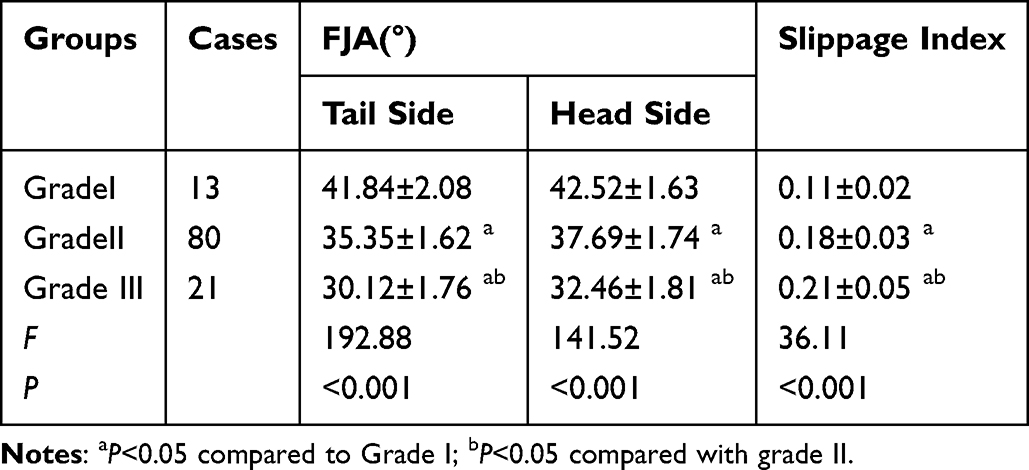 |
Table 3 Analysis of FJA and Slippage Index in Patients with Different Degrees of Degeneration ( |

 |
Figure 3 Radiological comparison of the normal Angle and sagittal Angle of FJA in the L4-5 segment. |
Correlation Analysis
Pearson correlation analysis showed that Weishaupt classification was negatively correlated with FJA (r=−0.823, P<0.001) and positively correlated with slippage index (r=0.756, P<0.001, Table 4).
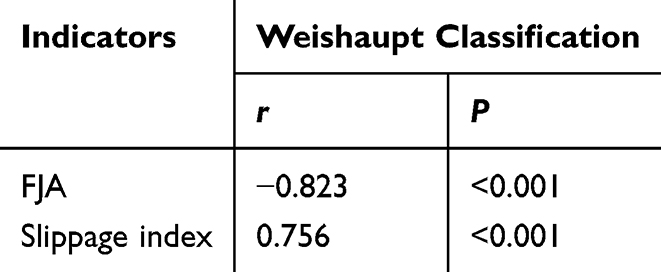 |
Table 4 Correlation Analysis |
Analysis of P-F Angle, and P-F Angle Asymmetry in Two Groups of Patients
Compared with the non-DS group, the P-F angle in the DS group was significantly increased (P<0.05). There was no significant difference in left-right asymmetry between the two groups (P>0.05, Table 5 and Figure 4). The axial MRI image of the pedicle-facet joint showed that the connection Angle between the pedicle and the facet joint in the spondylolisthesis group was significantly greater than that in the non-spondylolisthesis group, further verifying the morphological difference (Figure 5).
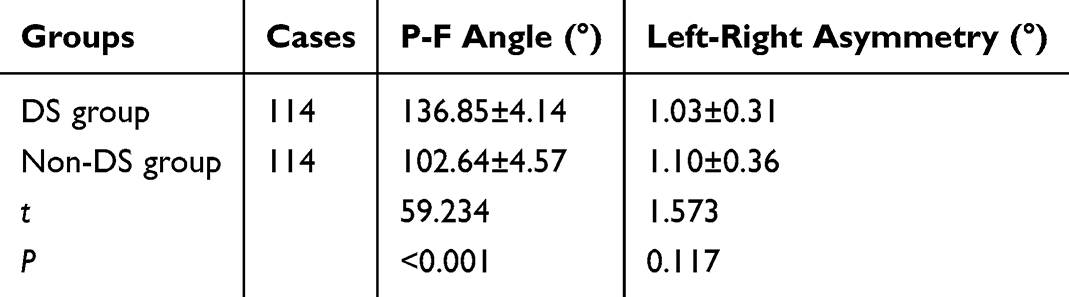 |
Table 5 Analysis of P-F Angle, and P-F Angle Asymmetry in Two Groups of Patients ( |

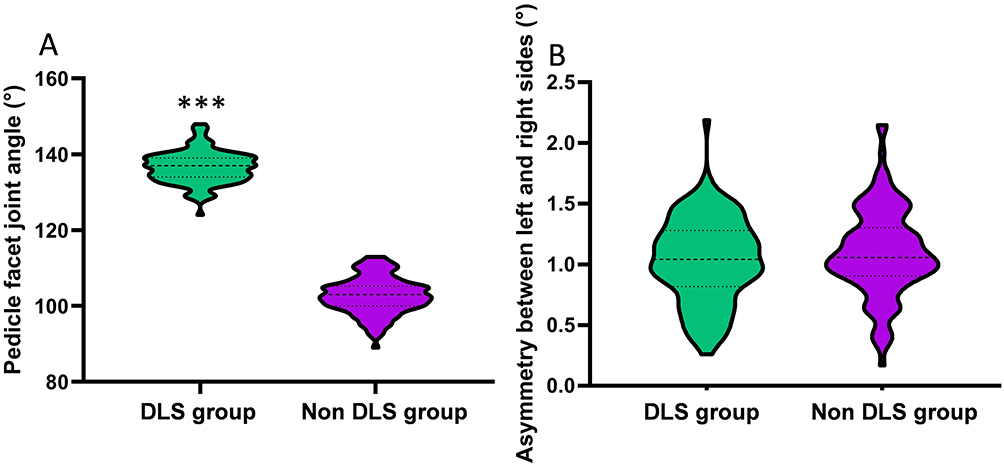 |
Figure 4 Analysis of P-F angle and P-F angle asymmetry in Two Groups of Patients. (A) Comparison of P-F angle between two groups; (B) Comparison of left-right asymmetry between two groups. Notes: Compared with the non-DS group, * * * P<0.05. |
 |
Figure 5 Axial MRI image of the pedicle - facet joint of the L4-5 segment. |
ROC Curve Analysis About the Predictive Value of FJA, L4IA and P-F Angle for DS at L4-5
ROC curve confirmed that the cut-off values of FJA, L4IA and P-F angle were 42.57, 9.63 and 122.17 respectively, and the AUC values were 0.893, 0.766 and 0.858, respectively, which had certain predictive value for DS at L4-5 (Table 6 and Figure 6).
 |
Table 6 ROC Curve Analysis About the Predictive Value of FJA, L4IA and P-F Angle for DS at L4-5 |
 |
Figure 6 ROC curve analysis about the predictive value of FJA, L4IA and P-F angle for DS at L4-5. |
Discussion
DS is a degenerative disease of the spine that is more common in people over 50 years old. DS begins with intervertebral disc degeneration, which can alter spinal biomechanics and increase the load on facet joints, leading to segmental lesions. Over time, DS may develop into symptomatic lumbar spinal stenosis or progressive malformation.17 The FJ, as key structures in the spine that maintain stability, are closely related to the occurrence and development of DS. The results of this study showed that the FJA and FJA difference between the L4-5 segments was smaller, L4IA and P-F angle was greater, and the degree of FJ degeneration was more severe in the DS group. Besides, as the degree of degeneration increased, FJA decreased and the slippage index increased. In addition, FJA, L4IA, and P-F angle had certain predictive value for DS, indicating that the sagittal transformation of the FJ surface was closely related to the degree of degeneration in patients with DS. These findings provided an important theoretical basis for the diagnosis and treatment of DS, which helped clinical doctors better understand the disease mechanism and provided a reference for developing more effective treatment plans.
In addition to age, gender, and obesity, changes in the local structure and morphology of the lumbar spine may play an important role in the complex etiology of DS.18,19 The FJs are key factors in maintaining spinal stability, and the lumbar FJs and intervertebral discs form the spinal triad complex. When the lumbar spine is subjected to a shear force generated by gravity, it tends to slide forward. The FJs of the lumbar spine are crucial for maintaining the stability of the posterior column of the spine and can resist forward shear stress.20,21 The articular surfaces of the facet joints in the non-spondylolisthesis group were mostly arranged in a coronal position (the joint space was closer to the anteroposterior direction), while in the spondylolisthesis group, they significantly tended towards the sagittal position (the joint space was closer to the anteroposterior direction). This directional difference has clear biomechanical significance: The coronal articular surface forms a mechanical barrier through the “interlocking mechanism”, effectively restricting the sagittal displacement between the vertebral bodies. Sagittal formation causes the articular surface to be parallel to the sagittal plane, significantly reducing the ability to block forward slip.22,23 Imaging and measurement data jointly confirm that the sagittal direction reduces the effective contact area between the articular surface and the intervertebral disc, weakens the resistance to forward shear force, and makes the lumbar segments more prone to forward slip.24 Under normal circumstances, the upper lumbar spine joints tend to be sagittal, allowing the lumbar spine to have better flexion and extension functions. A study suggests that the orientation of the FJ may be closely related to the development and lateralization of intervertebral disc herniation.25 FJ is a functional joint that plays an important role in maintaining the stability of spinal movement. When subjected to excessive loads, the FJ may undergo degenerative changes, affecting the stability of the lumbar spine.26 Previous studies have reported using FJA 60.19 ° as the boundary, with values below 60.19 ° considered as sagittal direction, otherwise as coronal level.27 In this study, the changes in FJA of patients with DS were analyzed, and it was found that the FJA of the DS group was significantly lower than that of the non-DS group. Besides, as the degree of degeneration increased, FJA gradually decreased, and the slippage index gradually increased. This result indicated that the FJA of patients in the DS group tended to be sagittal, while the FJA of patients in the non-DS group tended to be coronal. This might be because the contact surface between the FJA sagittal direction and the intervertebral disc becomes smaller, weakening the forward force of impedance, making the lumbar segment more prone to displacement when shear force increases, thereby increasing the risk of lumbar spondylolisthesis.28 Under normal circumstances, the coronal direction of the FJ can limit the sagittal displacement between vertebral bodies through the “locking effect”. Sagittarization leads to the joint surface being more parallel to the sagittal plane, reducing the mechanical resistance to forward slip.29 In addition, during the degeneration process, joint cartilage wear, joint capsule relaxation, and decreased ligament elasticity (such as the yellow ligament and joint capsule ligament) further exacerbate joint instability. Degenerated FJ cannot effectively distribute the axial load of intervertebral discs, resulting in stress concentration in the vertebral endplate and pedicle regions, which may accelerate endplate degeneration and pedicle morphology changes.30 The increase in the proportion of Weishaupt grades II and III indicated that the degree of joint degeneration in patients with spondylolisthesis was more severe. Degeneration not only manifests as narrowing of joint spaces and formation of osteophyte, but may also be accompanied by synovitis and decreased joint fluid, thereby reducing joint buffering capacity. These structural degeneration and biomechanical imbalances work together to form a vicious cycle, ultimately leading to anterior vertebral slippage.31 In addition, this study found that the L4IA of patients in the DS group was significantly higher than that of the non-DS group. L4IA may be related to the force acting on the L4 lumbar spine. When L4IA increases, the anterior inclination of the lumbar spine increases, the forward shear force decreases, and the vertebral body gradually slides forward, significantly increasing the risk of L4 vertebral body slippage. Forward leaning of the vertebral body increases the angle of lumbar lordosis, shifting the center of gravity forward and further increasing the shear force of L4 vertebral body forward sliding.32
P-F angle is the angle between the midpoint line of the anterior and posterior edges of the vertebral body and the joint gap of the facet joint. The increase in P-F angle may reflect adaptive changes in pedicle morphology. During the process of degeneration, the pedicle may undergo remodeling due to long-term abnormal stress, such as a decrease in bone density or a change in the orientation of bone trabeculae, increasing the connection angle between the pedicle and the FJ. This morphological change may weaken the anchoring effect of the pedicle on the facet joints and reduce the stability between the vertebral bodies.33 Research has found that P-F angle may play an important role in maintaining lumbar stability P-F angle.34 According to reports, DS patients have significantly increased P-F angle, and logistic analysis shows that P-F angle is a risk factor for the occurrence of DS,35 which is similar to the result of our present study. It may be because as the P-F angle increases, the FJ surface tends to level. The reduction in the volume of the FJ leads to a decrease in resistance to pre-shear forces, resulting in a significant decrease in the stability of the lumbar spine. This study confirmed through a large-sample case-control analysis that patients with degenerative anterior spondylolisthesis of lumbar vertebrae 4–5 have significant morphological abnormalities and aggravated degeneration of the facet joints, specifically manifested as reduced FJA (sagittal) in the L4-5 segment and increased pedicle-FJA (horizontal). Guo et al conducted a specialized analysis of the L4-L5 segments and found that a reduction in FJA is an independent risk factor for degenerative slippage, and the shear force risk significantly increases when FJA is less than 60°.27 The case-control study by Kong et al also confirmed that the increase in the pedicle-FJA is closely related to the biomechanical imbalance of the lumbar vertebrae segments, which is highly consistent with the result in this study that the Angle in the spondylolisthesis group (136.85±4.14°) was significantly greater than that in the non-spondylolisthesis group (102.64±4.57°).36 However, this study systematically focused on the L4-5 segment with a high incidence of degenerative slippage for the first time, excluded the interference of adjacent segments in multi-segment studies, and clarified the specific association pattern of “sagittal-horizontal-degeneration” for this segment. The morphological indicators (FJA, vertebral arch-FJA) and degeneration grading (Weishaupt) were analyzed collaboratively, confirming the vicious cycle mechanism of “morphological abnormalities accelerating degeneration and degeneration aggravating morphological abnormalities”, while previous studies mostly analyzed morphology or a single dimension of degeneration alone.37–39 The findings of this study not only verified the core conclusions of previous research, but also achieved supplementation and expansion in terms of segmental specificity, mechanism depth, and clinical practicality.
In addition, ROC curve analysis in this study found that the AUC of FJA, L4IA, and P-F angle were 0.893, 0.766, and 0.858, respectively. It was believed that FJA, L4IA, and P-F angle had certain predictive value for DS at the L4-5 vertebrae. The normal lumbar FJs are arranged in a coronal position, forming a “locking mechanism” that can effectively resist sagittal displacement between vertebral bodies. When FJA<42.57 °, the articular surface tends towards the sagittal plane, resulting in a decrease in its obstruction area in the horizontal plane and a significant reduction in the resistance to anterior vertebral slip.40 Meanwhile, the wear of articular cartilage, relaxation of joint capsule, and reduction of synovial fluid during the degeneration process further exacerbate joint instability. In addition, the increase in FJA asymmetry may lead to stress concentration in unilateral joints, causing local subchondral bone sclerosis or cystic degeneration, further disrupting the symmetry stability of the motion segment. L4IA enlargement (>9.63 °) reflects a tendency towards forward vertebral body tilt, which is closely related to spinal pelvic sagittal balance compensation.41 When the lumbar lordosis increases, the forward shift of the center of gravity puts greater forward shear force on the L4 vertebral body. An increase in the P-F angle (>122.17 °) indicates adaptive remodeling of the pedicle morphology. Long-term abnormal stress can lead to changes in the orientation of pedicle bone trabeculae, decreased bone density, and weakened ability to anchor articular processes.42 The ROC curve analysis showed that FJA had the highest predictive performance (AUC=0.829), as it directly reflected the mechanical properties of the articular process. The AUC of L4IA and P-F angle were relatively low (0.683 and 0.733), which might be related to their susceptibility to multiple factors such as individual pelvic parameter differences and muscle compensation.
The clinical value of this study is mainly reflected in three aspects: ① Segmental specific focus: For the first time, it systematically confirmed the independent association between sagittal facet joint (reduced FJA) and horizontal facet joint (increased pedicle-facet joint Angle) of the L4-5 segment and anterior spondylolidosis, making up for the deficiency of insufficient attention paid to this high-incidence segment in previous multi-segment studies. Compared with the association between lumbar intervertebral disc protrusion and muscle morphology that Guvercin et al43 focused on, this study reveals the core role of bony structural changes in the facet joints in DS, providing a new perspective for the study of the “structural-function” association. ② Clinical evaluation optimization Clarifying the predictive thresholds of FJA (Cut-off value 42.57°), L4IA (9.63°), and pedicle-FJA (122.17°) can be incorporated into the preoperative imaging evaluation system to help clinicians more accurately determine the risk of spondylolisch (such as taking stable intervention in advance for patients with FJA<42.57°). ③ Deepening mechanism explanation: It has been confirmed that the synergy between facet joint degeneration (Weishaupt classification) and morphological changes, that is, degeneration reduces joint stability by intensifying sagittal/horizontal degeneration, while morphological abnormalities accelerate degeneration. The revelation of this vicious cycle provides a theoretical basis for targeted intervention (such as facet joint arthroplasty).
In general, the DS group had smaller FJA and FJA difference, larger L4IA and P-F angle at L4-5 segment, and a more serious degree of FJ degeneration. At the same time, FJA, L4IA and P-F angle had certain predictive value for DS at L4-5, indicating that DS at L4-5 was closely related to the sagittalization, levelization and degeneration degree of facet joint. However, this study still had certain limitations. This study was a single-center retrospective study with a small sample size. Only the relationship between the direction of the articular process and the degree of degeneration was analyzed, and the possible influence of age on the sagittal orientation of the articular process was not analyzed. Further research could be conducted to verify our present conclusion in the future.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by The Ethics Committee of Nanchang Hongdu Hospital of TCM. Written informed consent was obtained from the study participants and the participation in the study and all methods were carried out in accordance with relevant guidelines and regulations. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to Participate
The patients participating in the study all agree to publish the research results. Written informed consent to participate was obtained from all of the participants in the study.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. He Y, Wang W, Zhou H. et al. Imaging analysis and predictive nomogram construction for degenerative lumbar spondylolisthesis with severe clinical symptom based on propensity score matching. Sci Rep. 2023;13(1):4161. doi:10.1038/s41598-023-31224-4
2. Liu Z, Dai G, Cao Y, et al. Analysis of Degenerative and Isthmic Lumbar Spondylolisthesis from the Difference of Pelvic Parameters and the Degree of Degeneration through Imaging Data. J Pers Med. 2023;13(9):1420. doi:10.3390/jpm13091420
3. Wang DF, Chen XL, Han D, et al. The effect of sagittal alignment, coronal balance, and segmental stability on preoperative patient-reported outcomes in patients with degenerative lumbar spondylolisthesis. BMC Surg. 2023;23(1):48. doi:10.1186/s12893-023-01947-2
4. Ye X, Li J, Shangguan Z, Wang Z, Chen G, Liu W. Are the facet joint parameters risk factors for cage subsidence after TLIF in patients with lumbar degenerative spondylolisthesis? Eur Spine J. 2024;33(9):3523–3533. doi:10.1007/s00586-024-08393-5
5. Lee CY, Lee SH. Response to: clinical Implication of Mid-Range Dynamic Instability in Lumbar Degenerative Spondylolisthesis. Asian Spine J. 2020;14(5):766–767. doi:10.31616/asj.2020.0412.r2
6. Kitanaka S, Takatori R, Arai Y, et al. Facet Joint Osteoarthritis Affects Spinal Segmental Motion in Degenerative Spondylolisthesis. Clin Spine Surg. 2018;31(8):E386–E390. doi:10.1097/BSD.0000000000000674
7. Wang PT, Zhang JN, Liu TJ, Yang JS, Hao DJ. Comparison of degenerative lumbar spondylolisthesis and isthmic lumbar spondylolisthesis: effect of pedicle screw placement on proximal facet invasion in surgical treatment. BMC Musculoskelet Disord. 2022;23(1):6. doi:10.1186/s12891-021-04962-7
8. Nakasa T, Ikuta Y, Kawabata S, Sakurai S, Moriwaki D, Adachi N. Development of osteophytes and joint space narrowing is associated with cartilage degeneration of the osteochondral fragment in the osteochondral lesion of the talus. J Orthop Sci. 2024;29(5):1242–1247. doi:10.1016/j.jos.2023.08.013
9. Gregson CL, Hardcastle SA, Murphy A, et al. High Bone Mass is associated with bone-forming features of osteoarthritis in non-weight bearing joints independent of body mass index. Bone. 2017;97:306–313. doi:10.1016/j.bone.2017.01.005
10. Schönnagel L, Caffard T, Zhu J, et al. Decision-making Algorithm for the Surgical Treatment of Degenerative Lumbar Spondylolisthesis of L4/L5. Spine. 2024;49(4):261–268. doi:10.1097/BRS.0000000000004748
11. Kuraishi S, Takahashi J, Mukaiyama K, et al. Comparison of Clinical and Radiological Results of Posterolateral Fusion and Posterior Lumbar Interbody Fusion in the Treatment of L4 Degenerative Lumbar Spondylolisthesis. Asian Spine J. 2016;10(1):143–152. doi:10.4184/asj.2016.10.1.143
12. Matz PG, Meagher RJ, Lamer T, et al. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2016;16(3):439–448. doi:10.1016/j.spinee.2015.11.055
13. Li K, Zhang Z, Ran J, Ma L, Meng X. Unilateral Endoscopic and Unilateral Biportal Endoscopic surgery for lumbar spinal stenosis: a systematic review and meta-analysis. Front Surg. 2025;12:1585783. doi:10.3389/fsurg.2025.1585783
14. Baymurat AC, Tokgöz MA, Abdulaliyev F, Tosun MF, Can MM, Şenköylü A. Which lumbar vertebra should be the lowest level of fusion in adolescent idiopathic scoliosis of Lenke types 5 and 6? Acta Orthop Traumatol Turc. 2024;58(2):116–123. doi:10.5152/j.aott.2024.23204
15. Priya A, Narayan RK, Ghosh SK, Sarangi PK. Analysing lumbar pedicle morphometry observed via traditional and recent modalities. J Orthop. 2023;43:17–24. doi:10.1016/j.jor.2023.07.022
16. Hu J, Zhang Y, Duan C, Peng X, Hu P, Lu H. Feasibility study for evaluating early lumbar facet joint degeneration using axial T1 ρ, T2, and T2* mapping in cartilage. J Magn Reson Imaging. 2017;46(2):468–475. doi:10.1002/jmri.25596
17. Rangwalla K, Filley A, El Naga A, et al. Degenerative lumbar spondylolisthesis: review of current classifications and proposal of a novel classification system. Eur Spine J. 2024;33(5):1762–1772. doi:10.1007/s00586-023-07818-x
18. Huang Y, Wang W, Zhang L, Teng Y, Zhan Z. The Relationship Between MRI Findings of Posterior Ligamentous Complex and Lumbar Instability in Degenerative Spondylolisthesis. Int J Gen Med. 2024;17:2279–2287. doi:10.2147/IJGM.S452735
19. Chen Y, Zhou Y, Chen J, et al. A systematic review and meta-analysis of risk factors for reoperation after degenerative lumbar spondylolisthesis surgery. BMC Surg. 2023;23(1):192. doi:10.1186/s12893-023-02082-8
20. Tang X, Yuan H, Huang X, et al. Endoscopic Joint Capsule and Articular Process Excision for the Treatment of Lumbar Facet Joint Syndrome: a Retrospective Study. J Pain Res. 2024;17:3187–3196. doi:10.2147/JPR.S471503
21. Touboul E, Salomon-Goëb S, Boistelle M, Sobhy Danial J, Deprez V, Goëb V. Lumbar zygapophyseal joints injections under ultrasound guidance an alternative to fluoroscopy guidance in the management of low back pain. Sci Rep. 2022;12(1):3615. doi:10.1038/s41598-022-07695-2
22. Przyklenk A, Hackl M, Iuga AI, et al. Computed tomography-based angle measurements of the sagittal capitulum and trochlea position in relation to the humeral shaft. Surg Radiol Anat. 2023;45(5):571–580. doi:10.1007/s00276-023-03118-7
23. Liu H, Li S, Zheng Z, Wang J, Wang H, Li X. Pelvic retroversion is the key protective mechanism of L4-5 degenerative spondylolisthesis. Eur Spine J. 2015;24(6):1204–1211. doi:10.1007/s00586-014-3395-7
24. Degulmadi D, Dave B, Krishnan A, Patel D. The Relationship of Facet Joint Orientation and Tropism with Lumbar Disc Herniation and Degenerative Spondylolisthesis in the Lower Lumbar Spine. Asian Spine J. 2019;13(1):22–28. doi:10.31616/asj.2018.0116
25. Ekşi MŞ, Özcan-ekşi EE, Orhun Ö, et al. Association between facet joint orientation/tropism and lumbar intervertebral disc degeneration. Br J Neurosurg. 2024;38(2):293–300. doi:10.1080/02688697.2020.1864289
26. Wu Y, Wu J, Qin T, et al. Cervical facet joint degeneration, facet joint angle, and paraspinal muscle degeneration are correlated with degenerative cervical spondylolisthesis at C4/5: a propensity score-matched study. Spine J. 2024;24(12):2232–2242. doi:10.1016/j.spinee.2024.07.007
27. Guo M, Kong C, Lu S, Sun X, Li X, Lu S. Predictors of L4-L5 Degenerative Lumbar Spondylolisthesis: L4 Inclination Angle and Facet Joint Angle. World Neurosurg. 2019;130:e680–e686. doi:10.1016/j.wneu.2019.06.188
28. Wang JW, Shi PZ, Zhu XD, et al. Influence of the facet joint angle on facet joint degeneration following pedicle screw fixation without fusion in thoracolumbar fractures. J Back Musculoskelet Rehabil. 2023;36(2):337–346. doi:10.3233/BMR-210235
29. Kim DH, Kim BS, Kim JH, Cho CH. Outcomes and complications after treatment for anteromedial facet fracture of the coronoid process: a systematic review. J Orthop Sci. 2024;29(6):1489–1495. doi:10.1016/j.jos.2023.11.002
30. Wang L, Huang FS, Sun CH, Yin J, Zhang Q. Finite element analysis of bending and standing manipulation in the treatment of lumbosacral joint disorder. Zhongguo Gu Shang. 2019;32(6):519–523. doi:10.3969/j.issn.1003-0034.2019.06.007
31. Daher M, Rezk A, Baroudi M, et al. Lumbar Spondylolisthesis Grading: current Standards and Important Factors to Consider for Management. World Neurosurg. 2024;190:311–317. doi:10.1016/j.wneu.2024.07.194
32. Zhang X, Zhang Y, Gu Z, Li G. Comparison of midline lumbar interbody fusion and minimally invasive transforaminal lumbar interbody fusion for treatment of lumbar degeneration disease. Sci Rep. 2024;14(1):22154. doi:10.1038/s41598-024-73213-1
33. Meng H, Gao Y, Lu P, et al. Risk factor analysis of disc and facet joint degeneration after intersegmental pedicle screw fixation for lumbar spondylolysis. J Orthop Surg Res. 2022;17(1):247. doi:10.1186/s13018-022-03082-9
34. Xu Y, Le X, Zhang Q, et al. Superior-segment Bilateral Facet Violation in Lumbar Transpedicular Fixation, Part I: a Biomechanical Study of Blocking Superior Facets. Spine. 2020;45(11):E624–E630. doi:10.1097/BRS.0000000000003380
35. Zhou Q, Zhang JX, Zheng YF, et al. Effects of different pedicle screw insertion depths on sagittal balance of lumbar degenerative spondylolisthesis, a retrospective comparative study. BMC Musculoskelet Disord. 2021;22(1):850. doi:10.1186/s12891-021-04736-1
36. Kong Q, Wei B, Niu S, Liao J, Zu Y, Shan T. Age, pelvic incidence, facet joint angle and pedicle-facet angle as correlative factors for isthmic spondylolisthesis: a retrospective case control study. BMC Musculoskelet Disord. 2023;24(1):497. doi:10.1186/s12891-023-06569-6
37. Zhang Z, Zou J, Lu P, et al. Analysis of lumbar spine loading during walking in patients with chronic low back pain and healthy controls: an OpenSim-Based study. Front Bioeng Biotechnol. 2024;12:1377767. doi:10.3389/fbioe.2024.1377767
38. Liu X, Huang Z, Zhou R, et al. The Effects of Orientation of Lumbar Facet Joints on the Facet Joint Contact Forces: an In Vitro Biomechanical Study. Spine. 2018;43(4):E216–E220. doi:10.1097/BRS.0000000000002290
39. Chung SB, Lee S, Kim H, Sh L, Kim ES, Eoh W. Significance of interfacet distance, facet joint orientation, and lumbar lordosis in spondylolysis. Clin Anat. 2012;25(3):391–397. doi:10.1002/ca.21222
40. Capozzi A, Truglia S, Buttari B, et al. Carbamylation of β2-glycoprotein I generates new autoantigens for antiphospholipid syndrome: a new tool for diagnosis of ‘seronegative’ patients. Rheumatology (Oxford). 2022;61(10):4187–4197. doi:10.1093/rheumatology/keac045
41. Cacciola G, Anastasi G, Bertino S, et al. Anatomical differences in the bony structure of L5 and L4: a possible classification according to the lateral tilt of the pedicles. J Orthop. 2018;15(1):205–209. doi:10.1016/j.jor.2018.01.024
42. Matsukawa K, Yato Y, Hynes RA, et al. Comparison of Pedicle Screw Fixation Strength Among Different Transpedicular Trajectories: a Finite Element Study. Clin Spine Surg. 2017;30(7):301–307. doi:10.1097/BSD.0000000000000258
43. Guvercin Y, Kanat A, Gundogdu H, Abdioglu AA, Guvercin AR, Balik MS. How does the side of lumbar disc herniation influence the psoas muscle size at the L4-5 level in patients operated for unilateral Hip arthroplasty? Int J Neurosci. 2024;134(5):468–473. doi:10.1080/00207454.2022.2115907
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.