")
Back to Journals » Psychology Research and Behavior Management » Volume 17
The Heterogeneity of Symptom Burden and Fear of Progression Among Kidney Transplant Recipients: A Latent Class Analysis
Authors Zhang Y , Liu S , Miao Q, Zhang X, Wei H, Feng S, Li X
Received 13 December 2023
Accepted for publication 29 February 2024
Published 18 March 2024 Volume 2024:17 Pages 1205—1219
DOI https://doi.org/10.2147/PRBM.S454787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Ying Zhang,* Sainan Liu,* Qi Miao, Xu Zhang, He Wei, Shuang Feng, Xiaofei Li
The First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaofei Li, Transplantation and Hepatobiliary Department, The First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China, Tel +15940564748, Email [email protected]
Purpose: Kidney transplant recipients (KTRs) may experience symptoms that increase their fear of progression (FoP), but a dearth of research examines the issue from a patient-centered perspective. Our study aimed to first determine the category of symptom burden, then to explore the differences in characteristics of patients in different subgroups, and finally to analyze the impact of symptom subgroup on FoP.
Patients and Methods: Sociodemographic and Clinical Characteristics, Symptom Experience Scale, and Fear of Progression Questionnaire-Short Form were used. Latent class analysis was used to group KTRs according to the occurrence of symptoms. We used multivariate logistic regression to analyze the predictors of different subgroups. The differences in FoP among symptom burden subgroups were analyzed by hierarchical multiple regression.
Results: Three subgroups were identified, designated all-high (20.5%), moderate (39.9%), and all-low (39.6%) according to their symptom occurrence. Multivariate logistic regression showed that gender, post-transplant time, per capita monthly income, and hyperuricemia were the factors that distinguished and predicted the all-high subgroup (P < 0.05). Hierarchical multiple regression showed that symptom burden had a significant effect on FoP (class1 vs class3: β = 0.327, P < 0.001; class2 vs class3: β = 0.104, P = 0.046), explaining the 8.0% variance of FoP (ΔR2 = 0.080).
Conclusion: KTRs generally experience moderate or low symptom burden, and symptom burden is an influencing factor in FoP. Identifying the traits of KTRs with high symptom burden can help clinicians develop targeted management strategies and ease FoP of KTRs.
Keywords: kidney transplant, symptom burden, fear of progression, latent class analysis
Introduction
Kidney transplantation (KT) can effectively improve the survival rate and quality of life of patients with end-stage renal disease (ESRD), which is an important way for ESRD patients to return to normal life.1 China firmly secured its position as the world’s second-largest country for transplants by successfully performing a staggering 12,721 KTs in 2022, according to the China Scientific Registry of Kidney Transplantation (CSRKT).
KTs can effectively improve ESRD symptoms.2 However, because of the side effects of immunosuppressive therapy and chronic rejection, kidney transplant recipients (KTRs) still experience a high symptom burden,3 where the incidence of symptoms is as high as 79%.4,5 In addition, related procedures during KT can lead to symptoms in the recipient. Studies have shown a high rate of ureteral stent colonization in KTRs, which in turn increases the risk of urinary tract infections.6 Symptoms can directly or indirectly affect the health of KTRs. Studies have shown that symptoms after KT reduce quality of life,3,7,8 affect medication compliance,4 reduce the positive evaluation of one’s health status, resulting in greater psychological pressure,9 and can even change the outcome of transplantation.7,10 Therefore, assessing the symptom experience of KTRs is of utmost importance to KTRs and health care professionals (HCPs) to understand disease status, disease development, and disease outcome.11
The National Institute of Nursing Research (NINR) carried out a seminar on “Advancing Symptom Science Through Symptom Cluster Research” in 2015, which determined the strategy of symptom management centered on symptom clusters and clarified that symptom cluster management is the focus of future research.12 Moreover, understanding symptom clusters and their internal relationships is helpful for future symptom management.13 However, most of the current studies on symptom clusters focus on variables and carry out status research,14 correlation research,15 and longitudinal research.16 This symptom clustering method quantifies symptoms and evaluates the overall symptom experience of patients but ignores the heterogeneity of individual symptom experience of patients, thus limiting the implementation of individual-centered symptom management.17 It is worth mentioning that expert consensus points out that future research on symptoms should focus on the symptom experience of individual patients, and that the heterogeneity of symptom experience may be the key point of symptom management.12 Current studies have shown that individual-centered clustering methods mainly focus on tumors,18 cardiovascular diseases,19 and chronic kidney diseases,20 so more research of this type is needed in KT.
For KTRs, the fear of potential graft rejection, infection, and cancer is one of the major sources of psychological stress.21 Patients often experience uncertainty about the progression of their disease when they begin to exhibit symptoms. This uncertainty can lead to a fear of disease progression and recurrence.22 Fear of progression (FoP) refers to the individual’s fear of existing diseases, including the physical, social, and psychological consequences of fear of disease progression or recurrence, which is different from traditional psychological dysfunction.23 FoP can reduce the quality of life of patients,24 reduce the confidence of patients in self-care,25 and promote patients to adopt negative coping styles.22 A high FoP score indicates that patients do not receive sufficient supportive care needs.26 In addition, patients with FoP reaching the clinical level are more likely to be diagnosed with mental illness.27 It is undeniable that FoP is persistent, and long-term FoP will hurt patients.28 According to the theory of unpleasant symptoms (TOUS),29 there is a two-way feedback path between psychological factors and symptoms; that is, symptoms can affect FoP. Studies have shown that psychological symptoms are predictors of FoP.30 Symptom experience has been positively correlated with FoP.25,31 At present, there is insufficient evidence on the impact of symptom burden of KTRs on FoP, and this study aimed at filling this gap.
We investigated the symptom burden of KTRs from a novel perspective. Latent class analysis (LCA) is a research method that uses human-centered variables to categorize patients by the similarity of a certain feature, attempting to explain the individual latent feature classification by the fewest number of target categories.32 In contrast to traditional clustering methods, LCA is a more flexible probabilistic-based method.33 As a result, LCA has emerged as an effective method to evaluate the diversity in patients’ symptom experiences.34 This study aimed to use LCA to identify different subgroups of symptom burden in KTRs, explore potential predictors of these subgroups, and examine differences in FoP among the subgroups.
Materials and Methods
Design and Participants
The convenience sampling method was used to select allogeneic KTRs according to the inclusion and exclusion criteria at two tertiary hospitals in Liaoning and Jilin provinces in China. Included in this study were KTRs with age ≥18 years old, first KT, and postoperative time ≥3 months who consented to participate. KTRs with also two or more organ transplants, a history of cognitive dysfunction or psychosis, severe physical dysfunction, or malignant tumors requiring simultaneous treatment were excluded. Nylund-Gibson35 suggests that the sample size for LCA should be at least 300 cases. There were 381 valid questionnaires in this study.
Data Collection Procedure
Between October and December 2022, we collected data through both online and offline questionnaires. Before distribution, we obtained consent from all participants and informed them of the study’s purpose, how to complete the questionnaire, and the confidentiality measures in place. We distributed a total of 425 questionnaires, including 100 offline and 325 online. After filtering out illogical and regular answers, as well as samples that were completed too quickly, we successfully collected 381 samples, resulting in an effective recovery rate of 90%.
Research Tools
Sociodemographic and Clinical Characteristics
Sociodemographic information included age, gender, body mass index (BMI), educational level, marital status, residence, mode of living, primary caregivers, employment status, medical payment method, and per capita monthly income. The clinical characteristics included post-transplant time, dialysis type, dialysis time, complications, and immunosuppressive agents.
Symptom Experience Scale
The scale was adapted by Du14 on the basis of Transplant Symptom Occurrence and Symptom Distress Scale-59 (MTSOSD-59R). A total of 62 items were used to assess the symptom experience of transplant patients from the three dimensions: symptom occurrence, symptom severity, and symptom distress. The Likert 5-level scoring method was used, with a minimum score of 0 and a maximum score of 4. The higher the scale’s total score, the higher the symptom burden of patients. Cronbach’s α of the three dimensions has been reported to be 0.916, 0.992, and 0.990.14 Cronbach’s α in our study was 0.928, 0.936, and 0.942.
Fear of Progression Questionnaire-Short Form
The Fear of Progression Questionnaire-Short Form (FoP-Q-SF) is a unidimensional scale that derives from the Fear of Progression Questionnaire (FoP-Q), which was adapted by Mehnert36 in 2006 to assess patients’ apprehension of disease progression or recurrence. The FoP-Q-SF comprises 12 items and employs a Likert 5-point scale, with a maximum score of 60. A higher score indicates greater severity of fear of progression, with a clinical definition level of ≥34 points. In 2015, Wu37 adapted the scale to align with Chinese culture and partitioned it into two dimensions, namely physical health and social family, with a Cronbach’s α of 0.883. This questionnaire has been used in KT.38 Cronbach’s α in our study was 0.915.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. All donated kidneys are given voluntarily with written informed consent, in accordance with the Declaration of Istanbul. Approval was granted by the Ethics Committee of the first affiliated hospital of China Medical University (number: 202373). Questionnaires were issued with the informed consent of the subjects.
Statistical Analysis
Data analysis was performed using Mplus version 8.3 and SPSS version 25.0. Continuous variables with normal distribution are denoted by mean and standard deviation (SD), non-normal data are described by median and interquartile range, and categorical variables are reported as frequency and percentage. Univariate analysis was performed using analysis of variance and chi-square test. The Bonferroni method was used for post hoc analysis, and the corrected P value (P = 0.0167) indicated statistical significance.
LCA was utilized to examine the symptom burden of KTRs. Since the average incidence of symptoms in this sample was 24.2%, symptoms with an incidence of ≥25% were included in the LCA study to ensure that the selected symptoms could represent all KTRs to the greatest extent. To prevent local maximum solutions, the random starting value was set at 200, and 10 ideal values were chosen. The Akaike information criterion (AIC), Bayesian information criterion (BIC), sample size adjusted Bayesian information criterion (aBIC), and entropy determined the optimal number of the latent class.39,40 The smaller the AIC, BIC, and aBIC values, the better the model fitting. Entropy at an omnibus index of ≥0.8 indicated good classification. Statistical differences between different subgroups were determined using the Lo-Mendell-Rubin likelihood ratio test (LMR) and bootstrap likelihood ratio test (BLRT). When LMR and BLRT showed P < 0.05, the model with k categories was considered to perform better than the model with k−1 categories. Multivariate logistic regression was used to explore the influence of sociodemographic and clinical feature data on different latent classes. Hierarchical multiple regression was used to explore the effect of latent classes on FoP.
Results
Participant Characteristics
In this study, 54.9% of the KTRs were > 45 years old and 65.6% were male, details of which are shown in Table 1.
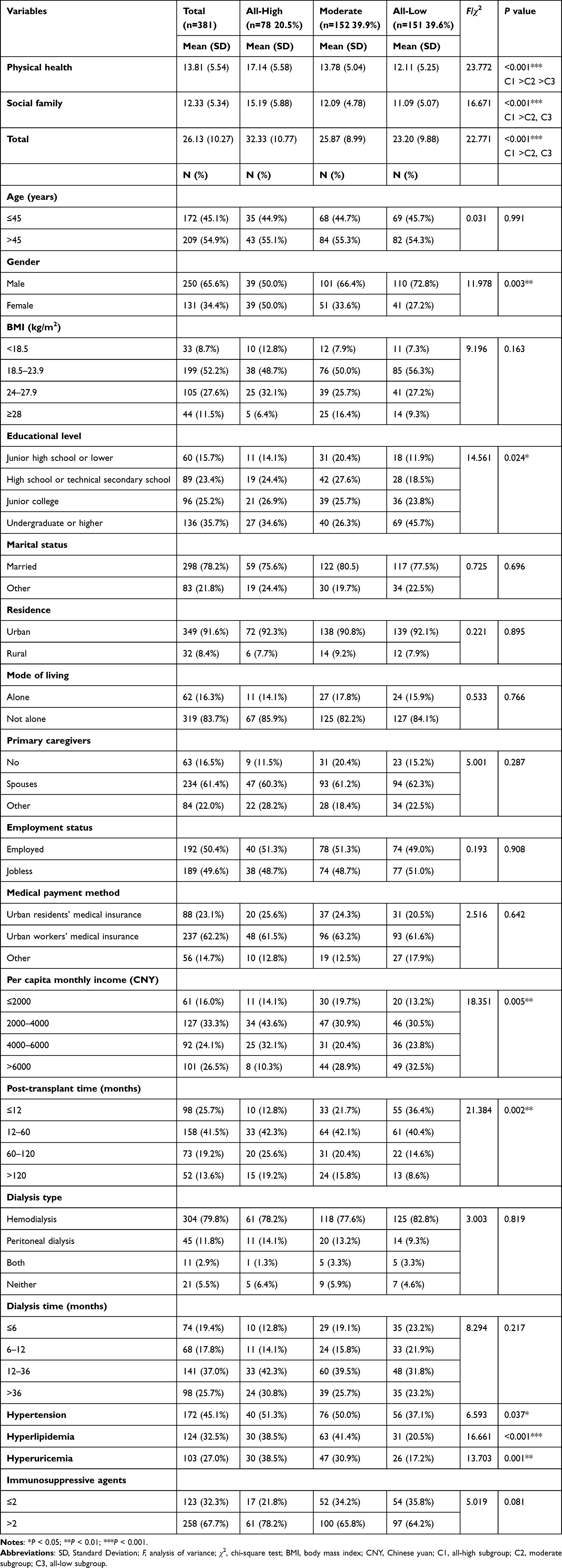 |
Table 1 Characteristics of Kidney Transplant Recipients by the Symptom Burden (n = 381) |
Results of Latent Class Analysis
A total of 29 symptoms were included in LCA, and the model fitting is shown in Table 2. The LMR of the 4–class model was not statistically significant (P > 0.05), despite having the lowest AIC and aBIC values. In the remaining models, the entropy of the 3–class model is 0.861, and the AIC, BIC, and aBIC values were relatively small. Additionally, the LMR and BLRT are significant (P < 0.05) for the 3-class model. In summary, this study suggested that the 3–class model provided the best fit. The average posterior probabilities of KTRs belonging to each latent class were 0.946, 0.920, and 0.947, respectively.
 |
Table 2 Fit Indices for the Latent Class Analysis in Kidney Transplant Recipients (n=381) |
Based on this, the category probability distribution of the three categories on each item was further obtained, as shown in Figure 1 and Table 3. In our study, we identified three distinct classes of symptoms. The first class, which accounted for 20.5% of the sample, was characterized by a high incidence of all symptoms. We named this category “all-high” and represented it with a rectangular line. The second class, which accounted for 39.9% of the sample, had a moderate incidence of symptoms. We named this category “moderate” and represented it with a square line. The third class, which accounted for 39.6% of the sample, had a low incidence of all symptoms. We named this category “all-low” and represented it with a triangle line.
 |
Table 3 The Probability for Each Symptom (n=381) |
 |
Figure 1 Category probability plot of the 3 latent classes. Probability of symptom occurrence for the total sample and each of the latent classes for the 29 symptoms on the Symptom Experience Scale that occurred in ≥25% of the total sample (n=381). Symptom groups were determined using latent class analysis (LCA). |
Differences in Sociodemographic and Clinical Characteristics Between Latent Classes
The results are given in Table 1 and showed that there were statistically significant differences in gender, educational level, per capita monthly income, post-transplant time, hypertension, hyperlipidemia, and hyperuricemia between the three latent classes (P < 0.05).
Multivariate Logistic Regression Analysis of Latent Classes
The all-low subgroup was used as the reference group. The collinearity diagnosis of the included variables showed that the tolerance was >0.1 and the VIF was <10, indicating that there was no obvious collinearity between the included variables. The likelihood ratio χ2 value of the regression model was 90.371, P < 0.001, indicating that the final model was significantly established. The results of MLR are described in Table 4.
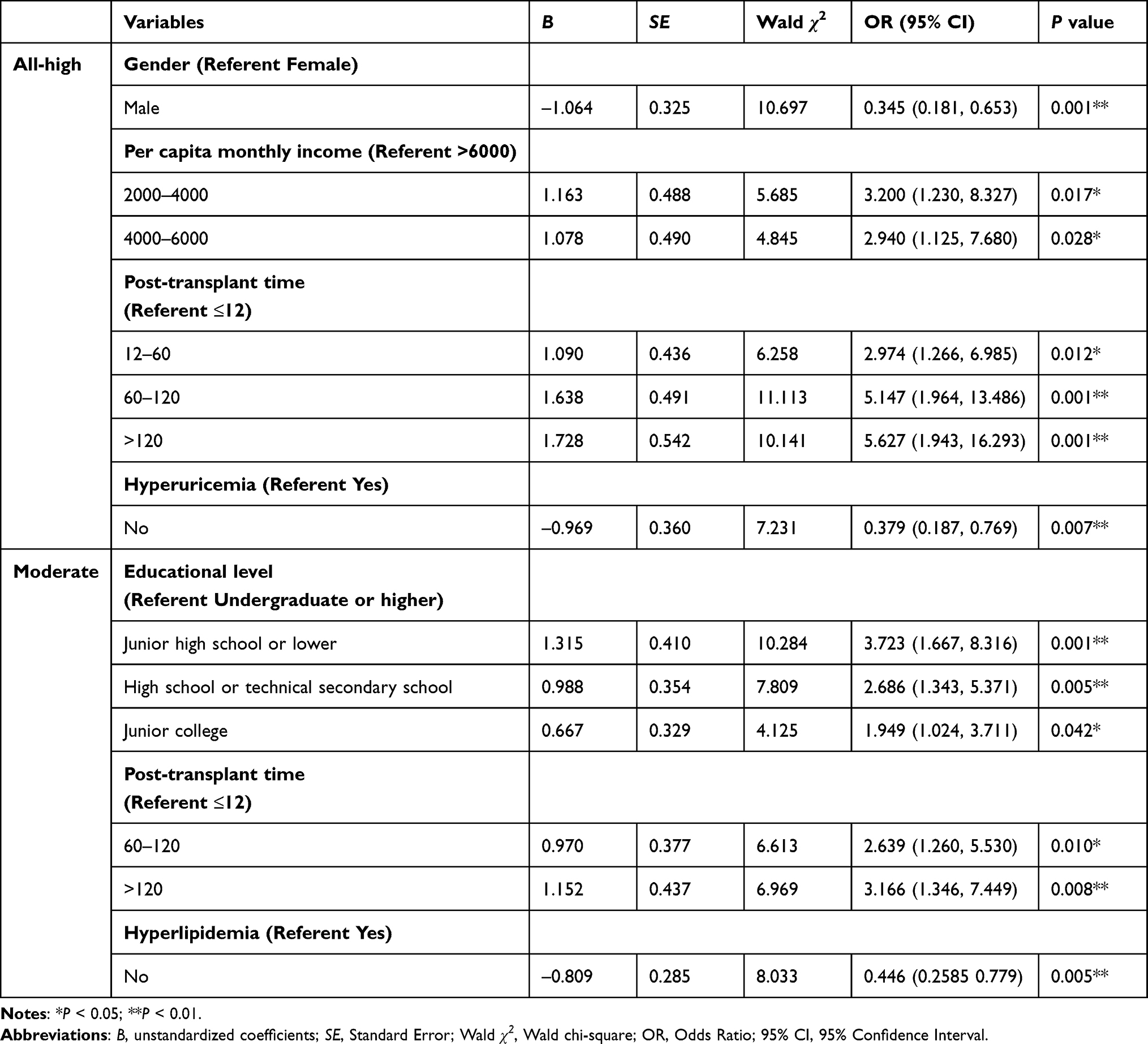 |
Table 4 Multivariate Logistic Regression Analysis of the Latent Classes (n=381) |
Compared with the all-low subgroup, gender, per capita monthly income, post-transplant time, and hyperuricemia were the predictors of the all-high group. Females, KTRs with lower per capita monthly income, longer post-transplant time, and concurrent hyperuricemia were more likely to report a high symptom burden. Additionally, education, post-transplant time, and hyperlipidemia were identified as predictors of the moderate group. KTRs with lower education, longer post-transplant time, and concurrent hyperlipidemia were more likely to report a moderate symptom burden.
Association Between Distinct Latent Classes of Symptoms with Fear of Progression
As shown in Table 1, there was a statistically significant difference in FoP between KTRs in different symptom subgroups (P < 0.05). Through post hoc analysis, we found that in the physical health dimension, all-high subgroup > moderate subgroup > all-low subgroup; in the social family dimension and total score, all-high subgroup > moderate subgroup, all-high subgroup > all-low subgroup, there was no significant difference between moderate subgroup and all-low subgroup.
To further investigate whether symptom burden predicts FoP, a hierarchical multiple regression was conducted with symptom burden as the independent variable and FoP as the dependent variable. The specific results are shown in Table 5. After adjusting for covariates (age, hyperuricemia, per capita monthly income) in model 2, different symptom burden subgroups (class1 vs class3: β = 0.327, P < 0.001; class2 vs class3: β = 0.104, P = 0.046) were significantly positively associated with FoP. The subgroups explained 8.0% of the variance in FoP (ΔR2 = 0.080, P < 0.001), and the overall model was significant (F = 12.150, P < 0.001), explaining 17.0% of the variance in FoP.
 |
Table 5 Differences in Fear of Progression Among the Latent Classes (n=381) |
Discussion
In this study, we addressed the heterogeneity of symptom burden among KTRs. We grouped patients into three categories to study demographic data and symptom burden. Our research found that gender, per capita monthly income, post-transplant time, and hyperuricemia predicted high symptom burden among KTRs. Symptom burden can also predict FoP.
The LCA conducted in this study identified three distinct latent classes among KTRs: the all-high subgroup, moderate subgroup, and all-low subgroup. Similarly, three symptom subgroups (low symptom, moderate symptom, and high symptom) were identified in hemodialysis patients.20 The proportion of the moderate subgroup was the highest (39.9%), followed by the all-low subgroup (39.6%), indicating that most KTRs generally have a moderate or lower symptom burden after surgery, consistent with previous studies.41 Interestingly, we found that the top three symptoms in the all-low subgroup were trembling hands, excessive appetite, and thinning of hair/hair loss, which were all somatic symptoms caused by immunosuppressive therapy. The top five symptoms of the all-high subgroup were concentration or memory problems, tiredness, nervousness, mood swings, and anxiety, mainly psychological symptoms, suggesting that psychological symptoms may be the main cause of high symptom burden after KT. This is a novel finding in the present study. Consistent with the results of Uyar,42 the negative emotion level of KTRs is typically higher than the medium level. Previous studies have also confirmed that anxiety and depression are common symptoms after KT.43 Cognitive and emotional factors can impact the sleep quality of KTRs, resulting in increased levels of fatigue.44 This highlights the interconnectedness of psychological and physical symptoms, where mental health can have a significant impact on physical well-being. However, there are no studies currently available for comparison with KT, it would be beneficial to conduct longitudinal studies to confirm the high incidence of symptoms in the high symptom burden group. In short, when combined with previous studies, the results consistently demonstrate that the symptoms experienced by KTRs are complex. Furthermore, current research indicates that symptoms are considered more important by KTRs than clinical indicators.45 As a result, HCPs should promptly and comprehensively assess patients’ symptoms, particularly addressing psychological symptoms effectively, to alleviate the overall symptom burden.
Analyzing the characteristics of patients with high symptom burden can help identify at-risk groups early, enabling personalized interventions. In this study, women were more likely to have a higher burden of symptoms, consistent with previous studies.46 On the one hand, women are more emotionally dependent and emotionally sensitive than men, leading to women’s tendency to express their negative emotions and more likely to have pessimistic thoughts on their health status, while negative cognitive psychological factors are positively correlated with symptom burden,47 On the other hand, there are differences in coping between women and men. Women’s psychological endurance is weak, and women are more inclined to adopt negative coping styles such as avoidance and surrender.48 In addition, sex hormones can also explain the biological differences in symptom burden.49 The findings of a longitudinal study revealed a significant improvement in sleep deprivation among male patients compared to their female counterparts 12 months after KT.44 This suggests that women may face challenges in managing their symptoms. Therefore, HCPs can support female patients in managing their symptoms and overall recovery by providing information, psychological support, career guidance, and access to support networks.
KTRs with a per capita monthly income of 2000–6000 are more likely to be in the all-high subgroup. Such results are similar to those of previous research50 that proved that poor financial burden can increase the symptom burden. Having a better financial situation will encourage KTRs to choose a better lifestyle. Moreover, it has been found that there is a link between financial difficulties and medication adherence among patients.4 Poor medication adherence can result in more severe symptoms.51 Financial strain can also affect a patient’s ability to manage their condition.52 Patients who are facing significant financial difficulties may be less likely to seek medical attention or follow through with treatment, which can ultimately lead to more severe symptoms.50 It’s worth mentioning that the study revealed some surprising results. It was found that having a per capita monthly income of less than 2,000 was not a predictor of this particular segment. It is possible that having a low income can cause more burden on caregivers.53 This may result in KTRs avoiding reporting any symptoms that they experience to prevent additional economic burden and psychological pressure on their families. However, KT is a significant financial burden for patients.54 To help patients meet this challenge, HCPs can help by offering financial counseling and support, as well as information on available resources to help alleviate financial stress. By providing these resources, HCPs can help patients manage their financial strain and improve their overall health outcomes.
Post-transplant time was associated with symptom burden, which confirmed previous studies.8 With longer post-transplant time, the side effects of immunosuppressive therapy and the symptoms caused by chronic rejection gradually appeared. In addition, KTRs with longer transplantation time have lower self-management ability,55 which can also lead to increased symptom burden. However, Veltkamp46 believes that there is no correlation between postoperative transplantation time and symptom burden. The possible explanation is that they used a combination of Dialysis Symptom Index and MTSOSD-59R tools to evaluate KTRs, including some symptoms of kidney disease that were alleviated after transplantation. That is, the relationship between post-transplant time and symptoms varies depending on the symptoms assessed. Future research should be conducted to explore and understand the relationship between these two factors.
This study is the first to identify an association between hyperuricemia and symptom burden. High uric acid can promote the development of kidney disease by inducing inflammatory response and oxidative stress,56 lead to glomerular hypertrophy and renal tubular interstitial fibrosis, hinder endothelial nitric oxide production, lead to endothelial cell dysfunction, affect graft function, and even lead to graft loss,57 which will undoubtedly increase the psychological pressure of patients. Hyperuricemia can also lead to hypertension,56,58 cardiovascular disease,58 and diabetes,59 thus aggravating the symptom burden of KTRs. Therefore, it is necessary for HCPs to closely monitor the serum uric acid level of KTRs, and timely take corresponding treatment measures according to the situation, such as adjusting diet and drug therapy,60 to improve the symptom burden and ensure the quality of life and long-term survival rate of KTRS.
The FoP score of KTRs was 26.13±10.27, of which ≥34 points accounted for 24.4%. That is, about a quarter of KTRs’ FoP reached the level of clinical diagnosis, and the results were slightly higher than those of Lin.61 The possible explanation is that 94.5% of KTRs experienced dialysis, and the return to dialysis will cause psychological stress in KTRs.21 This study explored the relationship between patient-centered symptom burden subgroups and FoP for the first time. The results showed that symptom burden was the influencing factor of FoP, which was similar to the results of previous studies.26,27 Symptom experience is the patient’s subjective perception, which indirectly reflects the patient’s view of the disease.3 When the symptom burden is heavy, KTRs will have a negative understanding of future disease progression and disease outcome, worry about daily life and their health status, and worry about becoming a family and social burden, thus triggering FoP.62 Hall63 showed that the severity of somatic symptoms indirectly affects patients’ perceived stress by affecting FoP, and also confirmed that FoP is an intermediary variable between physical symptoms and emotional distress.64 The above results indicate that symptom burden plays an important role in FoP. Studies have shown that patients with high FoP want support beyond treatment.65 Through post hoc analysis, we found that there was no difference in the total score of FoP between the all-low subgroup and the moderate subgroup, which suggests that HCPs should focus on KTRs in the all-high subgroup and provide psychological cognitive intervention66 or behavioral exercise intervention67 to reduce patients’ FoP by changing individuals and their internal psychological experience. However, there are few studies on FoP in KTRs. Future studies can further explore the influencing factors of FoP in KTRs and develop effective psychological interventions.
Study Strengths and Limitations
This study is the first to explore the relationship between symptom burden and FoP in KTRs. Meanwhile, our investigation was a multi-center study, and samples from two tertiary hospitals were selected for research and analysis. However, this study was cross-sectional, and thus, we could not accurately determine the influencing factors of each symptom burden subgroup, while this study only carried out potential category analyses for a limited number of symptoms and did not achieve a comprehensive assessment of symptoms. Future research should focus on the longitudinal study of symptom clusters in KTRs and further determine factors to predict patients with high symptom burden, to lay a foundation for effective symptom management in KTRs.
Conclusion
In conclusion, this study is the first to analyze symptom clusters of KTRs from a patient-centered perspective. The symptom burden of KTRs was mostly moderate or lower, and the latent classes included the all-high subgroup, moderate subgroup, and all-low subgroup. High symptom burden is more likely to occur in patients who are female, have a per capita monthly income of 2000–6000, post-transplant time >12 months, and have concomitant hyperuricemia. In addition, symptom burden was the influencing factor of FoP, and the FoP score of the all-high subgroup was the highest. These findings can help healthcare providers identify patients at high risk for developing severe symptoms. By providing personalized and predictive interventions early in disease progression, patients can improve the effectiveness of symptom management and reduce symptom burden. This, in turn, could help reduce the FoP and improve disease prognosis.
Acknowledgments
The author would like to express their deepest appreciation to all the staff and patients in the two centers involved in this study. The author also would like to acknowledge the professors who guided this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tingle SJ, Figueiredo RS, Moir JA, Goodfellow M, Talbot D, Wilson CH. Machine perfusion preservation versus static cold storage for deceased donor kidney transplantation. Cochrane Database Syst Rev. 2019;3(3):Cd011671. doi:10.1002/14651858.CD011671.pub2
2. Taylor K, Chu NM, Chen X, et al. Kidney disease symptoms before and after kidney transplantation. Clin J Am Soc Nephrol. 2021;16(7):1083–1093. doi:10.2215/CJN.19031220
3. Wang Y, Van Der Boog P, Hemmelder MH, Dekker FW, De Vries A, Meuleman Y. Understanding health-related quality of life in kidney transplant recipients: the role of symptom experience and illness perceptions. Transpl Int. 2023;36:10837. doi:10.3389/ti.2023.10837
4. Teng S, Zhang S, Zhang W, et al. Symptom experience associated with immunosuppressive medications in Chinese kidney transplant recipients. J Nurs Scholarsh. 2015;47(5):425–434. doi:10.1111/jnu.12157
5. Gentile S, Beauger D, Speyer E, et al. Factors associated with health-related quality of life in renal transplant recipients: results of a national survey in France. Health Qual Life Outcomes. 2013;11(1):88. doi:10.1186/1477-7525-11-88
6. Sarier M, Seyman D, Tekin S, et al. Comparision of ureteral stent colonization between deceased and live donor renal transplant recipients. Transplant Proc. 2017;49(9):2082–2085. doi:10.1016/j.transproceed.2017.09.028
7. Purnajo I, Beaumont JL, Polinsky M, Alemao E, Everly MJ. Trajectories of health-related quality of life among renal transplant patients associated with graft failure and symptom distress: analysis of the BENEFIT and BENEFIT-EXT trials. Am J Transplant. 2020;20(6):1650–1658. doi:10.1111/ajt.15757
8. Wang H, Du C, Liu H, et al. Exploration of symptom experience in kidney transplant recipients based on symptoms experience model. Qual Life Res. 2020;29(5):1281–1290. doi:10.1007/s11136-019-02404-5
9. Zhang L, Wang J, Chen T, Tian M, Zhou Q, Ren J. Symptom clusters and quality of life in cervical cancer patients receiving concurrent chemoradiotherapy: the mediating role of illness perceptions. Front Psychiatry. 2021;12:807974. doi:10.3389/fpsyt.2021.807974
10. Loban K, Horton A, Robert JT, et al. Perspectives and experiences of kidney transplant recipients with graft failure: a systematic review and meta-synthesis. Transplant Rev. 2023;37(2):100761. doi:10.1016/j.trre.2023.100761
11. Langegård U, Ahlberg K, Björk-Eriksson T, et al. The art of living with symptoms: a qualitative study among patients with primary brain tumors receiving proton beam therapy. Cancer Nurs. 2020;43(2):E79–e86. doi:10.1097/NCC.0000000000000692
12. Miaskowski C, Barsevick A, Berger A, et al. Advancing symptom science through symptom cluster research: expert panel proceedings and recommendations. J Natl Cancer Inst. 2017;109(4):djw253. doi:10.1093/jnci/djw253
13. Aktas A, Walsh D, Rybicki L. Symptom clusters: myth or reality? Palliat Med. 2010;24(4):373–385. doi:10.1177/0269216310367842
14. Du CY, Wu SS, Fu YX, Wang H, Zhao J, Liu HX. Transplant-related symptom clusters in renal transplant recipients. Clin Nurs Res. 2021;30(3):343–350. doi:10.1177/1054773820920484
15. Fu L, Feng X, Jin Y, et al. Symptom clusters and quality of life in gastric cancer patients receiving chemotherapy. J Pain Symptom Manage. 2022;63(2):230–243. doi:10.1016/j.jpainsymman.2021.09.003
16. Rha SY, Lee J. Stable symptom clusters and evolving symptom networks in relation to chemotherapy cycles. J Pain Symptom Manage. 2021;61(3):544–554. doi:10.1016/j.jpainsymman.2020.08.008
17. Lockwood MB, Chung S, Puzantian H, et al. Symptom cluster science in chronic kidney disease: a literature review. West J Nurs Res. 2019;41(7):1056–1091. doi:10.1177/0193945918808766
18. Luo J, Liu R, Luo Y, et al. The high burden of symptoms associated with cognitive impairment in lung cancer patients: a latent class analysis. Asia Pac J Oncol Nurs. 2023;10(4):100200. doi:10.1016/j.apjon.2023.100200
19. Ye Y, Mei J, Zhang J, Zhao Q, Fan X. The heterogeneity of physical and anxiety symptoms and quality of life among patients with heart failure: a latent class analysis. J Cardiovasc Nurs. 2022;37(6):558–569. doi:10.1097/JCN.0000000000000867
20. Lockwood MB, Lash JP, Pauls H, et al. Physical symptom cluster subgroups in chronic kidney disease. Nurs Res. 2020;69(2):100–108. doi:10.1097/NNR.0000000000000408
21. Low JK, Crawford K, Manias E, Williams A. Stressors and coping resources of Australian kidney transplant recipients related to medication taking: a qualitative study. J Clin Nurs. 2017;26(11–12):1495–1507. doi:10.1111/jocn.13435
22. Lebel S, Maheu C, Tomei C, et al. Towards the validation of a new, blended theoretical model of fear of cancer recurrence. Psychooncology. 2018;27(11):2594–2601. doi:10.1002/pon.4880
23. Dankert A, Duran G, Engst-Hastreiter U, Keller M, Herschbach P. Fear of progression in patients with cancer, diabetes mellitus and chronic arthritis. Die Rehabil. 2003;42(3):155. doi:10.1055/s-2003-40094
24. Liu QW, Qin T, Hu B, Zhao YL, Zhu XL. Relationship between illness perception, fear of progression and quality of life in interstitial lung disease patients: a cross-sectional study. J Clin Nurs. 2021;30(23–24):3493–3505. doi:10.1111/jocn.15852
25. Xiong J, Qin J, Zheng G, Gao Y, Gong K. The relationship between symptom perception and fear of progression in patients with chronic heart failure: a multiple mediation analysis. Eur J Cardiovasc Nurs. 2023;22(6):638–646. doi:10.1093/eurjcn/zvad024
26. Goebel S, Mehdorn HM. Fear of disease progression in adult ambulatory patients with brain cancer: prevalence and clinical correlates. Support Care Cancer. 2019;27(9):3521–3529. doi:10.1007/s00520-019-04665-9
27. Lucas AR, Pan JH, Ip EH, et al. Validation of the Lee-Jones theoretical model of fear of cancer recurrence among breast cancer survivors using a structural equation modeling approach. Psychooncology. 2023;32(2):256–265. doi:10.1002/pon.6076
28. Yang Y, Li W, Wen Y, et al. Fear of cancer recurrence in adolescent and young adult cancer survivors: a systematic review of the literature. Psychooncology. 2019;28(4):675–686. doi:10.1002/pon.5013
29. Lenz ER, Pugh LC, Milligan RA, Gift A, Suppe F. The middle-range theory of unpleasant symptoms: an update. ANS Adv Nurs Sci. 1997;19(3):14–27. doi:10.1097/00012272-199703000-00003
30. Yang Y, Sun H, Liu T, et al. Factors associated with fear of progression in Chinese cancer patients: sociodemographic, clinical and psychological variables. J Psychosom Res. 2018;114:18–24. doi:10.1016/j.jpsychores.2018.09.003
31. Yang L, Liu J, Liu Q, Wang Y, Yu J, Qin H. The relationships among symptom experience, family support, health literacy, and fear of progression in advanced lung cancer patients. J Adv Nurs. 2023;79(9):3549–3558. doi:10.1111/jan.15692
32. Formann AK, Kohlmann T. Latent class analysis in medical research. Stat Methods Med Res. 1996;5(2):179–211. doi:10.1177/096228029600500205
33. Vermunt JK. Latent class models for clustering: a comparison with K-means. Can J Marketing Res. 2002;20(3):36–43.
34. Ryan CJ, Vuckovic KM, Finnegan L, et al. Acute coronary syndrome symptom clusters: illustration of results using multiple statistical methods. West J Nurs Res. 2019;41(7):1032–1055. doi:10.1177/0193945918822323
35. Nylund-Gibson K, Garber AC, Carter DB, et al. Ten frequently asked questions about latent transition analysis. Psychol Methods. 2023;28(2):284–300. doi:10.1037/met0000486
36. Mehnert A, Herschbach P, Berg P, Henrich G, Koch U. Fear of progression in breast cancer patients--validation of the short form of the fear of progression questionnaire (FoP-Q-SF). Z Psychosom Med Psychother. 2006;52(3):274–288. doi:10.13109/zptm.2006.52.3.274
37. Wu Q, Ye Z, Li L, Liu P. Reliability and validity of Chinese version of fear of progression questionnaire-short form for cancer patients. Chin J Nurs. 2015;50(12):1515–1519.
38. Liu S, Zhang Y, Miao Q, et al. The mediating role of self-perceived burden between social support and fear of progression in renal transplant recipients: a multicenter cross-sectional study. Psychol Res Behav Manag. 2023;16:3623–3633. doi:10.2147/PRBM.S424844
39. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equation Model. 2014;21(2):263–279.
40. Celeux G, Soromenho G. An entropy criterion for assessing the number of clusters in a mixture model. Journal of Classification. 1996;13(2):195–212. doi:10.1007/BF01246098
41. Magadi W, Lightfoot CJ, Memory KE, et al. Patient activation and its association with symptom burden and quality of life across the spectrum of chronic kidney disease stages in England. BMC Nephrol. 2022;23(1):45. doi:10.1186/s12882-022-02679-w
42. Uyar B. The analysis of immunosuppressant therapy adherence, depression, anxiety, and stress in kidney transplant recipients in the post-transplantation period. Transpl Immunol. 2022;75:101686. doi:10.1016/j.trim.2022.101686
43. Sung C, Hershberger PE, Lockwood MB. Sickness symptoms in kidney transplant recipients: a scoping review. West J Nurs Res. 2023;45(4):344–362. doi:10.1177/01939459221128125
44. Knobbe TJ, Kremer D, Eisenga MF, et al. Sleep quality, fatigue, societal participation, and health-related quality of life in kidney transplant recipients: a cross-sectional and longitudinal cohort study. Nephrol Dial Transplant. 2023;39(1):74–83. doi:10.1093/ndt/gfad148
45. Morton RL, Tong A, Howard K, Snelling P, Webster AC. The views of patients and carers in treatment decision making for chronic kidney disease: systematic review and thematic synthesis of qualitative studies. BMJ. 2010;340(jan19 2):c112. doi:10.1136/bmj.c112
46. Veltkamp DMJ, Wang Y, Meuleman Y, et al. Age and gender differences in symptom experience and health-related quality of life in kidney transplant recipients: a cross-sectional study. Nephrol Dial Transplant. 2023;38(7):1701–1718. doi:10.1093/ndt/gfad023
47. Gunarathne T, Tang LY, Lim SK, Nanayakkara N, Damayanthi H, Abdullah KL. Factors associated with symptom burden in adults with chronic kidney disease undergoing hemodialysis: a prospective study. Int J Environ Res Public Health. 2022;19(9):5540. doi:10.3390/ijerph19095540
48. Yuan Y, Lin L, Wang H, et al. Related factors to the coping style of patients with sudden sensorineural hearing loss. Int Health. 2023;15(2):198–206. doi:10.1093/inthealth/ihac046
49. Carrero JJ, Hecking M, Chesnaye NC, Jager KJ. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat Rev Nephrol. 2018;14(3):151–164. doi:10.1038/nrneph.2017.181
50. Chan DNS, Cheng Q, Miaskowski C, So WKW. Association between financial hardship and symptom burden in patients receiving maintenance dialysis: a systematic review. Int J Environ Res Public Health. 2021;18(18). doi:10.3390/ijerph18189541
51. Wu JR, Moser DK. Health-related quality of life is a mediator of the relationship between medication adherence and cardiac event-free survival in patients with heart failure. J Card Fail. 2021;27(8):848–856. doi:10.1016/j.cardfail.2021.03.004
52. Khoury JE, Atkinson L, Bennett T, Jack SM, Gonzalez A. Coping strategies mediate the associations between COVID-19 experiences and mental health outcomes in pregnancy. Arch Womens Ment Health. 2021;24(6):1007–1017. doi:10.1007/s00737-021-01135-2
53. Xiao P, Zhou Y. Factors associated with the burden of family caregivers of elderly patients with femoral neck fracture: a cross-sectional study. J Orthop Surg Res. 2020;15(1):234.
54. Fletcher BR, Damery S, Aiyegbusi OL, et al. Symptom burden and health-related quality of life in chronic kidney disease: a global systematic review and meta-analysis. PLoS Med. 2022;19(4):e1003954. doi:10.1371/journal.pmed.1003954
55. Xie J, Liu J, Liu M, Yan J, Ding S, Ma K. Self-management and related psychosocial variables among renal transplant patients. Transplant Proc. 2019;51(3):734–741. doi:10.1016/j.transproceed.2019.01.033
56. Wang S, Zhang L, Hao D, et al. Research progress of risk factors and early diagnostic biomarkers of gout-induced renal injury. Front Immunol. 2022;13:908517. doi:10.3389/fimmu.2022.908517
57. Kim DG, Choi HY, Kim HY, et al. Association between post-transplant serum uric acid levels and kidney transplantation outcomes. PLoS One. 2018;13(12):e0209156. doi:10.1371/journal.pone.0209156
58. Dissanayake LV, Zietara A, Levchenko V, et al. Lack of xanthine dehydrogenase leads to a remarkable renal decline in a novel hypouricemic rat model. iScience. 2022;25(9):104887. doi:10.1016/j.isci.2022.104887
59. Gong R, Xu Z, Wei X. The association between vitamin D3 and diabetes in both hyperuricemia and non-hyperuricemia populations. Endocrine. 2021;74(1):90–99. doi:10.1007/s12020-021-02778-y
60. Liu L, Jia HH, Zhou YQ, Liu YR, Yin F, Liu XF. The illness perception and health promotion behaviour of young and middle-aged patients with hyperuricaemia: a qualitative study. Nurs Open. 2022;9(2):1343–1352. doi:10.1002/nop2.1179
61. Lin W, Liu L, Wan J, Liu J, Yang M, Ma H. The status and factors associated with fear of progression in recipients of renal transplantation. Chin J Nurs. 2022;57(01):73–78.
62. Dinkel A, Marten-Mittag B, Kremsreiter K. Association between daily worry, pathological worry, and fear of progression in patients with cancer. Front Psychol. 2021;12:648623. doi:10.3389/fpsyg.2021.648623
63. Hall DL, Lennes IT, Pirl WF, Friedman ER, Park ER. Fear of recurrence or progression as a link between somatic symptoms and perceived stress among cancer survivors. Support Care Cancer. 2017;25(5):1401–1407. doi:10.1007/s00520-016-3533-3
64. Hall DL, Jimenez RB, Perez GK, et al. Fear of cancer recurrence: a model examination of physical symptoms, emotional distress, and health behavior change. J Oncol Pract. 2019;15(9):e787–e797. doi:10.1200/JOP.18.00787
65. Maheu C, Hébert M, Louli J, et al. Revision of the fear of cancer recurrence cognitive and emotional model by Lee-Jones et al with women with breast cancer. Cancer Rep. 2019;2(4):e1172. doi:10.1002/cnr2.1172
66. Tauber NM, O’Toole MS, Dinkel A, et al. Effect of psychological intervention on fear of cancer recurrence: a systematic review and meta-analysis. J Clin Oncol. 2019;37(31):2899–2915. doi:10.1200/JCO.19.00572
67. Kang DW, Fairey AS, Boulé NG, Field CJ, Wharton SA, Courneya KS. A randomized trial of the effects of exercise on anxiety, fear of cancer progression and quality of life in prostate cancer patients on active surveillance. J Urol. 2022;207(4):814–822. doi:10.1097/JU.0000000000002334
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.