Back to Journals » Local and Regional Anesthesia » Volume 17
The Gluteus Deep Investing Fascia Compartment Block: A Novel Technique for Posterior Femoral Cutaneous Nerve Block
Authors Shabani M ![]() , Beye SA
, Beye SA ![]() , Traore A, Echave P, Raingeval X
, Traore A, Echave P, Raingeval X ![]() , Coulibaly D
, Coulibaly D ![]() , Crespo S
, Crespo S
Received 27 December 2023
Accepted for publication 11 April 2024
Published 24 April 2024 Volume 2024:17 Pages 55—65
DOI https://doi.org/10.2147/LRA.S455702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Video abstract of “The Gluteus Deep Investing Fascia Compartment Block” [455702].
Views: 622
Majaliwa Shabani,1 Seydina Alioune Beye,2,* Abdoulaye Traore,3 Pablo Echave,4,* Xavier Raingeval,5,* Daouda Coulibaly,6 Sophie Crespo7,*
1Health_unit, International Committee of the Red Cross, Bamako, Mali; 2Anesthesia Department, Clinique Périnatale Mohamed VI, Bamako, Mali; 3Anesthesia Department, Hôpital Somine Dolo de Mopti, Mopti, Mali; 4Anesthesia Department, Université de Sherbrooke, Sherbrooke, Quebec, Canada; 5Association de Développement et de Recherche en Anesthésie Locorégionale Echoguidée (ADRALE), Paris, France; 6Surgery Department, Centre de Santé de Référence de Kidal, Kidal, Mali; 7Health Unit, International Committee of the Red Cross, Geneva, Switzerland
*These authors contributed equally to this work
Correspondence: Majaliwa Shabani, Health Unit, International Committee of the Red Cross, HAMDALLAYE RUE 239, Postal Office Box: 58, Bamako, Mali, Email [email protected]
Purpose: The posterior femoral cutaneous nerve (PFCN) block is used in regional anesthesia for lower extremity surgery. This study introduces a new ultrasound-guided technique called the “Gluteus-Deep Investing Fascia compartment Block (GDIF block)“ for blocking the PFCN. This approach involves injecting local anesthetic into the potential space between the gluteus maximus muscle and the deep investing fascia, named the ‘Gluteus Deep Investing Fascia Compartment’. The study discusses the anatomical and sonographic features crucial for identifying this compartment and explores the potential benefits of this approach for achieving effective PFCN block. Additionally, it examines the clinical application of the GDIF block for PFCN block as part of the Complete Lower Extremity Fascia Tri-compartment Block technique, named ”CLEFT Block.” This technique combines the suprainguinal fascia iliaca block with GDIF compartment block for PFCN and a sciatic nerve block as exclusive anesthesia technique.
Patients and Methods: Nine patients with weapon-related lower limb injuries underwent surgery at district hospitals supported by the International Committee of the Red Cross. Between October and December 2023, seventeen above-knee procedures were performed for the nine patients using the GDIF block as part of a CLEFT block technique. Anesthesia was performed with a CLEFT block technique using a volume ratio of 1:1 of 1% lidocaine and 0.5% levobupivacaine.
Results: The GDIF block technique for PFCN blockade was performed successfully in all patients without complications, achieving complete PFCN blockade. The CLEFT block technique proved effective as the sole anesthetic technique for seventeen above-knee procedures. All surgeries were completed successfully without additional pain medication or conversion to general anesthesia.
Conclusion: The GDIF block appears to be a promising technique for anesthetic management, alone or as part of the CLEFT block. Further research with a larger patient population is necessary to validate these findings.
Keywords: posterior femoral cutaneous nerve block, deep investing fascia, sciatic nerve block, gluteal deep investing fascia compartment block, GDIF block, CLEFT block
Introduction
The posterior femoral cutaneous nerve (PFCN) is predominantly sensory and plays a significant role in innervating the posterior aspect of the thigh, the perineum and occasionally the leg.1,2 Despite its importance in innervating a substantial area, the block of this nerve is rarely, if ever, addressed in regional anesthesia literature.3–6
For above-knee surgery requiring regional anesthesia, performing a PFCN block alongside the sciatic (SN) nerve block is essential.7,8 Additionally, incomplete blocks in below-knee surgery may be due to the PFCN’s innervation extending beyond the popliteal fossa, highlighting the importance of including a PFCN block.9,10
Various perineural approaches to block the PFCN at the gluteal crease or at the thigh have been proposed in the literature. However, the main challenge is the localization of the PFCN, which can be difficult to identify by ultrasound and, given its purely sensory nature, neurostimulation offers little assistance.11–14
We have hypothesized that, instead of attempting to visualize the PFCN, the diffusion of the injectate into the space bounded by the epimysium of the gluteus maximus muscle and the deep investing fascia, through which the nerve passes, could allow for its effective blockade within its distinct compartment: The Gluteus-Deep Investing Fascia Compartment (GDIF Compartment).
By combining the PFCN block with the sciatic nerve block, injecting the local anesthetic into their respective compartments could promote rapid onset while decreasing the failure rate of PFCN blockade compared to an isolated sciatic nerve block in a conventional approach.15,16
We present a case series involving nine patients with weapon-related injuries where the Complete Lower Extremity Fascia Tri-compartment Block (CLEFT Block) technique was used. This technique included a blockade of the PFCN within the gluteal-deep investing fascia compartment, the suprainguinal fascia iliaca compartment (SIFI) block, and the sciatic nerve block within the subgluteal compartment, as the sole anesthetic method, optionally supplemented by light sedation. Prior to anesthesia and surgery, written informed consent was obtained from all adult patients. For children, written informed consent was obtained from their legal guardians or parents. All adult patients, and legal guardians or parents for children, were asked to provide separate written informed consent for publication. The study was approved by the Ethics Committee of Somine Dolo Hospital in Mopti, registered under Number 01/2024, and the Ethics Committee of Université des Sciences, des Techniques et des Technologies de Bamako, registered under Number 2024/15/USTTB. The study was conducted in full compliance with the Declaration of Helsinki.
The Posterior Femoral Cutaneous Nerve
The posterior femoral cutaneous nerve is a purely sensory nerve derived from the anterior rami of S1 through S3. The posterior femoral cutaneous nerve (PFCN) traverses from the pelvis, lying initially medial to the sciatic nerve and then beneath the gluteus maximus along with the inferior gluteal artery. Within the gluteal area, the posterior femoral cutaneous nerve resides consistently beneath the deep investing fascia (DIF) of the gluteus maximus muscle.1,2,11
The PFCN emerges from the lower edge of the gluteus maximus and continues down the posterior aspect of the thigh and the leg, giving off femoral and sural branches.1,2 The terminal branches of the posterior femoral cutaneous nerve may provide cutaneous innervation as distal as the heel.2
The Deep Investing Fascia of the Gluteus Maximus and Clinical Implication
In the gluteal region, the gluteus maximus muscle overlays the sciatic nerve, positioned laterally to the posterior femoral cutaneous nerve and the inferior gluteal artery. The sciatic nerve runs through a defined intermuscular space known as the “subgluteal compartment”, bounded by the ischial tuberosity and the greater trochanter, lying dorsal to the quadratus femoris and ventral to the gluteus maximus.1–3 The DIF creates an anatomical partition between the gluteus maximus and the sciatic nerve (Figure 1).11
 |
Figure 1 Sonoanatomy details of the deep investing fascia and compartments. Notes: 1, epimysium of gluteus maximus; 2, deep investing Fascia; 3, inferior gluteal artery; 4, posterior femoral cutaneous nerve; 5, epimysium of quadratus femoris; 6, sciatic nerve; CT, conjoint tendon of biceps femoris. |
The sciatic nerve emerges from the “subgluteal compartment” and is situated posteriorly to the adductor magnus muscle, with the DIF of the thigh serving as a partitioning barrier. This fascia delineates the separate anatomical pathway of the posterior femoral cutaneous nerve (PFCN), which is confined within a distinct compartment formed anteriorly by the DIF of the thigh, laterally by the long head of the biceps femoris (LHBF), and superiorly by the overlying gluteus maximus and semitendinosus muscles.11
The DIF serves as a distinct anatomical barrier between the posterior femoral cutaneous nerve (PFCN) and the sciatic nerve within the gluteal and subgluteal regions. This fascial layer creates continuous distinct compartments that house both nerves. This separation could clarify why the local anesthetic (LA) tends to spread either upward or downward within their respective compartments, typically without intermingling.11
Description of the Block Technique
In the transgluteal approach, as described by Hadzic A, the patient is placed in lateral decubitus position with the operative side up, and the leg is flexed at the knee if possible (Figure 2A). The sciatic nerve is located beneath the gluteus maximus muscle, above the quadratus femoris muscle, and is situated between two key bony landmarks: the ischium and the trochanter (Figure 2A and D).6 A curvilinear ultrasound probe is utilized for adult patients, while a linear probe may be employed for pediatric patients and slender adults. Both the sciatic and posterior femoral cutaneous (PFCN) nerves are accessed via the same entry point.
 |
Figure 2 (A). Patient position and probe placement: probe is placed between the greater trochanter and ischial tuberosity. (B). Two-step technique for the blockade of PFCN and SN: dash arrow shows the needle direction for PFCN blockade within the Gluteus deep investing fascia compartment and needle shadow for SN blockade within the subgluteal compartment by traversing the deep investing fascia.(C and D), Sonoanatomy: Injectate diffusion into the Gluteus Deep investing fascia compartment for PFCN blockade and into the subgluteal compartment for SN blockade: 1, PFCN; 2, epimysium of Gluteus maximus muscle; CT, conjoint tendon for biceps femoris and semi tendinous; 3, inferior gluteal artery; 4, Deep investing fascia of gluteus maximus; 5, epimysium of quadratus femoris; LA, local anesthetic. |
Step 1: The needle is guided medially and deeply, placing its tip between the epimysium of gluteus maximus muscle and the tendon of the biceps femoris, staying within the deep investing fascia of the gluteus maximus muscle (Figure 2B). Near this location, the inferior gluteal artery is often noted just medial to the PFCN, positioned between the DIF and the epimysium of gluteus maximus muscle. The goal is to locate the potential space between the epimysium of the gluteus maximus and the DIF that lies over the conjoint tendon of the biceps femoris and semitendinosus muscles, which are prominent at the ischial tuberosity (Figures 1 and 2B). Careful hydro dissection is performed using 5 to 10 mL of local anesthetic, which spreads towards the PFCN while remaining above the DIF of the gluteus maximus, thereby acting as a barrier between the PFCN and the sciatic nerve (Figure 2B, C, D and video link).
Step 2: The needle is then reoriented towards the sciatic nerve by penetrating the deep investing fascia of the gluteus maximus muscle, where the remaining local anesthetic is administered in the subgluteal compartment (Figure 2B, C, D and video link)
By scanning down to the gluteal crease, the diffusion of the local anesthetic can be visualized, along with the DIF that segregates the sciatic nerve and PFCN into their respective compartment (Figure 3).
 |
Figure 3 (Ai). Probe position using a transgluteal approach by placing the needle transversely on the posterior buttock, between the ischial tuberosity and the greater trochanter. (Aii). Simulated needle path using an in-plane approach in the “two-step technique” for the gluteal deep investing fascia compartment (GDIF) block (dashed arrow) and the sciatic nerve block within the subgluteal compartment (solid arrow). GMM, gluteus maximus muscle; QFM, Quadratus femoris muscle; CT, tendon conjoint; IT, ischial tuberosity; GT, Greater trochanter; SN, sciatic nerve (white arrow); small white triangles (▲) for demarcation of the DIF (Aiii). Local anesthetic diffusion (blue-shaded area) within the gluteus deep investing fascia compartment and the subgluteal compartment separated by the DIF.(Bi) Scan downward by moving the probe from the buttock (probe position (Ai)) to the gluteal crease (probe position (Bi)) to visualize the diffusion of local anesthetics from the gluteal to the gluteal crease.(Aiii),(Bii) and (Biii):Diffusion of local anesthetics from the gluteal to the subgluteal region: The DIF of the thigh, a continuum of the DIF of the gluteus maximus, separates the sciatic nerve and PFCN, both nerves surrounded by local anesthetics (blue-shaded area) within their respective compartments. ST, semitendinosus muscle; LHBF, long head of biceps femoris; AMM, adductor magnus muscle; SN, sciatic nerve (white arrow); PFCN, posterior femoral cutaneous nerve (Yellow arrow). |
In our protocol, the PFCN block serves as an adjunct to the sciatic nerve block combined to the suprainguinal fascia iliaca (SIFI) block for above-knee surgery. This combined nerve block technique was named the Complete Lower Extremity Fascia Tri-compartment Block, with the acronym CLEFT block. A high volume of low-concentration local anesthetic is required to effectively block the nerves (Femoral nerve, Obturator nerve, LFCN,PFCN, Sciatic) in their respective compartments.
For our CLEFT block (triple compartments block regimen), a volume ratio of 1:1 of 0.5% levobupivacaine and 1% lidocaine is used, totaling a volume of 0.8mL/kg as maximum limit.
The volume of local anesthetic is divided as follows: 60% (0.5 mL/kg) is allocated to the SIFI block, and the remaining 40% is distributed between the sciatic nerve and PFCN blocks. For adult patients, a 100mm insulated echogenic needle for nerve block is used, while a 50mm needle is preferred for pediatric patients. As a compartment-diffusing block, this procedure does not require nerve stimulation and is performed under strict aseptic conditions.
Tips for successful identification of GDIF compartment
Drawing from the author’s experience with the CLEFT technique, initiating the procedure with the SIFI block in a neutral position proves beneficial for alleviating patient pain during subsequent repositioning to a lateral position, taking advantage of the onset of the SIFI block.
It is advisable to commence the procedure by performing the GDIF block for the easy identification of the GDIF compartment first and the subgluteal compartment for sciatic nerve block secondarily.
For the GDIF block realization, attempt to localize the inferior gluteal artery, avoiding contact. Position the tip of the needle within the DIF, in contact with the conjoint tendon of the biceps femoris and semitendinosus muscles; resistance should be felt during hydro dissection testing. Slowly withdraw the needle while attempting hydro dissection until the GDIF compartment opens (refer to the video link).
Case Series
Patients and Methods
Data for this study were retrospectively collected from the Kidal Health Referral Center, a hospital supported by the International Committee of the Red Cross (ICRC), during the period from October to December 2023. The dataset is succinctly summarized in Table 1. All nine patients included in the case series underwent the CLEFT block technique, which includes a suprainguinal fascia iliaca (SIFI) compartment block, combined with a GDIF compartment block for PFCN, and a sciatic nerve block within the subgluteal compartment, serving as the exclusive anesthesia technique. The PFCN block was performed using the Gluteus deep investing fascia (GDIF) compartment block for all patients in this case series.
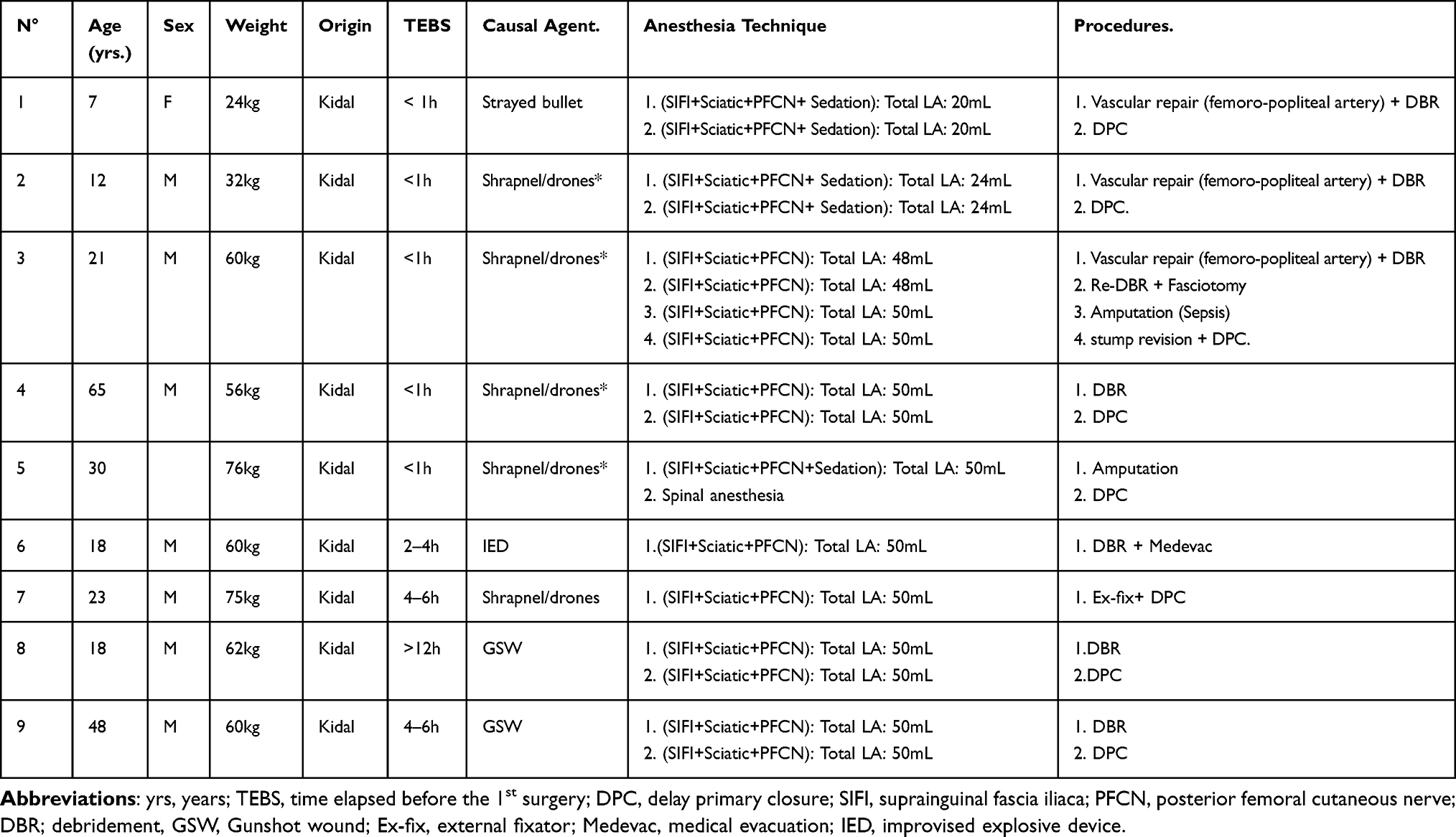 |
Table 1 Summary of Case Series |
Results
A total of seventeen blocks were successfully administered to the nine patients undergoing various procedures, particularly those involving above-knee surgery (Table 1).
Prior to surgery, a skin sensitivity test (Pinprick and Light Touch) was performed, revealing adequate coverage of the areas innervated by the PFCN, the sciatic nerve, the obturator nerve, the femoral nerve, and the lateral femoral cutaneous nerve in all patients. Motricity was not assessed in all patients due to the nature of the injury, which included traumatic amputation, complex open fracture, delayed primary closure, and stump revision after above-knee amputation, as well as unstable weapon wounds with vascular injury. Notably, there was no necessity for additional analgesics or conversion to general anesthesia in any of the cases. Within this patient cohort, two children and one adult also received light sedation before the administration of the blocks.
The GDIF compartment block, as part of the CLEFT block technique, provided adequate anesthesia for above-knee surgery in all seventeen consecutive surgical procedures (100% success rate).
Discussion
The Posterior Femoral Cutaneous Nerve (PFCN) is an important sensory nerve responsible for providing sensory innervation to a large portion of the skin on the back of the thigh, the perineum and, occasionally, areas of the lower leg.1,2 The PFCN is significant also for its potential role in pain syndromes related to nerve entrapment or injury.17,18
In the context of regional anesthesia, for surgery involving the posterior aspect of the thigh, and some extent below-knee surgery, the PFCN block should be considered as valuable component of the anesthetic plan.2,9,10,14 Despite its critical role, PFCN blockade is less frequently discussed in literature compared to other neural structures like the lumbar plexus or its branches, and the sciatic nerve.3–6
In our PFCN block technique, we target the Gluteal Deep Investing Fascia (GDIF) compartment, a potential space between the epimysium of the gluteus maximus and the DIF of the gluteus maximus above the conjoint tendon at the ischial tuberosity. The inferior gluteal artery, which accompanies the PFCN, serves as a key ultrasound landmark and must be avoided during this approach. Our GDIF compartment block aims for anesthetic diffusion within this compartment rather than precise nerve localization. The diffusion compartment extends into the subgluteal region, and the DIF acting as an anatomical barrier (Figure 4). This could explain the delayed or unsuccessful anesthesia of the PFCN from an isolated sciatic nerve block at the gluteal and subgluteal levels.11,15
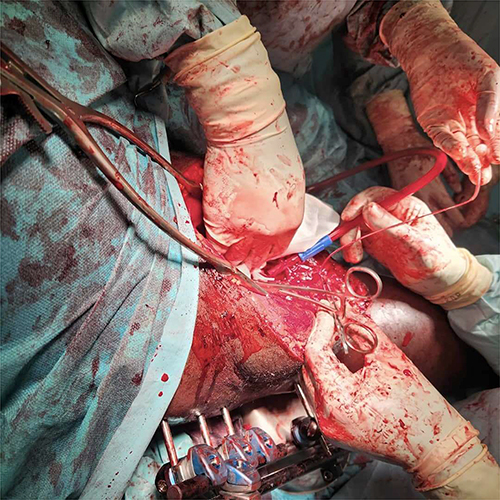 |
Figure 4 Vascular repair of popliteal artery and external fixation for fracture immobilization from a gunshot wound under regional anesthesia using CLEFT block technique combining SIFI block with sciatic block and GDIF compartment block for PFCN. Hôpital Somine Dolo de Mopti, Sevaré, Mali.Somine Dolo Hospital, Mopti, Mali. |
Techniques for PFCN block via a subgluteal approach or at the mid-thigh level have been proposed but remain underutilized in practice.3–6,9–11,14,19 The PFCN’s visibility, due to anatomical variations or in obese patients, may be limited.11,13,19 Johnson et al suggested the potential feasibility of a subgluteal PFCN block in a cadaveric study, and Xiuhua et al reported the use of a combined subgluteal PFCN block with sciatic and femoral blocks for below-knee surgery.9,11
In practice, we use a transgluteal approach for sciatic block and GDIF compartment block in conjunction with the SIFI block for above-knee surgery. This strategy, named CLEFT block, has significantly reduced the number of spinal anesthesia for lower limb surgery in patients with gunshot wounds and allowed the management of high-risk critical patients with hemodynamic instability requiring vascular repair or amputation in ICRC-supported hospitals in Mali (Figure 4).16
The CLEFT block technique was successful in blocking all five nerves- femoral nerve, obturator nerve, lateral femoral cutaneous nerve, PFCN and sciatic - of importance for above-knee surgery.
In a randomized controlled trial for total hip replacement, ultrasound-guided SIFI block achieved a 67% success rate for blocking all three nerves (femoral, lateral cutaneous, and obturator) according to Tarekegn et al and Desmet et al20,21 Additionally, a cadaver study by Vermeylen et al demonstrated successful blockade of these same nerves using ultrasound-guided SIFI block when 40 mL of local anesthetic was administered.22
In our protocol for CLEFT block technique, we adhered to a maximum volume of 0.8 mL/kg for local anesthetics in our combined technique for SIFI, SN, and PFCN blocks, with 60% of the volume (0.5 mL/kg) allocated to the SIFI block. This volume limitation aligns with similar protocols used in studies by Ponde et al who explored the spread of local anesthetic in the fascia iliaca compartment.23 However, it is important to acknowledge that the effectiveness of the SIFI block may be impacted by the volume of local anesthetic used, as highlighted in the studies.22,23
Several publications describe successful management of high-risk patients using regional anesthesia techniques combining paravertebral lumbar plexus and parasacral sciatic nerve block for above knee major surgery.24,25 However, it’s important to note that unlike our CLEFT block technique, these combined blocks are complex procedures requiring advanced skills and carry a higher risk of complications, as highlighted by Gupta et al.26
Several studies have demonstrated the feasibility of performing major lower limb surgery, above-knee amputations or knee arthroplasties in high-risk patients using a combination of sciatic, obturator, and femoral nerve blocks. In some cases, the lateral femoral cutaneous nerve was also included in the block. However, these studies have limitations.27–32
Firstly, most of the studies did not include a block of posterior femoral cutaneous nerve (PFCN). This nerve innervates the skin on the back of the thigh, and its blockade is crucial for complete anesthesia during these procedures.1,2
Secondly, achieving consistent blockade of the PFCN during a sciatic nerve block is challenging, with reported failure rates of approximately 85% and 32% for the anterior and posterior approaches, respectively.15 This inconsistency can lead to inadequate pain control and discomfort intraoperatively, leading to the administration of moderate to deep sedation.31
In contrast, our CLEFT block technique achieved adequate anesthesia for seventeen consecutive major above-knee and knee procedures without requiring additional sedation or conversion to general anesthesia. Notably, this technique also achieved consistent block of the posterior femoral cutaneous nerve.
Clinical Implications
The Complete Lower Extremity Fascia Tri-compartment Block, also known as the CLEFT Block technique, is a triple compartment nerve block targeting the suprainguinal fascia iliaca (SIFI), gluteal-deep investing fascia (GDIF), and subgluteal compartments. It requires two needle insertion points and offers a viable alternative to both general and spinal anesthesia for high-risk patients undergoing above-knee surgeries.
The Complete Lower Extremity Fascia Tri-compartment Block (CLEFT block) presents as a potentially safe and effective solution for anesthesia and postoperative analgesia in major lower extremity surgery including knee arthroplasty and above-knee amputation, even as a sole anesthetic technique. It achieves this by targeting three critical nerves: the femoral, obturator, and sciatic nerves. Additionally, the CLEFT block encompasses all femoral cutaneous nerves, including the posterior femoral cutaneous (PFCN), lateral femoral cutaneous (LFCN), intermediate femoral cutaneous, and medial femoral cutaneous nerves.
Compared to more complex and potentially risky proximal nerve blocks like the combined parasacral and lumbar plexus blocks, the CLEFT Block technique boasts several advantages.24–26 It has a lower risk of complications, is easier to learn and perform, and can be executed faster while achieving similar results in terms of the covered anatomical areas and blocked nerves (posterior femoral cutaneous, sciatic, femoral, obturator, and lateral femoral cutaneous nerves).
Compared to other block techniques like the “Quadri Block” (involving femoral, obturator, lateral femoral cutaneous, and sciatic nerves) and the SOFT block (Sciatic, Obturator, and Femoral nerve block Technique), the CLEFT technique appears faster.29,30 It uses only two needle insertion points and avoids directly targeting individual nerves. Instead, the local anesthetic diffuses through three compartments: the suprainguinal fascia iliaca, gluteal-deep investing fascia, and subgluteal compartments. This approach potentially reduces the overall block performance time by minimizing the time spent on neural structure identification (scanning) and needle placement.
Furthermore, the CLEFT block technique consistently blocked the posterior femoral cutaneous nerve (PFCN), achieving a 100% success rate in a series of 17 consecutive blocks. This contrasts with the Quadriblock and Soft Block techniques, where PFCN blockade is inconsistent and has a high failure rate.15,29–32
The GDIF compartment block, when administered as a standalone technique, can potentially serve as a motor-sparing block. In this context, the deep investing fascia acts as a barrier, impeding the local anesthetic from reaching the sciatic nerve during cutaneous surgery on the posterior aspect of the thigh, thereby enhancing ambulatory, safety, and recovery.11
Strengths and Limitations
The GDIF block for the PFCN, along with the SN block using the same needle entry point via the transgluteal approach, offers a more accessible option compared to complex and potentially risky blocks like the parasacral plexus block, which require greater expertise in regional anesthesia. Our study showed that the GDIF block effectively covered the PFCN’s innervation area. The GDIF block, combined with SN and SIFI blocks known as CLEFT block technique, a five in two block technique, can serve as the sole anesthetic technique for above-knee surgeries.
However, our findings have limitations. First, the study is retrospective and non-comparative, and the limited sample size restricts generalizability. Second, being conducted in an austere environment with war-wounded patients, the study faced constraints in data collection, including information on performance time, onset time, and duration of anesthesia and analgesia.
Additionally, the technique requires three blocks using a large volume of local anesthetic, raising concerns about local anesthetic systemic toxicity, which should be closely monitored, especially in war surgery settings with limited resources.
As a compartment block technique, the CLEFT block allows the use of lower concentrations of local anesthetics, reducing the potential for local anesthetic systemic toxicity (LAST). Our protocol employs a volume ration of 1:1 of lidocaine 1% and levobupivacaine 0.5% at a total dose of 0.8 mL/kg, distributed among the three compartments: 60% of the volume for the SIFI compartment block, and the remaining volume for the subgluteal compartment for the sciatic nerve block and GDIF block for the PFCN block. This approach provides sufficient volume for the blocks while maintaining a lower concentration and avoiding exceeding the recommended total dose, further minimizing the risk of LAST.
Future Research
Our study involved weapon wounded patients in low resource setting, further research on a larger scale, in general population, may be required to corroborate our findings and to perform a comparative analysis of our combined three-block technique (CLEFT block) against other anesthetic methods.
A more methodical study in a more controlled environment, allowing for a more detailed analysis of the “GDIF” block alone and in the context of the CLEFT block, including elements such as the performance time, the onset time, the duration of the block, the success rate, the use of sedation, the conversion rate to general anesthesia and the duration of analgesia, will allow to define the place of our approach in comparison to existing techniques for locoregional anesthesia of above-knee surgery.
Our study employed the transgluteal approach that target GDIF compartment for PFCN block and subgluteal compartment for SN block, which lays the groundwork for future comparisons with the subgluteal approach that targets the SN and the PFCN individually using a perineural technique.
Conclusion
The Gluteal Deep Investing Compartment Block (GDIF compartment block) is presented as an alternative to the subgluteal PFCN block when the PFCN is not visible or when the injection point is unsuitable or inaccessible due to skin infection, burn, hematoma, or proximal femoral fracture. The CLEFT block technique, serve as a safe and accessible alternative compared to more complex, advanced, and risky regional anesthesia techniques (lumbar plexus and parasacral plexus blocks), as well as general and spinal anesthesia in high-risk patients. The Gluteal Deep Investing compartment block (GDIF block) for PFCN enriches the repertoire of blocks that can be performed without requiring advanced expertise in ultrasound-guided regional anesthesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jiamjunyasiri A, Tsutsumi M, Muro S, Akita K. Origin, course, and distribution of the posterior femoral cutaneous nerve and the spatial relationship among its branches. Anat Sci Int. 2023;98(4):540–547. doi:10.1007/s12565-023-00721-x.
2. Feigl GC, Schmid M, Zahn PK, Avila González CA, Litz RJ. The posterior femoral cutaneous nerve contributes significantly to sensory innervation of the lower leg: an anatomical investigation. Br J Anaesth. 2020;124(3):308–313. doi:10.1016/j.bja.2019.10.026.
3. Hadzic A. Hadzic’s Textbook of Regional Anesthesia and Acute Pain Management,
4. Rodziewicz TL, Patel S, Garmon EH. Lower extremity blocks. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available from https://www.ncbi.nlm.nih.gov/books/NBK470184/.
5. Tran DQ, Salinas FV, Benzon HT, Neal JM. Lower extremity regional anesthesia: essentials of our current understanding. Reg Anesth Pain Med. 2019:rapm-2018–000019. PMID: 30635506. doi:10.1136/rapm-2018-000019
6. Hadzic A. Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia.
7. Genc C, Akdeniz S, Canikli S, Selcuk Kusderci H, Kefeli Celik H, Tulgar S. Ultrasound-guided suprainguinal fascia iliaca block as part of anesthesia management for lower extremity surgeries: a single-center retrospective cohort feasibility study. Cureus. 2023;15(10):e47795. doi:10.7759/cureus.47795.
8. Almeida CR. Deep fascia iliaca block combined with sacral plexus block for Hip fracture surgery: a retrospective series of cases. Indian J Anaesth. 2023;67(6):560–563. doi:10.4103/ija.ija_540_22.
9. Xiuhua X, Zhiqiang Q, Quanhong Z. Posterior femoral cutaneous nerve block improves regional anaesthesia for below-knee surgery. Br J Anaesth. 2021;126(5):e171–e172. doi:10.1016/j.bja.2021.02.002.
10. Hamilton DL. Is posterior femoral cutaneous nerve block clinically relevant in awake foot and ankle surgery? Comment on Br J Anaesth. 2021; 126: e171-2. Br J Anaesth. 2022;128(1):e8-e10–2. doi:10.1016/j.bja.2021.09.029
11. Johnson CS, Johnson RL, Niesen AD, Stoike DE, Pawlina W. Ultrasound-guided posterior femoral cutaneous nerve block: a cadaveric study. J Ultrasound Med. 2018;37(4):897–903. doi:10.1002/jum.14429.
12. Wang TC, Yang CC. Letter to the editor: ultrasound-guided posterior femoral cutaneous nerve block. Agri. 2018;30(2):102–103. doi:10.5505/agri.2018.75688.
13. Meng S, Lieba-Samal D, Reissig LF, et al. High-resolution ultrasound of the posterior femoral cutaneous nerve: visualization and initial experience with patients. Skeletal Radiol. 2015;44(10):1421–1426. doi:10.1007/s00256-015-2177-6.
14. Topçu I, Aysel I. Ultrasound guided posterior femoral cutaneous nerve block. Agri. 2014;26(3):145–148. doi:10.5505/agri.2014.26122.
15. Ota J,Sakura S,Hara K,Saito Y. Ultrasound-Guided Anterior Approach to Sciatic Nerve Block: A Comparison with the Posterior Approach. Anesthesia & Analgesia. 2009;108:660–665. doi:10.1213/ane.0b013e31819b0640.
16. Shabani M, Beye SA, Traore A, Raingeval X, Coulibaly D, Crespo S. Combined supra-inguinal fascia iliaca, sciatic nerve, and posterior femoral cutaneous nerve blocks in austere settings for hemodynamically unstable patients with vascular injuries from weapon wounds: a case series. Local Reg Anesth. 2024;17:19–27. doi:10.2147/LRA.S452367
17. Kachniarz B, Dellon AL. Relief of sitting pain by resecting posterior femoral cutaneous nerve, and elucidation of its anatomical branching pattern. J Reconstr Microsurg. 2021;37(8):687–693. doi:10.1055/s-0041-1726027.
18. Sheplay KA, Sheplay AW. Posterior femoral cutaneous nerve impingement post marathon: a case report. Pain Pract. 2023;23(8):970–973. doi:10.1111/papr.13231
19. Kang C, Hwang DS, Song JH, et al. Clinical analyses of ultrasound-guided nerve block in lower-extremity surgery: a retrospective study. J Orthop Surg (Hong Kong). 2021;29(1):2309499021989102. doi:10.1177/2309499021989102.
20. Tarekegn F, Sisay A. Amanuel sisay, A review of evidence-based clinical practice on fascia iliaca compartment block for lower limb injury. Ann Med Surg. 2021;69:102758. doi:10.1016/j.amsu.2021.102758
21. Desmet M, Vermeylen K, Van HI, et al. A longitudinal supra-inguinal fascia iliaca compartment block reduces morphine consumption after total hip arthroplasty. Reg Anesth Pain Med. 2017;42(3):327–333. doi:10.1097/AAP.0000000000000543
22. Vermeylen K, Soetens F, Leunen I, et al. The effect of the volume of supra-inguinal injected solution on the spread of the injectate under the fascia iliaca: a preliminary study. J Anesth. 2018;32(6):908–913. doi:10.1007/s00540-018-2558-9
23. Ponde V, Gursale A, Chavan D, Johari A, Osazuwa M, Nagdev T. Fascia iliaca compartment block: how far does the local anaesthetic spread and is a real time continuous technique feasible in children? Indian J Anaesthesia. 2019;63(11):932–937. doi:10.4103/ija.IJA_344_19
24. AMH H, Karmakar MK. Combined paravertebral lumbar plexus and parasacral sciatic nerve block for reduction of Hip fracture in a patient with severe aortic stenosis. Can J Anesth. 2002;49(9):946–950. doi:10.1007/BF03016880
25. Asao Y, Higuchi T, Tsubaki N, Shimoda Y.Combined paravertebral lumbar plexus and parasacral sciatic nerve block for reduction of hip fracture in four patients with severe heart failure. Masui. 2005;54(6):648–652.
26. Gupta N, Panwar V, Mishra S. Total spinal anaesthesia: a rare complication of psoas compartment block. Turk J Anaesthesiol Reanim. 2021;49(2):163–165. doi:10.5152/TJAR.2020.26918.
27. Chia N, Low TC, Poon KH.Peripheral nerve blocks for lower limb surgery--a choice anaesthetic technique for patients with a recent myocardial infarction? Singapore Med J. 2002;43(11):583–586.
28. Rizzo D, Giustiniano E, Pellicori D, Misiti CM, Cosco G. meniscectomy in a patient with eisenmenger's syndrome. Minerva Anestesiol. 1999;65(10):733–736. [Case report]]. doi:10.1213/ane.0b013e31818fc252
29. Terkawi AS, Mavridis D, Sessler DI, et al. Pain management modalities after total knee arthroplasty: a network meta-analysis of 170 randomized controlled trials. Anesthesiology. 2017;126(5):923–937. doi:10.1097/ALN.0000000000001607.
30. Taha AM, Darwich N. SOFT block (Sciatic, Obturator and Femoral nerve block Technique): a single-puncture, sole anesthetic for knee surgery. CanJ Anesth/J Can Anesth. 2017;64(12):1279–1281. doi:10.1007/s12630-017-0947-4
31. Chandran R, Beh ZY, Tsai FC, Kuruppu SD, Lim J. Lim JY: peripheral nerve blocks for above knee amputation in high-risk patients. J Anaesthesiol Clin Pharmacol. 2018;34(4):458–64. 10.4103/joacp.JOACP_346_17. doi:10.4103/joacp.JOACP_346_17
32. Kujak M, Pomerantz LH, Petrovic M. Regional technique provides complete surgical anesthesia for above-the-knee amputation: a viable alternative to general endotracheal anesthesia in a time of COVID-19. Cureus. 2022;14(5):e25364. doi:10.7759/cureus.25364
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.