Back to Journals » International Journal of General Medicine » Volume 18
The Global Immune-Nutrition Inflammation Index for Predicting Coronary Slow Flow Phenomenon in Patients with Angina and No Obstructive Coronary Arteries
Authors Guo J, Xiang ZZ, Ma DD
Received 30 January 2025
Accepted for publication 26 February 2025
Published 7 March 2025 Volume 2025:18 Pages 1325—1332
DOI https://doi.org/10.2147/IJGM.S516108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jiang Guo,1 Zhi-zhen Xiang,1 Dan-dan Ma2
1Department of Cardiovascular Medicine, Longquan People’s Hospital Affiliated to Lishui University, Lishui, People’s Republic of China; 2Department of Intensive Care Unit, Shenzhen Luohu Hospital Group Luohu People’s Hospital (The Third Affiliated Hospital of Shenzhen University), Shenzhen, People’s Republic of China
Correspondence: Dan-dan Ma, Email [email protected]
Background: Chronic inflammatory responses are involved in the initiation and development of the coronary slow flow phenomenon (CSFP). However, as a newly developed immuno-nutritional inflammation indicator, the global immune-nutrition inflammation index (GINI) has not been well elaborated for predicting CSFP in patients with angina and no obstructive coronary arteries (ANOCA).
Methods: A total of 1422 individuals with ANOCA were consecutively included in this study, of whom 93 developed CSFP (CSFP group). We selected 186 (1:2 matched) age- and sex-matched patients with ANOCA and angiographically proven normal coronary blood flow as the controls (the control group). Multivariate logistic regression analysis was used to investigate predictors of CSFP in patients with ANOCA. The optimal cutoff values for GINI were calculated.
Results: In total, 93 patients developed CSFP, including 29% (27) in one vessel, 28% (26) in two vessels, and 43% (40) in three vessels. Patients with CSFP had an elevated CRP level, white blood cell (WBC) count, neutrophil count, GINI, fasting blood glucose (FBG) level, and a lower lymphocyte count (P< 0.05). Multivariate logistic analysis showed that the GINI and FBG levels were independent predictors of CSFP in patients with ANOCA. Moreover, we found that the more vessels affected by CSFP, the higher the GINI level. The receiver operating characteristic (ROC) showed that GINI had a better predictive value than indicators alone. When the GINI AISI was > 84.1, the sensitivity and specificity were 88.2% and 58.7%, respectively [The Area Under the ROC curve (AUC): 0.774; 95% CI: 0.721– 0.827; P < 0.001].
Conclusion: Elevated GINI is a reliable predictor of CSFP in patients with ANOCA. Moreover, GINI had a superior predictive value compared to the indicators alone. As a newly developed inflammatory indicator, GINI can be used for further risk stratification of patients with ANOCA.
Keywords: global immune-nutrition inflammation index, coronary slow flow phenomenon, angina no obstructive coronary arteries, predictors
Introduction
The coronary slow flow phenomenon (CSFP) was first discovered by Tambe et al in 1972 and is characterized by delayed coronary blood flow in the absence of obstructive coronary artery disease (CAD).1 With the widespread use of coronary angiography (CAG), CSFP is common in clinical practice. According to literature, the incidence of CSFP varies from 1% to 7%.2 In fact, CSFP is not the only angiographic finding proven to have clinical significance. The international standardization of diagnostic criteria for microvascular angina suggested CSFP as a subtype of microvascular angina (MVA).3 It has been suggested that CSFP is associated with recurrent chest pain, arrhythmias, and adverse cardiovascular outcomes.4,5 Evidences suggested that inflammation, endothelial dysfunction, oxidative stress, or microvascular dysfunction may participate in the initiation and development of CSFP;6 however, the exact pathogenesis of CSFP remains undetermined. Nonetheless, it has been suggested that chronic local or systemic inflammatory reactions play a key role in the occurrence and development of CSFP.7–10
The global immune-nutrition inflammation index (GINI) is a newly developed indicator that combines blood biochemistry and blood routine components and can comprehensively assess the status of immunity, inflammation, and nutrition.11 As an easily acquired indicator in routine clinical practice, GINI has been suggested as a prognostic predictor in patients, with stage IIIC non-small cell lung cancer receiving definitive concurrent chemo-RT.11 Topkan et al also discovered that an elevated GINI value is closely related to a poor prognosis in patients, with glioblastoma multiforme undergoing the standard Stupp protocol.12 GINI has also been suggested as a valuable predictor of survival outcomes in grade 4 adult-type diffuse gliomas.13 Since immune-nutrition-inflammation also plays a key role in the initiation and development of CSFP, we speculated that the newly developed indicator may be a reliable tool for predicting the presence of CSFP in ANOCA patients. Hence, the present study aimed to investigate the association between GINI and CSFP in patients with ANOCA, which could be helpful for risk stratification and optimal management of these specific populations.
Methods
Study Population
This study was conducted between May 2019 and May 2024. The flowchart of the study is shown in Figure 1. The clinical and angiographic characteristics of 1422 individuals with ANOCA were recorded and analyzed. In total, 93 patients were diagnosed with CSFP (CSFP group). We selected two age and sex-matched patients from each of the 93 individuals. If there were more than 2, we used a simple random sampling method to select controls (n=186). The exclusion criteria are shown in Figure 1. This study was approved by the ethics committee of Luohu People’s Hospital and consent was obtained from all participants. This study was conducted in compliance with the Declaration of Helsinki. All patients informed consent before participation.
 |
Figure 1 The study flowchart. |
Coronary Angiography
All the patients received Judkins coronary angiography (CAG), and the Thrombolysis in Myocardial Infarction (TIMI) frame count (TFC) was used to assess the coronary blood flow.14 The first frame was determined when the contrast medium filled 70% of the proximal coronary vessel. The last frame was obtained when the contrast reached the mustache area for the left anterior descending artery (LAD), distal bifurcation of the longest bifurcation segment for the left circumflex artery (LCX), and first branch of the posterolateral artery for the right coronary artery (RCA).14 The TFC of LAD was divided by 1.7 to acquire the corrected TFC (cTFC) for the LAD.14 The cut-off value of TFC for the diagnosis of CSFP was 36.2±2.6 for the LAD (21.1±1.5 cTFC), 22.2±4.1 for the LCX, and 20.4±3.1 for the RCA.14 The mean TFC (mTFC) was calculated by dividing the sum of the TFC of the three coronary arteries by three.2,7–10
Laboratory Measurements
Blood samples were obtained from the antecubital area after overnight fasting on admission, before CAG. Blood routine, biochemical, and lipid indicators were tested in the central laboratory before CAG. The testing of CRP was carried out using the Abbott Architect c8000 Biochemistry Autoanalyzer, while blood cell counts were determined using the RUBY CELL-DYN Ruby version 2.2. The GINI was calculated as [(C-reactive protein×Monocytes×Platelets×Neutrophils)÷(Albumin×Lymphocytes)].11
Statistical Analysis
Categorical variables are presented as percentages and compared using the chi-square or Fisher’s exact test. Continuous variables are shown as the mean±standard deviation and were compared using t-tests. Multivariate regression analyses were used to explore the independent predictors of CSFP. The baseline indicators (p <0.1) were included in the univariate analysis, and parameters with p <0.05 were then added to the multivariate logistic regression analysis to determine the independent predictors of CSFP. Receiver operating characteristic (ROC) curve analysis was performed to assess the predictive value of the indicators for CSFP and to determine the cut-off value of GINI for the diagnosis of CSFP. The 2-sided P <0.05 was considered statistically significant.
Results
Baseline and Clinical Characteristics
Among 1381 individuals (excluding 41 patients), the incidence of CSFP was 6.73%. The demographic and clinical characteristics of patients are shown in Table 1. Although patients in the CSFP group had a higher prevalence of current smoking, hypertension, and diabetes mellitus, no significant difference was found between the two groups (p>0.05) (Table 1). Other demographic characteristics, including age, sex, and BMI, were also comparable between the two groups (p>0.05) (Table 1). The medication history before admission was also similar between the two groups (p>0.05) (Table 1).
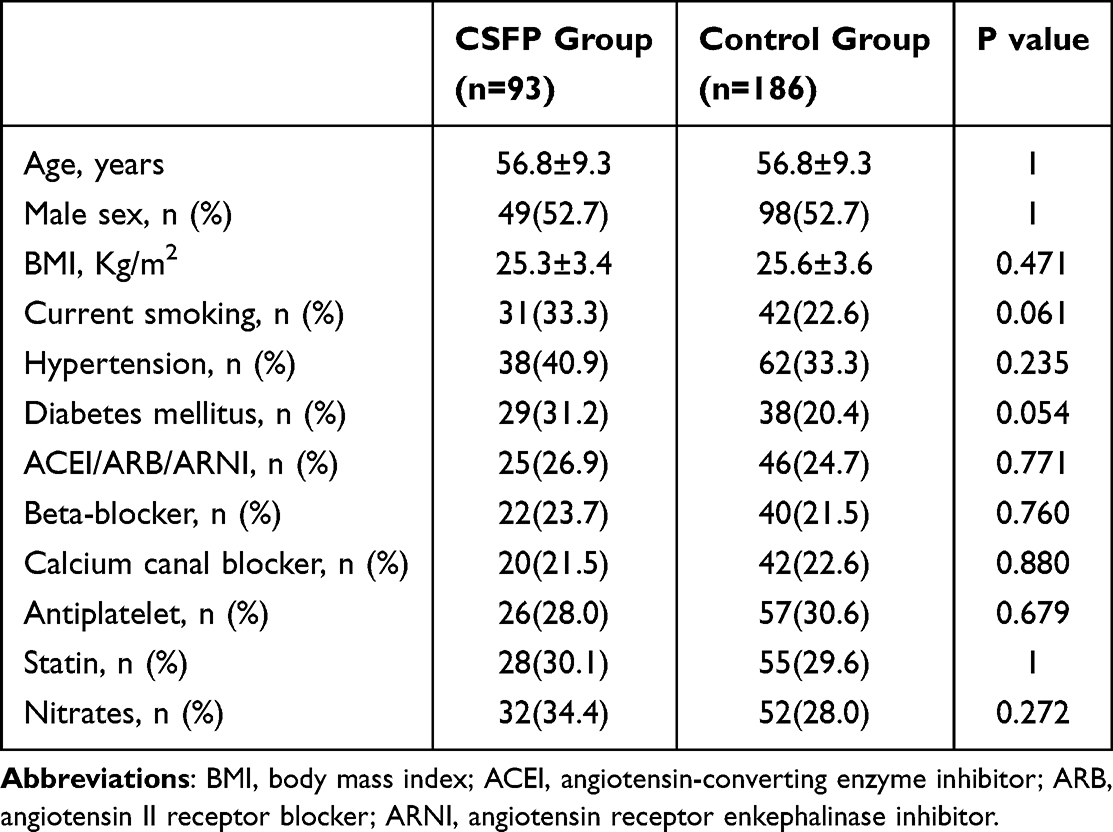 |
Table 1 Baseline Characteristics and Medication of the Two Groups |
Laboratory Parameters of the Two Groups
The comparison of laboratory parameters is displayed in Table 2. Patients with CSFP had an elevated CRP level, white blood cell (WBC) count, neutrophil count, GINI, fasting blood glucose (FBG) level, and a lower lymphocyte count (P<0.05). Other indicators including monocyte count, platelets count, Cr, uric acid, ALB, total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) showed no statistically significant differences (p>0.05) (Table 2).
 |
Table 2 Laboratory Parameters of the Two Groups |
Angiographic Findings of the Two Groups
The comparison of angiographic findings is presented in Table 3. In total, 93 patients developed CSFP: 29% (27) in one vessel, 28% (26) in two vessels, and 43% (40) in three vessels (Table 2). From the aspect of arteries affected, the most frequently affected was the RCA (Table 3). The TFCs in the CSFP group were significantly higher than those in the controls (p < 0.05) (Table 3).
 |
Table 3 Angiographic Findings of the Two Groups |
Predictors of CSFP
Univariate logistic regression analysis showed that GINI and FBG levels were associated with CSFP and were added to the multivariate logistic analysis to investigate the independent predictors for the occurrence of CSFP. We discovered that the GINI and FBG levels were independent predictors of CSFP in patients with ANOCA (Table 4). Moreover, we found that the more vessels affected by CSFP, the higher the GINI level (Figure 2). The ROC curve showed that GINI had a better predictive value than indicators alone (Table 5). When the GINI was >84.1, the sensitivity and specificity were 88.2% and 58.7%, respectively (P < 0.001) (Figure 3).
 |
Table 4 Univariate and Multivariate Logistic Regression Analysis for Presence of SCFP |
 |
Table 5 ROC Analysis of the Elevated Parameters |
 |
Figure 2 Correlation between the number of vessels affected by CSFP and GINI. |
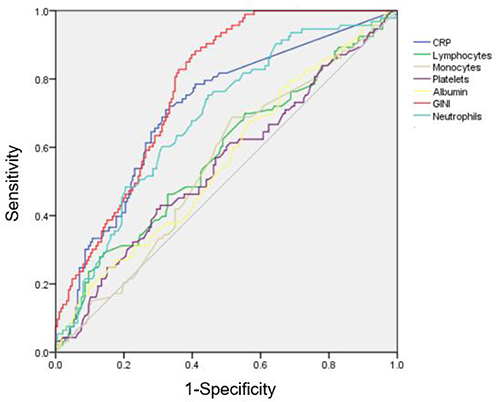 |
Figure 3 ROC curve showing the predicting value of risk factors for the presence of CSFP. |
Discussion
Our study revealed that the GINI and FBG levels were independent predictors of CSFP in patients with ANOCA. In addition, we found that GINI had a higher predictive value than the indicators alone. Moreover, the GINI increased as the number of arteries involved in CSFP increased. The GINI is a reliable indicator of risk assessment and a potential intervention target for CSFP in ANOCA.
ANOCA has been suggested as a common clinical entity. Nearly half of patients suspected of having coronary artery disease (CAD) undergoing CAG were found to have normal coronary arteries,15 which presents great challenges for the clinical management of these patients. They have unique and diverse pathogenesis. Moreover, ANOCA is quite different from the traditional atherosclerotic disease, which requires a new diagnostic method and new treatment strategies. Nonetheless, coronary microvascular disorders are the primary pathogenesis of ANOCA.15 Therefore, coronary function testing (CFT) is important for diagnosis and subtype determination.15 However, in clinical practice, CFT is difficult to perform in all ANOCA patients. Therefore, exploring alternative indicators for assessing ANOCA is of clinical significance. The international standardization of diagnostic criteria for microvascular angina suggested CSFP as a subtype of microvascular angina (MVA).3 Therefore, the coronary blood flow can be used to assess microvascular function in clinical practice. Investigating the predictors of CSFP could help us to understand the possible pathogenesis of ANOCA.
As early as 1972, angiographic findings of CSFP have been reported by Tambe et al.1 However, in the academic background of that time, CSFP was only recognized as an angiographic finding, and its clinical significance was not determined. However, with the rapid development of interventional cardiology, especially intracoronary function testing, the importance of CSFP has gradually been recognized. Reportedly, 20% of patients with CSFP experience recurrent chest pain resembling acute coronary syndrome.8–10 Moreover, in some cases, CSFP is associated with sudden cardiac death4 or the presence of ST-segment elevation myocardial infarction (STEMI).5 Therefore, investigation of potential risk factors is essential for the management of these patients.
Although the pathogenesis of CSFP remains unclear, chronic inflammatory reactions play a fundamental role in the initiation and development of CSFP. As a well-established parameter for assessing inflammation, C-reactive protein (CRP) level has been suggested as a reliable risk factor for CSFP.16 Moreover, in recent years, combined indicators from routine blood tests to assess the degree of inflammatory reaction, such as the neutrophil-to-lymphocyte ratio (NLR),7 systemic immune-inflammation index (SII) (NLR×total preoperative peripheral platelet count),7 systemic inflammation response index (SIRI) (neutrophil count×monocyte count/lymphocyte count),9 platelet-to-lymphocyte ratio,17 and Pan-Immune-Inflammation Value (neutrophil count×platelet count×monocyte count/lymphocyte count)18 have also been demonstrated to be associated with the presence of CSFP. Moreover, the most abundant protein in human plasma, albumin, together with its derivative parameters, such as the plasma fibrinogen-to-albumin ratio,10 plasma uric acid-to-albumin ratio,2 and neutrophil percentage-to-albumin ratio,8 have also been demonstrated as independent predictors of CSFP. The GINI combined indicators associated with CSFP, such as CRP, neutrophil count, platelet count, monocyte count, lymphocyte count, and albumin, so we suggest that the GINI may provide a better predictive value than the indicators alone. Therefore, we aimed to explore the association between GINI and CSFP in ANOCA patients.
As a newly developed indicator, GINI combines blood routine, CRP, and albumin, which can comprehensively reflect the immunological, inflammatory, and nutritional status of patients. However, the pathogenesis of CSFP and the close relationship between GINI and CSFP in patients still remain undetermined. GINI participated in initiation and development in various ways. We suggest that it is more reasonable and logical to interpret these results based on biochemical or cellular parameters separately. GINI can be presented as the CRP-to-albumin ratio (CAR)×PIV, CAR×SIRI×total preoperative peripheral platelet count, or CAR×SII×monocyte count. Recently, an association between the SII, SIRI, PIV, and CSFP has been reported. These indicators are calculated using three or more markers, and have been suggested as valuable predictors of CSFP. In a study performed by Wang et al that included 89 patients with CSFP and 167 normal controls with chest pain and normal coronaries, it was suggested that SII was an independent predictor of CSFP occurrence.7 Subsequently, Kaplangoray et al suggested in a retrospective study that PIV showed a superior predictive value for CSFP than NLR, PLR, and SII and could serve as a valuable and independent predictor of CSFP.18 A more recent study by Prof Wang included 1422 patients with ischemia and no obstructive coronary arteries (INOCA), of whom 89 were diagnosed with CSFP. They discovered that patients with CSFP had an elevated SIRI, which could improve the predictive value of CSFP compared with neutrophils, monocytes, and lymphocytes alone.9 These newly developed indices showed a better predictive value than the binary indices, which may be attributed to the more integrated parameters developed and less individualized differences.
As reported in previous studies, nutrition has been suggested as an important parameter in assessing the occurrence, development, and prognosis of various cardiovascular disease. Plasma albumin is the most widely used indicator for assessing the status of human nutrition. Numerous studies have demonstrated the predictive value of albumin level in the presence of CSFP.2,8,10 As a comprehensive indicator, GINI was first developed by Topkan et al,12 and has been demonstrated to be a prognostic indicator of tumor-related diseases.12,13 This study is the first to demonstrate an association between GINI and CSFP, which may provide a valuable and helpful parameter for the identification and management of patients with CSFP. We discovered that a higher GINI was a risk factor and independent predictor of CSFP in patients with ANOCA.
Limitations
This study had some limitations. First, it was a single-center study with a limited sample size. Second, due to the complex pathogenesis and varied indicators for predicting CSFP in the literature, although multivariate analysis was performed, residual confounding remains possible (medication adherence, socioeconomic factors, et al), which may introduce bias. Third, due to the inherent limitations of the retrospective design, `there may bring in a bias in the present study. Moreover, the study establishes associations, not causality, due to its observational design. Fourth, other important parameters for assessing inflammatory status, including IL-6, were not tested in our study. Moreover, whether anti-inflammatory treatment is useful in the management of CSFP remains unclear.
Conclusion
We suggested that higher GINI was a reliable indicator for the prediction of the presence of CSFP in ANOCA patients. GINI is significantly associated with CSFP, and further prospective studies are needed to confirm causality. The GINI is a promising parameter for the identification and management of patients with CSFP.
Data Sharing Statement
The datasets are available from the corresponding author upon reasonable request.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Tambe AA, Demany MA, Zimmerman HA, et al. Angina pectoris and slow flow velocity of dye in coronary arteries--a new angiographic finding. Am Heart J. 1972;84(1):66–71. doi:10.1016/0002-8703(72)90307-9
2. Zhang XJ, Hou AJ, Luan B, et al. Uric acid to albumin ratio as a novel predictor for coronary slow flow phenomenon in patients with chronic coronary syndrome and non-obstructive coronary arteries. BMC Cardiovasc Disord. 2024;24(1):358. doi:10.1186/s12872-024-04040-5
3. Ong P, Camici PG, Beltrame JF, Coronary Vasomotion Disorders International Study Group (COVADIS), et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol. 250;2018:16–20. doi:10.1016/j.ijcard.2017.08.068
4. Saya S, Hennebry TA, Lozano P, et al. Coronary slow flow phenomenon and risk for sudden cardiac death due to ventricular arrhythmias: a case report and review of literature. Clin Cardiol. 2008;31(8):352–355. doi:10.1002/clc.20266
5. Sen T. Coronary slow flow phenomenon leads to ST elevation myocardial infarction. Korean Circ J. 2013;43(3):196–198. doi:10.4070/kcj.2013.43.3.196
6. Wang X, Nie SP. The coronary slow flow phenomenon: characteristics, mechanisms and implications. Cardiovasc Diagn Ther. 2011;1(1):37–43. doi:10.3978/j.issn.2223-3652.2011.10.01
7. Dai XT, Kong TZ, Zhang XJ, et al. Relationship between increased systemic immune-inflammation index and coronary slow flow phenomenon. BMC Cardiovasc Disord. 2022;22(1):362. doi:10.1186/s12872-022-02798-0
8. Zang SW, Long JJ, Wang Y. Neutrophil percentage to albumin ratio as a predictor for coronary slow flow phenomenon in patients with myocardial ischemia with no obstructive coronary arteries. Int J Gen Med. 2024;17:3511–3519. doi:10.2147/IJGM.S477431
9. Chen YD, Wen ZG, Long JJ, et al. Association between systemic inflammation response index and slow coronary flow phenomenon in patients with ischemia and no obstructive coronary arteries. Int J Gen Med. 2024;17:4045–4053. doi:10.2147/IJGM.S481538
10. Yang SB, Cui Y, Hou JJ, et al. Assessment of the relationship between plasma fibrinogen-to-albumin ratio and slow coronary flow phenomenon in patients without obstructive coronary artery disease. BMC Cardiovasc Disord. 2023;23(1):540. doi:10.1186/s12872-023-03579-z
11. Topkan E, Selek U, Pehlivan B, et al. The prognostic value of the novel global immune-nutrition-inflammation index (GINI) in stage IIIC non-small cell lung cancer patients treated with concurrent chemoradiotherapy. Cancers. 2023;15(18):4512. doi:10.3390/cancers15184512
12. Topkan E, Kilic Durankus N, Senyurek S, et al. The global immune-nutrition-inflammation index (GINI) as a robust prognostic factor in glioblastoma patients treated with the standard stupp protocol. Int J Immunopathol Pharmacol. 2024;38:3946320241284089. doi:10.1177/03946320241284089
13. Aydin AA, Yuceer RO. Unraveling the predictive value of the novel global immune-nutrition-inflammation index (GINI) on survival outcomes in patients with grade 4 adult-type diffuse gliomas. Curr Oncol. 2024;31(9):5027–5039. doi:10.3390/curroncol31090372
14. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93(5):879–888. doi:10.1161/01.CIR.93.5.879
15. Microvascular Network (MVN), Samuels BA, Shah SM, Widmer RJ, et al. Comprehensive management of ANOCA, part 1-definition, patient population, and diagnosis: JACC state-of-the-art review. J Am Coll Cardiol. 2023;82(12):1245–1263. doi:10.1016/j.jacc.2023.06.043.
16. Wen ZG, Long JJ, Wang Y. Association between inflammatory burden index and coronary slow flow phenomenon in patients with chest pain and no obstructive coronary arteries. BMC Cardiovasc Disord. 2024;24(1):595. doi:10.1186/s12872-024-04281-4
17. Oylumlu M, Doğan A, Oylumlu M, et al. Relationship between platelet-to-lymphocyte ratio and coronary slow flow. Anatol J Cardiol. 2015;15(5):391–395. doi:10.5152/akd.2014.5376
18. Kaplangoray M, Toprak K, Deveci E, et al. Could pan-immune-inflammation value be a marker for the diagnosis of coronary slow flow phenomenon? Cardiovasc Toxicol. 2024;24(5):519–526. doi:10.1007/s12012-024-09855-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil Percentage to Albumin Ratio as a Predictor for Coronary Slow Flow Phenomenon in Patients with Myocardial Ischemia with No Obstructive Coronary Arteries
Zang SW, Long JJ, Wang Y
International Journal of General Medicine 2024, 17:3511-3519
Published Date: 14 August 2024