Back to Journals » Psychology Research and Behavior Management » Volume 12
The General Population’s View on Where to Seek Treatment for Gambling Disorder – a General Population Survey
Authors Håkansson A ![]() , Ford M
, Ford M ![]()
Received 15 August 2019
Accepted for publication 25 October 2019
Published 19 December 2019 Volume 2019:12 Pages 1137—1146
DOI https://doi.org/10.2147/PRBM.S226982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Anders Håkansson,1 Madison Ford1,2
1Faculty of Medicine, Department of Clinical Sciences Lund, Psychiatry, Lund University, Lund, Sweden; 2McGill Group for Suicide Studies, McGill University, Montreal, QC, Canada
Correspondence: Anders Håkansson
Lund University, Malmö Addiction Center, Södra Förstadsgatan 35, Plan 4, Malmö S-205 02, Sweden
Tel +46 703 135677
Email [email protected]
Background: More remains to be understood about attitudes towards treatment for gambling disorder and where to seek treatment. Given the low degree of treatment seeking behaviour in this condition, it may be of interest to study people’s perception about where to seek help in case of problem gambling. From a study originally aiming to address health correlates of problem gambling, the present sub-study aimed to examine the general population’s attitudes towards where to advise a person with problem gambling to seek treatment, and correlates of recommending a formal professional treatment modality.
Methods: A cross-sectional general population web survey in Sweden (N=2,038, 55% women, 6% lifetime problem gamblers) was conducted. Preferred advice for gambling-related treatment seeking was defined with a question asking about where one would hypothetically advise a friend to seek help for gambling addiction. Advice for professional vs peer support help was compared with respect to individual characteristics, in problem gamblers and non-problem gamblers.
Results: Fifty percent preferred to recommend peer support help for gambling, whereas among professional treatment options, the largest share preferred primary care (22%) or psychiatry/addiction psychiatry (18%), while few suggested occupational health-care (6%) or social services (3%). Opting for a professional treatment modality for problem gambling was unrelated to one’s own problem gambling, whereas those recommending professional treatment were younger and more likely to report psychological distress. In problem gamblers specifically, history of indebtedness was associated with recommending professional treatment.
Conclusion: Many people may not perceive gambling disorder to require professional treatment, and may recommend peer support outside of formal treatment systems. Younger individuals, as well as those with a personal history of psychological treatment needs, may be more prone to recommending formal treatment. The findings may have implications for treatment trajectories and may facilitate overcoming perceived treatment barriers.
Keywords: gambling disorder, problem gambling, treatment seeking, barriers, attitudes
Background
Gambling disorder is an addictive disorder known to be associated with a high degree of severe financial consequences, psychological suffering, and increased risk of suicide.1 Problem gambling is known to have a past-year prevalence of 2.3 percent of the population across countries, with past-year prevalence rates ranging from 0.5 to 7.6 percent.2 The reported population prevalence of the actual diagnosis is approximately 0.5 percent. Despite severe consequences, many individuals suffering from a gambling disorder have been reported to abstain from seeking treatment. Previous literature has focused on barriers to treatment perceived by gamblers,3–5 and many people with a gambling disorder may receive treatment for comorbid psychiatric conditions instead of the actual gambling condition.6
It is also known that the way problem gamblers seek help may differ markedly from each other, and that help-seeking for problem gambling may take place in several different settings. It is important to note that help-seeking has been shown to involve different types of contact, not typically perceived as professional treatment.7 Consequently, treatment options for a gambling disorder include both professional interventions within formal treatment systems, as well as peer support interventions.8,9 While formal treatment seeking is low, it also has been reported that self-recovery without peer support or formal treatment may be relatively common, indicating that the natural course in gambling disorder may be variable.10 Apart from structured gambling treatment offered by professional treatment providers, peer support organizations have played a significant role in providing support for people seeking help for a gambling disorder. This includes the widespread concept of the twelve-step-oriented Gamblers Anonymous (GA) movement.11,12 In the present setting, these peer support interventions are typically provided as group therapy, although face-to-face interventions also occur. A non-ideological organization (‘Society of Gambling Addicts'), separated from the twelve-step movement, provides peer support in the group or individual format, but shares the characteristics of the GA groups as providing non-formal support rather than formal treatment.13
The widening of treatment options for problem gambling may include the health care system outside specialized addiction psychiatry treatment. Although primary care traditionally may not be seen as a likely arena for gambling disorder treatment, it has been suggested that general practitioner facilities may serve as a viable option for patients suffering from this condition.14 It has also been suggested that this setting may be appropriate for both screening and treatment for problem gambling.15–17 Also, in some settings, psycho-therapeutic interventions for gambling disorder – and for other addictive conditions – in many cases are provided by the social services, rather than within the mental health sector. One example is the setting where the present study was conducted, Sweden, where the responsibility for therapeutic treatment for the present condition is divided between social services and the medical system.18,19
Thus, there is a remaining research gap with respect to how trajectories from problem gambling to an actual treatment intervention can be facilitated. Furthermore, barriers to existing treatment for gambling disorder are only partially understood. Therefore, in a general population survey originally addressing gambling behaviours and a number of potentially gambling-related health issues, the present study aimed to examine how the idea of seeking help for problem gambling is understood by the general population. This was expressed as the type of help an individual would hypothetically recommend to a friend experiencing problem gambling. Also, the study aimed to examine potential differences in characteristics of individuals recommending a professional treatment intervention, as compared to those favouring the advice to seek non-professional peer support.
Methods
Study Procedure
The present study was designed as a web survey, aiming to address a sample derived from the general population and with a representative distribution across gender and age groups. Respondents were recruited through an existing database of potential respondents belonging to the web panel of the market survey company Userneeds, a company operating in several European countries, and which recruits web panel members for market surveys and similar assessments (https://userneeds.com/en/). The same type of web panel recruitment previously has been used for other research related to gambling.20 Here, data was collected during seven days in April, 2019.
The study was approved by the ethics board of Sweden (file number 2019/01830). Informed consent was provided electronically, such that after recruitment and information about the study, a web panel participant was able to enter the survey online in case of providing informed consent.
Setting
The survey was carried out in Sweden, a country where formal responsibilities for the provision of gambling disorder treatment was formalized in new legislation commencing January 1, 2018. It was established that both the health-care system of the regions, as well as the social services of the municipalities, are responsible for the assessment and treatment of this condition, making the provision of gambling disorder treatment regulated in the same way as for substance use disorders. For addiction treatment overall, the split responsibility between health care and social services, organizationally separate, is well established in the present setting, although debated. Apart from interventions related only to practical social support, provided by the social services, and pharmaceutical treatment, provided exclusively by the health care sector, several treatment interventions can be provided by either the health care system or the social services, or both.18 Social services, i.e. the social authorities of the town/municipality, provide services which may include the provision of formal psychological or psycho-social treatment or referral to such treatment, or more informal support.18 Psychiatry/addiction treatment refers to specialized medical interventions in these disciplines,21 in contrast to the primary care system (general practitioner system) responsible for a wide range of mainly physical conditions but also psychiatric and addictive disorders typically perceived as less severe than those treated in specialized units. Primary care, however, has been highlighted as a setting for screening and treatment of addictive disorders, including problem gambling.22 Occupational health care in the present settings refers to primary care but provided specifically by units linked to the work place. For all treatment options, addiction treatment in the present setting is typically provided as face-to-face treatment, either individually or in a group format. Several types of psycho-therapeutic interventions could theoretically be provided either by social services or by any of the health care options, depending on local conditions.18 Conversely, within the health care sector, addiction/psychiatry can be considered a setting typically reserved for more severe conditions than the primary care or occupational health care systems.
The overall treatment uptake in Sweden for gambling disorder has been low, likely due to the lack of formal regulations of treatment for this condition prior to January, 2018. Where professional treatment has been provided, it mainly has involved cognitive-behavioural treatment,21 and clinical research in the setting has involved motivational and cognitive-behavioural interventions provided face to face23 or online.24 Aside from the formal treatment system, Sweden has a number of peer support groups, including both a GA movement and other peer support organizations. Also, a national free-of-charge helpline for problem gambling has been available during the last decade, providing brief advice to problem gamblers and their concerned significant others, and information about where treatment can be applied for.19
Participants
The present study was conducted as an online survey addressing participants of the web panel of a market survey company, with the intention to reach a sample of around 2000 people with a distribution of gender and age groups corresponding to the general population. The recruitment of new respondents was halted when the total number of complete answers was around 2,000. A total of 2,045 individuals completed the survey and were included in the study (55 percent women, 45 percent men, and another three respondents identified as transgender, another three individuals preferred not to report their gender). Seven responses were suspected to represent a second submission by the same individual, and were therefore excluded from the analyses, rendering a total sample of 2,038 individuals. Six percent fulfilled the criteria of a lifetime history of problem gambling, and seven percent reported a lifetime history of subjective indebtedness. Twenty-seven percent reported a history of ever having been prescribed a medical or psychological treatment from a physician due to psychological distress.
Measures
In addition to questions addressing a number of potential correlates of problem gambling (data not presented here), a separate aim was to assess respondents’ attitudes to gambling disorder treatment. This was addressed with the following item: “If a friend of yours were to develop an addiction to gambling, where would you primarily advise that person to seek help for the gambling addiction?”. Possible answers to choose from were the following: “an independent patients organization/peer support organization (such as Gamblers Anonymous, which corresponds to Alcoholics Anonymous, AA, for alcohol)”; “primary care” (expressed with the common Swedish wording for a GP’s facility); “occupational health care”; “social services of the municipality/town”; or “psychiatry or addiction health care in the health care system”. The question was designed in order to correspond – as closely as possible – to a previous study from the same geographical setting, addressing the corresponding research question for alcohol instead of gambling.25
Although the present paper does not address individuals’ own treatment-seeking, co-variates were chosen among variables known to be associated with treatment seeking for problem gambling. The respondents’ own degree of problem gambling, or absence thereof, was measured using the NODS-CLiP, an established three-item instrument for the screening for problem gambling, and where the endorsing of at least one item was defined as problem gambling.26 Age and gender have been reported to correlate with treatment seeking, where treatment seekers have been reported to be older and less likely to be female.27,28 In addition, amounts of gambling-related debts and financial difficulties have been reported to predict treatment attendance, as greater gambling debt and gambling-related financial difficulties have been reported to be positively related to treatment initiation.27,29 Additionally, alcohol use has been reported to be negatively associated with treatment seeking for problem gambling.28
The survey included a screening for problematic alcohol use, using the AUDIT-C,30 as well as questions about a history of past-year illicit drug use. Respondents’ own history of other treatment-seeking was addressed with questions about whether the individual had ever sought treatment for psychological distress and whether a physician had ever prescribed treatment (psychological or pharmaceutical) for psychological distress (i.e. not specifically for gambling or any other addictive disorder). Financial situation was assessed through questions about monthly income, and about a history of ever having experienced indebtedness. Among potential definitions of indebtedness, the subjective definition was chosen,31 in order to assess mainly the individual’s own impression of having been in financial difficulties (having been unable to fulfil financial duties).
Statistical Methods
Results were reported as a description of the distribution of answers related to the advice given to a potential friend with a gambling problem. Also, statistical comparisons were made for a number of potential correlates, between those recommending a non-professional, peer support intervention, and those recommending a professional institution for treatment-seeking. These comparisons were made using chi-squared tests. Variables demonstrating a significant association with professional treatment advice were entered in a logistic regression model. Prior to this, variables were examined with respect to possible intercollinearity.
Results
A total of 50 percent of respondents reported that they would primarily advise seeking help in an independent peer-support group, and among those reporting any of the professional treatment modalities, a large majority endorsed the options involving health-care, specifically primary care and psychiatry/addiction medicine. Only three percent reported that they would primarily advise seeking treatment in social authorities (Table 1). In the analysis of only individuals who endorsed criteria of problem gambling, the responses differed little from the overall picture. In this sub-group 47 percent chose the peer-support option, whereas the remaining 53 percent chose any of the professional treatment modalities (Table 1).
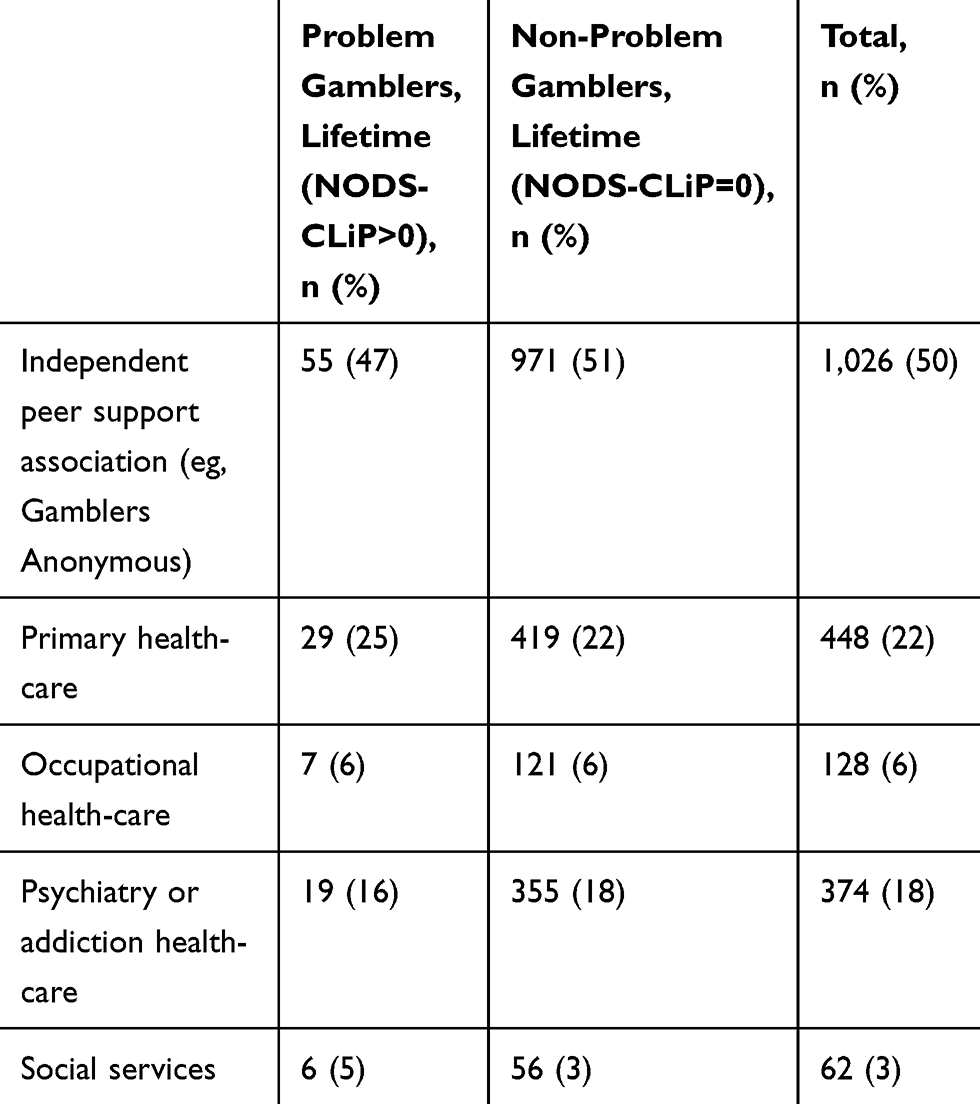 |
Table 1 Advice for Treatment-Seeking, All Respondents (N=2038) |
Whether or not an individual chose one of the professional treatment options was unrelated to the individual’s own problem gambling, indebtedness, past-year illicit drug use, or level of alcohol consumption, gender or income. Those endorsing one of the professional treatment options were, however, significantly younger and significantly more likely to report a history of requiring treatment for psychological distress, and significantly more likely to report having been prescribed such treatment from a physician (Table 2).
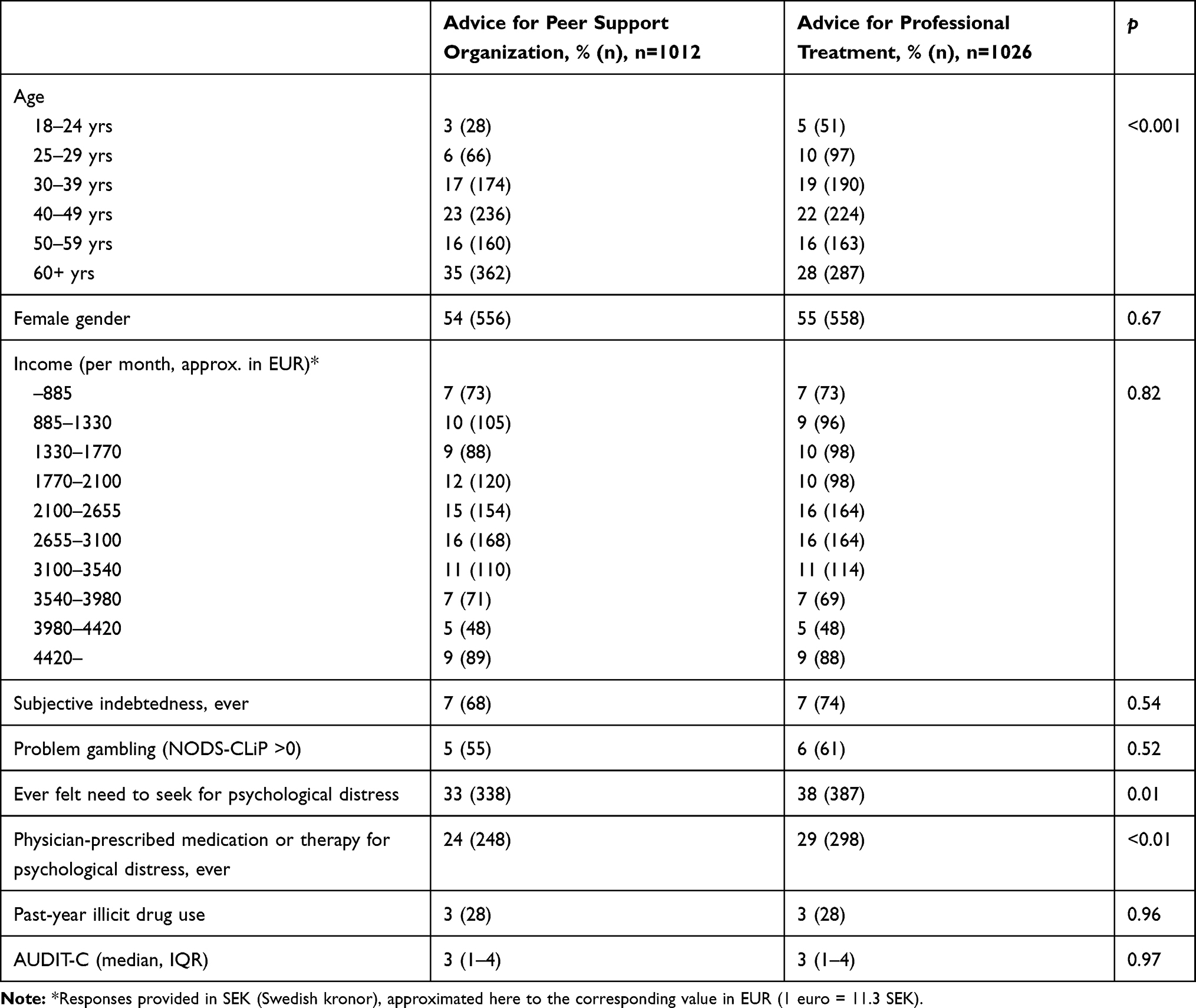 |
Table 2 Characteristics of Respondents Recommending a Professional Treatment Option vs a Peer Support Group. Chi-Squared Tests and Mann–Whitney Test. (N=2038) |
Due to a high correlation between the variables describing a need to seek treatment for psychological distress and a history of being prescribed treatment (r = 0.69), the variable with the strongest association with a professional treatment advice (having been prescribed treatment) was entered in a logistic regression model along with the age variable. Here, having been prescribed treatment remained significantly associated with professional treatment advice (OR 1.23 [1.01–1.50], Wald chi-square [df=1, n=1,012, positive=298, negative=714] = 4.18, p=0.04), as did age (OR 0.88 [0.83–0.94], Wald chi-square [df=1] = 15.86, p <0.001).
Among non-problem gamblers (n=1,922), as in the whole dataset, professional treatment advice was significantly associated with younger age, ever having felt a need to seek treatment for psychological distress, and ever receiving a prescription for treatment for psychological distress. In the logistic regression, professional treatment advice was associated with both age (OR 0.89 [0.84–0.95], Wald chi-square [df=1] = 13.61, p <0.001) and marginally associated with a history of ever receiving a prescription for psychological distress (OR 1.21 [0.99–1.49], Wald chi-square [df = 1, n = 951, positive=271, negative=680] = 3.31, p=0.07).
Among problem gamblers (n=116), professional treatment advice was not significantly associated with age, gender, income, substance use, having felt a need for treatment for psychological distress or having been prescribed such treatment. However, respondents recommending a professional treatment modality were significantly more likely to report a history of lifetime indebtedness (p<0.05). As only one variable was associated with the outcome measure, no logistic regression analysis was carried out (Table 3).
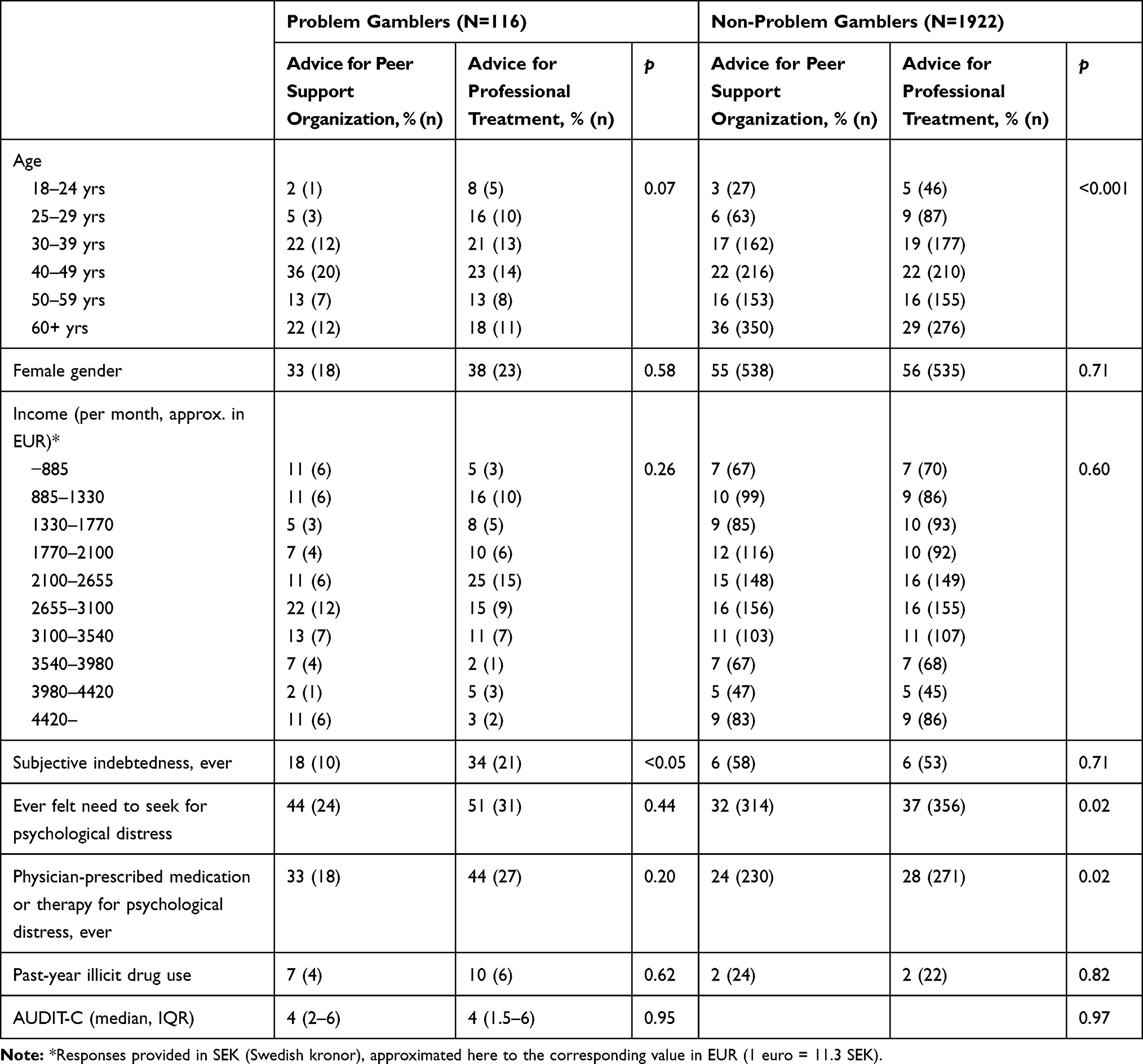 |
Table 3 Characteristics of Respondents Recommending a Professional Treatment Option vs a Peer Support Group. Problem Gamblers and Non-problem gamblers, Respectively |
Discussion
The present study aimed to assess attitudes to treatment seeking for problem gambling in the general population, as this condition is known to be associated with a low degree of treatment-seeking behaviour. A principal finding of the present study was that a very large proportion of the general population primarily reported a non-professional patient organization as the primary treatment option to which they would refer a friend with a hypothetical gambling disorder. Additionally, among professional treatment options, a large majority chose to advise contacting any of the health-care options, rather than the social authorities. Those recommending a professional treatment option were more likely to be people with a history of psychological treatment, and younger individuals. Despite this, another finding is that altogether, few variables described those who gave a professional treatment recommendation. Whether or not individuals have a history of problem gambling themselves may not influence attitudes towards formal treatment seeking, but among problem gamblers, a history of financial difficulties, aimed to describe a higher degree of severity, may make a person more prone to recommend formal treatment rather than peer support.
It has been demonstrated that the general impression of problem gambling in the general population, is that treatment for this condition is necessary. However, somewhat contrary to the findings of the present study, it has been demonstrated that problem gamblers may be less likely to endorse the belief that treatment and total gambling abstinence may be necessary.32 Thus, based on this finding, a difference between problem gamblers and non-problem gamblers in the present dataset would have been expected, but could not be seen here. However, in the present study, respondents were not given the choice to state that treatment for problem gambling is not necessary, as the wording of the question indicated that the advice provided to a problem gambler would be to go somewhere for help. It was possible, however, to choose a type of help outside the professional treatment system, which was the most common response chosen. Thus, in relation to the findings of Cunningham and co-workers, who demonstrated that a large percentage of the general population believed treatment was needed, the findings made here do not necessarily contrast theirs, as turning to a voluntary peer support organization also may be perceived as a treatment-seeking behaviour. Also, the findings of Cunningham and co-workers indicated that a stronger belief about problem gambling as a disease was related to a higher likelihood of believing that structured treatment would be necessary.32 Thus, in the present finding, it cannot be excluded that attitudes to the gambling disorder condition may have affected responses. Those who opted for advising a professional treatment were more likely to have their own treatment experience, although not primarily for the present condition but rather, for any kind of psychological distress. Therefore, having personal treatment experience may be associated with a higher degree of describing problem gambling as a disease.
One of the major findings of the present paper was the relationship between advising professional treatment and a personal history of having perceived psychological distress to a degree where one felt a need to seek treatment, and a history of having received a prescription for either medication or psychotherapy from a physician. Although it is hard to draw conclusions about the factors mediating these associations, it may be reasonable to believe that people with an experience of seeking or receiving treatment may be more prone to accept – and therefore also to provide others with a recommendation for – formal treatment. Interestingly, however, as this question specifically addressed treatment for problem gambling, the advice for formal treatment was unaffected by whether the respondent had an own history of this specific condition, i.e. problem gambling. Here, further study and possibly more in-depth survey techniques may be needed in order to shed light on how the treatment needs for problem gambling are viewed by people with different types of other treatment history. It is possible that an individual who has received treatment for mental health – regardless of whether that was related to gambling or not – may more readily accept the picture of problem gambling as a medical condition, involving a certain degree of comorbidity with other types of mental health problems.33
Although the group of problem gamblers in the sample was smaller, it could be demonstrated that in this group, specifically, those endorsing the professional treatment option were more likely to have a history of indebtedness. Thus, it may be argued that problem gamblers with a higher degree of consequences may be more likely to recommend a treatment option perceived as more institutional, rather than help-seeking outside of this formal system. Indebtedness is known to constitute one of the key consequences of a gambling disorder. Financial difficulties (and prior treatment experience related to gambling) predicted treatment-seeking in help-line callers in a US study,29 which is consistent with the findings of the present study, although this study assesses treatment recommendations rather than one’s own formal treatment-seeking. This is particularly interesting as the history of financial difficulties was not associated with a formal treatment recommendation in the overall study group, but specifically in respondents with a history of problem gambling.
Within the group endorsing one of the professional treatment options, it is of interest that a large majority recommended a health-care-based intervention rather than the social services, despite the study being conducted in a country where social services traditionally represent a very large share of the treatments provided for addictive diseases. It is also notable that health-care based recommendations were the most common choice, as the treatment responsibility for problem gambling is divided between two domains, the healthcare and social services, in the society. Previous research has shown that the choice for different kinds of treatment modalities may be related to the characteristics of the problem described. A US study demonstrated that patients with a gambling disorder were significantly more likely to receive treatment from social workers or psychologists if their condition was their primary diagnosis, and more likely to receive treatment from the medical sector if they had comorbid psychiatric diagnoses.34 More remains to be understood about the reasons why a significant proportion of the general population – including individuals who screen positive for problem gambling – may perceive problem gambling as a condition not primarily in need for a professional intervention and assessment, such as in the medical system. For example, this should be seen in the light of a gambling disorder being associated with high rates of psychiatric comorbidity33 and severe complications including suicide.1 It cannot be excluded that the large proportion of the respondents endorsing the non-professional help-seeking option, outside of the formal treatment system, may reflect a view on gambling disorder as a less serious condition with less severe complications than conditions typically seen in medical treatment systems.
The findings of the present study need to be seen in light of previous data describing the help-seeking process in problem gambling as complex, and involving a large range of potential help-seeking methods.7 Here, in a study addressing the general population, where most respondents do not meet criteria of an own history of problem gambling, we assessed different institutions and peer support settings for potential treatment in an indirect manner, i.e. a number of potential options to which one could advise a friend to seek for a gambling disorder. Given the present design, the more detailed options included by Rodda and co-workers were not applied here. Clearly, further research may need to address both public beliefs and attitudes towards problem gambling treatment, as well as actual help-seeking steps taken by individuals with a gambling problem.
The results of the present study can be compared to the previous study of attitudes to treatment-seeking for alcohol problems in the same setting. In the alcohol study, like in the present one, a non-professional support group was the recommendation chosen by the highest proportion of respondents, in comparison to other treatment modalities such as psychotherapy, pharmacological treatment or residential treatment. Among the treatment modalities recommended, a clear majority chose addiction specialists or psychiatry over primary care or occupational health-care. Similar to the present study, few respondents would recommend a friend or family member to seek alcohol treatment in social services.25 In contrast to the study addressing alcohol, occupational health-care and other types of primary health care were somewhat more commonly recommended for problem gambling than specialized addiction or psychiatric facilities. Although it is difficult to fully establish the reasons for this discrepancy, it cannot be excluded that a gambling disorder is perceived by the general population as a condition less likely to require specialized medical attention, as compared to an alcohol use disorder, thereby favouring medical treatment in a lower level of specialization, rather than the specialized addiction treatment. Also, problem gambling traditionally has not entered the medical sector to a large extent.21
The present study has limitations, particularly caused by the fact that the survey addressed members of a web panel who are more likely to answer online surveys in different disciplines. In the present study, six percent of respondents endorsed the criteria of a lifetime history of problem gambling. This is lower than in previous studies from the same setting where the same instrument has been used, and with the same or a similar type of data collection,35,36 but likely corresponds more closely to the general population prevalence of lifetime problem gambling, reported to be around 3–4 percent in the Swedish general population, although measured with a different instrument.37 Thus, the present study group may be skewed towards a somewhat higher degree of problem gambling and therefore, potentially, it cannot be excluded that individuals participating in a web survey panel, and who accept to participate in a study about gambling, may have other gambling patterns and other beliefs about gambling and gambling treatment than the rest of the general population.
Also, the conclusions drawn from the present study may be limited by the fact that this web survey contained relatively brief items, and for example, the format of the survey makes it difficult to examine the degree of gambling or problem gambling of the respondents, except for the established but brief screening tool used here for lifetime problem gambling. Thus, the current or recent gambling problems of respondents were not assessed. However, as the study addressed beliefs about treatment options, the background of respondents was assessed, such as their history of screening positive for lifetime problem gambling.
Likewise, it should be borne in mind that the respondents’ attitudes and beliefs about where to advise a person to seek treatment may not necessarily translate into how people with an emerging gambling problem may actually choose to seek or not to seek treatment. However, common beliefs about whether gambling disorder is a condition in need of formal treatment and the level of care appropriate are factors which are likely to affect actual treatment-seeking patterns in the society, particularly where concerned significant others are involved in the treatment seeking process. Thus, although the present study does not assess actual help seeking, it may provide insights of importance to the provision of treatment with a high degree of availability and acceptability to the general population. Further research may need to examine how public attitudes to gambling and problem gambling treatment translate into actual treatment-seeking in individuals with a gambling problem. Also, beyond the purpose of the present study, research into the acceptability and patient satisfaction in different treatment modalities is likely to be key to the overall treatment success in gambling disorder.
Conclusions
Based on the assumption that the attitude of the general population towards treatment for a condition may affect treatment-seeking behaviour for that condition, the present study demonstrated that a large proportion of the general population would not recommend a professional treatment modality for problem gambling, but rather would prefer to recommend a peer support group. The view on seeking professional treatment was more favourable in younger people and in those having a history of receiving a prescription of some treatment for any kind of psychological distress. Also, lifetime problem gamblers with a history of indebtedness were more likely to recommend professional treatment. The present findings may help design assessment, referrals and treatment uptake for patients in need of gambling disorder treatment.
Disclosure
Anders Håkansson reports grants from Svenska spel AB (state-owned gambling operator), during the conduct of the study; grants from Svenska spel AB (state-owned gambling operator), Systembolaget AB (state-owned alcohol monopoly), and Swedish Enforcement Authority outside the submitted work; financial support from Shire, outside the submitted work; working alongside Kontigo care, outside the submitted work. Madison Ford reports no conflicts of interest with this work.
References
1. Karlsson A, Håkansson A. Gambling disorder, increased mortality, suicidality, and associated comorbidity: a longitudinal nationwide register study. J Behav Addict. 2018;7:1091–1099.
2. Williams RJ, Volberg RA, Stevens RMG. The Population Prevalence of Problem Gambling. Methodological Influences, Standardized Rates, Jurisdictional Differences, and Worldwide Trends. Ontario Problem Gambling Research Centre and The Ontario Ministry of Health and Long Term Care; 2012.
3. Gainsbury S, Hing N, Suhonen N. Professional help-seeking for gambling problems: awareness, barriers and motivators for treatment. J Gambl Stud. 2014;30:503–519. doi:10.1007/s10899-013-9373-x
4. Hing N, Tiyce M, Holdsworth L, Nuske E. All in the family: help-seeking by significant others of problem gamblers. Int J Ment Health Addict. 2013;11:396–408. doi:10.1007/s11469-012-9423-0
5. Suurvali H, Cordingley J, Hodgins DC, Cunningham J. Barriers to seeking help for gambling problems: a review of the empirical literature. J Gambl Stud. 2009;25:407–424. doi:10.1007/s10899-009-9129-9
6. Kessler RC, Hwang I, LaBrie R, et al. DSM-IV pathological gambling in the National Comorbidity Survey replication. Psychol Med. 2008;38:1351–1360. doi:10.1017/S0033291708002900
7. Rodda SN, Dowling NA, Lubman DI. Gamblers seeking online help are active help-seekers: time to support autonomy and competence. Addict Behav. 2018;87:272–275. doi:10.1016/j.addbeh.2018.06.001
8. Choi SW, Shin YC, Kim DJ, et al. Treatment modalities for patients with gambling disorder. Ann Gen Psychiatry. 2017;16:23.
9. Rash CJ, Petry NM. Psychological treatments for gambling disorder. Psychol Res Behav Manag. 2014;7:285–295. doi:10.2147/PRBM.S40883
10. Slutske WS. Natural recovery and treatment-seeking in pathological gambling: results of two US national surveys. Am J Psychiatry. 2006;163:297–302. doi:10.1176/appi.ajp.163.2.297
11. McGrath DS, Kim HS, Hodgins DC, Novitsky C, Tavares H. Who are the anonymous? Involvement and predictors of gamblers anonymous attendance among disordered gamblers presenting for treatment. J Gambl Stud. 2018;34:1423–1434. doi:10.1007/s10899-018-9774-y
12. Schuler A, Ferentzy P, Turner NE, et al. Gamblers anonymous as a recovery pathway: a scoping review. J Gambl Stud. 2016;32:1261–1278. doi:10.1007/s10899-016-9596-8
13. Binde P. A Swedish mutual support society of problem gamblers. Int J Mental Health Addict. 2012;10:512–523. doi:10.1007/s11469-011-9335-4
14. Sullivan S, McCormick R, Lamont M, Penfold A. Problem gambling: patients affected by their own or another’s gambling may approve of help from general practitioners. N Zeal Med J. 2007;120:U2605.
15. Thomas SA, Piterman L, Jackson AC. Problem gambling: what do general practitioners need to know and do about it? Med J Austr. 2008;189:135–136. doi:10.5694/j.1326-5377.2008.tb01944.x
16. Thomas S. Problem gambling. Austr Fam Phys. 2014;43:362–364.
17. Tolchard B, Thomas L, Battersby M. GPs and problem gambling: can they help with identification and early intervention? J Gambl Stud. 2007;23:499–506.
18. Håkansson A. Addiction treatment in social services and health care. A Swedish model to challenge. Läkartidningen. 2015;112:
19. Widinghoff C, Håkansson A. Gambling disorder – a current issue in Sweden. Läkartidningen. 2018;115:
20. Håkansson A, Kostevski A, Ekblad S. Gambling habits, gambling norms, and problem gambling in foreign born and native populations in Denmark – a general population survey. Addict Behav Rep. 2019. doi:10.1016/j.abrep.2019.100183
21. Håkansson A, Karlsson A, Widinghoff C. Primary and secondary diagnoses of gambling disorder and psychiatric comorbidity in the Swedish health care system – a nationwide register study. Front Psychiatry. 2018;9:426.
22. Nehlin C, Nyberg F, Jess K. Brief intervention within primary care for at-risk gambling: a pilot study. J Gambling Stud. 2016;32:1327–1335. doi:10.1007/s10899-016-9610-1
23. Carlbring P, Jonsson J, Josephson H, Forsberg L. Motivational interviewing versus cognitive behavioral group therapy in the treatment of problem and pathological gambling: a randomized controlled trial. Cogn Behav Ther. 2010;39:92–103.
24. Carlbring P, Smit F. Randomized trial of internet-delivered self-help with telephone support for pathological gamblers. J Consult Clin Psychol. 2008;76:1090–1094. doi:10.1037/a0013603
25. Andréasson S, Danielsson AK, Wallhed-Finn S. Preferences regarding treatment for alcohol problems. Alcohol Alcohol. 2013;48:693–699.
26. Toce-Gerstein M, Gerstein DR, Volberg RA. The NODS-CLiP: a rapid screen for adult pathological and problem gambling. J Gambl Stud. 2009;25(4):541–555. doi:10.1007/s10899-009-9135-y
27. WeinstockJ, Burton S, RashCJ, et al. Predictors of engaging in problem gambling treatment: data from the West Virginia problem gamblers help network. Psychol Addict Behav. 2011;25:372 –379. doi:10.1037/a0023240
28. Braun B, Ludwig M, Braun B, Ludwig M, Sleczka P, Bühringer G, Kraus L. Gamblers seeking treatment: who does and who doesn’t. J. Addict. Behav. 2014;3:189–198. doi:10.1556/JBA.3.2014.3.7
29. Ledgerwood DM, Arfken CL, Wiedemann A, Bates KE, Holmes D, Jones L. Who goes to treatment? Predictors of treatment initiation among gambling help-line callers. Am J Addict. 2013;22:33–38. doi:10.1111/j.1521-0391.2013.00323.x
30. Bush K, Kivlahan DR, McDonnel MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Arch Intern Med. 1998;16:1789–1795. doi:10.1001/archinte.158.16.1789
31. Turunen E, Hiilamo H. Health effects of indebtedness: a systematic review. BMC Publ Health. 2014;14:489. doi:10.1186/1471-2458-14-489
32. Cunningham JA, Cordingley J, Hodgins DC, Toneatto T. Beliefs about gambling problems and recovery: results from a general population telephone survey. J Gambl Stud. 2011;27:625–631. doi:10.1007/s10899-010-9231-z
33. Lorains FK, Cowlishaw S, Thomas SA. Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction. 2011;106:490–498. doi:10.1111/add.2011.106.issue-3
34. Rodriguez-Monguio R, Errea M, Volberg R. Comorbid pathological gambling, mental health, and substance use disorders: health-care services provision by clinician specialty. J Behav Addict. 2017;6:406–415. doi:10.1556/2006.6.2017.054
35. Fransson A, Chóliz M, Håkansson A. Addiction-like mobile phone behavior – validation and association with problem gambling. Front Psychol. 2018;9:655. doi:10.3389/fpsyg.2018.00655
36. Karlsson J, Broman N, Håkansson A. Associations between problem gambling, gaming, and internet use: a cross-sectional population survey. J Addict. 2019;2019:1464858. doi:10.1155/2019/1464858
37. Abbott M, Romild U, Volberg R. The prevalence, incidence, and gender and age-specific incidence of problem gambling: results of the Swedish longitudinal gambling study (Swelogs). Addiction. 2017;113:699–707.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.