Back to Journals » Cancer Management and Research » Volume 14
The Future of Lung Cancer Screening: Current Challenges and Research Priorities
Authors Burzic A ![]() , O'Dowd EL
, O'Dowd EL ![]() , Baldwin DR
, Baldwin DR
Received 4 October 2021
Accepted for publication 30 January 2022
Published 16 February 2022 Volume 2022:14 Pages 637—645
DOI https://doi.org/10.2147/CMAR.S293877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Amna Burzic,1 Emma L O’Dowd,1,2 David R Baldwin1,2
1Department of Respiratory Medicine, Nottingham University Hospitals NHS Trust, Nottingham City Hospital, Nottingham, UK; 2Division of Medicine, University of Nottingham, Nottingham, NG5 1PB, UK
Correspondence: David R Baldwin, Department of Respiratory Medicine, Nottingham University Hospitals NHS Trust, Nottingham City Hospital, Nottingham, NG5 1PB, UK, Tel +44 115 9691169, Fax +44 115 9627723, Email [email protected]
Abstract: Lung cancer is the leading cause of cancer-related deaths worldwide, primarily because most people present when the stage is too advanced to offer any reasonable chance of cure. Over the last two decades, evidence has accumulated to show that early detection of lung cancer, using low-radiation dose computed tomography, in people at higher risk of the condition reduces their mortality. Many countries are now making progress with implementing programmes, although some have concerns about cost-effectiveness. Lung cancer screening is complex, and many factors influence clinical and cost-effectiveness. It is important to develop strategies to optimise each element of the intervention from selection and participation through optimal scanning, management of findings and treatment. The overall aim is to maximise benefits and minimise harms. Additional integrated interventions must include at least smoking cessation. In this review, we summarize the evidence that has accumulated to guide optimisation of lung cancer screening, discuss the remaining open questions about the best approach and identify potential barriers to successful implementation.
Keywords: lung cancer, screening, computed tomography
Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide because it is both common and the majority of people present clinically with late-stage disease, when even modern treatments have little impact on mortality. Early detection with low radiation dose CT (LDCT) reduces lung cancer-related mortality by detecting lung cancer at an early stage when it is amenable to potentially curative treatments. Two large randomised controlled trials, the US National Lung Screening Trial (NLST)1 and the Dutch-Belgian NELSON Trial,2 have shown that LDCT reduces lung cancer-specific mortality rate, and the larger of these, NLST, showed a significant all-cause mortality reduction of 6.7%.1 Both trials provide sufficient evidence to support the implementation of screening on the basis of clinical efficacy, although there is still debate about cost-effectiveness, where the specifics of implementation are key.3,4 Over the last ten years, since the publication of NLST, much research work has been published to inform those managing nascent screening programmes on how they should be structured. In this review, we will focus on current evidence on lung cancer screening in the UK, Europe and North America. We will describe the approach to developing a screening programme to show how each element contributes to a successful service and describe current challenges and future research priorities.
Defining and Selecting the Eligible Population
To make lung cancer screening viable, it must be clinically and cost-effective. One of the essential requirements is to apply screening to a population at risk of the disease. The screening test, LDCT, is relatively expensive compared with, say, the Faecal Immunochemical Test used for colorectal screening, and so it is important to target screening in populations where the chance of finding lung cancer is sufficiently high, in other words a high-risk group. Robust selection criteria for screening will therefore reduce the number of false-positives and subsequent scanning.
Although age and smoking status are known to be the greatest risk factors for developing lung cancer, several other important factors also contribute to risk.5 The NLST and NELSON trials used age and cumulative smoking exposure in their selection criteria. The US Preventive Services Task Force (USPSTF) subsequently recommended annual lung cancer screening in 2013 for individuals aged 55–80 who had a 30 pack-year smoking history and currently smoke or have quit within the past 15 years.6 In July 2020, the USPSTF revised these screening recommendations to include a lower entry age of 50 years and reduced the threshold for smoking exposure to 20 pack-years.7 However, there is concern that these criteria, although easy to apply, oversimplify lung cancer risk prediction by ignoring important risk factors, such as family history of lung cancer, smoking intensity, personal history of other respiratory diseases and asbestos exposure. Several multi-variable risk-prediction models to assess the risk of developing lung cancer have been developed with the aim to increase pre-test probability and thereby improve the effectiveness of screening. Both the modified Liverpool Lung Project (LLPv2)8 and US Prostate, Lung, Colorectal and Ovarian (PLCO) models9 have been shown to have greater sensitivity for lung cancer detection (compared with the original USPSTF 2013 criteria)10 and have been used to shape selection criteria for clinical trials.
The UK Lung Cancer Screening trial (UKLS) used an age of 50–75 years and LLP v2 risk ≥5% over 5 years for the selection criteria.11 2.1% of participants in the LDCT arm were found to have lung cancer on baseline imaging compared to 1.03% in NLST and 0.9% in NELSON.12 A study using PLCO instead of NLST criteria found an added 12.4% lung cancers would have been detected and 8.8% fewer individuals would have undergone screening.5 Following the success of the UKLS trial, several pilot programmes began in the UK including the Liverpool Health Lung Project and Lung Screen Uptake Trial.13,14 The Targeted Lung Health Check Programme has since been introduced in 10 regions in the UK and invites individuals aged 55 to 74 and 364 days of age that are registered with a GP who have ever smoked to a Lung Health Check.15 Attendees with a LLPv2 risk ≥2.5% over 5 years and/or PLCO risk ≥1.51% over 6 years are invited for LDCT.
However, studies looking at risk prediction models generally assess risk at a single time point and can lead to overdiagnosis due principally to a tendency to select older individuals and those who may have increased competing causes of death. Life expectancy in high-risk individuals must be considered since we know that lung cancer risk increases with age or change in smoking habits and that non-lung cancer-related mortality will also increase with age.16
Risk prediction models have not been widely adopted, although they are in use in several programmes including some in Canada. Further research is required to refine the optimal method that selects high-risk individuals that will derive the greatest benefits in real-world lung cancer screening. Different methods may be required in different countries where risk factors may differ17 and more research is required in never or minimal smokers.
Recruitment and Participation
Uptake into lung cancer screening programmes is a crucial consideration for success and effectiveness. Only 1.9% of eligible, high-risk individuals were screened in the US, despite approval for a national programme and reimbursement through the Centers for Medicaid18 and Medicare19 thereby demonstrating the real-world challenges in effective recruitment.20 The UKLS demonstrated that those considered to be at highest risk of developing lung cancer, such as current smokers and those from lower socioeconomic backgrounds, were also the least likely to enrol or complete lung cancer screening.21
In clinical trials, the methods of recruitment usually involve local strategies such as advertising. Only in UKLS was a true population approach used (although NELSON used this as one method alongside advertising).11 The population approach was shown to be inefficient, with over two thirds of people failing to respond and evidence that this included a disproportionate number of people who may have been eligible.
In the Lung Screen Uptake Trial (LSUT), the participation rate was 53%, more than double that of NELSON.22 The intervention group were invited to screening using “targeted, stepped and low burden” materials with the aim to minimise psychological barriers such as fear and stigma. No difference was demonstrated in rates of uptake between the control and intervention arms. However, uptake was improved among individuals living in areas of highest deprivation and lung cancer incidence, thus improving equity in screening uptake as well as overall screening effectiveness. This may be due to the use of a variety of previously studied methods that have been designed to increase participation, drawing on experience from other screening programmes.23 These include invitations from the primary care doctor, reminders, timed appointments, and low-burden invitation material. Reminders alone providing a second pre-scheduled appointment increased the uptake by non-responders by 24%. Given the increased participation rate in LSUT, these methods may represent a minimum standard.
Addressing psychological barriers is important with two of the most important being poor perception of lung cancer outcomes following early-stage detection and the stigma of lung cancer being a “self-inflicted disease”.24 Efforts to improve public education and therefore perception of lung cancer, including improved awareness of advances in treatment, is crucial to reducing stigma and associated fatalism. Another barrier is fear. In the UK, it is recognised that the word “cancer” may discourage participation and therefore, the term “lung health check” is used.
The UK primary care system is proving to be an important tool in improving participation in screening pilots. The Liverpool Lung Health Check invited individuals with a documented history of smoking or diagnosis of chronic obstructive pulmonary disease (COPD) recorded in primary care records. This targeted approach led to 40% uptake in the first round of the pilot programme, which suggests that electronic primary care records can aid recruitment to screening and thus stresses the importance of accurate smoking data.25 Where data are incomplete, automated text message systems can be used to update records. One small study found that almost half of respondents were current or ex-smokers who would be eligible for a Targeted Lung Health Check.26 A further barrier may be a lack of knowledge of local screening policies and guidelines for referral. Successful strategies to improve primary care engagement have previously included educational sessions, audit, and feedback on local outcomes.27 High false-positive rates may also lead to burdensome follow-up. However, clear guidelines assigning responsibility for further investigations required will help reduce the burden on primary care. Other significant barriers, including short consultation time and poor staffing, remain with an inadequately funded workforce.28
Other influencing factors for both high-risk individuals and those with disabilities include practical barriers such as travel distance and lack of transport or parking. A successful screening programme must be accessible to all eligible individuals, including those with a physical or learning disability or mental illness. Easy-read invitations and mobile scanners in hard-to-reach communities are a potential solution, as well as facilitation of transport.23 Successful pilot programmes, such as the Manchester and Liverpool Lung Health Check, provided easy access to scanners. Translation services must also be available to those with limited English language skills.
There may be an emerging role for social media and digital health “apps” for both recruitment and assessment of eligibility. Users could, for example, input their smoking habits on a regular basis for accurate monitoring, and the app could concurrently be used to provide smoking cessation support. However, smartphone users are more likely to be younger, have a higher educational background with higher income.29 Therefore, individuals in hard-to-reach communities such as those with lower socioeconomic backgrounds may not have access to this technology.
Optimising participation rates remains a priority for successful and effective implementation of a lung cancer screening programme. As programmes begin, it is important to design research that will test ways in which participation can be improved, as well as ongoing adherence to subsequent screening rounds. As evidence becomes available from other countries with different cultures, it is important to test whether optimal methods translate into ethnic groups in other countries with diverse cultures.
Psychological Factors
The psychological costs of screening must be considered prior to implementation of a national programme. The NLST, NELSON and the Pan-Canadian Early Detection of Lung Cancer Study (PAN-CAN) trials found no evidence of clinically adverse psychological impacts on generic health-related quality of life measures overall at short- or long-term follow-up for screened cohorts.30 Scores of anxiety and depression have been shown to differ by LDCT result with increased scores for those receiving indeterminate and suspicious results. However, these have been short-lived. Evidence has also shown that individual responses are affected by the quantity and quality of information provided prior to commencing screening.31 Individuals have also reported less psychological distress where physicians have adopted a person-centred approach to communication.32 These findings highlight the importance of providing good information and managing expectations in communicating screening results. Overall, this supports a person-centred approach where individuals receive adequate information to enable psychological preparedness for different screening results and their subsequent pathways.
Screening Process
To achieve a successful screening programme, thought must be given to screening capacity, equipment, information technology infrastructure, funding and quality standards and assurance. The Standard Protocol prepared for the Targeted Lung Health Checks Programme in the UK outlines specific expectations for technology, hardware and software required for LDCT screening.33
Radiation exposure must be as low as possible whilst maintaining good image quality. It is estimated that for every 22 lung cancer deaths prevented, there is 1 radiation-induced lung cancer.6 LDCT reduces the radiation dose to approximately one-fifth of conventional CT and advances in technology have considerably reduced the radiation dose by 3-fold or more.
Nodule Management
Robust nodule risk assessment and management guidelines can improve cost-effectiveness and reduce harm from excessive scans or investigations. Volumetric assessment is the preferred method to assess nodule size in lung cancer screening. Accurate assessment of nodule size is imperative to ensure appropriate subsequent management. It is widely accepted that semi-automated or fully automated volumetry is more accurate than diameter measurements with manual electronic callipers. Several different thresholds for defining a positive screen have been used. Two of the most used guidelines in the context of screening are the American College of Radiology (ACR) Lung RADS version 1.1 and the British Thoracic Society (BTS) Pulmonary Nodule Guideline.34,35 The BTS recommend volumetric assessment where possible, whereas the ACR mostly focus on diameter. These nodule guidelines include a stratified approach to management based on nodule size and separate recommendations for the management of sub-solid nodules as these generally have a better prognosis than equivalent size solid nodules and may be a potential source of overdiagnosis. Volumetric assessment, however, can vary between different volumetry software packages (VSPs). Some VSPs differ substantially from others in volume measurement and some can lead to significantly higher recall rates, thereby highlighting that volumetric software must remain constant to allow accurate comparisons and reduce false-positive rates.36
Screening Intervals
Optimising screening intervals following baseline LDCT can further improve cost-effectiveness and minimise harm. NELSON screened participants at baseline and 1, 3 and 5.5 years from baseline. During the 2.5-year interval to the final round, 17.3% scans detected stage 3B or 4 lung cancer compared to 6.8% at the 1-year interval LDCT after the baseline round. Furthermore, most of the interval cancers during the 2.5-year interval developed in the final 6 months.37 The USPSTF modelling looked at annual and biennial intervals and found annual scenarios to be the most efficient in terms of life-years gained, but with a higher gross cost.38
Personalised risk stratification following baseline LDCT is another potential solution to further minimise harm and improve cost-effectiveness. Negative LDCT by the American College of Radiology Lung Imaging Reporting and Data System (Lung-RADS) was found in 80.6% of individuals eligible for NLST.39 This was associated with 40 times lower relative risk of lung cancer at 2 years, compared to a positive baseline scan. The NELSON trial showed a negative baseline LDCT was associated with a 3% chance of lung cancer diagnosis in 10 years. An intermediate baseline LDCT was associated with an 8.8% chance of lung cancer diagnosis in 10 years whilst a positive baseline LDCT was associated with a 52% chance of lung cancer diagnosis in 10 years.2 Personalised risk stratification following a negative baseline LDCT could therefore halve the number of scans needed over a 10-year period. The 4-in-The-Lung-Run trial (4ITLR) is due to begin soon with the aim of showing whether a risk-stratified screening interval following negative baseline CT is not inferior to annual screening. Personalised risk stratification may be complex and would present a considerable challenge to facilitating informed decision-making for participants. Similar to the issue of simple vs more complex baseline risk assessment, personalised screen intervals need to be shown to have clear benefits if they are to be adopted.
Incidental Findings Management
Incidental findings are frequently detected during lung cancer screening. A systematic review of the prevalence of incidental findings found 14% of CT scans had findings requiring follow-up. Mendoza et al found approximately 10% of individuals in a screening programme had infectious or inflammatory lung lesions and that less than 1% of these lesions were associated with lung cancer.40 Some of these findings can be seen as an added benefit from the lung cancer screening programme. However, incidental findings can lead to extra costs and harm from unnecessary investigations, including psychological harm such as anxiety.41 Clear guidance on the management of incidental findings should form the basis of any CT screening protocol. Table 1 shows the recommendations in the NHS England Targeted Lung Health Check Programme.42
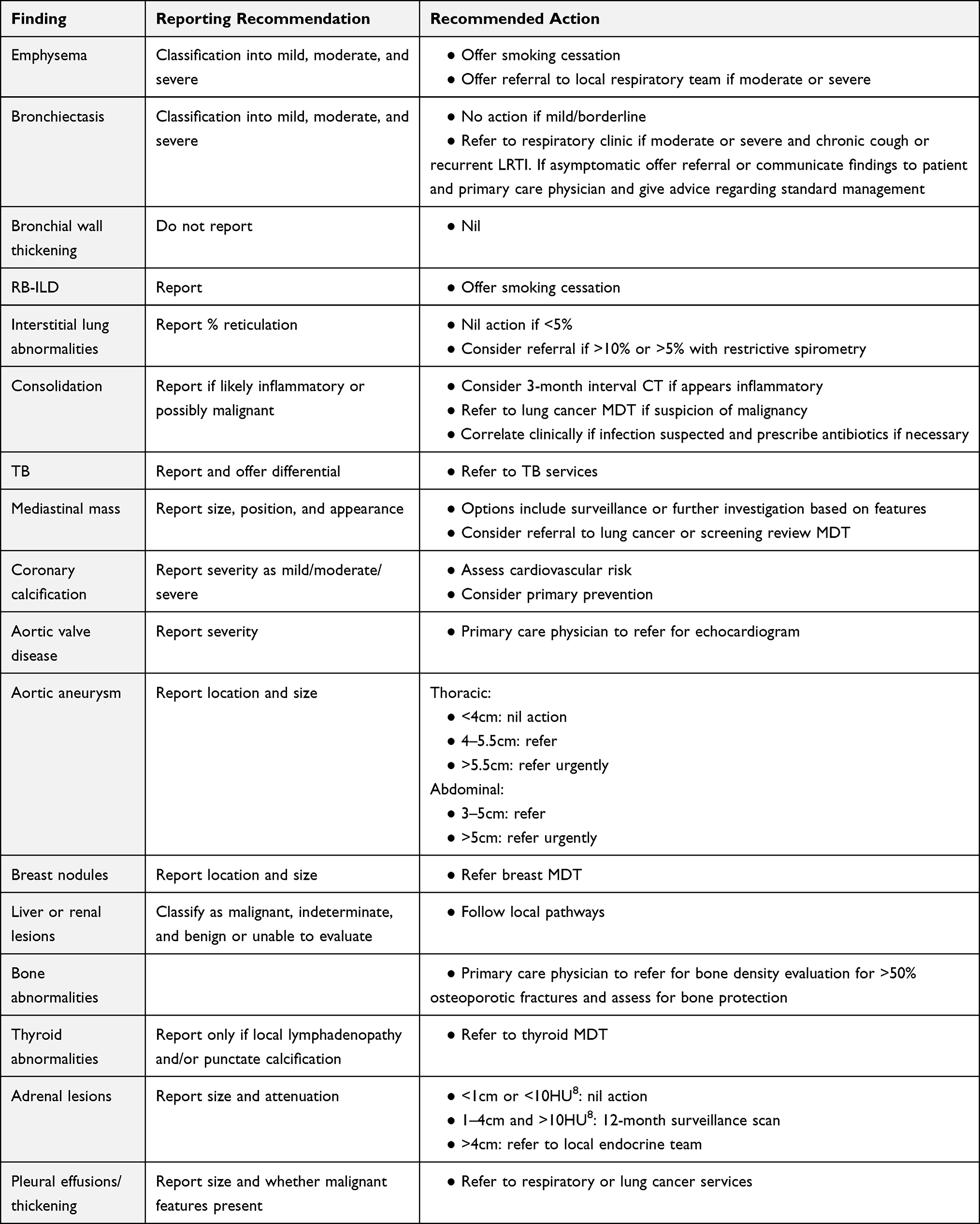 |
Table 1 Management Protocol for Common Incidental Findings on LDCT in Lung Cancer Screening (NHS England Targeted Lung Health Check Programme) |
Investigation Following Referral
A clear downstream management protocol for suspicious findings in LDCT has the potential to substantially reduce harms. NELSON and NLST showed that 61% of participants that had a form of diagnostic work up did not have lung cancer.43 The benign resection rates for these studies were 24% and 23%, respectively. Both the UKLS and the IELCAP have clear management protocols and achieved a benign resection rate of 10%. Overall, pooled data from the UK trials and implementation pilots (11,148 individuals) show a very low rate of harm including a 4.6% benign resection rate and no harm from invasive procedures for benign disease.44 This is mainly achieved by careful assessment of the risk of malignancy through PET CT scanning and judicious use of trans-thoracic lung biopsy.
Smoking Cessation
There is a recognised need to integrate lung cancer screening with smoking cessation. Previous studies have shown that integration of smoking cessation into screening has a significant impact on cost-effectiveness.45 However, previous studies have also expressed concern that screening may offer false reassurance to those who smoke, leading to either continued or renewed uptake of smoking. In the NELSON trial 14.5% of individuals in the screening arm stopped smoking compared to 19.1% in the control arm.46 This is in comparison to a background general population smoking cessation rate of 6–7% suggesting rates of smoking cessation were higher. Furthermore, a subgroup of NLST participants with a false-positive scan were shown to have higher rates of smoking cessation.47 Brain et al (2017) asked a high-risk population that had been randomized to screen arm and no screen control to complete questionnaires on smoking habits. Rates of smoking cessation in the control arm were 8% compared to 14% in the screen arm at 2 weeks post baseline scan results and 21% versus 24%, respectively, up to 2 years post recruitment (adjusted odds ratio 1.6, p = 0.003).48 Furthermore, the odds of smoking cessation at 2 years were higher if the scan had abnormalities requiring further tests (OR 2.29 compared with controls). This therefore provides further evidence that participation in LDCT screening improves smoking cessation rates, especially in individuals with a positive CT result.
Although the optimal strategy for integrating smoking cessation remains unknown, Cadham et al have recently shown that all smoking cessation interventions reduce lung cancer incidence and mortality versus screening alone.49 Minor differences were seen in cost between approaches and therefore choice should be based on practical issues and patient preferences.
Implementation Challenges and Unanswered Questions
To achieve successful implementation, several outstanding challenges must be addressed. It is necessary to establish the most optimal and cost-effective methods to identify and recruit high-risk and hard-to-reach individuals for screening as well as overcome identified barriers to participation. Further research will also need to identify how to optimise risk prediction models for the UK target population as well as incorporate life expectancy rather than risk stratification at a single time point. Training and workforce needs will also need to be addressed, including how to standardise requirements and quality assurance. Significant concerns exist regarding radiologist numbers to meet the needs of a screening programme. Further research into AI performance will be necessary prior to clinical implementation to support current workload pressures.
Quality Assurance
All screening programmes should have a documented quality assurance mechanism. For lung cancer screening, this includes a defined set of standards for each step of the pathway. This means that the participant pathways need to be clearly described, and for each point, the potential for unwarranted variation and error is considered. The individual topics are too numerous to list here but broadly encompass informed choice; equality; safety netting; technical aspects; training, monitoring and assessment of staff; measuring outcomes, both benefits and harms; governance; and funding capacity planning and sustainability.
Capacity
Although countries differ in the availability of both equipment and workforce, many are concerned about the ability of often over-stretched healthcare systems to deliver a full screening programme. This will likely result in some decisions to be made about both the design of programmes and the pace of implementation. The UK Royal College of Radiologists Clinical Radiology Workforce Census 2020 report found that one-in-ten radiologist posts were unfilled across UK hospitals.50 Along with the increased workload, these vacancies represent an estimated shortage of 33% of radiologists to meet current workload demands. An adequate and well-trained workforce will reduce overdiagnosis as well as false-positive and false-negative rates, thus improving the effectiveness of screening. To mitigate this, automated artificial intelligence (AI) has gained a lot of interest in improving risk prediction and has been shown to have excellent performance for nodule detection.51 Challenges remain, however, particularly in the detection of false-positive nodules. Further research will be required to optimise AI performance prior to clinical implementation. Modelling in the US, a relatively well-provided system, has estimated that the radiology workforce can absorb lung screening in most areas of the country but that there will be a potential issue with capacity in the more deprived, lower income communities, which are, paradoxically, at higher risk.52 A further modelling study predicted a major increase in surgery, most prominent in the first 5 years.53
Conclusion
Evidence from trials such as NLST and NELSON for the clinical effectiveness of lung cancer screening is conclusive, and there is a wealth of the literature published that has shaped modern screening pilot programmes. Many countries have now completed pilot programmes that have confirmed the efficacy of screening in detecting early-stage lung cancer. Some have shown improved outcomes, reflecting improvements in clinical management of pulmonary nodules and early-stage lung cancer, especially in the reduction of harms. Comparing these early implementation pilots, as well as established programmes (principally the US), allows reflection on how programmes can be adapted to capture the best aspects of each other, and where research is needed. Following the encouraging results from the pilots, many countries are actively engaged in the process of wider implementation. It is vital that the programmes are well organised with clear protocols and quality assurance standards. Future research should focus on optimising aspects of CT screening that could have important implications for clinical and cost-effectiveness in different healthcare settings.
Disclosure
Professor David R Baldwin reports personal fees from MSD, AstraZeneca, BMS, and Roche, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Aberle DR, Adams AM; National Lung Screening Trial Research T. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395–409. doi:10.1056/NEJMoa1102873.
2. de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503–513. doi:10.1056/NEJMoa1911793
3. Matthijs Oudkerk AD, Vliegenthart R, Henzler T, et al. European position statement on lung cancer screening. Lancet Oncol. 2017;18(12):e754–e66. doi:10.1016/S1470-2045(17)30861-6
4. Kauczor HU, Baird AM, Blum TG, et al. ESR/ERS statement paper on lung cancer screening. Eur Respir J. 2020;55(2). doi:10.1183/13993003.00506-2019
5. Tammemagi MC, Church TR, Hocking WG, et al. Evaluation of the lung cancer risks at which to screen ever- and never-smokers: screening rules applied to the PLCO and NLST cohorts. PLoS Med. 2014;11(12):e1001764. doi:10.1371/journal.pmed.1001764
6. Humphrey LL, Deffebach M, Pappas M, et al. Screening for lung cancer with low-dose computed tomography: a systematic review to update the US preventive services task force recommendation. Ann Intern Med. 2013;159(6):411–420. doi:10.7326/0003-4819-159-6-201309170-00690
7. Force USPST, Krist AH, Davidson KW, et al. Screening for lung cancer: US preventive services task force recommendation statement. JAMA. 2021;325(10):962–970. doi:10.1001/jama.2021.1117
8. Cassidy A, Myles JP, van Tongeren M, et al. The LLP risk model: an individual risk prediction model for lung cancer. Br J Cancer. 2008;98(2):270–276.
9. Tammemagi MC, Katki HA, Hocking WG, et al. Selection criteria for lung-cancer screening. N Engl J Med. 2013;368(8):728–736. doi:10.1056/NEJMoa1211776
10. Robbins HA, Alcala K, Swerdlow AJ, et al. Comparative performance of lung cancer risk models to define lung screening eligibility in the United Kingdom. Br J Cancer. 2021;124(12):2026–2034. doi:10.1038/s41416-021-01278-0
11. Baldwin DR, Duffy SW, Wald NJ, et al. UK Lung Screen (UKLS) nodule management protocol: modelling of a single screen randomised controlled trial of low-dose CT screening for lung cancer. Thorax. 2011;66(4):308–313. doi:10.1136/thx.2010.152066
12. Field JK, Duffy SW, Baldwin DR, et al. UK lung cancer RCT pilot screening trial: baseline findings from the screening arm provide evidence for the potential implementation of lung cancer screening. Thorax. 2016;71(2):161–170. doi:10.1136/thoraxjnl-2015-207140
13. Ruparel M, Quaife SL, Dickson JL, et al. Lung screen uptake trial: results from a single lung cancer screening round. Thorax. 2020;75(10):908–912. doi:10.1136/thoraxjnl-2020-214703
14. Duffy SW, Maroni R, Vulkan D, et al. Liverpool healthy lung programme – second year evaluation report; 2018. Available from: https://www.liverpoolccg.nhs.uk/media/3245/final-lhlp-2nd-year-report-10-july-2018-with-logos.pdf.
15. National Health Service England -N, Cancer, Programme. Targeted screening for lung cancer with low radiation dose computed tomography. Standard protocol prepared for the targeted lung health checks programme; 2019 [cited UK Government]. Available from: https://www.england.nhs.uk/wp-content/uploads/2019/02/targeted-lung-health-checks-standard-protocol-v1.pdf.
16. Ten Haaf K, Bastani M, Cao P, et al. A comparative modeling analysis of risk-based lung cancer screening strategies. J Natl Cancer Inst. 2020;112(5):466–479. doi:10.1093/jnci/djz164
17. Park S, Nam BH, Yang HR, et al. Individualized risk prediction model for lung cancer in Korean men. PLoS One. 2013;8(2):e54823. doi:10.1371/journal.pone.0054823
18. Centers f, Medicare, &, Medicaid, Services. Screening for lung cancer with Low Dose Computed Tomography (LDCT); 2015. Available from: https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&NCAId=274.
19. Verma V, Beriwal S. Medicare approves coverage for lung cancer screening: the case for symptomatic screening. JAMA Oncol. 2015;1(8):1027–1028. doi:10.1001/jamaoncol.2015.2165
20. Pham D, Bhandari S, Pinkston C, et al. Lung cancer screening registry reveals low-dose CT screening remains heavily underutilized. Clin Lung Cancer. 2020;21(3):e206–e11. doi:10.1016/j.cllc.2019.09.002
21. Ali N, Lifford KJ, Carter B, et al. Barriers to uptake among high-risk individuals declining participation in lung cancer screening: a mixed methods analysis of the UK Lung Cancer Screening (UKLS) trial. BMJ Open. 2015;5(7):e008254. doi:10.1136/bmjopen-2015-008254
22. Quaife SL, Ruparel M, Dickson JL, et al. Lung Screen Uptake Trial (LSUT): randomized controlled clinical trial testing targeted invitation materials. Am J Respir Crit Care Med. 2020;201(8):965–975. doi:10.1164/rccm.201905-0946OC
23. Baldwin DR, Brain K, Quaife S. Participation in lung cancer screening. Transl Lung Cancer Res. 2021;10(2):1091–1098. doi:10.21037/tlcr-20-917
24. Quaife SL, McEwen A, Janes SM, Wardle J. Attitudes towards lung cancer screening within socioeconomically deprived and heavy smoking communities: a qualitative study. Lancet. 2014;384:S16.
25. Ghimire B, Maroni R, Vulkan D, et al. Evaluation of a health service adopting proactive approach to reduce high risk of lung cancer: the Liverpool Healthy Lung Programme. Lung Cancer. 2019;134:66–71. doi:10.1016/j.lungcan.2019.05.026
26. Engela-Volker J, Eccles S. P163 Preparing wales for lung cancer screening – updating GP record smoking data using an automated text message system. Thorax. 2021;76(Suppl2):A156–A56. doi:10.1136/thorax-2021-BTSabstracts.272
27. Gesthalter YB, Koppelman E, Bolton R, et al. Evaluations of implementation at early-adopting lung cancer screening programs: lessons learned. Chest. 2017;152(1):70–80. doi:10.1016/j.chest.2017.02.012
28. Triplette M, Kross EK, Mann BA, et al. An assessment of primary care and pulmonary provider perspectives on lung cancer screening. Ann Am Thorac Soc. 2018;15(1):69–75. doi:10.1513/AnnalsATS.201705-392OC
29. Bol N, Helberger N, Weert JCM. Differences in mobile health app use: a source of new digital inequalities? Inf Soc. 2018;34(3):183–193. doi:10.1080/01972243.2018.1438550
30. Quaife SL, Janes SM, Brain KE. The person behind the nodule: a narrative review of the psychological impact of lung cancer screening. Transl Lung Cancer Res. 2021;10(5):2427–2440. doi:10.21037/tlcr-20-1179
31. Kummer S, Waller J, Ruparel M, et al. Mapping the spectrum of psychological and behavioural responses to low-dose CT lung cancer screening offered within a Lung Health Check. Health Expect. 2020;23(2):433–441. doi:10.1111/hex.13030
32. Slatore CG, Wiener RS, Golden SE, et al. Longitudinal assessment of distress among veterans with incidental pulmonary nodules. Ann Am Thorac Soc. 2016;13(11):1983–1991. doi:10.1513/AnnalsATS.201607-555OC
33. National Lung Screening Trial Research T. Lung cancer incidence and mortality with extended follow-up in the national lung screening trial. J Thorac Oncol. 2019;14(10):1732–1742. doi:10.1016/j.jtho.2019.05.044.
34. American College Radiology. Lung RADS v 1.1; 2019. Available from: https://www.acr.org/-/media/ACR/Files/RADS/Lung-RADS/LungRADSAssessmentCategoriesv1-1.pdf?la=en.
35. Callister ME, Baldwin DR, Akram AR, et al. British thoracic society guidelines for the investigation and management of pulmonary nodules. Thorax. 2015;70(Suppl 2):ii1–ii54. doi:10.1136/thoraxjnl-2015-207168
36. Soo E, Edey AJ, Mak SM, et al. Impact of choice of volumetry software and nodule management guidelines on recall rates in lung cancer screening. Eur J Radiol. 2019;120:108646. doi:10.1016/j.ejrad.2019.108646
37. Yousaf-Khan U, van der Aalst C, de Jong PA, et al. Final screening round of the Nelson lung cancer screening trial: the effect of a 2.5-year screening interval. Thorax. 2017;72(1):48–56. doi:10.1136/thoraxjnl-2016-208655
38. de Koning HJ, Meza R, Plevritis SK, et al. Benefits and harms of computed tomography lung cancer screening strategies: a comparative modeling study for the U.S. preventive services task force. Ann Intern Med. 2014;160(5):311–320. doi:10.7326/M13-2316
39. Silva M, Milanese G, Sestini S, et al. Lung cancer screening by nodule volume in lung-RADS v1.1: negative baseline CT yields potential for increased screening interval. Eur Radiol. 2021;31(4):1956–1968. doi:10.1007/s00330-020-07275-w
40. Mendoza DP, Chintanapakdee W, Zhang EW, et al. Management and outcomes of suspected infectious and inflammatory lung abnormalities identified on lung cancer screening CT. AJR Am J Roentgenol. 2021:1–10. doi:10.2214/AJR.20.25124.
41. Quaife SL, Vrinten C, Ruparel M, et al. Smokers’ interest in a lung cancer screening programme: a national survey in England. BMC Cancer. 2018;18(1):497. doi:10.1186/s12885-018-4430-6
42. National Health Service. England -N, Cancer, Programme. Targeted screening for lung cancer with low radiation dose computed tomography. Quality assurance standards prepared for the targeted lung health checks programme; 2020 [cited UK Government]. Available from: https://www.england.nhs.uk/wp-content/uploads/2019/02/targeted-screening-for-lung-cancer-quality-assurance-standard.pdf.
43. Field JK, Hansell DM, Duffy SW, et al. CT screening for lung cancer: countdown to implementation. Lancet Oncol. 2013;14(13):e591–600. doi:10.1016/S1470-2045(13)70293-6
44. Balata H, Ruparel M, O’Dowd E, et al. Analysis of the baseline performance of five UK lung cancer screening programmes. Lung Cancer. 2021;161:136–140. doi:10.1016/j.lungcan.2021.09.012
45. Cressman S, Peacock SJ, Tammemagi MC, et al. The cost-effectiveness of high-risk lung cancer screening and drivers of program efficiency. J Thorac Oncol. 2017;12(8):1210–1222. doi:10.1016/j.jtho.2017.04.021
46. van der Aalst CM, van den Bergh KA, Willemsen MC, et al. Lung cancer screening and smoking abstinence: 2 year follow-up data from the Dutch-Belgian randomised controlled lung cancer screening trial. Thorax. 2010;65(7):600–605. doi:10.1136/thx.2009.133751
47. Tammemagi MC, Berg CD, Riley TL, et al. Impact of lung cancer screening results on smoking cessation. J Natl Cancer Inst. 2014;106(6):dju084. doi:10.1093/jnci/dju084
48. Brain K, Carter B, Lifford KJ, et al. Impact of low-dose CT screening on smoking cessation among high-risk participants in the UK lung cancer screening trial. Thorax. 2017;72(10):912–918. doi:10.1136/thoraxjnl-2016-209690
49. Cadham CJ, Cao P, Jayasekera J, et al. Cost-effectiveness of smoking cessation interventions in the lung cancer screening setting: a simulation study. J Natl Cancer Inst. 2021;113(8):1065–1073. doi:10.1093/jnci/djab002
50. Royal C, of, Radiologists. Clinical radiology: UK workforce consensus 2020 report; 2021. Available from: https://www.rcr.ac.uk/system/files/publication/field_publication_files/clinical-radiology-uk-workforce-census-2020-report.pdf.
51. Chamberlin J, Kocher MR, Waltz J, et al. Automated detection of lung nodules and coronary artery calcium using artificial intelligence on low-dose CT scans for lung cancer screening: accuracy and prognostic value. BMC Med. 2021;19(1):55. doi:10.1186/s12916-021-01928-3
52. Smieliauskas F, MacMahon H, Salgia R, et al. Geographic variation in radiologist capacity and widespread implementation of lung cancer CT screening. J Med Screen. 2014;21(4):207–215. doi:10.1177/0969141314548055
53. Blom EF, Ten Haaf K, Arenberg DA, et al. Treatment capacity required for full-scale implementation of lung cancer screening in the United States. Cancer. 2019;125(12):2039–2048. doi:10.1002/cncr.32026
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.