Back to Journals » Journal of Inflammation Research » Volume 19
The Future of Hydrogen Peroxide as a Biomarker for Airway Inflammation
Authors Gagliani C, Benfante A, Principe S, Scichilone N ![]()
Received 26 November 2025
Accepted for publication 6 February 2026
Published 12 February 2026 Volume 2026:19 552263
DOI https://doi.org/10.2147/JIR.S552263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Claudia Gagliani,1 Alida Benfante,1 Stefania Principe,2 Nicola Scichilone1
1PROMISE Department, Division of Respiratory Medicine, University of Palermo, Palermo, Italy; 2Amsterdam UMC, Department of Pulmonary Medicine, University of Amsterdam, Amsterdam, Netherlands
Correspondence: Nicola Scichilone, PROMISE Department, Division of Respiratory Medicine, University of Palermo, Via del Vespro 129, Palermo, 90127, Italy, Email [email protected]
Abstract: Airway inflammation has traditionally been assessed using invasive or semi-invasive techniques, prompting growing interest in non-invasive biomarkers. Exhaled breath condensate (EBC) offers a repeatable and well-tolerated method to evaluate airway inflammation and oxidative stress, with hydrogen peroxide (H2O2) emerging as a biomarker with relevant translational potential for disease monitoring and treatment response. This narrative review aimed to evaluate the potential H2O2 in EBC as a non-invasive biomarker for disease monitoring and treatment response in inflammatory respiratory diseases. Key clinical studies investigating H2O2 in patients with asthma, COPD, bronchiectasis and acute lung conditions were analyzed. Exhaled H2O2 levels are elevated in several inflammatory respiratory diseases, reflecting airway oxidative stress and disease instability, with higher concentrations observed in untreated or exacerbated patients, which decline in response to therapy. These findings indicate that H2O2 appears to be a promising tool for assessing airway oxidative stress and inflammation. Further research is needed to validate its clinical relevance and support its integration into standard clinical management.
Keywords: exhaled breath, diagnosis, disease monitoring, respiratory diseases, clinical practice
Introduction
Airway inflammation has been evaluated in various studies through either invasive techniques (eg, bronchoalveolar lavage fluid and bronchial biopsies)1,2 or semi-invasive methods such as sputum induction.3 Difficulties in reaching and exploring the nature of airway inflammation, especially in the distal portion of the bronchial tree, has limited the characterization of the inflammatory changes in clinical practice and for research purposes. In recent years, increasing attention has been given to non-invasive methods for evaluating and monitoring airway inflammation. In this context, exhaled breath has emerged as a valuable, non-invasive tool for collecting biological samples and assessing oxidative stress in respiratory diseases.4
Exhaled breath consists of a gaseous phase containing volatile organic compounds such as nitric oxide (NO), carbon monoxide (CO), ethane, and pentane, and a water-vapor phase containing aerosol particles. These particles can be condensed via a cooling system, resulting in what is known as exhaled breath condensate (EBC).5
EBC collection is completely non-invasive and repeatable It is typically performed during tidal breathing using a nose clip and saliva trap, under controlled temperature and collection time, with a condenser made of inert material and no resistance or filter between the subject and the device.6 It is a well-tolerated method and can be applied to both adult and pediatric populations, including patients with acute symptoms. Most important, since EBC collection does not involve bronchoprovocation, unlike sputum induction or bronchoscopy, it does not alter the degree of airway inflammation during the procedure.7
EBC contains various non-volatile substances, including markers of oxidative stress. Increased oxidative stress, resulting from an imbalance between the generation and scavenging of reactive oxygen species (ROS), such as hydrogen peroxide (H2O2), is a key mechanism in several inflammatory respiratory diseases, including asthma and COPD.8 For this reason, it has been suggested that the concentrations of these mediators in EBC may reflect the inflammatory status of the disease and may be modulated by therapeutic interventions.
ROS are oxygen-containing reactive molecules produced mainly by oxidant enzymes and are subsequently neutralized by scavenging systems, which include both enzymatic and non-enzymatic reactions. Under normal physiological conditions, ROS are generated in nearly every subcellular organelle within the cell9 including the plasma membrane, cytosol, endoplasmic reticulum, Golgi apparatus, mitochondria, nucleus and others.10
Some ROS are purposefully produced through enzymatic pathways, including lipoxygenases and cyclooxygenases, to carry out specific biological functions and regulate cellular homeostasis.11 Upon inflammatory stimuli, leukocytes and respiratory epithelial cells release ROS and reactive nitrogen species (RNS), disrupting intracellular redox balance and leading to oxidative stress and an increased production of ROS.12
H2O2 is a key oxidative metabolite commonly found in cells, tissues, and bodily secretions. Due to its small size and polarity, it freely diffuses across biological membranes. H2O2 is primarily produced through the dismutation of superoxide anions generated by activated inflammatory cells such as neutrophils, macrophages, and particularly eosinophils. Notably, H2O2 is volatile and can transition into the gaseous phase, making it detectable in exhaled air.13 During inflammatory processes, increased oxidative stress triggers respiratory bursts, resulting in excessive production of superoxide anions (O2−) and a subsequent rise in H2O2 levels.14
Beyond being a mere byproduct of oxidative metabolism, H2O2 acts as a signaling molecule, modulating cytokine production, leukocyte recruitment, and epithelial barrier function. Because of its volatility and ability to equilibrate with air, H2O2 can be measured non-invasively in EBC.
The current narrative review examines the major clinical studies in humans on the use of H2O2 in EBC as a non-invasive biomarker for assessing airway inflammation, highlighting its potential applications in disease diagnosis, monitoring and treatment response, and discussing factors influencing the variability of exhaled H2O2.
Methods
We conducted a comprehensive literature search using PubMed, Cochrane, Google Scholar, EMBASE, ISRCTN, MEDLINE, and Web of Science. Studies including patients of all ages were considered. We focused on observational studies, including longitudinal, cross-sectional, cohort, case-control, as well as randomized controlled trials, involving patients with respiratory diseases from whom exhaled H2O2 was collected. Only full-text articles published in English were included, while studies that did not involve breath sample collection or that assessed biomarkers other than exhaled H2O2 were excluded.
Two clinical researchers (NS and CG) independently reviewed all retrieved articles based on the predefined inclusion and exclusion criteria, with any discrepancies resolved through discussion with a third reviewer (SP) to reach consensus. Information extracted from each study included author, title, study population, disease type, analytical techniques, clinical application of exhaled H2O2, and key findings. References were managed using a reference management software, and all extracted data were organized in an Excel database maintained securely on University servers.
Study Characteristics
The included studies varied in terms of patient populations, analytical assays, and data normalization strategies. The main findings are summarized in Table 1 and extensively discussed. Populations ranged from pediatric to adult patients and encompassed different respiratory diseases, including asthma, COPD, bronchiectasis, and interstitial lung disease (Figure 1 and Table 2). Elevated H2O2 levels in EBC were consistently observed across these conditions, correlating with airway hyperresponsiveness and eosinophilic inflammation, as indicated by associations with eosinophil counts in induced sputum.15
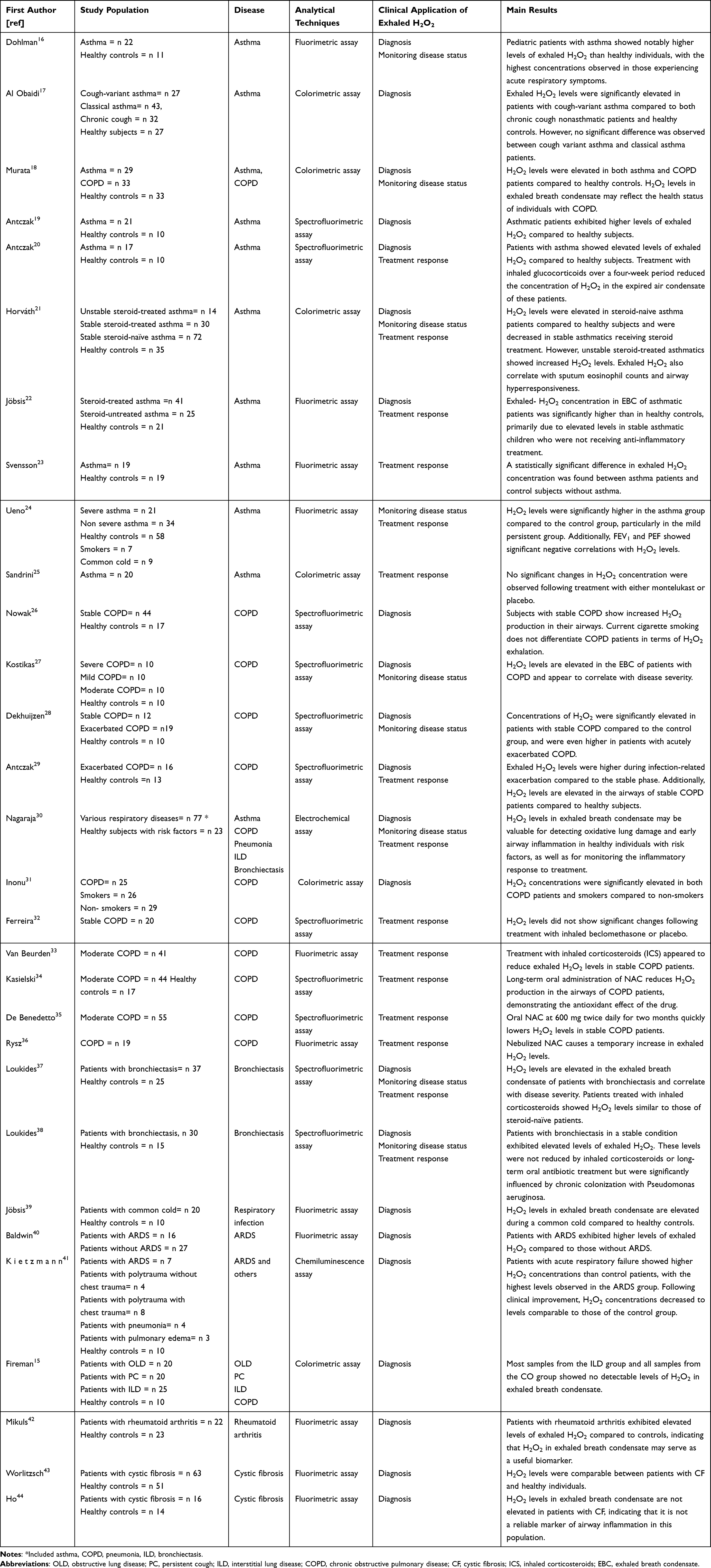 |
Table 1 Summary of the Main Studies and Principal Results |
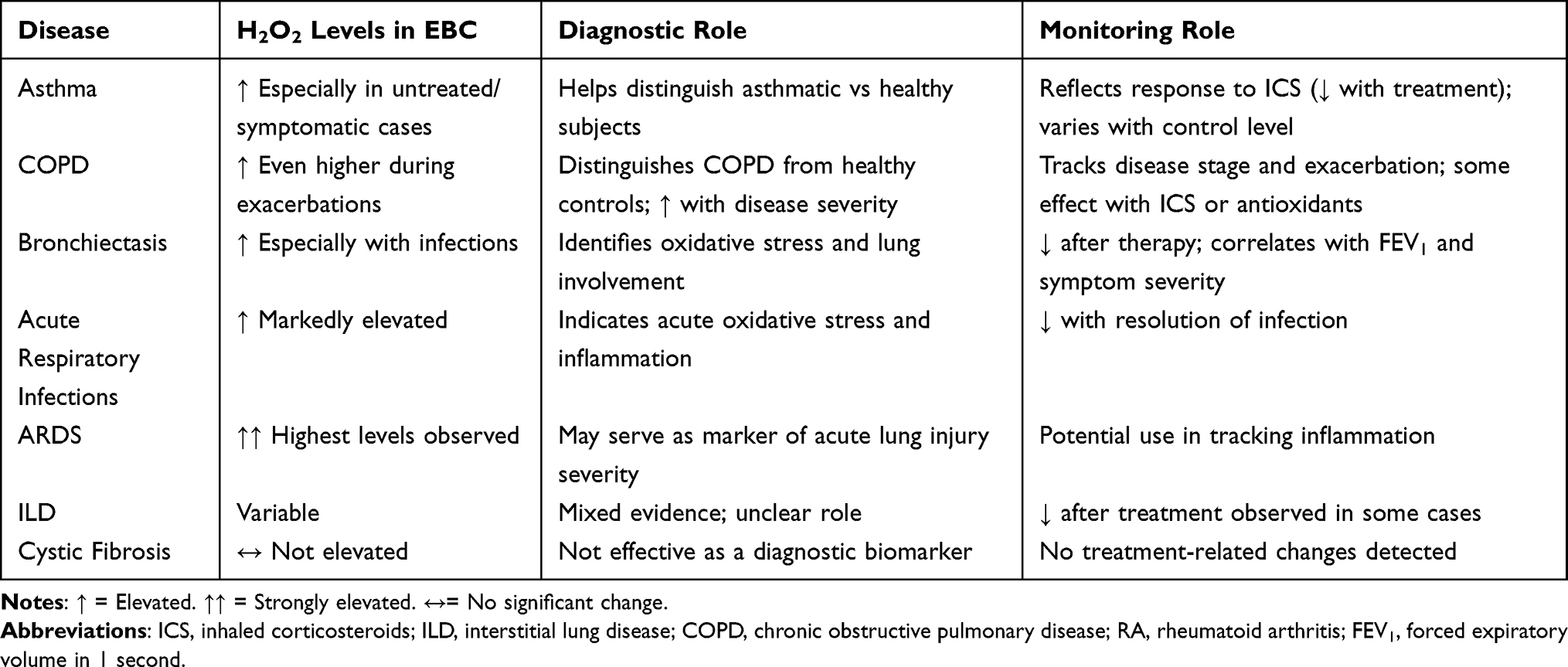 |
Table 2 Disease Group Summaries and Role of Exhaled- H2O2 |
 |
Figure 1 The schematic involvement of exhaled H2O2 in respiratory diseases. |
Analytical techniques for H2O2 quantification included the Amplex Red assay,45 as well as luminescent,46 colorimetric,47 magnetic resonance-based48 and electrochemical49 approaches.
Variations in sample collection, normalization strategies, and reporting units contributed to heterogeneity among studies. These differences were carefully recorded and considered in synthesizing the results, allowing for a nuanced interpretation of the clinical significance of exhaled H2O2.
The Significance and Clinical Implication of Exhaled H2O2 in Respiratory Disease
Diagnostic Potential of Exhaled H2O2 in Asthma
In the context of asthma, oxidative stress exerts multiple harmful effects, including lung tissue injury, bronchial hyperresponsiveness, epithelial cell damage and apoptosis, enhanced pro-inflammatory responses, inactivation of antioxidant enzymes, airflow obstruction, and increased mucus production. These changes significantly contribute to both disease severity and chronic progression.
Several studies have investigated the potential role of H2O2 as a non-invasive biomarker for distinguishing asthmatic patients from healthy individuals. One of the earliest contributions16 assessed exhaled H2O2 levels in a cohort of 33 children. The study demonstrated that pediatric asthma patients exhibited significantly higher concentrations of exhaled H2O2 compared to healthy controls, with even greater levels observed in asthmatic individuals presenting with acute respiratory symptoms, involving both upper and lower airway infections. Although pulmonary function test results showed a marked deterioration from baseline in some patients, the correlation between impaired lung function and elevated H2O2 concentrations in exhaled breath condensate was not statistically significant. Other studies17–19 have since confirmed the finding that exhaled H2O2 concentrations are significantly higher in both adult and pediatric asthmatic patients compared to healthy individuals, particularly among those who are untreated. Moreover, all of the cited studies reported no significant correlation between exhaled H2O2 levels and FEV1, suggesting that H2O2 concentration may not directly reflect disease severity. In contrast, Antczak et al20 had previously demonstrated a strong inverse correlation between exhaled H2O2 concentration and FEV1% predicted, which may be explained by the role of reactive oxygen species in promoting bronchial hyperresponsiveness and subsequent bronchoconstriction.
Notably, exhaled H2O2 has also been investigated as a potential biomarker to distinguish between different asthma phenotypes. In a cross-sectional study,21 patients with cough variant asthma exhibited higher levels of H2O2 compared to those with non-asthmatic chronic cough and healthy controls. However, no significant differences in exhaled H2O2 were observed between patients with cough variant asthma and those with classical asthma.
Monitoring Asthma Status and Treatment Response
Many studies have utilized exhaled H2O2 to monitor asthma status and evaluate the effects of disease-modifying treatments, such as corticosteroids and other anti-inflammatory agents, on airway oxidative stress in asthmatic patients. Jobsis et al22 demonstrated that exhaled H2O2 levels were significantly elevated in asthmatic children not receiving anti-inflammatory treatment compared to healthy controls. In contrast, although asthmatic children treated with corticosteroids also exhibited higher H2O2 levels than healthy controls, this difference was not statistically significant. These findings have been supported by several other studies, which confirmed that treatment with inhaled corticosteroids (ICS) significantly reduces exhaled H2O2 concentrations. ICS-treated asthmatic patients consistently exhibit lower levels of exhaled H2O2 compared to steroid-naïve individuals.21,23,24 Notably, Antczak et al20 reported a significant decrease in H2O2 concentrations in EBC after four weeks of ICS therapy, as compared to a placebo group, suggesting a rapid anti-inflammatory response to ICS treatment associated with a reduction in oxidative stress markers.
Horváth et al21 analyzed subgroups of asthmatic patients based on disease control status and found that exhaled H2O2 levels were reduced in steroid-treated patients with stable asthma. In contrast, patients with unstable asthma exhibited persistently elevated H2O2 levels despite corticosteroid therapy, suggesting that oxidative stress may remain uncontrolled in certain cases of poorly managed asthma. This contrasts with the findings of Ueno et al24 who reported that H2O2 levels were lower in patients with severe asthma compared to those with mild persistent asthma. Moreover, the effect of montelukast on exhaled H2O2 has also been studied.25 No significant changes in the concentration of H2O2 were detected with either montelukast or placebo treatment, suggesting that montelukast may not significantly influence airway oxidative stress as measured by exhaled H2O2.
Diagnostic Potential of Exhaled H2O2 in COPD
A crucial aspect of COPD pathogenesis is the imbalance between proteolytic enzymes, such as elastase, and their inhibitors, notably α1-antitrypsin. The interplay between exogenous factors, such as cigarette smoke, environmental pollution, prior infections, and occupational exposures, and endogenous factors, including airway hyperreactivity, antioxidant capacity, genetic predisposition, age, and sex, explains the heterogeneity observed in COPD development.50 Similarly, an imbalance between the production of reactive oxygen and nitrogen species (ROS/RNS) and the capacity of antioxidant defenses results in oxidative and nitrosative stress.51 This stress causes damage to cellular components, thereby contributing to both the severity and chronic progression of the disease.
Various studies have demonstrated the ability of exhaled H2O2 in EBC to distinguish patients with COPD from healthy subjects. In particular, it has been shown that patients with COPD typically exhibit higher levels of exhaled H2O2 compared to healthy controls,26,27 and its production further increases during exacerbations28–30 according to the increase of oxidative stress. In addition to differentiating COPD patients from healthy subjects, exhaled H2O2 has been linked with clinical parameters. Significant correlations have been observed between exhaled H2O2 levels and lung function as measured by FEV1, neutrophil count in induced sputum, and dyspnea severity (MRC scale) were observed. Notably, these associations were present only in patients with moderate to severe disease, highlighting the potential role of H2O2 as a biomarker of disease progression and severity.27 Moreover, Inonu et al31 showed that H2O2 levels in EBC were similar between smokers and COPD patients, and both were higher than those in non-smokers, suggesting that the oxidant burden in the lungs of smokers is comparable to that in COPD patients.
Monitoring COPD Status and Treatment Response
The potential role of H2O2 in monitoring COPD status and treatment response has been explored in several pilot studies. Specifically, H2O2 levels in EBC have been investigated in patients with stable versus unstable COPD, revealing that H2O2 concentrations are higher in unstable COPD patients compared to those with stable disease, although the latter still exhibit elevated levels compared to healthy subjects.27 Similarly, patients with moderate and severe COPD show increased H2O2 levels relative to those with mild disease, indicating a correlation between H2O2 concentration and disease severity.28 Murata et al18 also identified a significant correlation between COPD Assessment Test (CAT) scores and H2O2 levels in COPD patients, further linking exhaled H2O2 concentrations to patient-reported health status.
The effects of COPD treatments on H2O2 levels in EBC are variable. One study reported that ICS therapy did not significantly affect H2O2 concentrations.32 Conversely, Van Beurden et al33 demonstrated that ICS treatment reduced H2O2 levels in EBC, with no return to baseline values after a second washout period, suggesting a possible carry-over effect. Moreover, the impact of antibiotic therapy during infectious exacerbations29 and long-term oral N-acetylcysteine treatment34,35 on exhaled H2O2 levels has also been evaluated. These studies demonstrated a reduction in H2O2 concentrations in EBC, although levels in stable COPD patients remained higher than those in healthy controls. Conversely, nebulized N-acetylcysteine administration in stable COPD patients resulted in a transient increase in exhaled H2O2 levels, indicating a mild pro-oxidant effect.36
Other Respiratory Diseases
The ability of H2O2 to assess airway inflammation and monitor treatment response has been demonstrated in a variety of respiratory diseases beyond asthma and COPD. Studies have found higher concentrations of H2O2 in the EBC of patients with bronchiectasis compared to healthy subjects, indicating enhanced oxidative stress in these patients. Moreover, a significant negative correlation has been observed between H2O2 levels and lung function, as assessed by FEV1, suggesting a strong inverse relationship between oxidative stress and disease severity.30,37 Later studies confirmed these preliminary findings, further reporting that higher H2O2 levels are observed in patients with Pseudomonas aeruginosa colonization, in those receiving long-term oral antibiotic therapy, and in patients with more severe symptoms.38 Moreover, elevated levels of exhaled H2O2 have been detected in acute respiratory infections39 and in various types of acute lung diseases, particularly in patients with ARDS.40
Patients with acute lung infiltrates, whether focal or diffuse, showed significantly higher H2O2 concentrations compared to healthy controls, with the highest median levels observed in the ARDS group.41
Whereas data regarding interstitial lung disease (ILD) remain controversial, a pilot study15 reported no significant difference in H2O2 concentrations in EBC between ILD patients and healthy controls. Conversely, another pilot study by Mikuls et al42 found increased levels of exhaled H2O2 in patients with rheumatoid arthritis-associated ILD compared to healthy controls, suggesting that H2O2 could be a potentially useful biomarker.
Contrary to findings in other respiratory diseases, studies conducted on cystic fibrosis have consistently shown that no elevated levels of H2O2 are detected in EBC, suggesting that H2O2 may not serve as a reliable marker of inflammation in this specific condition.43,44
The potential of H2O2 as a biomarker for monitoring treatment response in various respiratory diseases has been investigated. In particular, Nagaraja et al30 evaluated the inflammatory response to treatment by comparing exhaled H2O2 levels before and after therapeutic intervention. Their findings demonstrated a significant decrease in H2O2 levels following treatment in patients with asthma, COPD, bronchiectasis, pneumonia and interstitial lung disease, supporting the potential of exhaled H2O2 as a non-invasive biomarker for assessing inflammatory response to treatment in respiratory conditions.
Factors Influencing the Variability in Exhaled H2O2 Concentration
Several factors may influence H2O2 concentration in EBC; the key results are summarized in Table 3.
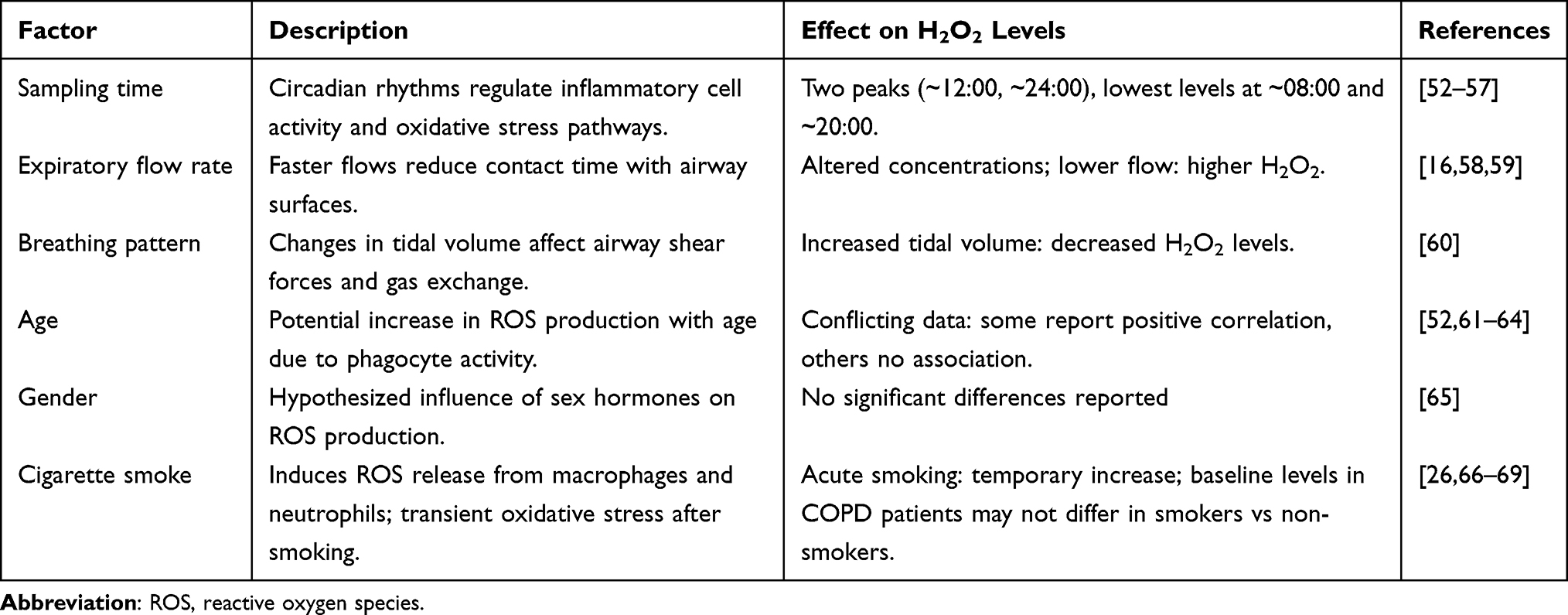 |
Table 3 Factors Influencing the Variability in Exhaled H2O2 Concentration |
Diurnal Variability
Several studies have investigated the circadian rhythm of exhaled H2O2, demonstrating a distinct diurnal pattern characterized by fluctuations in H2O2 levels throughout the day. In particular, Nowak et al52 reported two peak concentrations occurring around 12:00 and 24:00 hours, with the lowest levels observed at approximately 08:00 and 20:00 hours. A plausible explanation for this variation lies in the circadian regulation of inflammatory cell activity.53 Specifically, phagocytes and airway epithelial cells, both key sources of H2O2, undergo fluctuations in number and function throughout the day. These rhythmic changes may contribute directly to the temporal variations in exhaled H2O2 levels.
Moreover, circadian variations have been reported in several biological mechanisms relevant to oxidative stress and inflammation, including the expression of leukocyte receptors54 circulating levels of adhesion molecules55 and overall antioxidant capacity.56 These interrelated factors likely underlie the observed circadian fluctuations in exhaled H2O2 concentrations, as documented both in healthy individuals and in patients with chronic inflammatory airway diseases, such as COPD.57
Flow Rate and Breathing Pattern Variability
The influence of respiratory parameters, such as expiratory flow rate and breathing pattern, on the concentration of H2O2 in EBC has been evaluated. In a explorative study, Schleiss et al58 demonstrated that faster expiratory flow rates resulted in altered H2O2 concentrations, suggesting that exhaled H2O2 is primarily generated within the bronchial airways, with minimal alveolar contribution. The same study also highlighted the role of length of expiration: when a fixed volume of air is collected, lower flow rates, leading to longer expiration times, were associated with higher H2O2 concentrations.59 However, this finding remains controversial, as other studies have reported no significant correlation between H2O2 levels and expiratory flow rate.16 Additionally, breathing pattern has been shown to affect H2O2 concentrations; specifically, an increase in tidal volume was associated with a significant decrease in H2O2 levels across all subjects.60
Gender and Age Influence
The relationship between exhaled H2O2 and age has been investigated in several studies, producing conflicting results. Research conducted in pediatric population evaluated H2O2 concentrations in EBC and found no evidence of age dependence.61,62 In contrast, Nowak et al52 reported a positive correlation between H2O2 levels and age in never-smokers, attributing this to an age-related increase in ROS production by activated phagocytes, as supported by recent findings.63 However, Jobsis et al64 noted that their control group was not age-matched, suggesting that age-related differences in exhaled H2O2 might have influenced their results. Nonetheless, they argued that it is unlikely that healthy children produce more ROS in their airways than healthy young adults. They emphasized the need for future studies to establish normative reference values for exhaled H2O2 across a broad age range.
In addition to age, the potential influence of gender on exhaled H2O2 has been investigated, based on the hypothesis that sex hormones may modulate the production of this inflammatory mediator. However, no significant effect of gender on H2O2 concentrations has been documented.65
Influence of Cigarette Smoke
Although cigarette smoke contains high levels of oxidants, the hydrogen peroxide detected in EBC does not appear to originate directly from the smoke itself.26 Rather, cigarette smoke stimulates alveolar macrophages and polymorphonuclear leukocytes to release ROS, including H2O2. This mechanism provides the rationale for investigating the effect of tobacco smoking on exhaled H2O2 levels in various populations.
In healthy subjects, cigarette smoking has been shown to increase H2O2 concentrations in EBC, accompanied by enhanced neutrophil chemotactic activity.66 However, Guatura et al67 observed that although there was a significant rise in mean exhaled H2O2 levels 30 minutes after smoking a single cigarette, baseline H2O2 levels were similar between smokers and non-smokers. This suggests that in healthy individuals smoking induces a transient increase in airway oxidative stress, which may return to baseline within a few hours of abstinence. Additionally, in asthmatic patients, acute cigarette smoking causes a slight decrease in exhaled NO concentration, which is associated with an increase in exhaled H2O2 levels. This rise in H2O2 indicates an acute release of reactive oxygen species in the airways, potentially leading to enhanced formation of peroxynitrite, a reactive nitrogen species, hat may contribute to the observed reduction in exhaled NO.68
In patients with COPD, studies have not demonstrated significant differences in exhaled H2O2 levels between smokers and ex-smokers, suggesting a possible saturation effect or disease-related ceiling in oxidative biomarker expression.69
Future Research Direction
Future research in this field should focus on several key areas to advance our understanding and clinical application of EBC biomarkers. Notably, recent evidence on exhaled H2O2 remains limited, highlighting a clear gap in current knowledge and emphasizing the need for updated and rigorous research.
First, it is important to establish reference values for the various inflammatory biomarkers in healthy individuals. This baseline is essential to interpret changes observed in disease states accurately. Second, studies assessing the reproducibility of these measurements are needed to ensure reliability and consistency across different settings and times. Additionally, large-scale longitudinal studies will be crucial to observe how these biomarkers fluctuate over time and correlate with disease progression or response to treatment. Another important direction is to explore how EBC markers relate to clinical symptoms, lung function tests, and other established methods for measuring airway inflammation, which will help clarify their clinical significance. Finally, a deeper understanding of the mechanisms behind the formation of EBC and its relationship to the airway lining fluid is necessary. This knowledge will improve the interpretation of EBC findings and their connection to underlying airway pathology. Overall, progress in this area depends on conducting rigorous studies focused on reproducibility, developing more sensitive and specific assays for detecting mediators, and establishing standardized normal values. This is especially important given that many laboratories currently report inconsistent results for the same biomarkers, highlighting the need for greater harmonization and methodological refinement.
Conclusions
This umbrella review outlines the promising potential of exhaled H2O2 as a biomarker in inflammatory lung diseases. Measurements of exhaled H2O2 in EBC provide valuable insights into the pathophysiology of inflammatory lung diseases. Thanks to its completely noninvasive nature, EBC is suitable for repeated measurements, offering information on airway inflammation both during stable phases of the disease and exacerbations. Furthermore, in pediatric populations, noninvasive techniques to assess airway inflammation are essential, given the limitations of relying mainly on symptoms and lung function tests to evaluate the patient’s underlying pathobiological state.
Although EBC mainly consists of water vapor with other chemical compounds present in trace amounts, modern highly sensitive diagnostic tests enable effective analysis of these samples. Exhaled H2O2 in EBC has shown great potential in distinguishing patients with inflammatory airway diseases such as asthma or COPD from healthy subjects.
Given the complex pathophysiology of these conditions, H2O2 may be even more informative when used as part of a multimodal biomarker panel, complementing other physiological and biochemical measures.
However, the interpretation of H2O2 levels remains controversial, with heterogeneity across studies likely due to differences in methodology, patient populations, and analytical techniques.
Additionally, H2O2 levels correlate strongly with disease severity, disease control, and response to conventional treatments across various respiratory diseases. However, most studies analyzing the effects of therapies on exhaled H2O2 are observational; therefore, controlled trials are needed to evaluate its utility in specific disease management.
Nevertheless, the clinical use of exhaled H2O2 is limited by high variability in measurements influenced by factors such as diurnal variation, breathing pattern, and flow rate. Several methodological challenges also need to be addressed, including the standardization of sample collection, validation of analytical techniques, and harmonization of the diverse collection devices, which vary significantly in efficiency.70
In conclusion, although measurement of exhaled H2O2 is not yet a routine clinical practice for guiding respiratory disease management, it remains a promising tool with expected broader adoption. Notably, a significant gap exists in recent evidence, highlighting the need for up-to-date research to validate the clinical relevance and reproducibility of exhaled H2O2. Despite encouraging preliminary results, technical limitations and unresolved methodological issues need to be resolved. Further research is required to firmly establish the clinical role of H2O2 in EBC before recommending this technique for routine respiratory care.
With rapid technological advancements, more compact, user-friendly, and precise analyzers for EBC assessment are expected to become available soon, facilitating the diagnosis and monitoring of disease activity in patients with asthma and other inflammatory airway conditions.
Data Sharing Statement
Data will be made available on reasonable request from the corresponding author.
Acknowledgments
In rare case of ambiguity in the text, generative AI (ChatGPTversion 4) was employed to provide contextual clarification where the meaning was not explicitly clear. The AI tool was not used for literature classification, idea generation, writing or preparation.
Author Contributions
CG wrote the original draft, was responsible for the data curation and the methodology applied to the paper. AB and SP supervised the paper, validated and edited the original draft. NS was responsible for the conceptualization of the paper, supervised the paper, and edited the original draft. All authors approved the final version of the paper. All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper was not funded.
Disclosure
C. Gagliani, N. Scichilone, A. Benfante have nothing to disclose. S. Principe received Unrestricted Grant from European Union’s HORIZON Research and Innovation program and Unrestricted Grant from Innovative Medicines Initiative 2 Joint Undertaking (JU). The authors declare that they have no other conflicts of interest.
References
1. Jeffery PK, Laitinen A, Venge P. Biopsy markers of airway inflammation and remodelling. Respir Med. 2000;
2. Reynolds HY. Use of bronchoalveolar lavage in humans—past necessity and future imperative. Lung. 2000;178(5):271–15. doi:10.1007/s004080000032
3. Holz O, Kips J, Magnussen H. Update on sputum methodology. Eur Respir J. 2000;16(2):355. doi:10.1034/j.1399-3003.2000.16b26.x
4. Ahmadzai H, Huang S, Hettiarachchi R, Lin JL, Thomas PS, Zhang Q. Exhaled breath condensate: a comprehensive update. Clin Chem Lab Med. 2013;51(7). doi:10.1515/cclm-2012-0593
5. Horváth I, Barnes PJ, Loukides S, et al. A European respiratory society technical standard: exhaled biomarkers in lung disease. Eur Respir J. 2017;49(4):1600965. doi:10.1183/13993003.00965-2016
6. Horváth I, Hunt J, Barnes PJ. Exhaled breath condensate: methodological recommendations and unresolved questions. Eur Respir J. 2005;26(3):523–548. doi:10.1183/09031936.05.00029705
7. Davis MD, Montpetit A, Hunt J. Exhaled breath condensate. Immunol Allergy Clin North Am. 2012;32(3):363–375. doi:10.1016/j.iac.2012.06.014
8. Winterbourn CC. Reconciling the chemistry and biology of reactive oxygen species. Nat Chem Biol. 2008;4(5):278–286. doi:10.1038/nchembio.85
9. Gupta DK, Palma JM, Corpas FJ,eds..Reactive Oxygen Species and Oxidative Damage in Plants Under Stress.Springer International Publishing;2015. doi:10.1007/978-3-319-20421-5
10. Ahsan H, Ali A, Ali R. Oxygen free radicals and systemic autoimmunity. Clin Exp Immunol. 2003;131(3):398–404. doi:10.1046/j.1365-2249.2003.02104.x
11. Kozlov AV, Javadov S, Sommer N. Cellular ROS and antioxidants: physiological and pathological role. Antioxidants. 2024;13(5):602. doi:10.3390/antiox13050602
12. Mittal M, Siddiqui MR, Tran K, Reddy SP, Malik AB. Reactive oxygen species in inflammation and tissue injury. Antioxid Redox Signal. 2014;20(7):1126–1167. doi:10.1089/ars.2012.5149
13. Conner GE, Salathe M, Forteza R. Lactoperoxidase and hydrogen peroxide metabolism in the airway. Am J Respir Crit Care Med. 2002;166(supplement_1):S57–S61. doi:10.1164/rccm.2206018
14. Bajaj P, Ishmael FT. Exhaled breath condensates as a source for biomarkers for characterization of inflammatory lung diseases. J Anal Sci Methods Instrum. 2013;03(01):17–29. doi:10.4236/jasmi.2013.31004
15. Fireman E, Shtark M, Priel IE, et al. Hydrogen peroxide in Exhaled Breath Condensate (EBC) vs eosinophil count in Induced Sputum (IS) in parenchymal vs airways lung diseases”. Inflammation. 2007;30(1–2):44–51. doi:10.1007/s10753-007-9020-8
16. Dohlman AW, Black HR, Royall JA. Expired breath hydrogen peroxide is a marker of acute airway inflammation in pediatric patients with asthma. Am Rev Respir Dis. 1993;148(4_pt_1):955–960. doi:10.1164/ajrccm/148.4_Pt_1.955
17. Ahmad Al Obaidi A. Expired breath condensate hydrogen peroxide concentration and pH for screening cough variant asthma among chronic cough. Ann Thorac Med. 2007;2(1):18. doi:10.4103/1817-1737.30357
18. Murata K, Fujimoto K, Kitaguchi Y, Horiuchi T, Kubo K, Honda T. Hydrogen peroxide content and pH of expired breath condensate from patients with asthma and COPD. COPD J Chronic Obstr Pulm Dis. 2014;11(1):81–87. doi:10.3109/15412555.2013.830094
19. Antczak A, Nowak D, Shariati B, Krol M, Piasecka G, Kurmanowska Z. Increased hydrogen peroxide and thiobarbituric acid-reactive products in expired breath condensate of asthmatic patients. Eur Respir J. 1997;10(6):1235–1241. doi:10.1183/09031936.97.10061235
20. Antczak A, Kurmanowska Z, Kasielski M, Nowak D. Inhaled glucocorticosteroids decrease hydrogen peroxide level in expired air condensate in asthmatic patients. Respir Med. 2000;94(5):416–421. doi:10.1053/rmed.1999.0801
21. Horváth I, Donnelly LE, Kiss A, et al. Combined use of exhaled hydrogen peroxide and nitric oxide in monitoring asthma. Am J Respir Crit Care Med. 1998;158(4):1042–1046. doi:10.1164/ajrccm.158.4.9710091
22. Jöbsis Q, Raatgeep HC, Hermans PW, de Jongste JC. Hydrogen peroxide in exhaled air is increased in stable asthmatic children. Eur Respir J. 1997;10(3):519–521.
23. Svensson S, Olin A, Larstad M, Ljungkvist G, Toren K. Determination of hydrogen peroxide in exhaled breath condensate by flow injection analysis with fluorescence detection. J Chromatogr B. 2004;809(2):199–203. doi:10.1016/S1570-0232(04)00513-6
24. Ueno T, Kataoka M, Hirano A, et al. Inflammatory markers in exhaled breath condensate from patients with asthma. Respirology. 2008;13(5):654–663. doi:10.1111/j.1440-1843.2008.01315.x
25. Sandrini A, Ferreira IM, Gutierrez C, Jardim JR, Zamel N, Chapman KR. Effect of montelukast on exhaled nitric oxide and nonvolatile markers of inflammation in mild asthma. Chest. 2003;124(4):1334–1340. doi:10.1378/chest.124.4.1334
26. Nowak D, Kasielski M, Antczak A, Pietras T, Bialasiewicz P. Increased content of thiobarbituric acid-reactive substances and hydrogen peroxide in the expired breath condensate of patients with stable chronic obstructive pulmonary disease: no significant effect of cigarette smoking. Respir Med. 1999;93(6):389–396. doi:10.1053/rmed.1999.0574
27. Kostikas K, Papatheodorou G, Psathakis K, Panagou P, Loukides S. Oxidative stress in expired breath condensate of patients with COPD. Chest. 2003;124(4):1373–1380. doi:10.1378/chest.124.4.1373
28. Dekhuijzen PN, Aben KK, Dekker I, et al. Increased exhalation of hydrogen peroxide in patients with stable and unstable chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1996;154(3):813–816. doi:10.1164/ajrccm.154.3.8810624
29. Antczak A, Ciebiada M, Pietras T, Piotrowski WJ, Kurmanowska Z, Górski P. Exhaled eicosanoids and biomarkers of oxidative stress in exacerbation of chronic obstructive pulmonary disease. Arch Med Sci. 2012;2:277–285. doi:10.5114/aoms.2012.28555
30. Nagaraja C, Shashibhushan B, Sagar Asif M, Manjunath P. Hydrogen peroxide in exhaled breath condensate: a clinical study. Lung India. 2012;29(2):123. doi:10.4103/0970-2113.95303
31. Inonu H, Doruk S, Sahin S, et al. Oxidative stress levels in exhaled breath condensate associated with COPD and smoking. Respir Care. 2012;57(3):413–419. doi:10.4187/respcare.01302
32. Ferreira IM, Hazari MS, Gutierrez C, Zamel N, Chapman KR. Exhaled nitric oxide and hydrogen peroxide in patients with chronic obstructive pulmonary disease: effects of inhaled beclomethasone. Am J Respir Crit Care Med. 2001;164(6):1012–1015. doi:10.1164/ajrccm.164.6.2012139
33. Van Beurden WJC, Harff GA, Dekhuijzen PNR, Van Der Poel-Smet SM, Smeenk FWJM. Effects of inhaled corticosteroids with different lung deposition on exhaled hydrogen peroxide in stable COPD patients. Respiration. 2003;70(3):242–248. doi:10.1159/000072004
34. Kasielski M, Nowak D. Long-term administration of N-acetylcysteine decreases hydrogen peroxide exhalation in subjects with chronic obstructive pulmonary disease. Respir Med. 2001;95(6):448–456. doi:10.1053/rmed.2001.1066
35. De Benedetto F, Aceto A, Dragani B, et al. Long-term oral n-acetylcysteine reduces exhaled hydrogen peroxide in stable COPD. Pulm Pharmacol Ther. 2005;18(1):41–47. doi:10.1016/j.pupt.2004.09.030
36. Rysz J, Stolarek RA, Luczynski R, et al. Increased hydrogen peroxide concentration in the exhaled breath condensate of stable COPD patients after nebulized N-acetylcysteine. Pulm Pharmacol Ther. 2007;20(3):281–289. doi:10.1016/j.pupt.2006.03.011
37. Loukides S, Horvath I, Wodehouse T, Cole PJ, Barnes PJ. Elevated levels of expired breath hydrogen peroxide in bronchiectasis. Am J Respir Crit Care Med. 1998;158(3):991–994. doi:10.1164/ajrccm.158.3.9710031
38. Loukides S, Bouros D, Papatheodorou G, Lachanis S, Panagou P, Siafakas NM. Exhaled H2O2 in steady-state bronchiectasis. Chest. 2002;121(1):81–87. doi:10.1378/chest.121.1.81
39. Jöbsis RQ, Schellekens SL, Fakkel-Kroesbergen A, Raatgeep RHC, De Jongste JC. Hydrogen peroxide in breath condensate during a common cold. Mediators Inflamm. 2001;10(6):351–354. doi:10.1080/09629350120102398
40. Baldwin Stephen R, Grum Cyril M, Boxer Laurence A, Simon Richard H, Ketai Loren H, Devall Larry J. Oxidant activity in expired breath of patients with adult respiratory distress syndrome. Lancet. 1986;327(8471):11–14. doi:10.1016/S0140-6736(86)91895-7
41. Kietzmann D, Kahl R, Müller M, Burchardi H, Kettler D. Hydrogen peroxide in expired breath condensate of patients with acute respiratory failure and with ARDS. Intensive Care Med. 1993;19(2):78–81. doi:10.1007/BF01708366
42. Mikuls TR, O’Dell JR, Ertl R, Bergman DA, Rennard SI. Examining the exhaled levels of hydrogen peroxide in rheumatoid arthritis: a pilot study. Ann Rheum Dis. 2006;65(9):1252–1253. doi:10.1136/ard.2005.050641
43. Worlitzsch D, Herberth G, Ulrich M, Doring G. Catalase, myeloperoxidase and hydrogen peroxide in cystic fibrosis. Eur Respir J. 1998;11(2):377–383. doi:10.1183/09031936.98.11020377
44. Ho L, Faccenda J, Innes J, Greening A. Expired hydrogen peroxide in breath condensate of cystic fibrosis patients. Eur Respir J. 1999;13(1):103–106. doi:10.1183/09031936.99.13110399
45. Koczulla R, Dragonieri S, Schot R, et al. Comparison of exhaled breath condensate pH using two commercially available devices in healthy controls, asthma and COPD patients. Respir Res. 2009;10(1):78. doi:10.1186/1465-9921-10-78
46. Honour JW. Gas chromatography-mass spectrometry. In: Wheeler MJ, Hutchinson JSM editors. Hormone Assays in Biological Fluids. Humana Press; 2006:53–74. doi:10.1385/1-59259-986-9:53
47. Langford VS, Graves I, McEwan MJ. Rapid monitoring of volatile organic compounds: a comparison between gas chromatography/mass spectrometry and selected ion flow tube mass spectrometry. Rapid Commun Mass Spectrom. 2014;28(1):10–18. doi:10.1002/rcm.6747
48. Brinkman P, van Zee AHMD, Wagener AH. Breathomics and treatable traits for chronic airway diseases. Curr Opin Pulm Med. 2019;25(1):94–100. doi:10.1097/MCP.0000000000000534
49. Paredi P, Kharitonov SA, Barnes PJ. Correlation of exhaled breath temperature with bronchial blood flow in asthma. Respir Res. 2005;6(1):15. doi:10.1186/1465-9921-6-15
50. Koyama H, Geddes DM. Genes, oxidative stress, and the risk of chronic obstructive pulmonary disease. Thorax. 1998;53(Supplement 2):S10–S14. doi:10.1136/thx.53.2008.S10
51. Aruoma OI. Free radicals, oxidative stress, and antioxidants in human health and disease. J Am Oil Chem Soc. 1998;75(2):199–212. doi:10.1007/s11746-998-0032-9
52. Nowak D, Kałucka S, Białasiewicz P, Król M. Exhalation of H2O2 and thiobarbituric acid reactive substances (TBARs) by healthy subjects. Free Radic Biol Med. 2001;30(2):178–186. doi:10.1016/S0891-5849(00)00457-3
53. Gibbs J, Ince L, Matthews L, et al. An epithelial circadian clock controls pulmonary inflammation and glucocorticoid action. Nat Med. 2014;20(8):919–926. doi:10.1038/nm.3599
54. Xu RB, Liu ZM, Zhao Y. A study on the circadian rhythm of glucocorticoid receptor. Neuroendocrinology. 1991;53(1):31–36. doi:10.1159/000125792
55. Maple C, Kirk G, McLaren M, Veale D, Belch JJF. A circadian variation exists for soluble levels of intercellular adhesion molecule-I and E-selectin in healthy volunteers. Clin Sci. 1998;94(5):537–540. doi:10.1042/cs0940537
56. Wilking M, Ndiaye M, Mukhtar H, Ahmad N. Circadian rhythm connections to oxidative stress: implications for human health. Antioxid Redox Signal. 2013;19(2):192–208. doi:10.1089/ars.2012.4889
57. Van Beurden WJC, Dekhuijzen PNR, Harff GA, Smeenk FWJM. Variability of exhaled hydrogen peroxide in stable COPD patients and matched healthy controls. Respiration. 2002;69(3):211–216. doi:10.1159/000063622
58. Gajdocsi R, Bikov A, Antus B, Horvath I, Barnes PJ, Kharitonov SA. Assessment of reproducibility of exhaled hydrogen peroxide concentration and the effect of breathing pattern in healthy subjects. J Aerosol Med Pulm Drug Deliv. 2011;24(6):271–275. doi:10.1089/jamp.2011.0875
59. Exhaled breath condensate- methodological recommendations and unresolved questions.pdf.
60. Assessment of reproducibility of exhaled hydrogen peroxide concentration and the effect of breathing pattern in healthy subjects.pdf.
61. Griese M, Latzin P, Beck J. A noninvasive method to collect nasally exhaled air condensate in humans of all ages. Eur J Clin Invest. 2001;31(10):915–920. doi:10.1046/j.1365-2362.2001.00875.x
62. Expired breath hydrogen peroxide is a marker of acute airway inflammation in pediatric patients with asthma.pdf.
63. Giorgi C, Marchi S, Simoes ICM, et al. Mitochondria and Reactive Oxygen Species in Aging and Age-Related Diseases. In: International Review of Cell and Molecular Biology. Vol. 340. Elsevier; 2018:209–344. doi:10.1016/bs.ircmb.2018.05.006
64. Jobsis Q, Raatgeep H, Schellekens S, Hop W, Hermans P, De Jongste J. Hydrogen peroxide in exhaled air of healthy children: reference values. Eur Respir J. 1998;12(2):483–485. doi:10.1183/09031936.98.12020483
65. Gessner C, Kuhn H, Seyfarth HJ, et al. Factors influencing breath condensate volume. Pneumologie. 2001;55(9):414–419. doi:10.1055/s-2001-16947
66. Nowak D, Antczak A, Krol M, et al. Increased content of hydrogen peroxide in the expired breath of cigarette smokers. Eur Respir J. 1996;9(4):652–657. doi:10.1183/09031936.96.09040652
67. Guatura SB, Martinez JAB, Bueno PCDS, Santos MLD. Increased exhalation of hydrogen peroxide in healthy subjects following cigarette consumption. Sao Paulo Med J. 2000;118(4):93–98. doi:10.1590/S1516-31802000000400004
68. Horváth I, Donnelly LE, Kiss A, Balint B, Kharitonov SA, Barnes PJ. Exhaled nitric oxide and hydrogen peroxide concentrations in asthmatic smokers. Respiration. 2004;71(5):463–468. doi:10.1159/000080630
69. Nowak D, Kasielski M, Pietras T, Białasiewicz P, Antczak A. Cigarette smoking does not increase hydrogen peroxide levels in expired breath condensate of patients with stable COPD. Monaldi Arch Chest Dis Arch Monaldi Mal Torace. 1998;53(3):268–273.
70. Effros RM, Biller J, Foss B, et al. A simple method for estimating respiratory solute dilution in exhaled breath condensates. Am J Respir Crit Care Med. 2003;168(12):1500–1505. doi:10.1164/rccm.200307-920OC
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.