Back to Journals » Clinical Ophthalmology » Volume 17
The Feasibility of an Educational Cartoon Video for Improving Adherence with Amblyopia Treatment in Children
Authors Aljohani S ![]() , Wang J, Scheiman M, Tan QQ
, Wang J, Scheiman M, Tan QQ ![]() , Xu H, Almutairi N, Alshammeri S
, Xu H, Almutairi N, Alshammeri S
Received 5 April 2023
Accepted for publication 31 May 2023
Published 7 June 2023 Volume 2023:17 Pages 1639—1646
DOI https://doi.org/10.2147/OPTH.S415892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saeed Aljohani,1 Jingyun Wang,2 Mitchell Scheiman,3 Qing-Qing Tan,4 Hongxin Xu,5 Nawaf Almutairi,1 Saleh Alshammeri1
1Department of Optometry, College of Applied Medical Science, Qassim University, Buraydah, Qassim, Saudi Arabia; 2SUNY College of Optometry, New York, NY, USA; 3Salus University, Wyncote, PA, USA; 4Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 5Panorama Windows Ltd, New York, NY, USA
Correspondence: Saeed Aljohani, Email [email protected]
Background: Previous studies have shown that it is necessary to evaluate adherence during the treatment process, using educational intervention methods which have been shown to improve adherence with patching treatment. A previous study reported that an educational cartoon had significantly improved adherence with patching. However, this black-white cartoon is not commercially available.
Objective: This study investigates the feasibility of a 4-minute educational cartoon video in improving adherence with patching therapy for amblyopic children.
Methods: Children (3 to 10 years old) with unilateral amblyopia who were prescribed 2 hours or 6 hours of patching per day were enrolled. Objective adherence to the treatment was tracked using a microsensor. Children returned after 4 weeks ± 2 days to measure adherence. Participants with adherence ≤ 50% were eligible to watch the educational cartoon video. They continued with the previously prescribed treatment (2 hours or 6 hours patching) for an additional week to evaluate the follow-up adherence.
Results: A total of 27 participants were enrolled. The mean age (SD) was 6.6 (1.5) years. Twenty-two participants (12 in the 2 hours patching group and 10 in the 6 hours patching group) had adherence ≤ 50% and watched our cartoon video. The cartoon video improved mean adherence (SD) from 29.6% (11.9%) to 56.8% (12.1%) in all 22 participants from both regimens (paired 2-tailed t-test, t= − 11, P < 0.000).
Conclusion: The Educational cartoon video is feasible for use in a clinical setting. These data showed a trend of improvement in adherence with both patching regimens in children after watching the educational cartoon video.
Keywords: educational cartoon, amblyopia, adherence, patching
Introduction
Amblyopia is the leading cause of vision impairment in children, with a prevalence of 1.5% to 4%.1,2 While patching has been shown to be effective treatment for unilateral amblyopia in children 3 to 8 years old,3–8 occlusion dose monitors studies for patching have shown that adherence to patching is on average poor and the actual occlusion dose received is usually not the prescribed dose.9–13
Therefore, there is a critical need to improve adherence to patching treatment. An educational cartoon story has been shown to be an effective strategy to improve adherence.12,14,15 The educational cartoon story explains to the child the importance of adherence to the prescribed treatment. In a randomized clinical trial, an educational cartoon story, a reward calendar sticker, and an information leaflet for parents were compared for their effectiveness in improving adherence in low socioeconomic status areas in the Netherlands.14 The study reported that the educational cartoon story had the most beneficial effect on adherence with patching. However, the cartoon used in that study is not commercially available, and specifically designed for 4 years-old children.
Given the previous effectiveness of the educational cartoon, this research created an educational cartoon video with features that would be attractive to children of this generation including the use of color and narration with a child’s voice. Using an online application called Pixton, an educational cartoon story that explains the importance of wearing an eye patch to treat amblyopia was created. Forty-three pictures were designed to show children an action and a consequence (Figure 1). The story’s script was written with the supervision of a speech-language pathologist to ensure that the language level was appropriate for children 3 to 10 years old. The video was produced in stupendous colorful scenes, and a child’s voice was used to explain the scenes of the story. Because short attention spans are a common characteristic of young children under the age of 10,16 a duration of 4 minutes was thought to be appropriate for 3 to 10 years old children.
 |
Figure 1 Examples of some pictures from our educational cartoon video story developed for patching. |
The aim of this study was to investigate the feasibility of using this educational cartoon video in a clinical setting during amblyopia treatment with patching for non-adherent children.
Methods
This prospective clinical pre-implementation and post-implementation study was conducted between January 2019 and December 2022. The research protocol and informed consent for this study were approved by Salus University Institutional Review Board (IRB #: HSA1803). The study was conducted according to the Declaration of Helsinki on the performance of human research. Parents and participants were provided written informed consent and assent respectively, and Health Insurance Portability and Accountability Act authorization was obtained prior to study participation.
Participants
Participants in this study were recruited from St. Christopher’s Hospital for Children, Philadelphia, USA, The Eye Institute, Philadelphia, USA, and Qassim University Medical City, Qassim, Saudi Arabia. There were two groups of participants. The first group was the “2 hours/day patching regimen group”, and the second group was the “6 hours/day patching regimen group”. Major eligibility criteria for both groups were as follows: (1) age 3 to 10 years; (2) unilateral amblyopia (interocular difference of best corrected visual acuity ≥0.2 logMAR) associated with strabismus, anisometropia, or both; (3) objective adherence with the prescribed patching regimen (either 2 hours/day or 6 hours/day) ≤50%; (4) agreement to wear an eye patch with a sensor attached for a period of 4-weeks. Criteria for strabismus and anisometropia, as well as spectacle correction requirements, followed the guidelines of the Amblyopia Treatment Study by PEDIG.17 Exclusion criteria for both groups were as follows: (1) adherence > 50% with either patching regimens; (2) participants who have equal vision in both eyes after finishing the prescribed amblyopia treatment; (3) cognitive impairment that prohibits accurate data collection.
Procedures
Phase One: Objective Adherence to the Initial Prescribed Treatment
During study visit #1 (30–45 minutes), participants were asked to wear an eye patch with a sensor attached via the Eye Patch Assistant (EPA) to hold the microsensor (TheraMon®) in place instead of the regular patch. The EPA was designed to facilitate consistent positioning on the eyepatch for comfortable wear and prevent loss of the sensor.18 The EPA is a horseshoe-shaped device made of biocompatible silicone material (Elastosil). It has a recessed opening positioned such that the microsensor fits flush for positioning on the skin adjacent to the temporal aspect of the eye being patched. The open side of the EPA was positioned toward the nose to allow for comfortable spectacle wear over the eye patch. Enrolled participants were asked to wear the patch according to the prescribed number of hours by their eye doctor (2 hours/day or 6 hours/day) for 4 weeks ± 2 days. A micro sensor that was attached to the EPA was used at each time a participant applied an eye patch to measure adherence.
Phase Two: Educational Video Intervention
After 4-weeks ± 2 days, participants returned for study visit #2 (15–30 minutes) for an investigator to read the microsensor for adherence. Participants who had adherence ≤50% watched the cartoon-video. The child and his/her parent were asked to watch the 4-minute video one time. The parents or guardians were instructed not to talk to their child while he/she was watching the video. The investigator monitored the child while looking at the video to ensure that the child is not distracted or looking at something else in the clinic. The child continued wearing the eye patch and returned after one week ± 2 days for study visit #3 (15–30 minutes) to allow for reading the sensor again.
Statistical Analysis
Data were collected in Excel (Microsoft Corporation, USA), and then statistical analysis was performed using the SPSS software package (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp., USA). Adherence for each participant was defined as the actual number of hours of wearing the patching/prescribed hours. The mean adherence for all participants and the standard deviation (SD) were calculated. Paired t-tests were used to determine if the cartoon videos improved adherence from the baseline. Results were deemed statistically significant for p-value <0.05.
Results
Of the 27 participants, 11 were females; the mean age (SD) was 6.6 (1.5) years. Twelve participants were prescribed 6 hours/day; 15 were prescribed 2 hours/day. Because 10 participants in the 6 hours/day group and 12 participants in the 2 hours/day group had adherence ≤50%, a total of 22 of them were eligible to participate in the educational cartoon video intervention study. None of the 22 participants missed any of the follow-up visits (Table 1).
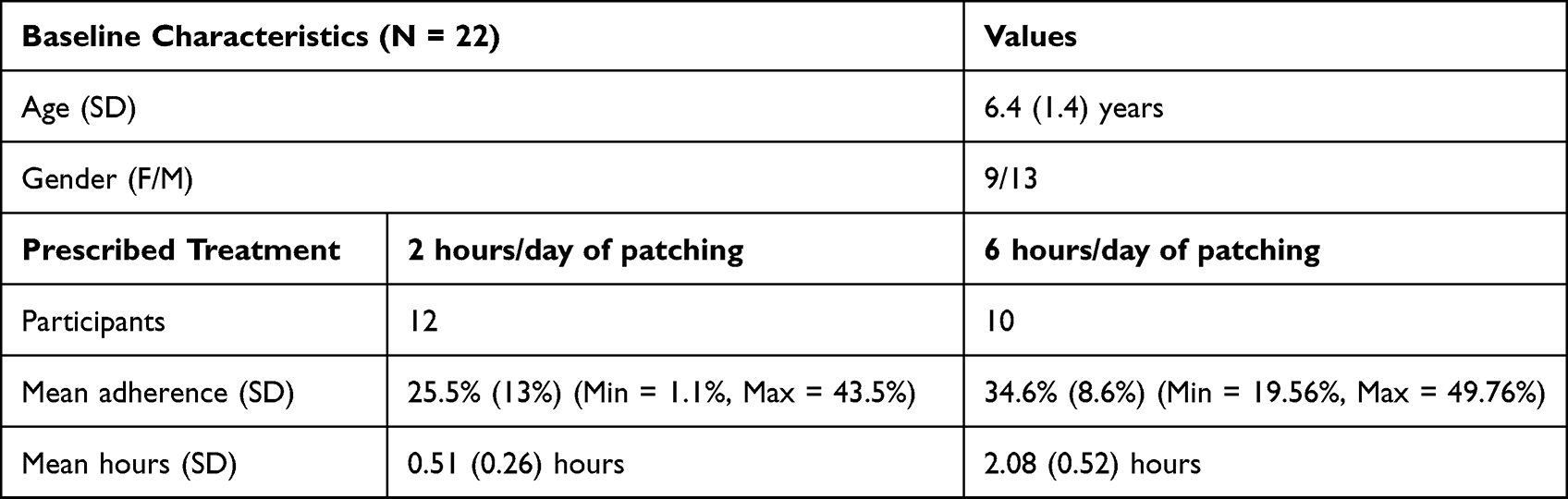 |
Table 1 Baseline Characteristics of All Eligible Participants |
Figures 2a and b summarize every participant’s mean adherence before and after the intervention. Mean adherence was improved for all participants by the cartoon video. The cartoon video improved mean adherence (SD) from 29.6% (11.9%) to 56.8% (12.1%) in all 22 participants from both regimens (paired 2-tailed t-test, t= −11, P < 0.000). All children reported enjoying watching the cartoon video. Mean adherence of all participants shows a trend of decline over a period of 30 ± 2 days, and after participants watched the cartoon videos, adherence increased over a period of 7 ± 2 days (Figure 3).
 |
Figure 2 Participant’s mean adherence before and after the intervention. Notes: (a) The mean adherence before and after intervention for participants in the 2 hours/day regimen group. (b) The mean adherence before and after intervention for participants in the 6 hours/day regimen group. Blue indicates adherence before intervention; orange indicates adherence after intervention. |
 |
Figure 3 Adherence behavior for all participants during the study. Notes: Shows adherence over a period of 30 ± 2 days for all participants. After intervention, mean adherences over a period of 7 ± 2 days for all participants improved. Blue indicates adherence before intervention; orange indicates adherence after intervention. |
At baseline, the mean adherence (SD) for the 2 hours/day regimen group was 25.5% (13%) and the mean daily hours (SD) was 0.51 (0.26) hours; after watching the cartoon video, the mean adherence (SD) with 2 hours/day regimen improved to 52.8% (14.2%) and mean daily hours (SD) increased significantly to 1.06 (0.28) hours (paired 2-tailed t-test, T = −6.59, P < 0.000) (Figure 4a). At the baseline, mean adherence (SD) with the 6 hours/day regimen group was 34.6% (8.6%) and the mean daily hours (SD) was 2.08 (0.52) hours; after watching the cartoon video, the mean adherence (SD) with the 6 hours/day regimen improved to 61.7% (6.7%) and the mean daily hours (SD) increased significantly to 3.7 (0.4) hours (paired 2-tailed t-test, t= −10.83, P < 0.000) (Figure 4b).
 |
Figure 4 Overall mean adherence before and after intervention. Notes: (a) Shows the significant difference in overall mean adherence with 2 hours/day patching regimen before and after intervention, (b) Shows the significant difference in overall mean adherence with 6 hours/day patching regimen before and after intervention. Blue indicates adherence before intervention; orange indicates adherence after intervention. |
Finally, adherence was compared in the first week of the treatment period with adherence in the week after the intervention. Mean adherence in the first week of treatment (SD) was 33.1% (20.1%) and 36.2% (16.8%) versus 52.8% (14.2%) and 61.7% (6.7%) for participants in the 2 hours/day regimen group and 6 hours/day regimen group, respectively (paired 2-tailed t-test, t= −5.43, P < 0.000).
Discussion
This is the first study in the United States and Saudi Arabia to investigate the feasibility of using an educational cartoon video for improving adherence to amblyopia treatments. This study demonstrated the feasibility of the educational cartoon video in a clinical setting, and perhaps the cartoon is successful in circumstances where adherence is low, but only moderately useful in cases where adherence is closer to 50%.
Previously, an education cartoon was reported to be effective in improving adherence to patching in the Netherlands. Loudon et al reported significant improvement in adherence to patching for children receiving some type of educational materials (cartoon story, calendar stickers, and an information leaflet for parents) compared to children in the control group who did not receive the educational materials.12 The authors, however, did not specify which of the educational materials had the greatest effect. Later, Tjiam et al, in a randomized clinical trial, demonstrated that children who viewed a cartoon story had significantly better adherence than children who received calendar stickers or a leaflet information.14 A video of the cartoon story could be more attractive to children. Also, in an attempt to increase the appeal of the cartoon a few parameters were changed (Table 2). The video was produced in stupendous colorful scenes with an appropriate duration of 4 minutes, and comprehensible language by a child’s voice. However, this study did not directly investigate whether our new cartoon would be more effective than the one used by Tjiam et al.
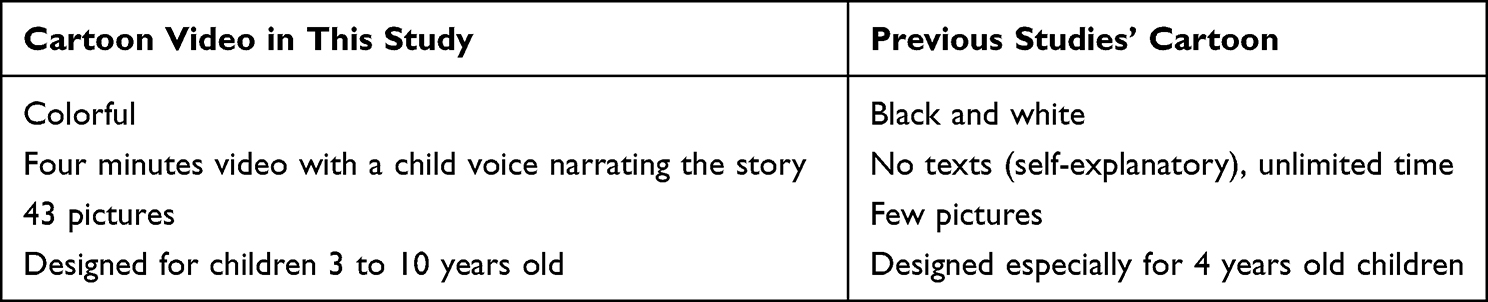 |
Table 2 Comparison Between the Cartoon Story Used in Previous Studies and Our Cartoon Video |
Previously, Wallace et al reported a decreasing trend in adherence to patching over time,11 and the participants in this study showed a similar trend before implementation of the cartoon video (Figure 3). Thus, clinicians might incorporate an educational cartoon either for all patients being treated of amblyopia at the first visits, or after a follow-up at which it becomes evident that adherence is lower than expected. Tjiam and Loudon et al did not compare adherence before and after children viewed the cartoon story. Therefore, it is hard to know if the child and his/her parents were already adherent without the cartoon.12,14 In contrast, this study monitored adherence for four weeks and identified non-adherent participants to determine when to use the cartoon video.
The results of the current study encourage researchers to investigate more engaging strategies to improve adherence to all amblyopia treatment modalities. These findings suggest that clinicians consider educating children via cartoons/videos. Educating children might become a standard component of the treatment plan for amblyopia.
A small sample size is one of this study’s limitations. Nevertheless, this study was focused on testing the feasibility of using the educational cartoon video to improve adherence to amblyopia treatment in the clinical setting. For the same reason, including a control group was unnecessary. Moreover, there was a one 10-year-old child (participant #3 in Figure 2a) who did not appear interested or engaged by the language and the scenes of the cartoon as other children. Therefore, the language and the scenes might need to be improved slightly for this age group in future.
This study was designed to follow up with children a week after watching the cartoon video, which was similar to Tjiam et al clinical trial.14 Thus, it will be informative if future studies follow-up with children for a longer time to measure the long-term effect of the intervention. This will determine if children need to be educated multiple times during the treatment process.
Conclusion
The educational cartoon video is feasible for use in a clinical setting in 3–10 years old children with amblyopia treatments. One week after children watched the video, our results showed a trend of improvement in adherence to patching treatments.
Abbreviation
EPA, Eye Patch Assistant.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, (SA), upon reasonable request.
Acknowledgments
The authors would like to thank the Deanship of Scientific Research, Qassim University for funding publication of this project. The authors would also like to thank all children and their parents for the participation in this study. The abstract of this paper was presented at ARVO 2020 conference as a poster with interim findings. The poster’s abstract was published in Investigative Ophthalmology & Visual Science, June 2020, Vol. 61, 506.
Disclosure
Dr Jingyun Wang reports grants from National Eye Institute, during the conduct of the study; non-remunerative Advisory Board member for Percept Corporation, outside the submitted work. The authors report no other conflicts of interest in this work and declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
References
1. Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008;115(7):1229–36.e1. PubMed PMID: 17953989; PubMed Central PMCID: PMC4839485. doi:10.1016/j.ophtha.2007.08.001.
2. McKean-Cowdin R, Cotter SA, Tarczy-Hornoch K, et al. Prevalence of amblyopia or strabismus in asian and non-Hispanic white preschool children: multi-ethnic pediatric eye disease study. Ophthalmology. 2013;120(10):2117–2124. PubMed PMID: 23697956; PubMed Central PMCID: PMC4848013. doi:10.1016/j.ophtha.2013.03.001
3. Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268–278. PubMed PMID: 11879129. doi:10.1001/archopht.120.3.268.
4. Holmes JM, Kraker RT, Beck RW, et al. A randomized trial of prescribed patching regimens for treatment of severe amblyopia in children. Ophthalmology. 2003;110(11):2075–2087. PubMed PMID: 14597512.
5. Repka MX, Kraker RT, Beck RW, et al.; Pediatric Eye Disease Investigator G. A randomized trial of atropine vs patching for treatment of moderate amblyopia: follow-up at age 10 years. Arch Ophthalmol. 2008;126(8):1039–1044. PubMed PMID: 18695096; PubMed Central PMCID: PMC2614351. doi:10.1001/archopht.126.8.1039
6. Wallace DK, Lazar EL, Holmes JM, et al.; Pediatric Eye Disease Investigator Group. A randomized trial of increasing patching for amblyopia. Ophthalmology. 2013;120(11):2270–2277. PubMed PMID: 23755872; PubMed Central PMCID: PMC3833469. doi:10.1016/j.ophtha.2013.04.008
7. Wallace DK, Kraker RT, Beck RW, et al.; Pediatric Eye Disease Investigator Group. Randomized trial to evaluate combined patching and atropine for residual amblyopia. Arch Ophthalmol. 2011;129(7):960–962. PubMed PMID: 21746992; PubMed Central PMCID: PMC3156057. doi:10.1001/archophthalmol.2011.174
8. Wallace DK, Pediatric Eye Disease Investigator G, Edwards AR, et al. A randomized trial to evaluate 2 hours of daily patching for strabismic and anisometropic amblyopia in children. Ophthalmology. 2006;113(6):904–912. PubMed PMID: 16751033; PubMed Central PMCID: PMC1609192. doi:10.1016/j.ophtha.2006.01.069
9. Wang J. Compliance and patching and atropine amblyopia treatments. Vision Res. 2015;114:31–40. PubMed PMID: 25743080. doi:10.1016/j.visres.2015.02.012
10. Awan M, Proudlock FA, Gottlob I. A randomized controlled trial of unilateral strabismic and mixed amblyopia using occlusion dose monitors to record compliance. Invest Ophthalmol Vis Sci. 2005;46(4):1435–1439. PubMed PMID: 15790912. doi:10.1167/iovs.04-0971
11. Wallace MP, Stewart CE, Moseley MJ, et al. Compliance with occlusion therapy for childhood amblyopia. Invest Ophthalmol Vis Sci. 2013;54(9):6158–6166. PubMed PMID: 23882695. doi:10.1167/iovs.13-11861
12. Loudon SE, Fronius M, Looman CW, et al. Predictors and a remedy for noncompliance with amblyopia therapy in children measured with the occlusion dose monitor. Invest Ophthalmol Vis Sci. 2006;47(10):4393–4400. PubMed PMID: 17003431. doi:10.1167/iovs.05-1428
13. Fielder AR. Electronic monitoring of treatment compliance in patching for amblyopia. Surv Ophthalmol. 2000;44(6):539–540. PubMed PMID: 10914521. doi:10.1016/S0039-6257(00)00120-X
14. Tjiam AM, Holtslag G, Van Minderhout HM, et al. Randomised comparison of three tools for improving compliance with occlusion therapy: an educational cartoon story, a reward calendar, and an information leaflet for parents. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):321–329. PubMed PMID: 22820813. doi:10.1007/s00417-012-2107-4
15. Tjiam AM, Holtslag G, Vukovic E, et al. An educational cartoon accelerates amblyopia therapy and improves compliance, especially among children of immigrants. Ophthalmology. 2012;119(11):2393–2401. PubMed PMID: 22920669. doi:10.1016/j.ophtha.2012.05.035
16. Berk LE. Child Development.
17. Cotter SA, Foster NC, Holmes JM, et al.; Pediatric Eye Disease Investigator G. Optical treatment of strabismic and combined strabismic-anisometropic amblyopia. Ophthalmology. 2012;119(1):150–158. PubMed PMID: 21959371; PubMed Central PMCID: PMC3250558. doi:10.1016/j.ophtha.2011.06.043
18. Wang J, Xu H, De La Cruz B, et al. Improved monitoring of adherence with patching treatment using a microsensor and Eye Patch Assistant. J AAPOS. 2020;24(2):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessing Previous Strategies and Presenting a Novel Smart Glasses to Enhance Adherence to Amblyopia Therapy in Children
Aljohani S
Patient Preference and Adherence 2025, 19:1497-1508
Published Date: 21 May 2025