Back to Journals » Journal of Pain Research » Volume 18
“The Fact [Is] That There Is No Easy Way”. A Qualitative Study of the Experiences of Aotearoa New Zealand Clinicians with Opioid Tapering for Chronic Non-Cancer Pain
Authors Fu R ![]() , Bean D, Te Morenga L, Frei D, Devan H
, Bean D, Te Morenga L, Frei D, Devan H ![]()
Received 18 April 2025
Accepted for publication 20 October 2025
Published 18 November 2025 Volume 2025:18 Pages 6137—6147
DOI https://doi.org/10.2147/JPR.S535298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Rao Fu,1 Debbie Bean,2 Lisa Te Morenga,3 Daniel Frei,1 Hemakumar Devan4
1Department of Anaesthesia and Pain Management, Wellington Regional Hospital, Health New Zealand Te Whatu Ora, Wellington, New Zealand; 2Centre for Person Centred Research, Auckland University of Technology, Auckland, New Zealand; 3Research Centre for Hauora and Health, Massey University, Wellington, New Zealand; 4Rehabilitation Teaching and Research Unit (RTRU), Department of Medicine, University of Otago, Wellington, New Zealand
Correspondence: Rao Fu, Department of Anaesthesia and Pain Management, Wellington Regional Hospital, Health New Zealand Te Whatu Ora, Wellington, New Zealand, Tel +61 0426412686, Email [email protected]
Objective: Opioid tapering is a complex process for both clinicians and patients with chronic pain. This qualitative study explored the experiences of Aotearoa New Zealand clinicians in managing opioids for patients with chronic non-cancer pain.
Methods: Purposive and snowball sampling were used to interview nineteen health professionals including general practitioners (n=5), pain medicine specialists (n=5), addiction medicine specialists (n=4), pain fellows (n=3), addiction medicine registrar (n=1) and a pain nurse practitioner (n=1). Data were collected using a face-to-face focus group and fourteen individual interviews conducted via Zoom. The data were analysed using a Reflexive Thematic Analysis approach. Independent parallel coding was done by members of our research team, and the final themes were iteratively developed by mutual consensus.
Results: This qualitative study suggests that meaningful opioid tapering requires a patient-centred approach that considers the individual’s unique sociopsychobiomedical context. Clinicians emphasised the importance of building trust, addressing fears, and tailoring tapering regimens to patients’ needs and motivations. While opioid tapering is a complex process for all patients, participants acknowledged unique considerations for supporting people living in rural areas – Māori and Pasifika and their whānau (families and significant others) addressing social determinants of health. There were overwhelming accounts of clinician distress from all participants especially for rural general practitioners due to the lack of support, conflicting practices, limited resourcing, and time constraints.
Conclusion: These findings call for a co-ordinated, multidisciplinary approach to opioid tapering that addresses systemic inequities and prioritises patient and clinician well-being.
Keywords: Aotearoa New Zealand, opioid tapering, chronic non-cancer pain, clinician distress, resource constraints, person-centered care
Introduction
One in five people in Aotearoa New Zealand (NZ) live with chronic non-cancer pain.1 Opioids are commonly prescribed for chronic non-cancer pain conditions despite the limited efficacy and association with significant morbidity and mortality with long-term use.2 In Aotearoa NZ, from 2008 to 2012, a total of 325 deaths were primarily attributable to opioid use with 179 deaths due to unintentional overdose.3 The National Coronial Information System (2018) reported that opioid use was the highest primary contributor of drug-related deaths.4
Chronic pain disproportionately affects Māori - the Indigenous population of Aotearoa NZ. Māori adults are 1.4 times more likely than non-Māori adults to report chronic pain yet experience greater barriers to access specialist pain services in NZ and are often under-represented in specialised pain services.1,5 Furthermore, Māori adults have higher dispensed oral morphine equivalent daily dose (oMEDD) when compared to non-Māori adults receiving treatment for similar conditions.6 Thus, there are likely inequities in the burden of opioid-related harm for Māori compared to non-Māori with chronic pain.
Opioid tapering aims to achieve a gradual reduction of opioid dosing to reduce the harms associated with prolonged opioid usage. The 2016 Centres for Disease Control and Prevention (CDC) guideline recommends opioid tapering or discontinuation when the harms of long-term opioid use outweigh the benefits.7 International studies have identified several barriers to implementation of opioid tapering programmes in the primary care setting. These include clinician time constraints, lack of clinician expertise in managing complex opioid prescriptions, a lack of effective alternative therapies, emotional burden on providers, and fear of breaking the trust between patient and provider. Factors which promote opioid tapering include patient motivation to taper opioids, clinician’s ability to empathise with patients’ experience, individualisation of tapering method, collaborative shared decision making and ongoing support during tapering.8–10
In the Aotearoa NZ context, there is no primary research to understand the current practices of primary and tertiary care clinicians in tapering opioids for people with chronic non-cancer pain. As Māori experience significant inequities in pain prevalence and in accessing tertiary pain services, there may be specific considerations in managing opioid tapering for Māori. Furthermore, effective tapering requires the integration between primary and tertiary healthcare specialists. It is not known whether there are unique barriers and/or facilitators encountered in a tertiary pain management setting and/or with co-ordination between primary and tertiary care service providers.
To address these gaps, we aimed to understand Aotearoa NZ clinicians’ current practices of tapering opioids, attitudes, barriers, and opportunities to facilitate opioid tapering for chronic non-cancer pain management.
Methods
Study Design
Guided by a contextual constructionist approach which posits that knowledge is local and context dependent, an exploratory qualitative study design was chosen to understand how opioid tapering is currently practiced by various medical specialists across Aotearoa NZ. Semi-structured individual interviews11 and focus groups12 were used as data collection methods. The consolidated criteria for reporting qualitative research (COREQ) checklist was used to report the study findings.13
Recruitment and Selection Criteria
Eligibility criteria included current NZ medical council registered general practitioners (GPs), addiction medicine specialists, and pain specialists who have prescribed or attempted opioid tapering on at least one patient with chronic non-cancer pain in the past two years.
A purposive and snowball sampling strategy informed our recruitment strategy. Our purposive sampling was guided by clinicians from different geographical locations (rural and urban), area of practice (with or without access to a nearby pain service), and those who treat a higher proportion of Māori patients in their practice. GPs were recruited through expression of interest through known contacts. Pain specialists were identified from “National register of doctors” who are actively practicing in the Medical Council of Aotearoa NZ website including members who are known to the research team.14 Addiction specialists were identified through our contacts with the local Addiction Service based in Wellington, NZ.
Electronic invitations including the study information sheet and consent form were e-mailed to potential participants and written informed consent was obtained prior to the interview. The participants informed consent included publication of anonymised responses/direct quotes. Recruitment was ceased once thematic saturation has occurred with no further unique themes were identified.15
Data Collection
Individual interviews and focus groups were conducted via Zoom® and in person between August and Nov 2022 using a semi-structured interview guide (Appendix 1). The interview guide was developed based on a focused literature review on opioid tapering and chronic non-cancer pain.16 The interview guide was finalised in consultation with our clinical advisory team comprising two pain medicine specialists, a GP, and a pain management physiotherapist.
All interviews were digitally recorded via Zoom® or an audio-recorder and transcribed verbatim using a professional transcription service. All the interviews were conducted by RF, supported by HD. NVivo software was used to code and organise the written transcripts into overarching themes and subthemes. Mind mapping tools were employed to visually represent the development of these themes and subthemes in a group setting to facilitate further classification and exploration of the relationships between them.
Analysis
The Braun and Clarke’s 6-step Reflexive Thematic Analysis approach was chosen as it does not prescribe a specific qualitative tradition when the research questions are essentially evaluative.17 Transcription and analysis began immediately after the first interview so that any unconsidered relevant questions were added to the following interviews. Debrief meetings held after each interview between RF and HD were an important aspect of meaning making of the data. RF conducted the initial coding of all the qualitative data and presented those initial codes and sub-themes to HD and DB. HD and DB coded a sub-set of interviews to add further interpretation and meaning to the initial codes. Then RF, HD and DB iteratively discussed the meaning of initial codes to generate an initial draft of themes and sub-themes. These were presented to the research and clinical advisory team to generate further discussions, interpretation and making sense of the data. The final themes and sub-themes were discussed and decided upon by mutual consensus by the whole team.
Reflexivity
RF, male, with a background in anaesthesia and pain medicine led the qualitative data analysis with the support of HD (physiotherapy background and pain management researcher) and DB (health psychology background and pain management researcher) who have previous training in reflexive TA. As RF had no qualitative research experience, he underwent a thematic analysis training workshop prior to data collection. The research and analysis spanned over two years. Initially, RF’s understanding of opioid tapering was predominantly shaped by his anaesthetic training, where he started the research with the assumption that chronic non-cancer pain patients should minimise opioid usage with the aim to tapering opioids completely off whenever possible. However, as RF progressed through the pain fellowship, his comprehension of opioid tapering became more nuanced, recognising the complexities of opioid tapering with the overall goal is to achieve patient well-being rather than solely focusing on opioid reduction. His views on the complexity of opioid tapering are further shaped by his spouse who is a GP working with patients with complex pain issues on long-term opioids.
Ethics
Ethics approval was sought from the University of Otago Human Ethics Committee (Health) - H22/106. The study protocol was also approved by the Ngāi Tahu (A Māori Iwi (tribe) with an existing relationship with the University of Otago).
Results
Nineteen health professionals were interviewed between August and November 2022 including GPs (n=5), pain medicine specialists (n=5), addiction medicine specialists (n=4), pain fellows (n=3), addiction medicine registrar (n=1) and a nurse practitioner in pain management (n=1). Of the interviewed participants, 42% were men and the majority (74%) were employed in the tertiary care setting, while the remaining (26%) were employed in the primary care setting. The interviews consisted of one face-to-face focus group (consistent of 6 individuals) and fourteen individual Zoom® interviews.
We generated four major themes: (1) Understanding the person and context (2) Cumulative & intersectional disadvantages (3) Confrontation, ethical conflict, and clinician distress (4) Mahi Tahi – Working together. Table 1 provides an overview of four major themes, sub-themes, and supplementary quotes.
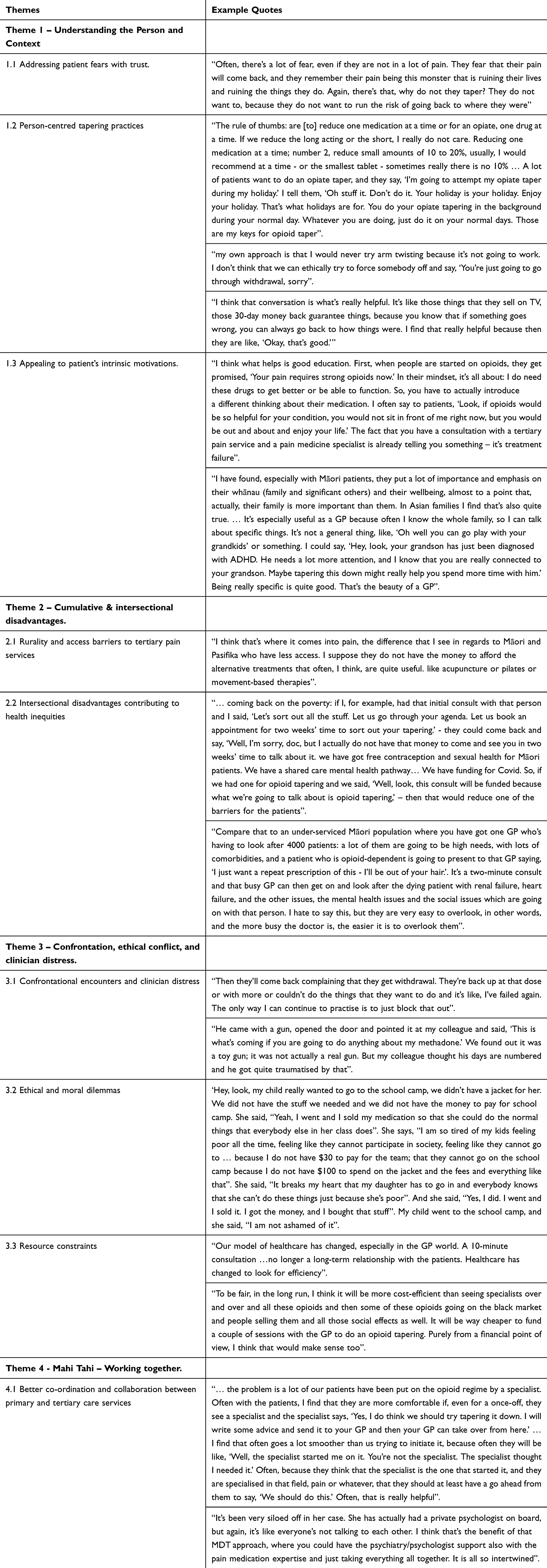 |
Table 1 Themes & Subthemes |
Theme 1 – Understanding the Person and Context
Effective opioid tapering requires an empathetic understanding of a patient’s unique sociopsychobiomedical circumstances. The tapering regimen should be tailored, adaptable, gradual, and mindful of the patient’s life situation. As one pain specialist mentioned, the approach is
find out where the patient is at in their journey and see how receptive they are to a different perspective… and really listen to not only their pain story… their perspective and ideals and world view, and then be able to work within that to support and provide for them an alternative that actually means something.
Opioid tapering is often linked to patients’ concerns about the prognosis of their pain condition, need for strong medications, expectation of increased pain with opioid reduction, fear of withdrawal symptoms, and patients’ lack of awareness of the long-term side effects of opioids. Patients often hold the view that opioids were initially prescribed to aid them, and tapering may seem counterintuitive to their management. Stronger medications were often perceived as more effective for their pain management.
This situation is further complicated by changes in prescribing regulations due to the rising number of opioid-related deaths. Some patients may view opioid tapering as more about protecting doctors from legal consequences rather than being in their best interests. One pain specialist stated that:
you can help with that motivation by having some trust in that therapeutic relationship with you as the treating person who’s not there for any ulterior motives… trust in the practitioner they’ve got.
Understanding the patient’s genuine concerns about opioid tapering, and establishing trust were identified as critical components of person-centred opioid tapering.
Person-centred opioid tapering practices involved acknowledging and respecting patient’s autonomy for optimal outcomes (Table 1). By establishing mutual trust, clinicians were able to appeal to the patient’s intrinsic motivations when tapering opioids. One strategy involved collaboratively working with patients to help them understand about the risks associated with chronic opioid use and the lack of evidence supporting its long-term effectiveness in managing chronic non-cancerous pain conditions. Another strategy was to connect the benefits of opioid tapering with benefits that are meaningful to the patient. This was noticeable with general practitioners as they have long-standing relationships with not only the patients but their whole whānau (family and significant others).
Theme 2 – Cumulative & Intersectional Disadvantages
Clinicians from rural areas especially GPs shared their challenges of working in a rural setting with limited or no access to specialised tertiary pain services offering multi-modal care. These often include group-based pain management programmes and access to psychologists and physiotherapists. Participants shared the importance of recognising and addressing unique social determinants of health to support tapering opioids in general and more specifically for Māori & Pasifika patients and their whānau. A GP explained,
I think that’s where it comes into pain, the difference that I see in regards to Māori and Pasifika who have less access. I suppose they don’t have the money to afford the alternative treatments that often, I think, are quite useful. like acupuncture or pilates or movement-based therapies.
Multiple levels of disadvantage of living in a rural setting, lack of stable housing, and poverty could make opioid tapering process not a priority for patients living in rural areas. One GP suggested “Well, look, this consult will be funded because what we’re going to talk about is opioid tapering”, – then that would reduce one of the barriers for the patients”.
Another rural GP highlighted the systemic constraints of working remotely with in underfunded and overstretched practices, “the more busy the doctor is, the easier it is to overlook them (opioid tapering)”.
Theme 3 – Confrontation, Ethical Conflict, and Clinician Distress
Several participants expressed frustration over the limited guidance available for opioid tapering because opioid tapering lacks standard protocols necessitating personalised consideration for its initiation and maintenance. One pain specialist stated,
The fact that there is no easy way, there’s absolutely nothing that exists that can help guide me. We do not have a protocol that says: this is what you do. I make it up based on what they’re willing to do. It’s not based on science.
In a sense, “making it up based on what they’re willing to do” is what is needed to adapt to the patient’s personal situation. Nevertheless, the process is a demanding task for the clinician.
This difficult task is further complicated by the feeling that some GPs are unequipped with the knowledge and skills to carry this task. One GP reported,
I only discovered this last year, but chronic persistent pain is not on the GP training curriculum. Something which affects one in five people, costs New Zealand $15 billion a year, … Yet it’s not on the curriculum for the College teaching GPs how to be GPs. That’s indefensible. That’s just embarrassing.
Another GP explains that her expertise in managing chronic pain patients and opioids was developed experientially through struggling patient interactions rather than formal training. She recounts, “…was I ever really taught it? No… I definitely think that we as GPs have to seek out that education. “
An overlooked barrier to opioid tapering is the strain it places on physicians and its consequential impact. The process often evokes considerable distress. Clinicians described how opioid tapering can be associated with a personal sense of failure and frustration, experiences of being bullied, coerced or threatened with physical violence, and can also contribute to fractions, conflict or disagreement between colleagues.
First, opioid tapering contributed to clinician dissatisfaction, frustration, and sense of failure. For example, one pain specialist expressed how a patients’ lack of success with opioid tapering may be internalised, leading to a sense of failure as a clinician.
Second, many clinicians discussed feeling coerced, intimidated, or even physically threatened in opioid-related consultations. They described how patients requesting continuation of opioids may directly or indirectly threaten to accuse them of being a bad doctor or making complaints if they reduce the opioids, and express praise when opioids are continued. They indicated that this may be a particular problem for less experienced clinicians or those new to a particular area or practice. Coercion could also occur, as described by one GP:” [opioid tapering] creates a huge amount of conflict, drama, anger, emotion, all sorts, directed often at us, and we do not need the pain”.
In the most extreme cases, the intimidating behaviour involved threats of physical violence towards the clinician, which could lead to experiences of trauma for the clinician involved and create fear amongst colleagues.
Third, opioid tapering contributed to clinician strain by leading to conflict between practitioners. There were notable inconsistencies between clinicians, and when one is prepared to work hard to taper opioids with a patient, another clinician may undermine this process by providing a higher dose.
This not only creates conflict and a sense of disrespect or distrust between clinicians but can also be confusing for the patient. Further, this GP noted how once she had expressed the view that the opioids should be reduced but another doctor had continued the dose, it can reflect badly on you; “it makes you look like you were wrong”.
Tapering a patient’s medication can pose ethical and emotional dilemmas for clinicians contributing to distress. A GP shares the story where a patient, genuinely experiencing pain, resorts to selling medication due to financial struggles. Specialists decide to taper off the medication upon learning about the situation. A GP recalls an interaction with a patient who faced financial struggles and resorted to selling opioids to support her family. Despite this, the patient still experienced inadequately controlled pain. This interaction exemplifies the complex relationship between pain management, opioid tapering, and aberrant opioid use, all of which are intricately linked to the patient’s social circumstances. The situation is ethically and emotionally challenging. While the clinician, who has young children themself, empathises with the sacrifices made to support one’s family, the aberrant behaviour calls for intervention to ensure patient and community safety. However, this is further complicated by the risk of inadequate pain treatment for the patient.
Theme 4 - Mahi Tahi – Working Together
A co-ordinated, pro-equity, public health approach to support opioid tapering was an aspiration for most clinicians. Supporting resources should be made for more accessible primary healthcare, social support, and culturally informed multidisciplinary chronic pain care.
Clinicians expressed hope for an ideal system where there is a multidisciplinary approach where there weren’t big barriers for people to access things. So if the person had pain. we’d be able to get them into a physio without them having to pay huge amounts of money.
A pain specialist suggested that through empowering and equipping general practitioners with resources to oversee the tapering regimen would prove to be a cost-effective measure.
Power differentials between specialists and GPs also exist, especially when specialists initiated opioid prescriptions. In such cases, GPs may feel the need to obtain further support from specialists for the tapering process. Specialists, especially those in private practice, may operate in isolation, potentially neglecting the multidisciplinary team approach in the management of chronic pain and opioid tapering.
Discussion
This qualitative study explored Aotearoa NZ clinicians’ experiences of opioid tapering for people with chronic non-cancer pain. The results suggest successful opioid tapering is an individualised journey, and it relies on understanding the patient’s life situation in a sociopsychobiomedical framework. Clinicians need to address patients’ fears, establish trust, and gradually reduce the opioid dosage in a way that empowers the patient to feel in control and that is intrinsically meaningful to them. While opioid tapering is a complex process for all patients, clinicians identified unique considerations for people living in rural areas especially for Māori and Pasifika patients and their whānau acknowledging their social determinants of health. There were overwhelming accounts of clinician distress from all participants especially for rural GPs due to the lack of support, conflicting practices, limited resourcing, and time constraints. Participants aspired for a systemic overhaul that would acknowledge this complexity through a collaborative, multidisciplinary approach.
Our findings add to the current understanding of complexity and nuances of opioid tapering practices in chronic non-cancer pain management not only in Aotearoa NZ but globally. Previous research has demonstrated that although long-term opioid use is associated with significant risks, opioid tapering is a challenging and stressful process for patients and poses significant harm. Magnan et al showed that opioid tapering was linked to increased emergency department visits and hospitalisations, fewer primary care visits, and decreased adherence to antihypertensive and antidiabetic medications.18 Furthermore, abrupt discontinuation of opioids was also associated with overdose on heroin.19 Increase in heroin use was also correlated with reduction in opioid prescribing following changes to opioid prescribing regulation in Australia.20 The conundrum of opioid tapering is further complicated by the development of complex persistent dependence in patients within the grey zone between opioid dependence and addiction, where opioid tapering can lead to worsening of pain and psychiatric dysfunction.21 Altogether these studies highlight opioid tapering is complex and can be problematic if done abruptly and without considering the risks and benefits in the context of sociopsychobiomedical framework.
While data on opioid prescription and tapering for people with chronic non-cancer pain in Aotearoa NZ is unavailable, the National Pain Survey conducted by Chronic Pain Australia in 2023 showed 1 in 5 respondents were forced to reduce their opioids.22 The crux of opioid tapering is knowing when and how to taper. As one of our participants emphatically stated that we should all be “avoiding arm twisting”. The overarching goal of opioid tapering is to mitigate the harms caused by inappropriate opioid use, while recognising the important role opioids play in managing acute pain and in exceptional circumstances for some patients with chronic non-cancer pain.23 The objective is not simply to taper opioid use for the sake of tapering, but rather to minimise harm and enhance patient function. This is grounded on the principles of mutual trust, understanding and empowerment as expressed by the clinicians in our study.
The negative impact of opioid tapering practices on clinicians’ wellbeing was evident from our participants’ discourse and narratives shared. A similar finding by a qualitative study of GPs from Australia also highlighted the challenges in opioid tapering practices due to variations in prescribing practices amongst GPs and limited support from the public health system.8 Our findings suggest the opioid tapering process is time and resource consuming. It requires a tailored approach considering the sociopsychobiomedical factors driving the patient’s opioid use. From a clinician’s perspective the process was often perceived as unrewarding and lacking clear success metrics. Clinicians themselves may feel underprepared in dealing with these challenging consults. This is especially difficult when opioid tapering is not without potential harms.18,20,24 The difficulties were further exacerbated by confrontational nature of the consultations and resource limitations to access multidisciplinary pain management services.
Challenges to accessing multidisciplinary, specialised pain services were more pronounced in our interviews from GPs working in rural settings. The Royal New Zealand college of General Practitioners’ workforce survey showed that of more than 3400 GPs (48%) reported high levels of burnout. This trend is more pronounced in rural areas.25 Additionally, the correlation between rurality and increased prescription rates of potent opioids is evident in the report by the Health Quality and Safety Commission of NZ.26 This data is personified by the stories shared by our participants of the lone GPs practicing in rural NZ, feeling unsupported, on the brink of burnout and when faced with ongoing demands for pain relief from patients where the default option was to repeat the prescription. A finding that aligns with a qualitative study conducted in the US, experiencing emotional burden to primary healthcare practitioners with opioid tapering due to resource constraints and limited training.9
Our findings call for pro-equity approaches to opioid tapering considering intersectional disadvantages for people living in rural areas, Māori and Pasifika patients. In Aotearoa NZ, Māori are disproportionately affected by rurality, poverty, and poorer health outcomes in addition to higher burden of chronic pain.27,28 In Australia, the Pennington Institute report in Australia underscores the disproportionate representation of First Nations people in the growing toll of unintentional overdoses.29 A similar trend was observed in Aotearoa NZ where Māori were approximately three times more likely to die of an overdose when compared to Pākehā/European.30 This calls for the need of culturally informed, strengths-based approaches from a te ao Māori (Māori worldview) perspective when approaching opioid tapering. Recent recommendations to ensure pain services meet the needs of Māori include focusing on the multidimensional aspects of pain, incorporating tikanga (cultural protocols) to provide respectful care, and supporting tino rangatiratanga or autonomy for self-management.31 These recommendations are highly relevant for opioid tapering in the context of chronic pain in Aotearoa NZ.
Strengths and Limitations
A unique strength of our study is our qualitative exploration drawing from the collective experiences of pain specialists, addiction medicine specialists, and GPs from Aotearoa NZ, which could be applicable to other contexts with public health funding systems. Further exploration is needed from the patient’s perspective to identify the enablers and challenges of tapering opioids in the context of Aotearoa NZ. Next, the co-ordination of tertiary and primary care providers could be further explored to support rural GPs with opioid tapering. The use of online delivered pain management consultations, online pain management programmes,32 and community-based pain management initiatives complementary to support opioid tapering could be further investigated. Our findings showed the unique challenges faced by rural GPs in supporting Māori patients and their families. Further research could explore rural primary care practices and Māori community providers’ views on supporting patients in rural areas with opioid tapering.
Conclusion
This is the first study to explore Aotearoa NZ clinicians’ experiences of opioid tapering for people with chronic non-cancer pain. Successful opioid tapering for people with chronic non-cancer pain relies on understanding the patient in a sociopsychobiomedical framework. While opioid tapering is a complex process for all patients, there are unique considerations for supporting people living in rural areas – Māori and Pasifika and their whānau addressing social determinants of health. There were overwhelming accounts of clinician distress especially for rural GPs calling for a collaborative, multidisciplinary approach to opioid tapering practices.
Acknowledgments
We would like to acknowledge all healthcare professionals involved in the study and our clinical advisory team for their time and support for this project. Advisors: Dr Jane Thomas, Dr Leinani Aiono-Le-Tagaloa, Ms Dagmar Hempel, Dr Louise Lynch, Dr Buzz Burrell. The abstract was presented in form as an e-poster at the Australian and New Zealand College of Anaesthetists (ANZCA) Annual Scientific Meeting (ASM) 2023.
Funding
This research project was funded by the Campbell Barrett Trust and Health Research Council of New Zealand (Ref #22-667) as part of a Health Delivery project grant aimed to develop and implement a whānau focused, story-based opioid tapering support intervention.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Annual Update of Key Results 2015/16: new Zealand Health Survey. Ministry of Health. Available from: http://www.health.govt.nz/system/files/documents/publications/annual-update-key-results-2015-16-nzhs-dec16-v2.pdf.
2. Warner EA. Opioids for the treatment of chronic noncancer pain. Am J Med. 2012;125(12):1155–1161. doi:10.1016/j.amjmed.2012.04.032
3. Shipton EE, Shipton AJ, Williman JA, Shipton EA. Deaths from opioid overdosing: implications of coroners’ inquest reports 2008-2012 and annual rise in opioid prescription rates: a population-based cohort study. Pain Ther. 2017;6(2):203–215. doi:10.1007/s40122-017-0080-7
4. NCIS factsheet: drug-related deaths in NZ in 2018. National Coronial Information System. Available from: https://www.ncis.org.au/wp-content/uploads/2022/06/2019-NZ-NCIS-fact-sheet-Mortality-data-series-Drugs.pdf.
5. Burri A, Rice D, Kluger N, Kluger M. Ethnic- and sex-related differences in pain characteristics, psychological distress and pain-related disability in patients attending a New Zealand teaching hospital pain service. N Z Med J. 2018;131(1470):51–64.
6. Crawford CVP, Sutton J, Higgie K, Dawkins C. The impact on community opioid dispensing of engagement with a multidisciplinary chronic pain service.
7. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1–49. doi:10.15585/mmwr.rr6501e1
8. Hamilton M, Mathieson S, Gnjidic D, et al. Barriers, facilitators, and resources to opioid deprescribing in primary care: experiences of general practitioners in Australia. Pain. 2022;163(4):e518–e526. doi:10.1097/j.pain.0000000000002340
9. Kennedy LC, Binswanger IA, Mueller SR, et al. “those conversations in my experience don’t go well”: a qualitative study of primary care provider experiences tapering long-term opioid medications. Pain Med. 2018;19(11):2201–2211. doi:10.1093/pm/pnx276
10. Kuntz JL, Dickerson JF, Schneider JL, et al. Factors associated with opioid-tapering success: a mixed methods study. J Am Pharm Assoc. 2021;61(3):248–257.e1. doi:10.1016/j.japh.2020.12.019
11. Patton MQ. Qualitative Evaluation and Research Methods. SAGE Publications, inc; 1990.
12. Morgan DL. Reconsidering the role of interaction in analyzing and reporting focus groups. Qual Health Res. 2010;20(5):718–722. doi:10.1177/1049732310364627
13. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
14. The Medical Council of New Zealand. Register of doctors. Available from: https://www.mcnz.org.nz/registration/register-of-doctors/.
15. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
16. Australian Pain Society Board APS Guiding Principles for Pain Management. Available from: https://www.apsoc.org.au/PDF/Position_Paper/APS_Guiding_Principles_for_Pain_Management_AUG24.pdf.
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
18. Magnan EM, Tancredi DJ, Xing G, Agnoli A, Jerant A, Fenton JJ. Association between opioid tapering and subsequent health care use, medication adherence, and chronic condition control. JAMA Network Open. 2023;6(2):e2255101–e2255101. doi:10.1001/jamanetworkopen.2022.55101
19. Hallvik SE, El Ibrahimi S, Johnston K, et al. Patient outcomes after opioid dose reduction among patients with chronic opioid therapy. Pain. 2022;163(1):83–90. doi:10.1097/j.pain.0000000000002298
20. Nielsen S, Xia T. Interventions for reducing the prescribing of pharmaceutical opioids in Australia: are they effectively reducing opioid harm? Med J Austr. 2024;220(6):311–312. doi:10.5694/mja2.52259
21. Manhapra A, Arias AJ, Ballantyne JC. The conundrum of opioid tapering in long-term opioid therapy for chronic pain: a commentary. Subst Abus. 2018;39(2):152–161. doi:10.1080/08897077.2017.1381663
22. Chronic Pain Australia. 2023 National Pain Survey. 2023. Available from: https://chronicpainaustralia.org.au/wp-content/uploads/2023/07/National-Pain-Survey-2023-Report-FULL-SURVEY.pdf.
23. Faculty of pain medicine - The Australian and New Zealand College of Anaesthetists (ANZCA). Statement regarding the use of opioid analgesics in patients with chronic non-cancer pain PS 01. 2021.
24. Larochelle MR, Lodi S, Yan S, Clothier BA, Goldsmith ES, Bohnert ASB. Comparative Effectiveness of Opioid Tapering or Abrupt Discontinuation vs No Dosage Change for Opioid Overdose or Suicide for Patients Receiving Stable Long-term Opioid Therapy. JAMA Network Open. 2022;5(8):e2226523. doi:10.1001/jamanetworkopen.2022.26523
25. Royal New Zealand College of General Practitioners. 2022 Workforce Survey. Available from: https://www.rnzcgp.org.nz/resources/data-and-statistics/2022-workforce-survey/.
26. Health Quality and Safety Commission. Atlas of Healthcare Variation - Opioids. Available from: https://public.tableau.com/app/profile/hqi2803/viz/Opioidssinglemap/AtlasofHealthcareVariationOpioids.
27. Crengle S, Davie G, Whitehead J, de Graaf B, Lawrenson R, Nixon G. Mortality outcomes and inequities experienced by rural Māori in Aotearoa New Zealand. Lancet Reg Health West Pac. 2022;28:100570. doi:10.1016/j.lanwpc.2022.100570
28. Hobbs M, Ahuriri-Driscoll A, Marek L, Campbell M, Tomintz M, Kingham S. Reducing health inequity for Māori people in New Zealand. Lancet. 2019;394(10209):1613–1614. doi:10.1016/S0140-6736(19)30044-3
29. Penington Institute. Australia’s Annual Overdose Report. 2023.;
30. New Zealand Drug Foundation. Fatal overdoses in Aotearoa 2017-2021. Available from: https://drugfoundation.org.nz/articles/overdose-report-2017-2022.
31. Antunovich D, Romana J, Lewis GN, Morunga E, Bean DJ. The lived experience of chronic pain for Māori: how can this inform service delivery and clinical practice? A systematic review and qualitative synthesis. N Z Med J. 2024;137(1591):62–73. doi:10.26635/6965.6271
32. Perry MA, Devan H, Davies C, et al. iSelf-Help: a co-designed, culturally appropriate, online pain management programme in Aotearoa. Res Involvement Engag. 2022;8(1):6. doi:10.1186/s40900-022-00339-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.