")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
The Expression of Plasmacytoid Dendritic Cells and TLR7/9-MyD88-IRAKs Pathway in Chronic Eczema Lesions
Authors Wen J, Weng J, Lu W, Tao X, Cheng H, Tang Y
Received 3 February 2023
Accepted for publication 13 April 2023
Published 24 April 2023 Volume 2023:16 Pages 1079—1087
DOI https://doi.org/10.2147/CCID.S405491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Jiamin Wen,1 Jitian Weng,2 Wei Lu,3 Xiaohua Tao,3 Hao Cheng,4,* Yi Tang3,*
1Department of Dermatology, People’s Hospital of Tiantai County, Zhejiang University, Taizhou, People’s Republic of China; 2School of Public Health, Hangzhou Normal University, Zhejiang University, Hangzhou, People’s Republic of China; 3Center for Plastic & Reconstructive Surgery, Department of Dermatology, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Zhejiang University Hangzhou 310014 People’s Republic of China; 4Department of Dermatology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yi Tang, Center for Plastic & Reconstructive Surgery, Department of Dermatology, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Zhejiang University, 158 Shangtang Road, Xiacheng District, Hangzhou, 310014, People’s Republic of China, Tel +86-13968076453, Fax +86-0571-85335800, Email [email protected] Hao Cheng, Zhejiang University School of Medicine Sir Run Run Shaw Hospital, Hangzhou, Zhejiang, 310016, People’s Republic of China, Tel +86-13588706943, Fax +86-571-86006975, Email [email protected]
Purpose: To investigate the expression of Plasmacytoid Dendritic Cells (pDCs) and TLR7/9-MyD88-IRAKs pathway in chronic eczema lesions.
Patients and Methods: Lesional tissues and the surrounding healthy tissues were collected from 25 individuals with chronic eczema, and immunohistochemistry was used to detect and comparatively analyze the expression profile of CD123, CD2AP, toll-like receptor 7 (TLR7), toll-like receptor 9 (TLR9) along with interleukin-1 receptor-associated kinase 1 (IRAK1) and interferon regulatory factor 7 (IRF7) in signaling pathways.
Results: The positive rates of CD2AP + pDC and CD123 + pDC in lesional tissues were significantly elevated compared to the surrounding healthy tissues (P < 0.05). They were distributed in both the epidermal and dermal layers of the lesional tissue, but the majority were in the dermal layer. The TLR7, TLR9, IRAK1 and IRF7 were more expressed in dermal layers of the lesional tissue with higher positive rates of expression compared to the surrounding healthy tissues (P < 0.05). IRAK1 and IRF7 were expressed in a small amount in the epidermal layer with higher positive rates of expression than in the surrounding healthy tissues (P < 0.05), while the positive rates of TLR7 and TLR9 expression in the epidermal layer were not statistically different from those in the surrounding healthy tissues (P > 0.05).
Conclusion: PDC and TLR7/9-MyD88-IRAKs pathways are actively expressed in chronic eczema lesions and may be involved in pathogenesis and disease progression.
Keywords: eczema, plasmacytoid dendritic cells, toll-like receptor 7, toll-like receptor 9, immunohistochemistry
Introduction
As a group of inflammatory skin diseases with exudative tendencies caused by a variety of internal and external factors, eczema has a high recurrence rate in clinical practices, and long-term use of glucocorticoid for the treatment of the disease has great side effects, seriously reducing the quality of life of patients. Although there has been much clinical research on eczema (including specific types of eczema such as atopic dermatitis, hand and foot eczema, etc.) nationally as well as internationally along with a focus on its treatment, however, its pathogenesis has not yet been clarified. Recently, research on related traditional Chinese medicine in the treatment of eczema has been increasing compared to before. However, due to individual differences and the complexity of eczema, no clear therapeutic regimen has been formed. Therefore, the pathogenesis associated with chronic eczema and its treatment needs to be figured out urgently. This research studied plasmacytoid dendritic cells and TLR7/9-MyD88-IRAKs signal pathways and explored the relationship between CD2AP, CD123, toll-like receptor 7 (TLR7), toll-like receptor 9 (TLR9), interleukin-1 receptor-associated kinase 1 (IRAK1), type-I interferon regulatory factor 7 (IRF7) expression along with the pathogenesis of chronic eczema by immunohistochemistry, providing relevant research support for understanding the pathogenesis of chronic eczema.
Materials and Methods
Lesional Tissues
The lesional tissues and the surrounding healthy tissues for this study were collected from 25 individuals with chronic eczema between January 1, 2012, and December 30, 2021, at the Department of Dermatology, Zhejiang Provincial People’s Hospital, and all the included subjects met the diagnostic criteria for clinical chronic eczema. Individuals having diseases like viral hepatitis, autoimmune diseases, tuberculosis, or diabetes were all excluded from this study. The medical ethics committee of the hospital approved this research (QT2022282).
The Main Reagents
Rabbit anti-human CD2AP monoclonal antibody and mouse anti-human CD123 monoclonal antibody were bought from Abcam, USA, and rabbit anti-human IRAK1 monoclonal antibody, rabbit anti-human IRF7 monoclonal antibody, mouse anti-human TLR7 monoclonal antibody, and rabbit anti-human TLR9 monoclonal antibody were bought from CST, USA. Hydrogen peroxide, antigen retrieval solution, HRP-conjugated secondary antibody, and DAB chromogenic solution for immunohistochemistry were purchased from Beijing Solarbio Life Sciences.
Methods
CD2AP, CD123, IRAK1, IRF7, TLR7, and TLR9 were obtained from lesional tissues and surrounding healthy tissues of 25 individuals with chronic eczema for immunohistochemical staining, and paraffin sections were made after fixation in 4% paraformaldehyde, and serial sections of 4 μm were performed. The immunohistochemical procedure was as follows: firstly, the tissue samples were baked in an oven at 60 ° C for half an hour to melt the wax, followed by xylene-gradient ethanol-water dewaxing and immersion. Subsequently, to remove endogenous peroxidase hydrogen peroxide was added; then the antigen was retrieved using antigen retrieval solution (EDTA Antigen Retrieval solution), and after membrane penetration and blocking, diluted primary antibodies (rabbit anti-human CD2AP monoclonal antibody 1:100 dilution, mouse anti-human CD123 monoclonal antibody 1:100 dilution, rabbit anti-human IRAK1 monoclonal antibody 1:50 dilution, rabbit anti-human IRF7 monoclonal antibody 1:200 dilution, mouse anti-human TLR7 monoclonal antibody 1:50 dilution, and rabbit anti-human TLR9 monoclonal antibody 1:100 dilution) were added followed by overnight incubation. The primary antibody was washed off after removal the next day followed by incubation at room temperature with HRP secondary antibody. Afterward, DAB was used for color rendering, hematoxylin was used to stain the nucleus, and the slides were mounted to observe and record the results.
Interpretation of Immunohistochemical Staining Results
Cells presenting brownish-yellow or yellow-brown granules in the cell membrane and/or cytoplasm under optical microscopy were positive cells. Positive rate = the number of cases containing positive cells/total number of cases * 100%. The expression intensity was scored semi-quantitatively according to the percentage of positive cells and staining intensity: five lesional skin tissues dominated by the epidermis and five lesional tissues dominated by the superficial dermis were randomly selected from each section under a 400-magnification optical microscope, and the expression intensity of each field was counted. Intensity score (A): 0 points represented unstained cells; 1 point represented yellowish color; 2 points represented brownish-yellow; 3 points represented dark brown. Positive cell rate score (B): positive cell rate < 33% counted as 1 point; 33% ~ 66% counted as 2 points; > 66% counted as 3 points. The expression intensity of a single field was equal to that of A*B. Expression intensity, in this case, = expression intensity in 5 random fields/5. Normal skin around the lesion was counted in the same manner as the lesion.
Statistical Processing Was Performed Using SPSS 25.0 Statistical Software
Non-normally distributed measurement data were represented as M (P25, P75), and the Mann–Whitney U-test was used to compare the two groups. Enumeration data were shown as frequency and constituent ratio, and the x2 test was used to compare the two groups. P < 0.05 indicated a statistically significant value.
Results
Expression and Distribution of CD2AP in Chronic Eczema
CD2AP was expressed in the dermis and epidermal layers of skin tissue, mainly in the basal layer of the epidermis and papillary dermis (Figure 1). The positive rate of CD2AP + pDC in the epidermal layer of lesional tissues was notably higher than in the epidermal layer of surrounding healthy tissues (P < 0.05), while the expression intensity of CD2AP was substantially elevated compared to surrounding healthy tissues (P < 0.05). Similarly, the positive rate of CD2AP + pDC in the dermal layer of lesional tissues was significantly higher than in the surrounding healthy skin tissues (P < 0.05), and the expression intensity of CD2AP was substantially elevated compared to the surrounding healthy tissues (P < 0.05) (Table 1).
 |
Table 1 The Positive Rate and Intensity of CD2AP Expression in 25 Cases of Chronic Eczema and 18 Cases of Normal Skin Around Eczema |
 |
Figure 1 Expressions of CD2AP in chronic eczema lesions and the perilesional normal skin at the edge (SP *400). (a) Epidermic of skin lesion. (b) Dermis of skin lesion. (c) Perilesional normal skin. (a) More CD2AP+ monocyte-like cells with brown cytoplasm were observed in the epidermal of chronic eczema lesions. (b) More CD2AP+ monocyte-like cells with brown cytoplasm were observed in the dermal papillary layer of chronic eczema lesion. (c) Almost no of CD2AP+ monocyte-like cells with brown cytoplasm were observed in both epidermal and papillary layer of perilesional normal skin of the lesion. |
Expression and Distribution of CD123 in Chronic Eczema
CD123 is mainly expressed in the dermis with a small amount in the epidermal layer, mainly in the basal layer (Figure 2). The positive rate of CD123 + pDC in the epidermal layer of lesional tissues was notably higher than in the epidermal layer of surrounding healthy tissues (P < 0.05), while the expression intensity of CD123 was considerably elevated compared to the surrounding healthy tissues (P < 0.05). Similarly, the positive rate of CD123 + pDC in the dermal layer of lesional tissues was much higher compared to the surrounding healthy skin tissues (P < 0.05), and the expression intensity of CD123 was remarkably increased compared to the surrounding healthy tissues (P < 0.05) (Table 2).
 |
Table 2 The Positive Rate and Intensity of CD123 Expression in 22 Cases of Eczema and 18 Cases of Normal Skin Around Eczema |
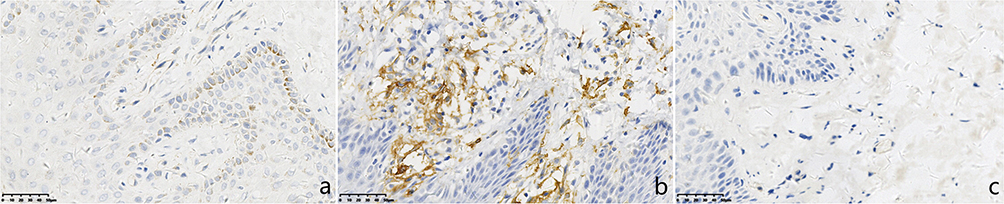 |
Figure 2 Expressions of CD123 in chronic eczema lesions and the perilesional normal skin at the edge (SP *400). (a) Epidermic of skin lesion. (b) Dermis of skin lesion. (c) Perilesional normal skin. (a) A few CD123+ monocyte-like cells with brown cytoplasm were observed in the epidermal of chronic eczema lesions. (b) More CD123+ monocyte-like cells with brown cytoplasm were observed in the dermal papillary layer of chronic eczema lesion. (c) Almost no of CD123+ monocyte-like cells with brown cytoplasm were observed in both epidermal and papillary layer of perilesional normal skin of the lesion. |
Expression and Distribution of TLR7 in Chronic Eczema
TLR7 was mostly expressed in the cell cytoplasm, mainly in the papillary dermis of chronic eczematous lesions (Figure 3). The positive rate of TLR7 expression in the epidermis was increased compared to the surrounding healthy tissues (P < 0.05). However, the expression intensity was not significantly different from that in the surrounding healthy tissues (P > 0.05). The positive rate and expression intensity of TLR7 expression in the dermis were much higher than in the surrounding healthy tissues (P < 0.05) with almost no expression of related factors in the surrounding healthy tissues (Table 3).
 |
Table 3 The Positive Rate and Intensity of TLR7 Expression in 17 Cases of Chronic Eczema and 13 Cases of Normal Skin Around Eczema |
 |
Figure 3 Expressions of TLR7 in chronic eczema lesions and the perilesional normal skin at the edge (SP *400). (a) Epidermic of skin lesion. (b) Dermis of skin lesion. (c) Perilesional normal skin. (a) A few TLR7+ cells with brown cytoplasm were observed in the epidermal of chronic eczema lesions. (b) A few TLR7+ cells with brown cytoplasm were observed in the dermal papillary layer of chronic eczema lesion. (c) Few TLR7+ cells with brown cytoplasm were observed in both epidermal and papillary layer of perilesional normal skin of the lesion. |
Expression and Distribution of TLR9 in Chronic Eczema
TLR9 was expressed in the epidermis of chronic eczema lesions and tissues around the lesions, and the positive rate and there was no notable variation in the positive rate and expression intensity compared to those of the surrounding healthy tissues (P > 0.05), mainly in the basal layer of the epidermis and the cytoplasm of cells. The positive rate and intensity of TLR9 expression in the dermis were significantly higher than in the surrounding healthy tissues (P < 0.05), and were expressed in the nucleus and cytoplasm of the dermis (Figure 4) (Table 4).
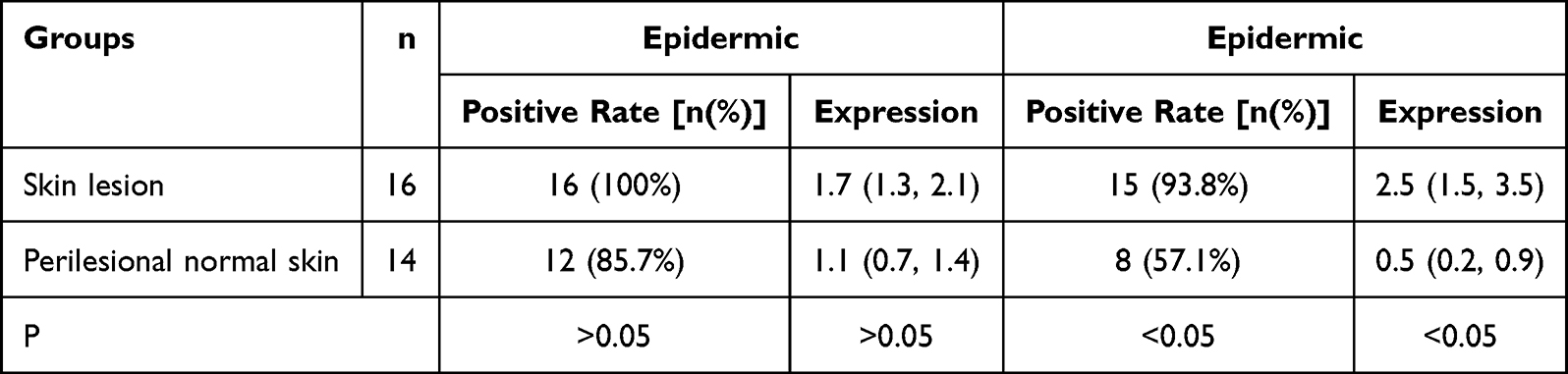 |
Table 4 The Positive Rate and Intensity of TLR9 Expression in 16 Cases of Chronic Eczema and 14 Cases of Normal Skin Around Eczema |
 |
Figure 4 Expressions of TLR9 in chronic eczema lesions and the perilesional normal skin at the edge (SP *400). (a) Epidermic of skin lesion. (b) Dermis of skin lesion. (c) Perilesional normal skin. (a) A few TLR9+ cells with brown cytoplasm were observed in the epidermal of chronic eczema lesions. (b) A few TLR9+ cells with brown cytoplasm were observed in the dermal papillary layer of chronic eczema lesion. (c) Few TLR9+ cells with brown cytoplasm were observed in both epidermal and papillary layer of perilesional normal skin of the lesion. |
Expression and Distribution of IRAK1 in Chronic Eczema
IRAK1 was mainly expressed in the superficial dermis of chronic eczema lesions, with a small amount in the epidermal layer, mainly in the basal layer and spinous layer and the expressing cells were monocytes (in their cytoplasm and nucleus) (Figure 5). The positive rate and intensity of IRAK1 expression in the epidermis of chronic eczema lesions were elevated compared to the surrounding healthy tissues (P < 0.05). The positive rate and expression intensity of IRAK1 in the dermis of chronic eczema lesions was increased compared to the adjacent tissues of the lesions (P < 0.05) (Table 5).
 |
Table 5 The Positive Rate and Intensity of IRAK1 Expression in 23 Cases of Chronic Eczema and 20 Cases of Normal Skin Around Eczema |
 |
Figure 5 Expressions of IRAK1 in chronic eczema lesions and the perilesional normal skin at the edge (SP *400). (a) Epidermic of skin lesion. (b) Dermis of skin lesion. (c) Perilesional normal skin. (a) More IRAK1+ cells with brown cytoplasm were observed in the epidermal of chronic eczema lesions. (b) More IRAK1+ cells with brown cytoplasm were observed in the dermal papillary layer of chronic eczema lesion. (c) Almost no of IRAK1+ cells with brown cytoplasm were observed in both epidermal and papillary layer of perilesional normal skin of the lesion. |
Expression and Distribution of IRF7 in Chronic Eczema
IRF7 is mainly expressed in the dermis with a small amount in the epidermal layer, mainly in the basal layer (Figure 6). The positive rate and expression intensity of IRF7 in the epidermal layer of lesional tissues was notably higher than in the epidermal layer of surrounding healthy tissues (P < 0.05). Similarly, the positive rate and expression intensity of IRF7 in the dermal layer of lesional tissues was much higher compared to the surrounding healthy tissues (P < 0.05) (Table 6).
 |
Table 6 The Positive Rate and Intensity of IRF7 Expression in 22 Cases of Chronic Eczema and 16 Cases of Normal Skin Around Eczema |
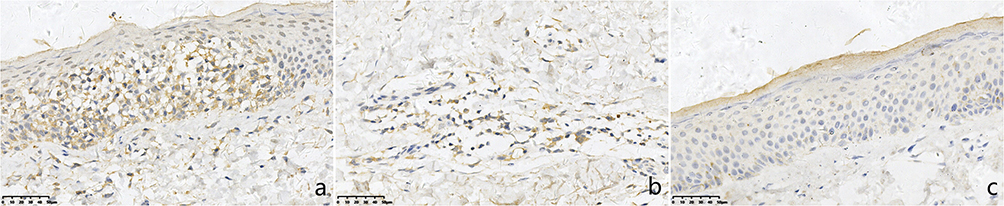 |
Figure 6 Expressions of IRF7 in chronic eczema lesions and the perilesional normal skin at the edge (SP *400). (a) Epidermic of skin lesion. (b) Dermis of skin lesion (c) Perilesional normal skin. (a) More IRF7+ cells with brown cytoplasm were observed in the epidermal of chronic eczema lesions. (b) More IRF7+ cells with brown cytoplasm were observed in the dermal papillary layer of chronic eczema lesion. (c) Almost no of IRF7+ cells with brown cytoplasm were observed in both epidermal and papillary layer of perilesional normal skin of the lesion. |
Discussion
“Eczema”or“atopic dermatitis (AD)”is commonly described by intense itching, erythematous patches, blisters, scabs.1 Related surveys demonstrate eczema as the disease with the highest rate of dermatology-related outpatient visits in China, including its highest rate of initial and subsequent visits.2 Meanwhile, foreign statistical studies on eczema showed that the overall prevalence of eczema was 9.9%,3 indicating that one in ten citizens was afflicted with chronic eczema. In addition, a multi-center study found that higher urbanization and traffic-related exposures may be risk factors for eczema in adults.4 With the development of urbanization, eczema might increasingly become a critical skin disease affecting people’s daily life. However, the pathogenesis of eczema has not yet been clarified, and it is generally known to be closely related to Th1/Th2 immune dysfunction.5 As an important type of eczema, atopic dermatitis has attracted increasing attention from relevant researchers and the public in recent years. Nakashima et al6 found that the main cytokines in the pathogenesis of AD are Th2 cytokines, but Th1 and Th17 immune responses might also be involved in the pathogenesis of some AD subtypes and chronic AD lesions. More studies have found that atopic dermatitis is not limited to Th1 and Th2 immune dysfunction but is caused by Th1/Th2/Th17/Treg multiple cell subsets. At present, the clinical use of Anti-Interleukin-4/Interleukin-13 (Anti-IL-4/IL-13) monoclonal antibody-targeted biological agents, Janus kinase 1 (JAK1) inhibitors and topical glucocorticoids and other treatment methods can effectively relieve clinical symptoms.7–9 However, the condition is still easy to recur, and long-term medication has side effects and causes economic pressure. Therefore, there is no effective way to cure AD. Specific monoclonal antibodies against Th1 and Th17 pathways have been found to be more prone to major side effects compared with Th2 in clinical trials.10 The pathogenesis and progression of atopic dermatitis and eczema need to be further explored. The cases selected in this study were mainly chronic eczematous lesional tissues, and the possibility of their further diagnosis of atopic dermatitis could not be ruled out.
PDCs: a recently discovered subtype of characteristic dendritic cells (DCs) derived from lymphoid precursor DCs with plasmacytoid morphology, and CD2AP and CD123 are specific surface marker molecules for pDCs.11–13 Previous studies have found a significant increase in pDCs and partially activated TLR signaling pathways (TLR7/9, IRAK1, IRF7) in psoriasis vulgaris lesions;14 an increase in pDCs but inactivated TLR signaling pathways in verruca vulgaris (VV) lesions.15 Lin et al16 found that epidermal sensitizer protein allergen (EC) is the most essential sensitization pathway in atopic dermatitis. PDCs mediate the regulation of dermal dendritic cells (dDCs) via IFN-γ and reduces Th2 responses resulting from EC sensitization. PDC is capable of generating large amounts of type I interferons.17 This function plays a critical role in effective antiviral defense. Factors such as impaired epidermal barrier function, chronic inflammation, and disturbed skin flora all contribute to increased viral susceptibility in AD patients.18–20 Chronic eczematous lesions also present similar problems. This study found that CD2AP and CD123 specifically expressed in pDC were higher in chronic eczema lesions than in normal lesions, suggesting that pDCs accumulate in chronic eczema lesions, mainly in the superficial dermis and basal layer of the epidermis.
PDCs can highly express TLR7 and TLR8 as well as TLR9.21 TLR-mediated signaling plays an important role in initiating adaptive immunity. Vijay Kumar22 have revealed that TLR-mediated signaling can directly regulate effector T cells and Treg cells. Activation of TLR8 signaling plays a significant role in the pathogenesis of AD.23 TLR7, TLR8 and TLR9 are localized in intracellular compartments, such as the endoplasmic reticulum, endosome, lysosome, or endolysosome, which are highly homologous and may directly or indirectly affect the pathogenesis of AD. TLR signaling pathways are roughly divided into MyD88- and TRIF-dependent pathways according to specific adaptor recruitment.24 MyD88 can activates the NF-κB signaling pathway.25 NF-κB is another distal signaling pathway during mast-cell activation and is a pivotal transcription factor associated with AD.26,27 TLR7 and TLR9 recruit an adaptor MyD88 containing a Toll-IL-1 receptor (TIR) domain.28 Through TLR7/9-MyD88-IRAKs channels, interleukin 1 receptor-binding kinase-related family IRAKs, are recruited to form a complex with MyD88, Myddosome. Among TLR7, TLR8, and TLR9 signaling in pDCs, IRF7 can bind to the Myddosome and is directly activated by IRAK1 and so on. Activation of IRF7 leads to the induction of Type I IFN.29 And elevated IFN-α can further up-regulate TLR7,30,31 To a certain extent, it plays a positive feedback effect. This research revealed that TLR7/9 expression was notably elevated in dermal tissues of chronic eczema lesions than in the surrounding healthy tissues. At the same time, IRAK1 and IRF7 downstream of the TLR7/9-MyD88-IRAKs pathway were also higher than in the surrounding healthy tissues, mainly in the papillary dermis. Considering that the TLR7/9-MyD88-IRAKs pathway is involved in the inflammatory response to chronic eczema.
Conclusion
In summary, this study investigated the active expression of plasmacytoid dendritic cells (pDCs) and TLR7/9-MyD88-IRAKs pathway in chronic eczema, which suggests that the abnormal increase of pDCs and the abnormal activation of TLR signaling may be involved in the pathogenesis and disease progression of chronic eczema. This research provides a theoretical basis and new directions for the mechanistic study of related subsequent chronic eczema treatment to a certain extent.
Abbreviations
IRF 7, interferon regulatory factor 7; IRAK1, interleukin-1 receptor-associated kinase 1; LCs, Langerhans cells; pDCs, plasmacytoid dendritic cells; TLR7, toll-like receptor 7; TLR9, toll-like receptor 9; VV, verruca vulgaris; DCs, dendritic cells.
Acknowledgments
The authors thank the fund of Health and Family Planning Commission of Zhejiang Province provided funding for this work.
Ethics
Written informed consent was obtained from all participants. The study protocol was approved by Ethics Committee Zhejiang Provincial People ‘s Hospital and the reference number was QT2022282. Participants under 18 years of age in the control group required parental informed consent to participate. And we confirm that our study complies with the Declaration of Helsinki.
Disclosure
Dr Yi Tang reports grants from the fund of Health and Family Planning Commission of Zhejiang Province (2019PY001), during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Navarrete-Rodríguez EM, Del-Río-Navarro BE, Reyes Noriega N, et al. Have the prevalence of eczema symptoms increased in the Mexican pediatric population? Prevalence and associated factors according to Global Asthma Network Phase I. World Allergy Organ J. 2022;15(11):100710. doi:10.1016/j.waojou.2022.100710
2. Zhang G, Gong X, Zhu B, Liu C, Jing L, Jinyu X. 2019年中国医学科学院皮肤病医院门诊病种分析 [Patterns of skin diseases among outpatients attending Hospital of Dermatology of Chinese Academy of Medical Sciences in 2019]. Chin J Dermatol. 2022;55(2):150–152. Chinese.
3. Mortimer K, Lesosky M, García-Marcos L, et al.; Global Asthma Network Phase I Study Group. The burden of asthma, hay fever and eczema in adults in 17 countries: GAN Phase I study. Eur Respir J. 2022;60(3):2102865. doi:10.1183/13993003.02865-2021
4. Juan W, Yinping Z, Baizhan L, et al. Eczema, facial erythema, and seborrheic dermatitis symptoms among young adults in China in relation to ambient air pollution, climate, and home environment. Indoor Air. 2021;32(1):e12918. doi:10.1111/ina.12918
5. Bieber T, Novak N, Herrmann N, Koch S. Erratum to: role of dendritic cells in atopic dermatitis: an update. Clin Rev Allergy Immunol. 2011;41(3):254–258. doi:10.1007/s12016-010-8224-0
6. Nakashima C, Yanagihara S, Otsuka A. Innovation in the treatment of atopic dermatitis: emerging topical and oral Janus kinase inhibitors. Allergol Int. 2021;71(1):40–46. doi:10.1016/j.alit.2021.10.004
7. Aikaterini T, Maria K, George K, et al. The JAK/STAT pathway and its selective inhibition in the treatment of atopic dermatitis: a systematic review. J Clin Med. 2022;11(15):4431. doi:10.3390/jcm11154431
8. Krzysztof S, Magdalena T, Nowicki Roman J. JAK-STAT inhibitors in atopic dermatitis from pathogenesis to clinical trials results. Microorganisms. 2020;8(11):1743. doi:10.3390/microorganisms8111743
9. Aranez V, Ambrus Jr J. Immunologic adverse effects of biologics for the treatment of atopy. Clin Rev Allergy Immunol. 2019;59(2):220–230. doi:10.1007/s12016-019-08739-8
10. Damsin T, Libon F, Nikkels AF, Dezfoulian B. Dermatite atopique : la révolution thérapeutique est en marche [Atopic dermatitis: the therapeutic revolution is underway]. Rev Med Liege. 2022;77(5–6):377–383. French.
11. Dzionek A, Fuchs A, Schmidt P, et al. BDCA-2, BDCA-3, and BDCA-4: three markers for distinct subsets of dendritic cells in human peripheral blood. J Immunol. 2000;165(11):6037–6046. doi:10.4049/jimmunol.165.11.6037
12. Fraga Garth R, Peter C. Plasmacytoid dendritic cells in keratoacanthoma and squamous cell carcinoma: a blinded study of CD123 as a diagnostic marker. J Cutan Pathol. 2020;47(1):17–21. doi:10.1111/cup.13573
13. Narittee S, Aung Phyu P, Cameron YC, et al. Dual expression of TCF4 and CD123 is highly sensitive and specific for blastic plasmacytoid dendritic cell neoplasm. Am J Surg Pathol. 2019;43(10):1429–1437. doi:10.1097/PAS.0000000000001316
14. Tang Y, Qiang Z, Rui H, Wei L, Xiaohua T, Hao C. 寻常型银屑病皮损组织中浆细胞样树突状细胞和TLR7/9通路表达的研究 [Distribution of plasma cell-like dendritic cells and expression of TLR7/9 pathway related molecules in psoriasis vulgaris]. Zhejiang Med J. 2020;42(6):533–535, 539, 647–648. Chinese.
15. Tang Y, Xiaoxia Z, Rui H, Qiang Z, Hao C. Expression of Langerhans cell and plasmacytoid dendritic cell markers, and toll-like receptor 7/9 signaling pathway proteins in verruca vulgaris lesions. Medicine. 2020;99(8):e19214. doi:10.1097/MD.0000000000019214
16. Lin JY, Wu WH, Chen JS, et al. Plasmacytoid dendritic cells suppress Th2 responses induced by epicutaneous sensitization. Immunol Cell Biol. 2020;98(3):215–228. doi:10.1111/imcb.12315
17. Ghanem Mustafa H, Shih Andrew J, Houman K, et al. Proteomic and single-cell transcriptomic dissection of human plasmacytoid dendritic cell response to influenza virus. Front Immunol. 2022;13:814627. doi:10.3389/fimmu.2022.814627
18. Werfel T, Irvine AD, Bangert C, et al. An integrated analysis of herpes virus infections from eight randomized clinical studies of baricitinib in adults with moderate-to-severe atopic dermatitis. J Eur Acad Dermatol Venereol. 2022;36(9):1486–1496. doi:10.1111/jdv.18193
19. Maureen M, De La Cruz Nydia C, Matthias R, Lisa W. Herpes simplex virus 1 can bypass impaired epidermal barriers upon ex vivo infection of skin from atopic dermatitis patients. J Virol. 2022;96(17):e0086422. doi:10.1128/jvi.00864-22
20. Wan J, Shin DB, Syed MN, Abuabara K, Lemeshow AR, Gelfand JM. Risk of herpesvirus, serious, and opportunistic infections in atopic dermatitis: a population-based cohort study. Br J Dermatol. 2021;186(4):664–672. doi:10.1111/bjd.20887
21. Yim LY, Lau CS, Vera Sau-Fong C. Heightened TLR7/9-induced IL-10 and CXCL13 production with dysregulated NF-ҝB activation in CD11chiCD11b+ dendritic cells in NZB/W F1 mice. Int J Mol Sci. 2019;20(18):4639. doi:10.3390/ijms20184639
22. Toll-Like KV. Receptors in adaptive immunity. Handb Exp Pharmacol. 2021;225(3):510–519. doi:10.1007/164_2021_543
23. Yoon W, Kim EJ, Park Y, Kim S, Park YK, Yoo Y. Bacterially delivered miRNA-mediated toll-like receptor 8 gene silencing for combined therapy in a murine model of atopic dermatitis: therapeutic effect of miRTLR8 in AD. Microorganisms. 2021;9(8):1715. doi:10.3390/microorganisms9081715
24. Obayed UM, Sweet Matthew J, Ashley M, Stuart K, Bostjan K. TRIF-dependent TLR signaling, its functions in host defense and inflammation, and its potential as a therapeutic target. Journal of leukocyte biology. 2016; 100(1):27–45. DecauxG. Long-term treatment of patients with inappropriate secretion of antidiuretic hormone by the vasopressin receptor antagonist conivaptan, urea, or furosemide. Am J Med. 2001;110:582–584. doi:10.1016/s0002-9343(01)00678-7
25. Kawai T, Akira S. The role of pattern-recognition receptors in innate immunity: update on toll-like receptors. Nat Immunol. 2010;11(5):373–384. doi:10.1038/ni.1863
26. Kang YM, Kim HM, Lee M, An HJ. Oleanolic acid alleviates atopic dermatitis-like responses in vivo and in vitro. Int J Mol Sci. 2021;22:12000. doi:10.3390/ijms222112000
27. Li G, Wu H, Sun L, et al. (-)-α-bisabolol alleviates atopic dermatitis by inhibiting MAPK and NF-κB signaling in mast cell. Molecules. 2022;27(13):3985. doi:10.3390/molecules27133985
28. Uematsu S, Takeuchi O, Kato H, et al. Interleukin-1 receptor-associated kinase-1 plays an essential role for Toll-like receptor (TLR)7- and TLR9-mediated interferon-{alpha} induction. J Exp Med. 2005;201(6):915–923. doi:10.1084/jem.20042372
29. Duan T, Du Y, Xing C, Wang HY, Wang RF. Toll-like receptor signaling and its role in cell-mediated immunity. Front Immunol. 2022;13:812774. doi:10.3389/fimmu.2022.812774
30. Melissa S, Marco C. The multifaceted biology of plasmacytoid dendritic cells. Nat Rev Immunol. 2015;15(8):471–485. doi:10.1038/nri3865
31. Yutaro K, Himanshu K, Shohei K, Taro K, Osamu T, Shizuo A. Cutting edge: TLR-Dependent viral recognition along with type I IFN positive feedback signaling masks the requirement of viral replication for IFN-{alpha} production in plasmacytoid dendritic cells. J Immunol. 2009;182(7):3960–3964. doi:10.4049/jimmunol.0804315
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.