Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 17
The Estimation of Cementoenamel Junction Crestal Bone Distance in Mandibular Anterior Teeth
Authors Ahmed AS ![]() , Ali BJ, Hassan BK
, Ali BJ, Hassan BK ![]() , Sabah Mohammad A
, Sabah Mohammad A ![]()
Received 19 August 2024
Accepted for publication 6 December 2024
Published 8 January 2025 Volume 2025:17 Pages 13—20
DOI https://doi.org/10.2147/CCIDE.S492129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Ammar Sh Ahmed,1 Banaz Jabbar Ali,2 Ban Karem Hassan,2 Abbas Sabah Mohammad3
1Department of Pedodontics, Orthodontic and Preventive Dentistry, College of Dentistry, Mustansiriyah University, Baghdad, Iraq; 2Department of Periodontics, College of Dentistry, Mustansiriyah University, Baghdad, Iraq; 3Al-Sabah Center, Al- Yarmouk, Baghdad, Iraq
Correspondence: Ban Karem Hassan, College of Dentistry, Mustansiriyah University, 6 street Al Mustansiriya, Baghdad, 10052, Iraq, Tel +9647901468790, Email [email protected], [email protected]
Purpose: The study aimed to measure the distance from the cementoenamel junction (CEJ) to the alveolar bone crest on both the buccal and lingual sides of the anterior mandibular teeth utilizing cone beam computed tomography (CBCT).
Materials and Methods: Cone-beam computed tomography (CBCT) was utilized to measure the distance between CEJ and the alveolar bone crest on both the buccal and lingual sides of the mandible’s anterior teeth.
Results: The mean of the distance on buccal side for the central, lateral, and canine teeth were (1.6 mm), (1.6 mm), and (1.5 mm) respectively. On the lingual side, the mean for all teeth (central, lateral, and canine) was 1.7 mm. The study demonstrated a significant difference in distance across age groups (< 30 and ≥ 30 years) for all teeth on both the buccal and lingual sides, except for the canine on the buccal side.
Conclusion: The distance from the CEJ to the bone crest on both the buccal and lingual sides varies significantly by age group. This data is essential for developing orthodontic, implant, and periodontal therapies.
Keywords: alveolar bone crest, canines, cementoenamel junction, central incisors, cone-beam computed tomography, lateral incisors
Introduction
Cone beam computed tomography (CBCT) is the principal tool for assessing alveolar bone form in oral diagnostics. Several studies have found no significant difference in CBCT accuracy in evaluating alveolar bone thickness or height vs physical direct bone measurement, the gold standard for reference.1,2
The most recent radiographic technology for the maxillofacial region is CBCT. In contrast to panoramic images, CBCT provides an accurate view of the jawbone. Measurements are unreliable due of the distortion in panoramic photos. In addition, CBCT can generate cross-sectional (buccolingual), axial, coronal, sagittal, and panoramic views. Conventional panorama cameras only produce one-dimensional images, either mesiodistal or anteroposterior, with the option of superimposing photos.3
The advantages of cone beam computed tomography (CBCT) are the ability to assess all possible locations and anatomical features, the absence of superimposition, and uniform magnification. Furthermore, the cost and effective dosage are less than those of multidetector CT (MDCT). In reality, the effective dose of CBCT is over 45 times lower than MDCT.4
CBCT has been shown in numerous studies to accurately measure alveolar bone loss.5,6 CBCT images were used in several investigations to quantify the thickness of facial bone on anterior teeth as well as the distance between the CEJ and the alveolar bone crest.7–12
Periodontitis is a persistent, host-mediated inflammation defined by dental plaque contamination that results in alveolar bone loss13 According to the consent report from the Classification World Workshop 2017, the loss rate in alveolar bone was used to directly predict the severity and progression of periodontitis.14 The cementoenamel junction (CEJ) is the anatomical separation of the crown and root surfaces.15 The distance between the CEJ and the facial bone crest (FBC) may be an essential factor. Some authors found a direct relationship between the patient’s age and this distance.7,8 The cementoenamel junction (CEJ) is a static marker used to assess clinical attachment loss (CAL) or periodontal disease.16
CAL is the most effective measure of periodontal damage, and it has been used to study the major risk factors of periodontal disease in adults.17,18 The radiographic measurement of alveolar bone height and clinical attachment loss (CAL) is used to assess the decline of supporting periodontal tissue in periodontitis13,19,20 as well as to track disease progression and therapy impact on the periodontium.21,22
Thus, the CEJ is an important marker for periodontists; yet, various challenges arise when measuring the CEJ, such as difficulty probing, particularly when it is subgingival.23 Periodontal disease is characterized by connective tissue loss and alveolar bone degeneration that begins at the coronal level.24 Assessing the residual alveolar bone prior to periodontal therapy is critical for developing a more accurate treatment plan because it provides trustworthy information on the hard tissue architecture.25
Although cone-beam computed tomography (CBCT) enhances imaging precision and three-dimensional evaluation of bone structures, nothing is known about its specific role in precisely identifying the distance between the cementoenamel junction (CEJ) and the bone crest. This measurement is significant in orthodontics, periodontics, and implantology since bone height and shape influence treatment outcomes as well as problems prevention.26,27 However, there is still a lack of robust evidence comparing CBCT to traditional imaging modalities in terms of diagnostic value and clinical decision-making, as well as consensus on standardized protocols for using CBCT for CEJ-bone crest exams. Future study is needed to quantify the benefits of CBCT in identifying bone levels, set criteria for its use in CEJ-bone crest examinations, and determine its usefulness in enhancing treatment regimens across dentistry specialties.28 The present study aimed to evaluate the distance from the cementoenamel junction (CEJ) to the bone crest buccally and the bone crest lingually of mandibular anterior teeth.
Materials and Method
The study’s participants underwent CBCT scans for a variety of reasons, including impacted tooth extraction, dental implant therapy, and orthodontic therapy. A total of 104 CBCT images were evaluated. 1248 surface area for the six lower anterior teeth. The G*Power 3.1 software was used to calculate the sample size of teeth surface, with a statistical power of 90% with the adjusted alpha value of (0.0008) was used for Type I error after applying the (Bonferroni correction).
Between 2019 and 2022, all CBCT scans were performed to diagnose or plan a treatment. The images were captured using the same equipment and typical settings. All of the scans were requested as part of normal dental care. This study has been approved by Pedodontics, Orthodontic and Preventive Dentistry scientific committee at College of Dentistry, Mustansiriyah University. Because the study was retrospective in nature, no further approval was required. No patient consent was required by the institutional review board because the data being used does not contain direct identifiers such as name or medical record number and the study complied with the Declaration of Helsinki. A structured study protocol was followed to collect the following data for each patient: sex, age, distance. CEJ-FBC and CEJ-LBC at central incisors (CI), lateral incisors (LI), and canines (C) on both the buccal and lingual sides of mandibular teeth, as well as the right and left sides.
Inclusion and Exclusion Criteria
CBCTs from people over the age of 18 with no history of orthodontic treatment or significant tooth resorption were included. The study excluded people under the age of 18, as well as those who had dental implants, prosthetic or endodontic restorations on their anterior mandibular teeth. Participants who had been traumatized or were undergoing osseous/regenerative surgery were excluded.
Radiographic Image Analysis
The study included CBCT pictures from 64 females and 40 males aged 18 to 60 (mean age 32.3 +_ 10.4). A Rotograph Evo 3D CBCT machine was utilized, with the following exposure parameters: 86 kV, 5 mA, 6–8 seconds exposure time, and 0.4 mm voxel size (Figure 1).
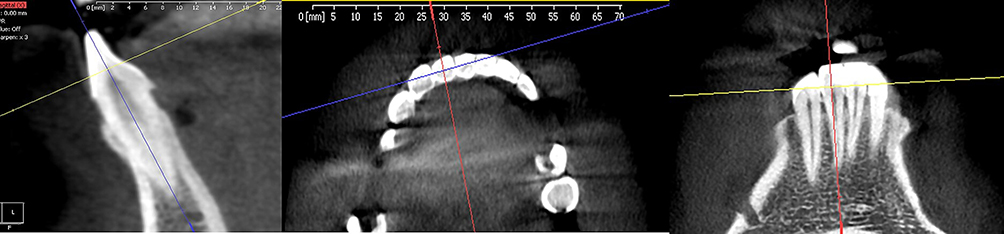 |
Figure 1 Identifying tooth long axis in the three planes. |
Upper and lower dental arches were captured in an 8 cm x 8 cm cylindrical field of view. The examination focused on the mandibular incisors and canines. First, the Villa 3D planner application was used to create an axial cross-section at the level of dental fissures on the mandibular anterior teeth. Next, a line was drawn at the highest convexity of the tooth’s vestibular contour, followed by another at the maximum convexity of its lingual face. The lines were drawn consistently in the middle of the root canal cross-section.
We used the following steps to identify the slice position for the measurements: the roots long axis was identified in the centre of the tooth in axial, coronal and sagittal plane. The alveolar crest was identified in the axial plane, and a buccopalatal slice was traced across the center of the root. The coronal slice was then used to calculate the root’s long axis. Figure 1 depicts anatomic sites (FAB, CEJ, and LBC) used as reference points. Measurements were taken from the CEJ to the FBC and the CEJ to the LBC (Figure 2).
 |
Figure 2 Measurement of BBC-CEJ and LBC-CEJ. |
Statistical Analysis
Data was introduced into Microsoft Excel and analyzed using IBM-SPSS Statistics 26 software. Descriptive statistics characterised the data using frequency, percentage, mean, standard deviation, minimum and maximum. The data was examined using the Shapiro–Wilk test, and the Levene's test assessed the normality and homogeneity of the data, which found that it was not normally distributed. Consequently, the Mann–Whitney test was employed to compare the two groups between gender, site, side and age groups. The P-value <0.05 was considered statistically significant. The graph was made using GraphPad-Prism version 10.
The teeth were analyzed using CBCT. After a week, the same radiologist collected and evaluated the data. A paired t-test was used on 11 random CBCT scans to measure intraobserver reliability, and no significant differences were discovered.
Result
A total of 104 images of CBCT were used in this study for the six anterior teeth, including images from 40 males and 64 females. 1248 surfaces were included in this study, with age range (18–60) years and a mean of 32.3 years.
Table 1 shows descriptive information, including (mean, SD, Minimum and Maximum) for CEJ-BBC and CEJ-LBC measures on the six anterior teeth. Table 2 and 3 compare the mean (BBC - CEJ) (LBC - CEJ) distance according to gender, tooth side, and age using the Mann–Whitney test.
 |
Table 1 Descriptive Statistics for All Variables Showing Mean Value, Standard Deviation, Minimum and Maximum Values for Each Variable |
 |
Table 2 The Mean Distance Between the CEJ and BBC at Different Variable |
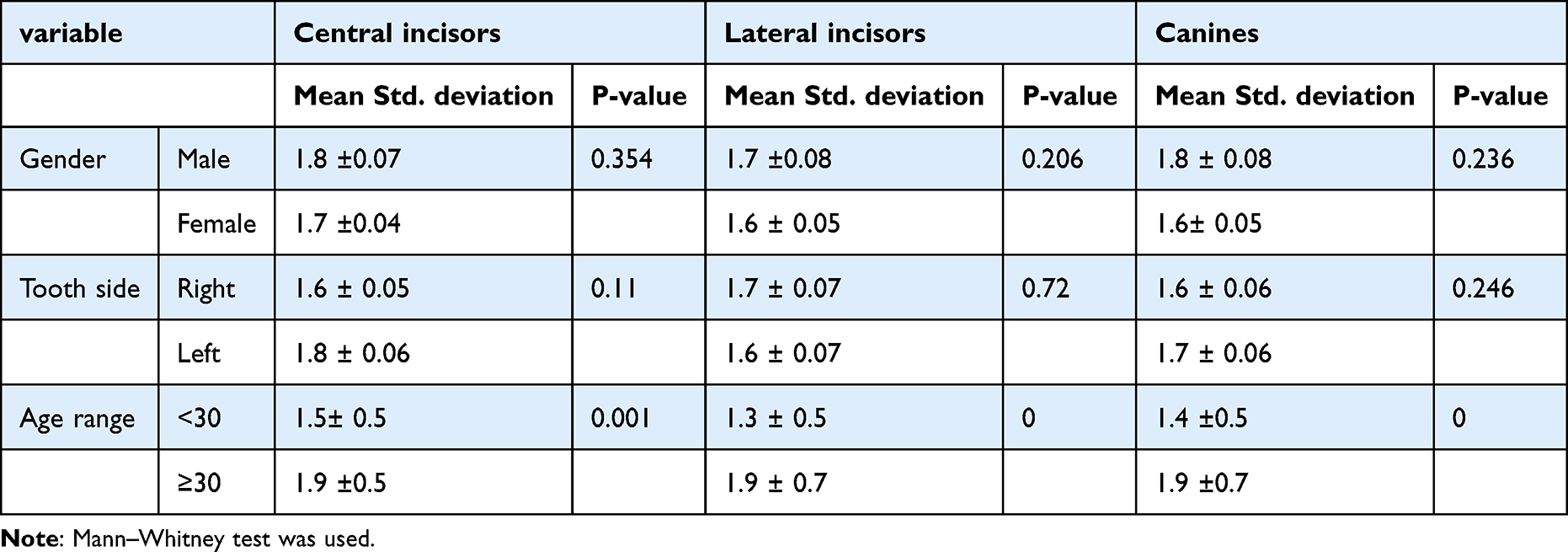 |
Table 3 The Mean Distance Between the CEJ and LBC at Different Variable |
There was no significant difference across tooth sides, in gender we found a significant difference in (CEJ-BBC) only in laterals, while when comparing the distance according to age, we found a significant difference in (BBC - CEJ) and (LBC - CEJ) in all teeth except in canine when we measure (CEJ-BBC) as in Figures 3 and 4, and when we compare the distances of (CEJ-BBC) and (CEJ-LBC) for the central, lateral and canine, there were significant between them except for lateral; there was no significant difference. As shown in Figure 5.
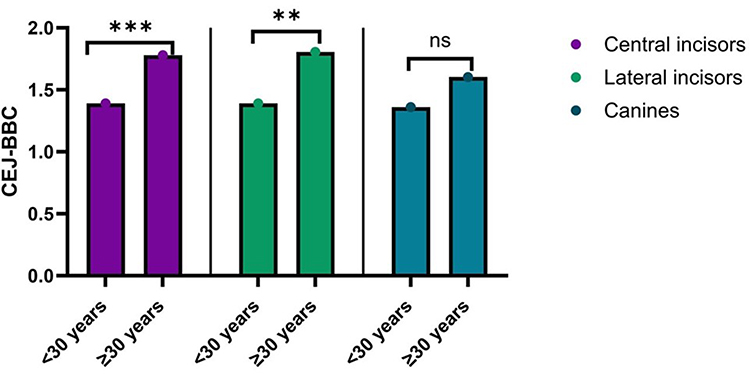 |
Figure 3 Assessment the distances of (CEJ-BBJ) between different age groups. Significant difference ** p < 0.01, *** p < 0.001 using man Whitney test, ns indicate not significant. |
 |
Figure 4 Assessment the distances of (LBJ- CEJ) between different age groups. Significant difference ** p < 0.01, *** p < 0.001 using man Whitney test. |
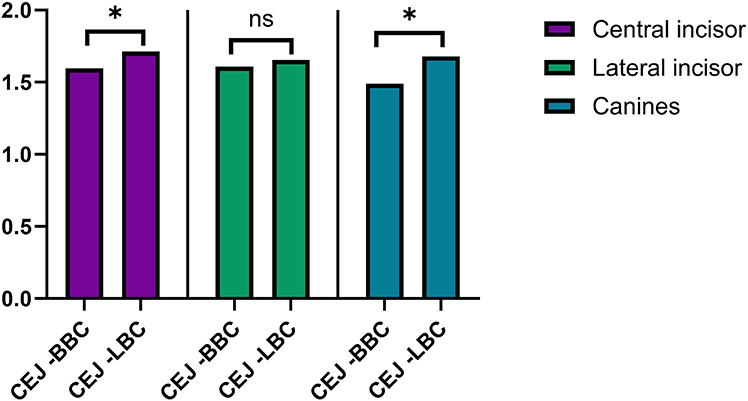 |
Figure 5 Comparison of the distances between (CEJ-BBC) and (CEJ_LBC) for the (central, lateral incisor and canine). Significant difference * p < 0.05, ns indicate not significant. |
Discussion
The main purpose of this study was to assess the distance from the cementoenamel junction to the buccal bone crest (CEJ-BBC) and from the cementoenamel junction to the lingual bone crest (CEJ-LBC) for the six lower anterior teeth (left canine, lateral, central and right central, lateral, canine).
The biological parameter is the distance between the cementoenamel junction and the bone crest, which includes connective tissue and junctional epithelium.29 Periodontal disease is well known to cause connective tissue loss and alveolar bone degradation, which begins at the coronal level.24 In periodontology, the clinical attachment level is the primary clinical metric, acting as a meaningful standard for both short and long-term evaluation.30 In CBCT, reference points and lines were used to determine alveolar bone changes, including the tooth apex, cementoenamel junction, and long axis. The alveolar crest (AC) is the highest coronal elevation of the alveolar bone.31
The loss of alveolar bone gives a decent indicator of the total supporting structures’ attachment loss.32 A radiographic examination of periodontal bone loss is crucial for diagnosing, treating, and predicting the outcome of periodontitis.33 Periapical, bitewing, and panoramic radiographs were commonly used during radiographic examinations.33,34 Plain radiography suffers from inherent constraints such as distortion, magnification, and superimposition of surrounding anatomical features34–36 These disadvantages frequently restrict the use of these radiographs.33
According to our study, the estimated distances from the CEJ to BBC for central, lateral and canine (1.6+_0.6, 1.6+_0.6 and 1.5+_0.6) and CEJ and LBC (1.7+_0.6, 1.7+_0.7 and 1.8+_0.6) and this is less than found in Srebrzyńska-Witek et al study37 in which the mean for CEJ and BBC in central, lateral and canine are (2.26+-0.08,2.29+_0.08 and 2.34+_0.09) and for CEJ and LBC (2.54+_0.1,2.51+_0.09 and 2.51+_0.09). According to previous studies38–40 the normal range for bone height around the CEJ is 1 to 3 mm.
The studies investigate that people without periodontal disease often have space of 2 mm.41 For younger individuals, the average height of alveolar bone at the CEJ is 1.4 mm, but the average rises to 3 mm for those over 45 years old.42
According to Armitage, a radiographic measurement of 2 mm or greater from the CEJ to the bone crest is a good cut-off indicating bone loss.43 According to Darby et al 2005, there is no bone loss if the gap between the CEJ and alveolar bone crest level is ≤2 mm, while if the distance is >2 and less than 3, consider bone loss and definitive bone loss if the distance is ≥3 mm.44
Comparing the distance from CEJ to the bone in different age groups revealed statistically significant differences (p = 0.000) between age groups (less than 30 years and ≥ 30 years) in which increased bone loss with increased age, and this is in agreement with AlTarawneh et al45 who found significant differences (p < 0.05) in the distance from CEJ to the bone in different age groups for all points of measurement (CEJ-Distal, CEJ-Midlabial, CEJ-Mesial) on all teeth except that for lateral incisors on CEJ-Midlabial, on canines at CEJ-Midlabial, and CEJ-Distal. However, distances increased with age for all points of measurement. These results are consistent with other investigations,7,12 other research found no significant variations for these parameters with increasing age.11,46 Some investigations have reported increased (CEJ-FBC) distance among adults 50 or older.8,12
Conclusions
CBCT accurately determines the position of the CEJ about the BBC and LBC. There is a statistically significant variation in the distance between the CEJ and the alveolar bone crest both buccally and lingually across age groups (under 30 vs 30+). The collected data is vital for designing orthodontic, implant, and periodontal treatments.
Acknowledgments
The authors would like to thank Mustansiriyah University / Baghdad- Iraq for its support in the present work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Van Dessel J, Nicolielo L, Huang Y, et al. Accuracy and reliability of different cone beam computed tomography (CBCT) devices for structural analysis of alveolar bone in comparison with multislice CT and micro-CT. Eur J Oral Implantol. 2017;10(1):95–105.
2. Li Y, Deng S, Mei L, et al. Accuracy of alveolar bone height and thickness measurements in cone beam computed tomography: a systematic review and meta-analysis. Oral Surg Oral Medi Oral Pathol Oral Radiology. 2019;128(6):667–679. doi:10.1016/j.oooo.2019.05.010
3. Perschbacher S. Making the Most of Cone Beam CT. Responsibly. Oral Health. 2009;99(7):6.
4. Ludlow JB, Ivanovic M. Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol. 2008;106(1):106–114. doi:10.1016/j.tripleo.2008.03.018
5. Vandenberghe B, Jacobs R, Yang J. Detection of periodontal bone loss using digital intraoral and cone beam computed tomography images: an in vitro assessment of bony and/or infrabony defects. Dentomaxillofacial Radiol. 2008;37(5):252–260. doi:10.1259/dmfr/57711133
6. Banodkar AB, Gaikwad RP, Gunjikar TU, Lobo TA. Evaluation of accuracy of cone beam computed tomography for measurement of periodontal defects: a clinical study. J Indian Soci Periodon. 2015;19(3):285–289. doi:10.4103/0972-124X.154176
7. Zekry A, Wang R, Chau AC, Lang NP. Facial alveolar bone wall width–a cone‐beam computed tomography study in A sians. Clin Oral Implants Res. 2014;25(2):194–206. doi:10.1111/clr.12096
8. Ghassemian M, Nowzari H, Lajolo C, Verdugo F, Pirronti T, D’Addona A. The thickness of facial alveolar bone overlying healthy maxillary anterior teeth. J Periodon. 2012;83(2):187–197. doi:10.1902/jop.2011.110172
9. Vera C, De Kok IJ, Reinhold D, et al. Evaluation of buccal alveolar bone dimension of maxillary anterior and premolar teeth: a cone beam computed tomography investigation. Int J Oral Maxillofac Implants. 2012;27(6).
10. El Nahass H, Naiem N. Analysis of the dimensions of the labial bone wall in the anterior maxilla: a cone‐beam computed tomography study. Clin Oral Implants Res. 2015;26(4):e57–e61. doi:10.1111/clr.12332
11. Januário AL, Duarte WR, Barriviera M, Mesti JC, Araújo MG, Lindhe J. Dimension of the facial bone wall in the anterior maxilla: a cone‐beam computed tomography study. Clin Oral Implants Res. 2011;22(10):1168–1171. doi:10.1111/j.1600-0501.2010.02086.x
12. H-m W, J-w S, M-f Y, X-y C, Q-h J, F-m H. Analysis of facial bone wall dimensions and sagittal root position in the maxillary esthetic zone: a retrospective study using cone beam computed tomography. Int J Oral Maxillofac Implants. 2014;29(5).
13. Papapanou PN, Sanz M, Buduneli N, et al. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions. J Periodon. 2018; 89:S173–S82.
14. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodon. 2018; 89:S159–S72.
15. Ceppi E, Dall’Oca S, Rimondini L, Pilloni A, Polimeni A. Cementoenamel junction of deciduous teeth: SEM-morphology. Eur J Paediatr Dent. 2006;7(3):131–134.
16. Preshaw P, Kupp L, Hefti A, Mariotti A. Measurement of clinical attachment levels using a constant‐force periodontal probe modified to detect the cementoenamel junction. Journal of Clinical Periodontology. 1999;26(7):434–440. doi:10.1034/j.1600-051X.1999.260704.x
17. Yaragani A, Sushuma K, Guduri V, et al. The influence of tobacco consumption on periodontal health: a stratified analysis based on type of tobacco use. J Fam Med Primary Care. 2020;9(4):2061–2066. doi:10.4103/jfmpc.jfmpc_1071_19
18. Duque A, Martínez P-J, Giraldo A, et al. Accuracy of cotinine serum test to detect the smoking habit and its association with periodontal disease in a multicenter study. Medicina Oral, Patología Oral y Cirugía Bucal. 2017;22(4):e425. doi:10.4317/medoral.21292
19. Dietrich T, Ower P, Tank M, et al. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions–implementation in clinical practice. Br Dent J. 2019;226(1):16–22. doi:10.1038/sj.bdj.2019.3
20. Hoath B, Wiebe C, Fulle De Owen MI G, Giannelis G, Larjava H. Current status of the classification of periodontal diseases. Canadian J Dental Hygi. 2016;50(3).
21. Goodson J, Haffajee A, Socransky S. The relationship between attachment level loss and alveolar bone loss. Journal of Clinical Periodontology. 1984;11(5):348–359. doi:10.1111/j.1600-051X.1984.tb01331.x
22. Hossain MZ, Fageeh HN, Elagib MFA. Prevalence of periodontal diseases among patients attending the outpatient department at the college of dentistry, King Khalid University, Abha, Saudi Arabia. City Dental College J. 2018;10(1):9–12. doi:10.3329/cdcj.v10i1.13835
23. Hug H, Van’t Hof M, Spanauf A, Renggli H. Validity of clinical assessments related to the cemento-enamel junction. J Dental Rese. 1983;62(7):825–829. doi:10.1177/00220345830620071301
24. Hou Y, Wang X, Zhang C-X, et al. Risk factors of periodontal disease in maintenance hemodialysis patients. Medicine. 2017;96(35):e7892.
25. Leung CC, Palomo L, Griffith R, Hans MG. Accuracy and reliability of cone-beam computed tomography for measuring alveolar bone height and detecting bony dehiscences and fenestrations. Am J Orthodontics Dentofacial Orthopedics. 2010;137(4):S109–S19. doi:10.1016/j.ajodo.2009.07.013
26. Shujaat S, Keen D, Siddiqui Z. The role of CBCT in diagnosing and managing periodontal disease: a systematic review. Internl J Peri Resto De. 2020;40(5):665–671.
27. Papageorgiou SN, Almuzian M, Bearn D, et al. Comparative analysis of CBCT vs. panoramic radiographs in orthodontics: diagnostic accuracy and limitations. European J Orthod. 2018;40(5):519–526. doi:10.1093/ejo/cjx093
28. Lee SM. Assessing alveolar bone loss using cone-beam computed tomography: a review of methodologies and clinical applications. J Clinical Periodon. 2019;46(10):1052–1062.
29. Lindhe J, Lang NP, Karring T. Clinical Periodontology and Implant Dentistry. Blackwell Munksgaard Oxford; 2008.
30. Rheu G-B, Ji S, Ryu -J-J, et al. Risk assessment for clinical attachment loss of periodontal tissue in Korean adults. J Adv Prosthodontics. 2011;3(1):25. doi:10.4047/jap.2011.3.1.25
31. Kook Y-A, Kim G, Kim Y. Comparison of alveolar bone loss around incisors in normal occlusion samples and surgical skeletal class III patients. Angle Orthodontist. 2012;82(4):645–652. doi:10.2319/070111-424.1
32. Kiliç A, Efeoglu E, Yilmaz S, Orgun T. The relationship between probing bone loss and standardized radiographic analysis. Periodo Clini Investig. 1998;20(1):25–32.
33. Corbet E, Ho D, Lai S. Radiographs in periodontal disease diagnosis and management. Australian Dental Journal. 2009; 54:S27–S43.
34. Mol A. Imaging methods in periodontology. Periodontology. 2000;34(1):34–48. doi:10.1046/j.0906-6713.2003.003423.x
35. Kim TS, Obst C, Zehaczek S, Geenen C. Detection of bone loss with different X‐ray techniques in periodontal patients. J Periodon. 2008;79(7):1141–1149. doi:10.1902/jop.2008.070578
36. Brägger U. Radiographic parameters: biological significance and clinical use. Periodontology. 2000;39(1):73–90. doi:10.1111/j.1600-0757.2005.00128.x
37. Srebrzyńska-Witek A, Koszowski R, Różyło-Kalinowska I, Piskórz M. CBCT for estimation of the cemento-enamel junction and crestal bone of anterior teeth. Open Med. 2020;15(1):774–781. doi:10.1515/med-2020-0211
38. de Faria Vasconcelos K, Evangelista K, Rodrigues C, Estrela C, De Sousa T, Silva M. Detection of periodontal bone loss using cone beam CT and intraoral radiography. Dentomaxillofacial Radiol. 2012;41(1):64–69. doi:10.1259/dmfr/13676777
39. Zhou Z, Chen W, Shen M, Sun C, Li J, Chen N. Cone beam computed tomographic analyses of alveolar bone anatomy at the maxillary anterior region in Chinese adults. J Biomed Res. 2014;28(6):498. doi:10.7555/JBR.27.20130002
40. Mol A, Balasundaram A. In vitro cone beam computed tomography imaging of periodontal bone. Dentomaxillofacial Radiol. 2008;37(6):319–324. doi:10.1259/dmfr/26475758
41. Wong BK, Leichter JW, Chandler NP, Cullinan MP, Holborow DW. Radiographic study of ethnic variation in alveolar bone height among New Zealand dental students. J Periodon. 2007;78(6):1070–1074. doi:10.1902/jop.2007.060366
42. Persson RE, Hollender LG, Persson GR. Assessment of alveolar bone levels from intraoral radiographs in subjects between ages 15 and 94 years seeking dental care. J Clinical Period. 1998;25(8):647–654. doi:10.1111/j.1600-051X.1998.tb02501.x
43. Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999;4(1):1–6. doi:10.1902/annals.1999.4.1.1
44. Darby IB, Lu J, Calache H. Radiographic study of the prevalence of periodontal bone loss in Australian school‐aged children attending the Royal Dental Hospital of Melbourne. J Clinical Period. 2005;32(9):959–965. doi:10.1111/j.1600-051X.2005.00767.x
45. AlTarawneh S, AlHadidi A, Hamdan AA, Shaqman M, Habib E. Assessment of bone dimensions in the anterior maxilla: a cone beam computed tomography study. J Prosthodontics. 2018;27(4):321–328. doi:10.1111/jopr.12675
46. Nowzari H, Molayem S, Chiu CHK, Rich SK. Cone beam computed tomographic measurement of maxillary central incisors to determine prevalence of facial alveolar bone width≥ 2 mm. Clin Implant Denti Related Res. 2012;14(4):595–602. doi:10.1111/j.1708-8208.2010.00287.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.