Back to Journals » Journal of Inflammation Research » Volume 15
The Efficacy of Percutaneous Transhepatic Gallbladder Drainage Combined with Gallbladder-Preserving Cholecystolithotomy in High-Risk Patients with Acute Calculous Cholecystitis
Authors Kang C, Zhang J, Hou S, Wang J, Li X, Li X, Chi X, Shan H, Zhang Q, Liu T
Received 22 February 2022
Accepted for publication 13 April 2022
Published 10 May 2022 Volume 2022:15 Pages 2901—2910
DOI https://doi.org/10.2147/JIR.S363610
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monika Sharma
Chunbo Kang, Jie Zhang, Shiyang Hou, Jinlei Wang, Xubin Li, Xiaowei Li, Xiaoqian Chi, Haifeng Shan, Qijun Zhang, Tiejun Liu
General Surgery Department, Beijing Rehabilitation Hospital of Capital Medical University, Beijing, 100144, People’s Republic of China
Correspondence: Tiejun Liu, General Surgery Department, Beijing Rehabilitation Hospital of Capital Medical University, Xixiazhuang, Badachu Road, Shijingshan District, Beijing, 100144, People’s Republic of China, Tel/Fax +86 10 5698 1152, Email [email protected]
Objective: This study aimed to investigate the value of combining percutaneous transhepatic gallbladder drainage (PTGD) with gallbladder-preserving cholecystolithotomy (GPC) in high-risk patients with acute calculous cholecystitis.
Methods: Clinical data from 74 high-risk patients with acute calculous cholecystitis, admitted to our hospital between October 2018 and September 2021, were analyzed retrospectively. All the patients underwent PTGD, and 59 of them underwent delayed cholecystectomy, while 14 patients were subjected to GPC 8– 12 weeks after the PTGD; one patient, whose life expectancy was fewer than 6 months, was not treated for gallstones after PTGD.
Results: In all 74 patients, symptom remission was achieved after the PTGD therapy, and the incidence of catheter-related complications was 10.8%. Among the 59 patients who underwent delayed cholecystectomy (DC) after PTGD, there was a complication incidence of 6.8%. Of the 14 patients who underwent GPC after the PTGD, 13 patients were subjected to the removal of drainage tubes, 1 patient received cholecystostomy catheter draining externally, and two patients (14.3%) had complications. There were no perioperative deaths.
Conclusion: Percutaneous transhepatic gallbladder drainage, combined with GPC, is a safe and effective treatment that is suitable for high-risk patients with acute calculous cholecystitis who cannot receive DC. This combined method allows for early acute cholecystitis to settle, helps to remove gallstones at a later stage, and solves the problem of long-term tube drainage after PTGD.
Keywords: percutaneous transhepatic gallbladder drainage, PTGD, gallbladder-preserving cholecystolithotomy, GPC, high-risk acute calculous cholecystitis
Corrigendum for this paper has been published.
Acute calculous cholecystitis is a common cholelithiasis complication for which the optimal therapy approach is laparoscopic cholecystectomy.1,2 Generally, the mortality rate is less than 0.5% for both open and laparoscopic cholecystectomy. However, cholecystectomy causes a markedly increased incidence of mortality in patients with a high surgical risk, and the mortality of elderly patients and patients with internal medical comorbidity can be as high as 10%,3 with the maximum reported mortality being 16.6%.4 Percutaneous transhepatic gallbladder drainage (PTGD) is a minimally invasive, safe, and effective non-surgical therapy that is particularly suitable for patients with acute calculous cholecystitis who present at high surgical risk.5–7 Additionally, PTGD can promptly relieve gallbladder pressure and cholecystitis symptoms, avoid a series of complications linked to acute calculous cholecystitis, and help patients with acute calculous cholecystitis with a high surgical risk to manage the acute critical period.8 For most patients, if their general condition allows them to endure general anesthesia and cholecystectomy after the remission of acute cholecystitis, delayed cholecystectomy (DC) is performed. In general, for high-risk patients who still cannot undergo delayed cholecystectomy after PTGD, long-term biliary drainage is needed, but it reduces the quality of life and comfort of patients, and increases the incidence of complications and readmission.9 As an alternative, gallbladder-preserving cholecystolithotomy (GPC) under local anesthesia or conscious sedation can be performed on a small number of patients with gallstones who have a high surgical risk and are in a poor general condition and cannot endure general anesthesia or cholecystectomy.
Materials and Methods
Between October 2018 and September 2021 in our hospital, a total of 74 high-risk patients with acute calculous cholecystitis (The Tokyo Guidelines, Grade III10) underwent PTGD therapy; 59 of these patients underwent DC and 14 patients were subjected to GPC 8–12 weeks after the PTGD. Additionally, 13 patients were subjected to the removal of drainage tubes, one patient received cholecystostomy catheter draining externally due to an obstructed cystic duct. In addition, another patient continued the drainage with a PTGD tube instead of other therapies for gallstones after the PTGD because their life expectancy was less than 6 months.
Patient Demographics
A retrospective analysis was conducted of the data of 74 high-risk patients with acute calculous cholecystitis. These patients consisted of 33 males and 41 females and were aged 66–98 years, with an average age of (73.1 + 6.3) years. Among them, 65 patients had multiple gallstones, 9 patients had a single gallstone, and 3 patients had combined choledocholithiasis, as shown in Table 1. These patients were assessed as grade III according to the Tokyo Guidelines for acute cholecystitis at admission.
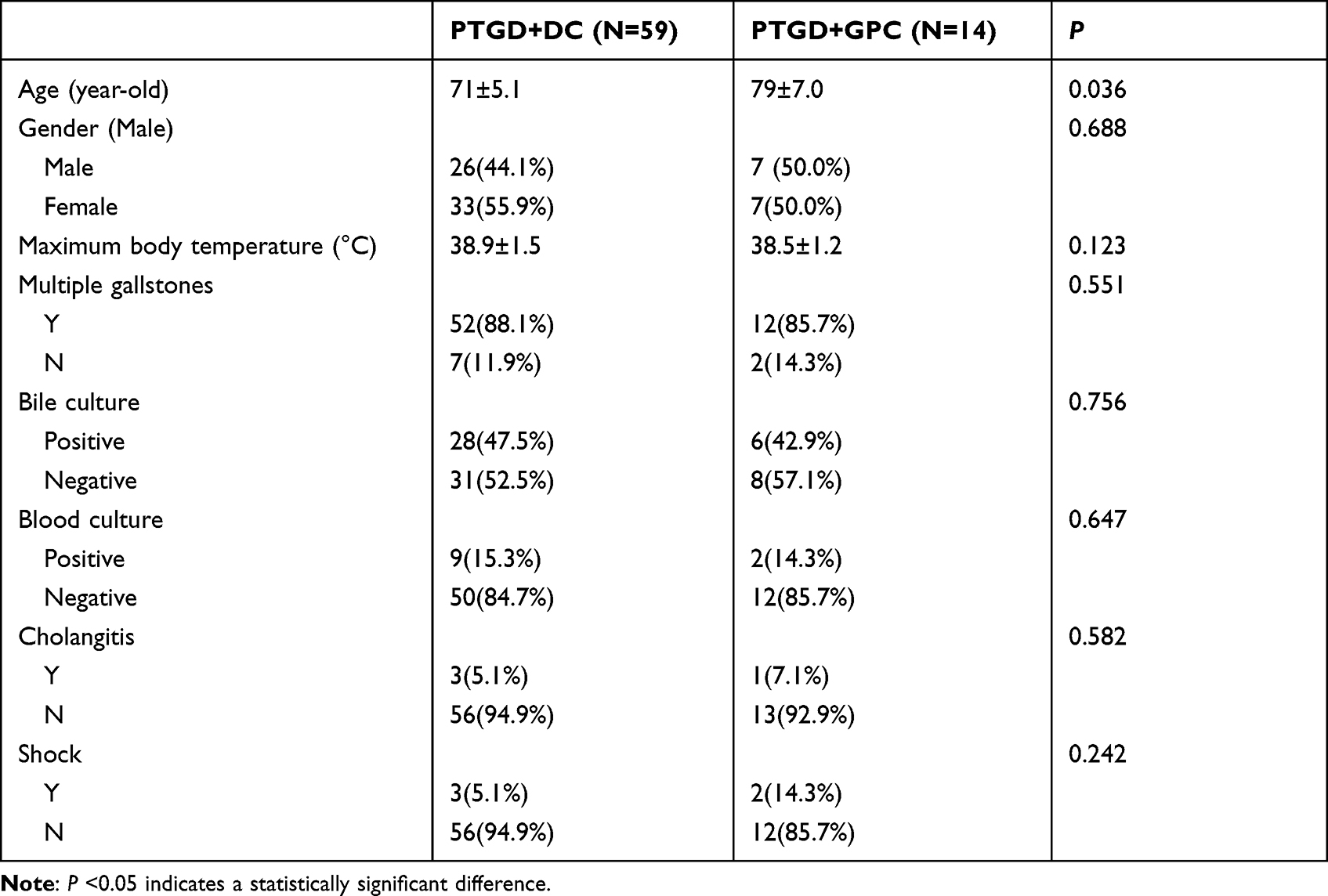 |
Table 1 Table of General Information on Patients |
Concomitant Diseases
Concomitant diseases included cerebrovascular accident, pulmonary infection, coronary heart disease, hypertension, diabetes, chronic obstructive pulmonary disease, chronic renal failure, atrial fibrillation, heart failure, and cirrhosis, as detailed in Table 2.
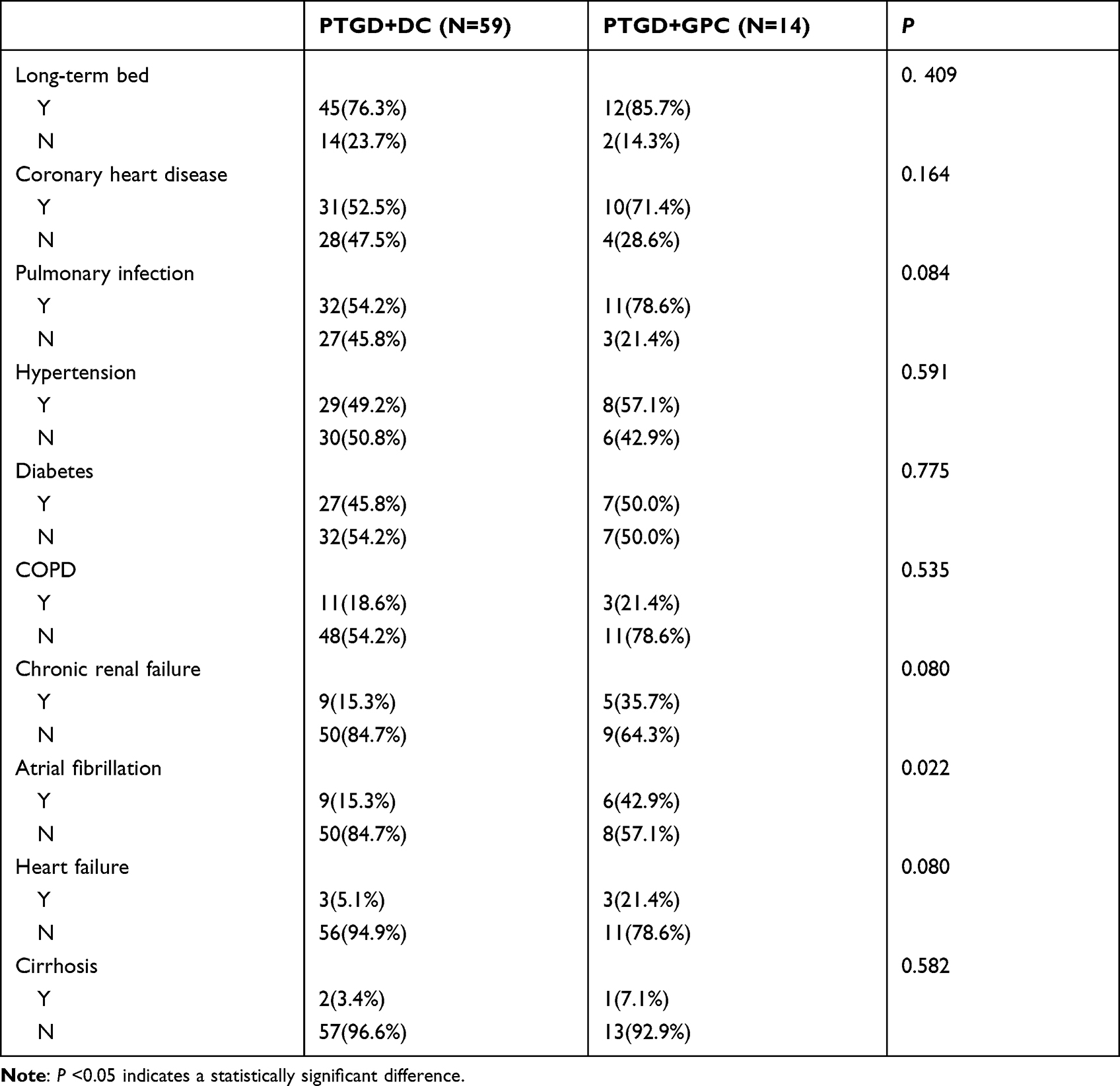 |
Table 2 Concomitant Diseases of Patients |
Surgical Indications and Contraindications
Surgical risk assessment was carried out according to the guidelines provided by the American Society of Anesthesiologists.11 Concomitant diseases that increased the risk of mortality in patients with acute calculous cholecystitis included long-term bedrest after cerebrovascular sequela, severe cardiovascular disease, advanced cirrhosis, pulmonary infection, chronic renal failure, and heart failure.
Preoperative Preparation
The laboratory examinations before PTGD included a white blood cell count, hemoglobin, aspartate transaminase, alanine aminotransferase, γ-glutamyl transpeptidase, total bilirubin, direct bilirubin, alkaline phosphatase, C-reactive protein, procalcitonin, and albumin counts. Blood gas analysis and coagulation function, and myocardial enzyme examinations were also performed, as detailed in Table 3. With regard to the imaging examinations, the findings of abdominal computed tomography, magnetic resonance cholangiopancreatography (MRCP), and abdominal ultrasound were as follows: Ultrasonic Murphy sign positive, incarcerated stones were present in the gallbladder neck, an enlarged gallbladder was observed, as well as a thickened gallbladder wall, and effusion presented around the gallbladder.
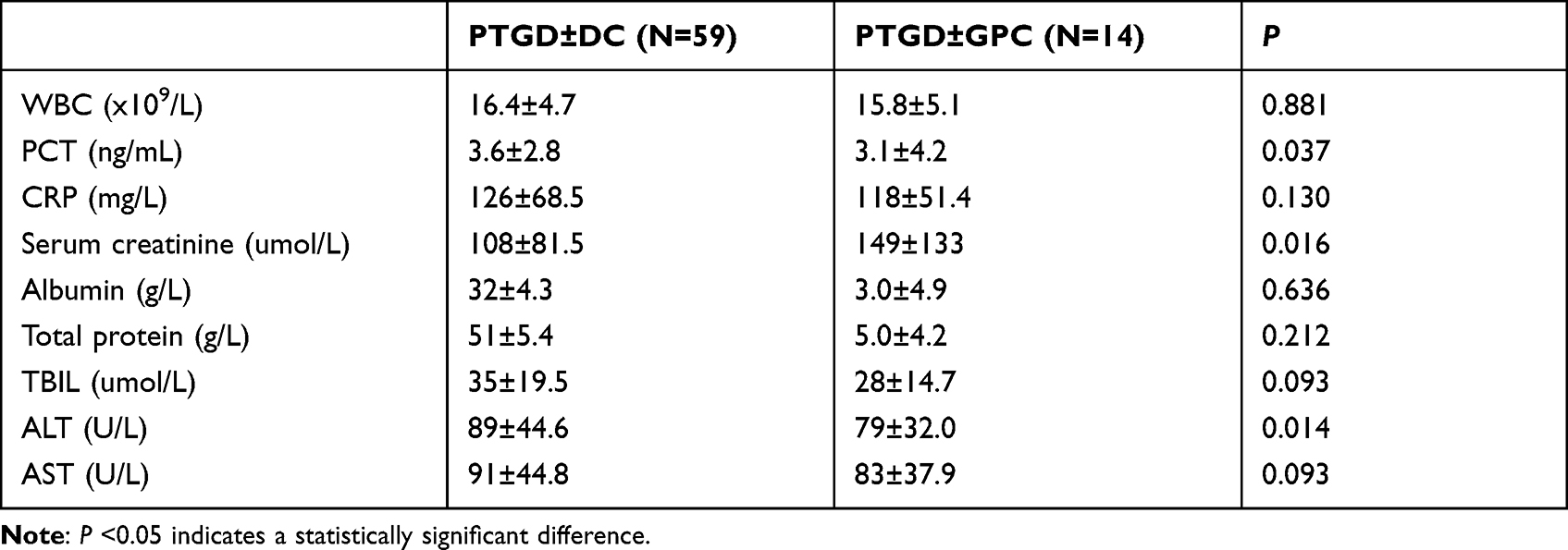 |
Table 3 Preoperative Data of Two Groups |
Indications of PTGD Surgery
The following were observed as indications for the need for PTGD surgery.
Indications of Gallbladder-Preserving Cholecystolithotomy
The following were observed as indications for conducting gallbladder-preserving cholecystolithotomy.
① Cholelithiasis;
② An inability to receive DC due to multiple serious systemic complications;
③ A life expectancy of more than 6 months.
Surgical Contraindications
The contraindication of PTGD surgery is a serious coagulation disorder, and the contraindications of gallbladder-preserving cholecystolithotomy include uncontrolled systemic infection or sepsis, uncorrected coagulopathy, a life expectancy of fewer than 6 months, or unstable vital signs.
Operation Methods and Materials
Percutaneous transhepatic gallbladder drainage and GPC can be performed under local anesthesia. The intravenous injection of midazolam hydrochloride and fentanyl citrate is required for sedation in a few patients in a state of agitation and delusion. None of the patients in this study were subjected to general anesthesia. The GPC required a percutaneous nephrolithotomy puncture kit (ultrasonic puncture needle, spring guide wire 0.89 mm x1, dilator 10 Fr x1, 12 Fr x1, 14 Fr x1, 18 Fr x1, 22 Fr x1, T-handle sheath 22 Fr, and a renal pelvis balloon catheter 22 Fr, Create Medic Co., Ltd.).
Percutaneous Transhepatic Gallbladder Drainage
The patient was placed in a supine position and received abdominal color ultrasonography. Appropriate puncture points were selected in the right hypochondriac region, and routine disinfection and draping were carried out. After successful local anesthesia with lidocaine, a single-use drainage tube (Bard NAVARRETM, Universal Drainage Catheter with Nitinol, 8 Fr. Bard Access Systems, Inc.) was inserted into the gallbladder cavity under ultrasonic guidance.
Precautions
The usual puncture route passes through the liver into the gallbladder, because the formation of a mature sinus tract takes shorter compared with transabdominal PTGD.12–14 One dose of antibiotics (third-generation cephalosporin or ciprofloxacin) was intravenously injected 30 minutes before the PTGD.
Gallbladder-Preserving Cholecystolithotomy
This procedure is often performed 6–8 weeks after transhepatic PTGD, whereas the surgery is generally carried out 8–12 weeks after transabdominal PTGD, ie, when the patient’s systemic infection symptoms have disappeared and a mature sinus tract has formed.
After disinfection and draping, local anesthesia was provided around the sinus tract, the original PTGD drainage tube was cut and removed, and a guidewire was placed into the gallbladder, as shown in Figure 1A. The sinus tract was dilated with a percutaneous nephrolithotomy puncture kit, using the trocar technique, until the placement of a 22 Fr. 17 cm sheath was possible, as shown in Figure 1B–D. An electronic choledochoscope was inserted into the gallbladder via the sinus tract (14 Fr., Olympus CHF-V), bile was extracted, and normal saline was infused through the choledochoscope to clearly display the gallbladder cavity and stones, as shown in Figure 1E and F. All the gallstones were removed with a stone basket under the choledochoscope, as shown in Figure 1G. The inside of the gallbladder cavity was checked repeatedly with the choledochoscope to confirm the absence of any residual stones or obstruction of the cystic duct, as shown in Figure 1H.
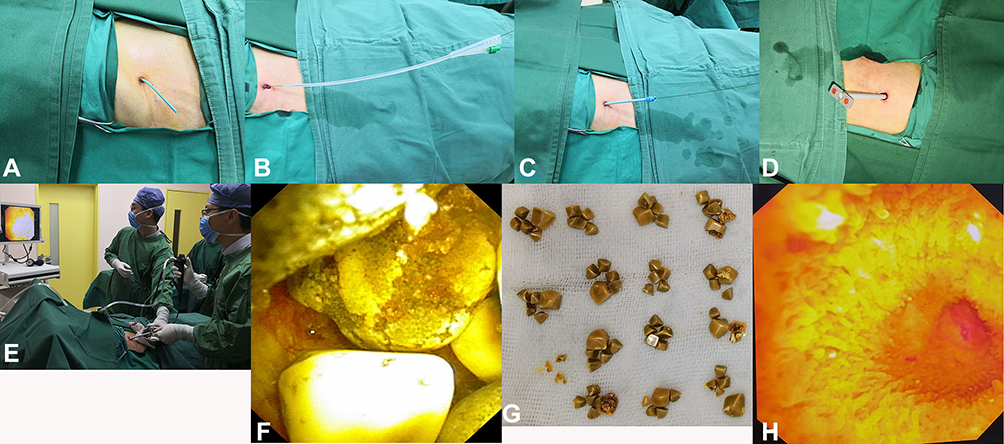 |
Figure 1 (A) Cut the PTGD drainage tube; (B) dilate the sinus tract with water balloon; (C) insert dilation sheaths into the puncture sinus tract one by one; (D) replace dilation sheaths one by one; (E) insert a choledochoscope into the gallbladder through the dilation sheath; (F) stones in the gallbladder; (G) removed gallstones; (H) unobstructed cystic duct and no residual stone in the gallbladder. |
Precautions
The electronic choledochoscope is placed into the gallbladder cavity through a 22 Fr sheath, and all the gallstones are removed one by one, with a stone basket placed under the choledochoscope. Cholecystography is performed during the surgery to confirm that there are no residual gallstones and the cystic and common bile ducts are unobstructed. A gallbladder drainage tube (18Fr) is indwelt and removed after one week of being clamped, provided the patient is suffering no discomfort, and the local area is subjected to compression bandaging. When large gallstones cannot be removed through the sheath, they are crushed by an intracorporeal laser lithotripter (Holmium laser machine, Versa pulse power suit 100W), and then removed. If there are stones in the common bile duct, endoscopic retrograde cholangiopancreatography (ERCP) and an endoscopic sphincterotomy (EST) may be performed for stone removal under a duodenoscope.
Technical Flow Charts
(1)The PTGD flow chart
Once the abdominal pain, fever, and any other symptoms of discomfort have stopped, typically within 2–3 weeks of the PTGD, the patient will undergo cholecystography. If the cystic duct and common bile duct are unobstructed, the drainage tube is clamped; then, the patient is discharged with follow-up observation. If the cholecystogram showed biliary tract obstruction, continuous drainage would be continued with the PTGD drainage tube, and, subsequently, the patient will be discharged with regular follow-up observation (Figure 2).
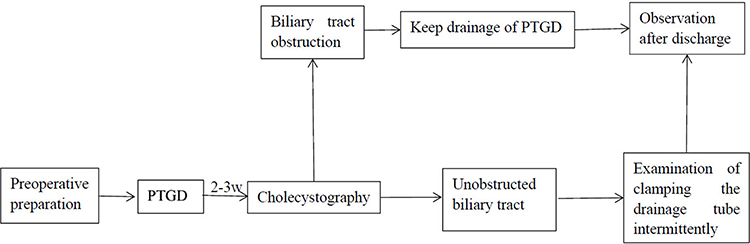 |
Figure 2 PTGD flow chart. |
(2)The GPC flow chart
① Preoperative examination and evaluation were carried out within 8–12 weeks of the PTGD. If the patient had no surgical contraindications, a cholecystectomy was performed. ② If the patient had surgical contraindications and there was an “unresectable gallbladder”, the sinus tract was dilated and a choledochoscopic cholecystolithotomy was performed under local anesthesia. ③After the cholecystolithotomy, a cholecystography was again performed. If the cystic duct was obstructed, a preoperative evaluation was carried out again after adjustment of the general condition. If the patient had no surgical contraindications, a cholecystectomy was performed; otherwise, the drainage tube was left in place, and the patient was discharged with follow-up observation. ④ After the cholecystolithotomy, a cholecystography was performed. If the cystic duct was unobstructed and there were no residual stones, the drainage tube was removed one week after being clamped, and the patient was discharged with follow-up observation. ⑤ If the cholecystograms showed choledocholithiasis, ERCP and EST were performed. After the cholecystography was repeated to confirm that there were no residual stones, the discharge tube was removed and the patient was discharged (Figure 3).
 |
Figure 3 Flow chart of gallbladder-preserving cholecystolithotomy. |
Postoperative Treatment
(1)In the case of PTGD, the drainage tubes were kept unobstructed as much as possible and flushed regularly. Cholecystography was performed 2–3 weeks after puncture and drainage. If there was no intraperitoneal leakage of the contrast agent and no stones in the common bile duct, and the cystic and common bile ducts were unobstructed, the PTGD drainage tube could be clamped. Provided they experienced no discomfort, the patient could go home and have regular follow-up visits. If the cystic duct was obstructed, the PTGD drainage tube was kept open.
(2)With respect to GPC, after each cholecystolithotomy, the drainage tube was routinely indwelt to drain bile from the gallbladder. Patients who were stable and had no abdominal pain or fever could go home and were asked to return to the clinic every 1–2 weeks for another cholecystolithotomy or re-examination. Finally, when the cholecystogram showed no residual gallstones, as well as unobstructed cystic and common bile ducts, the drainage tube was clamped for internal drainage. If there was no serious complaint of discomfort, the drainage tube was removed after one week (Figure 1). If the cholecystogram showed an obstructed cystic duct, the PTGD drainage tube was kept open.
(3)Once all the gallstones were removed, the patients were given ursodeoxycholic acid, po, 500 mg, qd x 6–12 months. The patient’s liver function was monitored every 3 months for adverse drug reactions, and abdominal ultrasonography was performed 1, 3, and 6 months after the removal of the drainage tube to check for recurrence of the cholelithiasis or cholecystitis.
Statistical Analysis
The continuous variables conforming to a normal distribution were expressed by mean ± standard deviation. The continuous variables that did not conform to a normal distribution were expressed by the median and a 95% confidence interval. Depending on the presence of a normal distribution, a t-test or non-parametric test was carried out to compare the continuous variables between the two groups. Categorical variables were expressed by frequency and incidence, and a chi-square test or Fisher’s exact test was used to compare the incidence. All statistical analyses were conducted using the SPSS Statistics (v.22; IBM, Corp, Armonk, NY) software.
Complications
In this study, a total of 74 high-risk patients with acute calculous cholecystitis underwent PTGD therapy, and 8 of them developed catheter-related complications (10.8%). Among them, 4 patients had catheter displacement (5.4%) and received a second PTGD treatment, 3 patients had intraoperative or postoperative bile leakage (4.1%), and 1 patient had bleeding of the gallbladder (1.4%).
A total of 14 PTGD patients underwent gallbladder-preserving cholecystolithotomy, and 2 of them experienced complications (14.3%). One patient developed cholangitis, another patient developed bleeding of the sinus tract. Both were managed conservatively.
Results
A total of 74 patients underwent PTGD therapy and 59 of these patients underwent laparoscopic cholecystectomy, 4 of whom had complications (6.8%). After the PTGD, all the patients’ abdominal pain and fever are relieved and none of them required emergency or immediate surgery. A total of 14 patients underwent GPC and routine cholecystography. The post GPC cholecystograms of 13 patients showed no residual stones in the gallbladder and common bile duct, the contrast agent entering the duodenum can be observed; accordingly, these patients were discharged after their drainage tubes were removed. One patient who had an obstructed cystic duct. After surgical evaluation, this patient was still at high risk with respect to a cholecystectomy so the gallbladder drainage tube was not removed. Abdominal ultrasonography, MRCP, and abdominal CT examinations were performed 1, 3, and 6 months after GPC to evaluate the recurrence of cholelithiasis and cholecystitis. During a mean follow-up period of 13 months, recurrent gallstones were found in 2 (15.4%) of the 13 patients after removal of the drainage tubes, and recurrent symptoms were found in 1 patient (7.7%). At present, none of the patients have been re-hospitalized and none required additional surgical treatment. One patient was not treated for gallstones after PTGD as their life expectancy was less than 6 months.
Discussion
Ultrasound-guided PTGD is considered the preferred therapy for high-risk patients with acute calculous cholecystitis. The treatment is very effective for relieving gallbladder obstructions and alleviating acute gallbladder infection, with a response rate of 98.6%–100%. The incidence and mortality associated with puncture and drainage were found to be 4.1% and 1.4%, respectively.15–17 However, as gallstones can still exist after PTGD, these patients are at risk of a recurrence of acute cholecystitis at any time. Patients that underwent PTGD only were reported to have a relapse rate of 46% after 3 years.18 Some studies also suggested that, without removal of the gallbladder after PTGD, the risk of an emergency visit or re-hospitalization related to gallstones was almost 50%.7 The preferred therapy for high-risk patients with acute calculous cholecystitis is PTGD followed by DC.17,19 This therapy not only avoids the complications resulting from the long-term presence of gallstones but also has obvious advantages over an emergency cholecystectomy in terms of lowering the difficulty of surgery, reducing postoperative complications and the rate of conversion to laparotomy, and shortening the postoperative length of stay and the operation time.8,17,20 It was reported that DC could be performed after PTGD in nearly two-thirds of high-risk patients with acute calculous cholecystitis, and the overall mortality was decreased to 2.7%, further indicating that this therapy was effective.15,17 This rate makes a striking contrast compared with the mortality in high-risk patients with acute calculous cholecystitis who directly undergo cholecystectomy (10–19%).3,7,17 In clinical practice, some high-risk patients with acute calculous cholecystitis suffer abdominal infection and poor general health after the drainage of PTGD, and they are still not allowed to receive DC; as such, they require long-term tube drainage. In this study, 74 high-risk patients with acute calculous cholecystitis underwent PTGD. Fifty-nine of these patients (79.7%) underwent DC but 15 patients (20.3%) were not allowed to have a cholecystectomy. Of this group, 13 patients were subjected to GPC under local anesthesia and then to the removal of the drainage tubes, and only 2 patients (2.7%) required long-term drainage tubes for bile drainage (One patient was treated with GPC, but needed a long-term indwelling drainage tube due to cystic duct obstruction.). Compared with a related paper15 reporting that two-thirds of PTGD patients required long-term tube drainage, this study found a significantly lower percentage, indicating that the treatment observed herein improved the patients’ quality of life to a large extent and reduced medical costs.
Akiyama et al and Kerlan et al first described the use of GPC for the treatment of gallstones in 1985, and Kellett et al made improvements to the procedure in 1988.21 In recent years, with the increasingly widespread use of GPC in China, the surgical method of removing stones while at the same time preserving the gallbladder has gained favor among Chinese patients.22 However, laparotomy has to be performed under general anesthesia and cannot be used for high-risk patients with severe cholelithiasis. The patients in this study were advanced in age (>75 years) and had coronary heart disease, chronic hemodialysis, and pulmonary infection, as well as other complications, such as requiring long-term bed rest after a cerebrovascular accident. Even though their condition was improved after PTGD, 15 patients (20.3%) were still unable to undergo cholecystectomy. Such high-risk gallstones are clinically known as “unresectable gallstones”. In general, these patients require long-term indwelling of gallbladder- puncture drainage tubes, which changes the patients’ quality of life to some extent and an increase in the possibility of catheter-related complications and readmission.15 In other words, the treatment of cholelithiasis and the removal of PTGD drainage tubes have been challenging in clinical practice. The innovation represented by the current study lies in how the sinus tract for the gallbladder puncture drainage tube is dilated under local anesthesia, after which all the gallstones are removed with a stone basket under the choledochoscope, without the need for general anesthesia or epidural anesthesia. Other advantages include that, since GPC is easy to perform, there is no need for it to be carried out in an operating theatre, and as it is less invasive to patients, they can directly return to the ward or go home for observation after completion of the cholelithotomy. During the 13-month follow-up period, recurrent cholelithiasis was found in 2 (15.4%) of the 13 patients after removal of the drainage tubes. Although this rate was significantly higher than the stone relapse rate (3.7–7.6%) reported elsewhere,21,22 this may have been due to the surgical indications in these existing studies, whereby only patients with a single gallstone or a few gallstones (<3), a gallbladder wall thickness of ≤4 mm, and contraction ≥30% were selected for GPC.22,23 In this study, to solve issues related to the drainage tube indwelling in high-risk patients with gallstones after PTGD the number of gallstones was not limited. In addition, some patients had abnormal gallbladder concentration and contraction functions resulting from past acute cholecystitis; as such, there was an increased postoperative gallstone relapse rate and no patients underwent further surgery. The literature22,23 reported that 94.9% of patients were asymptomatic after GPC, approximately 70% of patients with recurrent gallstones were also asymptomatic, and only a few patients had slight discomfort in the upper abdomen. Gallbladder-preserving cholecystolithotomy not only avoids the risks of general anesthesia but also preserves the gallbladder and avoids the common complications of performing a cholecystectomy, such as bile duct injury, and postcholecystectomy syndrome.24,25 Of course, our research observation time and quantity are limited, and we still need a lot of data and multi center research.
Conclusion
Percutaneous transhepatic gallbladder recurrent gallbladders r drainage, combined with GPC, is suitable for high-risk patients with severe acute calculous cholecystitis who cannot undergo DC. The surgery is relatively simple, can be performed under local anesthesia, and is characterized by a high degree of safety and only a few surgical contraindications. This method not only enables high-risk patients with acute calculous cholecystitis to manage the high-risk inflammation phase before the removal of the gallstones but also solves the problem of long-term tube drainage after PTGD. As this study was a single-center study, the number of cases was limited, and the follow-up time was short. Accordingly, more clinical data are required to support its findings. However, it would appear that, to some extent, this combination method offers an alternative to the treatment of unresectable gallstones.
Abbreviations
PTGD, percutaneous transhepatic gallbladder drainage; GPC, gallbladder-preservation cholecystolithotomy; DC, delayed cholecystectomy; CCDE, cholecystostomy catheter draining externally; COPD, chronic obstructive pulmonary disease; CRF, chronic renal failure; AF, Atrial fibrillation; HF, heart failure; WBC, white blood cell; PCT, procalcitonin; CRP, C-reactive protein; Cr, serum creatinine; ALB, albumin; TBIL, total bilirubin; ALT, alanine transaminase; GOT, Glutamic-oxal(o)acetic transaminase; TP, Total protein; CT, computed tomography; MRCP, magnetic resonance cholangio pancreatography; UDCA, ursodeoxycholic acid; ERCP, endoscopic retrograde cholangio-pancreatography; EST, endoscopic sphincterotomy; SPSS, statistical package for the social sciences.
Ethics Approval and Consent to Participate
I confirm that I have read the Editorial Policy pages. This study was conducted with approval from the Ethics Committee of Beijing Rehabilitation Hospital of Capital Medical University (2018bkkyLW005). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
This study was funded by Beijing Rehabilitation Hospital Affiliated to Capital Medical University (2019R-001; 2020-038). The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yamashita Y, Takada T, Kawarada Y, et al. Surgical treatment of patients with acute cholecystitis: Tokyo guidelines. J Hepatobiliary Pancreat Surg. 2007;14:91–97. doi:10.1007/s00534-006-1161-x
2. Ansaloni L, Pisano M, Coccolini F. 2016 WSES guidelines on acute calculous cholecystitis. World J Emerg Surg. 2016;11:25. doi:10.1186/s13017-016-0082-5
3. Huber DF, Martin EW, Cooperman M. Cholecystectomy in elderly patients. Am J Surg. 1983;146:719–722. doi:10.1016/0002-9610(83)90326-4
4. Lin D, Wu S, Fan Y, et al. Comparison of laparoscopic cholecystectomy and delayed laparoscopic cholecystectomy in aged acute calculous cholecystitis: a cohort study. Surg Endosc. 2020;34:2994–3001. doi:10.1007/s00464-019-07091-4
5. Patel N, Chick JFB, Gemmete JJ, et al. Interventional radiology-operated cholecystoscopy for the management of symptomatic cholelithiasis: approach, technical success, safety, and clinical outcomes. Am J Roentgenol. 2018;210:1164–1171. doi:10.2214/AJR.17.18690
6. Cherng N, Witkowski ET, Sneider EB, et al. Use of cholecystostomy tubes in the management of patients with primary diagnosis of acute cholecystitis. J Am Coll Surg. 2012;214:196–201. doi:10.1016/j.jamcollsurg.2011.11.005
7. Winbladh A, Gullstrand P, Svanvik J, Sandström P. Systematic review of cholecystostomy as a treatment option in acute cholecystitis. HPB. 2009;11:183–193. doi:10.1111/j.1477-2574.2009.00052.x
8. Han J, Xue D, Tuo H, et al. Percutaneous transhepatic gallbladder drainage combined with laparoscopic cholecystectomy versus emergency laparoscopic cholecystectomy for the treatment of moderate acute cholecystitis: a meta-analysis. J Laparoendoscop Adv Surg Techniq. 2021. doi:10.1089/lap.2021.0579
9. Stirrat J, Patel NR, Stella SF, et al. Safety and efficacy of percutaneous gallstone extraction in high-risk patients: an alternative to cholecystectomy or long-term drainage. J Am Coll Surg. 2021;232(2):195–201. doi:10.1016/j.jamcollsurg.2020.09.019
10. Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25:41–54. doi:10.1002/jhbp.515
11. Apfelbaum JL, Connis RT, Nickinovich DG, Nickinovich DG; Committee on Standards and Practice Parameters; American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice advisory for pre-anesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on preanesthesia evaluation. Anesthesiology. 2012;116:522–538. doi:10.1097/ALN.0b013e31823c1067
12. Kim SK, Mani NB, Darcy MD, et al. Percutaneous cholecystolithotomy using cholecystoscopy. Tech Vasc Interventional Rad. 2019;22:139–148. doi:10.1053/j.tvir.2019.04.006
13. Nemcek AA, Bernstein JE, Vogelzang RL. Percutaneous cholecystostomy: does transhepatic puncture preclude a transperitoneal catheter route? JVIR. 1991;2:543–547. doi:10.1016/S1051-0443(91)72239-2
14. Hatjidakis AA, Karampekios S, Prassopoulos P, et al. Maturation of the tract after percutaneous cholecystostomy with regard to the access route. Cardiovasc Intervent Radiol. 1998;21:36–40. doi:10.1007/s002709900208
15. Bala M, Mizrahi I, Mazeh H, et al. Percutaneous cholecystostomy is safe and effective option for acute calculous cholecystitis in select group of high‑risk patients. Eur J Trauma Emerg Surg. 2016;42:761–766. doi:10.1007/s00068-015-0601-1
16. Li M, Li N, Ji W, et al. Percutaneous cholecystostomy is a definitive treatment for acute cholecystitis in elderly high-risk patients. Am Surg. 2013;79:524–527. doi:10.1177/000313481307900529
17. Bao J, Wang J, Shang H, et al. The choice of operation timing of laparoscopic cholecystectomy (LC) after percutaneous transhepatic gallbladder drainage (PTGBD) for acute cholecystitis: a retrospective clinical analysis. Ann Palliat Med. 2021;10(8):9096–9104. doi:10.21037/apm-21-1906
18. Ha JP, Tsui KK, Tang CN, Siu WT, Fung KH, Li MK. Cholecystectomy or not after percutaneous cholecystostomy for acute calculous cholecystitis in high-risk patients. Hepatogastroenterology. 2008;55:1497–1502.
19. Hung YL, Chong SW, Cheng CT, et al. Natural course of acute cholecystitis in patients treated with percutaneous transhepatic gallbladder drainage without elective cholecystectomy. J Gastrointest Surg. 2020;24:772–779. doi:10.1007/s11605-019-04213-0
20. Tan HY, Jiang DD, Li J, He K, Yang K. Percutaneous transhepatic gallbladder drainage combined with laparoscopic cholecystectomy: a meta-analysis of randomized controlled trials. J Laparoendosc Adv Surg Tech A. 2018;28:248–255. doi:10.1089/lap.2017.0514
21. Kellett MJ, Wickham JE, Russell RC. Percutaneous cholecystolithotomy. Br Med J. 1988;296:453e455. doi:10.1136/bmj.296.6620.453
22. Li B, Lin Y, Nie B, et al. Systematic review and pathway enrichment analysis of Chinese medicine in preventing recurrence and improving prognosis of cholelithiasis after gallbladder-preserving lithotripsy. Ann Palliat Med. 2021. doi:10.21037/apm-20-1135
23. Qu Q, Chen W, Liu X, et al. Role of gallbladder-preserving surgery in the treatment of gallstone diseases in young and middle-aged patients in China: results of a 10-year prospective study. Surgery. 2020;167:283–289. doi:10.1016/j.surg.2019.09.001
24. Thurley PD, Dhingsa R. Laparoscopic cholecystectomy: postoperative imaging.AJR. Am J Roentgenol. 2008;191:794e801. doi:10.2214/AJR.07.3485
25. Goldacre MJ, Wotton CJ, Abisgold J, Yeates DG, Collins J. Association between cholecystectomy and intestinal cancer: a national record linkage study. Ann Surg. 2012;256:1068e1072. doi:10.1097/SLA.0b013e3182759efb
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.