Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Efficacy of Internet-Based Interventions in Family-Centered Empowerment Among Children with Chronic Diseases: A Mixed-Methods Systematic Review
Authors Mulyana AM ![]() , Rakhmawati W
, Rakhmawati W ![]() , Wartakusumah R, Fitri SYR
, Wartakusumah R, Fitri SYR ![]() , Juniarti N
, Juniarti N ![]()
Received 13 September 2023
Accepted for publication 3 November 2023
Published 9 November 2023 Volume 2023:16 Pages 3415—3433
DOI https://doi.org/10.2147/JMDH.S440082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aep Maulid Mulyana,1,* Windy Rakhmawati,2,* Riki Wartakusumah,3,* Siti Yuyun Rahayu Fitri,2,* Neti Juniarti4,*
1Nursing Internship Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 2Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 3Departement of Nursing Science, Faculty of Medicine Public Health and Nursing, Universitas Gadjah Mada, Sleman, Yogyakarta, 55284, Indonesia; 4Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia
*These authors contributed equally to this work
Correspondence: Windy Rakhmawati, Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia, Tel +62 821-1949-2124, Email [email protected]
Background: The incidence of chronic diseases in children is increasing worldwide, which can disrupt the quality of life. Family empowerment (FE) is one approach to strengthen family care among children with chronic diseases. In addition, internet has the potential in healthcare service interventions for families.
Purpose: This study aimed to determine the efficacy of internet-based family empowerment interventions among children with chronic diseases.
Methods: The study used a mixed-methods systematic review. A literature review was conducted following PRISMA guidelines using the PubMed, Scopus, ScienceDirect, and CINAHL databases. We used the PCC framework: chronic diseases (Population), family empowerment (Concept), and internet-based intervention (Context). Studies were eligible if published between 2013 and 2023, full-text, original study design, and focused on family empowerment in children with chronic diseases. Studies would be excluded if they were not in English or if the population was adults. The quality of the studies was assessed using the Mixed Methods Appraisal Tool (MMAT) version 2018. The study analysis used Sequential Explanatory Synthesis, which is a quantitative study (QUAN) synthesis followed by a qualitative study (QUAL) synthesis, then integrated using the QUAL data transformation technique.
Results: We highlight the quantitative study findings that an internet-based family empowerment intervention positively impacted family members’ ability to care for children with chronic diseases with a mean Family Empowerment Scale (FES) total score of 4.13. We analyzed six study and identified four themes regarding efficacy of internet-based interventions in empowering families with children with chronic diseases: knowledge; availability of resources and time-saving; connectedness and communication; and family management and self-confidence.
Conclusion: Our study highlights that online-based interventions in family empowerment positively impact enhancing all domains of empowerment. This findings suggest that internet-based family interventions need to be adopted to fulfill the care needs of children with chronic diseases sustainably.
Keywords: children, efficacy, family empowerment, internet, online, chronic disease
Introduction
The incidence of chronic diseases is increasing in several developed and developing countries, while the prevalence of chronic diseases in children remains sporadic. Data from the United Nations Children’s Fund (UNICEF) in 2020 indicates that approximately 1.2 million adolescents and children under 20 die yearly due to chronic diseases, contributing to 13% of the total deaths from chronic diseases globally.1 In the child population in the United States, it is estimated that 1% to 3% experience hypertension, and one in five children suffers from obesity. The incidence of type 2 diabetes in those under 20 has quadrupled, from 22,820 cases in 2010 to 84,131 cases in 2050.2 The World Health Organization (WHO) through the International Agency for Research on Cancer (IARC) estimates that 8677 Indonesian children aged 0–14 years had cancer in 2020, making it the highest number compared to other countries in Southeast Asia.3 An estimated 400,000 children aged 0–19 years develop cancer each year, including leukemia, brain cancer, lymphoma and solid tumors.4
Children with chronic diseases are at a higher risk of experiencing a diminished quality of life.5 Consistent with Megari’s research (2013), individuals living with chronic diseases can have a negative impact on their quality of life, leading to deteriorating health, delayed development, prolonged illness duration, the need for intensive medical care, and limitations in capabilities, functionality, and productivity.6
The role of the family is crucial in helping to address the issues that arise in children with chronic diseases.7 Implementing a family-centered approach in the care of children with chronic diseases enhances family involvement and full participation in caregiving, decision-making, and improving the child’s quality of life.8 Additionally, nurses play a vital role in assisting parents in addressing the challenges that arise in children with chronic diseases.9,10
The Family-Centered Empowerment Model (FCEM) is one of approaches to strengthen family health.8,11 FCEM provides opportunities for families to engage in comprehensive child care.12 The Family-Centered Empowerment Model can help improve patients’ quality of life of methamphetamine users and their families.13 Consistent with the findings of Minooei et al (2016), it shows that Family-Centered Empowerment (FCE) interventions can assist parents in identifying needs, enhancing engagement, self-confidence, and the quality of life of children with chronic kidney failure.14
Internet has the potential in healthcare service interventions. A Systematic Review and Meta-analysis study show statistically significant improvements in the quality of life after Nurse-led Telehealth Intervention among adults with chronic diseases.15 Another study indicates that telehealth technologies have proven effective in improving self-care skills, self-monitoring, and enhancing clinical outcomes among older adults with chronic diseases.16 However, based on the author’s research, a similar study has yet to identify telehealth use in Family Empowerment (FE) within the pediatric population with chronic diseases.
Previous study findings show that internet use has several benefits in child care, including increased knowledge, convenience, self-management, quality of life, scheduled visits, care coordination, privacy, cost efficiency, comfort, independence, and reduced hospitalizations and health visits.17–20 In contrast, other studies state that it is easier for families to communicate with medical service providers during face-to-face meetings compared to telehealth in relationships with health professionals. Challenges in the use of telehealth include a lack of face-to-face interaction, concerns about compromised confidentiality, and the potential for misdiagnosis. In line with other studies, there is no significant difference in the knowledge scores of families who use the internet in the health care of children with special care needs, undergoing chemotherapy, and care during the COVID-19 pandemic.20–23 Based on the results of a 1945 study of parents who use the internet, only half reported being able to distinguish the quality of online resources or feeling confident using online information to make health decisions.23
There is a research gap in that previous studies have only focused on quantitative or qualitative analysis related to understanding the impact of internet-based interventions on family empowerment for children with chronic diseases. Conclusive information regarding the benefits and impact of using telehealth in FE for children with chronic disease is essential. Therefore, it is important to conduct a review study of previous studies using a comprehensive approach involving a combined review of quantitative and qualitative studies to gain broad and deep insights into understanding the impact of internet-based FCE interventions on families facing multiple pediatric chronic conditions. This study aims to conduct a mixed-method systematic review to determine the efficacy of internet-based family empowerment interventions among children with chronic diseases.
Materials and Methods
Study Design
This study uses a mixed-methods systematic review that follows the framework by Pluye & Hong (2014) and Pace et al (2012).24,25 This method is suitable for the subject of this study to explore comprehensive identification and integration of quantitative and qualitative research methodologies with complex data synthesis that allows for an in-depth understanding of a topic. The framework consists of seven stages: formulating review questions, establishing eligibility criteria, applying study search strategies, identifying studies, determining relevant studies, assessing study quality, and synthesizing studies.25
Review Question and Eligibility Criteria
The review question developed in this study is “how efficacy of the internet-based intervention in family empowerment among children with chronic diseases?”. The inclusion criteria in this study were based on the PCC question framework. Population: children with chronic disease; Concept: family empowerment; and Context: internet-based intervention. A study was eligible for inclusion including articles published from 2013 to 2023, full-text, original study design, and topic of family empowerment focusing on children with chronic diseases. Studies were excluded if they were not in English and adult population. All researchers independently conducted studies included screening articles, appraising study quality, analyzing studies, and reporting results.
Search Strategy
The search strategy for this study followed the PRISMA guideline.26–28 A literature review was conducted using PubMed, Scopus, ScienceDirect, and CINAHL databases. The keyword adjusts the medical subject heading (MeSH) term using a boolean, including (“family empowerment” OR “parent empowerment” OR “family-centred empowerment” OR “family empowering” OR “parent empowering”) AND (“children” OR “adolescents” OR “child” OR “teenager” OR “kids” OR “pediatric”) AND (“chronic disease” OR “chronic illness” OR “long term conditions” OR “chronic conditions”) AND (“internet” OR “online” OR “web” OR “technology” OR “virtual” OR “digital” OR “telehealth” OR “telenursing”).
Critical Appraisal
Study quality was assessed using the Mixed Methods Appraisal Tool (MMAT) version 2018 from Hong et al (2018).29 We assessed articles independently conducted by two authors. The evaluation for study quality was consistent with five questions and four categories for response options across all study designs, including “yes”, “no”, and “cannot tell”. Scoring is done by providing a presentation for each question for each study design, with a range of 0–100%. Appraisal of studies based on MMAT criteria and tools for inclusion of study categories, namely quantitative non-randomized studies, quantitative randomized controlled trials, mixed methods studies, qualitative studies. After the assessment is carried out independently by each author, then the authors combine and recheck together to get the final results of the study appraisal. We did not exclude studies with low methodological quality to find a broad range of results and minimize study bias.
Data Extraction
Data extraction in this study was conducted using the tabulation method in Microsoft Excel (Microsoft Corp., New York, USA). Data extraction summaries were done separately and divided into two groups: qualitative studies and quantitative studies, with each group presented in three subgroups of identification results, including study characteristic tables, intervention model and outcomes tables, and summary of findings tables. The items identified in the three subgroups of analysis included the study characteristic table comprising the study year, study design, location, setting, population, age, sample, parents’ education, parents’ occupation, model, and intervention; the intervention model and outcomes table including the study year, intervention model, length of study, follow-up, intervention duration, instrument of FE, process/procedure of intervention, measurement, and outcome; and the summary of findings table comprising the study year, intervention model, aims of study, and results.
Synthesis
Sequential Explanatory Synthesis consists of two phases: the synthesis of quantitative studies (QUAN) to provide initial information, followed by the synthesis of qualitative studies (QUAL) to confirm and support the findings of the QUAN synthesis. Firstly, the synthesis of QUAN study results and mixed methods collected in tables is conducted. Secondly, the findings of QUAL studies and mixed methods are integrated. Then, the interpretation of the results of both stages is carried out to reveal the findings. Convergent synthesis is used in this study, and the study’s results are integrated using the data transformation technique of QUAL.25
Results
Description of Study Selection
The study’s findings obtained 2280 articles from the four databases used, including PubMed, Scopus, ScienceDirect, and CINAHL. After removing duplicates from the collected articles and title screening, 61 articles remained. Then, selection based on title, full-text, topic, and language, there were 17 articles remaining. Therefore, after screening based on inclusion criteria, six articles were eligible for inclusion in this study (Figure 1). Then, the quality assessment of the included studies was analyzed using the Mixed Methods Appraisal Tool (MMAT) version 2018 (Table 1).
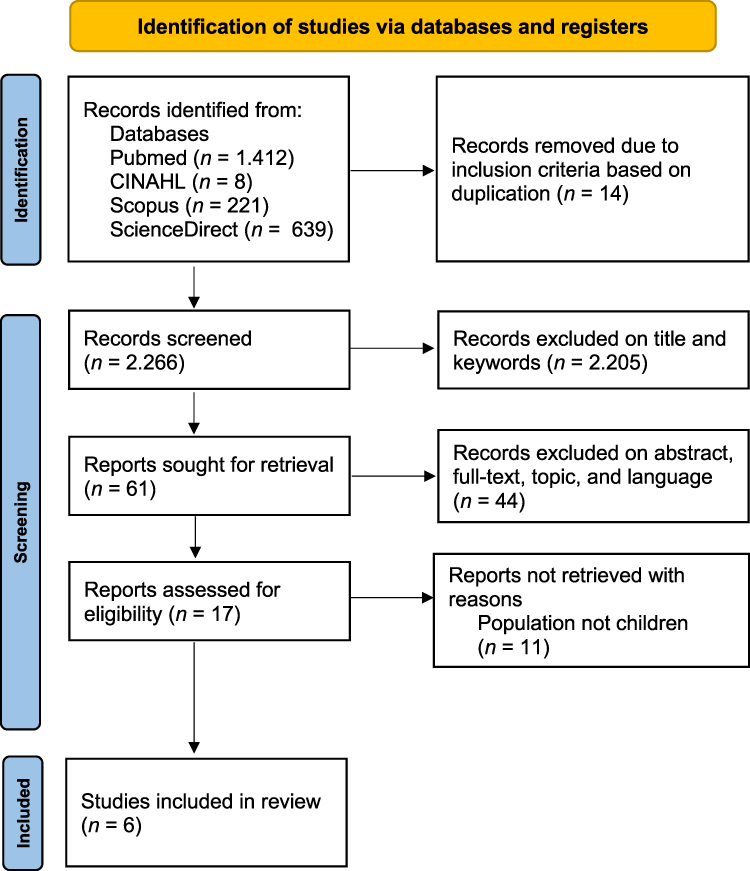 |
Figure 1 PRISMA Flow diagram. Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated :guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons. |
 |
Table 1 Quality Assessment of Included Studies Using the Mixed Methods Appraisal Tool (MMAT) Version 2018 |
Quantitative Study
Characteristics of Study
Four studies were analyzed, including study year, design, location, setting, population, age, sample, parents’ education, occupation, and intervention model (Table 2 and 3). The included studies comprised quantitative studies and mixed-methods (4 studies), including quantitative non-randomized studies (n=2), quantitative randomized controlled trials (n=1), and mixed-methods (n=1). The studies were conducted in the United Kingdom (n=2), Japan (n=1), and Italy (n=1) and were conducted in hospitals (n=1) and homes (n=3).
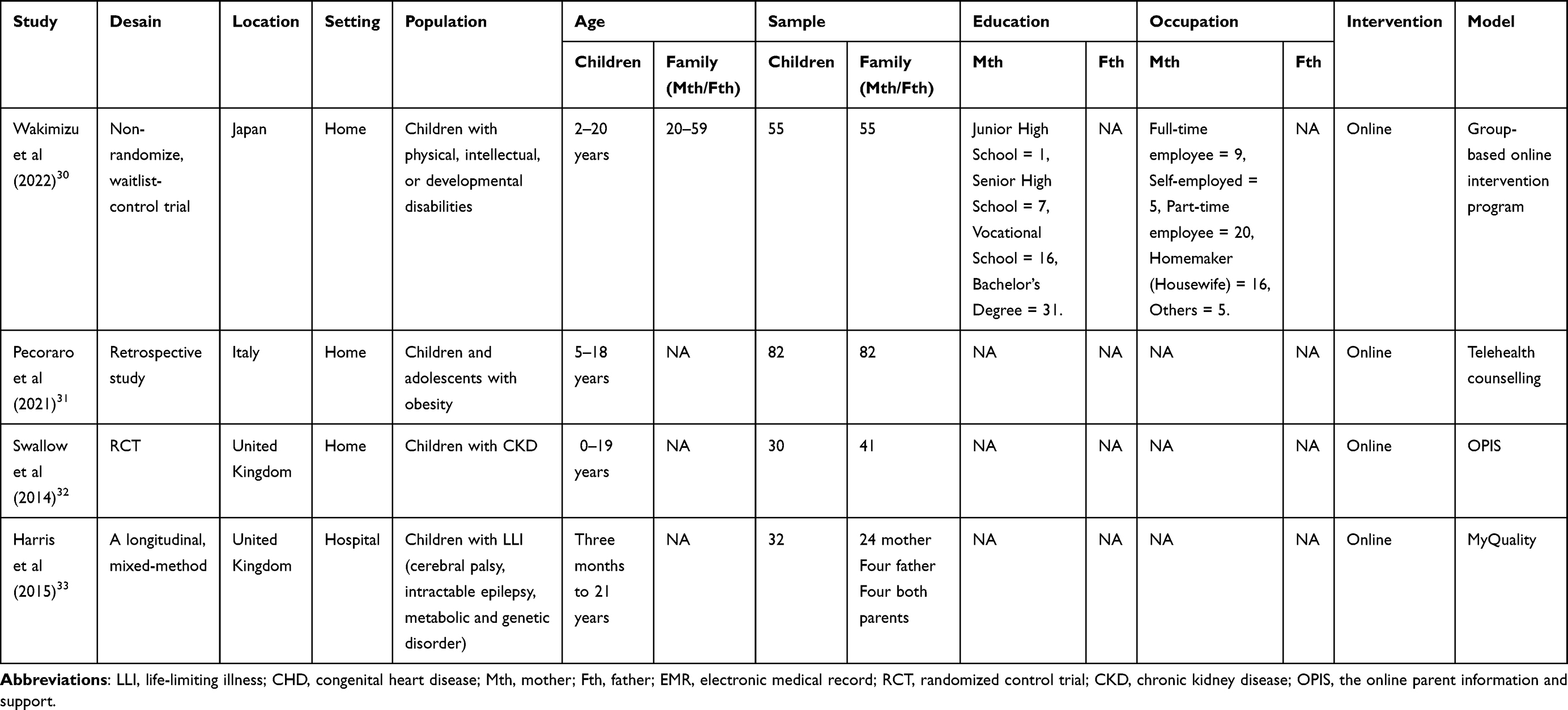 |
Table 2 Characteristics of Quantitative Studies and Mixed-Method Study (n = 4) |
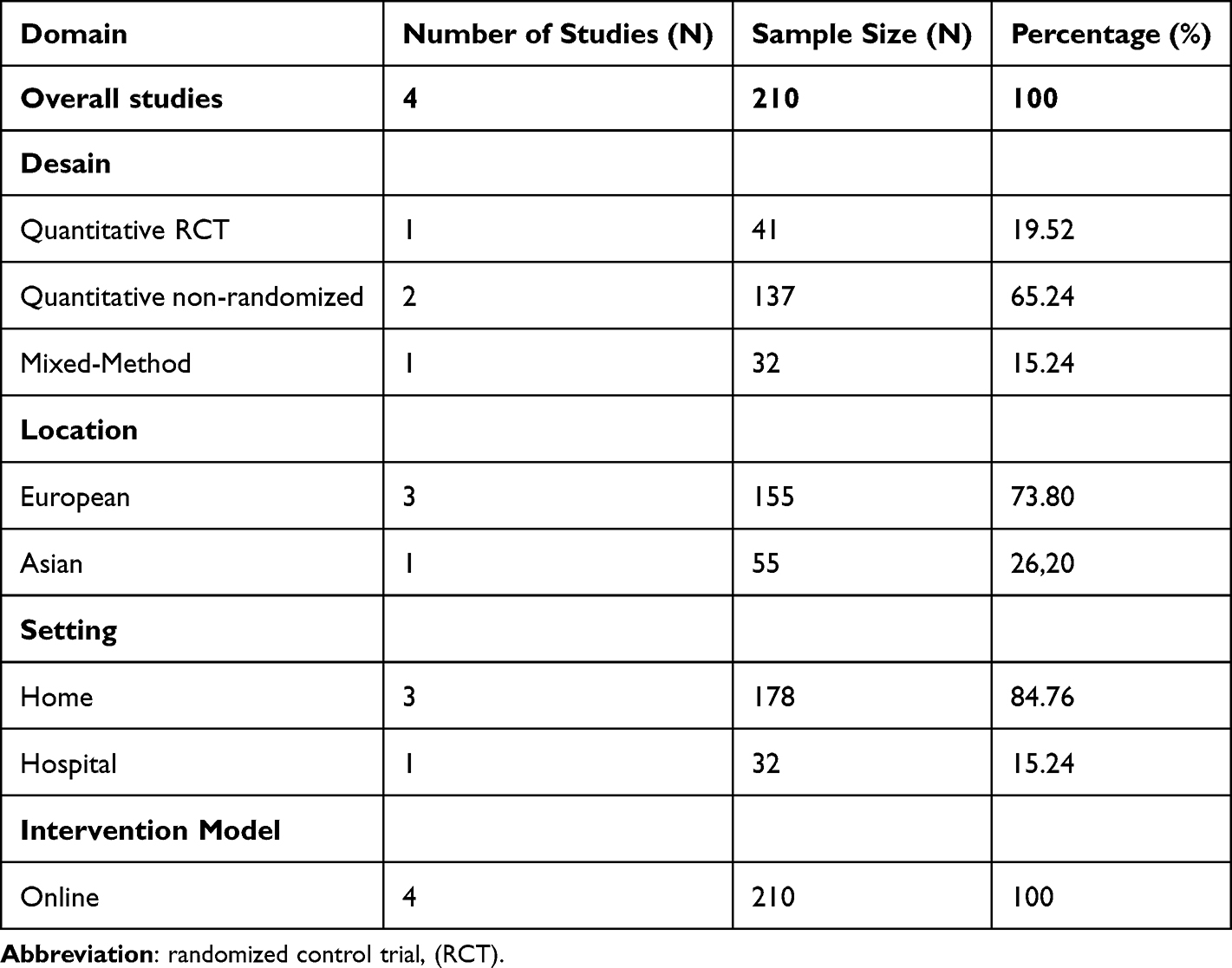 |
Table 3 Summary of Findings of Quantitative Studies and Mixed-Method Study (n = 4) |
The total sample of this study consisted of 199 children and 210 parents, with the population in this study including children aged 0–21 years with obesity (n=1), physical, intellectual, or developmental disabilities (n=1), chronic kidney disease (CKD) (n=1), and life-limiting illness (LLI) (such us cerebral palsy, intractable epilepsy, metabolic and genetic disorders) (n=1). Only one study provided information about the parents’ age, occupation, and highest education level,30 with the majority of parents aged 20–59 years, most having vocational and bachelor’s degrees (47 individuals), 20 working part-time, and 16 being homemakers. Overall, the majority were non-randomized 65.24%, carried out in Europe 73.80%, interventions implemented at home 84.76%, and 100% online-based intervention models.
Internet-Based Intervention of Family Empowerment Model
Four studies were analyzed, and we found that the intervention models used were telehealth counselling, Online Parenting Information and Support (OPIS), MyQuality, and a group-based online intervention program. After families received the intervention, follow-up was conducted using the FES with varying durations in each study, ranging from 3 weeks to 3 months (Table 4). The intervention procedures were primarily administered to families, especially parents, and allowed for the involvement of children with varying durations. Here are the four internet-based family empowerment models identified:
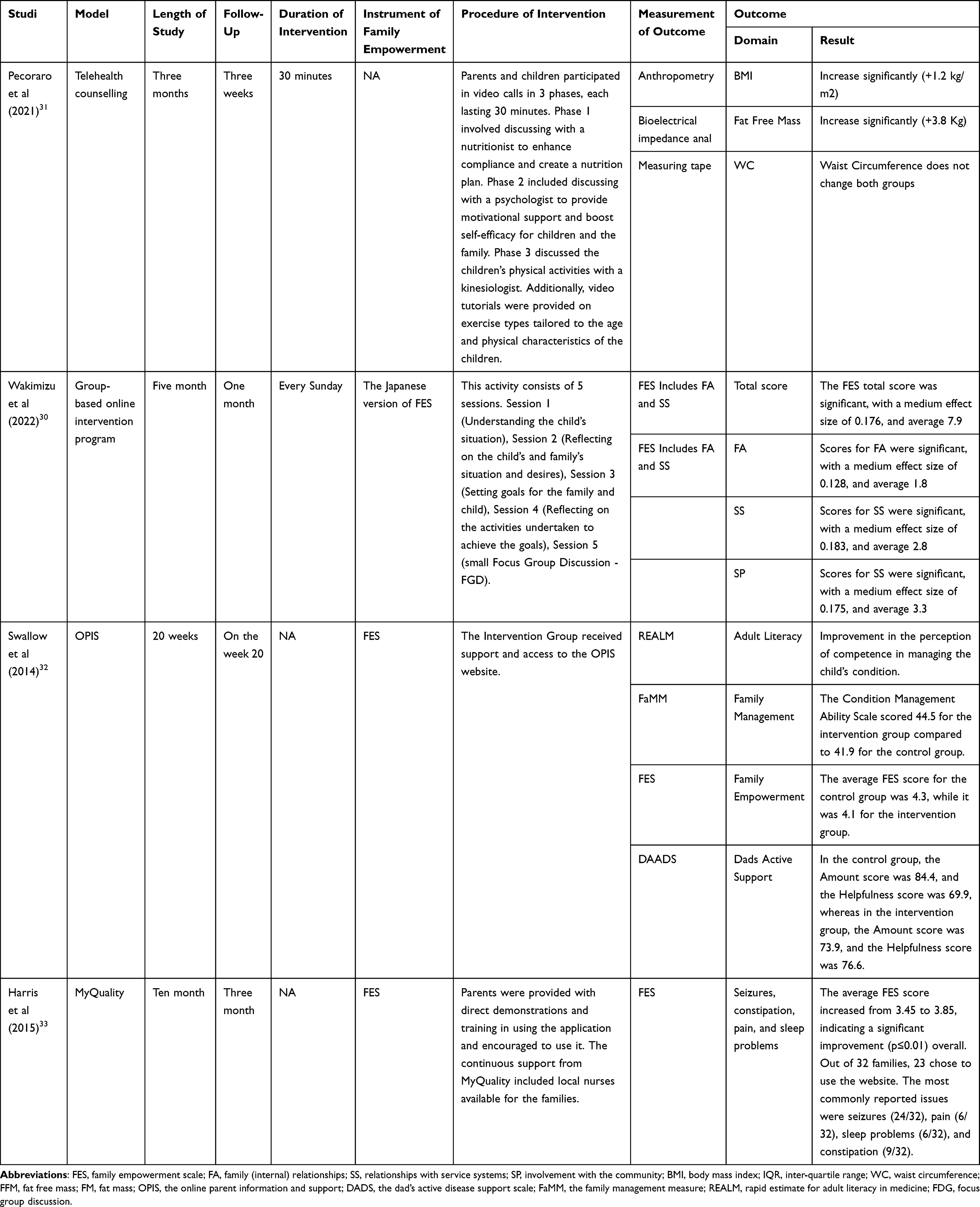 |
Table 4 Intervention Model and Outcomes of Quantitative Studies and Mixed-Method Study (n = 4) |
Model 1: Parents and children participated in video calls in three phases, each lasting 30 minutes. Phase 1 involved discussions with a nutritionist to improve compliance and create a nutrition plan. Phase 2 included discussions with a psychologist to provide motivational support and restore the children’s and the family’s self-efficacy. In Phase 3, discussions were held with a kinesiologist regarding the children’s physical activities. Additionally, video tutorials were provided on exercise types tailored to the age and physical characteristics of the children.
Model 2: This activity consists of 5 sessions. First, understanding the child’s situation. Second, reflecting on the child and family’s situation and desires. Third, setting goals for the family and child. Fourth, reflecting on the activities carried out to achieve the goals. Lastly, a small focus group discussion (FGD).
Model 3: The Intervention Group received support and access to the OPIS website.
Model 4: Parents were provided with hands-on demonstrations and training in using the application and invited to use it. Ongoing MyQuality support provided local nurses for the families.
Outcomes
Four quantitative studies revealed that after online interventions were conducted to empower families with children with chronic diseases, there was a significant improvement in FES (Family Empowerment Scale) and clinical outcomes for the children.30–33 First, after receiving telehealth counselling in FE, there was a significant increase in the child’s BMI (Body Mass Index), Fat-Free Mass, and Waist Circumference (p < 0.000). Second, a group-based online intervention program significantly impacted the total FES score, particularly showing a significant improvement in the Family Advocacy (FA) subdomain and the relationship with Social Support (SS). Families experienced lower caregiving burdens and higher self-confidence. Third, the results of using the OPIS (Online Parenting Information and Support) system showed a significant FES score of 4.3 on average, and parents experienced an increase in their perception of competence and confidence in managing their child’s condition, thus understanding and mitigating the impact of their child’s condition. Fourth, MyQuality showed a positive effect on family empowerment. The average FES score increased from 3.45 to 3.85, indicating a significant improvement (p ≤ 0.01) overall (Table 4).
We highlight the quantitative study findings that an internet-based family empowerment intervention positively impacted family members’ ability to care for children with chronic diseases with a mean Family Empowerment Scale (FES) total score of 4.13. This includes improvements in their skills and competencies, self-management, self-confidence, interactions with healthcare professionals, and the overall empowerment domain scores. Thus, it can aid in improving clinical outcomes for children with chronic diseases (Table 4 and 5).
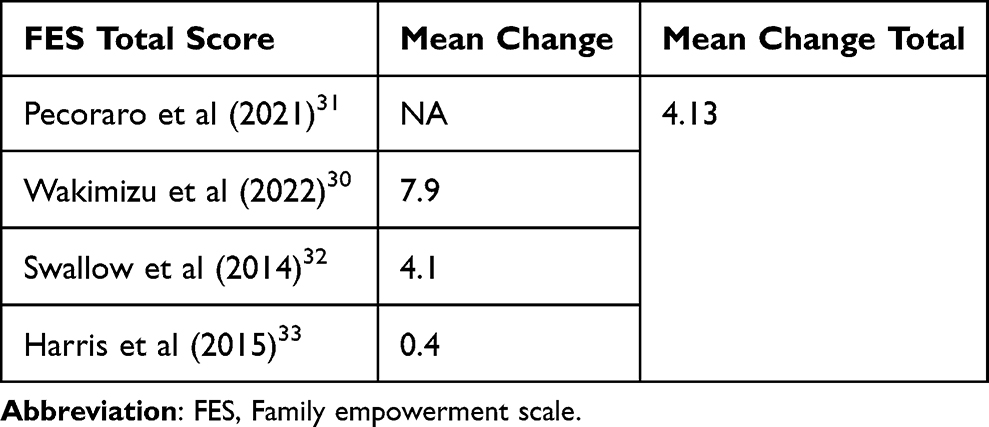 |
Table 5 Summary of Findings of Quantitative Studies and Mixed-Method Study (n = 4) |
Qualitative Study
Characteristics of Study
The three studies that have been analyzed encompass various items, including study years, research design, research locations, settings, populations, age ranges, samples, parental education levels, parental occupations, and the intervention models used (Table 6). The studies included in the analysis involved qualitative studies (n=2), including a phenomenological study (n=1) and an observational study (n=1), as well as mixed-methods studies (n=1). These studies were conducted in various locations, including the United Kingdom (n=1), Australia (n=1), and the United States (n=1), conducted in two settings, including hospitals (n=2) and one at home (n=1).
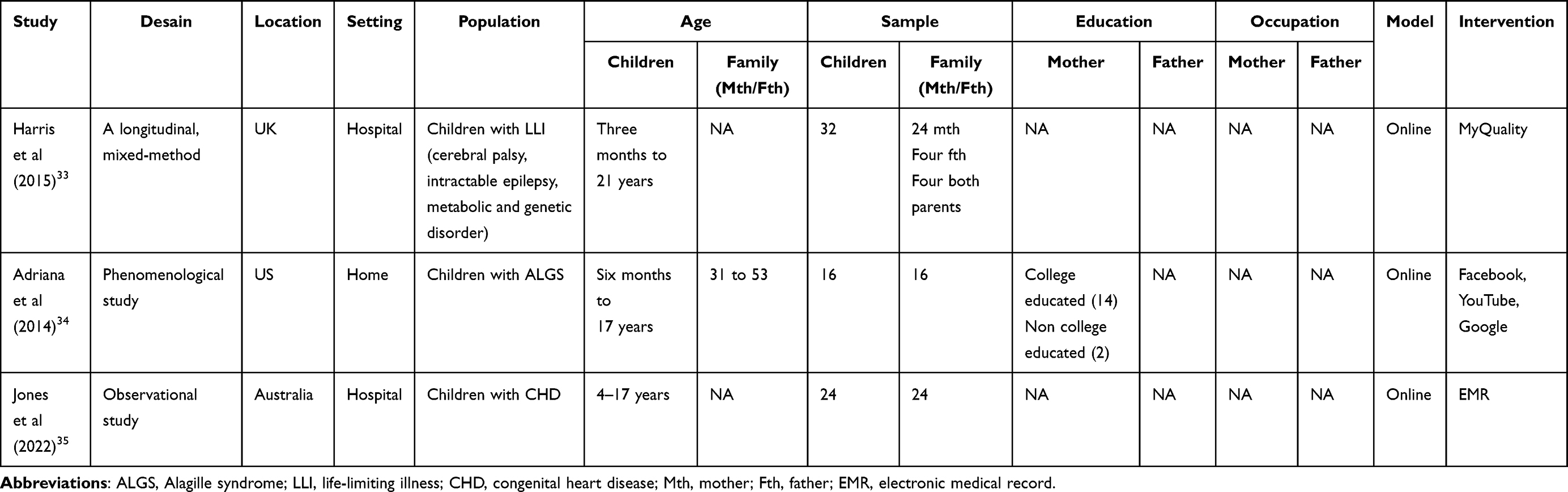 |
Table 6 Characteristics of Qualitative Studies and Mixed-Method Study (n = 3) |
The total sample involved in this research comprised 72 children and 72 parents, with the age range of children spanning from 3 months to 21 years. These children had various conditions such as cerebral palsy, difficult-to-treat epilepsy, metabolic disorders, and genetic disorders (n=1), Alagille Syndrome (ALGS) (n=1), and Congenital Heart Disease (CHD) (n=1). Only one study provided information about the parents’ highest level of education, with the majority having a high level of education, totalling 14 individuals.30 In contrast, the other two had a low level of education. Overall, these three studies described FE interventions that adopted online-based models.
Internet-Based Intervention of Family Empowerment Model
The intervention models used in the qualitative studies included MyQuality, Facebook, YouTube, Google, and Electronic Medical Records (EMR). Follow-up assessments were conducted to measure FE scores using the Family Empowerment Scale (FES), the Family’s Experience of Pediatric Surgical Mortality (PSM) Questionnaire, and the Chronic Sorrow Questionnaire–Caregiver Version, with a follow-up period ranging from 3 to 10 months (Table 7). The procedures for the FE models identified were as follows:
 |
Table 7 Interventions Model and Outcomes of Qualitative Studies and Mixed-Method Study (n = 3) |
Model 1: Family education encompassed the following aspects: understanding the workings of warfarin, its indications, and factors affecting therapy stability; target therapy and dosage; dosing administration; determining when to test INR (International Normalized Ratio); utilizing healthcare services; managing INR levels at home; and discussing subtherapeutic INR levels.
Model 2: Parents were provided with hands-on demonstrations and training in using applications or websites and encouraged to use them. Additionally, in the case of MyQuality, local nurses were involved to facilitate the family’s access to nearby healthcare services.
Outcomes
The three qualitative studies that were analyzed revealed that after online interventions were conducted to empower families with children with chronic diseases using three online intervention models, parents expressed positive outcomes.33–35 First, parents who used MyQuality reported that the website was easy and convenient. It helped manage care, increased their abilities and confidence to share information, facilitated easy access to information, improved their understanding of the disease, and contributed to managing their child’s health. Second, parents who used Facebook, YouTube, and Google indicated that they used online communication for various purposes. This included enhancing their knowledge, accessing information, increasing their awareness and empowerment in managing their child’s illness, helping their child, connecting with other parents with similar experiences, and communicating with service providers. However, the majority of parents used online communication during challenging times. Parents also reported that online communication could trigger unpleasant feelings about negative health information. Third, after using EMR, parents stated that they knew warfarin management, the ability to manage warfarin independently, saved time and felt supported by healthcare services (Table 7 and Table 8).
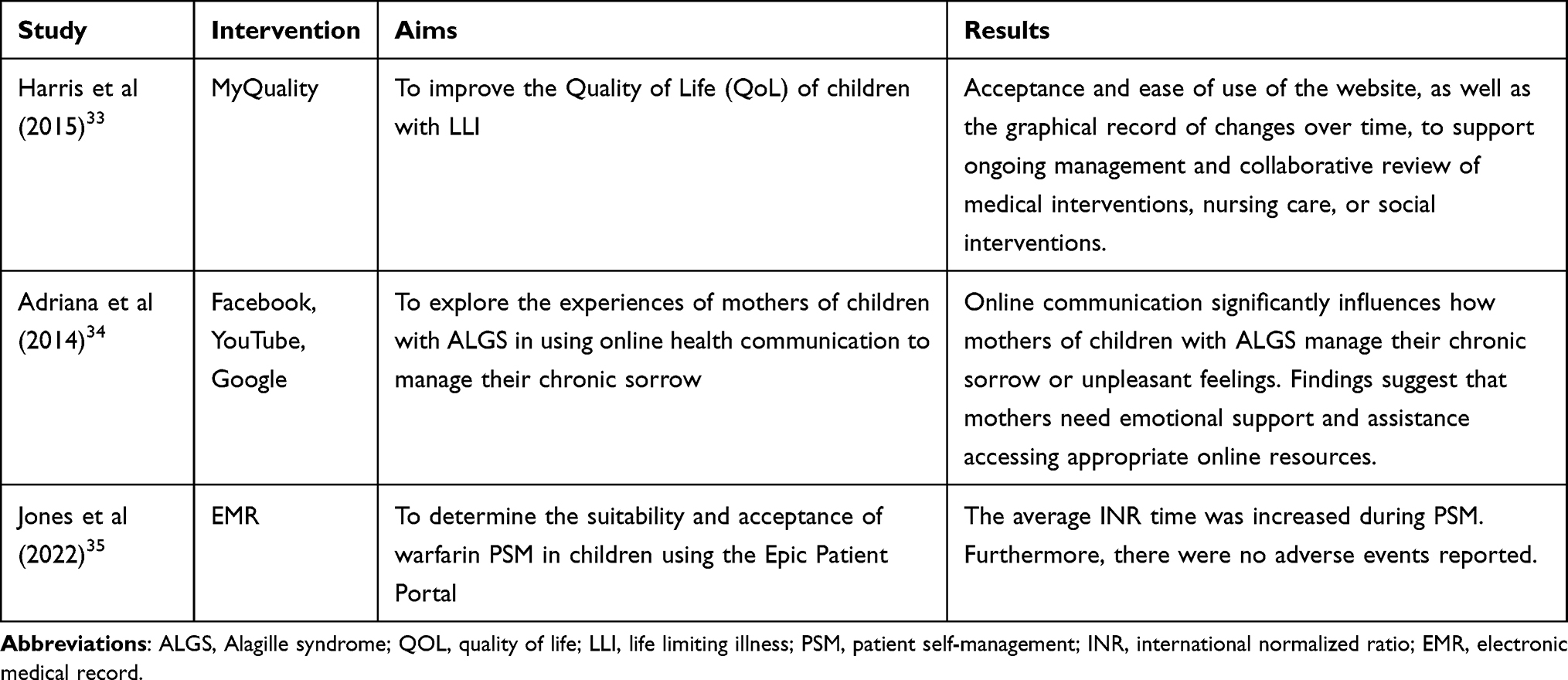 |
Table 8 Summary of Findings of Qualitative Studies and Mixed-Method Study (n = 3) |
The findings from the analysis of qualitative studies support the findings from the analysis of quantitative studies. We emphasize that internet-based interventions in empowering families with children with chronic diseases have positive impacts, including enhancing knowledge, management skills, and confidence, facilitating easy access to information and time-saving, providing convenience, fostering connections with other parents with similar experiences, enabling communication with service providers, and feeling supported by healthcare services.
Combined Evidence Thematic Synthesis of Quantitative and Qualitative Studies
Our combined findings from six studies reveal that online-based interventions in FE positively impact the total FES scores across all empowerment domains.30–35 This study categorizes the findings according to the theme of the results, which are knowledge, availability of resources and saving time, connectedness and communication, and family management and self-confidence.
Theme 1: Knowledge Enhancement
We found four studies that revealed online-based interventions in FE can enhance parental literacy, which assists parents in independently caring for children with chronic diseases.32–35 The use of applications helps improve understanding of the child’s condition and aids in clinical management comprehension.33 Additionally, parents expressed that information from online sources was crucial in increasing their knowledge, information, and empowerment in controlling their child’s illness, including understanding medical instructions or recommendations.34
Theme 2: Availability of Resources and Saving Time
We found three studies that reported that online methods can assist families in providing resource support and facilitating access to needed information.30,33,35 Acceptance, comfort, and ease of website use to support ongoing management and collaborative review of medical interventions, nursing care, or social interventions.33 Parents feel supported when they need assistance or advice. Furthermore, it helps families save time and reduce decision-making time.35
Theme 3: Connectedness and Communication
The four studies analyzed explain that internet-based family empowerment provides significant opportunities for relationships and communication between families, healthcare services, and other families facing similar issues.30,33–35 Parents use online communication for various purposes and establish connections with others experiencing similar experiences. Parents receive assistance or advice from healthcare services when needed.35 However, many parents still use online communication primarily during challenging times.34
Theme 4: Family Management and Self-Confidence
Five studies indicate that after internet-based family empowerment, there is an improvement in parents’ ability to self-manage and an increase in self-confidence.30–33,35 Parents reported increased caregiving skills and self-confidence, enabling them to share information and communicate about their child’s illness.33 Furthermore, the trust and responsibility provided by these interventions make them confident in managing their child’s illness independently.35
Discussion
Principal Finding
The primary objective of this mixed-methods systematic review is to assess the efficacy of internet-based interventions in FE for children with chronic diseases. Our findings from quantitative studies indicate that internet-based family empowerment interventions positively impact family abilities in caring for children, such as enhancing skills and competence, promoting self-management, boosting self-confidence, improving interactions with healthcare professionals, and enhancing total empowerment domain scores. This, in turn, can contribute to improved clinical outcomes for children with chronic diseases.30–33 These findings are supported by the results of the qualitative studies, which suggest that internet-based interventions can enhance knowledge, management skills, and self-confidence, as well as provide convenience, facilitate connections with parents facing similar issues, enable communication with service providers, and offer support from healthcare services.33–35
Based on the six studies, the implementation of internet-based family empowerment can be applied to families with children with chronic diseases such as obesity, physical, intellectual, and developmental disabilities, chronic kidney disease, cerebral palsy, difficult-to-treat epilepsy, metabolic disorders, and genetic disorders, Alagille Syndrome, and Congenital Heart Disease.30–35
Our findings in the current study are supported by previous research. The study conducted by Minooei et al (2016) demonstrated that FE interventions can positively enhance the quality of life of children suffering from chronic kidney disease, both in terms of physical and psychosocial aspects.14 This improvement is reflected in the reports of the children themselves but also in the experiences of their parents.36 These findings align with the study conducted by Shogi et al (2019), which explained that empowering parents of children with cancer can significantly reduce the caregiving burden.12 Furthermore, a family-focused empowerment approach has also been shown to increase self-efficacy and self-esteem in children with asthma.37
The study by Dang et al (2017) explained that providing interventions using mobile phones can help improve self-care efficacy and the quality of life of patients with heart disease.38 This is further supported by other research indicating better physical and mental health outcomes and an increase in self-efficacy among diabetes patients receiving telehealth training models.39 Consistent with the findings of Knight et al (2014), through remote monitoring technology (mHealth), patients can achieve significant improvements in various aspects of their health.40
The intervention models used in FE through online or internet-based approaches included MyQuality, Facebook, YouTube, Google, EMR, telehealth counselling, OPIS, and Group-based online intervention programs.30–35 The procedures used varied and encompassed empowerment components such as the education process, direct demonstration and training, goal setting, family self-management, reflection on activities, and discussions and communication. This aligns with previous research that developed stages of FE without an internet-based approach in chronic patient management, including exploring reality, beliefs, and expectations; considering and making decisions; developing abilities in managing care; strengthening confidence; and evaluating program outcomes.41,42
Based on the combined results of quantitative and qualitative studies, we identified several thematic outcomes following internet-based family empowerment interventions, including increased knowledge, availability of resources and time-saving, connectedness and communication, family management and self-confidence.30–35 This aligns with the study by Sayani et al (2019), which showed significant time and cost savings for patients receiving care for chronic diseases or infections through telemedicine in remote areas.43
The use of the internet still has its limitations. Findings from this study regarding internet use include online triggers. Online communication can trigger sadness and unpleasant feelings in families because they often encounter negative information about their child’s illness.34 However, the development of online media or applications should pay attention to clear and comprehensive information aspects and maintain consultation services to reduce the ambiguity of information received by families. Consistent with previous studies, it was revealed that a weakness in internet-based FE models is the limited internet connectivity, especially in geographically unsupported areas.44 Additionally, not everyone has resources like smartphones to engage in FE.30
Overall, the findings of this study reveal that the implementation of online-based interventions in FE has a positive impact on enhancing all empowerment domains.30–35 However, the potential of internet technology plays a crucial role in determining intervention strategies in healthcare, especially in the context of children with chronic diseases. Technological advancements are driving the adoption of telehealth as an electronic information and communication service to improve health, which can be widely utilized.45,46
Strength and Limitations
This study still has some limitations that could potentially bias the findings. In qualitative and quantitative studies, most did not thoroughly explain confounding factors that could influence the research outcomes, and some did not clarify the intervention procedures and duration. Furthermore, the assessment of study quality using MMAT involved only two individuals, potentially introducing bias into the quality assessment results, not being able to access some full-text articles, and limiting references to English only may have limited the study’s results.
Despite its limitations, several benefits of this study should also be acknowledged. First, the study implemented a comprehensive search strategy, strict inclusion and exclusion criteria, and a systematic data extraction and quality assessment process. Second, there is a lack of research on implementing internet technology in FE for children with chronic diseases. Furthermore, this is the first mixed-method systematic review to identify the use of internet-based interventions in empowering families of children with chronic diseases. The study involved countries worldwide, including Europe, America, Australia, and Asia. While the existing evidence is still limited, the findings of this study provide some strong indications of the effects of implementing internet-based interventions in empowering families with children with chronic diseases. However, these study findings represent four continents and can serve as valuable information for healthcare providers and governments as a basis for policy and strategic interventions.
Implications for Clinical Practice and Policy
The implications of our findings suggest that internet-based interventions in family empowerment may have benefits in reducing problems in children with chronic diseases. This review offers a broader health intervention strategy, which allows nurses or health care providers to engage in internet-based interventions. The findings of this study support that internet-based family empowerment interventions should be adopted to meet the health care needs of children with chronic diseases.
Integrating pediatric nursing practice into internet-based care programs can be a new strategy in clinical practice. The approach of internet-based intervention in family empowerment for children with chronic diseases can be considered as a clinical policy to improve promising services in pediatric care with the principles of family empowerment.
Conclusion
We present a mixed-method systematic review that explores the implementation of internet-based interventions in empowering families with children with chronic diseases. Our study identified six quantitative and qualitative studies, revealing that online intervention models can be used to empower families dealing with children suffering from chronic conditions such as obesity, physical and intellectual disabilities, developmental disabilities, chronic kidney disease, cerebral palsy, epilepsy, metabolic disorders, genetic disorders, Alagille Syndrome, and Congenital Heart Disease. The efficacy of internet-based family empowerment interventions is reflected in improving knowledge, availability of resources and time-saving, enhanced connectedness and communication, family management and self-confidence.
This study highlights that online-based interventions in FE positively impact enhancing empowerment across various domains. This study can serve as a foundation for further research on similar topics. As a future research direction, conducting a meta-analysis on the four efficacy themes of internet-based interventions in empowering children with chronic diseases is warranted.
Acknowledgments
The authors appreciated the Universitas Padjadjaran, Sumedang, West Java, Indonesia, for supporting and facilitating the database search access.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. UNICEF. Noncommunicable diseases. United Nations Children’s Fund-UNICEF; 2020. Available from: https://data.unicef.org/topic/childhealth/noncommunicable-diseases/.
2. Sentell T, Choi SY, Ching L, Quensell M. Prevalence of Selected Chronic Conditions Among Children, Adolescents, and Young Adults in Acute Care Settings in Hawaii. Centers Dis Control Prev. 2020;17(4):1–10.
3. Bayu D Penderita Kanker Anak Indonesia Terbanyak di Asia Tenggara (Indonesia has the highest number of pediatric cancer patients in Southeast Asia). Data Indonesia; 2022. Available from: https://dataindonesia.id/ragam/detail/penderita-kanker-anak-indonesia-terbanyak-di-asia-tenggara.
4. WHO. Childhood cancer. World Health Organization; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer-in-children.
5. Ariani A, Yuda Novira R, Yosoprawoto M. Kualitas Hidup Anak dengan Penyakit Jantung (Quality of Life for Children with Heart Disease). J Kedokt Brawijaya. 2012;27(1):56–60. doi:10.21776/ub.jkb.2012.027.01.10
6. Megari K. Quality of life in chronic disease. Heal Psychol Res. 2013;1(e27):141–148. doi:10.4082/hpr.2013.e27
7. Muriati SE, Damayanti EAF. Dukungan Keluarga Dengan Kualitas Hidup Anak (Family Support with Children’s Quality of Life). Nerspedia. 2019;2:51–58.
8. Borhani F, Najafi MK, Rabori ED, Sabzevari S. The effect of family-centered empowerment model on quality of life of school-aged children with thalassemia major. Iran J Nurs Midwifery Res. 2011;16(4):292–298.
9. Berman A, Synder S, Frandsen G. Kozier & Erb’s Fundamentals of Nursing: Concepts, Process, and Practice. Pearson Education, Inc; 2016.
10. Yanitawati MA, Widianti E. Hubungan Perilaku Sakit Dalam Aspek Psikososial Dengan Kualitas Hidup Remaja Thalasemia (The Relationship of Pain Behavior in Psychosocial Aspects with Quality of Life of Thalassemia Adolescents). Int J Med. 2017;5(1):38–47.
11. Keshvari M, Hedayati B, Moeini M, Alhani F. A survey on the effect of implementation of a family-centered empowerment model on blood pressure and empowerment dimensions in the elderly people with hypertension. J Educ Health Promot. 2015;4(94):1–10. doi:10.4103/2277-9531.171808
12. Shoghi M, Shahbazi B, Seyedfatemi N. The effect of the Family-Centered Empowerment Model (FCEM) on the care burden of the parents of children diagnosed with cancer. Asian Pacific J Cancer Prev. 2019;20(6):1757–1764. doi:10.31557/APJCP.2019.20.6.1757
13. Ghasemi A, Rahimi Foroshani A, Kheibar N, et al. Effects of family-centered empowerment model based education program on quality of life in methamphetamine users and their families. Iran Red Crescent Med J. 2014;16(3). doi:10.5812/ircmj.13375
14. Minooei MS, Ghazavi Z, Abdeyazdan Z, Gheissari A, Hemati Z. The Effect of the Family Empowerment Model on Quality of Life in Children with Chronic Renal Failure: children's and Parent’s Views. Nephrourol Mon. 2016;8(4):1–7. doi:10.5812/numonthly.36854
15. Lee AYL, Wong AKC, Hung TTM, Yan J, Yang S. Nurse-led Telehealth Intervention for Rehabilitation (Telerehabilitation) Among Community-Dwelling Patients With Chronic Diseases: systematic Review and Meta-analysis Corresponding Author: registration. J Med Internet Res. 2022;24(11):1–15. doi:10.2196/40364
16. Guo Y, Albright D. The effectiveness of telehealth on self-management for older adults with a chronic condition: a comprehensive narrative review of the literature. J Telemed Telecare. 2017;1–12. doi:10.1177/1357633X17706285
17. Pace R, Pluye P, Bartlett G, et al. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int J Nurs Stud. 2012;49(1):47–53. doi:10.1016/j.ijnurstu.2011.07.002
18. Culmer N, Smith T, Stager C, et al. Telemedical Asthma Education and Health Care Outcomes for School-Age Children: a Systematic Review. J Allergy Clin Immunol Pract. 2020;8(6):1908–1918. doi:10.1016/j.jaip.2020.02.005
19. Ferro F, Tozzi AE, Erba I, et al. Impact of telemedicine on health outcomes in children with medical complexity: an integrative review. Eur J Pediatr. 2021;180(8):2389–2400. doi:10.1007/s00431-021-04164-2
20. Kodjebacheva GD, Culinski T, Kawser B, Amin S. Satisfaction with pediatric telehealth according to the opinions of children and adolescents during the COVID-19 pandemic: a literature review. Front Public Heal. 2023;11:1–11. doi:10.3389/fpubh.2023.1145486
21. Kodjebacheva GD, Tang C, Groesbeck F, Walker L, Woodworth J, Schindler-Ruwisch J. Telehealth Use in Pediatric Care during the COVID-19 Pandemic: a Qualitative Study on the Perspectives of Caregivers. Children. 2023;10(2):20311. doi:10.3390/children10020311
22. Karimi N, Zarifsanaiey N, Vizeshfar F. Comparison of the effect of electronic learning and blended learning on the empowerment of the caregivers of cancer patients under chemotherapy. Support Care Cancer. 2022;2537–2543. doi:10.1007/s00520-021-06682-z
23. Knapp C, Madden V, Wang H, Sloyer P, Shenkman E. Internet use and eHealth Literacy of low-income parents whose children have special health care needs. J Med Internet Res. 2011;13(3):e75. doi:10.2196/jmir.1697
24. Pace R, Pluye P, Bartlett G, et al. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int J Nurs Stud. 2012;49(1):47–53. doi:10.1016/j.ijnurstu.2011.07.002
25. Pluye P, Hong QN. Combining the Power of Stories and the Power of Numbers: mixed Methods Research and Mixed. Annu Rev ofPublic Heal. 2014;35(2):1–17. doi:10.1146/annurev-publhealth-032013-182440
26. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
27. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. doi:10.1016/j.ijsu.2010.02.007
28. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
29. Hong QN, Pluye P, Fabregues S, et al. Mixed Methods Appraisal Tool (MMAT) Version 2018. BMJ Open. 2018:1–10.
30. Wakimizu R, Matsuzawa A, Fujioka H, et al. Effectiveness of a peer group-based online intervention program in empowering families of children with disabilities at home. Front Pediatr. 2022:1–18. doi:10.3389/fped.2022.929146
31. Pecoraro P, Gallè F, Muscariello E, Di V. A telehealth intervention for ensuring continuity of care of pediatric obesity during the CoVid-19 lockdown in Italy. Nutr Metab Cardiovasc Dis. 2020;31:3502–3507. doi:10.1016/j.numecd.2021.09.026
32. Swallow VM, Knafl K, Santacroce S, Smith T, Carolan I, Hons MA. An Interactive Health Communication Application for Supporting Parents Managing Childhood Long-Term Conditions: outcomes of a Randomized Controlled Feasibility Trial Corresponding Author. JMIR Res Protoc. 2014;3:1–19. doi:10.2196/resprot.3716
33. Harris N, Beringer A, Fletcher M. Families’ priorities in life-limiting illness: improving quality with online empowerment. Arch Dis Child. 2016;101(3):247–252. doi:10.1136/archdischild-2015-308769
34. Glenn AD. Using online health communication to manage chronic sorrow: mothers of children with rare diseases speak. J Pediatr Nurs. 2015;30(1):17–24. doi:10.1016/j.pedn.2014.09.013
35. Jones S. Using an electronic medical record patient portal for warfarin self-management: empowering children and parents. Res Pract Thromb Haemost. 2023;7(2):100066. doi:10.1016/j.rpth.2023.100066
36. Davarpanah M, Fayazi S, Shariati A, Mirhosseini SD. The Effect of a Family-centered Empowerment Model on the Quality of Life of Patients With Stroke. J Client-Centered Nurs Care. 2020;6(1):13–22. doi:10.32598/jccnc.6.1.293.4
37. Teymouri F, Alhani F, Kazemnejad A. The Effect of Family-Centered Empowerment Model on Self-Efficacy and Self-Esteem of the Children With Asthma. Prev Care Nurs Midwifery J. 2017;7(1):18–26.
38. Dang S, Karanam C, Go O, Care P. Outcomes of a Mobile Phone Intervention for Heart Failure in a Minority County Hospital Population. Telemed e-Health. 2017;23(6):1–12. doi:10.1089/tmj.2016.0211
39. Young H, Miyamoto S, Ward D, Dharmar M, Tang-feldman Y, Berglund L. Sustained Effects of a Nurse Coaching Intervention via Telehealth to Improve Health Behavior Change in Diabetes. Telemed e-Health. 2013;828–834. doi:10.1089/tmj.2013.0326
40. Knight E, Stuckey MI, Petrella RJ. Health Promotion Through Primary Care: enhancing Self-Management With Activity Prescription and mHealth. Clin Featur. 2014;42(3):90–99. doi:10.3810/psm.2014.09.2080
41. Wacharasin C, Phaktoop M, Sananreangsak S. Examining the Usefulness of a Family Empowerment Program Guided by the Illness Beliefs Model for Families Caring for a Child With Thalassemia. J Fam Nurs. 2015;21(2):295–321. doi:10.1177/1074840715585000
42. Farahani PV, Pou DH, Alhani F, Ashori M, Azadnia M. Investigating the Effect of Family-Centered Empowerment Model on the Lifestyle of Children Suffering From Leukemia. J Holist Nurs Midwifery. 2018;28(3):198–204. doi:10.29252/HNMJ.28.3.198
43. Sayani S, Muzammil M. Addressing cost and time barriers in chronic disease management through telemedicine: an exploratory research in select low- and middle-income countries. Ther Adv Chronic Dis. 2019;10:1–10. doi:10.1177/2040622319891587
44. Notario PM, Gentile E, Amidon M, Angst D, Lefaiver C, Webster K. Home-Based Telemedicine for Children with Medical Complexity. Telemed e-Health. 2019;2(3):1–10. doi:10.1089/tmj.2018.0186
45. Fernandez-Moyano AM, López-Jimeno W. Telehealth. N Engl J Med. 2018;378(4):401–402. doi:10.1056/NEJMc1715239
46. Domhardt M, Schröder A, Geirhos A, Steubl L, Baumeister H. Efficacy of digital health interventions in youth with chronic medical conditions: a meta-analysis. Internet Interv. 2021;24. doi:10.1016/j.invent.2021.100373
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.