Back to Journals » Journal of Pain Research » Volume 11
The efficacy of electromyographic biofeedback on pain, function, and maximal thickness of vastus medialis oblique muscle in patients with knee osteoarthritis: a randomized clinical trial
Authors Raeissadat SA, Rayegani SM ![]() , Sedighipour L, Bossaghzade Z, Abdollahzadeh MH, Nikray R, Mollayi F
, Sedighipour L, Bossaghzade Z, Abdollahzadeh MH, Nikray R, Mollayi F
Received 29 March 2018
Accepted for publication 7 August 2018
Published 8 November 2018 Volume 2018:11 Pages 2781—2789
DOI https://doi.org/10.2147/JPR.S169613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Überall
Seyed Ahmad Raeissadat,1 Seyed Mansoor Rayegani,2 Leyla Sedighipour,1 Zeynab Bossaghzade,2 Mohamad Hesam Abdollahzadeh,2 Rojin Nikray,2 Fazeleh Mollayi3
1Physical Medicine and Rehabilitation Research Center and Department, Clinical Research Development Center, Shahid Modarres Hospital, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Physical Medicine and Rehabilitation Research Center and Department, Shohadaye Tajrish Hospital, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 3Department of Sport Sciences, Payame Noor University, Tehran, Iran
Introduction: The aim of this survey was to examine the effect of adding electromyographic biofeedback (EMGBF) to isometric exercise, on pain, function, thickness, and maximal electrical activity in isometric contraction of the vastus medialis oblique (VMO) muscle in patients with knee osteoarthritis (OA).
Methods: In this clinical trial, 46 patients with a diagnosis of knee OA were recruited and assigned to two groups. The case group consisted of 23 patients with EMGBF-associated exercise, and the control group was made up of 23 patients with only isometric exercise. Data were gathered via visual analog scale (VAS) score, the Persian version of the Western Ontario and McMaster Universities Osteoarthritis Index and Lequesne questionnaires, ultrasonography of the VMO, and surface electromyography of this muscle at baseline and at the end of the study. Variables were compared before and after the exercise program in each group and between the two groups.
Results: At the end of the study, there were no significant differences between the two groups regarding measured variables. Only the VAS score was significantly less in the case group. Although all assessed parameters, except for VMO muscle thickness, were found to be improved significantly in each group, the degree of change was not significantly different between the two groups, except for VAS score. VMO muscle thickness did not change significantly after exercise therapy in either of the groups.
Conclusion: Isometric exercises accompanied by EMGBF and the same exercises without biofeedback for 2 months both led to significant improvements in pain and function of patients with knee OA. Real EMGBF was not superior to exercise without biofeedback in any of the measured variables, except for VAS score.
Keywords: knee osteoarthritis, isometric quadriceps exercise, EMG biofeedback
Introduction
Osteoarthritis (OA) is one of the most common musculoskeletal disorders in the elderly.1 The global prevalence of symptomatic knee OA has been estimated to be 3.8%. Knee OA also imposes a great economic burden on societies, with knee and hip OA being the eleventh highest contributor to global disability.2 There is no definite treatment for knee OA; therefore, every once in a while, a new method to control pain and improve function in these patients is being suggested. New nonsurgical treatments include intra articular injection of ozone,3 hyaluronic acid,4 platelet-rich plasma and plasma rich in growth factors,5–7 new physical modalities, such as laser therapy,8 and new methods in exercise therapy, such as using an electromyographic biofeedback (EMGBF) device, for modifications in muscle–force balance and to reduce pain and improve function in patients with knee OA.9
Knee OA typically presents as pain and weakening of the quadriceps muscles that can affect patients’ walking ability.10,11 Consequently, a vicious cycle is established in which patients use the knee joint less frequently due to pain, which results in weakness of the muscles.12 Weakness of the muscles makes the knee joint more unstable and prone to degeneration. The vastus medialis oblique (VMO) is one of the muscles of the quadriceps group. Weakness of this muscle has been reported to be associated with aggravated pain in knee OA patients.13 An increase in VMO size after treatment of knee OA has been reported to ameliorate pain in the afflicted joint and to be beneficial for compensating for structural changes.14 Indeed, quadriceps muscle volume rather than quadriceps activation is a far more reliable prognostic factor.15
Previous studies have shown a significant decrease in maximum voluntary isometric contraction (MVIC) of the quadriceps muscles in patients with knee OA that can be improved by voluntary muscle activation.16,17 One of the treatment methods that can be easily used for elderly patients with knee OA is isometric exercise, the application of which has been associated with significant improvement in the MVIC of the quadriceps muscles.18
To enhance the patient’s active participation in treatment with isometric exercises, the EMGBF device has been designed to transform the action potential of the muscle into feedback signals of a visual or auditory nature, such that it can affect the subject’s voluntary activity.19,20 It has been shown that compliance of subjects and their motivation increases considerably when EMGBF is incorporated in their exercise programs.19 Application of this method in strengthening the VMO muscle has enabled therapists to correct misalignment of the patellofemoral joint.21 There is no consensus regarding the efficacy of this method in knee OA when incorporated with quadriceps strengthening exercises. Research has shown no significant additive effect of EMGBF on regular strengthening exercise programs in these patients. In patients with meniscal injury, EMGBF was an effective treatment modality in improving quadriceps muscle strength,22 while in other conditions, such as knee arthritis in rheumatoid arthritis in patients younger than 45 years, EMGBF was not shown to affect improvement significantly.23 This is the first study to evaluate the use of EMGBF in isometric exercise of quadriceps muscles regarding its effects on voluntary VMO muscle activity, pain, function, and maximal VMO muscle thickness in patients with knee OA in an Iranian population.
Methods
In this single-blinded, randomized controlled trial, patients with knee OA referred to Shohadaye Tajrish and Shahid Modarres hospitals in 2016 were screened to assign eligible patients to this study. The study was designed according to the CONSORT (consolidated standards of reporting trials) statement,24 and was registered at the Iranian Registry of Clinical Trials (www.irct.ir) under IRCT2017041513442N14.
Sample size
Sample size was calculated by the formula 2(Z1–β + Z1–α/2)σ2/d2, which is used for estimating the sample size for case–control studies. We estimated the sample size with our primary outcome: the visual analog scale (VAS). According to similar studies, σ=1.7, d=1.5, and estimated sample size was 21 for each group. As per our previous studies, we estimated a 10% dropout and decided to recruit 23 patients for each group.
Inclusion and exclusion criteria
Subjects with a definite diagnosis of knee OA according to the guidelines of the American College of Rheumatology with at least 6 months of knee pain, grade 1 or 2 joint cartilage degradation based on the Kellgren–Lawrence classification, and a body mass index (BMI) of <35 kg/m2 were invited to participate in this trial. On the other hand, subjects who had undergone physical therapy or intraarticular injection in the past 3 months, patients who had taken oral corticosteroids in the past 4 weeks, patients with a history of surgical interventions on their knees, subjects with a history of radiculopathy, or those with a history of systemic diseases, such as rheumatoid arthritis, were excluded.
Ethical considerations
Eligible subjects were given thorough explanations about the objectives of the study, its importance and methods, and were reassured that their data would be considered confidential, used anonymously, could be only accessed by the main authors, and that they could leave the study at will. Informed written consent was obtained from patients willing to participate. The institutional review board of Shahid Beheshti University of Medical Sciences reviewed and approved the study protocol, and the trial was implemented according to Declaration of Helsinki principles.
Enrollment and interventions
A total of 46 patients with knee OA were recruited and randomly assigned to two groups of controls (without biofeedback [BF]) and cases (EMGBF), using block randomization. Patients in both groups were taught isometric exercises for quadriceps muscles by a physical medicine and rehabilitation specialist. During the 2-month period of the study, all patients participated in twelve 15-minute exercise sessions in physical medicine and rehabilitation ward of Shahid Modarres Hospital under direct supervision of a specialist. All exercises were performed via an EMGBF device; however, in the control group, the active electrode was not connected, so subjects did not receive any feedback from the device, while patients in the EMGBF group received visual and auditory feedback. To perform isometric quadriceps exercise, with patient in supine position, a rolled towel with a width of approximately 10 cm was placed under the patient’s popliteal fossa and the subject asked to press the towel as hard as possible for 5 seconds. Then, the muscle was relaxed for 10 seconds and the cycle repeated for a total of 15 minutes.25,26 During therapeutic sessions, five patients left the study, mostly because of inability to participate in exercise sessions due to long distance to the hospital. At the end of the study, 21 patients in the case group and 20 patients in the control group had finished the sessions (Figure 1).
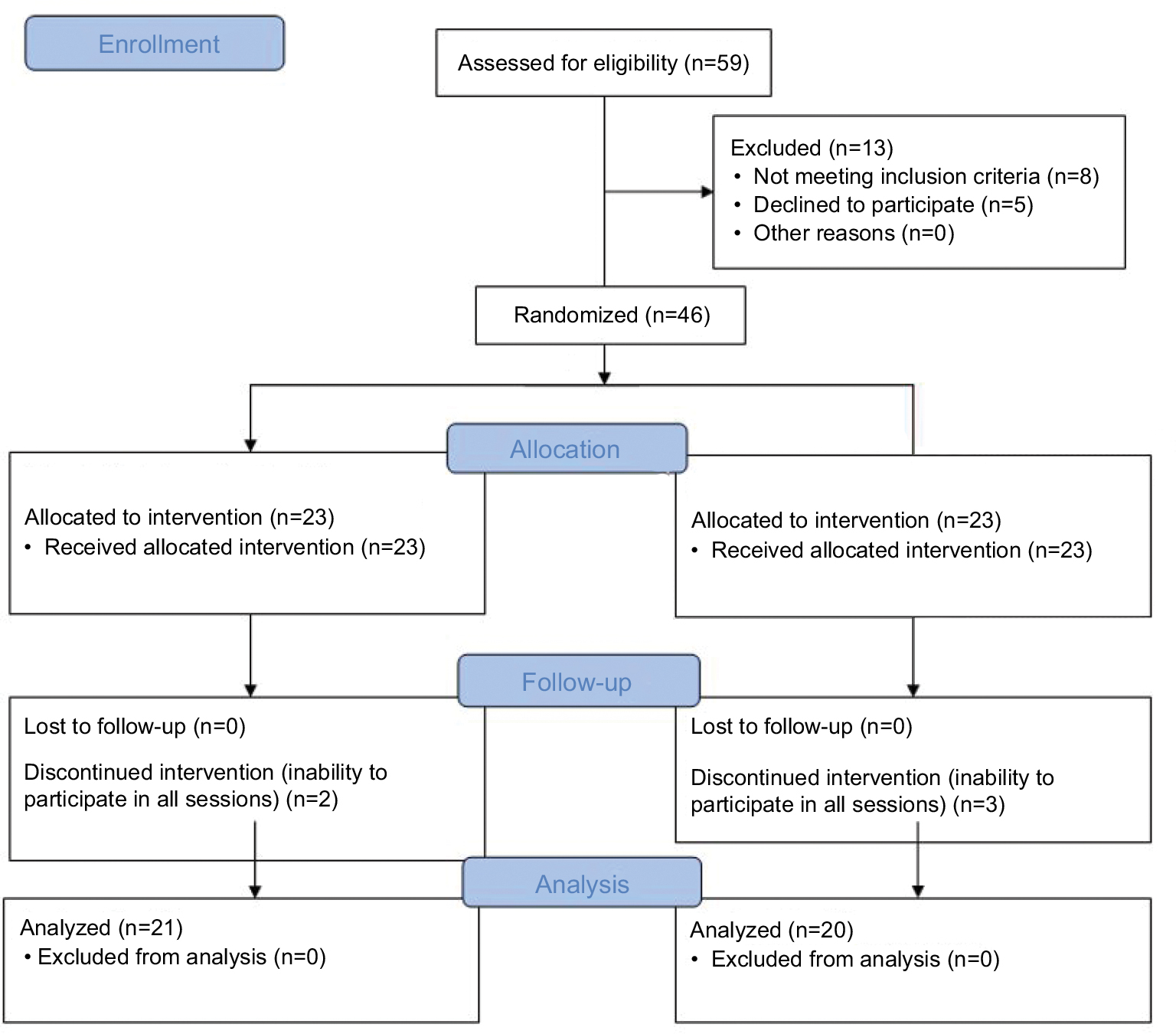 | Figure 1 Flowchart of the study. |
EMGBF settings
A single-channel MyoTrac Infiniti Continence Suite EMGBF device (Thought Technology, Montreal, Canada) was used and set on the muscle strengthening protocol. Skin (where the electrodes were going to be attached) was shaved and ethanol applied to decrease skin impedance. Gel-contained electrodes of the device were attached according to the SENIAM (surface electromyography for noninvasive assessment of muscles) protocol to record the electrical activity of the muscle.27 Active and reference electrodes were attached to record the electrical activity of the VMO muscle. The active electrode was attached 4 cm superiorly and the reference electrode 3 cm medially to the superomedial aspect of the patella. The ground electrode was also attached to the ipsilateral leg 2–3 cm inferior to the patella.
Patients were asked to lie in a supine position, a rolled towel of width approximately 10 cm was placed under the patient’s knee, and he/she was asked to press the towel as hard as possible for 5 seconds, relax for 10 seconds, and then repeat the process three times so that the device could detect and record three values of maximum voluntary activity of the muscle (action potential) and calculate the mean. The voluntary activity threshold of the patient was set at 20% less than the calculated mean.28 Each time the patients in the EMGBF group managed to contract their muscles beyond the established threshold, the device gave them positive feedback, which could be a puzzle getting completed one piece at a time or an animated car moving across the monitor. The physician increases the threshold at each session, according to the patients’ strength, so that they become encouraged to increase their muscle activity.
Parameters measured
Information was gathered by one of the researchers blinded to the group classification of patients. Collected data included age, sex, height, and weight for calculating BMI, grade of OA according to Kellgren–Lawrence classification, the side of the affected knee, duration of symptoms, pain severity, VMO muscle thickness, VMO muscle electrical activity, symptom severity, and functional status of the subjects. All measurements were performed once before the interventions and again at the end of the 2-month period. Pain severity was determined by patients on a scale of 0–10 by the means of the VAS.
Patients underwent ultrasound (US) assessment by a trained physiatrist using a 7–12 MHz probe (Alpinion E-Cube 7 US device). The patient lay in a supine position with the knee fully extended and muscles kept relaxed. The maximum thickness of the VMO muscle was measured at the proximal border of the patella, between the two superficial and deep aponeuroses.
The severity of the patients’ symptoms and their functional status was also assessed via the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Lequesne questionnaire. The Persian version of the WOMAC questionnaire was used, the validity and reliability of which have been evaluated and confirmed by Eftekhar-Sadat et al.16 The questionnaire includes five questions about pain severity (0–20), two items on joint stiffness (0–8), and 17 questions on functional limitations of the patient (0–68). Each item is scored on a scale of 0–4, and the greater the score, the worse the pain and function. The total score of the subjects from this index was reported from a total of 96.
The Persian version of the Lequesne questionnaire was also used to assess the severity of OA in participants. The validity and reliability of this questionnaire was studied and confirmed by Nadrian et al in 2012.29 It is comprised of five questions on pain severity, two on maximum walking ability, and four on daily activities. At the end of 12 exercise sessions, electrical activity of the VMO muscle is measured while patients were performing an MVIC of quadriceps muscles three times with intervals of 1 minute. The mean of these three measurements was calculated as the maximum electrical activity of the VMO muscle. Eventually, after the 2-month period of the study, subjects were asked to report their satisfaction from the treatments in percentages.
Statistical analysis
Data were analyzed using SPSS version 22 (IBM, Armonk, NY, USA). Qualitative variables are presented as frequency and percentage and quantitative variables calculated as means and SD. The χ2 test and Student’s t-test were used to assess the correlation between qualitative and quantitative variables, respectively. P<0.05 was considered statistically significant in all analyses.
Results
A total of 41 patients with OA in two groups of controls (exercise without BF) with 20 subjects (48.8%) and intervention (exercise + EMGBF) with 21 patients (51.2%) finished the study. The average age of the sample population was 58±8.4 years, ranging from 47 to 70 years. The majority of subjects were female (85.4%) and married (92.7%). Mean BMI was found to be 28.0±2.9 kg/m2, with a minimum of 20.5 and a maximum of 33.0. The affected side was quite balanced in the sample population, with 21 right knees (51.2%) and 20 left knees (48.8%). According to the Kellgren–Lawrence classification, 14 subjects (34.1%) had grade 1 OA and 27 (65.9%) were found to have grade 2 OA. Subjects reported having had knee pain for an average of 3.1±1.8 years. As presented in Table 1, there were no significant differences between the two groups regarding the basic characteristics of the subjects, which indicates a successful homogeneous randomization of the sample population.
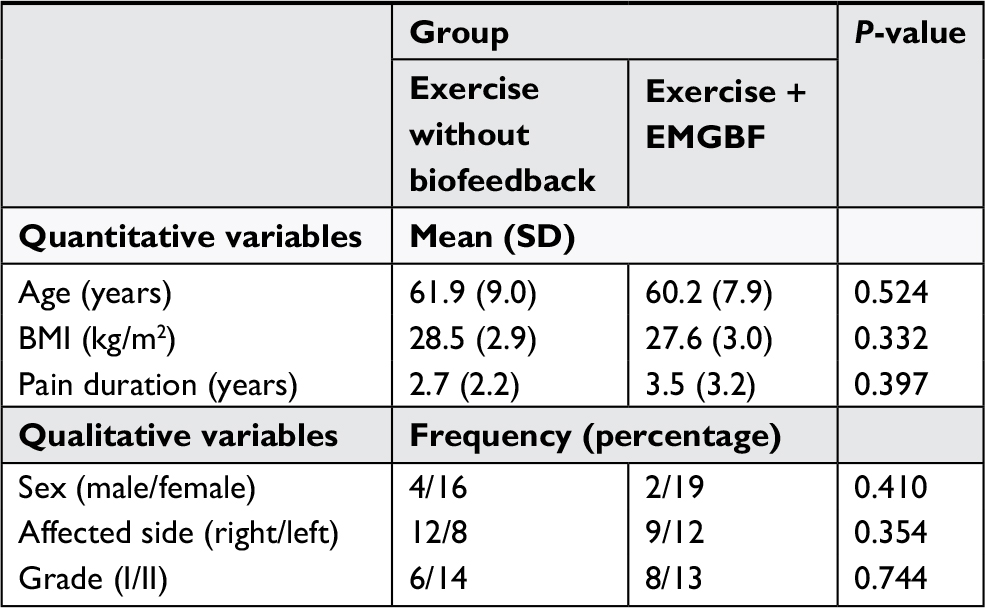 | Table 1 Differences in the basic characteristics of the sample population between the two case and control groups Abbreviations: BF, biofeedback; EMGBF, electromyographic BF; BMI, body-mass index. |
Table 2 presents differences in outcome measures between the two groups before and after interventions. Table 3 shows changes in outcome measures after intervention in each group and presents a comparison of changes between the two groups. As can be seen, there was no significant difference in VAS scores between the two groups before treatment (P=0.570), whereas after intervention, VAS scores were found to be significantly lower in the EMGBF group (P=0.002). Changes in VAS scores were found to be significant in both groups (P<0.001) and significantly greater in the EMGBF group compared to the control group (P<0.001).
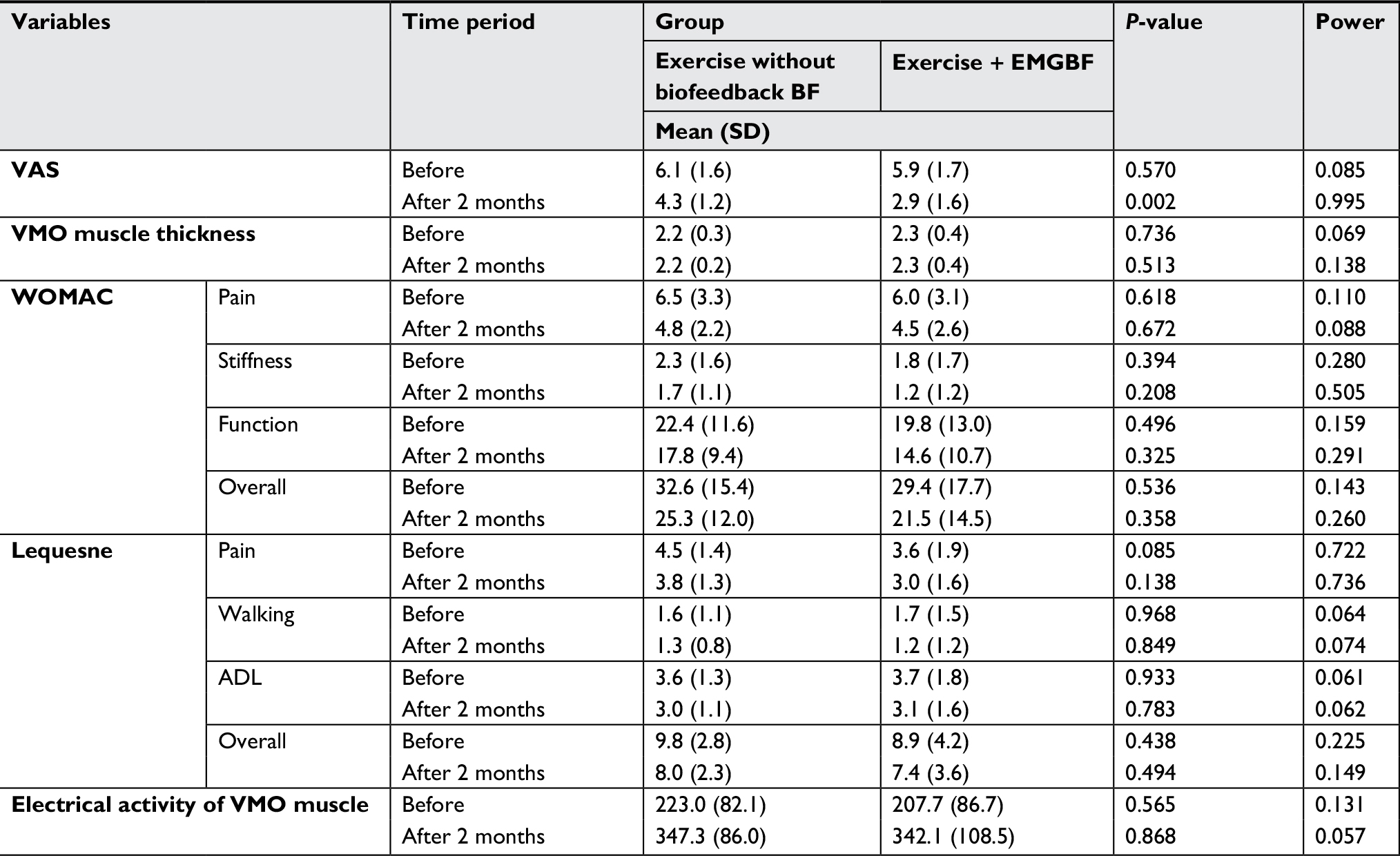 | Table 2 Differences between the two groups before and after intervention Abbreviations: ADL, activities of daily living; BF, biofeedback; EMGBF, electromyographic BF; VAS, visual analog scale; VMO, vastus medialis oblique; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. |
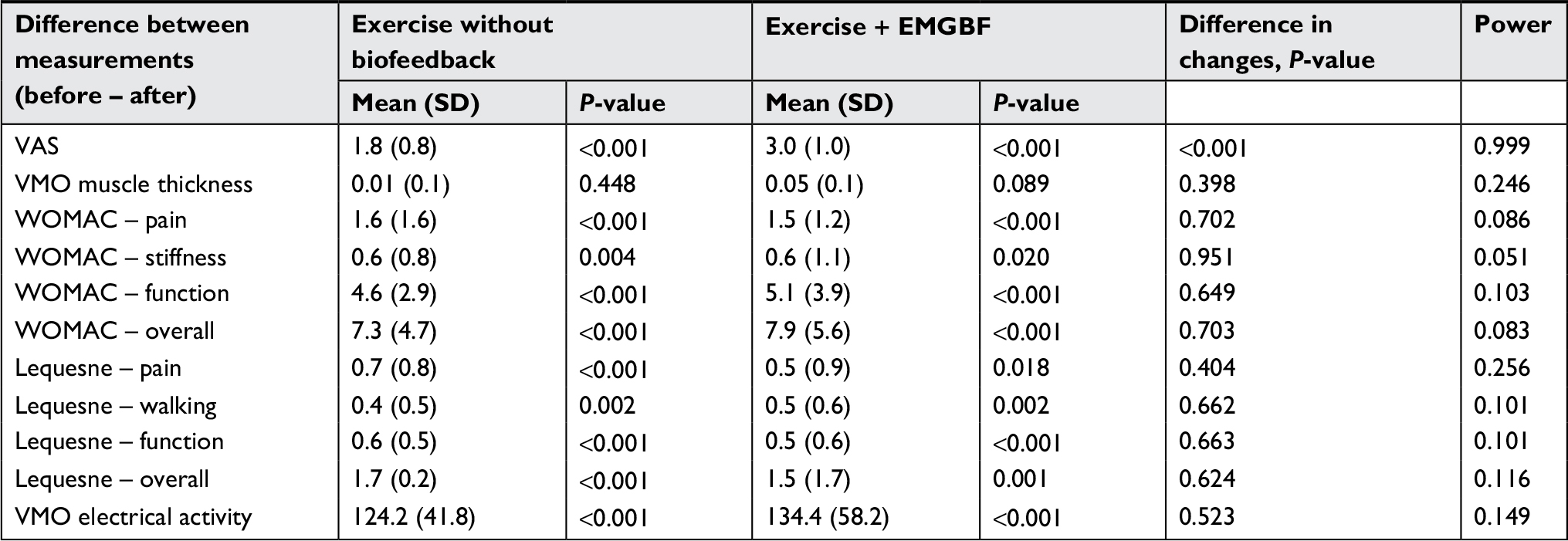 | Table 3 Changes in measured variables in each group and comparison between groups Abbreviations: BF, biofeedback; EMGBF, electromyographic BF; VAS, visual analog scale; VMO, vastus medialis oblique; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. |
VMO muscle thickness did not differ significantly between the two groups before (P=0.736) or after (P=0.513) intervention, nor did it change significantly in control (P=0.448) and (P=0.089) intervention groups. Changes in this parameter were not significantly different between the two groups (P=0.398) either. Scores obtained from the pain component of the WOMAC questionnaire were not significantly different between the two groups before intervention (P=0.618) or after it (P=0.672). Moreover, although the scores had changed significantly in each group (P<0.001) after intervention, the differences between them were not statistically significant (P=0.702). Results from the joint-stiffness and -function components of the WOMAC questionnaire and the total score of this index were also similar to its pain component.
The results of pain, walking ability, and function components of the Lequesne questionnaire along with the total score of this index also followed the same pattern as the WOMAC results. Differences between the two groups were not significant before or after intervention. Changes in each variable in each group were found to be significant, but the two groups did not differ significantly regarding changes in scores.
Similarly, the electrical activity of the muscle did not differ significantly between the two groups before (P=0.565) or after treatment (P=0.868). Though this parameter changed significantly in each group after intervention (P<0.001), the change was not significantly different between the two groups (P=0.523). After the 2-month period, patients were asked to report their satisfaction in percentages. The satisfaction of patients in the EMGBF group (80.9±8.9) was found to be significantly higher than the control group (63.0±14.9), with a P-value of 0.001. Comparison between the two groups regarding this outcome measure is presented in Figure 2.
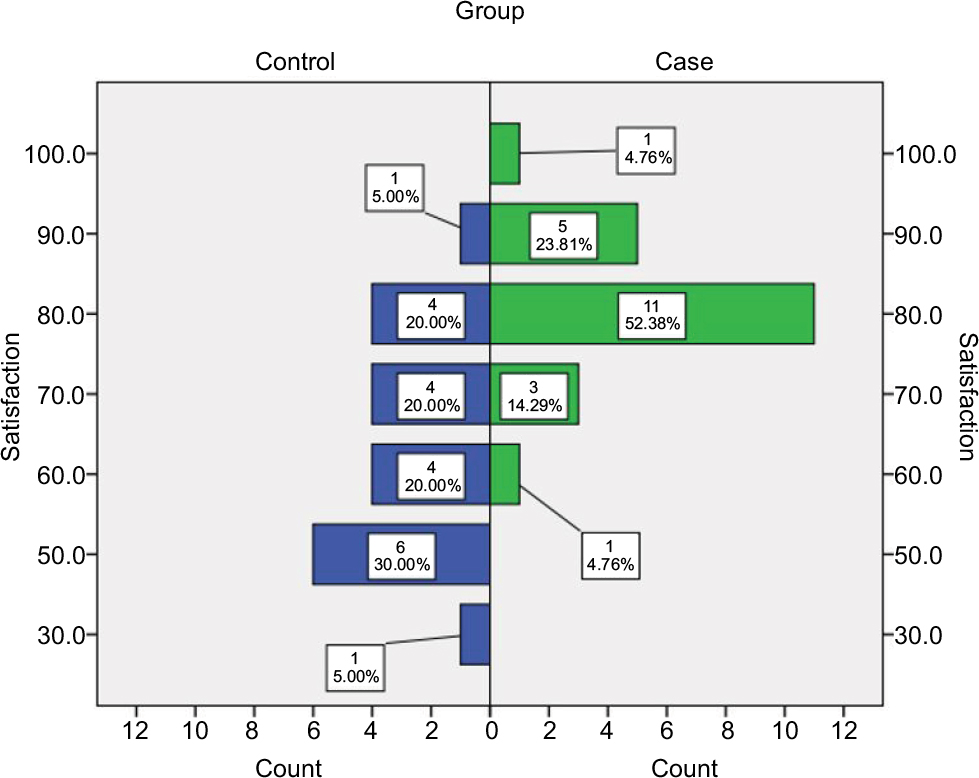 | Figure 2 Comparison of patient satisfaction between the two groups. |
Discussion
Recently, attention has been drawn to the application of BF methods in rehabilitation interventions, and gradually it has been accepted as an effective measure to decrease pain and increase efficacy of the main treatments.30,31 Regarding the effects of this method in patients with knee OA, some studies have shown its positive effects on pain relief and improvements in function and muscle strength in patients treated with exercise plus EMGBF, while others have found this method to provide no additional effects on patients.32 Considering the significant differences in the results of previous studies on this subject, lack of such evaluation on a sample of Iranian patients, the rising prevalence of this chronic disease, and the declining preference of patients for using medications and surgical interventions, the present trial was designed to assess the effects of EMGBF on voluntary VMO muscle activity, pain, function, and VMO muscle thickness in patients with knee OA when this method is used in isometric exercise of quadriceps muscles in these patients.
Based on the results, none of the outcome measures – pain, stiffness, function total scores of WOMAC questionnaire, pain, walking ability, function, total score of Lequesne questionnaire, or electrical activity of the muscle – was significantly different between the two groups before or after interventions. The changes in all these parameters after interventions were found to be statistically significant in both groups; however, changes were not significantly different between the two. Regarding VMO muscle thickness, changes in each group after interventions were found to be insignificant. The only variable for which changes were found to be significantly greater in the EMGBF group compared to the control group was VAS score. Patients in the EMGBF group were also found to be more satisfied with the treatments compared to the subjects in the control group.
Since improvements in none of the objective measures evaluated in these patients was found to be significantly greater in the EMGBF group compared to the control group, it seems that the greater improvements observed in the subjective measures of VAS score and patient satisfaction with treatment in the EMGBF group might be due to the psychological effects of the EMGBF method. Choi et al evaluated the effects of isometric exercise using USBF and EMGBF on MVIC, pain, and muscle thickness in patients with knee OA. Patients were recruited and randomly assigned to three groups: EMGBF, USBF, and control groups. Subjects in the control group were treated with conventional physical therapies, such as hot pack, US, and transcutaneous electrical nerve stimulation. Subjects in each group were trained or treated for 20 minutes three times a week for 8 weeks. MVIC in the EMGBF and USBF training groups was significantly increased compared with that in the control group, and the VAS score (for measurement of pain) in the EMGBF and USBF training groups was significantly decreased compared with that in the control group. Only the EMGBF training group showed significantly increased VMO thickness compared with before training.33 The results of that study are against our finding that VMO thickness did not change by EMGBF. This may be attributed to the different method of measuring VMO thickness applied in Choi et al.
As mentioned, previous studies have reported incongruent results. For instance, Nitz et al assessed the effects of EMGBF accompanied by strengthening exercises of the quadriceps muscles in patients with knee OA in 1983 and found this method to have no significant effect on the muscle strength of the patients.23 In another clinical trial conducted in 2010, Yilmaz et al assessed the effects of EMGBF on 40 patients with knee OA randomly assigned to two groups of controls undergoing classic exercises and cases undergoing the same exercises accompanied by EMGBF. The severity of knee pain, function, and muscle strength were found to be improved significantly in both groups, and there were no significant differences between the two groups.32 As such, the findings of these two studies were in line with the results of the present survey.
A systematic review by Wasielewski et al in 2011 also aimed to determine the effect of EMGBF on quadriceps muscles. They included eight clinical trials with 319 patients, 90 of which were patients with knee OA. Based on the findings of this study, EMGBF exerted positive short-term effects on pain and muscle strength among patients with acute problems, but was ineffective in patients with chronic conditions, including patellofemoral syndrome and knee OA.34 As such, the results of our study were compatible with the findings of this systematic review too.
On the other hand, in a study in 2011, Anwer et al evaluated the effects of EMGBF on the strength of quadriceps muscles in 33 patients with knee OA who were randomly assigned to two groups of control with 16 subjects and BF with 17 patients, and after 5 weeks of exercise with/without BF, found the maximum isometric strength of the quadriceps muscles to be significantly greater in the BF group compared to the control group (P=0.004).35 This is one of the studies whose findings were incompatible with ours. Lepley et al also conducted a systematic review in 2012 in which they showed that EMGBF had significant effects on the isometric strength of quadriceps muscles, but these authors did not limit their inclusion criteria to patients with knee OA.36 In a study by Dursun et al, EMGBF treatment did not lead to further clinical improvement in comparison with a conventional exercise program in patients with patellofemoral pain syndrome.37
It seems that all these related studies agree on the significant improvements in symptoms and function of patients treated with exercise accompanied by EMGBF; however, they disagree on whether these improvements are significantly different to that of exercise therapy without EMGBF. One of the sources of this discrepancy between the results of these studies could be observation bias, as in many of these trials, patients in the control group followed the exercise schedules at their homes, while subjects in the EMGBF group performed the exercises under direct supervision of the physicians. This issue was resolved in our study, as all our patients went through the same process for their exercises, and in patients of the control group, only the active electrode was not attached. Direct observation of patients in both groups ensured that all patients were performing the exercises, and this might be the reason that both groups gained almost the same results. One of the main limitations of the present study was patients declining our invitation to participate in our study. To resolve this problem, the aims and methods of the study and its importance were thoroughly explained to the patients, and they were encouraged to participate by a tutorial display of the exercise with EMGBF. Patients’ noncompliance with the exercise without BF program was another issue that we tried to overcome by contacting subjects before their upcoming exercise sessions and encouraging them to continue their participation.
Another shortcoming of this study was the evaluation of VMO with surface EMG. If we aim to evaluate the effect of EMGBF on VMO strength, the best device to do so is a dynamometer. Unfortunately at the time of this study, we did not have access to a dynamometer specifically designed to measure VMO strength. It is suggested that in further studies, tools other than the same surface EMG used for EMGBF be used to measure VMO strength. In addition to that, we suggest using other types of BF devices in future studies that work with pressure instead of electrical activity of muscles to help patients better activate the whole quadriceps complex and to evaluate its effect on pain and function of patients with knee OA. Due to the limited resources of this trial, a limited number of patients were included, and they were followed for only 2 months. In our study, VMO muscle thickness evaluated by sonographic examination did not change significantly in either of the two groups. This can be attributed to short-term follow-up. Long-term strengthening exercises of quadriceps muscle may lead to significant increases in muscle thickness than can be evaluated by sonographic examinations. However, as a highly sensitive imaging modality, magnetic resonance imaging may be helpful in detecting muscle thickness changes in this setting. In order to reach a consensus on the effects of EMGBF in conservative management of patients with knee OA, it is suggested that further investigations be conducted with larger samples, longer follow-up periods, and direct monitoring of patients’ exercise sessions.
Conclusion
Despite significant improvements in knee pain, joint stiffness, and function of patients with knee OA treated with isometric exercises accompanied by EMGBF, the effects of this method did not significantly exceed those of exercise without BF. This study highlights again the importance of quadriceps strengthening exercises in improving pain and function in patients with knee OA. The compliance of the patients with exercise and their motivation increased when EMGBF was accompanied by exercises, and as we know in elderly patients, it is very important to keep them motivated to adhere to their exercise program. One of the main purposes of rehabilitation in patients with knee OA is the reduction of pain, and as mentioned before, at least patients subjectively feel less pain when EMGBF is used. In conclusion, using EMGBF can have some advantages, and the judgment whether to use EMGBF or not is dependent on its availability, cost-effectiveness, and physician–patient preference.
Acknowledgments
An abstract of this paper has been previously published38 and was presented as a poster at the Annual European Congress of Rheumatology June 13–16, 2018; Amsterdam, the Netherlands. This article was extracted from the thesis written by Dr Zeynab Bossaghzade at the School of Medicine, Shahid Beheshti University of Medical Sciences (registration number 277). The authors would like to thank Mrs Mehrnaz Mehrabi as the coordinator of the Clinical Research Development Center of Shahid Modarres Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
Guccione AA, Felson DT, Anderson JJ, et al. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am J Public Health. 1994;84(3):351–358. | ||
Cross M, Smith E, Hoy D, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1323–1330. | ||
Raeissadat SA, Tabibian E, Rayegani SM, Rahimi-Dehgolan S, Babaei-Ghazani A. An inestigation into the efficacy of intra-articular ozone (O2-O3) injection in patients with knee osteoarthritis: a systematic review and meta-analysis. J Pain Res. In press 2018. | ||
Raeissadat SA, Rayegani SM, Forogh B, Hassan Abadi P, Moridnia M, Rahimi Dehgolan S. Intra-articular ozone or hyaluronic acid injection: which one is superior in patients with knee osteoarthritis? A 6-month randomized clinical trial. J Pain Res. 2018;11:111–117. | ||
Raeissadat SA, Babaee M, Rayegani SM, et al. An overview of platelet products (PRP, PRGF, PRF, etc.) in the Iranian studies. Future Sci OA. 2017;3(4):FSO231. | ||
Raeissadat SA, Rayegani SM, Ahangar AG, Abadi PH, Mojgani P, Ahangar OG. Efficacy of intra-articular Injection of a newly developed plasma rich in growth factor (PRGF) versus hyaluronic acid on pain and function of patients with knee osteoarthritis: a single-blinded randomized clinical trial. Clin Med Insights Arthritis Musculoskelet Disord. 2017;10:1179544117733452. | ||
Raeissadat SA, Rayegani SM, Hassanabadi H, et al. Knee osteoarthritis injection choices: platelet-rich plasma (PRP) versus hyaluronic acid (a one-year randomized clinical trial). Clin Med Insights Arthritis Musculoskelet Disord. 2015;8:CMAMD.S17894. | ||
Rayegani SM, Raeissadat SA, Heidari S, Moradi-Joo M. Safety and effectiveness of low-level laser therapy in patients with knee osteoarthritis: a systematic review and meta-analysis. J Lasers Med Sci. 2017;8(Suppl 1):S12–S19. | ||
Richards R, van den Noort JC, Dekker J, Harlaar J. Gait retraining with real-time biofeedback to reduce knee adduction moment: systematic review of effects and methods used. Arch Phys Med Rehabil. 2017;98(1):137–150. | ||
Demura T, Demura S, Uchiyama M, Sugiura H. Examination of factors affecting gait properties in healthy older adults: focusing on knee extension strength, visual acuity, and knee joint pain. J Geriatr Phys Ther. 2014;37(2):52–57. | ||
Sharma L, Dunlop DD, Cahue S, Song J, Hayes KW. Quadriceps strength and osteoarthritis progression in malaligned and lax knees. Ann Intern Med. 2003;138(8):613–619. | ||
Ettinger WH, Afable RF. Physical disability from knee osteoarthritis: the role of exercise as an intervention. Med Sci Sports Exerc. 1994;26(12):1435–1440. | ||
JOHANNES, W. Pain and disability in patients with osteoarthritis of hip or knee: the relationship with articular, kinesiological, and psychological characteristics. Pain. 1998;25:125–133. | ||
Wang Y, Wluka AE, Berry PA, et al. Increase in vastus medialis cross-sectional area is associated with reduced pain, cartilage loss, and joint replacement risk in knee osteoarthritis. Arthritis Rheum. 2012;64(12):3917–3925. | ||
Meier WA, Marcus RL, Dibble LE, et al. The long-term contribution of muscle activation and muscle size to quadriceps weakness following total knee arthroplasty. J Geriatr Phys Ther. 2009;32(2):35–38. | ||
Eftekhar-Sadat B, Niknejad-Hosseyni SH, Babaei-Ghazani A, Toopchizadeh V, Sadeghi H. Reliability and validity of Persian version of Western Ontario and McMaster Universities Osteoarthritis index in knee osteoarthritis. J Anal Res Clin Med. 2015;3(3):170–177. | ||
Kim H, Song CH. Comparison of the VMO/VL EMG ratio and onset timing of VMO relative to VL in subjects with and without patellofemoral pain syndrome. J Phys Ther Sci. 2012;24(12):1315–1317. | ||
Anwer S, Alghadir A. Effect of isometric quadriceps exercise on muscle strength, pain, and function in patients with knee osteoarthritis: a randomized controlled study. J Phys Ther Sci. 2014;26(5):745–748. | ||
Levitt R, Deisinger JA, Remondet Wall J, Ford L, Cassisi JE, Wall JR, Ford LOR. I. EMG feedback-assisted postoperative rehabilitation of minor arthroscopic knee surgeries. J Sports Med Phys Fitness. 1995;35(3):218–223. | ||
Ahamed NU, Sundaraj K, Ahmad RB, Nadarajah S, Shi PT, Rahman SM. Recent survey of automated rehabilitation systems using EMG biosensors. J Phys Ther Sci. 2011;23(6):945–948. | ||
Mcconnell J. The physical therapist’s approach to patellofemoral disorders. Clin Sports Med. 2002;21(3):363–387. | ||
Kirnap M, Calis M, Turgut AO, Halici M, Tuncel M. The efficacy of EMG-biofeedback training on quadriceps muscle strength in patients after arthroscopic meniscectomy. N Z Med J. 2005;118(1224):U1704. | ||
Nitz JC, Luparia L. The use of EMG biofeedback in quadriceps strengthening exercise for rheumatoid arthritis patients: a clinical trial. Aust J Physiother. 1983;29(4):127–132. | ||
Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869. | ||
Huang MH, Lin YS, Yang RC, Lee CL. A comparison of various therapeutic exercises on the functional status of patients with knee osteoarthritis. Semin Arthritis Rheum. 2003;32, (6):398–406. | ||
Cheing GL, Hui-Chan CW, Chan KM. Does four weeks of TENS and/or isometric exercise produce cumulative reduction of osteoarthritic knee pain? Clin Rehabil. 2002;16(7):749–760. | ||
Merletti R. Surface electromyography: The SENIAM project. Eur J Phys Rehab Med. 2000;36(4):167. | ||
Anwer S, Equebal A, Nezamuddin M, Kumar R, Lenka PK. Effect of gender on strength gains after isometric exercise coupled with electromyographic biofeedback in knee osteoarthritis: a preliminary study. Ann Phys Rehabil Med. 2013;56(6):434–442. | ||
Nadrian H, Moghimi N, Nadrian E, et al. Validity and reliability of the Persian versions of WOMAC Osteoarthritis Index and Lequesne Algofunctional Index. Clin Rheumatol. 2012;31(7):1097–1102. | ||
Giggins OM, Persson UM, Caulfield B. Biofeedback in rehabilitation. J Neuroeng Rehabil. 2013;10(1):60. | ||
Huang H, Wolf SL, He J. Recent developments in biofeedback for neuromotor rehabilitation. J Neuroeng Rehabil. 2006;3(1):11. | ||
Yılmaz OO, Senocak O, Sahin E, et al. Efficacy of EMG-biofeedback in knee osteoarthritis. Rheumatol Int. 2010;30(7):887–892. | ||
Choi YL, Kim BK, Hwang YP, Moon OK, Choi WS. Effects of isometric exercise using biofeedback on maximum voluntary isometric contraction, pain, and muscle thickness in patients with knee osteoarthritis. J Phys Ther Sci. 2015;27(1):149–153. | ||
Wasielewski NJ, Parker TM, Kotsko KM. Evaluation of electromyographic biofeedback for the quadriceps femoris: a systematic review. J Athl Train. 2011;46(5):543–554. | ||
Anwer S, Quddus N, Miraj M, Equebal A. Effectiveness of electromyographic biofeedback training on quadriceps muscle strength in osteoarthritis of knee. Hong Kong Physiother J. 2011;29(2):86–93. | ||
Lepley AS, Gribble PA, Pietrosimone BG. Effects of electromyographic biofeedback on quadriceps strength: a systematic review. J Strength Cond Res. 2012;26(3):873–882. | ||
Dursun N, Dursun E, Kiliç Z. Electromyographic biofeedback-controlled exercise versus conservative care for patellofemoral pain syndrome. Arch Phys Med Rehabil. 2001;82(12):1692–1695. | ||
Sedighipour L, Raeissadat SA, Rayegani SM, et al. AB0973 The efficacy of electromyographic biofeedback on pain, function and maximal thickness of vastus medialis oblique muscle in patients with knee oa; a randomised clinical trial. Annal Rheum Dis. 2018;77(Suppl 2):1610. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.