Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
The effects of single inhaler triple therapy vs single inhaler dual therapy or separate triple therapy for the management of chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials
Authors Lai CC ![]() , Chen CH, Lin CYH, Wang CY
, Chen CH, Lin CYH, Wang CY ![]() , Wang YH
, Wang YH
Received 8 January 2019
Accepted for publication 10 May 2019
Published 11 July 2019 Volume 2019:14 Pages 1539—1548
DOI https://doi.org/10.2147/COPD.S200846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chunxue Bai
Chih-Cheng Lai, 1 Cheng-Hsin Chen, 2 Charlotte Yu Hsuan Lin, 3 Cheng-Yi Wang, 2 Ya-Hui Wang 4
1Department of Intensive Care Medicine, Chi Mei Medical Center, Liouying, Tainan, Taiwan; 2Department of Internal Medicine, Cardinal Tien Hospital and School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan; 3Dornsife College of Letters, Arts and Sciences, University of Southern California, Los Angeles, CA, USA; 4Medical Research Center, Cardinal Tien Hospital and School of Medicine, College of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
Background: This study aims to compare the effects of single inhaler triple therapy comprised of inhaled corticosteroids (ICSs), long-acting β 2-agonists (LABAs), and long-acting muscarinic receptor antagonists (LAMAs) with dual therapies comprised of either LABA/LAMA, ICS/LABA or separate ICS/LABA plus LAMA triple therapy.
Methods: The Pubmed, Embase, and Cochrane databases were searched up to October 31st 2018. Only randomized controlled trials were included in the meta-analysis. The primary outcome was the rate of moderate-to-severe chronic obstructive pulmonary disease (COPD) exacerbations.
Results: Seven studies fulfilling the inclusion criteria were included in the meta-analysis. Single inhaler triple therapy was associated with a significantly lower risk of COPD exacerbation compared with LABA/LAMA (rate ratio, 0.69; 95% confidence interval [CI] 0.55 to 0.87, I 2=85%), and ICS/LABA (rate ratio, 0.81; 95% CI 0.73 to 0.89, I 2=29%) dual therapy. Single inhaler triple therapy led to a more significant improvement in lung function and quality of life compared with LABA/LAMA and ICS/LABA dual therapy. Single inhaler triple therapy was associated with a higher risk of pneumonia compared with LABA/LAMA (risk ratio, 1.38, 95% CI 1.14 to 1.67, I 2=0) dual therapy.
Conclusions: The use of single inhaler triple therapy for COPD patients can result in lower rates of moderate or severe exacerbations of COPD as well as improved lung function and quality of life compared with dual therapy with LABA/LAMA or ICS/LABA.
Keywords: COPD, triple therapy, randomized controlled trials, single inhaler
Corrigendum for this paper has been published
Introduction
Triple inhaled therapy comprised of inhaled corticosteroids (ICSs), long-acting β2-agonists (LABAs), and long-acting muscarinic receptor antagonists (LAMAs), has been recommended for chronic obstructive pulmonary disease (COPD) patients who still have clinically significant symptoms following the use of a dual inhaler with LABA plus LAMA or LABA plus ICS, and those who have a higher risk of exacerbation.1,2 Traditionally, patients receiving triple therapy need to use multiple inhalers several times a day. Typically, these patients used combined ICS/LABA in one inhaler and LAMA in another inhaler, and these inhalers may be of different types and designs.3–10 This may lead to incorrect use of the inhalers and affect the patient’s adherence to treatment.
Recently, a single inhaler containing triple therapy ICS, LABA, and LAMA has been developed as a more practical alternative, which may improve therapy compliance. At present, there are three different formulas for single inhaler triple therapy, including fluticasone furoate (FF)/umeclidinium (UMEC)/vilanterol (VI) in a once daily dry powder inhaler formulation (Trelegy Ellipta; GSK, Uxbridge, UK), extrafine beclomethasone dipropionate (BDP)/formoterol fumarate (FOR)/glycopyrronium bromide (GB) in a twice daily extra fine particle pressurized metered dose inhaler (pMDI) formulation (Trimbow; Chiesi, Parma, Italy), and budesonide (BUD)/GB/FOR in a co-suspension pMDI formulation (Aerosphere; Luton, UK, not approved).
Recently, several randomized controlled trials (RCTs) have shown that extrafine BDP/FOR/GB therapy could be associated was a lower rate of moderate-to-severe COPD exacerbations,11–13 as well as improved lung function and health-related quality of life13 compared with other treatment options. Bremner et al,14 showed that FF/UMEC/VI therapy was only better than open triple therapy (FF/VI plus UMEC) in terms of changes in lung function, health-related quality of life and safety. In contrast, Lipson et al, demonstrated that a single inhaler triple therapy with FF/UMEC/VI resulted in a lower rate of moderate or severe exacerbations and a lower rate hospitalization due to COPD, compared with dual therapy with FF/VI or UMEC/VI.15 In addition, another RCT16 showed that single inhaler therapy with FF/UMEC/VI was associated with improved lung function and health-related quality of life compared with BUD/FOR dual therapy. Ferguson et al,17 demonstrated that single inhaler triple therapy with BUD/GB/FOR could improve lung function compared with BUD/FOR dual therapy.
Although these previous RCTs11–17 provide important findings regarding the efficacy of single inhaler triple therapy for COPD patients, there were some differences among them in terms of study design, study subjects, the treatments compared, and the outcome analysis. A meta-analysis pooling the results of previous trials would be helpful to clarify these issues. Therefore, the current study performed a systematic review and meta-analysis of previous literature to determine the effect of single inhaler triple therapy with ICS/LABA/LAMA on the risk of exacerbation and other relevant outcomes in patients with COPD.
Methods
Study search and selection
To identify the clinical studies relevant to the present study, a systematic review of the literature within the PubMed, Embase, ClinicalTrials.gov, and Cochrane databases was performed until October 31st 2018 using the following search terms: LABA, LAMA, ICS, FF, UMEC, VI, BDP, formoterol, fumarate, GB, BUD, tiotropium bromide, and olodaterol. Only randomized clinical studies, which compared the clinical efficacy and adverse effects of single inhaler triple therapy, including FF/UMEC/VI, BDP/FOR/GB, and BUD/GB/FOR, with other treatment options for patients with COPD were included in the meta-analysis. The alternative treatments used for comparison included ICS/LABA and LAMA/LABA dual therapy and ICS/LABA plus LAMA separate triple therapy. Two authors (Lai CC & Wang CY) searched and examined the identified publications independently to avoid any bias. When they had a disagreement, a third author (Chen CH) discussed with them and made the final decision. Data including the year of publication, study design, site and duration, demographic characteristics of the study subjects, comparative therapy types, outcomes, and adverse events were extracted from each included study. The present study used Cochrane Risk as the bias assessment tool to assess the quality of the enrolled RCTs and the risk of bias.18
Definitions and outcomes
The primary outcome of the current study was the risk of moderate or severe COPD exacerbation. Secondary outcomes included changes in lung function from baseline in trough Forced expiratory volume in 1 s (FEV1), the change from baseline in St. George’s Respiratory Questionnaire (SGRQ), risk of COPD hospitalization, respiratory- and COPD-mortality and the risk of adverse events.
Statistical analysis
When two or more comparable studies (similar population characteristics, interventions, and outcome measures) were identified, a meta-analysis was conducted to generate a pooled estimate of the effects. Review Manager software (The Cochrane Collaboration 2008, Copenhagen) was used to develop a random-effects model and derive the pooled estimates and the associated 95% confidence intervals (CIs). The rate ratio was used to evaluate the exacerbation rates per patients per year, or during the follow-up. Risk ratios were used to estimate the dichotomous outcomes, such as death and safety. Mean differences (MDs) were used for continuous variables, such as the FEV1 and SGRQ scores.
For dichotomous outcomes, the summary risk ratios and 95% CIs were estimated; for continuous data, the summary MDs and 95% CIs were estimated. The degree of heterogeneity was evaluated with Q statistic generated from the χ2 test. The proportion of statistical heterogeneity was assessed by I2 measure. Heterogeneity was considered as significant when P-value was less than 0.10 or I2 more than 50%.
Results
Study selection and characteristics
A total of 3,037 articles were identified following the initial search; however, only seven studies,11–17 which fulfilled the inclusion criteria were included in the meta-analysis (Figure S1). In all of the studies except one,14 the risk of bias in each domain11–13,15–17 was classified as low risk (Figure S2 and S3). All of the included studies were randomized, double-blind, multicenter studies, which were designed to compare the clinical efficacy and safety of single inhaler triple therapy with other treatments for adult patients with COPD (Table 1). Three studies11–13 used BDP/FOR/GB single inhaler triple therapy, three studies14–16 used FF/UMEC/VI and one study17 used BUD/FOR/GB. Fiver studies11,13,15–17 used dual therapy with ICS/LABA or LABA/LAMA as the comparative treatments, and two studies12,14 used separate triple therapy with ICS/LABA plus LAMA as the comparative treatment. Overall, a total of 8,757 COPD patients were assigned to receive single inhaler triple therapy (Table S1). The mean age of the patients who received single inhaler triple therapy was 64.8 years, while 60.5% (n=5,295) and 29.4% (n=2,575) of the patients were ex-smokers and female, respectively. A total of 10,874 COPD patients who received alternative treatments, 6,345 received ICS/LABA dual therapy, 3,463 received LABA/LAMA dual therapy, and 1,066 received ICS/LABA plus LAMA separate triple therapy. The mean age of the patients receiving ICS/LABA, LABA/LAMA, and ICS/LABA plus LAMA treatment was 64.9, 65.0, and 63.3 years, respectively. The percentage of females among the patients receiving ICS/LABA, LABA/LAMA, and ICS/LABA plus LAMA treatment was 30.7%, 32.5%, and 22.9%, respectively, and the percentage of ex-smokers was 62.6%, 62.0%, and 53.3%, respectively.
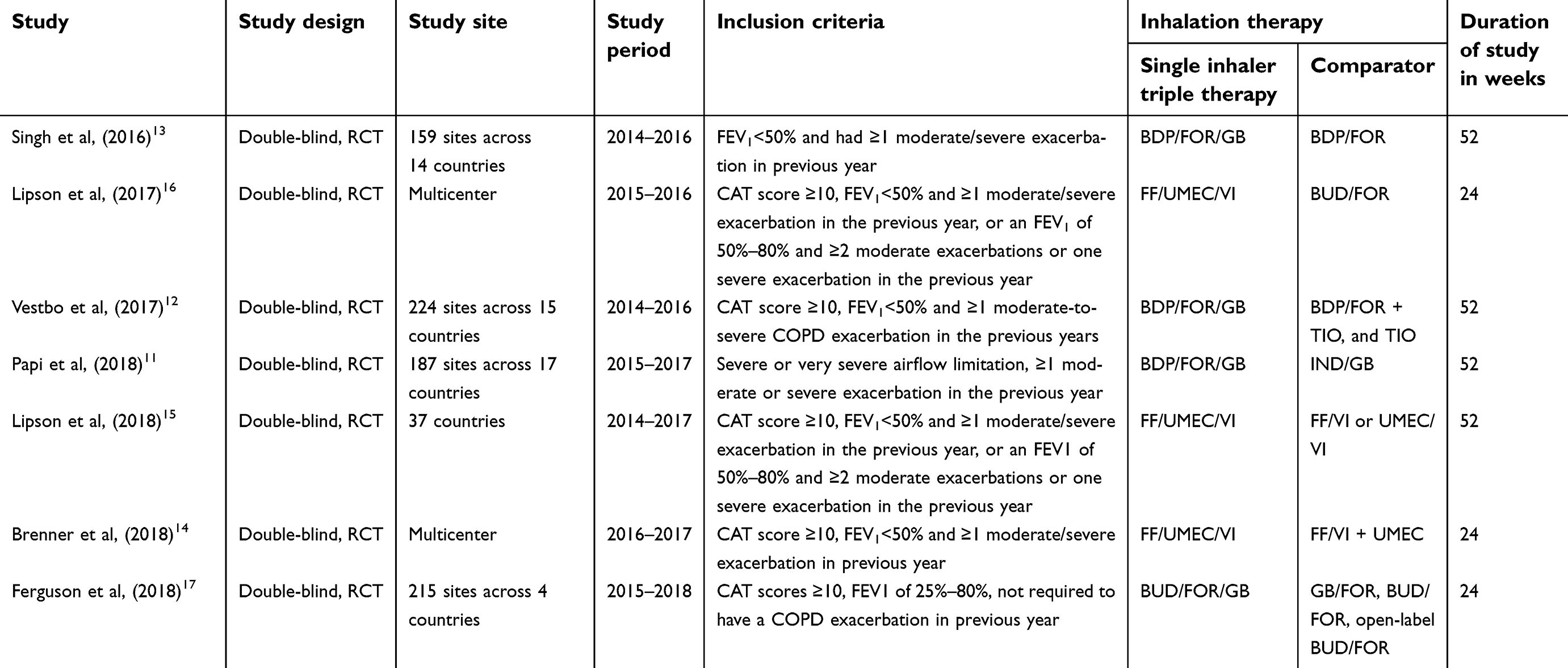 |
Table 1 Characteristics of enrolled studies |
Risk of moderate or severe COPD exacerbation
Three RCTs11,15,17 compared single inhaler triple therapy with LABA/LAMA dual therapy; it was found that single inhaler triple therapy was associated with a lower risk of COPD exacerbation compared with LABA/LAMA dual therapy (rate ratio, 0.69; 95% CI, 0.55 to 0.87, I2=85%; Figure 1). The four RCTs13,15–17 that compared single inhaler triple therapy with ICS/LABA revealed that single inhaler triple therapy could significantly reduce the risk of COPD exacerbations (rate ratio, 0.81; 95% CI, 0.73 to 0.89, I2=29%; Figure 1). Two RCTs12,14 compared single inhaler triple therapy with ICS/LABA plus LAMA separate triple therapy, however, no significant differences in the risk of moderate or severe COPD exacerbations were observed between the groups (rate ratio, 0.97; 95% CI, 0.85 to 1.10, I2=0%; Figure 1). Single inhaler triple therapy was associated with a significantly lower risk of COPD hospitalization compared with LABA/LAMA dual therapy (risk ratio, 0.68, 95% CI, 0.59 to 0.79), and ICS/LABA dual therapy (risk ratio, 0.87, 95% CI, 0.76 to 1.00; Figure S10). However, no significant differences while comparing to single inhaler triple therapy and separate triple therapy (risk ratio, 1.18; 95% CI, 0.77 to 1.81; Figure S10).
 |
Figure 1 Association of single inhaled triple with a rate of moderate or severe exacerbation. Abbreviations: IC, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic receptor antagonist. |
Secondary outcomes
Change in FEV1 was the secondary outcome of interest. Comparisons were made between single inhaler triple therapy and LABA/LAMA or ICS/LABA dual therapy and separate triple therapy in three, four, and two of the RCTs, respectively. Single inhaler triple therapy showed significant improvements in FEV1 compared with LABA/LAMA (MD, 0.03; 95% CI, 0.01 to 0.06, I2=72%) and ICS/LABA (MD, 0.10; 95% CI, 0.06 to 0.14, I2=94%) dual treatment. In contrast, no significant differences in FEV1 were noted between single inhaler triple therapy and separate triple therapy (MD, 0.01; 95% CI, −0.01 to 0.03, I2=0%; Figure 2).
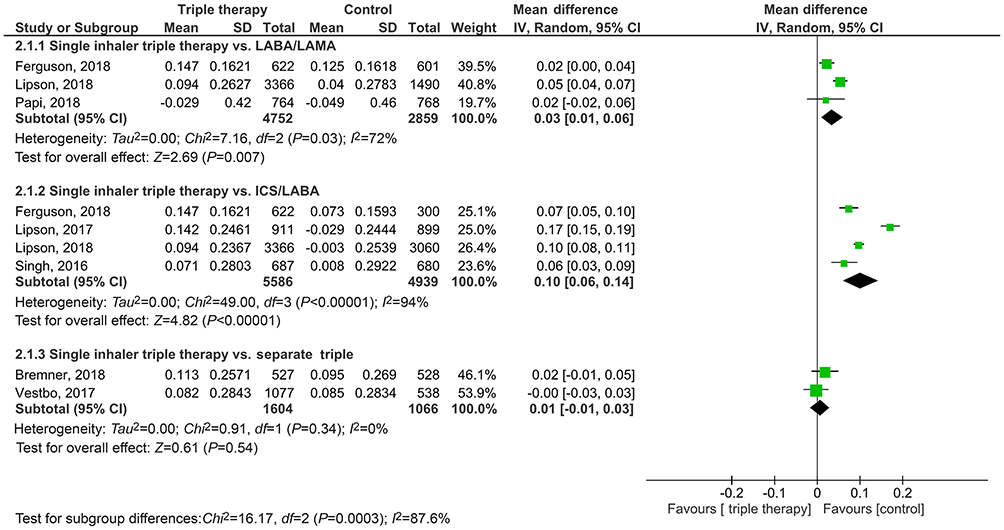 |
Figure 2 Association of single inhaled triple therapy with change of FEV1. Abbreviations: IC, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic receptor antagonist. |
Improvements in quality of life were determined using SGQR scores. Patients taking single inhaler triple therapy reported significantly higher improvements in quality of life compared with those taking LABA/LAMA dual therapy (MD, −1.59; 95% CI, −2.22 to −0.96, I2=0%)11,15,17 and ICS/LABA dual therapy (MD, −153; 95% CI, −2.23 to −0.84, I2=21%; Figure 3).13,15–17 In contrast, no significant differences were noted between the quality of life scores of patients taking single inhaler triple therapy and separate triple therapy (MD, 0.55; 95% CI, −2.19 to 3.29, I2=87%).12,14 A similar trend was observed in terms of SGQR responders which was defined as decrease from baseline in total score ≥4 (vs LABA/LAMA, risk ratio, 1.09; 95% CI, 1.03 to 1.15, I2=0%; vs ICS/LABA, risk ratio, 1.19; 95% CI, 1.10 to 1.28, I2=52%; vs separate triple therapy, risk ratio, 0.94; 95% CI, 0.87 to 1.01, I2=0%; Figure S5).
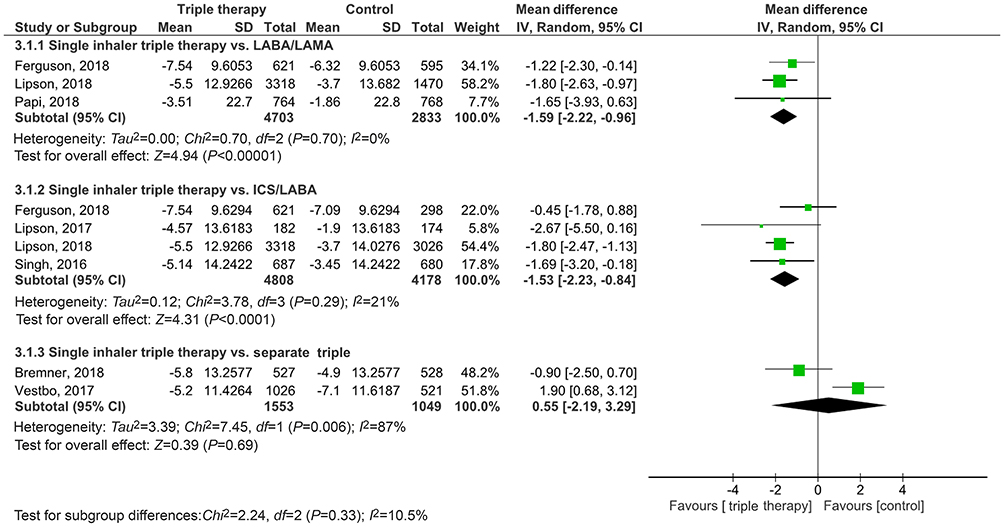 |
Figure 3 Association of single inhaler triple therapy with change of St. George’s Respiratory Questionnaire (SGRQ). Abbreviations: IC, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic receptor antagonist. |
In terms of overall mortality, no significant differences were found between single inhaler triple therapy and the other treatment options (vs LABA/LAMA, risk ratio, 0.99; 95% CI, 0.44 to 2.27, I2=31%; vs ICS/LABA, risk ratio, 1.00; 95% CI, 0.53 to 1.89, I2=0%; vs separate triple therapy, risk ratio, 0.48; 95% CI, 0.18 to 1.28, I2=49%; Figure S6). For respiratory mortality (Figure S7) and COPD mortality (Figure S8), there was also no significant difference between single inhaler triple therapy and the other treatment options.
Adverse events
Single inhaler triple therapy was associated with a significantly higher risk of pneumonia compared with LABA/LAMA dual therapy (risk ratio, 1.38, 95% CI, 1.14 to 1.67, I2=0), but no significant differences were found when it was compared with ICS/LABA dual therapy (risk ratio, 1.24, 95% CI, 0.83 to 1.85, I2=48) or separate triple therapy (risk ratio, 0.88, 95% CI, 0.51 to 1.52, I2=25; Figure 4). The risk of lower respiratory tract infection (LRTI) was investigated however, no significant differences were found between single inhaler triple therapy and the three alternative treatments (vs LABA/LAMA, risk ratio, 0.90; 95% CI, 0.73 to 1.11, I2=0%; vs ICS/LABA, risk ratio, 1.02; 95% CI, 0.85 to 1.23, I2=0%; vs separate triple therapy, risk ratio, 0.91; 95% CI, 0.37 to 2.26, I2=84%; Figure S9). In addition, there were no significant differences observed between single inhaler triple therapy and the comparative treatments in regard to the risk of treatment emergent adverse events, serious adverse events, and cardiovascular events (Figures S10–12). In addition, there were no significant differences observed between single inhaler triple therapy and the comparative treatments in regard to the risk of treatment emergent adverse events, serious adverse events, and cardiovascular events (Figures S7–9).
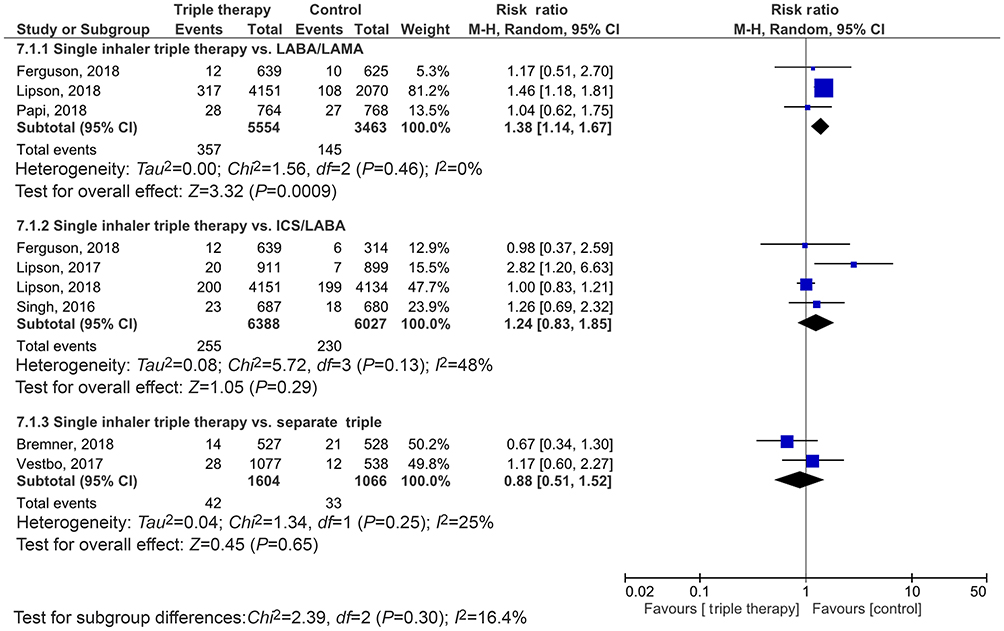 |
Figure 4 Association of single inhaler triple therapy with risk of pneumonia. Abbreviations: IC, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic receptor antagonist. |
Discussion
Guidance on the use of triple therapy with ICS/LABA and LAMA has been included in the COPD GOLD guidelines.19 The recent introduction of triple therapy with ICS/LABA/LAMA in a single inhalerprovides a convenient option for COPD patients with symptoms, which are uncontrolled by dual therapy or who are at high risk of exacerbation. Until now, few clinical trials have assessed the clinical efficacy of the single inhaler triple therapy in comparison with alternative dual therapy options or other treatments.
The present meta-analysis compared seven RCTs and identified several significant findings. It was found that single inhaler triple therapy was associated with a significantly lower risk of moderate or severe COPD exacerbations compared with dual therapy (ICS/LABA or LABA/LAMA). In addition, single inhaler triple therapy can provide additional benefits in terms of changes in FEV1 and SGQR compared with dual therapy. However, single inhaler triple therapy did not improve the overall mortality when compared with dual therapy. These findings are consistent with other recent meta-analyses.20,21 Zheng et al, revealed that triple therapy was associated with significantly lower rates of moderate or severe exacerbations compared with dual therapy with LABA/LAMA (RR, 0.78, 95% CI, 0.70 to 0.88) and ICS/LABA (risk ratio 0.77, 95% CI, 0.66 to 0.91), while the trough FEV1 and SGQR scores were favorable for triple therapy. Cazzola et al,21 reported that ICS/LABA/LAMA triple therapy reduced the risk of exacerbation (relative risk: 0.70, 95% CI 0.53–0.94) and improved trough FEV1 (MD, mL: +37.94, 95% CI 18.83 to 53.89) compared with LABA/LAMA dual therapy.
However, the triple therapies that were compared with dual therapies in these other meta-analyses20,21 included a mix of single inhaler triple therapy and separate triple therapies. Therefore, the effect of single inhaler triple therapy on the outcomes of advanced COPD patients remains unclear; this was the focus of the present study. Overall, the results of the present study suggest that the use of single inhaler triple therapy can help patients with advanced COPD achieve lower rates of moderate or severe exacerbations, as well as better lung function and improved quality of life compared with LABA/LAMA or ICS/LAMA dual therapy.
The current study found that single inhaler triple therapy carried a higher risk of pneumonia compared with LABA/LAMA dual therapy. However, there were no significant differences observed for the risk of pneumonia between single inhaler triple therapy and ICS/LABA dual therapy or separate triple therapy. This finding is consistent with a previous study,20 which reported a higher risk of pneumonia among triple therapy patients compared with LABA/LAMA dual therapy patients (relative risk, 1.53, 95% CI 1.25 to 1.87). These findings could be explained by the effect of ICS on the risk of pneumonia; it was demonstrated in the UPLIFT study22 that incidence rates of pneumonia were significantly higher in COPD patients taking ICS compared with those not taking ICS (0.068 vs 0.056, respectively; P=0.012). A meta-analysis by Horiata et al,23 also showed that LAMA/LABA dual therapy was associated with a significantly lower rate of pneumonia compared with LABA/ICS dual therapy (OR 0.57, 95% CI 0.42 to 0.79, P=0.0006, I2=0%).
It was found that the effect of triple therapy (ICS/LABA/LAMA) on the risk of pneumonia may vary according to the different ICSs administered in the different studies.11,15,17 The significant differences observed in the present meta-analysis may be attributed to the study by Lipson et al15. Among the three included studies,11,15,17 that compared triple therapy and LABA/LAMA dual therapy, a significant difference in the risk of pneumonia was only found in the study by Lipson et al15 who used FF as the ICS (risk ratio, 1.46, 95% CI, 1.18 to 1.81). No significant differences were observed in the study by Papi et al11 who used beclomethasone (risk ratio, 1.04, 95% CI, 0.62–1.75) or Ferguson et al17 who used BUD (risk ratio, 1.17, 95% CI, 0.51–2.70) as the ICS. The rate of pneumonia was much higher in the study by Lipson et al, (8%, 317/4181) compared with Papi et al, (2%, 18/764) and Ferguson et al (1.88%, 12/639). These findings suggest that using FF as an ICS in triple therapy may be associated with a higher risk of pneumonia. However, these data should be interpreted carefully due to the baseline COPD severity for the different studies, as well as age and other characteristics were wildly different in various studies. Lipson et al’s study15 enrolled high risk 2011 GOLD D COPD patients, all of whom has 2+ prior year exacerbations or 1+ prior year exacerbation if FEV1 was <50%. These were much more severe patients, older, frailer, and at higher risk of pneumonia than the patients enrolled by Ferguson et al,17 who enrolled 2011 GOLD B patients, with some 80% having no prior year exacerbations. Therefore, FF was doses in an older, sicker population for a year (the IMPACT population),15 while BUD was tested in younger, healthier patients for five and a half months in the KRONOS population).17 Further study is warranted to clarify this issue.
No significant differences were found between triple therapy in a single inhaler and separate inhalers in terms of all outcomes, including the rate of COPD exacerbation, changes in lung function and quality of life, and the risk of pneumonia and LRTIs. The similar effects observed between the two treatments are understandable as the medication and dosage used for triple therapy in a single inhaler and in separate inhalers are similar. However, all of the findings from the present analysis were extracted from enrolled RCTs, and patients in RCTs may follow the study design for inhaler use more accurately than can be expected in a real-life setting. Patients in the real world tend to have higher compliance when they use a single inhaler containing triple therapy compared with using multiple inhalers.23 Further investigation is warranted to compare the efficacy of triple therapy in a single inhaler and separate inhalers in the real world.
A major strength of the present meta-analysis was that only RCTs with a low risk of bias were included, and all of the studies had been published in the last three years. However, the present study also had several limitations. Although most of the studies only enrolled patients with FEV1<50% and a previous history of COPD exacerbations, some of the studies did not. In addition, the patients included in the analysis used different LAMA/LABA and ICS from different devices and in different dosing regimens. Moreover, the number of enrolled RCTs were limited in this meta-analysis, particularly because each had unique treatment arm comparisons (a few vs components only two trials vs open triples), and the head-to-head trials open vs single inhaler triple were limited to just over 1,000 patients. All these factors may affect the heterogeneity of the meta-analysis.
Conclusions
The current meta-analysis indicated that the use of single inhaler triple therapy for COPD patients can result in a lower rate of moderate or severe exacerbations of COPD, as well as improved lung function and quality of life compared with LABA/LAMA or ICS/LABA dual therapy. However, triple therapy did not reduce the patient’s overall mortality. In addition, they may increase their risk of pneumonia in comparison with LABA/LAMA dual therapy. The outcomes of the COPD patients were not affected by whether the triple therapy was administered in a single or separate inhalers.
Acknowledgment
This study was supported by grants from Cardinal Tien Hospital (CTH-104-1-2C01 and CTH-104-1-2A08).
Author contributions
CYW and CCL assessed the eligibility of studies for inclusion in the meta-analysis. CCL, CHC, CYHL, CYW, and YHW were all directly involved in the acquisition of data for analysis. All statistical analyses were performed by YHW. CCL and CYW wrote the first draft of the manuscript. All authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the manuscript, ensuring that questions related to the accuracy or integrity of any part of the manuscript were appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lipworth B, Jabbal S. A pragmatic approach to simplify inhaler therapy for COPD. Lancet Respir Med. 2017;5:679–681. doi:10.1016/S2213-2600(17)30264-3
2. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi:10.1164/rccm.201701-0218PP
3. Frith PA, Thompson PJ, Ratnavadivel R, et al. Glycopyrronium once-daily significantly improves lung function and health status when combined with salmeterol/fluticasone in patients with COPD: the GLISTEN study, a randomised controlled trial. Thorax. 2015;70:519–527. doi:10.1136/thoraxjnl-2014-206670
4. Maltais F, Mahler DA, Pepin V, et al. Effect of fluticasone propionate/salmeterol plus tiotropium versus tiotropium on walking endurance in COPD. Eur Respir J. 2013;42:539–541. doi:10.1183/09031936.00074113
5. Lee SD, Xie CM, Yunus F, et al. Efficacy and tolerability of budesonide/formoterol added to tiotropium compared with tiotropium alone in patients with severe or very severe COPD: a randomized, multicentre study in East Asia. Respirology. 2016;21:119–127. doi:10.1111/resp.12646
6. Jung KS, Park HY, Park SY, et al. Comparison of tiotropium plus fluticasone propionate/salmeterol with tiotropium in COPD: a randomized controlled study. Respir Med. 2012;106:382–389. doi:10.1016/j.rmed.2011.09.004
7. Hoshino M, Ohtawa J. Effects of adding salmeterol/fluticasone propionate to tiotropium on airway dimensions in patients with chronic obstructive pulmonary disease. Respirology. 2011;16:95–101. doi:10.1111/j.1440-1843.2010.01869.x
8. Hoshino M, Ohtawa J. Effects of tiotropium and salmeterol/fluticasone propionate on airway wall thickness in chronic obstructive pulmonary disease. Respiration. 2013;86:280–287. doi:10.1159/000351116
9. Hanania NA, Crater GD, Morris AN, et al. Benefits of adding fluticasone propionate/salmeterol to tiotropium in moderate to severe COPD. Respir Med. 2012;106:91–101. doi:10.1016/j.rmed.2011.09.002
10. Cazzola M, Ando F, Santus P, et al. A pilot study to assess the effects of combining fluticasone propionate/salmeterol and tiotropium on the airflow obstruction of patients with severe-to-very severe COPD. Pulm Pharmacol Ther. 2007;20:556–561. doi:10.1016/j.pupt.2006.06.001
11. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391:1076–1084. doi:10.1016/S0140-6736(18)30206-X
12. Vestbo J, Papi A, Corradi M, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet. 2017;389:1919–1929. doi:10.1016/S0140-6736(17)30188-5
13. Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting beta2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388:963–973. doi:10.1016/S0140-6736(16)31354-X
14. Bremner PR, Birk R, Brealey N, et al. Single-inhaler fluticasone furoate/umeclidinium/vilanterol versus fluticasone furoate/vilanterol plus umeclidinium using two inhalers for chronic obstructive pulmonary disease: a randomized non-inferiority study. Respir Res. 2018;19:19. doi:10.1186/s12931-018-0724-0
15. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378:1671–1680. doi:10.1056/NEJMoa1713901
16. Lipson DA, Barnacle H, Birk R, et al. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196:438–446. doi:10.1164/rccm.201703-0449OC
17. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. Lancet Respir Med. 2018;6:747–758. doi:10.1016/S2213-2600(18)30327-8
18. Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj. 2011;343:d5928. doi:10.1136/bmj.d5928
19. GOLD. Global Strategy for the diagnosis, management and prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2018; 2018. Available from: https://goldcoped.org/.
20. Zheng Y, Zhu J, Liu Y, et al. Triple therapy in the management of chronic obstructive pulmonary disease: systematic review and meta-analysis. Bmj. 2018;363:k4388. doi:10.1136/bmj.k4029
21. Cazzola M, Rogliani P, Calzetta L, et al. Triple therapy versus single and dual long-acting bronchodilator therapy in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Eur Respir J. 2018. doi:10.1183/13993003.01586-2018
22. Morjaria JB, Rigby A, Morice AH. Inhaled corticosteroid use and the risk of pneumonia and COPD exacerbations in the UPLIFT study. Lung. 2017;195:281–288. doi:10.1007/s00408-017-9990-8
23. Singh D, Corradi M, Spinola M, et al. Triple therapy in COPD: new evidence with the extrafine fixed combination of beclomethasone dipropionate, formoterol fumarate, and glycopyrronium bromide. Int J Chron Obstruct Pulmon Dis. 2017;12:2917–2928. doi:10.2147/COPD.S146822
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.