")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Effects of Self-Criticism and Self-Compassion on Adolescents’ Depressive Symptoms and Nonsuicidal Self-Injury
Authors Gao Y, Liu X , Liu J, Wang H
Received 14 April 2023
Accepted for publication 1 August 2023
Published 11 August 2023 Volume 2023:16 Pages 3219—3230
DOI https://doi.org/10.2147/PRBM.S417258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Yemiao Gao, Xia Liu, Jinmeng Liu, Hui Wang
Institute of Developmental Psychology, Faculty of Psychology, Beijing Normal University, Beijing, People’s Republic of China
Correspondence: Xia Liu, Institute of Developmental Psychology, Faculty of Psychology, Beijing Normal University, No. 19 Xinjiekouwai Street, Beijing, People’s Republic of China, Tel/Fax + 86 10 58806819, Email [email protected]
Purpose: Symptoms of depression increase during adolescence as do nonsuicidal self-injurious behaviors (NSSI). The present study aimed to investigate how self-criticism interacted with the effects of stressful life events on depressive symptoms and NSSI and whether self-compassion would buffer these negative effects.
Methods: A total of 908 Chinese adolescents (Mage = 13.46, SD = 0.57) completed a cross-sectional survey. The main and interacted effects of stressful life events, self-criticism, self-compassion on depressive symptoms and NSSI were examined respectively.
Results: The results showed that self-criticism significantly moderated the relationships between stressful events and depression and NSSI. Self-compassion could buffer the negative impacts of stressful events and self-criticism on NSSI but not on depression. High self-compassion significantly reduced the magnitude of the association between stressful life events and NSSI in adolescents with low self-criticism but not in those with high self-criticism.
Conclusion: Self-criticism exacerbated the negative impacts of stressful life events on both depressive symptoms and NSSI, but self-compassion only buffered the impact of stressful life events on NSSI. Interventions designed to reduce NSSI risk of Chinese adolescents may benefit from training them to improve self-compassion abilities and to be less self-critical.
Keywords: stressful life events, self-criticism, self-compassion, nonsuicidal self-injury, depressive symptoms
Introduction
Adolescence is a period marked by heightened risk for psychological and behavioral problems, including depression and nonsuicidal self-injury (NSSI). There is substantial evidence that depressive symptoms increase during adolescence.1 NSSI, a typically correlated but distinct behavior, is also a concern among adolescents.2 Defined as “the deliberate, self-inflicted damage of body tissue without suicidal intent and for purposes not socially or culturally sanctioned”,3 NSSI has become prevalent among adolescents in the community. The rates of lifetime NSSI in the adolescent population worldwide were as high as 22.9%, and the prevalence of NSSI in the past 12 months was approximately 18.6%.4 In recent years, researchers have started to study NSSI with depression conjointly due to their cooccurrence.5–7 However, there is a lack of clarity regarding the common and differential pathways to depressive symptoms and NSSI. In this study, we focused on how the common predictors of depressive symptoms and NSSI (ie, stressful life events, self-criticism, and self-compassion) jointly influence these problems and how the effects of these predictors vary.
Life stress is one of the most studied components of theories of depressive symptoms and NSSI. For example, both the diathesis-stress model8 and evolutionary theories9 of depression imply that life stress plays a prominent role in the development of depressive symptoms. According to several theoretical conceptualizations of NSSI, stressful life events may function as proximal predictors of this behavior.10,11 Those who encounter life stress are more likely to engage in NSSI to escape from unwanted emotional experiences, punish themselves, or cope with interpersonal problems (eg, NSSI elicits attention or facilitates escape from undesired social situations).11,12
However, not all adolescents with stressful experiences develop mental health problems equally. Whether stressful life events trigger adolescents’ depressive symptoms or self-injurious behavior depends on their sensitivity to stress. Self-criticism, a cognitive-personality vulnerability characterized by the tendency to constantly scrutinize and evaluate one’s performance in an overly harsh way, a sense of inferiority, self-directed anger, and hatred,13,14 has been found to be a common hallmark of depression and NSSI.15,16 According to the Benefit and Barrier Model of NSSI,17 self-criticism is linked to increased self-punishment desires and degraded positive views of oneself, which not only removes an important barrier to self-harm but also motivates individuals to directly choose self-harm over other coping behaviors.
Under adverse conditions, self-criticism can stimulate the threat system, eliciting feelings of anger and hatred with the self.18 Individuals who are fearful of experiencing and expressing these negative self-directed emotions may be more likely to feel depressed and hurt themselves.19 Of note, despite the common co-occurrence of NSSI and depressive symptoms,5,6 self-criticism may not have as strong an influence on NSSI as it does on depression, as NSSI serves various functions and there are many other barriers to NSSI that prevent negative emotions from manifesting as self-injurious behaviors.17 These factors may interact with self-criticism to contribute to NSSI. Empirically, while self-criticism has been shown to directly predict adolescent NSSI20,21 or in interaction with stressors,7 other studies reveals that self-criticism does not predict NSSI in adolescents.22,23 This variability suggests that self-criticism might trigger NSSI under certain conditions, emphasizing the importance of considering other factor in understanding the relationship between self-criticism, stressors, and NSSI in adolescents.
Despite the negative influence of self-criticism under stressful circumstances, individuals’ resilience factors are crucial for coping with stressful life events. Defined as an emotionally positive attitude toward oneself that helps protect against negative psychological outcomes, self-compassion has been suggested to bring insight into individual differences in response to stress.24 Self-compassion includes three aspects: self-kindness (being careful and understanding the self when confronted with difficult times), common humanity (recognizing one’s suffering, failures, and stress as a normal part of the human experience), and mindfulness (having a balanced awareness of negative thoughts and feelings without overidentification).25
From the perspective of emotion regulation, the existing literature has suggested that self-compassion may promote adaptive cognitive regulation of emotions and give rise to awareness and acceptance of negative situations.26,27 Additionally, self-compassion is negatively associated with maladaptive emotion regulation strategies related to depression and NSSI, such as experiential avoidance and rumination, in stress coping processes.26,28,29 Self-compassion is more than an absence of self-criticism.30 Rather, it is associated a soothing system of affect regulation which contributes to well-being and contentment.31,32 According to Gilbert’s theoretical work, there are three affect regulation systems (drive system, threat system, and soothing system) that interact with each other.31,32 Self-compassion may be seen as an adaptive affect regulation strategy linked to the soothing system, while self-criticism is linked to the overactivation of the threat system. Empirical research also provides neurophysiological evidence that the processes of self-criticism and self-compassion/reassuring are associated with different brain regions.33 In other words, the self-critical system can be distinct from the self-compassion/reassuring system, and self-compassion may buffer against self-criticism.14,30
Empirically, researchers have found that self-compassion or fear of compassion for self were directly associated with adolescent depression and NSSI.7,34 Evidence also shows that self-compassion could buffer the relationships between different stressors and depressive symptoms or NSSI in adolescents.7,35,36 For example, Lathren et al36 found that self-compassion significantly attenuated the relationship between perceived stress and adolescent depressive symptoms. Self-compassion was also found to serve as a buffer against engaging in later NSSI among Chinese adolescents with experiences of peer victimization.35 Moreover, individuals high in self-compassion reported a weaker association between self-criticism and depression.37,38 While previous studies have explored the interaction of self-compassion with stress or self-criticism on psychopathology, the examination of their joint influence, particularly with respect to NSSI, is less explored. It remains unclear whether self-compassion attenuates the relationship between self-criticism and NSSI, especially in the context of stressful events. At the same time, there is inconsistent evidence indicating that neither the scores of the total scale nor the subscales of self-compassion significantly moderated the association between negative experiences and depressive symptoms among young adults.39,40 Meanwhile, previous research suggests that self-compassion and childhood abuse interact on both adolescent depression and NSSI, but with different interaction patterns.7 Whether self-compassion plays a different protective role against depressive symptoms and NSSI in adolescents experiencing stressful life events has yet to be tested. Examining the role of such modifiable protective factors will help inform us of how to better intervene to attenuate the development of depression and/or NSSI in adolescents with different levels of self-criticism.
Taken together, the current study aimed to disentangle the roles for depressive symptoms and NSSI that self-compassion may play for adolescents with different levels of self-criticism when they encounter stressful life events. First, we hypothesized that stressful life events could significantly predict both depressive symptoms and NSSI. Second, it was expected that self-criticism would intensify the relationships of stressful life events with depressive symptoms and NSSI. Third, we postulated that self-compassion would buffer the aforementioned deleterious relationships, with the more self-compassionate group showing weaker associations between stressful life events, self-criticism, and depressive symptoms or NSSI than the less self-compassionate group. Furthermore, we hypothesized that the difference in the relationship between stressful life events and depression would be greater than the relationship between stressful life events and NSSI among adolescents with different levels of self-compassion. Given the sex differences in both depression and NSSI, especially during adolescence, the current study also investigated whether different aspects of self-compassion behave differently and whether the buffering effect of self-compassion varies by sex. These analyses were exploratory due to the discrepancies in the existing literature.
Methods
Participants
Participants were recruited with the cooperation of school authorities of two middle schools located in North China. A total of 1022 healthy adolescents were invited to participant in this study, and 93.8% of them (n = 959) agreed and participated in the current study. To ensure that participants responded carefully, validity checks were done on the responses. If participants selected the same options for all items, especially for scales containing reverse scoring questions, or did not complete the survey, these participants were removed from the analysis. Among the 959 participants, 51 were excluded because they failed the validity check, so the final sample consisted of 908 adolescents (435 males, 47.9%) aged 12–16 years old (Mage = 13.46, SD = 0.57). All participants were Chinese, and over half of them were from rural areas (58.7%). The median household income of families was ¥8000 per month (approximately $1222, range = $153 to $6112), which is approximately the same as the estimated average monthly household income in China (¥8047).41 The majority of participants’ fathers (56.6%) and mothers (54.4%) have received junior middle school education.
Procedure
The school administrators were informed of the purpose of the current study. With the help of the school administrators, we invited Grade 7 and Grade 8 students from the two schools to participate in the survey. Parental informed consent and informed assent forms from students were obtained prior to the study. Participants were informed that participation was voluntary and that all the collected data were confidential. Then, participants completed the self-report questionnaires during regular school hours. The questionnaires took approximately 20–30 minutes to complete. During the assessment in each class, questionnaires were administered by the headteacher and a trained research assistant. Each participant received a gift of stationery after the survey.
Furthermore, the NSSI and depression scales used in this study also served as screening tools to identify students experiencing these problems. At the end of the study, we gave feedback to the school mental health teachers, which included an overview of the current conditions of students and educational suggestions, for guiding interventions for students. All study procedures had the approval of the Research Ethics Committee of the affiliated university.
Measures
Stressful Life Events
Stressful life events were measured with the Adolescent Self-Rating Life Events Check List (ASLEC),42 which has been widely used among Chinese adolescents.43,44 The ASLEC is a self-report questionnaire including 26 stressful life events that are common in Chinese adolescents. The participants were required to report whether the event had occurred during the past 12 months or not. If the answer is “it never happened”, a score of 0 is given. If the answer is “it happened”, participants report the impact of the events on them on a scale ranging from 1 (not at all) to 5 (extremely serious). We used the mean score of all items in the current study. A higher score indicated a greater severity of the event. In our study, Cronbach’s α = 0.91.
Self-Criticism
The Forms of Self-Criticism/Self-Reassuring Scale (FSCRS)14 was used to measure the level of self-criticism. The FSCRS consists of 22 items, with two subscales measuring levels of self-criticism (Hated Self and Inadequate Self) and one subscale measuring self-reassurance (Reassured Self) in the context of perceived failure. In the current study, only the self-criticizing subscales were employed because our aim was to investigate the negative effects of self-criticism on adolescents’ mental health problems. The subscale of Inadequate Self assesses personal thoughts about their inadequacies, and Hated Self assesses self-dislike and an aggressive desire to hurt the self. Participants completed the 14-item Hated Self and Inadequate Self subscales rated on a 5-point Likert scale. We used the mean score of all items for data analyses. Since there was not a validated Chinese version of the FSCRS, we used a team of native Chinese speakers with a background in psychology and translation to translate and back translate the English questionnaire. The two subscales have been found to have good internal consistency with Cronbach’s α of 0.92.
Self-Compassion
Self-compassion was assessed using the Chinese version of the three positive components of the Self-compassion Scale,45,46 which consisted of self-kindness (5 items, eg, “I’m tolerant of my own flaws and inadequacies.”), common humanity (4 items, eg, “I try to see my failings as part of the human condition.”), and mindfulness (4 items, eg, “When something upsets me, I try to keep my emotions in balance.”). Since the current study aimed to examine the protective effects of self-compassion against maladaptive outcomes, we only used the positive components. Participants rated on a 5-point Likert scale from 1 (not like me at all) to 5 (like me very much). A total mean score of all items was used, with a higher mean score reflecting a higher level of self-compassion. In the present study, Cronbach’s α = 0.83.
Nonsuicidal Self-Injury
Nonsuicidal self-injury was measured with the modified version of the Adolescents Self-Harm Scale (DSHS),47 which has been used in previous studies among Chinese adolescents.48 The DSHS consisted of 18 kinds of NSSI behaviors (eg, self-cutting, self-burning, intentionally scratching to the point of bleeding). Participants rated the lifetime frequency of each listed NSSI behavior on a 4-point scale ranging from 1 (never) to 4 (five times or more) and the degree of physical damage caused by the behaviour on a 5-point scale ranging from (1) no damage to (5) very severe. The sum of products of frequency and severity scores was used, with higher scores indicating higher levels of NSSI. In the current study, Cronbach’s α = 0.93.
Depressive Symptoms
Participants reported depressive symptoms by the Center for Epidemiologic Studies Depression Scale for Children (CES-DC).49 The scale included 20 items (eg, “I do not think I can concentrate on my work”). All items were measured on a 4-point Likert scale ranging from 1 (never) to 4 (always). Mean scores of all items were used, with 4 items reverse-scored. The higher score they obtained, the higher level of depressive symptoms they had. In the current study, for CES-DC, Cronbach’s α = 0.91.
Covariates
Based on existing studies,50–52 we included age, sex, and subjective socioeconomic status (SES). Subjective SES was measured with the MacArthur scale,53 in which a social ladder with 10 rungs was presented. Participants were asked to choose the rung that they think best represents where they stand in our society. A higher rung indicated a higher level of subjective SES.
Data Analyses
Before the data analyses, we conducted Harman’s single-factor test54 to determine the common method variance of the self-reported variables. The results indicated that 30 factors’ initial eigenvalues were greater than 1, and the first factor explained less than 40% (ie, 20.57%) of the total variance, which means the data did not suffer from common method bias.
We first conducted a primary analysis to calculate the descriptive statistics of the study variables and compute the correlations among them. Since the NSSI data were positively skewed (skewness > 3; kurtosis > 10), we used log transformation to improve the normality of NSSI. The transformation resulted in acceptable skewness (ie, 1.23) and kurtosis (ie, 0.26) variables for testing the proposed model. Then, to test our hypotheses, we used Model 3 of the PROCESS macro in SPSS55 to perform bias-corrected bootstrapping analyses with 2000 samples. The procedure yielded 95% bias-corrected confidence intervals (95% CI) for significance levels,55 with the exclusion of zero indicating significant effects. Finally, PROCESS automatically performed simple slope analyses if any interaction was significant and generated the data points for plotting interactions. All continuous predictors were mean-centered before entering the model. In addition, less than 5% of the data were missing. Thus, listwise deletion was used to deal with missing data.
Results
Preliminary Analyses
Descriptive analyses showed that 37.3% (n = 339) of the participants reported a history of NSSI. The means, standard deviations, and correlations of the variables in our study are presented in Table 1. It was found that depressive symptoms had a significant association with sex. Both depressive symptoms and NSSI were negatively associated with SSES and self-compassion, and positively correlated with stressful life events and self-criticism.
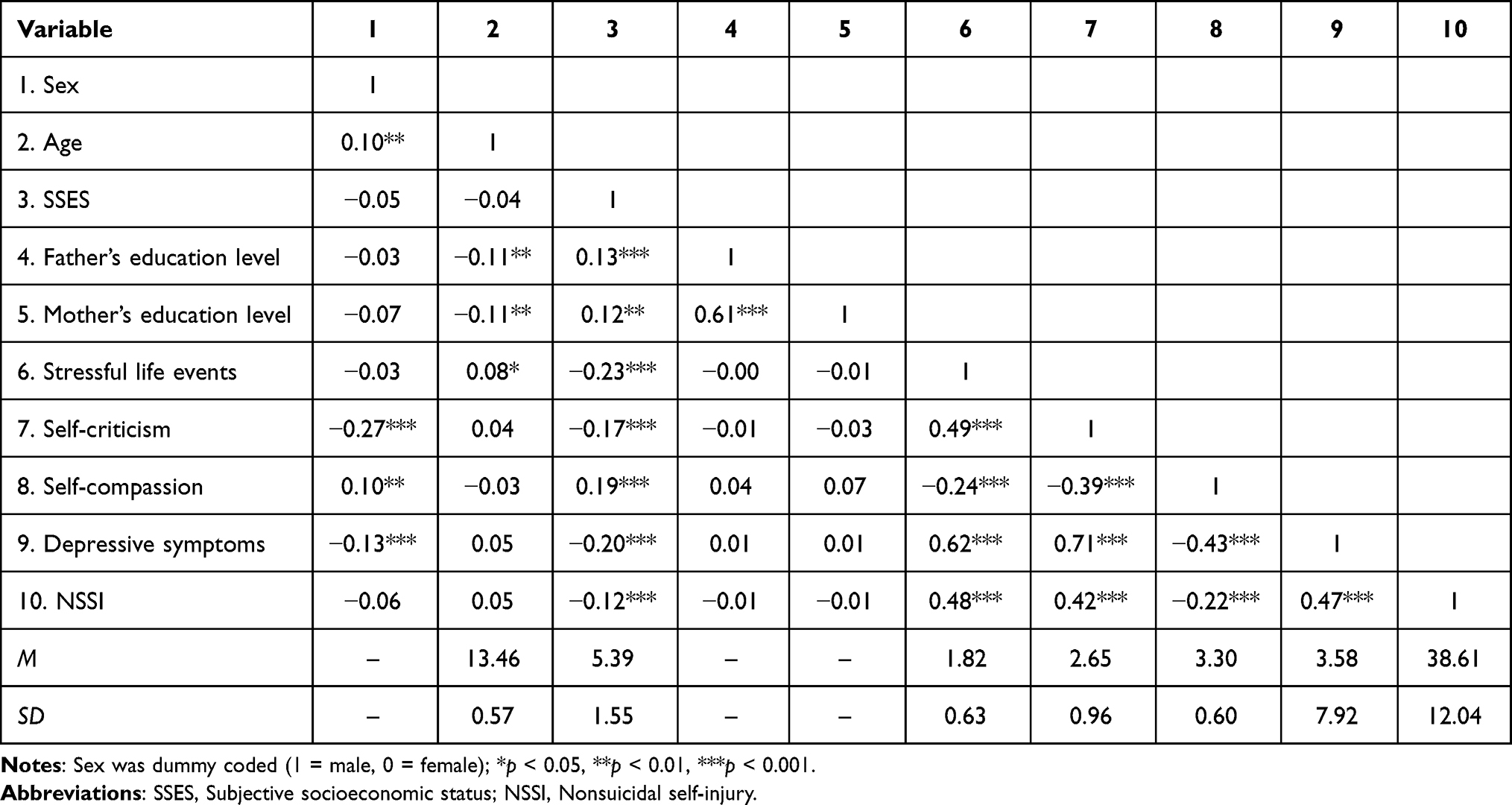 |
Table 1 Means, Standard Deviations, and Correlations Among the Study Variables |
Regression Analyses
As seen in Table 2, even though stressful life events (B = 3.79, SE = 0.35, p < 0.001), self-criticism (B = 5.78, SE = 0.35, p < 0.001), and self-compassion (B = −2.25, SE = 0.34, p < 0.001) all significantly predicted depressive symptoms, there was no significant three-way interaction (B = 0.28, SE = 0.23, p = 0.23). The two-way interaction of self-criticism and stressful life events on depressive symptoms was significant (B = 0.96, SE = 0.30, p < 0.01). Specifically, although life stress significantly predicted depressive symptoms for both the lower and higher self-criticism groups (ps < 0.001), the association between stressful life events and depressive symptoms was stronger among those with higher self-criticism.
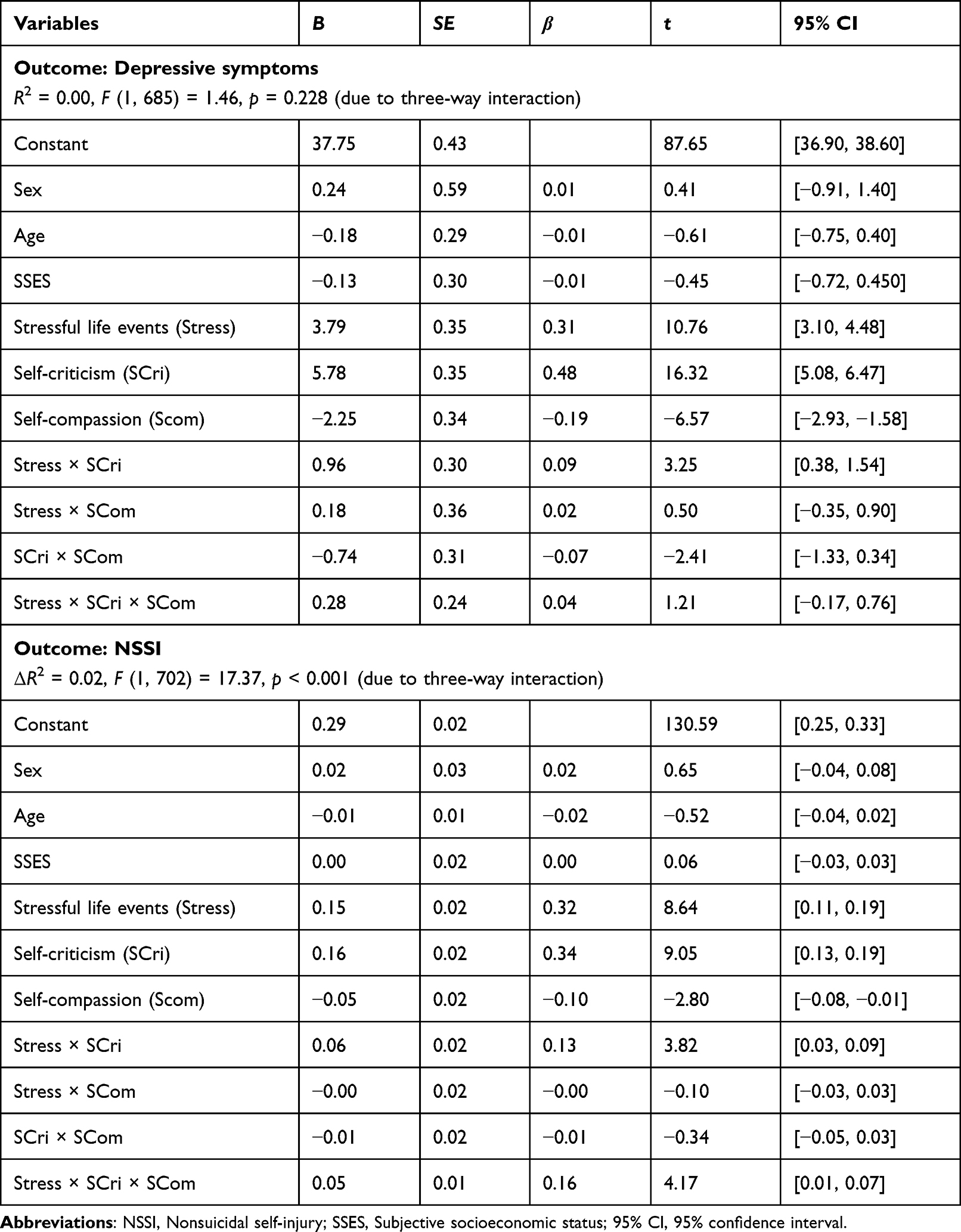 |
Table 2 Regression Analyses to Test the Moderating Effects of Self-Compassion and Self-Criticism in the Relationship Between Stressful Life Events and Depressive Symptoms/Nonsuicidal Self-Injury Among Adolescents |
For NSSI, stressful life events (B = 0.15, SE = 0.02, p < 0.001), self-criticism (B = 0.16, SE = 0.02, p < 0.001), and self-compassion (B = −0.05, SE = 0.02, p < 0.01) were all significant predictors of NSSI in the final model. Self-criticism also significantly interacted with life events (B = 0.06, SE = 0.02, p < 0.001). Additionally, the three-way interaction of life events, self-criticism, and self-compassion on NSSI was significant (B = 0.05, SE = 0.01, p < 0.001). The regressive results can be found in Table 2.
The results of the simple slope analyses for the three-way interaction on NSSI are shown in Figure 1A and B. At lower levels of self-compassion, stressful life events were significantly and positively related to NSSI in both the lower and higher self-criticism groups (−1SD: B = 0.15, SE = 0.04, p <0.001; +1SD: B = 0.16, SE = 0.02, p < 0.001; see Figure 1A). In the case of adolescents with higher self-compassion (see Figure 1B), the association between stressful life events and NSSI was significant only for those with high self-criticism (B = 0.25, SE = 0.03, p < 0.001) and not for those with low self-criticism (B = 0.04, SE = 0.03, p = 0.24). This result indicated the buffering role of self-compassion in the relationship between stressful life events and NSSI. However, this was only the case for those with lower self-criticism.
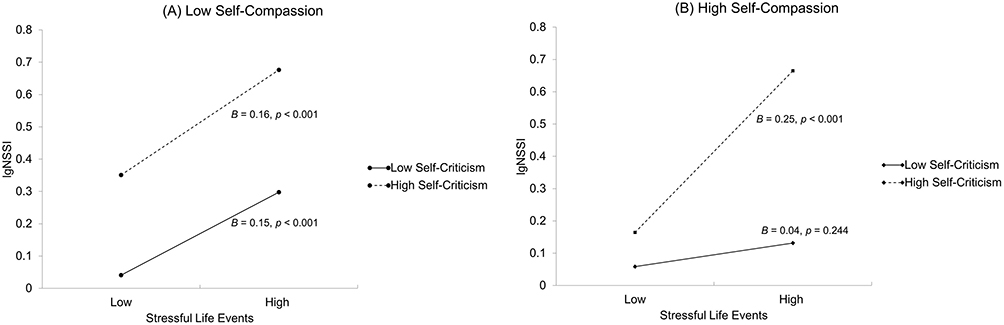 |
Figure 1 (A) The interaction effect of self-criticism and stressful life events at lower levels of self-compassion. (B) The interaction effect of self-criticism and stressful life events at higher levels of self-compassion. Abbreviation: NSSI, Nonsuicidal self-injury. |
Follow-Up Analyses
We also examined the moderating roles of the three components of self-compassion separately. The results indicated that the three-way interactions of stress, self-criticism, and each aspect of self-compassion on NSSI were significant (self-kindness: B = 0.04, SE = 0.01, p < 0.001; common humanity: B = 0.03, SE = 0.01, p < 0.01; mindfulness: B = 0.03, SE = 0.01, p < 0.01). The significant interaction patterns were similar to those shown in Figures 1A and B for total self-compassion. For depressive symptoms, significant three-way interactions were not found for self-kindness and common humanity but for mindfulness (B = 0.49, SE = 0.24, p < 0.05). However, life stress could significantly predict adolescents’ depressive symptoms regardless of the levels of their mindfulness.
Moreover, to test the potential sex differences in the interaction of stress, self-criticism, and self-compassion on depressive symptoms or NSSI, separate exploratory analyses were conducted for boys and girls. The results for boys revealed a similar pattern to that of the entire sample in that stressful life events, self-criticism, and self-compassion all had significant main effects on depressive symptoms or NSSI, but the three-way interaction was only significant for NSSI (B = 0.06, SE = 0.02, p < 0.001). The results of the simple slope analysis were similar to those reported for the overall sample in Figures 1A and B. Among girls, although the associations between stressful life events, self-criticism, self-compassion, and depressive symptoms resembled those observed among boys, self-compassion played a different role in NSSI for girls compared to boys. Specifically, self-compassion in girls exhibited no direct relationship with NSSI (B = −0.02, SE = 0.03, p = 0.38), nor did it moderate the relationship between stressful life events, self-criticism, and NSSI (B = 0.03, SE = 0.02, p = 0.09).
Discussion
In the present study, we examined whether self-criticism and self-compassion interacted with stressful life events to predict depressive symptoms and NSSI among Chinese adolescents. The results indicated that self-criticism exacerbated the effects of stressful life events on both adolescent depressive symptoms and NSSI. However, the protective roles of self-compassion differed for depressive symptoms and NSSI. That is, self-compassion could mitigate the effects of stressful life events on NSSI but not on depressive symptoms.
Although originally proposed as a characteristic of depression, research has shown that self-criticism is associated with a range of psychological maladjustments, including NSSI.15 Individuals with a critical view of the self are more likely to choose NSSI over other coping behavior not only because of emotion-regulation motivations but also out of desires for self-punishment.12,17 Consistent with prior empirical studies,21,56,57 we found that self-criticism was a strong correlate of depressive symptoms and NSSI. Additionally, in line with previous work on adolescents,58,59 self-criticism was found to confer vulnerability to both depression and NSSI, such that for adolescents high in self-criticism, elevated levels of life stress led to an augmentation of depressive symptoms and NSSI. When confronted with stressful events in daily life (eg, academic failure, punishment from teachers or parents), self-critical adolescents tend to ruminate on their negative experiences60 and the inadequate part of themselves.14 Therefore, they are more likely to experience emotional distress and develop self-persecution desires, which in turn increase the risk of depression and NSSI.
Although our results suggested that self-criticism appears to be more strongly associated with depressive symptoms than with NSSI, at the same time, we found that self-compassion only moderated the effect of risk factors on NSSI in adolescents but not on depressive symptoms. According to the present findings, the stable association between stressful life events and NSSI may be mitigated by self-compassion and its three components, yet only under low levels of self-criticism. Given that NSSI often functions to regulate negative emotions,11 while the intensity of stressful life events may be related to an augmentation of emotional distress and negative thoughts about oneself, engaging in self-compassion allows people to respond to negative feelings in a more self-nurturing and compassionate way rather than resorting to maladaptive and impulsive behavior, such as NSSI. Our findings also support the Benefit and Barrier Model of NSSI,17 in which a positive association with oneself could be a barrier to NSSI deterring people from deliberately self-harming. However, the buffering effect of self-compassion on the relationship between stressful life events and NSSI only existed in adolescents with low self-criticism. That is, among adolescents with high self-criticism, even though they can provide self-compassion toward themselves under the circumstance of increasing stress, they still reported a high level of NSSI. More notable, our results suggested that the protective effect of self-compassion on NSSI may differ between boys and girls, with self-compassion being less related to girls’ engagement in NSSI compared to boys. In the current sample, adolescent girls reported more self-criticism and less self-compassion than boys, which is consistent with prior findings.61,62 It is possible that female gender norms of being compassionate to others do not translate into how they show compassion to themselves.63 Thus, the association between stressful life events and NSSI may be stronger, and self-compassion may not act as an effective barrier to NSSI in girls because they generally have higher levels of self-criticism and lower levels of self-compassion. These findings suggested that when making efforts to build barriers to NSSI, it is critical to not only enhance one’s ability to self-care, but also to reduce negative reactions to stressful experiences. It may also be particularly beneficial for girls facing life stressors to receive external sources of compassion and support, given that the protective effect of their self-compassion is quite limited.
Previous evidence has shown that self-compassion significantly moderates the relationships between stressful experiences, self-criticism, and symptoms of depression,37,38,64 which is not the case in the present study. However, the samples of these studies only included adults. Compared to adulthood, adolescence is a period in which self-compassion is relatively lacking.25 Given the various stressors faced by most adolescents, being kind and understanding themselves to a small degree or realizing that other peers are going through the same problems may play a very weak role in attenuating negative emotional experiences. Nonetheless, it is enough to prevent adolescents from engaging in direct self-injurious behavior. Another reason why self-compassion showed a weak protective effect in the present study might be our choice of compassionate components. Existing literature has indicated that the association of compassionate (positive) subscale scores of SCS with psychopathology is fairly small,40 and the strong links between the total SCS score and psychiatric symptoms may be driven by uncompassionate (negative) indicators (ie, self-judgment, overidentification, and isolation).65,66 Although recent researchers have found a significant buffering effect of self-compassion on depression in adolescents,36,67 the self-compassion scores in these studies consisted of both the positive and negative subscales of SCS. Unlike previous studies, we only used the positive indicators in this study and found no significant buffering effects on depressive symptoms. Future studies are recommended to extend the existing findings by testing the roles of both positive and negative aspects of self-compassion.
Although self-compassion did not moderate the relationships between stress, self-criticism, and depressive symptoms in the present study, the higher levels of self-compassion were associated with fewer depressive symptoms, which was in line with the literature that highlighted the positive role of self-compassion in adolescent mental health.68 Moreover, the direct relationship of self-compassion with depressive symptoms was greater than that with NSSI. These findings may indicate that self-compassion still plays an important role in the development of depression. Therefore, fostering self-compassion may also be effective for most adolescents.
By examining the joint effects of self-compassion, self-criticism, and stress on adolescent depression and NSSI at the same time, our study adds to the existing research on adolescents. The current study also extends prior research by testing the sex differences in the above relationships and the effects of different aspects of self-compassion. Our findings suggest that being disappointed and critical of oneself is a risk factor for both depressive symptoms and NSSI. In contrast, being kind to the self and thinking about stressful experiences from a mindful perspective are related with fewer depressive emotions and could diminish the relationship between stressful life experiences and NSSI. Given the strong links of self-criticism with depression and NSSI, preventive interventions involving self-criticism need to be valued for helping adolescents. Moreover, the protective role of self-compassion also has preventive implications for adolescent mental health, especially for adolescents with stressful life experiences. Although few of the currently available programs for enhancing the level of self-compassion have investigated the effect on NSSI, some self-compassion training programs have been shown to be beneficial. For example, Gilbert’s31 compassion-focused approach may reduce adolescent self-injurious behavior by improving self-directed warmth and mindfulness. Considering self-compassion in the context of NSSI may allow school counselors or educators to help adolescents who injure themselves to recognize their personal worth and competencies. In this case, making efforts to improve adolescents’ self-compassion abilities may be a way to reduce NSSI risk. It has also been found that self-compassion related interventions could reduce self-criticism,69 so self-compassion enhancing programs may be effective in reducing NSSI, especially for self-critical adolescents. Additionally, girls who have encountered stressful life events should also receive more external support and care, as they have a tendency to be more self-critical and may lack sufficient self-compassion to protect against mental health problems. Furthermore, programs enhancing self-compassion have also shown positive effects on depression. For example, Bluth et al’s mindful self-compassion program helped decrease anxiety, depression, and perceived stress in adolescents.70 Training self-compassionate abilities, therefore, may be effective in protecting adolescents from developing depressive symptoms regardless of their stressful experiences.
Several limitations should be considered when interpreting the findings of the current study. First, we used a total score of stressful life events in this study, whereas different types of stressful events may work differently. Future research could benefit from using more valid tools to test the effects of different types of stressful life experiences. Second, although in the present study the relationships among variables were based on theoretical frameworks, the cross-sectional design of the study limited the causality of our conclusions and prevented analyses of depressive symptoms and NSSI changes at the with-person level. Third, the sample of the current study is limited to community adolescents in China. Therefore, the generalization of the present findings to other samples of different cultures should be extended with caution. Finally, there are other positive self-relating processes that may play buffering roles, such as self-compassion, self-reassurance, and mindfulness.71–73 Identifying the effects of different types of protective factors is an important direction for future research.
Conclusion
In summary, our findings suggested that self-criticism exacerbated the relationships between stressful life events and adolescent depressive symptoms and NSSI. Additionally, self-compassion showed a significant buffering effect on the negative impacts of stressful events and self-criticism on NSSI but not on the impacts on symptoms of depression. The results suggest the different roles of self-compassion in adolescent depressive symptoms and NSSI and show the value in enhancing self-compassion when making efforts to prevent and intervene adolescents’ engagement in nonsuicidal self-injury.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Please contact [email protected].
Ethics Approval and Informed Consent
Approval was obtained from the ethics committee of Institutional Review Board of the Faculty of Psychology, Beijing Normal University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Participants and their primary caregivers gave written informed consent for the assessment.
Acknowledgments
We are grateful to the students and their parents, the principal and teachers who contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (31900772).
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. 2012;379(9820):1056–1067. doi:10.1016/S0140-6736(11)60871-4
2. Lim KS, Wong CH, McIntyre RS, et al. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: a meta-analysis. Int J Environ Res Public Health. 2019;16(22):4581. doi:10.3390/ijerph16224581
3. What is self-injury? International society for the study of self-injury. Available from: https://www.itriples.org/what-is-nssi.
4. Gillies D, Christou MA, Dixon AC, et al. Prevalence and characteristics of self-harm in adolescents: meta-analyses of community-based studies 1990–2015. J Am Acad Child Adolesc Psychiatry. 2018;57(10):733–741. doi:10.1016/j.jaac.2018.06.018
5. Marshall SK, Tilton-Weaver LC, Stattin H. Non-suicidal self-injury and depressive symptoms during middle adolescence: a longitudinal analysis. J Youth Adolesc. 2013;42(8):1234–1242. doi:10.1007/s10964-013-9919-3
6. Tilton-Weaver L, Marshall SK, Svensson Y. Depressive symptoms and non-suicidal self-injury during adolescence: latent patterns of short-term stability and change. J Adolesc. 2019;75:163–174. doi:10.1016/j.adolescence.2019.07.013
7. Wu J, Liu S, Luo J, Li X, You J. The effects of childhood abuse, depression, and self-compassion on adolescent nonsuicidal self-injury: a moderated mediation model. Child Abuse Negl. 2023;136:105993. doi:10.1016/j.chiabu.2022.105993
8. Metalsky GI, Abramson LY, Seligman MEP, Semmel A, Peterson C. Attributional styles and life events in the classroom: vulnerability and invulnerability to depressive mood reactions. J Pers Soc Psychol. 1982;43(3):612–617. doi:10.1037//0022-3514.43.3.612
9. Hagen EH. Evolutionary theories of depression: a critical review. Can J Psychiatry Rev Can Psychiatr. 2011;56(12):716–726. doi:10.1177/070674371105601203
10. Liu RT, Cheek SM, Nestor BA. Non-suicidal self-injury and life stress: a systematic meta-analysis and theoretical elaboration. Clin Psychol Rev. 2016;47:1–14. doi:10.1016/j.cpr.2016.05.005
11. Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr Dir Psychol Sci. 2009;18(2):78–83. doi:10.1111/j.1467-8721.2009.01613.x
12. Taylor PJ, Jomar K, Dhingra K, Forrester R, Shahmalak U, Dickson JM. A meta-analysis of the prevalence of different functions of non-suicidal self-injury. J Affect Disord. 2018;227:759–769. doi:10.1016/j.jad.2017.11.073
13. Blatt SJ, Zuroff DC. Interpersonal relatedness and self-definition: two prototypes for depression. Clin Psychol Rev. 1992;12(5):527–562. doi:10.1016/0272-7358(92)90070-O
14. Gilbert P, Clarke M, Hempel S, Miles JNV, Irons C. Criticizing and reassuring oneself: an exploration of forms, styles and reasons in female students. Br J Clin Psychol. 2004;43(1):31–50. doi:10.1348/014466504772812959
15. Glassman LH, Weierich MR, Hooley JM, Deliberto TL, Nock MK. Child maltreatment, non-suicidal self-injury, and the mediating role of self-criticism. Behav Res Ther. 2007;45(10):2483–2490. doi:10.1016/j.brat.2007.04.002
16. Zelkowitz RL, Cole DA. Longitudinal relations of self-criticism with disordered eating behaviors and nonsuicidal self-injury. Int J Eat Disord. 2020;53(7):1097–1107. doi:10.1002/eat.23284
17. Hooley JM, Franklin JC. Why do people hurt themselves? A new conceptual model of nonsuicidal self-injury. Clin Psychol Sci. 2018;6(3):428–451. doi:10.1177/2167702617745641
18. Gilbert P, McEwan K, Irons C, et al. Self-harm in a mixed clinical population: the roles of self-criticism, shame, and social rank. Br J Clin Psychol. 2010;49(4):563–576. doi:10.1348/014466509X479771
19. Clarke M, Mcewan K, Ness J, Waters K, Basran J, Gilbert P. A descriptive study of feelings of arrested escape (entrapment) and arrested anger in people presenting to an emergency department following an episode of self-harm. Front Psychiatry. 2016;7:1–12. doi:10.3389/fpsyt.2016.00155
20. Burke TA, Fox K, Kautz M, Siegel DM, Kleiman E, Alloy LB. Real-time monitoring of the associations between self-critical and self-punishment cognitions and nonsuicidal self-injury. Behav Res Ther. 2021;137:103775. doi:10.1016/j.brat.2020.103775
21. Gong T, Ren Y, Wu J, Jiang Y, Hu W, You J. The associations among self-criticism, hopelessness, rumination, and NSSI in adolescents: a moderated mediation model. J Adolesc. 2019;72:1–9. doi:10.1016/J.ADOLESCENCE.2019.01.007
22. You J, Jiang Y, Zhang M, Du C, Lin MP, Leung F. Perceived parental control, self-criticism, and nonsuicidal self-injury among adolescents: testing the reciprocal relationships by a three-wave cross-lag model. Arch Suicide Res. 2017;21(3):379–391. doi:10.1080/13811118.2016.1199989
23. Baetens I, Claes L, Hasking P, et al. The relationship between parental expressed emotions and non-suicidal self-injury: the mediating roles of self-criticism and depression. J Child Fam Stud. 2015;24(2):491–498. doi:10.1007/s10826-013-9861-8
24. Liu S, Li CI, Wang C, Wei M, Ko S. Self-compassion and social connectedness buffering racial discrimination on depression among Asian Americans. Mindfulness. 2020;11(3):672–682. doi:10.1007/s12671-019-01275-8
25. Neff K. Self-compassion: an alternative conceptualization of a healthy attitude toward oneself. Self Identity. 2003;2(6):85–101. doi:10.1080/15298860309032
26. Allen AB, Leary MR. Self-compassion, stress, and coping. Soc Personal Psychol Compass. 2010;4(2):107–118. doi:10.1111/j.1751-9004.2009.00246.x
27. Finlay-Jones AL. The relevance of self-compassion as an intervention target in mood and anxiety disorders: a narrative review based on an emotion regulation framework. Clin Psychol. 2017;21(2):90–103. doi:10.1111/cp.12131
28. Chishima Y, Mizuno M, Sugawara D, Miyagawa Y. The influence of self-compassion on cognitive appraisals and coping with stressful events. Mindfulness. 2018;9(6):1907–1915. doi:10.1007/s12671-018-0933-0
29. Ewert C, Vater A, Schröder-Abé M. Self-compassion and coping: a meta-analysis. Mindfulness. 2021;12:1063–1077. doi:10.1007/s12671-020-01563-8
30. Werner AM, Tibubos AN, Rohrmann S, Reiss N. The clinical trait self-criticism and its relation to psychopathology: a systematic review—Update. J Affect Disord. 2019;246:530–547. doi:10.1016/j.jad.2018.12.069
31. Gilbert P. Introducing compassion-focused therapy. Adv Psychiatr Treat. 2009;15(3):199–208. doi:10.1192/apt.bp.107.005264
32. Gilbert P. An introduction to compassion focused therapy in cognitive behavior therapy. Int J Cogn Ther. 2010;3(2):97–112. doi:10.1521/ijct.2010.3.2.97
33. Longe O, Maratos FA, Gilbert P, et al. Having a word with yourself: neural correlates of self-criticism and self-reassurance. NeuroImage. 2010;49(2):1849–1856. doi:10.1016/j.neuroimage.2009.09.019
34. Xavier A, Pinto Gouveia J, Cunha M. Non-suicidal self-injury in adolescence: the role of shame, self-criticism and fear of self-compassion. Child Youth Care Forum. 2016;45(4):571–586. doi:10.1007/s10566-016-9346-1
35. Jiang Y, You J, Hou Y, et al. Buffering the effects of peer victimization on adolescent non-suicidal self-injury: the role of self-compassion and family cohesion. J Adolesc. 2016;53:107–115. doi:10.1016/j.adolescence.2016.09.005
36. Lathren C, Bluth K, Park J. Adolescent self-compassion moderates the relationship between perceived stress and internalizing symptoms. Pers Individ Differ. 2019;143(3):36–41. doi:10.1016/j.paid.2019.02.008.Adolescent
37. Kaurin A, Schönfelder S, Wessa M. Self-compassion buffers the link between self-criticism and depression in trauma-exposed firefighters. J Couns Psychol. 2018;65(4):453–462. doi:10.1037/cou0000275.supp
38. Wong CCY, Mak WWS. Differentiating the role of three self-compassion components in buffering cognitive-personality vulnerability to depression among Chinese in Hong Kong. J Couns Psychol. 2013;60(1):162–169. doi:10.1037/a0030451
39. Ford J, Klibert JJ, Tarantino N, Lamis DA. Savouring and self-compassion as protective factors for depression. Stress Health. 2017;33(2):119–128. doi:10.1002/smi.2687
40. Salinger J, Whisman M. Does self-compassion moderate the cross-sectional association between life stress and depressive symptoms? Mindfulness. 2021;12:1–10. doi:10.1007/s12671-020-01554-9
41. Households’ income and consumption expenditure in 2020. National Bureau of Statistics of China; 2021. Available from: http://www.stats.gov.cn/english/PressRelease/202101/t20210119_1812523.html.
42. Liu X, Liu LQ, Yang J, Zhao GF. Reliability and validity of the adolescents self-rating life events checklist. Chin J Clin Psychol. 1997;5(1):34–36.
43. Jiang Y, Zhang J, Ming H, Huang S, Lin D. Stressful life events and well-being among rural-to-urban migrant adolescents: the moderating role of the stress mindset and differences between genders. J Adolesc. 2019;74:24–32. doi:10.1016/j.adolescence.2019.05.005
44. Wang M, Li H, Deater-Deckard K, Zhang W. Interacting effect of catechol-O-methyltransferase (COMT) and monoamine oxidase A (MAOA) gene polymorphisms, and stressful life events on aggressive behavior in Chinese male adolescents. Front Psychol. 2018;9:1–9. doi:10.3389/fpsyg.2018.01079
45. Chen J, Yan L, Zhou L. Reliability and validity of Chinese version of self-compassion scale. Chin J Clin Psychol. 2011;19(6):734–736.
46. Neff KD. The development and validation of a scale to measure self-compassion. Self Identity. 2003;2(3):223–250. doi:10.1080/15298860309027
47. Feng Y. The Relation of Adolescents’ Self-Harm Behaviors, Individual Emotion Characteristics and Family Environment Factors. Central China Normal University; 2008.
48. He C, Wei H. Effect of parents’ phubbing on adolescents’ self-injury: a perspective of experiential avoidance model. Psychol Dev Educ. 2022;38(2):287–294. doi:10.16187/j.cnki.issn1001-4918.2022.02.16
49. Fendrich M, Weissman MM, Warner V. Screening for depressive disorder in children and adolescents: validating the center for epidemiologic studies depression scale for children. Am J Epidemiol. 1990;131(3):538–551. doi:10.1093/oxfordjournals.aje.a115529
50. Plener PL, Schumacher TS, Munz LM, Groschwitz RC. The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Personal Disord Emot Dysregulation. 2015;2(1). doi:10.1186/s40479-014-0024-3
51. Richardson AS, Bergen HA, Martin G, Roeger L, Allison S. Perceived academic performance as an indicator of risk of attempted suicide in young adolescents. Arch Suicide Res. 2005;9(2):163–176. doi:10.1080/13811110590904016
52. Wang Q, Liu X. Peer victimization and nonsuicidal self-injury among Chinese left-behind children: the moderating roles of subjective socioeconomic status and social support. J Interpers Violence. 2020;36(19):11165–11187. doi:10.1177/0886260519897346
53. Giatti L, Camelo LDV, Rodrigues JFDC, Barreto SM. Reliability of the MacArthur scale of subjective social status - Brazilian longitudinal study of adult health (ELSA-Brasil). BMC Public Health. 2012;12:1096. doi:10.1186/1471-2458-12-1096
54. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
55. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis.
56. Ehret AM, Joormann J, Berking M, Ehret AM, Joormann J, Berking M. Examining risk and resilience factors for depression: the role of self-criticism and self-compassion. Cogn Emot. 2015;29(8):1496–1504. doi:10.1080/02699931.2014.992394
57. Irons C, Gilbert P, Baldwin MW, Baccus JR, Palmer M. Parental recall, attachment relating and self-attacking/self-reassurance: their relationship with depression. Br J Clin Psychol. 2006;45(3):297–308. doi:10.1348/014466505X68230
58. Adams P, Abela JRZ, Auerbach R, Skitch S. Self-criticism, dependency, and stress reactivity: an experience sampling approach to testing Blatt and Zuroff’s (1992) theory of personality predispositions to depression in high-risk youth. Pers Soc Psychol Bull. 2009;35(11):1440–1451. doi:10.1177/0146167209343811
59. Wedig MM, Nock MK. Parental expressed emotion and adolescent self-injury. J Am Acad Child Adolesc Psychiatry. 2007;46(9):1171–1178. doi:10.1097/chi.0b013e3180ca9aaf
60. O’Connor RC, Noyce R. Personality and cognitive processes: self-criticism and different types of rumination as predictors of suicidal ideation. Behav Res Ther. 2008;46(3):392–401. doi:10.1016/j.brat.2008.01.007
61. Liu QQ, Yang XJ, Hu YT, Zhang CY. Peer victimization, self-compassion, gender and adolescent mobile phone addiction: unique and interactive effects. Child Youth Serv Rev. 2020;118:105397. doi:10.1016/j.childyouth.2020.105397
62. Bluth K, Campo RA, Futch WS, Gaylord SA. Age and gender differences in the associations of self-compassion and emotional well-being in a large adolescent sample. J Youth Adolesc. 2017;46(4):840–853. doi:10.1007/s10964-016-0567-2
63. Yarnell LM, Stafford RE, Neff KD, Reilly ED, Knox MC, Mullarkey M Meta-analysis of gender differences in self-compassion. Self Identity; 2015. Available from: https://www.tandfonline.com/doi/full/10.1080/15298868.2015.1029966.
64. Lassri D, Gewirtz-Meydan A. Self-compassion moderates the mediating effect of self-criticism in the link between childhood maltreatment and psychopathology. J Interpers Violence. 2022;37(23–24):NP21699–NP21722. doi:10.1177/08862605211062994
65. Muris P, Otgaar H, López A, Kurtic I, van de Laar I. The (non)protective role of self-compassion in internalizing symptoms: two empirical studies in adolescents demonstrating unwanted effects of using the self-compassion scale total score. Mindfulness. 2021;12(1):240–252. doi:10.1007/s12671-020-01514-3
66. Muris P, Petrocchi N. Protection or vulnerability? A meta-analysis of the relations between the positive and negative components of self-compassion and psychopathology. Clin Psychol Psychother. 2017;24(2):373–383. doi:10.1002/cpp.2005
67. Liu QQ, Hu YT. Self-compassion mediates and moderates the association between harsh parenting and depressive symptoms in Chinese adolescent. Curr Psychol. 2020. doi:10.1007/s12144-020-01034-2
68. Marsh IC, Chan SWY, MacBeth A. Self-compassion and psychological distress in adolescents—A meta-analysis. Mindfulness. 2018;9(4):1011–1027. doi:10.1007/s12671-017-0850-7
69. Wakelin KE, Perman G, Simonds LM. Effectiveness of self-compassion-related interventions for reducing self-criticism: a systematic review and meta-analysis. Clin Psychol Psychother. 2022;29(1):1–25. doi:10.1002/cpp.2586
70. Bluth K, Gaylord SA, Campo RA, Mullarkey MC, Hobbs L. Making friends with yourself: a mixed methods pilot study of a mindful self-compassion program for adolescents. Mindfulness. 2016;7(2):479–492. doi:10.1007/s12671-015-0476-6
71. Kim JJ, Doty JR, Cunnington R, Kirby JN. Does self-reassurance reduce neural and self-report reactivity to negative life events? Front Psychol. 2021;12:10–15. doi:10.3389/fpsyg.2021.658118
72. Petrocchi N, Dentale F, Gilbert P. Self-reassurance, not self-esteem, serves as a buffer between self-criticism and depressive symptoms. Psychol Psychother Theory Res Pract. 2019;92(3):394–406. doi:10.1111/papt.12186
73. Serrano DM, Rufino KA, Tran JK, Vujanovic AA. Association between sleep disturbances and suicide risk among firefighters: the moderating role of mindfulness. Mindfulness. 2020;11(12):2793–2803. doi:10.1007/s12671-020-01491-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.