Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
The Effects of Oral Sodium Bicarbonate on Renal Function and Cardiovascular Risk in Patients with Chronic Kidney Disease: A Systematic Review and Meta-Analysis
Authors Cheng F, Li Q, Wang J, Wang Z, Zeng F, Zhang Y ![]()
Received 15 October 2021
Accepted for publication 30 November 2021
Published 7 December 2021 Volume 2021:17 Pages 1321—1331
DOI https://doi.org/10.2147/TCRM.S344592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Fang Cheng,1,2 Qiang Li,1,2 Jinglin Wang,1,2 Zhendi Wang,3 Fang Zeng,1,2 Yu Zhang1,2
1Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Hubei Province Clinical Research Center for Precision Medicine for Critical Illness, Wuhan, People’s Republic of China; 3Department of Urology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Fang Zeng; Yu Zhang
Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Email [email protected]; [email protected]
Objective: Oral sodium bicarbonate is often used to correct acid-base disturbance in patients with chronic kidney disease (CKD). However, there is little evidence on patient-level benign outcomes to support the practice.
Methods: We conducted a systematic review and meta-analysis to examine the efficacy and safety of oral sodium bicarbonate in CKD patients. A total of 1853 patients with chronic metabolic acidosis or those with low-normal serum bicarbonate (22– 24 mEq/L) were performed to compare the efficacy and safety of oral sodium bicarbonate in patients with CKD.
Results: There was a significant increase in serum bicarbonate level (MD 2.37 mEq/L; 95% CI, 1.03 to 3.72) and slowed the decline in estimated glomerular filtration rate (eGFR) (MD − 4.44 mL/min per 1.73 m2, 95% CI, − 4.92 to − 3.96) compared with the control groups. The sodium bicarbonate lowered T50-time, an indicator of vascular calcification (MD − 20.74 min; 95% CI, − 49.55 to 8.08); however, there was no significant difference between the two groups. In addition, oral sodium bicarbonate dramatically reduced systolic blood pressure (MD − 2.97 mmHg; 95% CI, − 5.04 to − 0.90) and diastolic blood pressure (MD − 1.26 mmHg; 95% CI, − 2.33 to − 0.19). There were no statistically significant body weight, urine pH and mean mid-arm muscle circumference.
Conclusion: Treatment of metabolic acidosis with sodium bicarbonate may slow the decline rate of kidney function and potentially significantly improve vascular endothelial function in patients with CKD.
Prospero Registration Number: CRD42020207185.
Keywords: chronic kidney disease, metabolic acidosis, sodium bicarbonate, kidney function, cardiovascular risk
Introduction
Chronic kidney disease (CKD) is a serious public health issue, characterized by kidney structural and functional abnormalities.1 Diabetes mellitus and hypertension are common underlying diseases associated with CKD. Major complications of CKD include anemia, cardiovascular disease, renal osteodystrophy, and metabolic acidosis (MA).2,3 These complications are mainly responsible for the increased morbidity and mortality of the disease.
Metabolic acidosis is present in approximately 15% of patients with CKD, due to the inability of the kidney to synthesize ammonia and excrete hydrogen ions, and is a well-recognized complication of CKD.4 MA often brings about a range of adverse effects in CKD patients, such as insulin resistance, increased cardiovascular risk, impaired muscle function, systemic inflammation, lower bone mineral density and increased fracture risk.5–7 Moreover, the relationship between impaired renal function and increased mortality in the CKD patients is positively related.8,9 Even though MA is a recognized risk factor for CKD, there is no clinically established protocol for improving the condition of patients with predialysis CKD.
Cardiovascular disease is the main cause of death in CKD patients.10 In CKD patients, cardiovascular diseases mainly manifest as impaired vascular endothelial function and accelerate the progress of arteriosclerosis.11 The T50 calcification inhibition test (T50-test) is a comprehensive functional test that analyzes the overall propensity of serum calcification. The in vitro diagnostic test is used to measure the conversion of primary to secondary calciprotein particles into serum. The half-maximum time for this conversion is called “T50”, and the unit is minutes (min).12 Low T50-time was related to progressive aortic stiffening and to all-cause mortality in non-dialysis CKD patients.13 Interventions to decrease vascular calcification and thus reduce mortality in CKD patients are of great importance. Hypertension is one of the most relevant risk factors for cardiovascular disease and is closely linked to coronary heart disease and stroke. The pathogenesis of the arterial dysfunctions can only be partially explained by conventional cardiovascular risk factors, thus suggesting a mechanism related to renal insufficiency. Furthermore, MA can accelerate progression of cardiovascular disease.14,15 Low serum bicarbonate levels have been associated with low T50-time, and sodium bicarbonate supplementation appears to be an effective regulator of calcification propensity.
Clinical practice guidelines suggest that treatment with alkalinizing agents (sodium bicarbonate and sodium citrate) improves the renal function of patients with CKD. Oral sodium bicarbonate is more likely to correct acid-base disturbance in CKD patients than sodium citrate to counteract MA in clinical practice.16,17 There have been reports on the role of oral bicarbonate supplementation in correcting the MA.18,19 The 2012 Kidney Disease Improving Global Outcomes guideline suggests base administration for CKD patients with serum bicarbonate concentration <22 mEq/L.20 The National Kidney Disease Outcomes Quality Initiative (KDOQI) guideline recommends administration of a base to maintain the value within the normal range, which is 22–29 mEq/L.21 However, there are few patient-level data to support the practice of using oral bicarbonate supplementation in clinical.22,23 Moreover, only a few studies have indicated whether sodium bicarbonate can effectively prevent adverse cardiovascular outcomes in advanced CKD, and whether it is safe in the context of increased sodium load, rather than merely increasing circulating sodium bicarbonate concentration.
A previous meta-analysis of small trials suggested a modest beneficial effect of sodium bicarbonate on estimated glomerular filtration rate (eGFR) and serum bicarbonate levels, indicating an uncertain effect on progression of kidney disease.24 However, the study did not examine its effects on cardiovascular disease. To summarize the latest evidence on this topic, we conducted a systematic review and meta-analysis to examine the safety and efficacy of oral sodium bicarbonate supplementation in patients with CKD.
Patients and Methods
We conducted a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, and a prespecified registered protocol in PROSPERO (CRD42020207185).
Search Strategy
PubMed, Embase and Cochrane CENTRAL databases were searched for relevant full-text studies (published between Jan. 2015 and Aug. 2020) (Supplemental Table S1). We also searched Clinicaltrials.gov and abstracts presented in the American Society of Nephrology annual meetings (2015–2020). The search was limited to randomized controlled trials (RCTs) conducted on human subjects. No language restrictions were applied.
Inclusion and Exclusion Criteria
For inclusion, the studies had to meet the following criteria: (1) include patients with stage 3–5 CKD and chronic MA, or those with low-normal serum bicarbonate (22–24 mEq/L); (2) include oral sodium bicarbonate therapy for the treatment of CKD in the experimental group and no treatment, usual patient care, or placebo therapy in the control group; (3) randomized controlled trial and (4) be available as a full-text publication. The exclusion criteria were as follows: (1) studies on end-stage kidney disease (ESKD) patients, dialysis and kidney transplantation patients, (2) studies evaluating the effect of intravenous sodium bicarbonate on acute MA, (3) studies with inconsistent outcome indicators, (4) inability to extract the corresponding data, and (5) observational or non-randomized trials.
Measured Outcomes
1. Kidney disease progression end points: change in eGFR decline at the end of the study period; serum bicarbonate; serum creatinine; and change in urinary albumin-to-creatinine ratio (ACR).
2. Cardiovascular risk outcomes: T50-time (an indicator of vascular calcification); systolic and diastolic blood pressure (BP).
3. Adverse effects and electrolyte changes: body weight; 24 h urinary sodium excretion; urine pH; mean mid-arm muscle circumference; changes in electrolyte measurements (eg, serum albumin, serum phosphate, serum potassium, serum calcium).
Data Collection
The initial searches were independently conducted by two authors (Qiang Li and Jinglin Wang) according to the inclusion and exclusion criteria, and disagreements were settled through consensus. Subsequently, the authors further searched for the full text of the relevant studies to determine which among them ultimately satisfied the inclusion criteria and cross-checked. Data were extracted using a standard data extraction sheet, including author names, year of publication, number of participants receiving oral sodium bicarbonate or placebo, study type, baseline eGFR (mL/min per 1.73 m2), duration of follow-up, and outcomes.
The quality of the studies was independently assessed by two authors (Fang Cheng and Fang Zeng) without blinding to authorship or journal, using the Cochrane risk of bias tool in several domains, viz. blinding of investigators and participants, personnel and outcome assessors, completeness of outcome data, reporting of selected outcomes, random sequence generation, allocation concealment, and other sources of bias.
Patient and Public Involvement
No patients were involved.
Statistical Analysis
Heterogeneity was evaluated by using the Cochrane’s Q and I2 statistic values, where I2 < 50% and P > 0.10, indicated non-significant heterogeneity, and therefore, the fixed effect models were used to ensure the robustness and sensitivity of the selected models to detect outliers. On the contrary, in case of clinical heterogeneity, the random-effect model should be selected. A sensitivity analysis was performed using the fixed-effect models and reported separately if the result differed from that of the random-effect model. For continuous variables, MD with 95% CIs was used to assess the effects of treatment (such as eGFR decline, serum bicarbonate, etc.). We assessed publication bias using funnel plots to determine the asymmetry when the number of studies was more than 5. Publication bias was determined using Begg’s and Egger’s tests; P < 0.05 indicated statistical significance. Meta-analyses were performed using RevMan version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) and STATA 13.2 (StataCorp, College Station, TX, USA).
Results
Search Results
Following a comprehensive search of PubMed, Embase, Cochrane CENTRAL databases from 2015 to 2020, a total of 126 publications were identified, of which 108 were excluded because they were review articles, duplicate or unrelated publications, or not able to get full text. Full-text evaluation of 18 potentially relevant articles identified 11 eligible studies involving 1853 participants (Figure 1).
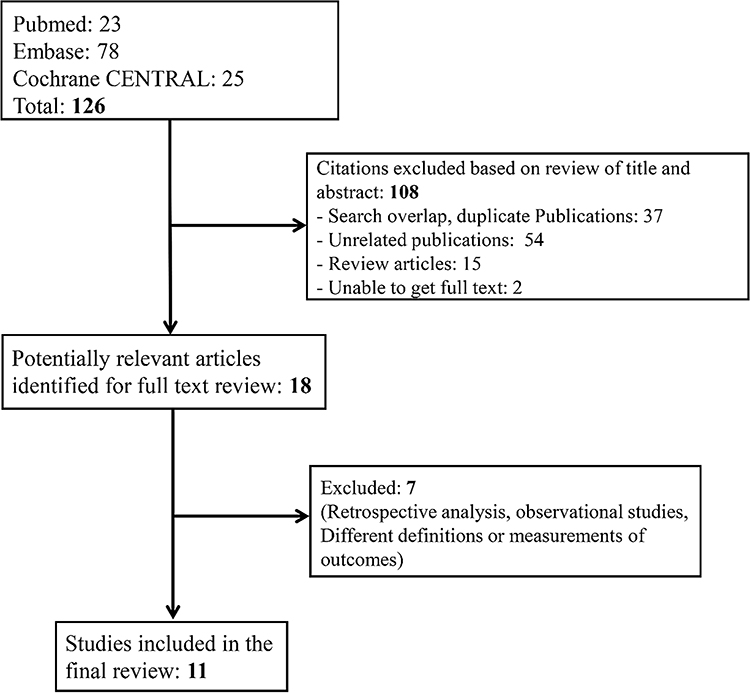 |
Figure 1 Flow chart showing number of citations retrieved by individual searches and number of trials included in the systematic review. |
Study Characteristics
In all 11 studies, the effects of oral sodium bicarbonate supplementation were compared with the effects noted in a control group (no treatment, usual care, or placebo), and the extracted information is summarized in Table 1. In most of the included studies, patients with stage 3–5 CKD and MA (serum bicarbonate, 22 mEq/L) were included, except for the studies by Raphael et al.,25 Melamed et al,26 and Goraya et al,27 where patients with low-normal serum bicarbonate levels (22–24 mEq/L). Goraya et al compared both sodium bicarbonate and dietary intervention (fruits and vegetables) with usual care.27 In the eligible studies, oral bicarbonate supplementation was intended to achieve serum bicarbonate levels between 24 and 28 mmol/L. The starting daily dose was calculated to replace half of the bicarbonate deficit (bicarbonate deficit in mmol=[24-serum bicarbonate in mmol/L]×[total body weight (kg)×0.5]). Depending on the dose required, participants took the medication two to three times per day. If the serum bicarbonate level was >28 mEq/L, the dose of sodium bicarbonate would be reduced by 50%. Raphael et al assigned participants to three groups: higher-dose (HD-NaHCO3; 0.8 mEq/kg of lean body weight per day), lower-dose (LD-NaHCO3; 0.5 mEq/kg of lean body weight per day) NaHCO3 and placebo groups.25 The study durations varied from 4 weeks to 5 years.
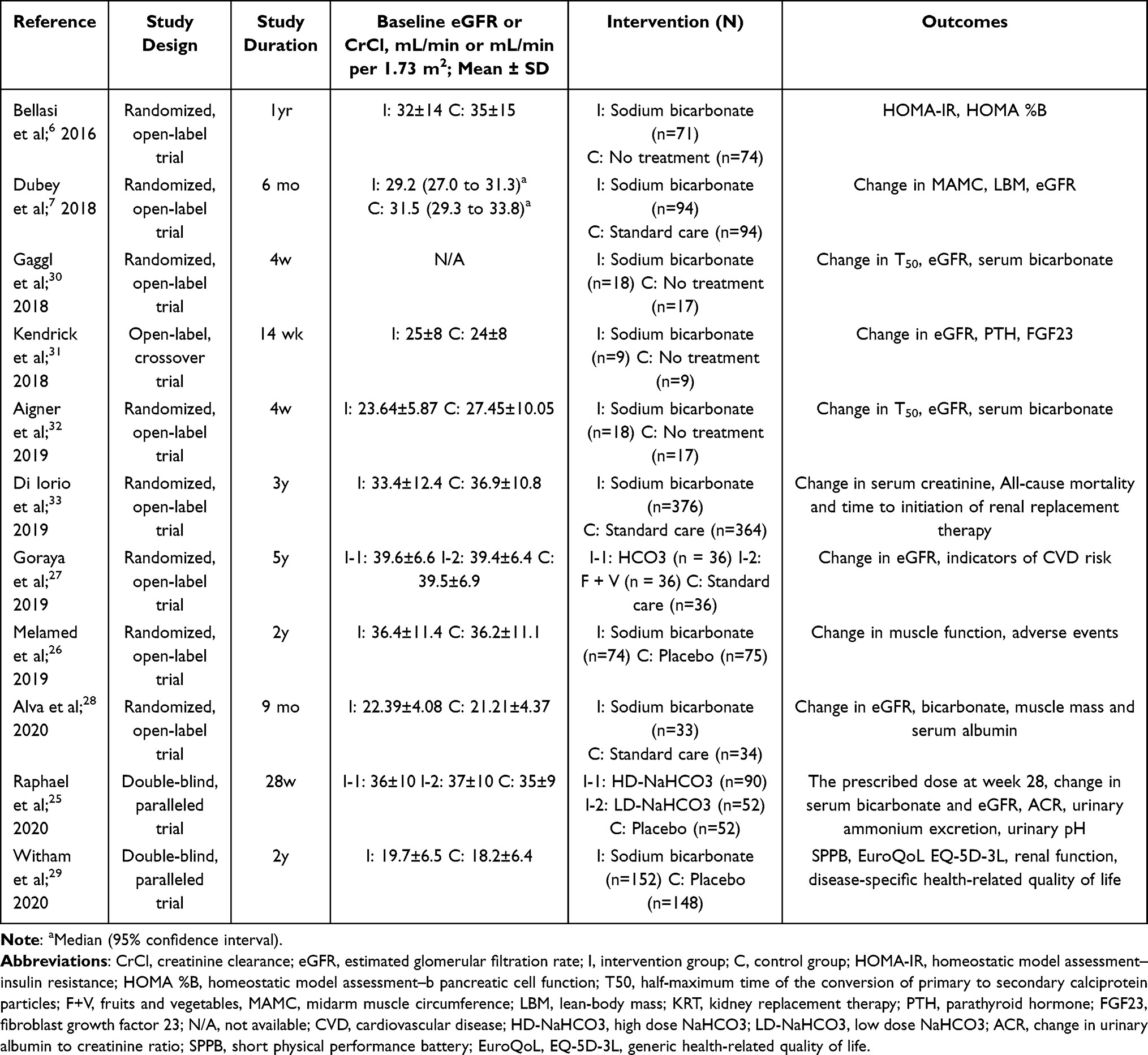 |
Table 1 Characteristics of the Authors, Interventions, and Outcomes of Included Trials |
Study Outcomes
The combined effects of oral sodium bicarbonate supplementation on kidney function (Table 2 and Figure 2), cardiovascular risk (Table 3 and Figure 3) and biochemical measurements (Table 4) are summarized, respectively.
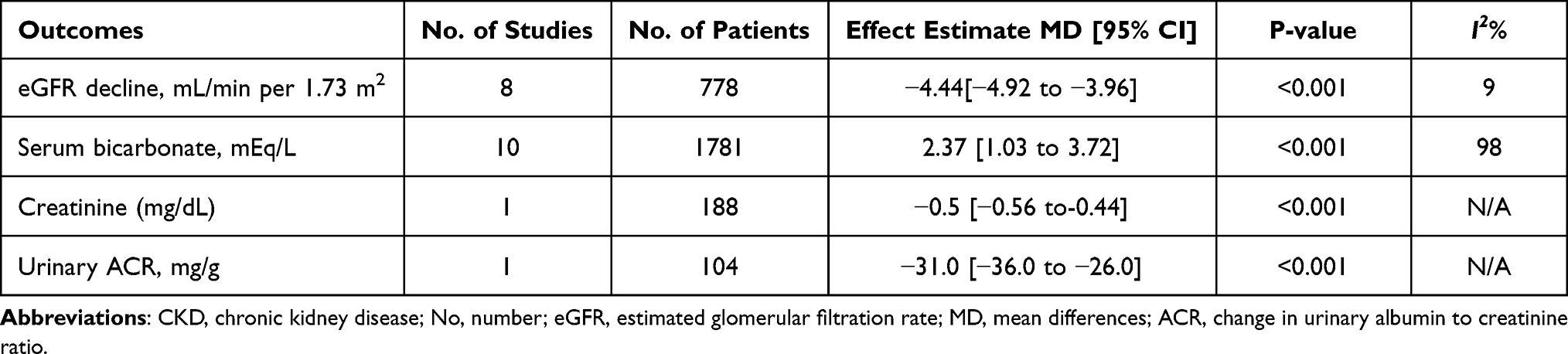 |
Table 2 The Effects of Oral Sodium Bicarbonate on Kidney Disease Progression End Points in Patients with CKD |
 |
Table 3 The Effects of Oral Sodium Bicarbonate on Cardiovascular Risk Outcomes in Patients with CKD |
 |
Table 4 The Effects of Oral Sodium Bicarbonate on Change in Biochemical Measurements |
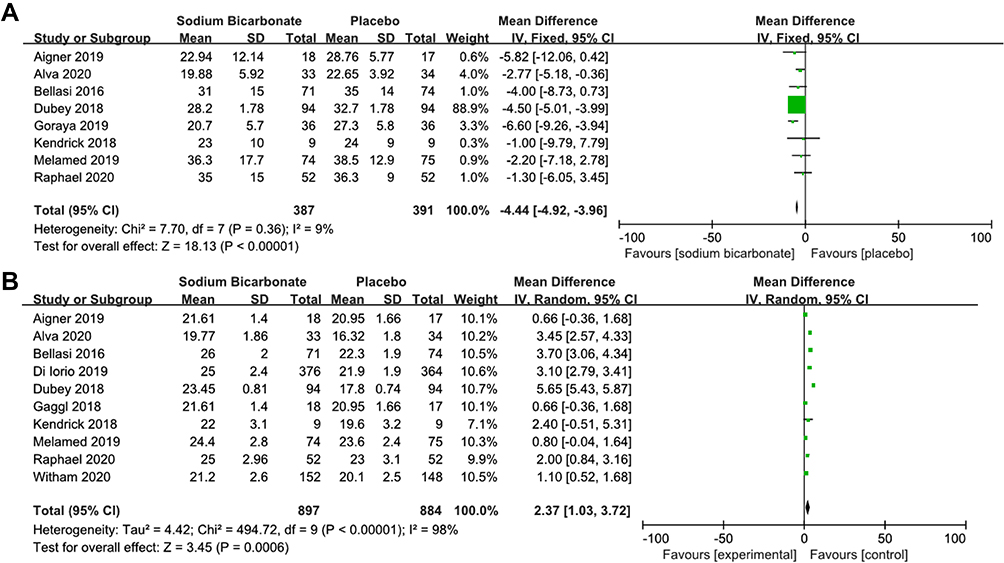 |
Figure 2 The decline in estimated glomerular filtration rate (eGFR) and serum bicarbonate level at the end of study period with oral sodium bicarbonate. (A) Forest plot of decline in eGFR. (B) Forest plot of serum bicarbonate level. Abbreviations: df, degrees of freedom; IV, inverse variance; SD, standard deviation; CI, confidence interval. |
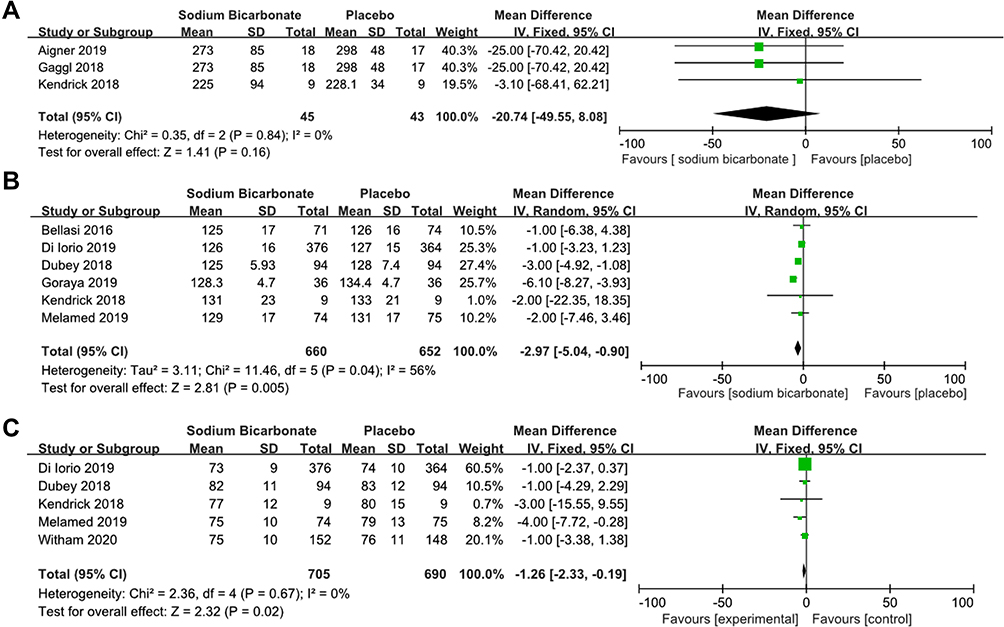 |
Figure 3 The effects of oral sodium bicarbonate on cardiovascular risk outcomes in patients with chronic kidney disease (CKD). (A) Forest plot of half-maximum time of the conversion of primary to secondary calciprotein particles (T50 time). (B) Forest plot of systolic blood pressure (BP). (C) Forest plot of diastolic BP. Abbreviations: df, degrees of freedom; IV, inverse variance; SD, standard deviation; CI, confidence interval. |
Kidney Function
The results indicated that oral sodium bicarbonate significantly slowed the decline in eGFR (MD −4.44 mL/min per 1.73 m2, 95% CI, −4.92 to −3.96) compared to that in the control groups: an eGFR increase of 4.44 mL/min per 1.73 m2 was noted in the sodium bicarbonate group. There was a significant increase in serum bicarbonate levels (MD, 2.37 mEq/L; 95% CI, 1.03 to 3.72) with treatment. The average serum bicarbonate level was ≥22 mEq/L in the oral sodium bicarbonate groups, except for those in the studies by Alva et al,28 and Witham et al.29 Overall, the analyses showed that oral sodium bicarbonate could significantly increase serum bicarbonate levels to the clinically recommended range or the KDOQI stipulations. In addition, oral sodium bicarbonate was significantly reduced in urinary ACR (MD −31.0 mg/g; 95% CI, −36.0 to −26.0) comparing with control group.
Cardiovascular Risk
The sodium bicarbonate intervention lowered the T50-time compared to that in the control group (MD −20.74 min; 95% CI, −49.55 to 8.08); however, there was no significant difference between the two groups. In addition, oral sodium bicarbonate markedly reduced systolic BP (MD −2.97 mmHg; 95% CI, −5.04 to −0.90) and diastolic BP (MD −1.26 mmHg; 95% CI, −2.33 to −0.19).
Biochemical Measurements
Oral sodium bicarbonate significantly increased serum calcium level (MD 0.12 mg/dl; 95% CI, 0.05 to 0.19) and serum phosphate level (MD 0.09 mg/dl; 95% CI, 0.04 to 0.15) compared to those in the control groups. However, there were no significant differences in serum potassium and serum albumin levels.
Adverse Effects
Oral sodium bicarbonate significantly increased the 24-hour urinary sodium excretion (MD 24.31 mEq/24 h; 95% CI, 21.74 to 26.89). In contrast to control group, sodium bicarbonate supplementation led to an increase in body weight (MD 0.25 kg; 95% CI, −1.12 to 1.61), urine pH (MD 0.23; 95% CI, 0.16 to 0.31), and mean mid-arm muscle circumference (0.14 cm; 95% CI, −0.46 to 0.74), although these changes were not statistically significant (Table 5).
 |
Table 5 Adverse Effects of Oral Sodium Bicarbonate in Patients with CKD |
Study Quality and Publication Bias
Supplemental Figure S1 outlines the publication bias of the included studies. Publication bias was not determined for outcomes other than serum bicarbonate levels because of the small number of studies (fewer than 10 studies) (Supplemental Table S2), Bias was determined using the Begg’s and Egger’s tests, and the results showed that there was publication bias for the outcome of serum bicarbonate levels.
Discussion
MA is a complication of CKD and is associated with bone demineralization, increased protein catabolism, and reduced insulin sensitivity.30,31 Current guidelines recommend treatment of MA in CKD with sodium (Na+)-based alkali, such as sodium bicarbonate.32 The association of MA with CKD progression and poor kidney function has been widely reported.27,33 An adverse effect of long-term sodium bicarbonate supplementation in patients with CKD is sodium mediated fluid retention, resulting in weight gain, peripheral edema, elevated blood pressure and even heart failure.34 Although previous studies have demonstrated an improvement in kidney function, differences in study protocol and small sample size prevented from reaching definitive conclusions.35 To date, there has been no consensus on the effect of oral sodium bicarbonate supplementation on vascular endothelial function. This meta-analysis focused on MA treatment in patients with CKD who received oral sodium bicarbonate versus patients who were untreated, received routine care, or a placebo.
Previous studies have revealed that serum bicarbonate levels were associated with kidney function and mortality in CKD patients.36 Mortality has been shown to increase at bicarbonate levels <17 and >27 mEq/L.37 The KDIGO 2012 guidelines recommend alkali therapy when the bicarbonate levels are <22 mEq/L but do not specify any evidence-based target levels. Similarly, the Renal Association of Great Britain and Caring for Australians with Renal Impairment proposal to maintain serum bicarbonate levels >22mEq/L.38 However, evidence-based optimal therapeutic targets for venous bicarbonate levels to be maintained in pre-dialysis CKD are unknown.
It is well‑known that decreased eGFR is very common in patients with CKD. eGFR is an indicator of disease severity used to monitor responses to treatment in clinical practice.39 Retrospective studies have confirmed that MA is associated with a more rapid decline in kidney function.40 It is estimated that 30–50% of patients with CKD develop MA, as the eGFR drops to 30–40 (mL/min/1.73m2).41 Krolewski et al confirmed that an eGFR loss of ≥3.3% per year occurs in CKD.42 Nonetheless, other studies have found that oral sodium bicarbonate therapy can reduce kidney dysfunction and delay the decline in eGFR.36 Therefore, the decline in eGFR was chosen as an indicator of the progression in renal function. Our results indicated that oral sodium bicarbonate supplementation significantly increased serum bicarbonate levels, resulting in a slower decline in eGFR and a reduction in ACR, which is in agreement with an earlier study that also showed a slower decline in eGFR after bicarbonate supplementation.43
Reducing vascular calcification can reduce mortality in patients with CKD.44 MA may contribute to increased inflammation45,46 and production of angiotensin II, aldosterone, and endothelin-1,47–49 which resulting in endothelial dysfunction in patients with CKD. Sodium bicarbonate supplementation appears to be an effective regulator of vascular calcification propensity. However, the effects of sodium bicarbonate on long-term cardiovascular function have not yet been clearly elucidated. Results of animal experiments showed that correction of MA could increase vascular calcification.50 Nevertheless, some studies have shown that the gradual development of MA with decreasing renal function could actually reduce vascular calcification.14 Observational studies have reported associations between lower serum bicarbonate levels and increased risks of endothelial dysfunction, hypertension, heart failure, and death.40 A previous study also indicated that correction of MA seems to have favorable effects on vascular function, which was assessed by flow-mediated dilation.24 In addition, compared with patients with bicarbonate concentrations between 22 and 26 mmol/L, patients with persistently high serum bicarbonate levels (>26 mmol/L) actually had an increased risk of heart failure and mortality.51
T50, a novel marker of serum calcification propensity, is used to determine the overall calcification propensity of serum before and after sodium bicarbonate treatment.13 Studies have shown that low T50-time is related to progressive aortic sclerosis and all-cause mortality in non-dialysis CKD, dialysis, and transplant patients.52 Our results showed that there was no significant difference in T50 between the sodium bicarbonate group and the control group. However, the positive effects of sodium bicarbonate may have been masked by the parallel increase in phosphate concentrations, which are expected to have an opposing effect on calcification propensity. An earlier study indicated that serum T50 was inversely associated with circulating phosphate, age, eGFR.53 The results of the study indicated that serum phosphate levels increased significantly, which contributed to explaining the phenomenon mentioned above. Furthermore, the results showed significantly increased serum calcium levels; however, serum calcium concentrations cannot reflect the nature of serum calcification. Due to impaired renal function in regulating calcium and abnormal bone transformation in patients with CKD, vascular calcification occurred in a considerable number of patients before the increase in blood calcium levels.54 Moreover, our study showed that sodium bicarbonate decreased systolic or diastolic BP. However, this may be attributed to the increased antihypertensive therapy when patients receive sodium bicarbonate in clinical practice.
Potential benefits of oral sodium bicarbonate supplementation on micro-nutritional status such as serum albumin, potassium levels, and mid-arm muscle circumference were investigated in a limited number of patients, and no significant differences were found in our analysis. A major concern regarding long-term sodium bicarbonate supplementation in patients with CKD is sodium-mediated fluid retention leading to peripheral and pulmonary edema, weight gain, and increased BP.55 A significant proportion of patients on sodium bicarbonate would require increased diuretic therapy. In addition, the results showed significantly increased urinary sodium excretion in patients with CKD after oral sodium bicarbonate therapy. Some studies have found an association between higher urinary sodium excretion and kidney disease progression and cardiovascular events.56,57 Diuretic therapy could also partially account for the increased urinary sodium excretion in the sodium bicarbonate group. Although blood pressures were comparable, this might be attributed to a higher dosage of diuretics. However, there was no significant increase in urine pH. Hence, these data indicated that sodium bicarbonate supplementation in patients with CKD was relatively safe.
Strengths and Limitations of This Study
- This is a comprehensive systematic review, including meta-analysis, of the effectiveness and safety of oral sodium bicarbonate in CKD patients.
- Our results show that sodium bicarbonate may slow the decline rate of kidney function and potentially significantly improve vascular endothelial function in patients with CKD.
- The main limitation of our analysis is the lack of long-term follow-ups of oral sodium bicarbonate on patient-centered endpoints, including mortality.
- Most of the included studies were single-center, open-label trials that enrolled only a small number of patients, preventing the analysis of patient-centered endpoints.
- There was significant clinical heterogeneity of the included trials, such as sodium bicarbonate dose, control strategy, baseline eGFR and serum bicarbonate levels, and treatment duration, so it was difficult to obtain an exact conclusion.
Conclusion
In this meta-analysis, the efficacy and safety of oral sodium bicarbonate in patients with CKD were investigated. The results suggested that treatment of MA with sodium bicarbonate may delay the decline of kidney function while maintaining serum calcification propensity in patients with CKD, indicating that treatment of MA with sodium bicarbonate is safe and overall improves kidney function.
Abbreviations
CKD, chronic kidney disease; MA, metabolic acidosis; RCT, randomized controlled trial; MD, mean differences; eGFR, estimated glomerular filtration rate; ESKD, end-stage kidney disease; ACR, change in urinary albumin-to-creatinine ratio; CPP, calciprotein particles; T50-time, half-maximum time of the conversion of primary to secondary calciprotein particles; BP, blood pressure.
Acknowledgment
The authors thank Qiling Xu for kindly providing the language checking help.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key R&D Program of China (2017YFC0909900), and National Key R&D Program of Hubei Province (No.2020BCA060).
Disclosure
The authors declare no conflict of interest.
References
1. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165–180. doi:10.1016/S0140-6736(11)60178-5
2. Reiss AB, Miyawaki N, Moon J, et al. CKD, arterial calcification, atherosclerosis and bone health: inter-relationships and controversies. Atherosclerosis. 2018;278:49–59. doi:10.1016/j.atherosclerosis.2018.08.046
3. Chen TK, Knicely DH, Grams ME. Chronic kidney disease diagnosis and management: aReview. JAMA. 2019;322(13):1294–1304. doi:10.1001/jama.2019.14745
4. Wesson DE, Buysse JM, Bushinsky DA. Mechanisms of metabolic acidosis induced kidney injury in chronic kidney disease. J Am Soc Nephrol. 2020;31(3):2019070677. doi:10.1681/ASN.2019070677
5. Kraut JA, Kurtz I. Metabolic acidosis of CKD: diagnosis, clinical characteristics, and treatment. Am J Kidney Dis. 2005;45(6):978–993. doi:10.1053/j.ajkd.2005.03.003
6. Bellasi A, Di Micco L, Santoro D, et al. Correction of metabolic acidosis improves insulin resistance in chronic kidney disease. BMC Nephrol. 2016;17(1):158. doi:10.1186/s12882-016-0372-x
7. Dubey AK, Sahoo J, Vairappan B, et al. Correction of metabolic acidosis improves muscle mass and renal function in chronic kidney disease stages 3 and 4: a randomized controlled trial. Nephrol Dial Transplant. 2020;35(1):121–129. doi:10.1093/ndt/gfy214
8. Madias NE. Metabolic acidosis and CKD progression. Clin J Am Soc Nephrol. 2021;16:310–312. doi:10.2215/CJN.07990520
9. Harambat J, Kunzmann K, Azukaitis K, et al. Metabolic acidosis is common and associates with disease progression in children with chronic kidney disease. Kidney Int. 2017;92(6):1507–1514. doi:10.1016/j.kint.2017.05.006
10. Weiner DE, Tabatabai S, Tighiouart H, et al. Cardiovascular outcomes and all-cause mortality: exploring the interaction between CKD and cardiovascular disease. Am J Kidney Dis. 2006;48(3):392–401. doi:10.1053/j.ajkd.2006.05.021
11. Townsend RR. Arterial stiffness and chronic kidney disease: lessons from the Chronic Renal Insufficiency Cohort study. Curr Opin Nephrol Hypertens. 2015;24(1):47–53. doi:10.1097/MNH.0000000000000086
12. Pasch A, Farese S, Gräber S, et al. Nanoparticle-based test measures overall propensity for calcification in serum. J Am Soc Nephrol. 2012;23(10):1744–1752. doi:10.1681/ASN.2012030240
13. Smith ER, Ford ML, Tomlinson LA, et al. Serum calcification propensity predicts all-cause mortality in predialysis CKD. J Am Soc Nephrol. 2014;25(2):339–348. doi:10.1681/ASN.2013060635
14. Abramowitz MK. Metabolic acidosis and cardiovascular disease risk in CKD. Clin J Am Soc Nephrol. 2018;13(10):1451–1452. doi:10.2215/CJN.10120818
15. Kendrick JB, Zelnick L, Chonchol MB, et al. Serum bicarbonate is associated with heart failure in the multi-ethnic study of atherosclerosis. Am J Nephrol. 2017;45(2):118. doi:10.1159/000454783
16. Chen W, Abramowitz MK. Advances in management of chronic metabolic acidosis in chronic kidney disease. Curr Opin Nephrol Hypertens. 2019;28(5):409–416. doi:10.1097/MNH.0000000000000524
17. Raphael KL. Approach to the treatment of chronic metabolic acidosis in CKD. Am J Kidney Dis. 2016;67(4):696–702. doi:10.1053/j.ajkd.2015.12.016
18. Brown DD, Roem J, Ng DK, et al. Low serum bicarbonate and CKD progression in children. Clin J Am Soc Nephrol. 2020;15(6):755–765. doi:10.2215/CJN.07060619
19. Ahmed AR, Lappin D. Oral alkali therapy and the management of metabolic acidosis of chronic kidney disease: a narrative literature review. World J Nephrol. 2018;7(6):117–122. doi:10.5527/wjn.v7.i6.117
20. Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2013;Suppl 3:1–150. doi:10.1038/kisup.2012.71
21. Lnker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713–735. doi:10.1053/j.ajkd.2014.01.416
22. Wesson DE, Simoni J. Acid retention during kidney failure induces endothelin and aldosterone production which lead to progressive GFR decline, a situation ameliorated by alkali diet. Kidney Int. 2010;78(11):1128–1135. doi:10.1038/ki.2010.348
23. Goraya N, Simoni J, Jo C, et al. Dietary acid reduction with fruits and vegetables or sodium bicarbonate reduces kidney injury in individuals with moderately reduced GFR due to hypertensive nephropathy. Kidney Int. 2012;81(1):86–93. doi:10.1038/ki.2011.313
24. Navaneethan SD, Shao J, Buysse J, et al. Effects of treatment of metabolic acidosis in CKD: a systematic review and meta-analysis. Clin J Am Soc Nephrol. 2019;14(7):1011–1020. doi:10.2215/CJN.13091118
25. Raphael KL, Isakova T, Ix JH, et al. A randomized trial comparing the safety, adherence, and pharmacodynamics profiles of two doses of sodium bicarbonate in CKD: the BASE pilot trial. J Am Soc Nephrol. 2020;31(1):161–174. doi:10.1681/ASN.2019030287
26. Melamed ML, Horwitz EJ, Dobre MA, et al. Effects of sodium bicarbonate in CKD stages 3 and 4: a randomized, placebo-controlled, multicenter clinical trial. Am J Kidney Dis. 2020;75(2):225–234. doi:10.1053/j.ajkd.2019.07.016
27. Goraya N, Munoz-Maldonado Y, Simoni J, et al. Fruit and vegetable treatment of chronic kidney disease-related metabolic acidosis reduces cardiovascular risk better than sodium bicarbonate. Am J Nephrol. 2019;49(6):438–448. doi:10.1159/000500042
28. Alva S, Divyashree M, Kamath J, et al. A study on effect of bicarbonate supplementation on the progression of chronic kidney disease. Indian J Nephrol. 2020;30(2):91–97. doi:10.4103/ijn.IJN_93_19
29. BiCARB study group. Clinical and cost-effectiveness of oral sodium bicarbonate therapy for older patients with chronic kidney disease and low-grade acidosis (BiCARB): a pragmatic randomised, double-blind, placebo-controlled trial. BMC Med. 2020;18(1):91. doi:10.1186/s12916-020-01542-9
30. Gaggl M, Aigner C, Cejka D, Sunder-Plassmann G. Fo021 oral sodium bicarbonate supplementation does not affect serum calcification propensity in patients with chronic kidney disease and chronic metabolic acidosis. Nephrol Dial Transplant. 2018;33(suppl_1):i9–i10. doi:10.1093/ndt/gfy104.fo021
31. Kendrick J, Shah P, Andrews E, et al. Effect of treatment of metabolic acidosis on vascular endothelial function in patients with CKD: a pilot randomized cross-over study. Clin J Am Soc Nephrol. 2018;13(10):1463–1470. doi:10.2215/CJN.00380118
32. Aigner C, Cejka D, Sliber C, et al. Oral sodium bicarbonate supplementation does not affect serum calcification propensity in patients with chronic kidney disease and chronic metabolic acidosis. Kidney Blood Press Res. 2019;44(2):188–199. doi:10.1159/000498975
33. Di Iorio BR, Bellasi A, Raphael KL, et al. Treatment of metabolic acidosis with sodium bicarbonate delays progression of chronic kidney disease: the UBI Study. J Nephrol. 2019;32(6):989–1001. doi:10.1007/s40620-019-00656-5
34. Sy J, Chen JLT, Kalantar-Zadeh K. New solutions to old problems-metabolic acidosis in chronic kidney disease. Ann Transl Med. 2020;8(19):1256. doi:10.21037/atm-2020-70
35. Susantitaphong P, Sewaralthahab K, Balk EM, et al. Short- and long-term effects of alkali therapy in chronic kidney disease: a systematic review. Am J Nephrol. 2012;35(6):540–547. doi:10.1159/000339329
36. de Brito-ashurst I, Varagunam M, Raftery MJ, Yaqoob MM. Bicarbonate supplementation slows progression of CKD and improves nutritional status. J Am Soc Nephrol. 2009;20(9):2075–2084. doi:10.1681/ASN.2008111205
37. Wu DYJ, Kilpatrick RD, Dadres S, et al. Association between serum bicarbonate and death in hemodialysis patients: is it better to be acidotic or alkalotic? Hemodial Int. 2010;9(1):87. doi:10.1111/j.1492-7535.2005.1121av.x
38. Kraut JA, Madias NE. Metabolic acidosis of CKD: an update. Am J Kidney Dis. 2016;67(2):307–317. doi:10.1053/j.ajkd.2015.08.028
39. Rosansky SJ. Renal function trajectory is more important than chronic kidney disease stage for managing patients with chronic kidney disease. Am J Nephrol. 2012;36(1):1–10. doi:10.1159/000339327
40. Menon V, Tighiouart H, Vaughn NS, et al. Serum bicarbonate and long-term outcomes in CKD. Am J Kidney Dis. 2010;56(5):907–914. doi:10.1053/j.ajkd.2010.03.023
41. Moranne O, Froissart M, Rossert J, et al. Timing of onset of CKD-related metabolic complications. J Am Soc Nephrol. 2009;20(1):164–171. doi:10.1681/ASN.2008020159
42. Krolewski AS, Niewczas MA, Skupien J, et al. Early progressive renal decline precedes the onset of microalbuminuria and its progression to macroalbuminuria. Diabetes Care. 2014;37(1):226–234. doi:10.2337/dc13-0985
43. Goraya N, Wesson DE. Clinical evidence that treatment of metabolic acidosis slows the progression of chronic kidney disease. Curr Opin Nephrol Hypertens. 2019;28(3):267–277. doi:10.1097/MNH.0000000000000491
44. Lai S, Muscaritoli M, Andreozzi P, et al. Sarcopenia and cardiovascular risk indices in patients with chronic kidney disease on conservative and replacement therapy. Nutrition. 2019;62:108–114. doi:10.1016/j.nut.2018.12.005
45. Kopple JD, Kalantar-Zadeh K, Mehrotra R. Risks of chronic metabolic acidosis in patients with chronic kidney disease. Kidney Int Suppl. 2005;Suppl 67(95):S21–7. doi:10.1111/j.1523-1755
46. Mehrotra R, Kopple JD, Wolfson M. Metabolic acidosis in maintenance dialysis patients: clinical considerations. Kidney Int Suppl. 2003;64(88):S13–S25. doi:10.1046/j.1523-1755
47. Wesson DE, Simoni J, Broglio K, et al. Acid retention accompanies reduced GFR in humans and increases plasma levels of endothelin and aldosterone. Am J Physiol Renal Physiol. 2011;300(4):830–837. doi:10.1152/ajprenal.00587.2010
48. Wesson DE, Jo CH, Simoni J. Angiotensin II receptors mediate increased distal nephron acidification caused by acid retention. Kidney Int. 2012;82(11):1184–1194. doi:10.1038/ki.2012.267
49. Wesson DE, Jo CH, Simoni J. Angiotensin II-mediated GFR decline in subtotal nephrectomy is due to acid retention associated with reduced GFR. Nephrol Dial Transplant. 2015;2015(30):762–770. doi:10.1093/ndt/gfu388
50. Shobeiri N, Adams MA, Holden RM. Vascular calcification in animal models of CKD: a review. Am J Nephrol. 2010;31(6):471–481. doi:10.1159/000299794
51. Dobre M, Yang W, Pan Q, et al. Persistent high serum bicarbonate and the risk of heart failure in patients with chronic kidney disease (CKD): a report from the chronic renal insufficiency cohort (CRIC) study. J Am Heart Assoc. 2015;4(4):e001599–e001599. doi:10.1161/JAHA.114.001599
52. Pasch A, Block GA, Bachtler M, et al. Blood calcification propensity, cardiovascular events, and survival in patients receiving hemodialysis in the EVOLVE trial. Clin J Am Soc Nephrol. 2017;12(2):315–322. doi:10.2215/CJN.04720416
53. Eelderink C, Te Velde-Keyzer CA, Frenay AS, et al. Serum calcification propensity and the risk of cardiovascular and all-cause mortality in the general population: the Prevend study. Arterioscler Thromb Vasc Biol. 2020;40(8):1942–1951. doi:10.1161/ATVBAHA.120.314187
54. Keyzer CA, de Borst MH, van den Berg E, et al. Calcification propensity and survival among renal transplant recipients. J Am Soc Nephrol. 2016;27(1):239–248. doi:10.1681/ASN.2014070670
55. Mannon EC, O’Connor PM. Alkali supplementation as a therapeutic in chronic kidney disease: what mediates protection? Am J Physiol Renal Physiol. 2020;319(6):F1090–F1104. doi:10.1152/ajprenal.00343.2020
56. Weir MR, Townsend RR, Fink JC, et al. Urinary sodium is a potent correlate of proteinuria: lessons from the chronic renal insufficiency cohort study. Am J Nephrol. 2011;36(5):397–404. doi:10.1159/000342966
57. Wahl P, Isakova T, Gutierrez OM, et al. Racial differences in mineral metabolism in the chronic renal insufficiency cohort (CRIC) study. Am J Kidney Dis. 2013;61(4):A98–A98. doi:10.1053/j.ajkd.2012.11.030
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.