")
Back to Journals » Drug Design, Development and Therapy » Volume 18
The Effects of Different Doses of Sufentanil on Intraoperative Cardiovascular Response and Postoperative Recovery in Patients Undergoing Cardiac Surgery: A Retrospective Cohort Study
Authors Li M , Li X, Wu Y, Zhang T, Li M, Chen Y
Received 23 November 2023
Accepted for publication 18 February 2024
Published 23 February 2024 Volume 2024:18 Pages 535—547
DOI https://doi.org/10.2147/DDDT.S449200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Meng Li, Xue Li, Yong Wu, Tianyu Zhang, Mengya Li, Ying Chen
Department of Anesthesiology, The Affiliated Lianyungang Hospital of Xuzhou Medical University, Lianyungang, Jiangsu, People’s Republic of China
Correspondence: Ying Chen, The Affiliated Lianyungang Hospital of Xuzhou Medical University, No. 6 East Zhenhua Road, Lianyungang, Jiangsu, People’s Republic of China, Email [email protected]
Objective: To investigate the correlation between the amount of sufentanil used during anesthesia and intraoperative hemodynamic fluctuation and postoperative recovery in patients undergoing cardiopulmonary bypass (CPB).
Materials and Methods: A retrospective analysis was performed on 454 patients undergoing elective heart surgery under CPB. Patients were divided into two groups according to the amount of sufentanil used during anesthesia: Group L (induced sufentanil 0.4– 0.6 ug /kg, maintained sufentanil 0.01– 0.02 ug/kg/min, n = 223) and Group H (induced sufentanil 4– 6 ug/kg, maintained sufentanil 0.02– 0.03 ug/kg/min, n = 231). Propensity score matching (PSM) was used at a 1:1 nearest-neighbor ratio to compare the two groups. Intraoperative use of vasoactive drugs, spontaneous heart rebound, secondary endotracheal intubation, postoperative mechanical ventilation time, the length of stay (LOS) in ICU, postoperative LOS in hospital, postoperative in-hospital mortality were analyzed.
Results: After matching, a total of 144 patients were included (72 patients in Group L, and 72 patients in Group H). Multivariate logistic regression analysis showed that the dosage of sufentanil during anesthesia was significantly correlated with the utilization rate of intraoperative vasoactive drugs (P < 0.001) and the success rate of spontaneous heart rebound (p = 0.001). The utilization rate of vasoactive drugs decreased significantly in Group H (OR, 0.062; 95% CI, 0.019– 0.200) compared to that of Group L. The success rate of spontaneous heart rebound (OR, 0.187; 95% CI, 0.071– 0.491) was higher in Group H. There were no differences on postoperative recovery outcomes between the two groups.
Conclusion: On the basis of our data, the use of high-dose sufentanil is beneficial to keep the cardiovascular response of patients in a stable state, but there is no significant effect on the quality of early postoperative recovery.
Keywords: sufentanil, extracorporeal circulation, cardiac anesthesia
Cardiovascular disease is the main cause of death in the world, accounting for about 1/3 of all deaths1–3 and is characterized by high incidence, high disability and high mortality. China is one of the countries with the highest cardiovascular mortality,4,5 and the prevalence is still on the rise, which will lead to more and more people face the risk of cardiac surgery. Cardiopulmonary bypass is one of the main methods of treating organic heart disease, and there are many challenges associated with anesthesia.
Patients undergoing cardiac surgery under CPB have special pathophysiological conditions and exhibit lower tolerance to anesthesia. Median sternotomy, cardiac arrest, and aortic cross-clamping will inevitably lead to systemic inflammatory reactions, causing ischemic damage and electrophysiological damage to myocardial tissue.6 In addition, the occurrence of lung injury caused by cardiac insufficiency itself leads to an increase in the incidence of postoperative pulmonary complications and aggravation of symptoms. Sufentanil is the most commonly used opioid in cardiovascular surgery, its analgesic and sedative effect is good, can provide better cardiovascular stability,7–10 and reduce the body’s work in the heart and other organs under anesthesia, thereby increasing the functional reserve of the heart. However, its dosage is still controversial.
Opioids are traditionally recommended for cardiac surgery because of their unique ability to maintain hemodynamic stability during anesthesia and improve cardiovascular responses caused by surgical stimulation.11 However, the different doses of perioperative opioids used in surgeries have been associated with adverse events, including somnolence, respiratory depression and cardiopulmonary arrest.12,13 The previous study has reported that the recommended sufentanil dose during general anesthesia induction is 0.1 ug/kg, not a higher dose.14 Bhavsar et al15 also reported a lower dose of sufentanil, compared with a standard dose, did not enhance fast-track conditions significantly in patients with coronary artery bypass grafting. Recently, the view that opioid-related adverse drug events were previously thought to be more likely to be associated with higher opioid doses is being debated. Some clinical reports have tended to the use of high-dose drugs. Two meta-analyses reported no significant differences were found in the risk of myocardial infarction, stroke, or reintubation when comparing high-dose opioids versus low-dose opioids in cardiac surgery, but low-dose opioid drugs only decreased postoperative intubation time.16,17 However, both the analyses were not specifically focused on the dose of opioids used.
The aim of this study is to evaluate the effects of high-dose sufentanil and low-dose sufentanil on cardiovascular response and short-term postoperative recovery in patients undergoing cardiac surgery under CPB. This study helps to determine whether higher doses of opioid use would be associated with greater perioperative adverse outcomes.
Data and Methods
General Information
This study follows the STROBE statement,18 has been approved by the Medical Ethics Committee of the First People’s Hospital of Lianyungang (KY-20220906001-01), and has applied for an informed consent exemption for the subjects. The study protocol complies with the Declaration of Helsinki. The trial was registered prior to enrollment at the Chinese Clinical Trial Registry (ChiCTR2200066713) on 14/12/2022. Patients aged 18–78 years undergoing elective cardiac surgery under CPB from December 2017 to December 2021 were selected. Inclusion criteria: ASA II–IV, surgical procedures included coronary artery bypass grafting (CABG), surgical correction of valvular disease (aortic, mitral, tricuspid, and pulmonary), combined surgery, surgery for ascending aortic disease, mixed surgery, and other cardiac procedures under CPB. Exclusion criteria: 1) patients requiring special induction; 2) participants in other programs; 3) known drug allergy; 4) pregnancy; 5) chronic renal insufficiency (serum creatinine > 2.0 mg/dL) or impaired liver function (serum bilirubin > 1.2 mg/dL) before surgery; 6) patients with a history of drug and alcohol abuse or long-term pain management with preoperative use of non-steroidal anti-inflammatory drug or opioids; and 7) patients with major intraoperative and postoperative indicators being not available through the case system.
Anesthetic Methods
Fasting for 12 h and no drinking for 4 h before surgery.19 A peripheral venous access was established after the patient was admitted to the room. Electrocardiogram (ECG), oxygen saturation (SpO2), heart rate (HR), and bispectral index (BIS) were routinely monitored. 1% lidocaine without epinephrine, a 5-cc syringe, and a 25-gauge needle will be needed for delivery of the local anesthetic.20 After local anesthesia, invasive blood pressure (IBP) was monitored by ultrasound-guided radial artery catheterization.
Anesthesia Induction
Midazolam 0.01–0.02 mg/kg, etomidate 0.15–0.30 mg/kg, and cis-atracurium 0.15–0.2 mg/kg were given intravenously. There are two induced doses of sufentanil, and the allocation method is random. The induced dose of sufentanil was 0.4–0.6 ug/kg in low-dose group (Group L), and 4–6 ug/kg in high-dose group (Group H). Under a visual laryngoscope, tracheal intubation was performed and volume-controlled ventilation mode was applied. Respiratory parameters were adjusted, RR 10–15 times/min, I:E = 1:2, and PETCO2 35–45 mmHg was maintained. During surgery, lung protective ventilation strategies were performed before and after CPB (including low-tidal VT 6–8 mL/kg according to ideal body weight, administration of 5 cmH2O positive end-expiratory pressure,21 and timely performance of recruitment maneuver, among others); Adjusting FiO222 to enable SPO2 to be maintained over 92% at a minimum level23 without pulmonary ventilation during CPB.21 The right internal jugular vein was punctured under the guidance of ultrasound, and a 7F three-lumen central venous catheter was placed to monitor the central venous pressure (CVP).
Anesthesia Maintenance
0.5–1.0% sevoflurane was inhaled, propofol 2–3 mg/kg/h and cis-atracurium 0.06–0.12 mg/kg/h were infused intravenously, BIS 40–60 was maintained as needed during the surgery. Group L was given sufentanil 0.01–0.02 ug/kg/min, Group H was given sufentanil 0.02–0.03 ug/kg/min. Noradrenaline, dopamine, dobutamine, epinephrine, milrinone, nitroglycerin, and other vasoactive drugs were used to maintain hemodynamics as needed intraoperatively. All patients were sent to the adult cardiac intensive care unit (CICU) for further treatment after surgery. When patients had stable hemodynamics, did not need or required little vasoactive medication (Vasoactive-Inotropic Score VIS ≤ 10), had adequate gas exchange, and did not have any major complications, such as sepsis, renal insufficiency, and neurological problems, and were conscious enough to maintain their normal ventilation, extubation was permitted.
Data Collection
Gender, age, BMI, ASA classification, type of cardiac surgery, prior comorbidities (personal history) including hypertension, diabetes mellitus, atrial fibrillation, chronic heart failure, previous myocardial infarction within 90 days, pulmonary hypertension, cerebral infarction, operation history, chronic obstructive pulmonary disease (COPD), etc. were collected; preoperative left ventricular ejection fraction (LVEF), the success rate of spontaneous heart rebound during operation, the use of vasoactive drugs, the amount of fluid in and out, the amount of blood loss, the transfusion amounts of allogeneic blood and autologous blood, the operation time, the duration of CPB, the amount of sufentanil used during operation, postoperative short-term prognostic indicators including postoperative complications (pulmonary infection, early postoperative respiratory failure, postoperative bleeding, arrhythmia, cerebral infarction…), time of postoperative mechanical ventilation (extubation time, h), LOS in ICU, LOS in hospital, in-hospital mortality, and second intubation rate after operation were also collected.
Postoperative complications were defined according to the criteria used by the European Society of Anesthesiology.24 Pulmonary infection was defined as a patient with a suspected infection who was prescribed antibiotics and met one or more of the following requirements at the same time: new or changed sputum, new or changed lung shadow, fever, and white blood cell count > 12 × 109/L. Early postoperative respiratory failure was defined as PaO2/FiO2 < 200 during ICU care. The occurrence of short-term postoperative complications can be queried from the patient’s in-hospital medical records.
The patients were divided into two groups according to the amount of sufentanil used during the operation: Group L (induced sufentanil 0.4–0.6 ug/kg, maintained sufentanil 0.01–0.02 ug/kg) and Group H (induced sufentanil 4–6 ug/kg, maintained sufentanil 0.02–0.03 ug/kg).
Statistical Analysis
SPSS 25.0 was used for statistical analysis. Propensity score matching (PSM) was performed to reduce the selection deviation and confounding effects between the two groups. Propensity score (PS) was calculated with logistic regression analysis, including covariates such as demographics, preoperative comorbidities, and surgical data. The covariates that have influence on both independent variables and dependent variables are selected for matching. The nearest neighbor method was used for matching at 1:1 (caliper value set to 0.2). After the propensity score was matched, the McNemar test or paired t-test was used to analyze the relationship between sufentanil infusion and major and secondary indicators.
Univariate logistic regression was used to analyze the relationship between each variable and positive results. The variables of P < 0.2 in univariate analysis were included in multivariate logistic regression to further analyze the correlation between outcome indexes and the use of sufentanil. These factors included NYHA (New York Heart Association function class), preoperative atrial fibrillation, type of operation, EF (ejection fraction), CPB time (cardiopulmonary bypass time), gender, preoperative smoking history, preoperative pulmonary hypertension. Patients with missing data on any matching factors were excluded from the propensity score matching analysis.
Results
From December 2017 to December 2021, 472 patients underwent open heart surgery under CPB. Of these, 454 patients were ultimately included in the analysis. Low-dose sufentanil was given intraoperatively in 223 patients and high-dose sufentanil was given intraoperatively in 231 patients (Table 1). After propensity score matching, there were 72 patients in each group (Figure 1). Baseline characteristics after propensity score matching were compared as follows (Table 2).
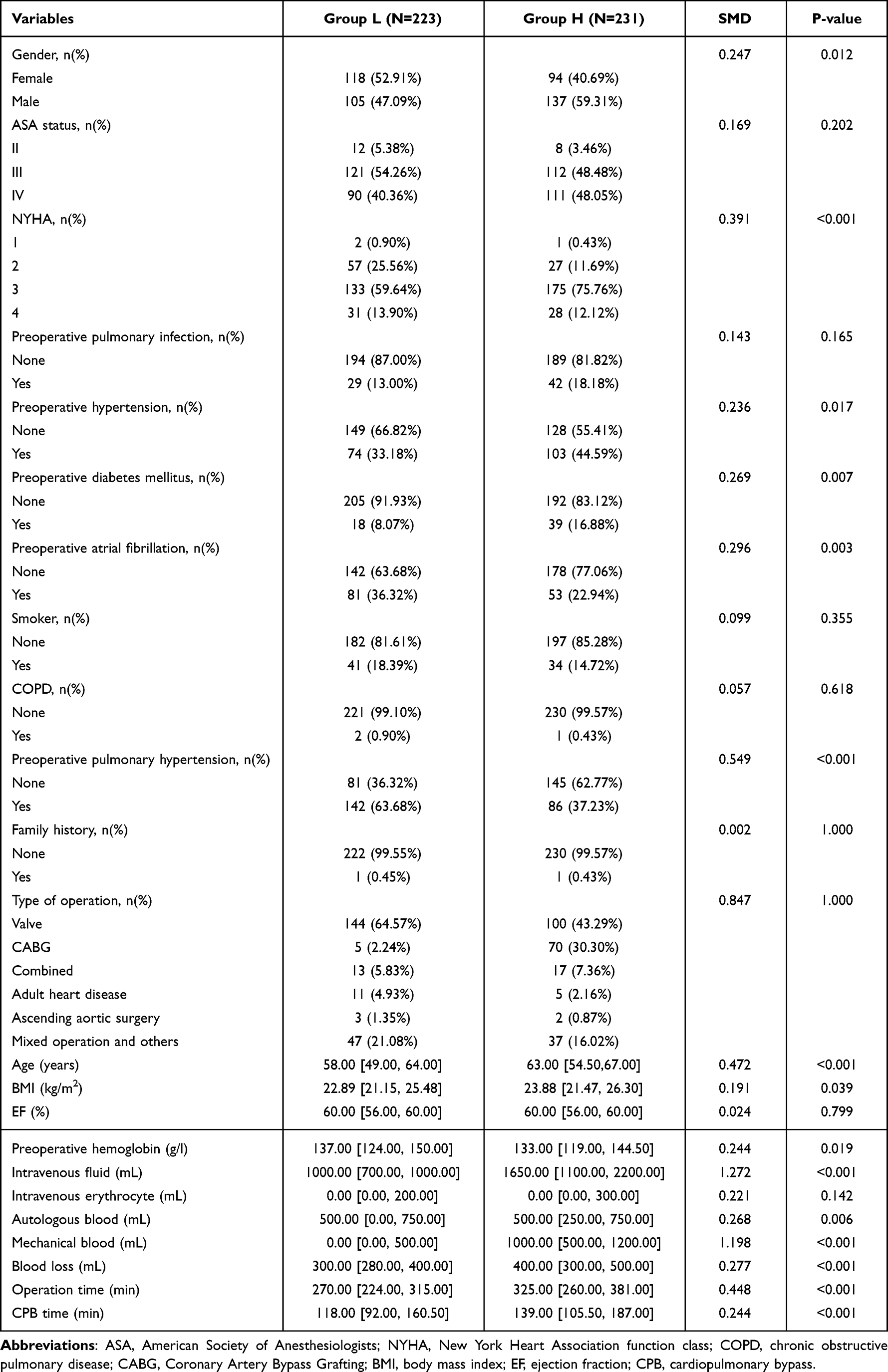 |
Table 1 Comparison of General Conditions Between the Two Groups Before PSM |
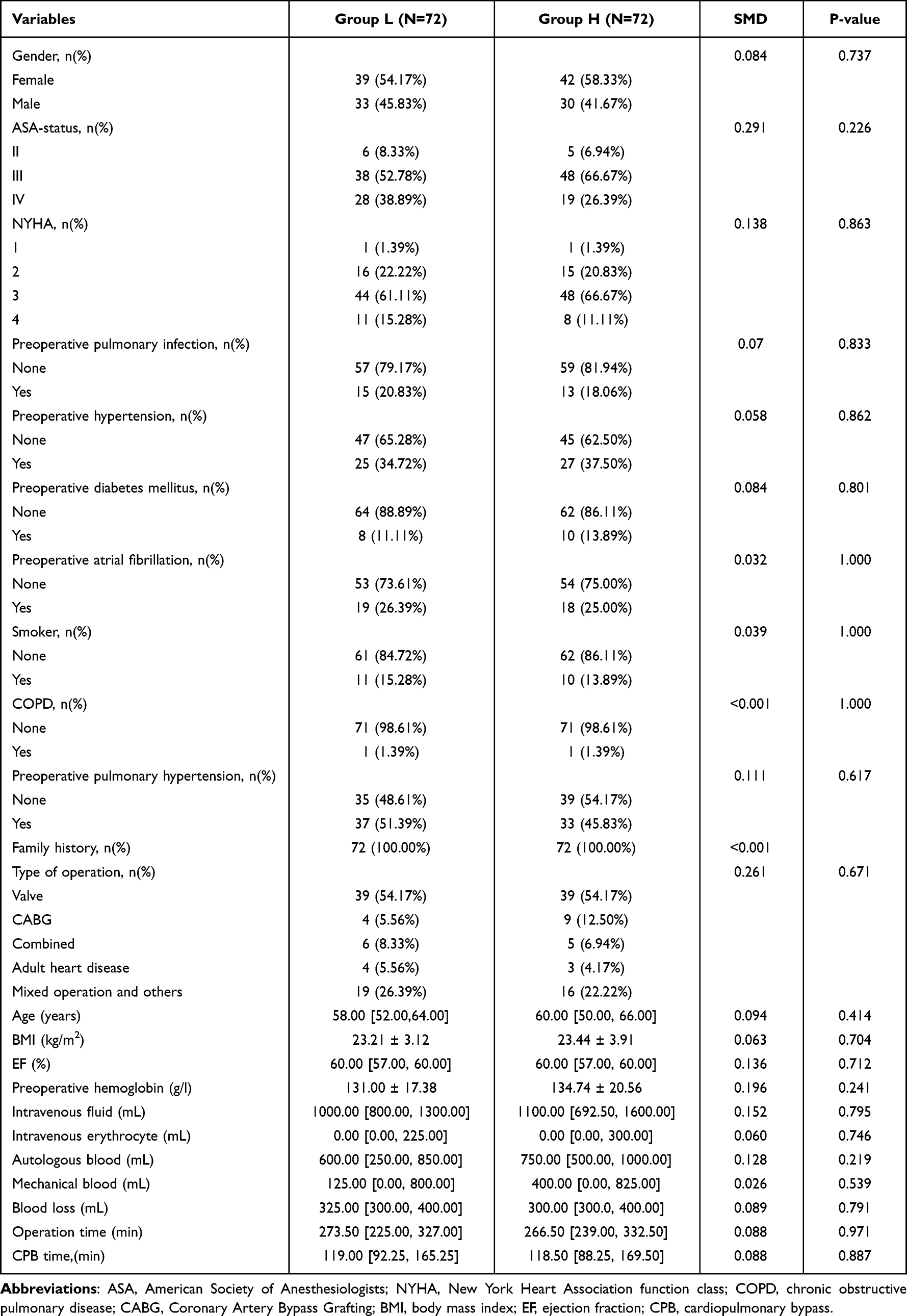 |
Table 2 Comparison of General Conditions Between the Two Groups After PSM |
 |
Figure 1 Flowchart of patient selection. Abbreviation: CPB, cardiopulmonary bypass. |
The matching results of the propensity score showed that there were significant differences in the utilization rate of vasoactive drugs (P < 0.001) and the heart rebound mode (P = 0.005) between high-dose sufentanil group (Group H) and low-dose sufentanil group (Group L). The utilization rate of vasoactive drugs in Group H was significantly lower than that in Group L (Table 3). There were no significant differences in secondary endotracheal intubation (P = 0.620), postoperative mechanical ventilation time (P = 0.701), postoperative LOS in hospital (P = 0.685), LOS in ICU (P = 0.128), and postoperative in-hospital mortality (P = 1.000) between the two groups (Table 3).
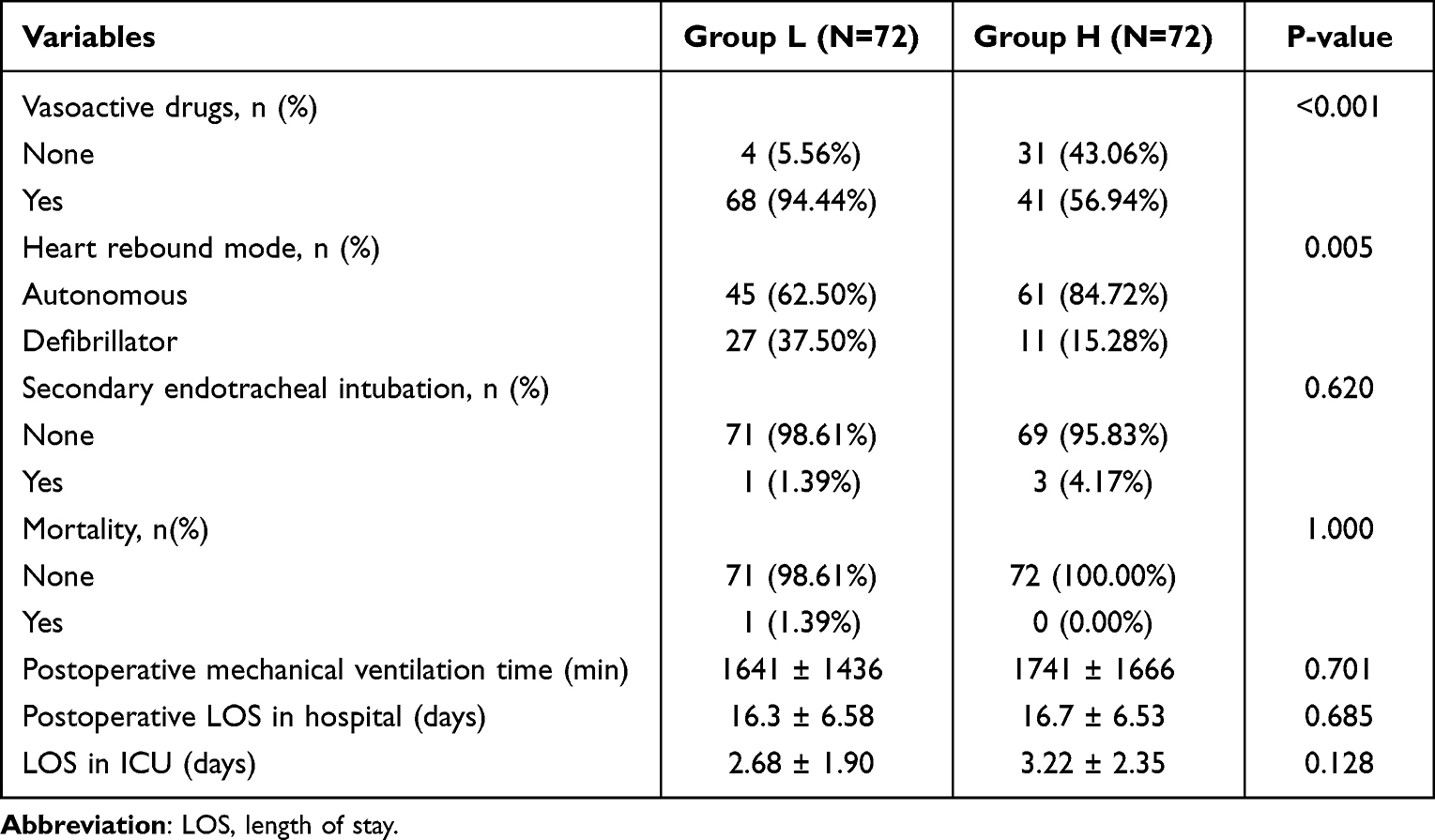 |
Table 3 Comparison of Perioperative Indexes Between the Two Groups After PSM |
According to the univariate regression analysis, intraoperative sufentanil infusion (OR, 0.078; 95% CI, 0.026, 0.236; P < 0.001), preoperative atrial fibrillation (OR, 4.836; 95% CI, 1.384,16.893; P = 0.014), CABG (OR,0.204;95% CI,0.060,0.696;P=0.011) and CPB time (OR,1.009;95% CI,1.001,1.017;P=0.021) were significantly related to the utilization rate of vasoactive drugs. (Table 4). Besides, the univariate regression analysis also showed that the use of sufentanil (OR, 0.301; 95% CI, 0.135, 0.669; P = 0.003), the gender (OR, 2.18; 95% CI, 1.206, 4.63; P = 0.043), preoperative atrial fibrillation (OR,0.182;95% CI,0.052,0.632;P=0.007), preoperative smoking history (OR,3.911;95% CI,1.502,10.183;P=0.005) and CABG (OR,3.383;95% CI,1.016,11.267;P=0.047) were correlated with the heart rebound mode (Table 5).
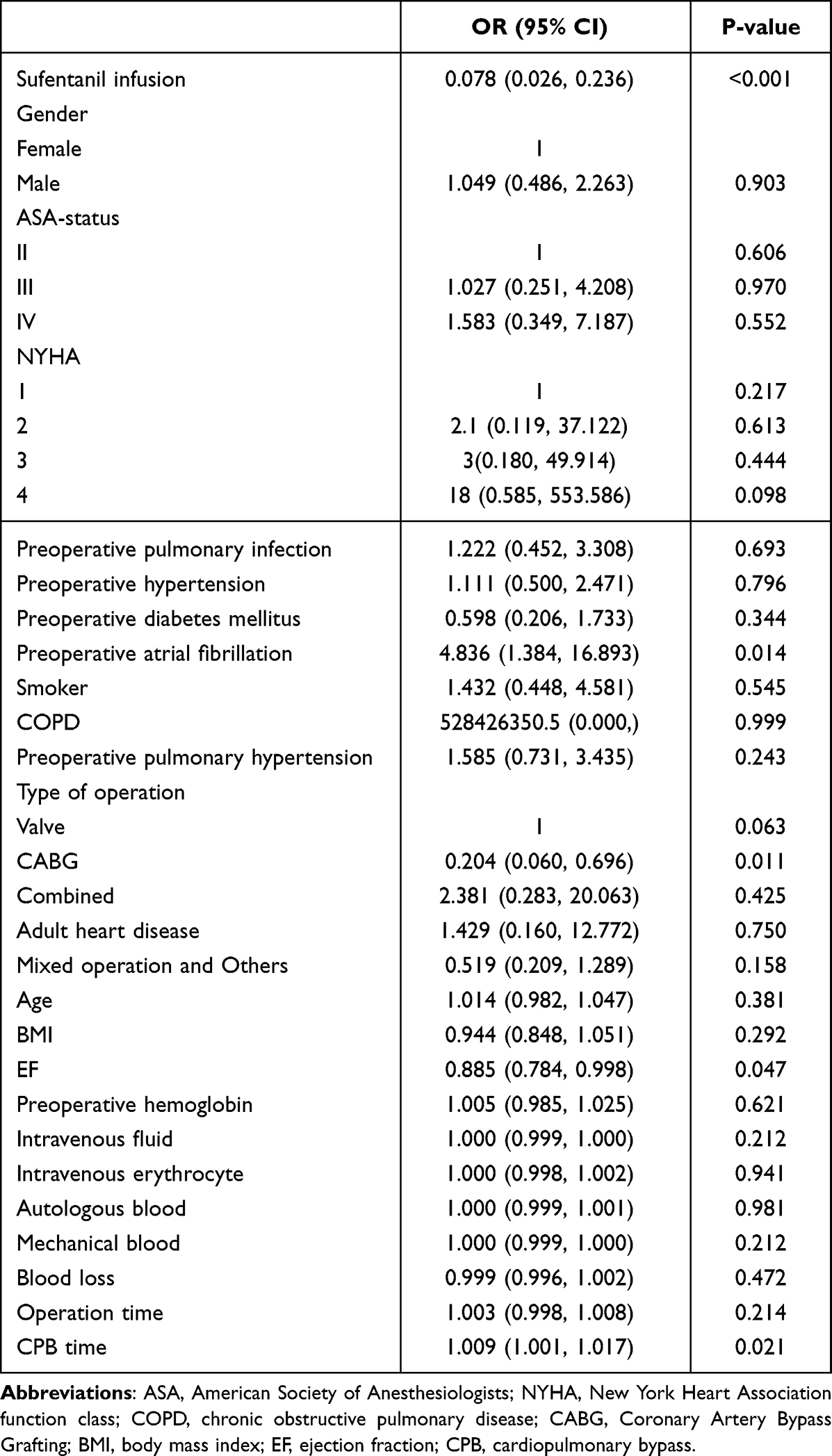 |
Table 4 Results of Univariate Analysis of Variables Associated with Vasoactive Drug Use |
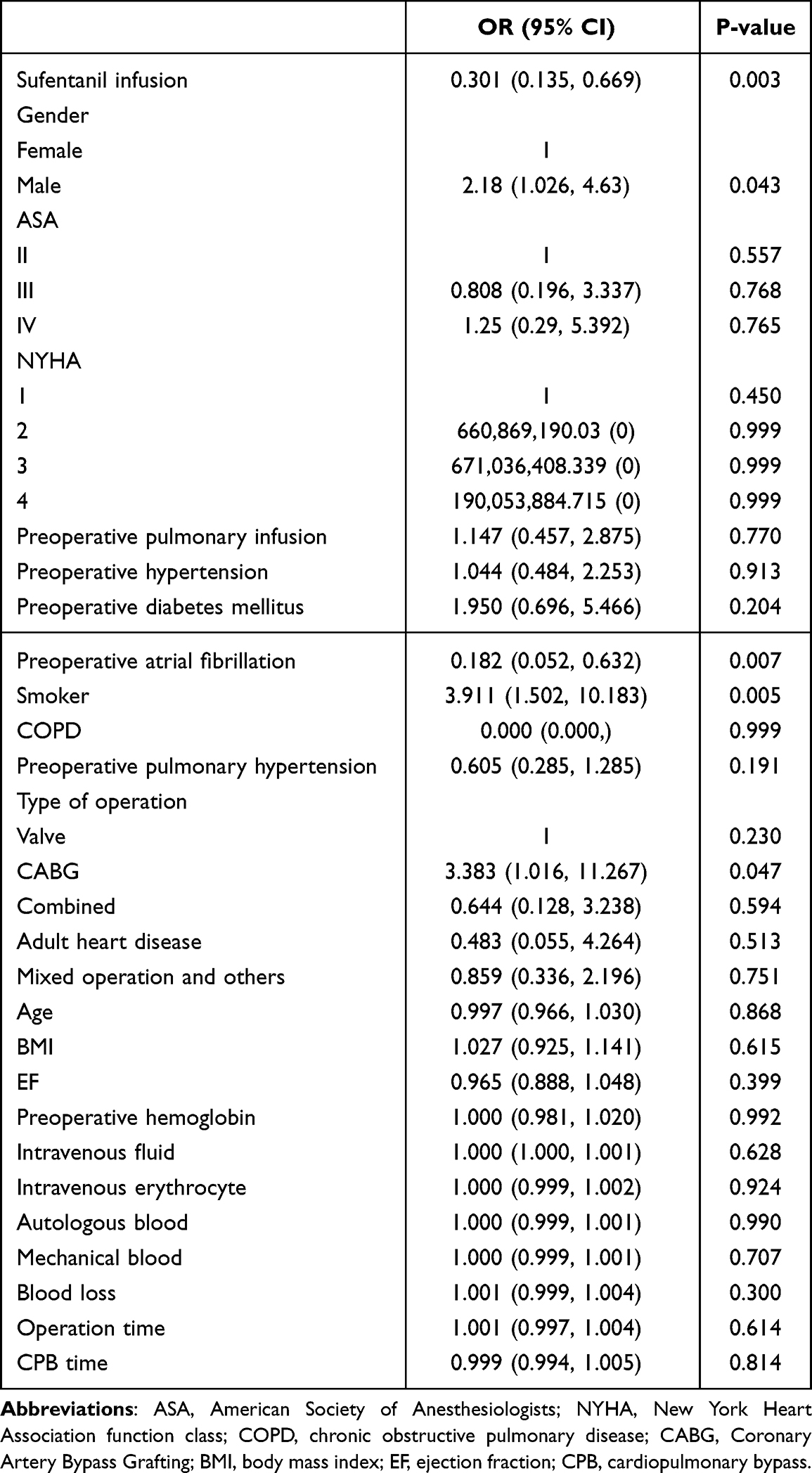 |
Table 5 Results of Univariate Analysis of Variables Associated with Heart Rebound Mode |
The variables of P < 0.2 in univariate regression were included in multivariate logistic regression analysis. The results showed that the intraoperative use of sufentanil was an important factor related to the utilization rate of vasoactive drugs (OR, 0.059; 95% CI, 0.017–0.199; P < 0.001) (Table 6). In addition, multivariate logistic regression analysis showed that intraoperative sufentanil infusion (OR, 0.187; 95% CI, 0.071–0.491; P = 0.001), preoperative history of atrial fibrillation (OR, 0.151; 95% CI, 0.037–0.614; P = 0.008), and preoperative smoking history (OR, 3.578; 95% CI, 1.013–12.630; P = 0.048) were also significant factors affecting the success rate of spontaneous heart rebound (Table 7).
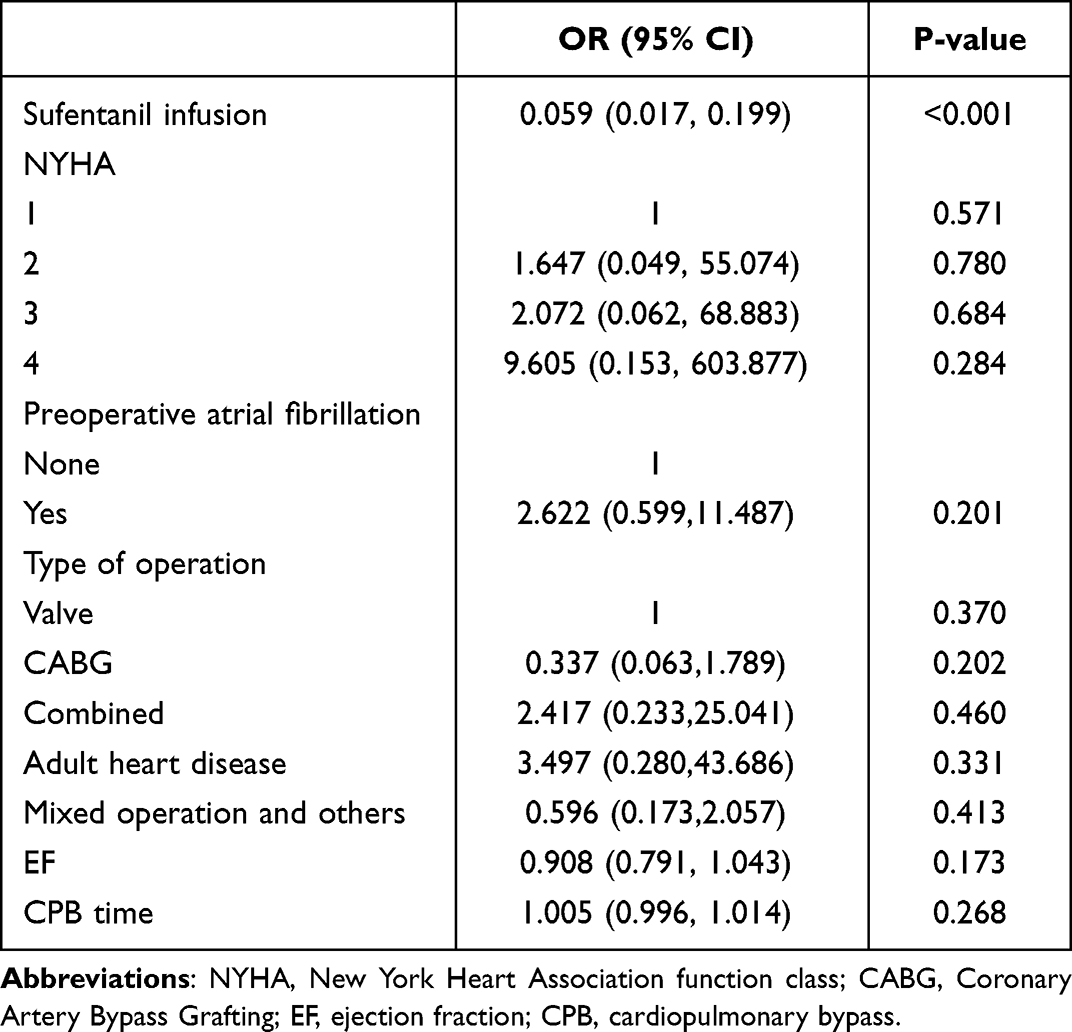 |
Table 6 Results of Multivariate Analysis of Variables Associated with Vasoactive Drug Use |
 |
Table 7 Results of Multivariate Analysis of Variables Associated with Heart Rebound Mode |
Discussion
This single-center retrospective cohort study showed that the use of sufentanil during anesthesia was associated with the use of intraoperative vasoactive drugs and the success rate of spontaneous heart rebound. Propensity score matching results reinforced the reliability of this analysis. Our results showed that, compared with the low-dose sufentanil group, high-dose sufentanil significantly reduced the use of vasoactive drugs during cardiac surgery under CPB and significantly increased the success rate of spontaneous heart rebound. There was no significant correlation in the duration of mechanical ventilation, postoperative LOS in hospital, and LOS in ICU between the two groups.
At present, there is no consensus on the standard of vasoactive drug utilization in cardiac surgery under CPB.25 There are also significant differences in the use of vasoactive drugs among centers.26 The use of large amounts of vasoactive drugs may be associated with an increased risk of organ dysfunction and increased postoperative in-hospital mortality.27,28 In this trial, the utilization rate of vasoactive drugs in the high-dose sufentanil group during surgery was lower than the cohorts in other studies, which was 54.5%. This may be related to the stable hemodynamics during the operation and the low incidence of malignant arrhythmia. Simoni et al29 showed that after the administration of sufentanil, a large peripheral compartment would be formed, resulting in a slow rise of the concentration in the central compartment. Continuous use of sufentanil had less impact on blood pressure and also led to more stable hemodynamics. The use of high-dose sufentanil suppresses the body’s stress responses,30 so that the body’s oxygen consumption during surgery does not increase with enhanced anesthesia and surgical trauma stimuli;30 at this point, the patient can maintain life with the lowest oxygen consumption and the lowest energy consumption during the operation, obtain the maximum functional reserve, and the utilization rate of vasoactive drugs during the operation is correspondingly lower.
Cardiac resuscitation is a crucial part of the concurrent phase after CPB in patients undergoing cardiac surgery. The ideal cardiac resuscitation is when the ascending aorta is opened and the heart can automatically rebound. If a patient fails to undergo spontaneous heart rebound, increases the number of defibrillations, or experiences arrhythmia after the rebound, it is highly likely to affect hemodynamic stability, leading to an extension of the auxiliary circulation period, or even failure to shut down the CPB machine. The patient’s LOS in ICU and hospital will also be prolonged, leading to an increase in complications and a corresponding increase in mortality. Poor myocardial protection during operation is a common cause of difficulty in cardiac resuscitation. In this study, the success rate of spontaneous heart rebound in the high-dose sufentanil group (84.72%) was significantly higher than that in the low-dose sufentanil group (62.5%). This may be related to the mechanism that sufentanil can simultaneously activate μ, κ, and δ opioid receptors. Related studies have shown that κ and δ opioid receptors, alone31 or together,32 are involved in reducing myocardial ischemia-reperfusion injury. Sufentanil binds to opioid receptors on the coronary endothelium, activates the cellular pathway, reduces the production of oxygen free radicals, and accordingly reduces the myocardial damage caused by oxidative stress. To a certain extent, the use of high-dose sufentanil can avoid irreversible myocardial injury and necrosis, improve myocardial energy supply, and maintain electrophysiological stability before the opening of the ascending aorta, which is beneficial to the recovery of cardiac function and smooth heart rebound of patients. In addition, similar to previous studies,33–35 this study confirmed that the history of preoperative smoking and atrial fibrillation were significantly associated with spontaneous heart rebound during CPB. However, multivariate logistics regression analysis did not show a correlation between spontaneous rebound success and other known risk factors, which may be due to the small sample size of this study, or because the medical data of patients undergoing cardiac surgery under CPB were collected and analyzed in only one tertiary medical center. The anesthetic and surgical conditions of all patients are generally similar, so it is difficult to reveal the statistically significant correlation between these variables and the success rate of spontaneous heart rebound.
There were wide differences in the duration of mechanical ventilation after cardiac surgery with CPB.36 This large range may be related to different patient populations, surgical procedures, and anesthesia conditions.37,38 The duration of postoperative mechanical ventilation of participants in this trial was 1899.87 minutes, which was longer than in cohorts from other studies.39 This may be related to the longer intraoperative CPB time (144.75 min), which has been shown in relevant studies to be a major cause of early extubation failure in patients undergoing cardiac surgery.40 According to previous studies, the duration of postoperative mechanical ventilation was associated with preoperative comorbidities and increased with patient age.37,38 Prolonged operative time and excessive intraoperative blood loss are also known risk factors for prolonged postoperative mechanical ventilation.41 The mean age of the patients included in this trial was significantly older than the cohort from other studies. Compared with 95.6% of the patients in this trial, only 50% of the patients in cohorts from other studies had an ASA grade III or above.
The traditional view is that heavy use of opioids in cardiovascular surgery will lead to slow postoperative awakening as well as prolonged mechanical ventilation and LOS in ICU, which is not conducive to postoperative rehabilitation.11,16,42 A multicenter Cochrane Trial43 reported that the use of high-dose opioid anesthesia was associated with prolonged extubation time (3–10.5 h) and LOS in ICU (0.4–8.7 h). However, in this trial, the use of high-dose sufentanil did not significantly extend the duration of postoperative mechanical ventilation in the included patients (P = 0.611). Given the differences in patient management by year and the high heterogeneity reported in this Cochrane report, such differences were not unacceptable. In addition, the study of Michael44 et al also reached a similar conclusion, that is, there was no difference in extubation time and LOS in hospital between the low-dose opioid group and the high-dose opioid group. The mechanisms involved, although unclear, may be related to the favorable anti-inflammatory effects of sufentanil. The use of high-dose sufentanil is effective in preventing acute lung injury and microatelectasis caused by inflammatory cascade after cardiac surgery, thereby preventing the occurrence of postoperative hypoxia, which reduces the incidence of prolonged postoperative mechanical ventilation and the LOS in ICU after cardiac surgery. As a potent opioid analgesic drug, sufentanil has an active metabolite produced in clinical use, which has a further residual effect, contributing to the reduction of postoperative gastrointestinal reactions and the LOS in ICU.
The limitations of this study are as follows: First, this retrospective study has more potential confounding factors than randomized controlled trials. Additionally, some patients were excluded by lack of data. Therefore, there may be selection bias in the samples. Second, the use rate of vasoactive drugs and the rate of spontaneous heart rebound were selected as hemodynamic indicators in this study due to the hemodynamic particularity of cardiac surgery under cardiopulmonary bypass, which can only indirectly reflect the stability of cardiovascular response. Third, the surgical and anesthetic conditions were broadly similar among all patients from a single-center study, making it difficult to reveal statistical associations between the different variables. Finally, the conclusions of this study needs to be further verified through a more comprehensive large-scale, multi-center prospective study.
In summary, the dose of sufentanil during operation was significantly correlated with the utilization rate of vasoactive drugs and the success rate of spontaneous heart rebound among patients who received cardiac surgery under CPB. The high-dose sufentanil had a better intraoperative cardiovascular response than the low-dose sufentanil, but there was no significant difference on the quality of early postoperative recovery.
Data Sharing Statement
All data generated or analyzed during this study are included in the article. Further inquiries about the datasets can be directed to the corresponding author on reasonable request.
Ethical Disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained approval from the Ethics Committee for analysis and publication of routinely acquired clinical data and informed consent was not required for this retrospective observational study.
Disclosure
The authors report no conflicts of interests in this work.
References
1. Aktiz-Biçak E, Kiliç Y, Elmastaş D, et al. Comparison of ultrasound guidance and palpation technique for femoral artery catheterization in children undergoing cardiac surgery. Cir Cir. 2023;91(5):633–640. doi:10.24875/CIRU.23000112
2. Lindstrom M, Decleene N, Dorsey H, et al. Global burden of cardiovascular diseases and risks collaboration, 1990–2021. J Am Coll Cardiol. 2022;80(25):2372–2425. doi:10.1016/j.jacc.2022.11.001
3. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
4. Afshin A, Sur PJ, Fay KA. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393(10184):1958–1972. doi:10.1016/S0140-6736(19)30041-8
5. Roth GA, Mensah GA, Fuster V. The global burden of cardiovascular diseases and risks: a compass for global action. J Am Coll Cardiol. 2020;76(25):2980–2981. doi:10.1016/j.jacc.2020.11.021
6. Pesonen E, Passov A, Salminen US, et al. Heparin binding protein in adult heart surgery. Ann Thorac Surg. 2019;107(4):1154–1159. doi:10.1016/j.athoracsur.2018.10.007
7. Bourdon F, Simon N, Lannoy D, et al. Quality control and stability of ketamine, remifentanil, and sufentanil syringes in a pediatric operating theater. Pediatric Anesthesia. 2019;29(2):193–199. doi:10.1111/pan.13563
8. Derakhshan P, Imani F, Koleini ZS, et al. Comparison of adding sufentanil and low-dose epinephrine to bupivacaine in spinal anesthesia: a randomized, double-blind, clinical trial. Anesth Pain Med. 2018;8(5):e69600. doi:10.5812/aapm.69600
9. Bovill JG, Sebel PS, Blackburn CL, et al. The pharmacokinetics of sufentanil in surgical patients. Anesthesiology. 1984;61(5):502–506. doi:10.1097/00000542-198411000-00004
10. Manfio JL, Santos LM, Carmona MJ, et al. Pharmacokinetic assessment of sufentanil in cardiac surgery. Drug Res. 2013;63(10):495–500. doi:10.1055/s-0033-1343470
11. Rong LQ, Kamel MK, Rahouma M, et al. High-dose versus low-dose opioid anesthesia in adult cardiac surgery: a meta-analysis. J Clin Anesth. 2019;57:57–62. doi:10.1016/j.jclinane.2019.03.009
12. Cine HS, Uysal E. Preemptive caudal anesthesia on back pain after lumbar discectomy: a randomized and controlled study. Cir Cir. 2023;91(5):641–647. doi:10.24875/CIRU.23000311
13. Herzig SJ, Stefan MS, Pekow PS, et al. Risk factors for severe opioid-related adverse events in a national cohort of medical hospitalizations. J Gen Intern Med. 2020;35(2):538–545. doi:10.1007/s11606-019-05490-w
14. Chen P, Zeng P, Gong Y, et al. Recommended dose of sufentanil during induction of general anesthesia to avoid coughing and drastic hemodynamic fluctuations in patients undergoing surgery. Int J Med Res. 2021;49(3):300060521996143. doi:10.1177/0300060521996143
15. Bhavsar R, Ryhammer PK, Greisen J, et al. Lower dose of sufentanil does not enhance fast track significantly-A Randomized Study. J Cardiothorac Vasc Anesth. 2018;32(2):731–738. doi:10.1053/j.jvca.2017.08.018
16. Wong WT, Lai VK, Chee YE, et al. Fast-track cardiac care for adult cardiac surgical patients. Cochrane Database Syst Rev. 2016;9(9):Cd003587. doi:10.1002/14651858.CD003587.pub3
17. Greco M, Landoni G, Biondi-Zoccai G, et al. Remifentanil in cardiac surgery: a meta-analysis of randomized controlled trials. J Cardiothorac Vasc Anesth. 2012;26(1):110–116. doi:10.1053/j.jvca.2011.05.007
18. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S4. doi:10.4103/sja.SJA_543_18
19. Engelman DT, Ben Ali W, Williams JB, et al. Guidelines for perioperative care in cardiac surgery: enhanced recovery after surgery society recommendations. JAMA Surg. 2019;154(8):755–766. doi:10.1001/jamasurg.2019.1153
20. Ailon J, Mourad O, Chien V, et al. Videos in clinical medicine. Ultrasound-guided insertion of a radial arterial catheter. New Engl J Med. 2014;371(15):e21. doi:10.1056/NEJMvcm1213181
21. Wahba A, Milojevic M, Boer C, et al. 2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery. Eur J Cardiothorac Surg. 2020;57(2):210–251. doi:10.1093/ejcts/ezz267
22. Bignami E, Guarnieri M, Saglietti F, et al. Mechanical ventilation during cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 2016;30(6):1668–1675. doi:10.1053/j.jvca.2016.03.015
23. Heinrichs J, Lodewyks C, Neilson C, et al. The impact of hyperoxia on outcomes after cardiac surgery: a systematic review and narrative synthesis. Can J Anaesth. 2018;65(8):923–935. doi:10.1007/s12630-018-1143-x
24. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
25. Mathis MR, Janda AM, Kheterpal S, et al. Patient-, clinician-, and institution-level variation in inotrope use for cardiac surgery: a multicenter observational analysis. Anesthesiology. 2023;139(2):122–141. doi:10.1097/ALN.0000000000004593
26. Vogt W, Läer S. Treatment for paediatric low cardiac output syndrome: results from the European EuLoCOS-Paed survey. Arch Dis Child. 2011;96(12):1180–1186. doi:10.1136/archdischild-2011-300370
27. Sommerfeld O, Von Loeffelholz C, Diab M, et al. Association between high dose catecholamine support and liver dysfunction following cardiac surgery. J Card Surg. 2020;35(6):1228–1236. doi:10.1111/jocs.14555
28. Willems A, Havaux R, Schmartz D, et al. The choice of perioperative inotropic support impacts the outcome of small infants undergoing complex cardiac surgery: an observational study. Minerva Anestesiol. 2023;89(9):753–761. doi:10.23736/S0375-9393.23.16622-3
29. Simoni RF, Pereira AM, Borega Rdos S, et al. Continuous infusion of remifentanil versus sufentanil in videolaparoscopic surgeries. A comparative study. Rev Bras Anestesiol. 2008;58(3):193–201. doi:10.1590/s0034-70942008000300001
30. Bergmann I, Szabanowski T, Bräuer A, et al. Remifentanil added to sufentanil-sevoflurane anesthesia suppresses hemodynamic and metabolic stress responses to intense surgical stimuli more effectively than high-dose sufentanil-sevoflurane alone. BMC Anesthesiol. 2015;15(1):3. doi:10.1186/1471-2253-15-3
31. Jang Y, Xi J, Wang H, et al. Postconditioning prevents reperfusion injury by activating delta-opioid receptors. Anesthesiology. 2008;108(2):243–250. doi:10.1097/01.anes.0000299437.93898.4a
32. Tanaka K, Kersten JR, Riess ML. Opioid-induced cardioprotection. Curr Pharm Des. 2014;20(36):5696–5705. doi:10.2174/1381612820666140204120311
33. Anghel D, Anghel R, Corciova F, et al. Preoperative arrhythmias such as atrial fibrillation: cardiovascular surgery risk factor. Biomed Res Int. 2014;2014:584918. doi:10.1155/2014/584918
34. Jones R, Nyawo B, Jamieson S, et al. Current smoking predicts increased operative mortality and morbidity after cardiac surgery in the elderly. Interact Cardiovasc Thorac Surg. 2011;12(3):1154–1159. doi:10.1510/icvts.2010.239863
35. Shahin Y, Gofus J, Harrer J, et al. Impact of smoking on the outcomes of minimally invasive direct coronary artery bypass. J Cardiothorac Surg. 2023;18(1):43. doi:10.1186/s13019-023-02104-9
36. Jacobs JP, He X, O’brien SM, et al. Variation in ventilation time after coronary artery bypass grafting: an analysis from the society of thoracic surgeons adult cardiac surgery database. Ann Thorac Surg. 2013;96(3):757–762. doi:10.1016/j.athoracsur.2013.03.059
37. Reddy SLC, Grayson AD, Griffiths EM, et al. Logistic risk model for prolonged ventilation after adult cardiac surgery. Ann Thorac Surg. 2007;84(2):528–536. doi:10.1016/j.athoracsur.2007.04.002
38. R BR, G FR, N SJ, et al. Prolonged pulmonary support after cardiac surgery: incidence, risk factors and outcomes: a retrospective cohort study. J Crit Care. 2015;30(5):940–944. doi:10.1016/j.jcrc.2015.04.125
39. Hessels L, G CT, Seevanayagam S, et al. Development and validation of a score to identify cardiac surgery patients at high risk of prolonged mechanical ventilation. J Cardiothorac Vasc Anesth. 2019;33(10):2709–2716. doi:10.1053/j.jvca.2019.03.009
40. I AM, Sharif H, Hamid M, et al. Fast track extubation in adult patients on pump open heart surgery at a tertiary care hospital. J Ayub Med Coll Abbottabad. 2016;28(4):639–643.
41. Nguyen Q, Coghlan K, Hong Y, et al. Factors associated with early extubation after cardiac surgery: a retrospective single-center experience. J Cardiothorac Vasc Anesth. 2021;35(7):1964–1970. doi:10.1053/j.jvca.2020.11.051
42. Myles PS, Daly DJ, Daly D, et al. A systematic review of the safety and effectiveness of fast-track cardiac anesthesia. Anesthesiology. 2003;99(4):982–987. doi:10.1097/00000542-200310000-00035
43. Zhu F, Lee A, Chee YE. Fast-track cardiac care for adult cardiac surgical patients. Cochrane Database Syst Rev. 2012;10:Cd003587.
44. Grant MC, Isada T, Ruzankin P, et al. Opioid-sparing cardiac anesthesia: secondary analysis of an enhanced recovery program for cardiac surgery. Anesthesia Analg. 2020;131(6):1852–1861. doi:10.1213/ANE.0000000000005152
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.