Back to Journals » Journal of Inflammation Research » Volume 18
The Effects of Da-Chai-Hu Decoction Alleviating Pancreatic Exocrine Dysfunction by Inhibiting Endoplasmic Reticulum Stress of Acinar Cell in Mice with Chronic Pancreatitis
Authors Yan Z, Chen X, Cao X ![]() , Fan J, Duan L, Wu N, Xin J, Li X, Xu X, Zhang H
, Fan J, Duan L, Wu N, Xin J, Li X, Xu X, Zhang H ![]()
Received 1 August 2025
Accepted for publication 18 November 2025
Published 22 December 2025 Volume 2025:18 Pages 18009—18024
DOI https://doi.org/10.2147/JIR.S555252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Zhangli Yan,1,2,* Xin Chen,3,* Xin Cao,3,* Jianwei Fan,3 Lifang Duan,3 Nan Wu,4 Jiaqi Xin,4 Xu Li,3 Xiaofan Xu,1,2 Hong Zhang1,2
1Medical Experiment Center, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, 712046, People’s Republic of China; 2Shaanxi International Cooperation Base, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, 712046, People’s Republic of China; 3Basic Medical Academy, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, 712046, People’s Republic of China; 4Comprehensive Cancer Center Münche, Klinikum der Technischen Universität München N, Munich, BY, 81675, Germany
*These authors contributed equally to this work
Correspondence: Xiaofan Xu, Medical Experiment Center, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, 712046, People’s Republic of China, Email [email protected] Hong Zhang, Shaanxi international cooperation base, Shaanxi University of Chinese Medicine, Xianyang, Shaanxi, 712046, People’s Republic of China, Email [email protected]
Background: Chronic pancreatitis (CP) is characterized by significant pancreatic exocrine dysfunction, with limited targeting therapeutic strategies. It has been reported that DCHD can effectively alleviate pancreatic injury in chronic pancreatitis; however, its effect and mechanism on pancreatic exocrine dysfunction remain unclear.
Objective: To investigate the therapeutic effects of Da-Chai-Hu Decoction (DCHD) on pancreatic exocrine dysfunction in CP and explore its underlying mechanisms.
Methods: Thirty male C57BL/6 mice were divided into control, CP model, and three DCHD dose groups (11, 22, 44 g/kg). CP was induced via repeated caerulein injections (50 μg/kg), followed by 3 weeks of DCHD treatment. Histopathological analysis of pancreatic tissue (via HE staining, IHC, IF), molecular assays (Western blot, RT-PCR), and RNA-seq were performed. LC-MS/MS identified chemical components in the serum of DCHD-treated mice, and network pharmacology predicted potential targets. Mouse pancreatic acinar cells (266– 6) exposed to caerulein and PI3K inhibitor LY294002 were treated with DCHD serum to validate pathways.
Results: DCHD not only alleviated pancreatic fibrosis (α-SMA) and inflammation (IL-6), but also maintained the level of Amylase. RNA-seq revealed that DCHD treatment downregulated the expression of genes related to inflammation, fibrosis, apoptosis, and ERS. The bioactive compounds in DCHD serum were identified by LC-MS/MS, and further were linked to PI3K/AKT and ERS pathway through network pharmacology. In vivo validation experiment showed that the expression of PI3K/AKT pathway and ERS markers in pancreatic tissue was significantly reduced in the DCHD group compared with CP mice (P< 0.05). In vitro, serum containing DCHD enhanced the mRNA level of Ptf1-α and Cpa1 which represent pancreatic exocrine function and inhibited ERS, apoptosis, and PI3K/AKT signaling activation in 266– 6 cells stimulated with caerulein. Furthermore, the expression of ERS marker including GRP78 and DDIT3 in acinar cells was significantly inhibited by PI3K inhibitors (LY294002) (P< 0.05). After treatment of LY294002, the effect of DCHD-containing serum alleviating ERS of acinar cells was abrogated.
Conclusion: DCHD suppress ERS by regulating the PI3K/AKT pathway in pancreatic acinar cells and further alleviates pancreatic exocrine dysfunction. This study confirms the therapeutic potential of DCHD in pancreatic exocrine dysfunction, and offers a new therapeutic option for CP with pancreatic exocrine dysfunction.
Keywords: Da-Chai-Hu Decoction, chronic pancreatitis, pancreatic exocrine dysfunction, endoplasmic reticulum stress, PI3K/AKT signaling pathway
Introduction
Chronic pancreatitis (CP) is a progressive inflammatory disease of the pancreas caused by multiple factors, including biliary diseases and long-term alcohol abuse, leading to damage and fibrosis of the pancreatic parenchyma.1 In recent years, with changes in dietary habits and lifestyle, the morbidity of CP has significantly increased.2 CP is characterized by significant pancreatic exocrine dysfunction, but the targeting therapeutic strategies were limited at present.
Da-Chai-Hu Decoction (DCHD), a classical traditional Chinese medicine (TCM) formula, was first documented in Zhang Zhongjing’s Treatise on Typhoid and Miscellaneous Diseases for the treatment of syndromes characterized by “interior-excess heat with liver-gallbladder disharmony”.3 Historically, DCHD has been prescribed to alleviate symptoms such as epigastric rigidity, jaundice, and digestive disorders, which are closely associated with hepatobiliary and pancreatic dysfunction.4,5 Modern pharmacological studies have validated DCHD’s efficacy in regulating hepatobiliary secretion and attenuating pancreatic inflammation, further provide supportive evidence for the utilization of DCHD in digestive disorders and pancreatic impairment.6 Meanwhile, the recently published <Expert consensus on integrated traditional Chinese and Western medicine diagnosis and treatment of chronic pancreatitis (2025)>7 explicitly recommends DCHD as a therapeutic option for CP patients. Our previous studies have revealed that DCHD attenuated pancreatic fibrosis by inhibiting macrophage infiltration and pancreatic stellate cell activation which played essential roles in the progression of CP.3,8,9 However, its effect and mechanism on pancreatic exocrine dysfunction remain unclear. Recently studies have demonstrated that the function of the endoplasmic reticulum of pancreatic acinar cells is impaired and ERS was triggered by inflammatory factor.10 As an important pathological event, ERS can lead to cellular damage and apoptosis, thereby exacerbating the progression of CP.11
This study utilizes a multi omics research framework that integrates transcriptomic analysis, network pharmacology and supplementary in vivo/ in vitro experiments to explore the therapeutic mechanisms of DCHD in alleviating pancreatic exocrine dysfunction by reducing acinar cell damage. Specifically, the aim of this study was to investigate the therapeutic effect of DCHD on pancreatic exocrine dysfunction in CP mice and elucidate the underlying molecular mechanisms, with a specific focus on ERS and its regulating pathway in pancreatic acinar cell.
Materials and Methods
Drugs and Reagents
The DCHD consists of several traditional Chinese medicinal herbs. Chai Hu (Bupleurum chinense DC., SXZY20230036) 15 g, Huang Qin (Scutellaria baicalensis Georgi, SXZY20230515) 9 g, Zhi Shi (Citrus aurantium L., SXZY20231007) 9 g, Shao Yao (Paeonia lactiflora Pall., SXZY20230635) 9 g and Ban Xia (Pinellia pedatisecta Schott, SXZY20230487) 9 g, Da Huang (Rheum palmatum L., SXZY20230182) 6 g, Sheng Jiang (Zingiber officinale Roscoe, SXZY20230398) 15 g and Da Zao (Ziziphus abyssinica Hochst, SXZY20230457) 20 g. All medicines were purchased from the Traditional Chinese Medicine Pharmacy of Shaanxi University of Chinese Medicine Hospital and authenticated by Prof. Hong Zhang. The extraction method and doses of DCHD were based on our previous studies,3,8,9 the standard clinical dose of DCHD for adults is 84 g, which translates to 1.2 g/kg/day for a 70 kg individual. To determine the equivalent dose for mice, a body surface area conversion factor of 9.1 was applied, accounting for the physiological differences between humans and mice. The middle dose was established as the equivalent clinical dose (ECD), with the low dose set at half the ECD and the high dose at double the ECD. Accordingly, the mice in the DCHD-treated groups were administered doses of 11, 22, and 44 g/kg/day, reflecting the weight of the crude DCHD formulation.
Antibodies: GAPDH (BM3874) was purchased from Wuhan Boster Biological Technology Co., Ltd. The following antibodies were purchased from Cell Signaling Technology (USA): Amylase (3796), IL-6 (12,912), α-SMA (19245), PI3K (4292), P-PI3K (4228), AKT (9272), and P-AKT (4060). Collagen I (ab270993), ATF6 (ab37149), and DDIT3 (ab11419) were purchased from Abcam (UK).
Preparation of Medicated Serum of DCHD and LC-MS/MS Analysis
The active compounds of DCHD were identified in our previous study, in the present study we focus on the medicated serum of DCHD. Male C57BL/6J mice (n=20) were administered DCHD (22 g/kg) by gavage for 7 days, and blood was collected two hours after the final gavage. The medicated serum of DCHD was obtained by centrifugation.
The DCHD, medicated serum of DCHD, and Control-serum samples were analyzed using an UPLC-ESI-MS/MS system (UPLC, ExionLC™ AD https://sciex.com.cn/) and Tandem mass spectrometry system (https://sciex.com.cn/). The analytical conditions were as follows, UPLC: column, Agilent SB-C18 (1.8 µm, 2.1 mm * 100 mm); The mobile phase was consisted of solvent A, pure water with 0.1% formic acid, and solvent B, acetonitrile with 0.1% formic acid. Sample measurements were performed with a gradient program that employed the starting conditions of 95%A, 5% B. Within 9 min, a linear gradient to 5% A, 95% B was programmed, and a composition of 5% A, 95% Bwaskept for 1 min. Subsequently, a composition of 95% A, 5.0% B was adjusted within 1.1 min and kept for 2.9 min. The flow velocity was set as 0.35 mL per minute; The column oven was set to 40°C; The injection volume was 2 μL. The effluent was alternatively connected to an ESI-triple quadrupole-linear ion trap (QTRAP)-MS.
Network Pharmacology Analysis
The detected compounds were analyzed using TCMSP (https://old.tcmsp-e.com/tcmsp.php), SWISSADME (http://www.swissadme.ch/), and SwissTargetPrediction (http://www.swisstargetprediction.ch/).12 Compounds with OB > 30 and DL > 0.18 were selected as active substances, and their corresponding target information was retrieved. The target names were converted to standardized Gene Symbols using the UniProt website.
Next, disease-related targets were identified by searching the GeneCards, OMIM, and Disgenet databases using keywords such as “Chronic pancreatitis”, and “Endoplasmic reticulum stress”. The targets of the compounds in DCHD were compared with the disease-related targets using Venny 2.1 online software. GO and KEGG pathway enrichment analyses of the overlapping targets were performed using the Metascape platform. The results were further visualized using the Bioinformatics platform.
This study complies with the requirements specified in 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China. The article stipulates that: When human information, data, or biological samples are used for human-involved life science and medical research under the following circumstances—where the research causes no harm to the human body and does not involve sensitive personal information or commercial interests—ethical review may be exempted.
Animal Experiments
Thirty Male C57BL/6J mice (6–8 weeks old) were obtained from the Experimental Animal Center of Shaanxi University of Chinese Medicine (license number SCXK (Shaanxi) 2021–001) and kept under standard conditions with free access to food and water. The mice were randomly assigned to five groups (n = 6) using a random number table: Control group, CP group, and three DCHD treatment groups (DCHD-L, DCHD-M, DCHD-H). CP and DCHD-treated groups received intraperitoneal injections of caerulein (Toronto Research Chemicals, Toronto, Canada) (50 μg/kg, 6 times/day at 1-hour intervals, 3 times a week) for 4 weeks. The Control group received saline injections. Starting from the 2nd week, the DCHD groups were treated with DCHD-L (11 g/kg), DCHD-M (22 g/kg), or DCHD-H (44 g/kg), while the Control and CP groups were administered an equal volume of saline once daily for 3 weeks. After 3 weeks of treatment, the mice were euthanized, and blood and pancreatic tissue samples were collected for further analysis. The experiment lasted for a total of 4 weeks. All animal experiments were conducted in compliance with the “Guidelines for the Care and Use of Laboratory Animals” and approved by the Animal Ethics Committee of Shaanxi University of Chinese Medicine (approval number: SUCMDL20210301006).
Cell Experiments
Male C57BL/6J mice were administered DCHD (11 g/kg, 22 g/kg, 44 g/kg) by gavage for 7 days, and blood was collected two hours after the final gavage. Pancreatic acinar cells (266–6) were purchased from Nanjing Cobioer Biotechnology Co., Ltd., and cultured in 1640 medium with 10% FBS in a 37°C incubator. Cells were plated at a density of 1×10^6 per well in 6-well plates, stimulated with caerulein (MedChemExpress, HY-A0190; 100 nM), the PI3K inhibitor LY294002 (MedChemExpress, HY-10108; 20 µM) and cultured in 1640 medium with 10% medicated serum of DCHD was administered at concentrations of DCHD-L (11 g/kg), DCHD-M (22 g/kg), and DCHD-H (44 g/kg), according to a previously established protocol,13 and the cells were treated for 24 hours.
H&E, Sirius Red Staining, and Histopathological Analysis
The pancreatic tissue samples were fixed in formaldehyde, dehydrated, and embedded in paraffin. Next, 3 µm sections of the pancreas were obtained and stained with hematoxylin and eosin (H&E) or Sirius Red staining solution. Histopathological scoring of the pancreas was performed according to the results of H&E staining based on previous methods.14,15
Immunohistochemistry and Immunofluorescence Staining
Pancreatic tissues were fixed, dehydrated, paraffin-embedded, and sectioned to 2 μm thickness. The sections were deparaffinized and underwent antigen retrieval. Following incubation with primary and secondary antibodies, images were captured using a microscope with a Zeiss imaging system (Carl Zeiss AG, Oberkochen, Germany). For immunofluorescence double staining, the samples were incubated with matched fluorescent secondary antibodies. After staining the nuclei with DAPI, the slides were sealed using an anti-fade reagent and images were captured with an Olympus IX51 microscope (Olympus, Tokyo, Japan).
RT-qPCR and Western Blot
Total RNA from pancreatic tissues or cells was extracted using a kit from SparkJade (Shandong Sparkjade Biotechnology Co., Ltd., China) and reverse-transcribed into cDNA. RT-PCR amplification was performed using SYBR Green kits with cycling conditions of 95°C for 5 seconds, 60°C for 30 seconds, and 72°C for 30 seconds, for a total of 40 cycles. The RT-PCR products were detected using the ABI-7500 detection system (Thermo Fisher Scientific). The sequences of each quantitative PCR primer are shown in Table 1.
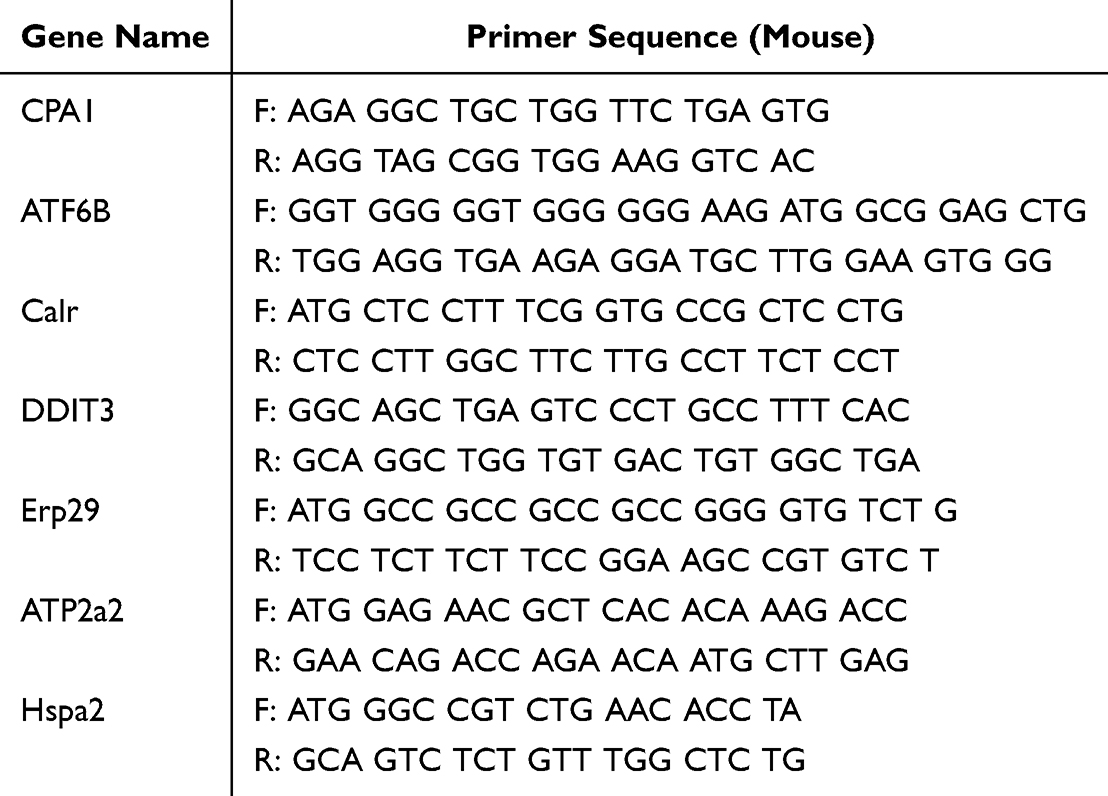 |
Table 1 Primers for Real-Time Fluorescent Quantitative PCR |
For Western blot, pancreatic tissues or cells were homogenized and centrifuged at low temperatures to obtain protein samples. Proteins were transferred to PVDF membranes (EMD Millipore, USA) and incubated with primary antibodies at 4°C overnight, followed by HRP-conjugated secondary antibodies at room temperature for 1.5 hours. Imaging was conducted using the BeyoECL Star chemiluminescence system (Beyotime Biotechnology, Shanghai, China).
Transcriptome Sequencing and Data Analysis
Total RNA was extracted from pancreatic tissue using TRIzol reagent (Invitrogen), and the RNA quality was assessed.16 The purified cDNA fragments were reverse transcribed, followed by ligation of Illumina sequencing adapters and PCR amplification. Sequencing was performed on the Illumina HiSeq2500 platform provided by Gene Denovo Biotechnology Co., Ltd. (Guangzhou, China).
Apoptosis Detection
Cells were fixed with 4% paraformaldehyde at room temperature for 30 minutes, then washed with 0.01M PBS. Each sample received 20 μL of labeling buffer followed by 18 μL of additional labeling buffer. Next, 20 μL of labeling solution was added to each sample and incubated at 37°C for 2 hours. The slides were sealed with anti-fade tablets, and images were captured using an Olympus IX51 microscope (Olympus, Tokyo, Japan).
Statistical Analysis Methods
Data analysis was performed using GraphPad Prism 9.5 software. Continuous data were expressed as mean ± standard deviation (mean ± SD). Normality tests were conducted to ensure the data followed a normal distribution, followed by homogeneity of variance tests to verify if the variances among groups were equal. One-way analysis of variance (ANOVA) was performed to determine significant differences between groups, and post hoc analysis was conducted to further explore differences between specific groups. A P-value < 0.05 was deemed statistically significant.
Results
DCHD Alleviates Pancreatic Damage and Exocrine Dysfunction in CP
CP model in mice was established by caerulein injection. After 4 weeks, the pancreatic tissue volume was significantly reduced (Figure 1A), and the pancreas-to-body weight ratio was markedly decreased (P<0.001) (Figure 1B). The pancreatic structure was severely disrupted, showing acinar cell atrophy, extensive inflammatory cell infiltration, and fibrous tissue deposition (Figure 1C). Following treatment with different concentrations of DCHD, the pancreatic volume, weight, and pathological damage were improved to varying degrees, with a significant reduction in fibrosis. Pathological scores of edemas, inflammation, fibrosis, and acinar atrophy were significantly lower (P<0.05) (Figure 1D). Among the treatments, the medium dose of DCHD (DCHD-M) showed the most effective results. Therefore, the medium dose of DCHD will be the focus in subsequent experiments to explore its therapeutic mechanism in CP.
Figure 1 Continued. Abbreviation: ns, no significant difference. Figure 1 DCHD Alleviates Pancreatic Damage and Exocrine Dysfunction in CP. (A) Representative figures of pancreatic tissues in different groups; (B) Pancreas-to-body weight ratio; (C) H&E staining and Sirius Red staining of pancreatic tissues; (D) Pathological scores based on H&E staining; (E) Representative immunohistochemical staining of amylase in pancreatic tissues (400×); (F) RT-qPCR analysis of Cpa-1 gene expression; (G) Western blot analysis of amylase protein expression levels. The region delineated by the blue dashed box in the upper image of each group is magnified in the corresponding lower image, thus enabling detailed observation of pancreatic tissue alterations. Data are mean ± SD. n=6. *P<0.05, **P<0.01, ***P<0.001. Abbreviation: ns, no significant difference.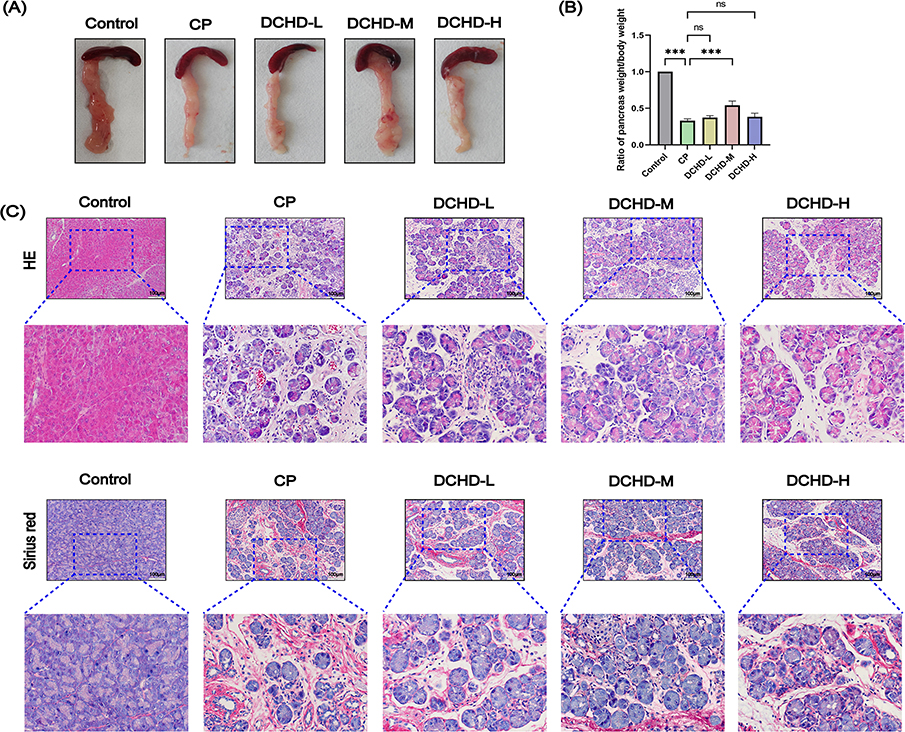
Amylase and Carboxypeptidase A are the primary digestive enzymes secreted by pancreatic acinar cells, and their expression decreases when acinar cells are damaged. Currently, their expression levels are used to measure pancreatic exocrine function.17 In our study, we observed that the amylase positive staining cells were significantly increased (Figure 1E), indicating notable exocrine dysfunction in the pancreatic tissue of the CP group. Additionally, in the CP group, acinar cell damage was accompanied by a significant reduction of Cpa-1 mRNA (Figure 1F) and Amylase protein (Figure 1G) in pancreatic tissue (P<0.05). After treatment with DCHD, the expression of Amylase and Cpa-1 significantly increased (P<0.05), suggesting that DCHD effectively reduces pancreatic inflammation, inhibits fibrosis progression, and protects pancreatic tissue and its exocrine function.
DCHD Reduces Pancreatic Inflammation and Fibrosis in CP Mice
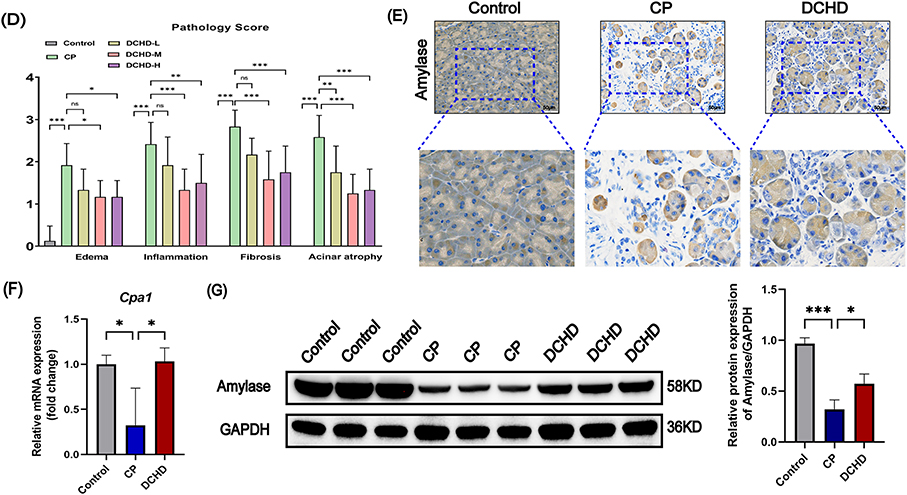
Immunohistochemical staining revealed significantly elevated expression of fi-brosis markers (CollagenI and α-SMA) and the inflammatory marker F4/80 in pancreatic tissues of CP mice compared to the control group, while DCHD treatment markedly reduced their expression (Figure 2A). Subsequently, Western blot analysis demon-strated increased levels of α-SMA and IL-6 in the CP group, which were attenuated by DCHD administration (P<0.05) (Figure 2B). Furthermore, RT-PCR validation con-firmed upregulation of inflammation- and fibrosis-related genes in CP mice, with DCHD significantly suppressing these alterations (P<0.05) (Figure 2C and D). Collectively, these results demonstrate that DCHD alleviates pancreatic inflammation and fibrosis in CP mice.
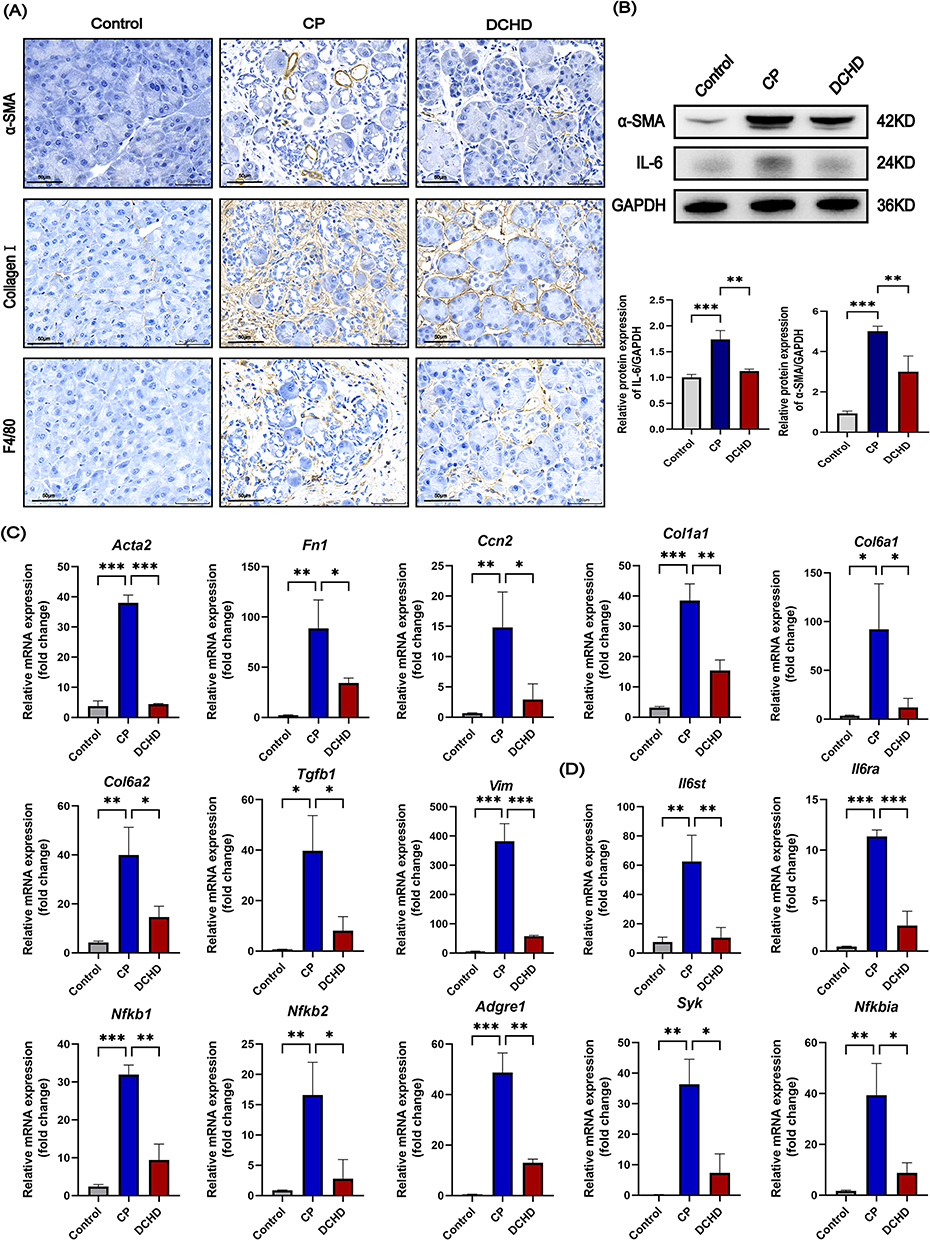 |
Figure 2 DCHD reduces pancreatic inflammation and fibrosis in CP mice. (A) Representative immunohistochemical staining of α-SMA, Collagen I and F4/80 in pancreatic tissues (400×); (B) Western blot analysis of α-SMA and IL-6 protein expression levels; (C and D) RT-qPCR analysis of fibrosis-related genes (C) and inflammation-related genes (D) in CP mice. Data are mean ± SD. n=6. *P<0.05, **P<0.01, ***P<0.001. |
DCHD Attenuates the Expression of mRNAs Correlated with Pancreatic Inflammation, ERS and Fibrosis via PI3K/AKT Signaling Pathway
The RNA-seq results revealed three distinct clusters among the Control, CP, and DCHD groups (Figure 3A), with significant gene expression differences between the groups (Figure 3B). In the CP group, genes related to inflammation (Figure 3C), Fibrosis (Figure 3D), and ERS (Figure 3E) were significantly upregulated, whereas DCHD treatment led to a marked downregulation of these related genes (P<0.05). This suggests that CP progression in mice involves not only inflammation and fibrosis but also ERS and apoptosis. DCHD appears to regulate these key events during CP progression, such as ERS. Further GO and KEGG analyses showed significant enrichment of the PI3K/AKT signaling pathway (ko04151) (Figure 3F–I), indicating that DCHD may exert its therapeutic effects in CP by modulating the PI3K/AKT signaling pathway.
Figure 3 Continued. Figure 3 Transcriptomic Analysis of Pancreatic Tissue. (A) PCA analysis; (B) Volcanic plot shows differences in gene expression; (C–E) Heatmaps display the expression of Inflammation (C), Fibrosis (D) and ERS (E) related differentially expressed genes in each group; (F–I) GO and KEGG enrichment analysis.

The Regulation of ERS by DCHD is Related to PI3K/AKT Pathway Through Analysis of Blood-Entering Components and Network Pharmacology
LC-MS/MS was employed to detect the compounds present in DCHD, control serum and DCHD-medicated serum (Figure 4A). To investigate the variation trend of the relative content of metabolites in different groups, K-means clustering (Figure 4B and C, Table 2) divides the differentially expressed metabolites (DEM) into 9 subcategories, with the abscissa representing the sample groups and the ordinate representing the standardized relative content of metabolites. Subclass 3 metabolites were expressed more in DCHD and medicated serum of DCHD, but less in control serum group, including: 2,5-dihydroxybenzoic acid; Gentisic Acid*Crotonoside; 2-hydroxyadenosine, Cycloleucine, Dihydrosphingosine-1-Phosphate, Guanosine et al which suggested that the above substances that can enter the blood circulation and play a role in DCHD. Therefore, the total ion chromatogram (TIC) profiles of these metabolites obtained through ionic extraction are presented in Figure 4C, the horizontal coordinate represents the retention time (in minutes) of the detected metabolites, and the vertical coordinate represents the ionic current intensity of the detected metabolites. Using the TCMSP, SwissDrugDesign, and SymMap databases, active compounds from DCHD were screened, and target prediction identified 1872 potential targets. Through searches of the Genecards, OMIM, and Disgent disease databases, 1998 CP-related, and 1229 ERS-related targets were identified. An intersection analysis revealed 222 common targets between DCHD, CP, and ERS (Figure 4D). KEGG enrichment analysis of these targets using the Metascape platform indicated that the PI3K/AKT signaling pathway was significantly enriched in both DCHD-CP-ERS (Figure 4E and F), suggesting that the PI3K/AKT signaling pathway may be a key target for DCHD in regulating ERS in CP.
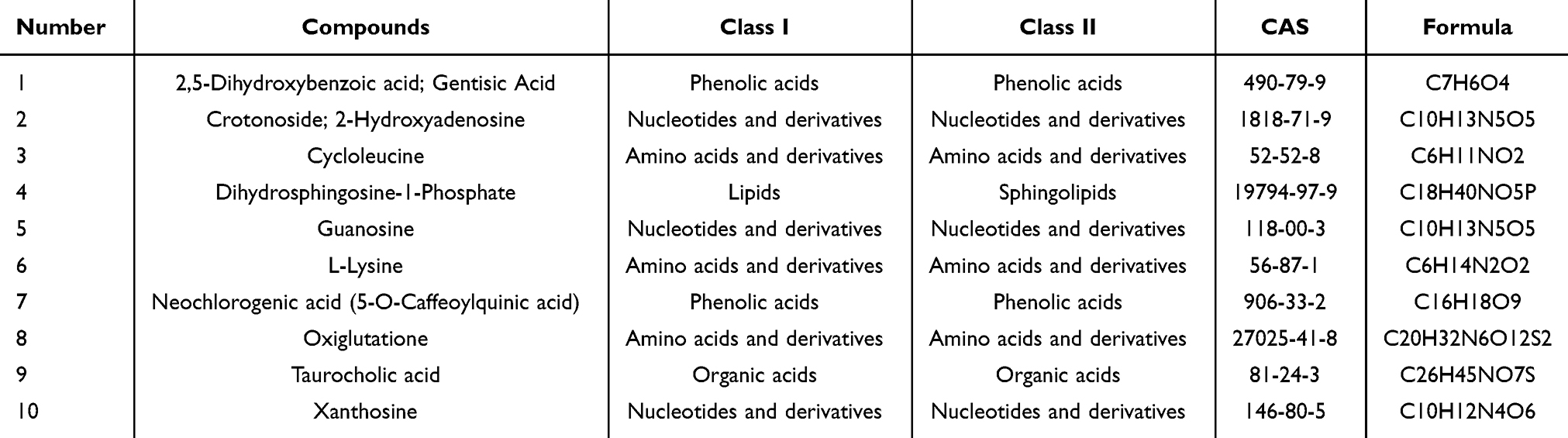 |
Table 2 Compounds Identified from Sub Class3 by UPLC-MS/MS |
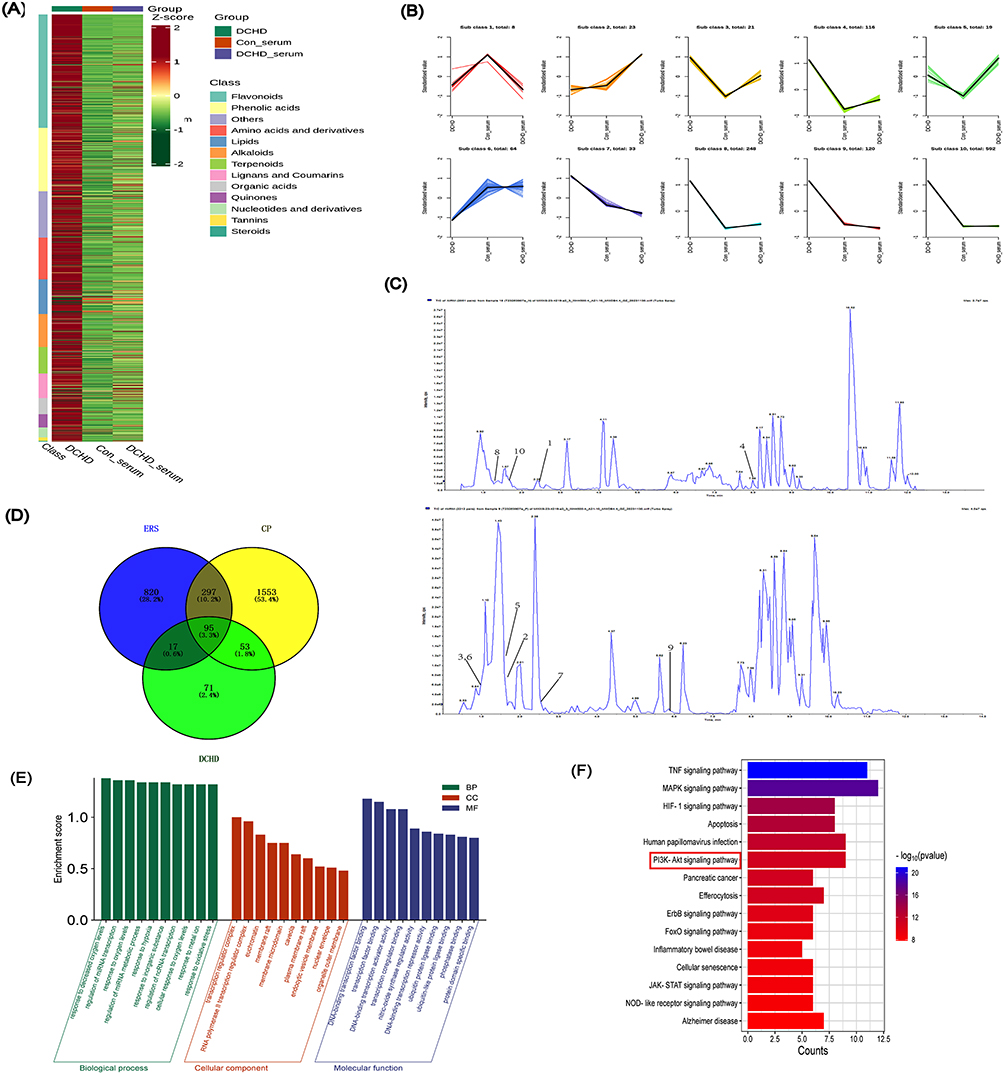 |
Figure 4 Network Pharmacology Analysis of DCHD in Regulating ERS in CP. (A) Clustering of the overall samples; (B) Differential metabolite K-means diagram; (C) Tic diagram of sub class3 metabolites detected by mass spectrometry; (D) Venn diagram showing the overlap between CP, DCHD and ERS related targets; (E and F) GO (E) and KEGG pathway (F) enrichment analysis of DCHD-CP-ERS targets, the area marked by the red dashed box in the figure represents the PI3K/AKT signaling pathway. |
DCHD Inhibited Pancreatic ERS and PI3K/AKT Signaling Pathway in vivo Experiments
To further validate the regulatory effect of DCHD on ERS in CP pancreatic tissues, we examined the expression of ERS markers ATF6, DDIT3, and GRP78.18 The results showed increased expression of ATF6, DDIT3, and GRP78 in the pancreatic tissues of CP mice (P<0.001). After DCHD treatment, the levels of ERS markers were significantly reduced (P<0.001) (Figure 5A), and the expression of ERS-related genes, including Atf6b, Calr, Ddit3, Erp29, Hspa2, and Atp2a2, was also markedly decreased (P<0.05) (Figure 5B), indicating that DCHD can inhibit ERS in the pancreatic tissues of CP mice. To further clarify the expression changes of ERS in pancreatic acinar cells during CP, we conducted immunofluorescence double staining (Amylase/DDIT3). The results showed increased expression of DDIT3 in the acinar cells of the CP group, whereas both markers were reduced following DCHD treatment (Figure 5C). These findings suggest that DCHD can alleviate ERS in acinar cells during the progression of CP.
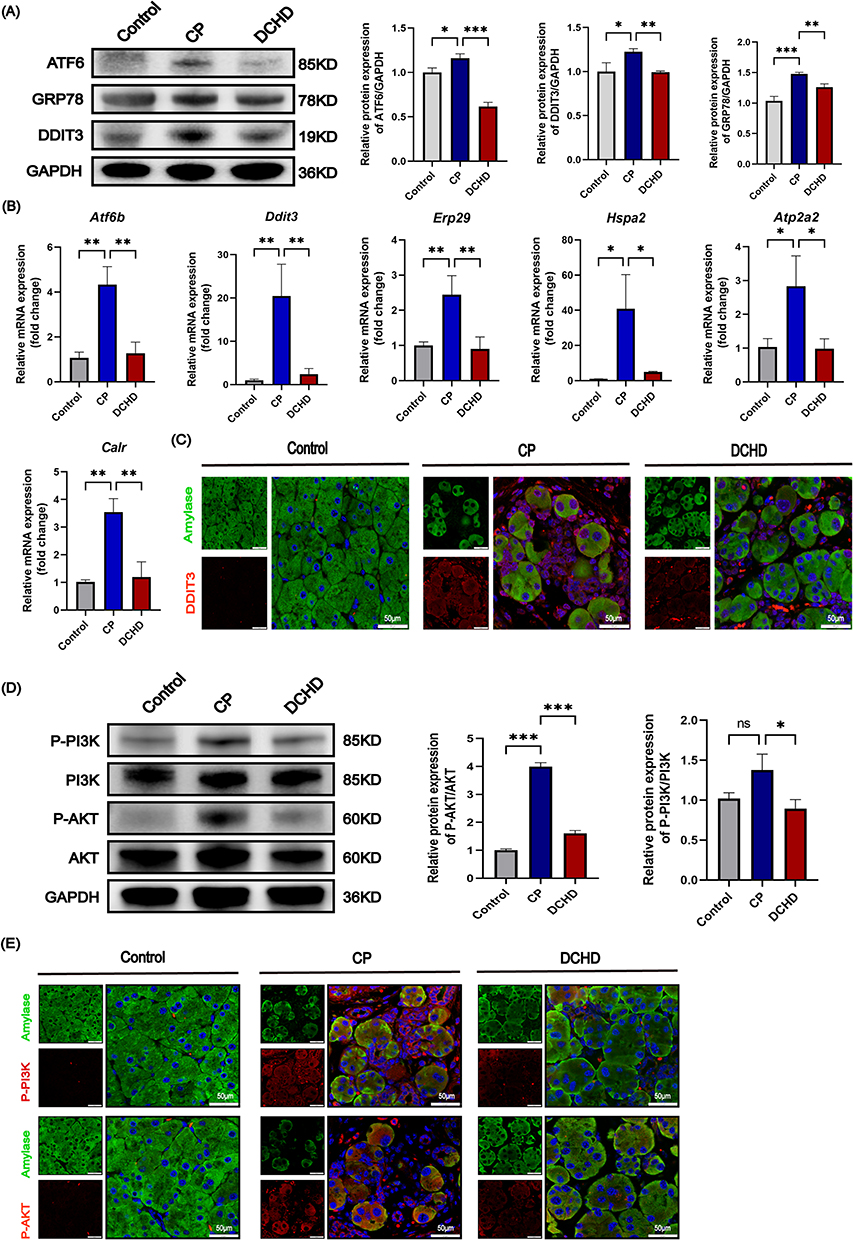 |
Figure 5 DCHD Inhibits Pancreatic ERS in vivo and the Mechanism. (A) Western blot analysis of ERS related proteins ATF6, DDIT3, and GRP78; (B) RT-PCR analysis of ERS related gene; (C) Immunofluorescence double staining showing DDIT3 and Amylase expression; (D) Western blot analysis the protein expression of P-PI3K, PI3K, P-AKT, and AKT; (E) Immunofluorescence double staining of Amylase and P-PI3K, Amylase and P-AKT in pancreatic tissues. Data are mean ± SD. n=6. *P<0.05, **P<0.01, ***P<0.001. Abbreviation: ns, no significant difference. |
Building on the transcriptomic findings, further experiments were conducted to confirm DCHD’s regulatory effect on the PI3K-AKT pathway during CP progression. Western blot analysis indicated elevated P-PI3K and P-AKT levels in CP mouse pancreatic tissues, which were significantly reduced following DCHD treatment (P<0.05) (Figure 5D), it suggests that DCHD can suppress the activation of the PI3K/AKT signaling pathway during CP progression. Additionally, immunofluorescence double staining (Amylase/P-PI3K, Amylase/P-AKT) demonstrated that P-PI3K and P-AKT expression increased in acinar cells of the CP group, but decreased after DCHD treatment, indicating that DCHD inhibits the activation of the PI3K/AKT signaling pathway specifically in pancreatic acinar cells (Figure 5E).
DCHD Attenuated ERS in Pancreatic Acinar Cells by Inhibiting the PI3K/AKT Signaling Pathway and Protected the Pancreatic Exocrine Function
To further explore the intervention effect of DCHD on acinar cells, we treated caerulein-induced 266–6 cells with different concentrations of DCHD-containing serum. After DCHD-containing serum intervention, the expression levels of ATF6, GRP78, and DDIT3 (Figure 6A) and P-PI3K and P-AKT (Figure 6B) in acinar cells were significantly lower compared to the caerulein-stimulated group (P<0.05). Furthermore, intervention with PI3K inhibitors (LY294002) in pancreatic acinar cells, the expression of PI3K was inhibited. At the same time, the expression of ERS related markers GRP78 and DDIT3 in acinar cells was significantly reduced (P<0.05). After treatment of LY294002, the effect of DCHD-containing serum alleviating ERS of acinar cells was abrogated (P<0.05) (Figure 6C).
Figure 6 Continued. Figure 6 Mechanisms of medicated serum of DCHD in regulating ERS in Pancreatic Acinar Cells. (A and B) Western blot analysis of ATF6, GRP78, DDIT3 (A), P-PI3K, P-AKT, PI3K, AKT (B) expression in 266–6 cell treated with or without DCHD-containing serum; (C) Western blot analysis of GRP78, DDIT3, P-PI3K, PI3K expression in 266–6 cell treated with or without PI3K inhibitors (LY294002); (D) RT-PCR analysis the mRNA expression of Bid and Apaf1 in CP and DCHD treated mice pancreatic tissue; (E) TUNEL staining to detect cell apoptosis treated with or without DCHD-containing serum (400×); (F) RT-PCR analysis the expression of Cpa1 and Ptf-1αin 266–6 acinar cell treated with or without DCHD-containing serum; (G) Immunofluorescence staining for amylase in 266–6 cells treated with or without DCHD-containing serum (600×). Data are mean ± SD. n=6. *P<0.05, **P<0.01, ***P<0.001. Abbreviation: ns, no significant difference.

PCR analysis revealed that DCHD treatment significantly downregulated the expression of apoptosis-related genes (Bid and Apaf1) in pancreatic tissue (P<0.001) (Figure 6D). Consistently, TUNEL staining demonstrated a marked reduction in acinar cell apoptosis after intervention with DCHD-containing serum (Figure 6E). Meanwhile, the expression of Cpa1 and Ptf1-α (markers represent the phenotype of acinar cell19) (P<0.01) (Figure 6F) and Amylase (Figure 6G) maintained high level. These results suggest that DCHD may inhibit ERS through the PI3K/AKT signaling pathway, thereby reducing acinar cell apoptosis and protecting pancreatic exocrine function.
Discussion
Chronic pancreatitis (CP) is a chronic inflammatory disease of the pancreas resulting from a complex interplay of genetic, environmental, and other factors.2 CP is typically characterized by persistent epigastric pain radiating to the back, pancreatic exocrine insufficiency, and endocrine dysfunction that often progresses to diabetes mellitus.20 Its etiology and pathogenesis are complex, and there is currently no specific treatment available. Extensive clinical applications have demonstrated DCHD’s efficacy in the management of various gastrointestinal disorders,21 Furthermore, clinical evidence has established its therapeutic potential in significantly ameliorating pancreatitis-associated symptoms, including abdominal pain, nausea, and vomiting. In this study, we found that DCHD alleviated inflammation and fibrosis in pancreatic tissues of caerulein-induced CP mice. Notably, the DCHD-treated group not only exhibited greater preservation of pancreatic acinar cells but also showed significantly increased expression of amylase and Cpa1, suggesting its protective effects against pancreatic exocrine dysfunction in CP. RNA-seq analysis revealed that pancreatic tissues from CP mice exhibited upregulation of genes related to inflammation, fibrosis, and ERS. In contrast, DCHD treatment concurrently suppressed the expression of these inflammation, fibrosis, and ERS-related genes. Recent studies have shown that ERS plays a significant pathogenic role in CP.22 The endoplasmic reticulum, as the primary site for protein synthesis, folding, and modification within cells, can have its function disrupted when responding to intracellular and extracellular stressors such as inflammation, hypoxia, or chemical stimuli. This disruption leads to the accumulation of unfolded or misfolded proteins in the ER, triggering an ERS response.23
Furthermore, double immunofluorescence staining demonstrated that DCHD suppressed ERS in acinar cells during CP progression. It is recognized that upon stimulation by inflammatory factors, pancreatic acinar cells experience impaired endoplasmic reticulum function, leading to disrupted protein synthesis and folding, which subsequently triggers ERS.10 When ERS exceeds the cellular adaptive capacity, it can promote cellular injury and even apoptosis, thereby exacerbating the pathological progression of CP.11 In the present study, we also found that ERS in pancreatic acinar cells is exacerbated during the progression of CP by double immunofluorescence staining, and DCHD could reverse this process. However, the underlying mechanism through which DCHD regulates ERS remains unclear.
Our transcriptomic and network pharmacology analyses revealed a significant enrichment of the PI3K/AKT signaling pathway. The PI3K/AKT signaling pathway, known to regulate cell growth, proliferation, and survival.24,25 Recent studies have revealed that the PI3K/AKT signaling pathway plays a critical role in the progression of acute lung injury by regulating ERS.26 In our present study, in vivo experimental validation demonstrated that DCHD inhibits the activation of the PI3K/AKT signaling pathway in pancreas during CP. These findings suggest that the anti-ERS effect of DCHD in CP may be related to the modulation of the PI3K/AKT signaling pathway. Therefore, we conducted in vitro experiments showing that DCHD-medicated serum alleviated caerulein-induced ERS and PI3K pathway activation in acinar cells. Notably, the protective effect of DCHD was not augmented by a PI3K inhibitor, indicating that DCHD may suppress acinar cell ERS primarily through the PI3K pathway. Furthermore, DCHD downregulated apoptosis-related genes in both pancreatic tissue and acinar cells, thereby mitigating the loss of exocrine function—a primary cause of clinical manifestations such as dyspepsia, steatorrhea, and malnutrition in CP patients.
Although this study confirmed that DCHD exerts a therapeutic effect on CP by improving pancreatic exocrine function through in vivo and in vitro studies, the current research results are only based on experimental models. The protective effect of DCHD on the exocrine function of CP patients remains unclear at present. In the future, it is necessary to conduct multi-center, large-sample clinical controlled studies to verify the protective effect of DCHD on the exocrine function of CP patients, so as to provide more sufficient and reliable evidence support for the clinical transformation and application of DCHD.
Conclusion
In summary, our study demonstrated that DCHD not only alleviates inflammatory damage and fibrosis in CP but also regulates the PI3K/AKT signaling pathway to suppress ERS in pancreatic acinar cells, further improve the pancreatic exocrine function as shown in Figure 7. This study confirms the therapeutic potential of DCHD in pancreatic exocrine dysfunction, and offers a new therapeutic option for CP with pancreatic exocrine dysfunction.
 |
Figure 7 Mechanism diagram of DCHD inhibiting ERS and restoring exocrine pancreatic function in CP. |
Abbreviations
CP, Chronic pancreatitis; DCHD, Dachaihu Decoction; ERS, Endoplasmic Reticulum Stress; DCHD-L, DCHD low-dose group; DCHD-M, DCHD medium-dose group; DCHD-H, DCHD high-dose group; HE, Hematoxylin-eosinstaining; α-SMA, Alpha smooth muscle actin; Collagen I, Collagen type I alpha 1 chain; IL-6, Interleukin 6; Amylase, α-Amylase; GAPDH, Glyceraldehyde-3-phosphate dehydrogenase; ATF6, Activating Transcription Factor 6; GRP78, 78 kDa Glucose-regulated Protein; DDIT3, DNA Damage Inducible Transcript 3; PI3K, Phosphoinositide 3-kinase; AKT, Protein Kinase B; DAPI, 4’,6-diamidino-2-phenylindole; RT-PCR, Reverse Transcription-Polymerase Chain Reaction; PVDF, Polyvinylidene fluoride; HRP, Horseradish Peroxidase; TCMSP, Traditional Chinese Medicines Systems Pharmacology Platform; OB, Oral bioavailability; DL, Drug-like properties; Uniprot, Universal Protein; GO, Gene Ontology; KEGG, Kyoto Encyclopedia of Genesand Genomes; PCA, Principal component analysis.
Data Sharing Statement
The data that support the findings of this study are available from the Xiaofan Xu upon reasonable request.
Ethics Statement
Animal experimental operations were conducted in accordance with the Animal care and handling guidelines and approved by the Animal Ethics Committee of Shaanxi University of Chinese Medicine (Approval number: SUCMDL20210301006).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82174201; 82104815); the Special Support Project for High Level Talents in Shaanxi Province (303/141020047); Qinchuangyuan Traditional Chinese Medicine Industry Innovation Cluster Project in Xianyang City, L2024-QCY-ZYYJJQ-X145.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Cassidy BM, Jiang F, Lin J, et al. Exploring the enigmatic association between PNLIP variants and risk of chronic pancreatitis in a large Chinese cohort. Pancreatology. 2024;24:511–521. doi:10.1016/j.pan.2024.03.002
2. Ashfaq A, Kolanu ND, Mohammed M, et al. Surgical interventions in chronic pancreatitis: a systematic review of their impact on quality of life. Cureus. 2024;16:e53989. doi:10.7759/cureus.53989
3. Li X, Yan Z, Cao X, et al. Dachaihu Decoction alleviates chronic pancreatitis by regulating MAPK signaling pathway: insights from network pharmacology and experimental validation. J Ethnopharmacol. 2025;337:118833. doi:10.1016/j.jep.2024.118833
4. Bi S, Liu Y, Lv T, et al. Preliminary exploration of method for screening efficacy markers compatibility in TCM prescriptions based on Q-markers: anti-inflammatory activity of Dachaihu decoction as an example. J Ethnopharmacol. 2023;312:116539. doi:10.1016/j.jep.2023.116539
5. Ju WJ, Du GL. Analysis of syndrome differentiation and treatment of da-Chai-Hu Decoction based on multivariate symmetry thought in Traditional Chinese medicine. Jiangsu J Tradit Chin Med. 2018;50:68–70. doi:10.3969/j.issn.1672-397X.2018.11.027
6. Liu XX, Ma YQ, Kong LY, Su YZ, Robinson N, Liu JP. Unveiling the therapeutic role of Dachaihu decoction in acute cholecystitis: a comprehensive systematic review and meta-analysis of its efficacy and safety. Front Pharmacol. 2024;15:1497072. doi:10.3389/fphar.2024.1497072
7. Tang WF, Wan MH, Chen X, et al. Expert consensus on integrated Traditional Chinese and Western Medicine diagnosis and treatment for chronic pancreatitis (2025). Chin J Integr Trad West Med Dig. 2025;33:382–394 doi:10.3969/j.issn.1671-038X.2025.04.04.
8. Duan LF, Xu XF, Zhu LJ, et al. Dachaihu decoction ameliorates pancreatic fibrosis by inhibiting macrophage infiltration in chronic pancreatitis. World J Gastroenterol. 2017;23:7242–7252. doi:10.3748/wjg.v23.i40.7242
9. Xu XF, Jiang TT, Liu F, et al. Effect of DaChaiHu Decoction on pancreatic fibrosis induced by DBTC combined with alcohol and the mechanism of TGF-beta/Smad signaling pathway. CJAP. 2016;32:444–448. doi:10.13459/j.cnki.cjap.2016.05.015
10. Lugea A, Gerloff A, Su HY, et al. The combination of alcohol and cigarette smoke induces endoplasmic reticulum stress and cell death in pancreatic acinar cells. Gastroenterology. 2017;153:1674–1686. doi:10.1053/j.gastro.2017.08.036
11. Amit K, Mohd Aslam S, Chandraiah G. Nanoceria ameliorates fibrosis, inflammation, and cellular stress in experimental chronic pancreatitis. ACS Biomater Sci Eng. 2023;9:1030–1042. doi:10.1021/acsbiomaterials.2c00933
12. Nogales C, Mamdouh ZM, List M, Kiel C, Casas AI, Hhhw S. Network pharmacology: curing causal mechanisms instead of treating symptoms. Trends Pharmacol Sci. 2022;43:136–150. doi:10.1016/j.tips.2021.11.004
13. Jin P, Yanting L, Sijia W, et al. Synergistic neuroprotective effects of two natural medicinal plants against CORT-induced nerve cell injury by correcting neurotransmitter deficits and inflammation imbalance. Phytomedicine. 2023;121:115102. doi:10.1016/j.phymed.2023.155102
14. Nan W, Xiao-Fan X, Jia-Qi X, et al. The effects of nuclear factor-kappa B in pancreatic stellate cells on inflammation and fibrosis of chronic pancreatitis. J Cell Mol Med. 2020;25:2213–2227. doi:10.1111/jcmm.16213
15. Xiao-Fan X, Jian-Wei F, Jia-Qi X, et al. Aspirin ameliorates pancreatic inflammation and fibrosis by inhibiting COX-2 expression in experimental chronic pancreatitis. J Inflamm Res. 2022;15:4737–4749. doi:10.2147/JIR.S375383
16. Miyuraj Harishchandra Hikkaduwa W, Hanquan L, Erliang Z. RNA-Seq experiment and data analysis. Methods Mol Biol. 2022;2418:405–424. doi:10.1007/978-1-0716-1920-9_22
17. Fernanda Duarte M, Guilherme FM, Gabriel DMN, Caio EGR, Andrea DG, Alexis FW. Postprandial hyperglycemia in patients with type 2 diabetes is reduced by raw insoluble fiber: a randomized trial. Nutr Metab Cardiovasc Dis. 2023;4753:374–375. doi:10.1016/j.numecd.2023.09.013
18. Donna K, Afshin S, Richard J. Methods for studying ER stress and UPR markers in human cells. Methods Mol Biol. 2015;1292:18. doi:10.1007/978-1-4939-2522-3_1
19. Mei J, Ana CA, Tye GD, et al. MIST1 and PTF1 collaborate in feed-forward regulatory loops that maintain the pancreatic acinar phenotype in adult mice. Mol Cell Biol. 2016;36:2945–2955. doi:10.1128/MCB.00370-16
20. Georg B, Aida H, Jens W, Markus ML, Julia M. Chronic pancreatitis. Lancet. 2020;396:499–512. doi:10.1016/S0140-6736(20)31318-0
21. Ruolei W, Fengjing J, Zhenguo Z, et al. Dachaihu decoction inhibits hypernutrition-induced liver metastasis from colorectal cancer by maintaining the gut vascular barrier. Cancer Pathog Ther. 2023;1:98–110. doi:10.1016/j.cpt.2023.02.003
22. Raghuwansh PS, Sushil KG, Ajay KD, Vikas D, Rajinder KD, Ashok KS. Endoplasmic reticulum stress is chronically activated in chronic pancreatitis. J Biol Chem. 2014;289:27551–27561. doi:10.1074/jbc.M113.528174
23. Amir A, Neil K, Cynthia L, et al. Endoplasmic reticulum stress in liver diseases. Hepatology. 2022;77:619–639. doi:10.1002/hep.32562
24. Ersahin T, Tuncbag N, Cetin-Atalay R. The PI3K/AKT/mTOR interactive pathway. Mol Biosyst. 2015;11:1946–1954. doi:10.1039/c5mb00101c
25. Wang M, Zhang J, Gong N. Role of the PI3K/Akt signaling pathway in liver ischemia reperfusion injury: a narrative review. Ann Palliat Med. 2022;11:806–817. doi:10.21037/apm-21-3286
26. Huang CY, Deng JS, Huang WC, Jiang WP, Huang GJ. Attenuation of lipopolysaccharide-induced acute lung injury by hispolon in mice, through regulating the TLR4/PI3K/Akt/mTOR and Keap1/Nrf2/HO-1 pathways, and suppressing oxidative stress-mediated ER stress-induced apoptosis and autophagy. Nutrients. 2020;12:1742. doi:10.3390/nu12061742
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.