Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 13
The Effects of Amalgam Contamination and Different Surface Modifications on Dentin Shear Bond Strength When Using Different Adhesive Protocols
Authors Alshehri N ![]() , Bin-Shuwaish M
, Bin-Shuwaish M
Received 20 February 2021
Accepted for publication 17 April 2021
Published 27 May 2021 Volume 2021:13 Pages 211—221
DOI https://doi.org/10.2147/CCIDE.S307545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Nojoud Alshehri, Mohammed Bin-Shuwaish
Restorative Dental Sciences Department, College of Dentistry, King Saud University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Nojoud Alshehri
College of Dentistry, King Saud University, Kingdom of Saudi Arabia
Tel +966 11 489 4865
Email [email protected]
Purpose: To evaluate the effect of amalgam contamination, different surface treatments, and adhesive protocols on dentin shear bond strength (SBS) to bulk-fill composite resin material.
Materials and Methods: Eighty teeth were fixed in molds, and the dentin was exposed and then polished. Sixty teeth were restored by amalgam and thermocycled to 10,000 cycles (5°C and 55°C, 30-second dwell time). The rest were restored with composite materials without amalgam predecessor. The samples were divided into G1 (with dentin pretreatment with 2% chlorhexidine gluconate), G2 (0.5 mm of dentin was removed), G3 (no surface modification), and G4 (samples were restored with bulk-fill composite). The bonded specimens were subdivided based on the adhesive protocol of the universal adhesive system used into etch-and-rinse and self-etch groups. Acid etching was done using 32% phosphoric acid. Composite resin was used for build-up using mold and glass. Specimens were cured and left for 24 h in distilled water at room temperature for polymerization reaction, underwent thermocycling for 5000 cycles, and were subjected to knife-edge shear bond testing. Descriptive statistics, independent t-tests, and one-way analysis of variance followed by pairwise comparisons were used to analyze the results.
Results: The highest mean SBS values were found in the control group where acid etching was used (24.46± 2.24 MPa), followed by self-etching in the same group (21.92± 2.54 MPa). Lower SBS values were associated with the amalgam-contaminated group. The lowest values were found in the dentin refreshment group when the self-etching mode was used (13.59± 1.73 MPa). Chlorhexidine treatment improved the mean SBS value compared with the no treatment or dentin refreshment groups for both adhesive protocols.
Conclusion: Amalgam contamination may affect SBS values. Acid etching improved SBS for non-contaminated dentin. Chlorhexidine improved SBS for amalgam-contaminated dentin as a surface treatment but had no significant effect.
Keywords: chlorhexidine, dentin refreshment, resin-based composite, universal adhesive system
Introduction
Amalgam has long been used as the restoration of choice in clinical restorative dentistry.1 These restorations may need to be replaced because of recurrent decay, fracture, esthetics, or marginal defects.2–4
Although secondary caries is more prevalent with the use of resin-based composite (RBC) restoration,5 it is commonly used as a direct replacement of amalgam.6 Continued improvement in the mechanical properties of RBCs have made them good options for the restoration of posterior teeth. The possibility of adhesion to tooth structure, conservative preparation, reasonable cost, and esthetic appearance add to the preference of RBC over amalgam restoration.7 Consequently, RBCs have been described as the “materials of choice” for replacing defective restorations.8
However, when choosing RBC, it is crucial that a clinically reliable adhesive interface is established. Adhesion to dentin may be affected by many factors, such as the material composition, operator technique, polymerization shrinkage of the restoration, the type of substrate, and the quality of the hybrid layer.9 Hence, adhesive technology has advanced markedly in the few past years in an attempt to minimize the adhesive/restoration and adhesive/tooth interface drawbacks. The recently introduced universal adhesive systems combine many advantages, including minimizing clinical steps and improving dentin bonding by incorporating 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP), which promotes chemical adhesion to the substrate, thereby promoting reliable bonding.10
Different surface treatment methods, each with a specific mechanism of action, have been introduced with the aim of improving bond strength to dentin. Some of these surface treatments modify the smear layer, exposing widely opened dentinal tubules; these techniques include phosphoric acid etching and erbium yttrium/aluminum/garnet laser treatment.11 Other methods inhibit the effect of matrix metalloproteinases, which contribute to degradation of the hybrid layer. One of the widely used matrix metalloproteinase inhibitors is chlorhexidine gluconate, which has been successfully used as a strong disinfectant during cavity preparations and was found to improve dentin shear bond strength (SBS) in the long term.12 Although these solutions may be promising, they have been mostly tested on sound tooth structures.
Nevertheless, amalgam restorations corrode with time, with high- and low-copper amalgams corroding comparably.13 These corrosive products were reported to be necessary for sealing the amalgam margins and for compensating for amalgam shrinkage after setting. However, in some cases, dentin underneath the amalgam may become contaminated with corrosive products, such as tin (Sn), zinc (Zn), and copper (Cu).14 Several studies have demonstrated that amalgam contamination can affect bond strength negatively.14–16 A study by Harnirattisai et al15 in 2007 compared the microtensile bond strength of discolored dentin to that of normal dentin, using different adhesive systems after amalgam removal. They found significantly greater bond strength for both adhesives used in non-discolored dentin. In 2016, Scholtanus14 compared the bond strength of discolored dentin containing Zn and Sn corrosive products with sound dentin using five different adhesive systems but found no significant difference between the tested groups and concluded that discolored dentin should be considered a different substrate for bonding and that staining does not impair bonding procedures. However, the study recommended a 3-step etch-and-rinse adhesive system to achieve adequate bond strength.
Reports on the effects of different surface treatments on bond strength of universal adhesive systems for bonding RBC to amalgam-contaminated dentin are scarce. Therefore, this study evaluated the bond strength of bulk-fill RBC bonded to amalgam-contaminated dentin after two different surface treatments: 2% chlorhexidine and removal of 0.5 mm of contaminated dentin. The null hypothesis was that there would be no significant difference in bond strength between the amalgam- and non-contaminated dentin bonded to bulk-fill composite using different surface treatments. A secondary hypothesis was that there would be no significant difference in bond strength between different universal adhesive system protocols.
Materials and Methods
Sample Selection and Sample Size Determination
Eighty extracted non-carious human molar teeth were collected from different clinics (private and governmental) in Riyadh, Saudi Arabia. This project was approved by the ethics committee of King Saud University (IRB number E-19-3846) and all human molar teeth were obtained after informed consent, in accordance with the Declaration of Helsinki. Teeth with caries, previous restorations, cracks, stains, or root canal treatment were excluded from the study. All teeth were cleaned and stored in 0.025% thymol at 4°C for two weeks until used.
Sample size was determined using G*Power 3.1.9.4 (University of Düsseldorf, Düsseldorf, Germany). The sample size was determined to detect an effect size of 0.56-unit difference among four comparison groups, the required number of samples in each group was 9.5 (n=10) at an alpha set to 0.05 and power=0.80.
Study Groups
The 80 teeth were randomly divided into the following groups (20 teeth per group) according to the surface treatments:
- G1: Composite restorations were bonded to the dentin surface that was previously contaminated with amalgam and that was treated with 2% chlorhexidine after amalgam removal, according to the manufacturer’s instructions.
- G2: Composite restorations were bonded to the dentin surface that was previously contaminated with amalgam and that was treated by removal of 0.5 mm of the dentin surface after amalgam removal (dentin refreshment).
- G3: Composite restorations were bonded to the dentin surface that was previously contaminated with amalgam, without any surface treatment after amalgam removal.
- G4 (control): Composite restorations were bonded to the sound dentin surface (without amalgam predecessor).
For each group, teeth were further subdivided into two adhesion subgroups (n=10 per subgroup): those where the adhesive was applied using the etch-and-rinse protocol and where it was applied using a self-etch protocol.
Sample Preparations
Teeth were fixed in a polyvinyl chloride container and embedded in orthodontic resin with the crown of each tooth exposed up to 1 mm below the central pit. For each tooth, the occlusal surface was cut perpendicularly to the long axis of the tooth to expose the dentin using a diamond saw. The specimens were then polished using 200- and 400-grit silicon paper rotating in an Automata grinding and polishing unit (Jean Wirtz Co., Düsseldorf, Germany) for 20 seconds to create a standardized smear layer. Samples were examined under a digital microscope (HiRoX, Tokyo, Japan) at 50x magnification to verify that no enamel islands were left.
Sample Treatments
Table 1 shows the materials used in the study. A customized polyvinyl putty index (6 mm in diameter and 4 mm in height) was fabricated to facilitate ease of amalgam condensation over the fresh dentin. Four high copper amalgam (Futura; Ardent, Arlandastad, Sweden) pins of 1 mm in diameter and 1 mm depth were placed at the four corners of the dentin surface of 60 teeth (G1, G2, and G3) using a suitable bur to facilitate amalgam fixation over dentin during the aging process and for ease of amalgam removal before composite bonding. The areas containing the amalgam pins were excluded from the subsequent composite bonding and testing. The putty index was removed after amalgam setting. Samples were then thermocycled for 10,000 cycles between 5°C and 55°C with a 30-second dwell time.17
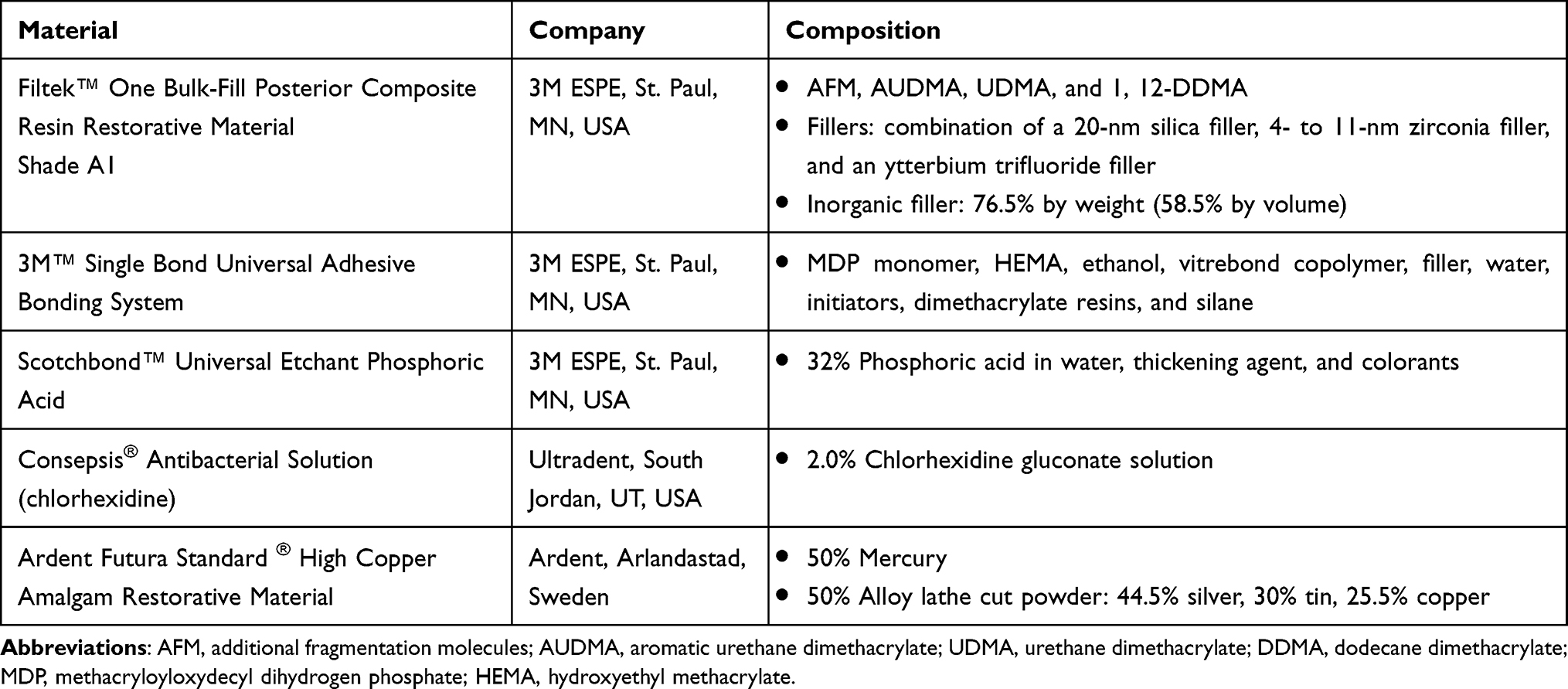 |
Table 1 Materials Used in the Study |
After thermocycling and careful removal of the amalgam, the amalgam restorations were replaced with Filtek Bulk one-fill restorative (A1 shade) (3M ESPE, St. Paul, MN, USA) using a universal adhesive system (Scotchbond Universal Adhesive; 3M ESPE, Maplewood, MN, USA) in each of two adhesion modes: etch-and-rinse and self-etch. In the etch-and-rinse protocol, the dentin surface was etched with 32% phosphoric acid (Scotchbond Universal Etchant; 3M ESPE, St. Paul, MN, USA) for 15 seconds, then washed for 15 seconds. Samples were dried using a cotton pellet, leaving the dentin moist. Using a microbrush, the adhesive was rubbed into the dentin surface for 20 seconds, air-dried for 5 seconds to evaporate the solvent, and light-cured for 10 seconds. In the self-etch protocol, the same steps were performed as in the etch-and rinse protocol but without acid etching.
Before composite bonding, two surface treatments were applied: 2% chlorhexidine di-gluconate (chlorhexidine) (Consepsis Cavity Cleanser; Bisco Inc., Schaumburg, IL, USA) or removal of 0.5 mm of amalgam-contaminated dentin.
Customized putty molds with height of 4 mm and diameter of 4 mm were fabricated to bond composite resin cylinders to the prepared dentin surfaces. Composite resin restorations were packed and light-cured in a single layer by means of a light-emitting diode curing system (Bluephase G2; Ivoclar Vivadent, Schaan, Liechtenstein) for 20 seconds using 1200 mW/cm2 light intensity. A glass slab was positioned to cover the top of the composite restorations before and during curing. After curing five teeth in each group, a radiometer (Demetron LED Radiometer, Kerr, Detroit, MI, USA) was used to check light intensity to ensure sufficient energy. Specimens were cured and left for 24 h in distilled water at room temperature for polymerization reaction. Samples were then thermocycled for 5000 cycles between 5°C and 55°C with a 30-second dwell time.
SBS Test
Specimens were subjected to knife-edge SBS testing at a cross-head speed of 1 mm/minute and 50 kg/f load cell until fracture. The values were calculated in newtons. SBS values were calculated as the ratio of the fracture load and bonding area and was expressed in megapascals (MPa) using Bluehill 3 software and a universal testing machine (Instron 5965; Instron Corp, Norwood, MA, USA).
Failure Mode Examination
De-bonded specimens were examined under a digital microscope at 50x magnification to evaluate the fracture pattern. Failure modes were classified as follows:
- Adhesive failure: failure at the bond interface.
- Composite Cohesive failure: failure within the restorative material.
- Dentin Cohesive failure: failure within the dentin.
- Mixed failure: failure that is partially adhesive and partially cohesive.
Statistical Analysis
Descriptive statistics such as mean, standard deviation, and minimum and maximum values were calculated for each subgroup. Pretest failures were excluded from statistical analyses. The independent t-test was used for intragroup comparison of shear values. One-way analysis of variance was used for intergroup comparison, followed by pairwise comparison or Tukey’s post hoc test. The results were deemed statistically significant at p<0.05, and all statistical analyses were performed using Stata/SE version 16.1 (StataCorp, College Station, TX, USA).
Results
The highest mean SBS values were found in G4 where acid etching was used, whereas the lowest SBS value was found related to the dentin refreshment group (G2) when the self-etching mode was used. Chlorhexidine treatment (G1) showed higher mean SBS values in comparison with the no treatment (G3) or dentin refreshment groups (G2) for both adhesive protocols. Figure 1 represents the SBS mean values among the different treatment groups for both adhesive protocols.
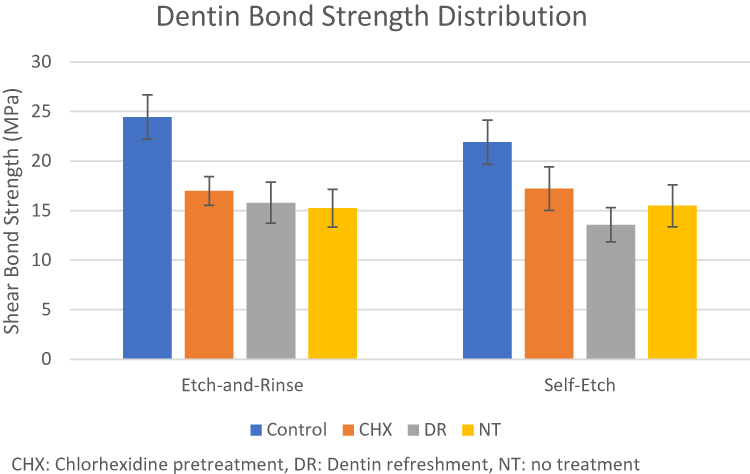 |
Figure 1 Shear bond strength (MPa) in all tested groups. |
SBS by Adhesion Protocols
Etch-and-Rinse Mode
The ANOVA results for study groups comparisons are presented in Table 2. In teeth in which the etch-and-rinse mode of adhesion was used, G4 showed the highest mean SBS value compared with all the treated groups (p<0.05). The second highest SBS value was obtained with chlorhexidine pretreatment (G1). Although this SBS value was higher than that obtained by dentin refreshment (G2) or no treatment (G3) of amalgam-contaminated dentin, the differences were not statistically significant (p>0.05). Dentin refreshment had almost the same mean SBS as the non-modified dentin (p>0.05).
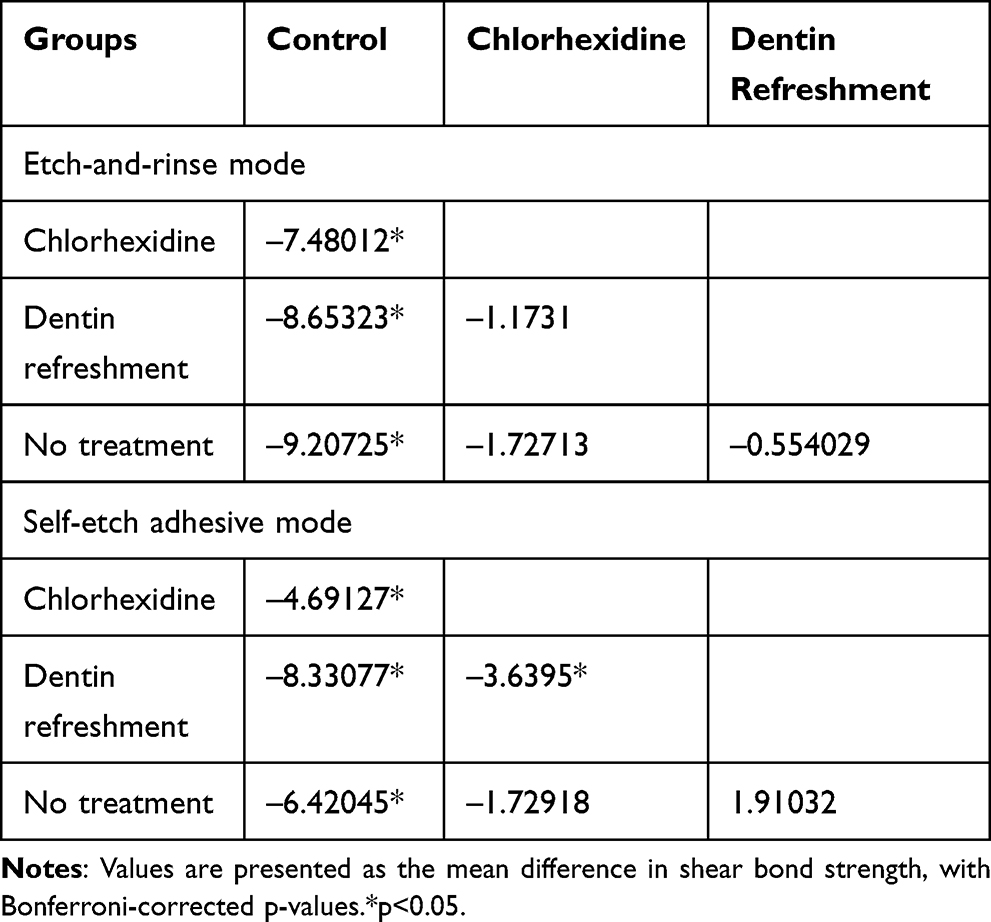 |
Table 2 ANOVA Test Results for the Study Groups Comparison for Each Adhesive Protocol |
Self-Etch Mode
Similar to the etch-and-rinse mode, when the self-etch mode of adhesive was used, the control group (G4) showed the highest mean SBS value (p<0.05). SBS in the group with chlorhexidine pretreatment (G1) was significantly higher than that of the group with dentin refreshment (G2) (p<0.05) but not of that of the non-modified group (G3). Non-modified dentin (G3) had a higher mean SBS than did the dentin refreshment group (G2), but the difference was not significant (p>0.05).
SBS by Dentin Pretreatment
An independent t-test with unequal variances was used for intragroup comparisons for each dentin pretreatment group (Table 3). In the control group (G1), etch-and-rinse adhesion resulted in a significantly higher mean SBS value than did self-etched dentin (p=0.017). Chlorhexidine-pretreated (G2) teeth had higher mean SBS values when using the self-etch than etch-and-rinse mode, but the difference was not significant (p= 0.767). In the dentin refreshment group (G2), the etch-and-rinse subgroup showed significantly higher SBS (p=0.019) than did the self-etched subgroup. In the no treatment group (G3), there was no significant difference between the etch-and-rinse and self-etched dentin in terms of mean SBS values (p=0.787).
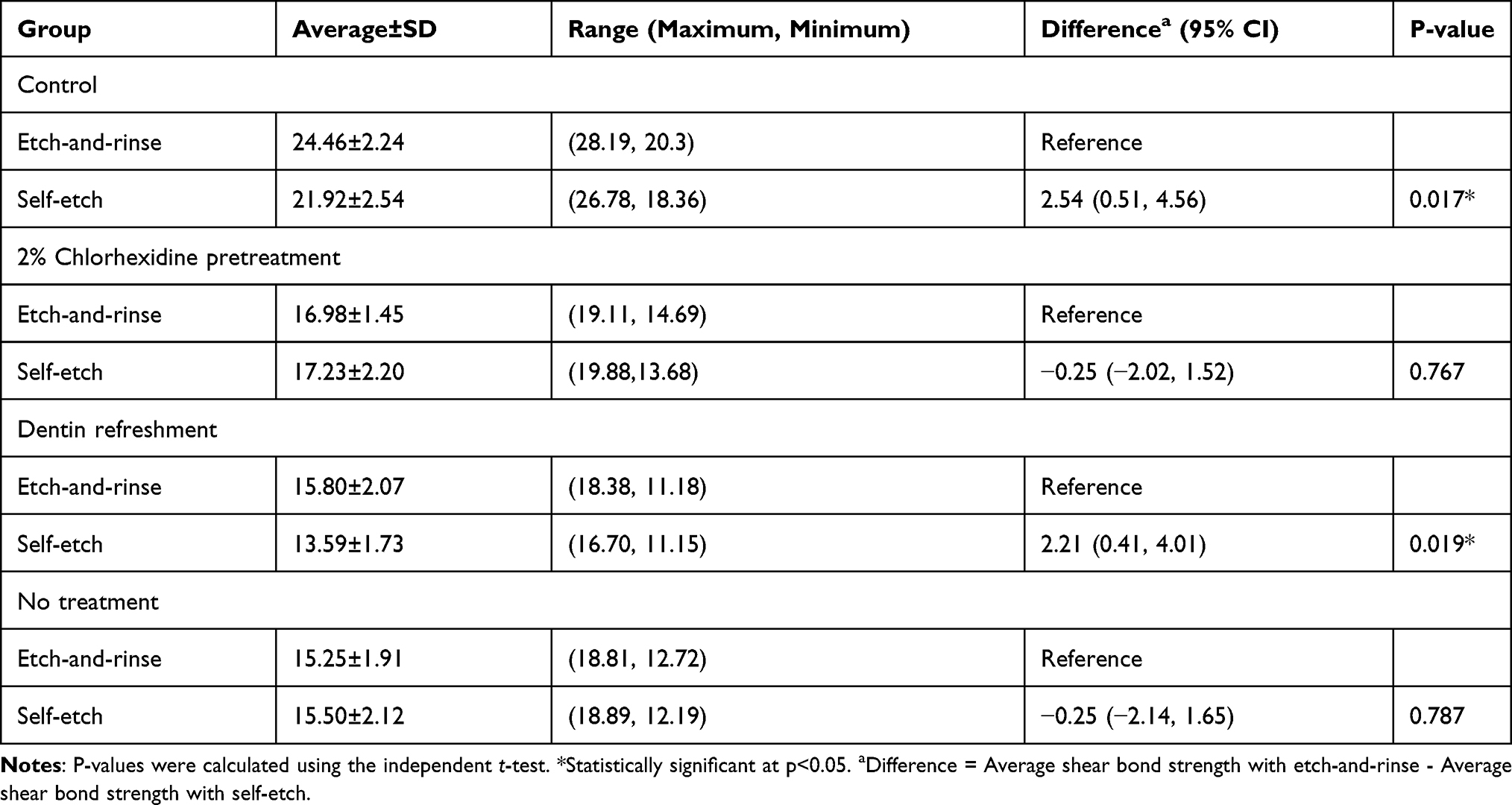 |
Table 3 Shear Bond Strength in (MPa) of the Tested Groups (n=20) |
Failure Mode
The failure mode distribution of all experimental groups is shown in Figure 2. The predominant failure mode was adhesive failure in all groups. Mixed and cohesive failure were mostly found in the control group for both adhesive protocols and in the untreated dentin group using the self-etch adhesive protocol. Figure 3A–D represents the different categories of failure from samples examined under the digital microscope.
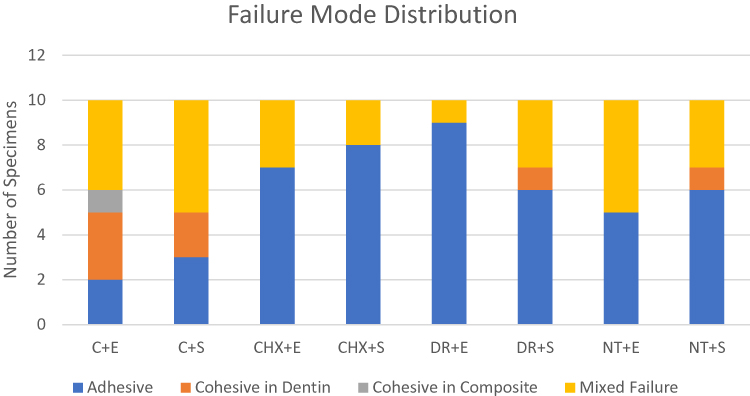 |
Figure 2 Distribution of adhesive failure types among experimental groups. |
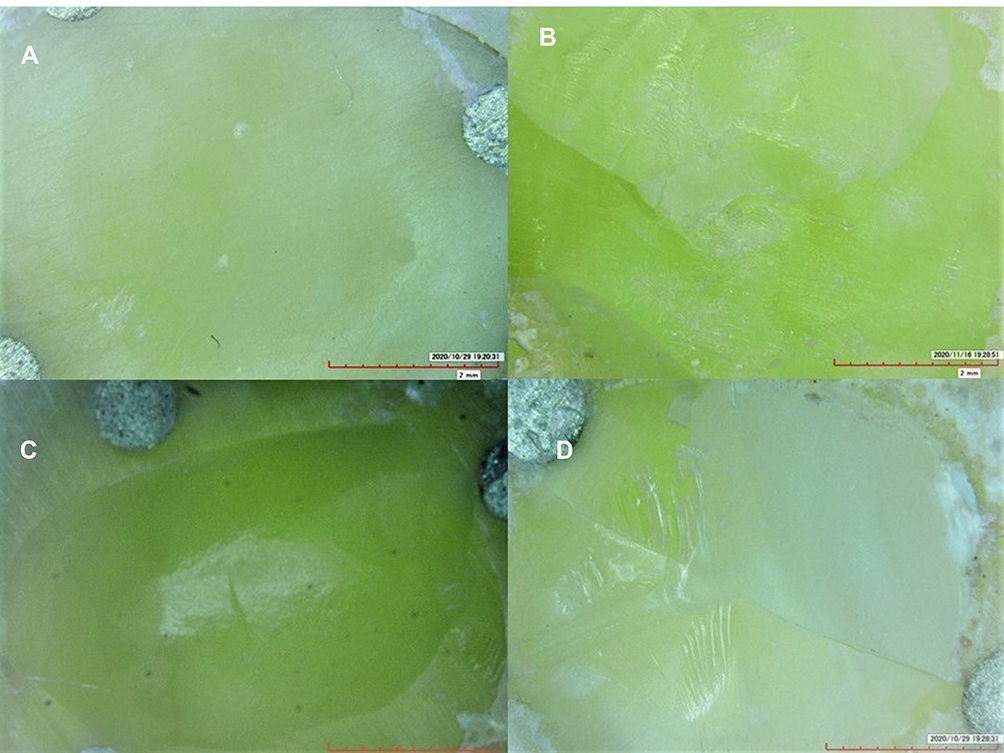 |
Figure 3 A photograph of the different types of failure. (A) Adhesive failure, (B) cohesive in composite, (C) cohesive in dentin, and (D) mixed. |
Discussion
The present study evaluated the effect of amalgam contamination, different surface treatments, and adhesive protocols on dentin SBS to bulk-fill composite resin material. Based on the results of this study, the SBS of non-contaminated dentin was significantly higher than that of amalgam-contaminated dentin; therefore, the null hypothesis that there would be no significant difference between amalgam- and non-contaminated dentin bonded to bulk-fill composite using different surface treatments was rejected. Additionally, dentin treatment in general affected the SBS; therefore, the secondary hypothesis that there would be no significant difference in bond strength between different protocols of the universal adhesive system was also rejected.
In the present study, dentin bond strength was negatively affected by amalgam contamination. These results are in agreement with previous works of Harnirattisai et al15 and Ghavamnasiri et al.16 Ghavamnasiri et al16 compared SBS of composite resin to different groups of discolored dentin after amalgam removal. They found a significant difference in bond strength between normal dentin and the discolored non-modified dentin after storage for 6 months, but not between those where 0.5-mm dentin was removed and stored for different periods of time and the non-modified groups. A possible explanation is that the presence of products of amalgam corrosion may affect adhesion or formation of an appropriate hybrid layer. These corrosive products might interfere with the full infiltration of resin monomers into the dentinal tubules. High concentrations of metals, such as Zn, may also retard polymerization.15,18 Moreover, these corrosive products bind to collagen fibrils, which are important components in hybrid layer formation, particularly silver sulfides, that cause staining.19 These corrosive products make the smear layer less etchable than normal dentin by reducing its solubility.15
In the current study, chlorhexidine application improved the SBS compared with the other amalgam groups regardless of the adhesion protocol used; however, the difference was only significant when compared with the dentin refreshment group with the self-etch mode. Chlorhexidine is a strong disinfectant used after cavity preparation.20 As a matrix metalloproteinase inhibitor, chlorhexidine also prevents degradation of the hybrid layer, and the loss of bond strength and nanoleakage in 2-year-aged specimens.21 Chlorhexidine pretreatment in the present study improved SBS for self-etch adhesive compared with the etch-and-rinse adhesive mode, concordant with the findings of Almozher and Alomari.22 Moreover, chlorhexidine pretreatment improved the SBS in the self-etch mode group compared with the no treatment group, which was in agreement with Bravo et al23 who compared dentin treated with chlorhexidine, restored them with self-etching and universal adhesives, and aged specimens for 3 and 6 months. This finding can partially be explained by the adhesive used in these systems, which was a mild acid etchant that may trigger less matrix metalloproteinase activity, therefore maintaining a sound hybrid layer.24
In contrast, the dentin refreshment group showed lower SBS with the self-etch than etch-and-rinse mode. The matrix metalloproteinase activity increased as the cavity depth increased, which may cause degradation of the hybrid layer that may in turn explain the lower bond strength in the self-etch group. Additionally, the deeper dentin surface contains more water and less inter-tubular dentin and collagen fibrils.25 All of these factors add to the contamination of the dentin by corrosive products.
In addition, the quality of the smear layer is depth-dependent.26 Since deep dentin layers have less mineral content, the chemical bond between hydroxyapatite and functional groups of 10-MDP might have been modified. In the etch-and-rinse group, the smear layer was removed, yielding better resin interlocking with the exposed dentin and therefore a higher bond strength (Figure 4).27
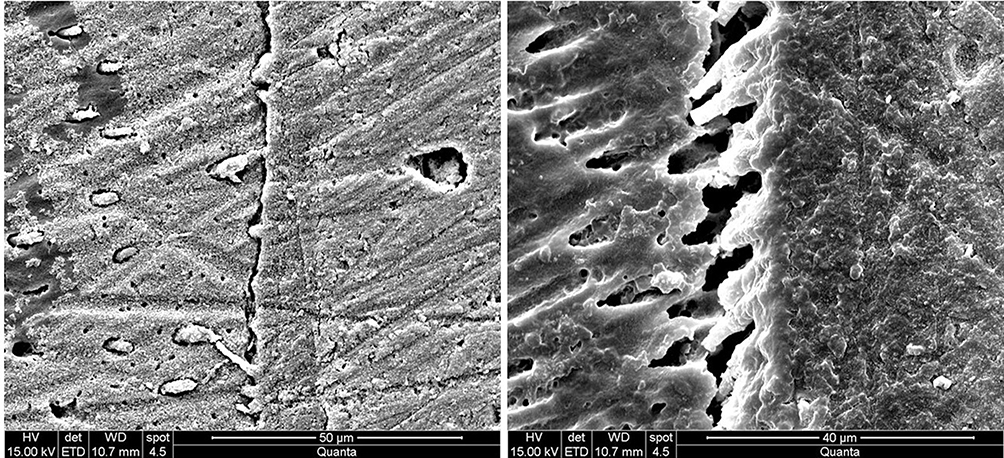 |
Figure 4 A photomicrograph of two different specimens with different magnifications that are bonded using the etch-and-rinse protocol in which the formation abundant resin tags are clear. |
Takamizawa et al28 attempted to clarify if the smear layer would affect adhesive bond strength when universal adhesive systems were used. They tested Scotchbond Universal Adhesive along with other universal and etch-and-rinse adhesive systems and found that the smear layer effect on bond strength was material-dependent, favoring etch-and-rinse adhesives. This was also confirmed here by our control group results, where the etch-and-rinse mode showed significantly higher SBS.
Single Bond Universal is a mild form of self-etching adhesive that relies on demineralization of approximately 1 µm of the dentin (Figure 5), and chemical interaction between the functional monomer and the remaining hydroxyapatite that provides a strong ionic bond. This chemical interaction does not imply a higher bond strength, but it contributes to a more durable bond, unlike bonding that involves an organic component and depends on weak van der Waals interactions and hydrogen bonding, which result in weaker degradation resistance.29
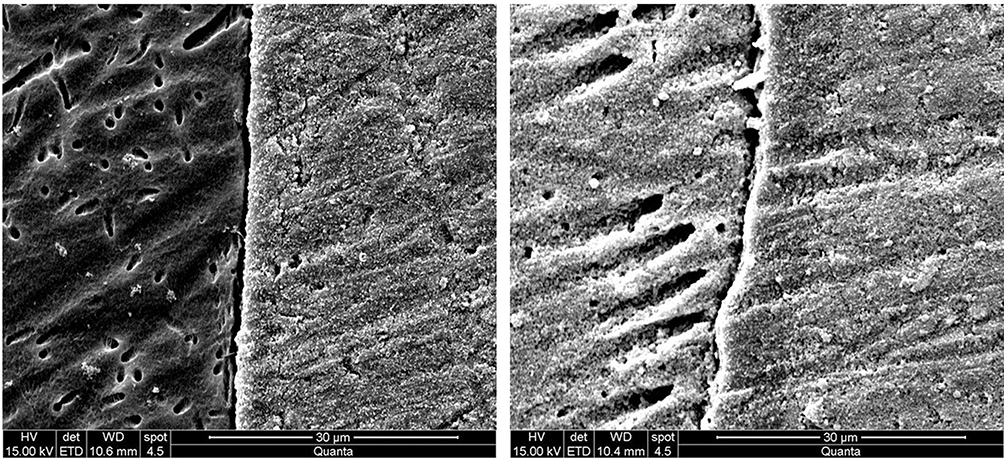 |
Figure 5 A photomicrograph of two different specimens with different magnifications that are bonded using the self-etch adhesive protocol showing demineralized dentin with no to little resin tags. |
One of the most widely used functional monomers is 10-MDP, which relies on a limited decalcification effect. The concept of adhesion decalcification was introduced by Yoshida et al30 who explained the chemical interaction of a carboxylic functional group with hydroxyapatite. This concept was adopted and modified into the modified adhesion route29 because the interaction of this functional monomer is unique. The functional monomer attacks the hydroxyapatite, releasing abundant calcium ions while ionically bonding to the remaining calcium of the hydroxyapatite substrate forming the hybrid layer. The remaining calcium will reassemble with 10-MDP into a 4-nm nanolayer, forming 10-MDP-Ca salts below the hybrid layer.31,32 This nano-layering is hydrolytically stable because a hydroxyl group interacts with Ca, forming CaRPO4 salts that are believed to improve clinical longevity of the adhesive interface.29
A clinical study in 2014 by Scholtanus and Özcan33 followed up (duration: 7 months to 3.5 years) teeth that were restored by extensively replacing amalgam restorations using a 3-step etch-and-rinse technique and a hybrid composite. They concluded that failure of composite resin restorations was mainly due to fracture, endodontic complications, and inadequate proximal contacts but did not relate failure to adhesion of the composite or recurrent decay.
Limitations
Although SBS testing is still the most common test of adhesion performance,34 it is subject to cohesive failures, especially with new adhesive systems.35 Additionally, the composite specimens might be stressed because of mold removal prior to testing, which may affect the true test values.36 However, because of the simplicity and validity of these tests, SBS testing continues to be used in in-vitro studies to evaluate the adhesion of resin composites to tooth structure.37
In-vitro investigations, as in the current study, evaluate the effectiveness of adhesion of certain materials and the bonding system to tooth structures in a controlled laboratory environment for a short period of time. Therefore, there is a great need for long-term clinical investigations.
Conclusion
In this study, it was evident that amalgam contamination may detrimentally affect the SBS of dentin. The adhesion modes of the universal adhesive system were both effective in producing adequate bonds to the amalgam- and non-contaminated dentin. The use of chlorhexidine after careful amalgam removal did not adversely affect the bond strength but increased the SBS when the self-etch mode protocol was used. Dentin refreshment was not effective in increasing bond strength, but it can be used for esthetic purposes. This study thus provided insight into the effects of different surface treatments on the bond strength of universal adhesive systems for bonding RBC to amalgam-contaminated dentin.
Abbreviations
SBS, shear bond strength; RBC, resin-based composite; Sn, tin; Zn, zinc; Cu, copper; MPa, megapascal.
Ethics Approval and Informed Consent
This project was approved by the ethics committee of King Saud University (IRB number E-19-3846) and all human molar teeth were obtained after informed consent, in accordance with the Declaration of Helsinki.
Acknowledgments
This manuscript presents a part of the doctorate dissertation of Nojoud Alshehri.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bharti R, Wadhwani KK, Tikku AP, Chandra A. Dental amalgam: an update. J Conserv Dent. 2010;13(4):204–208. doi:10.4103/0972-0707.73380
2. Mjor IA. Placement and replacement of restorations. Oper Dent. 1981;6:49–54.
3. Opdam NJ, Bronkhorst EM, Roeters JM, Loomans BA. A retrospective clinical study on longevity of posterior composite and amalgam restorations. Dent Mater. 2007;23(1):2–8. doi:10.1016/j.dental.2005.11.036
4. Drake CW, Maryniuk GA, Bentley C. Reasons for restoration replacement: differences in practice patterns. Quintessence Int. 1990;21(2):125–130.
5. Eltahlah D, Lynch CD, Chadwick BL, Blum IR, Wilson NHF. An update on the reasons for placement and replacement of direct restorations. J Dent. 2018;72:1–7. doi:10.1016/j.jdent.2018.03.001
6. Gordan VV, Riley JL
7. Ganesh N, Strassler HE. Posterior composite resin restorations: keys to long-term survivability. Compend Contin Educ Dent. 2019;40(2):120–121.
8. Lynch CD, Opdam NJ, Hickel R, et al. Guidance on posterior resin composites: academy of operative dentistry—European section. J Dent. 2014;42(4):377–383. doi:10.1016/j.jdent.2014.01.009
9. Moraschini V, Fai CK, Alto RM, Dos Santos GO. Amalgam and resin composite longevity of posterior restorations: a systematic review and meta-analysis. J Dent. 2015;43(9):1043–1050. doi:10.1016/j.jdent.2015.06.005
10. Carrilho E, Cardoso M, Marques Ferreira M, Marto CM, Paula A, Coelho AS. 10-MDP based dental adhesives: adhesive interface characterization and adhesive stability—a systematic review. Materials. 2019;12(5):790. doi:10.3390/ma12050790
11. Kucukyilmaz E, Botsali MS, Korkut E, Sener Y, Sari T. Effect of different modes of erbium: yttriumaluminum garnet laser on shear bond strength to dentin. Niger J Clin Pract. 2017;20(10):1277–1282. doi:10.4103/1119-3077.181402
12. Coelho A, Amaro I, Rascão B, et al. Effect of cavity disinfectants on dentin bond strength and clinical success of composite restorations—a systematic review of in vitro, in situ and clinical studies. Int J Mol Sci. 2021;22(1):353. doi:10.3390/ijms22010353
13. Mahler DB, Pham BV, Adey JD. Corrosion sealing of amalgam restorations in vitro. Oper Dent. 2009;34(3):312–320. doi:10.2341/08-94
14. Scholtanus JD. Hora est 2. Is door amalgaam verkleurd dentine een geschikt substraat voor hechting van composiet? [Is amalgam stained dentin a proper substrate for bonding resin composite?]. Ned Tijdschr Tandheelkd. 2016;123(6):313–315. doi:10.5177/ntvt.2016.06.16152
15. Harnirattisai C, Senawongse P, Tagami J. Microtensile bond strengths of two adhesive resins to discolored dentin after amalgam removal. J Dent Res. 2007;86(3):232–236. doi:10.1177/154405910708600307
16. Ghavamnasiri M, Eslami S, Ameri H, Chasteen JE, Majidinia S, Moghadam FV. Effect of amalgam corrosion products in non-discolored dentin on the bond strength of replaced composite resin. J Conserv Dent. 2015;18(1):25–29.
17. Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of dental restorations. J Dent. 1999;27(2):89–99. doi:10.1016/S0300-5712(98)00037-2
18. Wanichacheva N, Miyagawa Y, Ogura H. Polymerization of UDMA using zinc particles and 4-META with and without BPO. Dent Mater J. 2000;19(2):173–185. doi:10.4012/dmj.19.173
19. Ellender G, Ham KN, Harcourt JK. The ultrastructural localization of the corrosion products of dental amalgam. Aust Dent J. 1979;24(3):174–177. doi:10.1111/j.1834-7819.1979.tb02419.x
20. Fure S, Emilson CG. Effect of chlorhexidine gel treatment supplemented with chlorhexidine varnish and resin on mutans streptococci and actinomyces on root surfaces. Caries Res. 1990;24(4):242–247. doi:10.1159/000261275
21. Breschi L, Mazzoni A, Nato F, et al. Chlorhexidine stabilizes the adhesive interface: a 2-year in vitro study. Dent Mater. 2010;26(4):320–325. doi:10.1016/j.dental.2009.11.153
22. Almozher AA, Alomari M. Bond strength of adhesives to dentin surface treated with chlorhexidine. J Int Oral Health. 2016;8(12):1049.
23. Bravo C, Sampaio CS, Hirata R, Puppin-Rontani RM, Mayoral JR, Giner-Tarrida L. In-vitro comparative study of the use of 2% chlorhexidine on microtensile bond strength of different dentin adhesives: a 6 months evaluation. Int J Morphol. 2017;35(3):893–900. doi:10.4067/S0717-95022017000300016
24. De Munck J, Van den Steen PE, Mine A, et al. Inhibition of enzymatic degradation of adhesive-dentin interfaces. J Dent Res. 2009;88(12):1101–1106. doi:10.1177/0022034509346952
25. Zhang YR, Du W, Zhou XD, Yu HY. Review of research on the mechanical properties of the human tooth. Int J Oral Sci. 2014;6(2):61–69. doi:10.1038/ijos.2014.21
26. Perdigão J. Dentin bonding-variables related to the clinical situation and the substrate treatment. Dent Mater. 2010;26(2):e24–e37. doi:10.1016/j.dental.2009.11.149
27. Kenshima S, Reis A, Uceda-Gomez N, et al. Effect of smear layer thickness and pH of self-etching adhesive systems on the bond strength and gap formation to dentin. J Adhes Dent. 2005;7(2):117–126.
28. Takamizawa T, Barkmeier WW, Sai K, et al. Influence of different smear layers on bond durability of self-etch adhesives. Dent Mater. 2018;34(2):246–259. doi:10.1016/j.dental.2017.11.002
29. Van Meerbeek B, Yoshihara K, Van Landuyt K, Yoshida Y, Peumans M. From buonocore’s pioneering acid-etch technique to self-adhering restoratives. A status perspective of rapidly advancing dental adhesive technology. J Adhes Dent. 2020;22(1):7–34. doi:10.3290/j.jad.a43994
30. Yoshida Y, Van Meerbeek B, Nakayama Y, et al. Adhesion to and decalcification of hydroxyapatite by carboxylic acids. J Dent Res. 2001;80(6):1565–1569. doi:10.1177/00220345010800061701
31. Fukegawa D, Hayakawa S, Yoshida Y, Suzuki K, Osaka A, Van Meerbeek B. Chemical interaction of phosphoric acid ester with hydroxyapatite. J Dent Res. 2006;85(10):941–944. doi:10.1177/154405910608501014
32. Yoshihara K, Yoshida Y, Nagaoka N, et al. Nano-controlled molecular interaction at adhesive interfaces for hard tissue reconstruction. Acta Biomater. 2010;6(9):3573–3582. doi:10.1016/j.actbio.2010.03.024
33. Scholtanus JD, Özcan M. Clinical longevity of extensive direct composite restorations in amalgam replacement: up to 3.5 years follow-up. J Dent. 2014;42(11):1404–1410. doi:10.1016/j.jdent.2014.06.008
34. Burke FJ, Hussain A, Nolan L, Fleming GJ. Methods used in dentine bonding tests: an analysis of 102 investigations on bond strength. Eur J Prosthodont Restor Dent. 2008;16(4):158–165.
35. El Mourad AM. Assessment of bonding effectiveness of adhesive materials to tooth structure using bond strength test methods: a review of literature. Open Dent J. 2018;12:664–678. doi:10.2174/1745017901814010664
36. Van Noort R, Cardew GE, Howard IC, Noroozi S. The effect of local interfacial geometry on the measurement of the tensile bond strength to dentin. J Dent Res. 1991;70(5):889–893. doi:10.1177/00220345910700050501
37. Sirisha K, Rambabu T, Ravishankar Y, Ravikumar P. Validity of bond strength tests: a critical review-part II. J Conserv Dent. 2014;17(5):420–426. doi:10.4103/0972-0707.139823
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.