Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
The Effects of a Parental Behavior Modification Program to Prevent Pesticide Exposure Among Toddlers Living in Agricultural Areas of Thailand: An Experimental Study
Authors Ong-Artborirak P ![]() , Nganchamung T
, Nganchamung T ![]() , Ponrachom C, Wangkahart A, Siriwat S
, Ponrachom C, Wangkahart A, Siriwat S ![]()
Received 17 September 2025
Accepted for publication 8 January 2026
Published 13 January 2026 Volume 2026:19 563962
DOI https://doi.org/10.2147/JMDH.S563962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Parichat Ong-Artborirak,1 Thitirat Nganchamung,2 Chakkrit Ponrachom,3 Apiradee Wangkahart,4 Satinee Siriwat4
1Department of Research and Medical Innovation, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2College of Medicine and Public Health, Ubon Ratchathani University, Ubon Ratchathani, Thailand; 3Department of Physical Education, Faculty of Education, Kasetsart University, Bangkok, Thailand; 4Department of Community Health, Faculty of Public Health, Kasetsart University, Chalermphrakiat Sakon Nakhon Province Campus, Sakon Nakhon, Thailand
Correspondence: Satinee Siriwat, Department of Community Health, Faculty of Public Health, Kasetsart University, Chalermphrakiat Sakon Nakhon Province Campus, Sakon Nakhon, Thailand, Email [email protected]
Background: Pesticides pose health risks to vulnerable populations living in agricultural areas, especially children. However, effective interventions demonstrating biomarker-based reductions in pesticide exposure among toddlers remain scarce, including in Thailand.
Objective: This quasi-experimental study, using a pre-test/post-test design, aimed to assess the effect of a parental behavior modification program on pesticide exposure among young Thai children.
Methods: The sample consisted of 90 families with children aged 1– 3 years who lived within 50 meters of agricultural areas, including 46 in the intervention group and 44 in the control group. Guardians in the intervention group received a behavior modification program based on the Theory of Planned Behavior (TPB), which included three training sessions and one home visit. The control group did not receive any intervention. Acetylcholinesterase (AChE) levels in toddlers were measured via finger prick in both groups at three time points: baseline, follow-up 1 (two months after the end of the intervention), and follow-up 2 (five months after the end of the intervention).
Results: Linear mixed-model analysis showed that, from baseline to follow-up 1, hemoglobin-adjusted AChE (HAChE) levels in the intervention group were 1.307 U/g Hgb higher than in the control group (P = 0.047). From baseline to follow-up 2, HAChE levels were 2.332 U/g Hgb higher in the intervention group (P = 0.005), and AChE levels were also higher by 0.311 U/mL.
Conclusion: These findings suggest that the parental behavior modification program can effectively reduce pesticide exposure in young Thai children, and therefore the program should be considered for implementation as part of efforts to improve health outcomes among children living in agricultural areas of Thailand.
Keywords: parent, young children, farming family, behavior modification program, pesticide, cholinesterase
Introduction
The use of pesticides for increasing agricultural productivity is widespread worldwide, including Thailand. Between 2019 and 2021, the amount of pesticide use and imports into Thailand showed an increasing trend.1 Not only farmers, but also farming families and individuals living in agricultural areas, especially young children, are at risk of pesticide exposure due to pesticide drift and take-home pathways.2–4 Children may be particularly vulnerable to pesticide exposure, not only from agricultural environments but also within farming households, including through domestic pesticide use.4,5 Previous studies have revealed that children living in agricultural communities are more likely to be exposed to pesticides compared to those in non-agricultural areas.6
Additionally, behaviors and hygiene practices common among children, such as putting their hands or objects in their mouths, accompanying caregivers to farms, and walking barefoot, may increase their risk of pesticide exposure.7–9 Many studies have detected pesticide residues on children’s skin (eg, hands and feet), on household floors, and on children’s toys.8–12 Pesticide exposure in children can also be detected using biological markers, including urine for specific metabolites and blood for cholinesterase (ChE) activity related to organophosphate (OP) and carbamate (CA) pesticides.2,10,13 Exposure to pesticides can result in various health effects and unfavorable symptoms. Adverse effects in children include behavioral disorders, delayed neurodevelopment, and cancer.14–17 Common symptoms of pesticide exposure in children include skin and eye irritation, coughing, runny nose, nausea, vomiting, loss of appetite, and difficulty breathing.10,18
In Thailand, children living in agricultural areas, particularly those aged 1–3 years, are at high risk of exposure to OPs (eg, chlorpyrifos) and CAs (eg, carbaryl, carbofuran, methomyl), with pesticide residues detected on their skin in 60–100% of cases.8–10 Therefore, preventing pesticide exposure is crucial, particularly for toddlers who are unable to protect themselves. In this context, parents and caregivers play a vital role in safeguarding children. The development of parental behavior modification programs to prevent pesticide exposure in children living in agricultural areas is thus essential for achieving effective and sustainable solutions to this problem.
A literature review revealed that effective programs aimed at reducing pesticide exposure among young children in farming families are limited, particularly those assessed using internal exposure measures. Although various interventions have been carried out internationally, evidence of clear reductions in this population remains modest. One Thai study evaluated the effectiveness of a program only in terms of behavioral improvement, but it lacked data on biomarkers.5 Recently, a Parental Behavior Modification Program for Pesticide Exposure Prevention Among Children in Agricultural Areas was proposed as a role model for implementation in a Sub-District Health Promotion Hospital in Thailand.19 The program was designed using the Theory of Planned Behavior (TPB) framework and developed through Intervention Mapping (IM), a systematic, step-by-step approach that integrates theory and empirical evidence to design health promotion and education programs.20,21 However, although the program has been conceptually proposed, it has not yet been evaluated in practice. Extending previous findings, this research provides evidence regarding the effects of the intervention, particularly with respect to biological outcomes. Therefore, this study aimed to evaluate the effectiveness of the parental behavior modification program for pesticide exposure prevention, using ChE levels as a blood biomarker among young Thai children living in agricultural areas.
Materials and Methods
Study Design and Subjects
This research employed a quasi-experimental design using a pretest-posttest control group with a follow-up test. The study was conducted from April to October 2022 in Sakon Nakhon Province, a region characterized by extensive agricultural land use. Major economic crops include rice, cassava, rubber, oil palm, sugarcane, animal feed corn, pineapple, longan, rambutan, durian, mangosteen, coconut, and coffee. Additionally, the province is a key production area for fresh corn, tomatoes, and cantaloupe. Pesticides are used throughout the year in this region.
The G*Power program was used to calculate the sample size based on a comparison of two independent means, with an effect size of 0.6, a two-tailed test, a 95% confidence level, and 80% power. The minimum required sample size for both groups was 90 participants. To account for potential loss to follow-up, the sample size was increased by 20%, resulting in a total of 108 dyads of parents/caregivers and their children. Participants were identified using lists provided by Subdistrict Health Promotion Hospitals and through household surveys. Inclusion criteria were as follows: children aged 1–3 years living with their parents or caregivers, a caregiving duration of at least six months, residence in agricultural areas located within 50 meters of active farmland, and willingness of the parents or caregivers to provide information and participate in the study.
The intervention and control groups were selected from four districts in Sakon Nakhon Province: Chiang Khruea (intervention) and Khok Kong (control) in Mueang Sakon Nakhon District, Chan Phen (intervention) and Tao Ngoi (control) in Tao Ngoi District, Phok Noi (intervention) in Phanna Nikhom District, and Nong Phok Yai (control) in Kham Ta Kla District. These areas were chosen for their similar agricultural practices and socio-demographic characteristics. Crop types commonly grown in these areas include tomatoes, chilies, cantaloupe, potatoes, and cassava. Pesticides used, as identified through farmer interviews and surveys of crop fields and agricultural stores, included organophosphates and carbamates, which are known to be harmful to human health upon exposure.
The sample was selected based on the inclusion criteria from areas with similar contexts to ensure comparable activities across groups, and recruitment continued until the required sample size was reached. The alternating mountainous and lowland terrain, together with the more than 30-kilometer separation between intervention and control villages, minimized information or behavioral exchange and reduced contamination bias. Data collection was conducted simultaneously for both the experimental and control groups to control for differences in the timing and implementation of the intervention. This approach helped reduce potential temporal bias. Community-level group assignment was handled in a way that supported internal validity.
At baseline, the sample consisted of 108 children aged 1–3 years and their parents, equally divided into the experimental group (n = 54) and the control group (n = 54). Although the researchers thoroughly explained the research process, participation was entirely voluntary, and written informed consent was obtained to ensure ethical compliance. To limit loss to follow-up during the COVID-19 situation—which further restricted interpersonal contact—the researchers coordinated data collection at participants’ homes when participants were unable to travel to the study activities. However, due to illness during the outbreak and the inability of some parents to bring their children for blood sample collection within the data collection period, 18 participants were removed from both the experimental and control groups.
This study was approved by the Ethics Review Committee for Research Involving Human Research Subjects of Kasetsart University in Thailand (No. COA65/005). All parents or guardians of the participating children provided written informed consent prior to participation. All methods were carried out in accordance with the Declaration of Helsinki.
Data Collection
A preparatory workshop was conducted prior to implementing the Parental Behavior Modification Program for Pesticide Exposure Prevention among children living in agricultural areas. The workshop involved public health officers and village health volunteers from the target Subdistrict Health Promotion Hospitals, who were trained to serve as research assistants. An interviewer-administered questionnaire was used to collect baseline data from both the experimental and control groups. The questionnaire included sections on caregiver information (sex, age, education level, occupation, monthly income, relationship with the child, and duration of childcare), child information (sex and age), and pesticide prevention-related behaviors (bathing and washing the child’s hands and feet with soap after exposure to soil or dirt, avoiding taking the child to the farm, and cleaning the house with a wet cloth). In addition to the questionnaire, wipe samples were collected from the children’s hands and feet, and finger-prick blood samples were taken to measure ChE levels.
Following baseline data collection, the researcher implemented the behavior modification program in the experimental group over a one-month period, consisting of four weekly activities.19 Meanwhile, the control group continued with routine activities and received standard care provided by the local Subdistrict Health Promotion Hospital. Follow-up data were collected in both groups at 2 and 5 months after the intervention using finger-prick blood tests to assess changes in ChE levels. All data collection and intervention activities were conducted at the Subdistrict Health Promotion Hospitals. The data collection flowchart is shown in Figure 1.
 |
Figure 1 Data collection flowchart. |
Wipe Sampling on Children’s Hands and Feet
To detect the types and amounts of pesticide residues on the skin of children living in agricultural areas, surface wipe samples were collected from their hands and feet using 4×4 inch sterile gauze pads soaked in 3 mL of 40% isopropanol. The used gauze pads were placed in tightly sealed tubes and stored in a light-proof, refrigerated container. Seven target pesticides from the CAs and OPs groups—aldicarb, carbofuran, carbaryl, methomyl, prothiofos, pirimiphos-methyl, and chlorpyrifos—were analyzed. Pesticide residues were then extracted from the samples and analyzed to determine both type and concentration using High-Performance Liquid Chromatography (HPLC), following previously established methods.8,9 The pesticide residue levels were measured and reported as micrograms per combined hand and foot wipe sample (µg/sample). The limit of detection (LOD) and limit of quantification (LOQ) were 0.001 µg/sample and 0.003 µg/sample, respectively.
Blood ChE Testing in Children
Cholinesterase levels in the children’s blood were measured by a nurse, who cleaned the fingertip before collecting 10 microliters of capillary blood using a finger-prick method. The samples were analyzed using the EQM Test-mate ChE field kit (Model 400), which is based on the Ellman method, in combination with the AChE Assay Kit.22 The kit measured acetylcholinesterase (AChE) activity in units of U/mL. In addition, the kit automatically derived hemoglobin-adjusted erythrocyte cholinesterase (HAChE) to correct for potential interference from iron status. HAChE was calculated by dividing the AChE value by the hemoglobin (Hgb) result and is expressed in units of U/g Hgb.22 Both AChE and HAChE values were recorded simultaneously for each sample. Measurements were taken at baseline as well as at the 2-month and 5-month follow-up periods.
Parental Behavior Modification Program for Pesticide Exposure Prevention in Children Living in Agricultural Areas (for Subdistrict Health Promoting Hospitals)
This program, developed by Siriwat et al, aims to systematically strengthen parents’ capacity to prevent pesticide exposure in children living in agricultural areas.19 Designed in alignment with the roles and functions of Subdistrict Health Promoting Hospitals, the program focuses on identifying and modifying intrapersonal factors that influence parental behavior. Grounded in the TPB, it incorporates key constructs, including attitude, subjective norm, and perceived behavioral control, through learning methods tailored to parents’ local contexts.20 Upon completion, parents are expected to demonstrate positive attitudes toward preventing pesticide exposure in children, conformity to subjective norms through alignment with desirable reference groups, a greater sense of perceived behavioral control, and the adoption of effective preventive behaviors. The behavior change process is facilitated through a series of structured learning activities targeting behavioral determinants related to pesticide exposure. The program was implemented over one month and consists of four weekly activities, as outlined in Table 1.
 |
Table 1 Learning Activities in the Parental Behavior Modification Program for Pesticide Exposure Prevention in Children Living in Agricultural Areas |
Data Analysis
Data were recorded using the double-entry method by two individuals independently. Data analysis was conducted using STATA. Descriptive statistics, including frequency, percentage, mean, standard deviation (SD), median, and interquartile range (IQR), were used to summarize the participants’ characteristics and blood ChE levels. Fisher’s exact test and the Chi-square test were employed to compare categorical characteristics between the intervention and control groups. The independent t-test was used to compare continuous characteristics between groups and to analyze the mean blood ChE levels of young children in both groups at different time points. A linear mixed-effects model, incorporating an interaction term between intervention and time, was used to assess the intervention effect through difference-in-difference (DID) analysis at the 2-month and 5-month follow-ups compared to the baseline. Both unadjusted and adjusted models were applied, with the latter controlling for baseline characteristics that significantly differed between groups. A p-value of less than 0.05 was considered statistically significant.
Results
Table 2 presents the baseline characteristics of the young children and their caregivers. In both the intervention and control groups, the majority of caregivers were female (93.5% and 97.7%, respectively). The average caregiver age was 41.65 years in the intervention group and 34.32 years in the control group. Most caregivers had attained secondary education (54.3% and 50.0%) and worked as farmers (65.2% and 56.8%). Over half reported an average monthly income of less than 5000 baht (52.2% and 47.7%). The majority of caregivers were parents (52.2% and 72.7%, respectively). Regarding the children’s characteristics, most were male (54.3% in the intervention group and 61.4% in the control group), with a mean age of approximately 24 months in both groups. A comparison of baseline characteristics between the two groups showed significant differences in the mean caregiver age (P = 0.007) and the proportion of caregiver relationships to the child (P = 0.044). In addition, caregiver behaviors—including child bathing and hand/foot washing, bringing the child to the farm, and cleaning the floor with a wet cloth—as well as pesticide residues detected on children’s hands and feet showed no significant differences between the intervention and control groups, with the highest detection observed for pirimiphos-methyl and chlorpyrifos.
 |
Table 2 Baseline Characteristics of Young Children and Their Caregivers |
Blood ChE measurements in children, obtained using the Test-mate ChE field kit, revealed no significant differences in AChE or HAChE levels between the intervention and control groups at baseline or at the 2-month follow-up. However, a statistically significant difference in AChE levels was observed at the 5-month follow-up (P = 0.010), as shown in Table 3.
 |
Table 3 Blood ChE Measurements in Children Between the Intervention and Control Groups at Baseline, 2-Month Follow-Up, and 5-month Follow-Up |
The effectiveness analysis of the parental behavior modification program in preventing pesticide exposure among children living in agricultural areas, using a mixed-effects model, revealed that, from baseline to the 2-month follow-up, the HAChE level in the intervention group increased significantly more than in the control group by 1.3 U/g Hgb (P = 0.049). From baseline to the 5-month follow-up, the HAChE level in the intervention group increased by 2.3 U/g Hgb more than in the control group (P = 0.005). These results were obtained after adjusting for the caregiver’s age and their relationship to the child, as shown in Table 4.
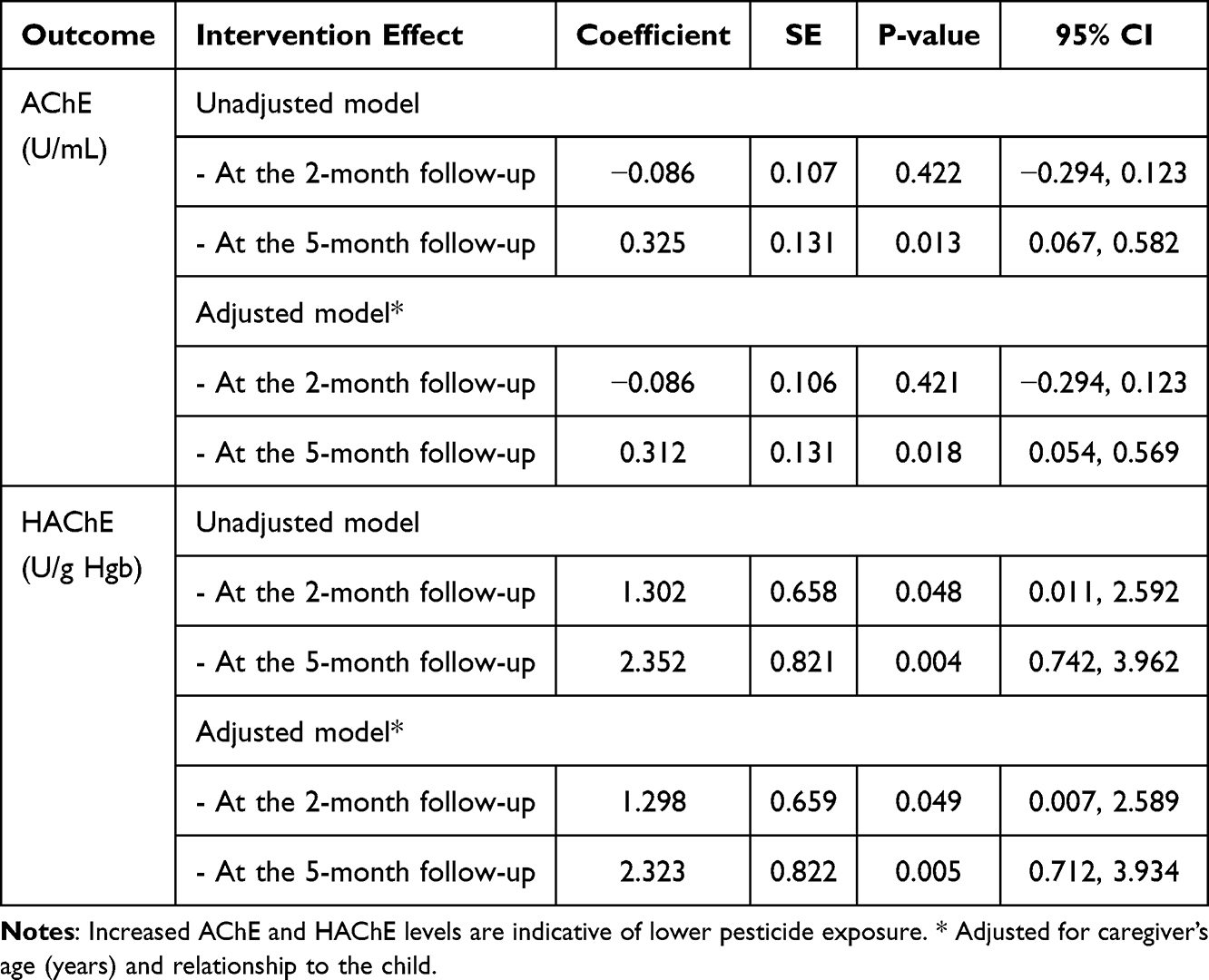 |
Table 4 Effectiveness of the Program on Blood ChE Levels in Toddlers at the 2- and 5-month Follow-Ups Compared to Baseline |
Discussion
The study results revealed that children living in agricultural areas in Thailand had very low ChE values, indicating potential risk of pesticide-related effects, particularly regarding neurodevelopment.14,15 This is likely due to the extensive use of CA and OP pesticides in Thai agriculture. Although some of these pesticides, such as chlorpyrifos and carbofuran, have been banned or restricted in many countries due to their high toxicity, they were still detected on the hands and feet of the young children in this study. Notably, chlorpyrifos and pirimiphos-methyl were found in over 50% of the children. Moreover, the children in this sample group lived within 50 meters of farmland, suggesting the influence of pesticide drift.2,23 Consequently, young children in these areas can be exposed through inhalation, dermal contact, and ingestion, including contaminated food and hand-to-mouth behaviors such as thumb-sucking.
The study on the effectiveness of the Parental Behavior Modification Program to prevent pesticide exposure among toddlers living in agricultural areas, using DID analysis in both unadjusted and adjusted models, found that AChE levels significantly increased at the 5-month follow-up, while HAChE levels significantly increased at both the 2-month and 5-month follow-ups compared to baseline. The observed increase in ChE levels suggests a reduced risk of exposure to OPs and CAs following participation in the program. This pattern may reflect AChE turnover in red blood cells, with the weaker effect at 2 months likely due to incomplete enzyme recovery. Although normative values for children have not been established, baseline AChE and HAChE levels were relatively low, related to common symptoms of pesticide exposure in children aged 1–3 years at similar enzyme activity levels.10 Following the 5-month intervention, AChE activity increased by over 20% from baseline, possibly indicating a clinically meaningful recovery of enzyme function. Overall, these findings suggest that the intervention, which was developed based on the TPB and its key constructs—attitude, subjective norm, and perceived behavioral control—was effective in modifying parental behaviors to reduce pesticide exposure in young children.20
This positive outcome may be attributed to the program’s components, which included training on the dangers and prevention of pesticide exposure in children, community knowledge sharing about childcare, hands-on practice of good hygiene in childcare, and home visits. These activities equipped parents and caregivers with knowledge, such as the routes of exposure and the negative effects of pesticides on children’s health, and practical skills to ensure proper hygiene and appropriate health care for children living in agricultural settings. Preventing pesticide exposure in children involves parental practices such as avoiding taking children to cultivated areas, ensuring they wear shoes rather than going barefoot both indoors and outdoors, increasing the frequency of showering or washing hands and feet, and cleaning the house more often. These behaviors are associated with reduced pesticide exposure in young children.7–10,24 In addition, regular follow-ups were conducted by village health volunteers, in collaboration with public health officials, who visited families to encourage and reinforce desirable childcare behaviors.
Similar to a previous study in Thailand that examined an educational intervention for caregivers to prevent residential pesticide exposure among young children in agricultural communities, providing booklets to inform caregivers about pesticide exposure and prevention can enhance their understanding and learning.5 This may promote more positive attitudes and strengthen their intention to adopt protective behaviors for their children. In the context of other countries, despite positive changes in knowledge and behavior from interventions targeting pesticide exposure in children of farming families, interventions achieving effective reductions in actual exposure levels remain less pronounced.25–30 A home-based intervention delivered by community health workers was associated with decreased trans-permethrin levels in floor wipe samples, while no significant reductions were observed for OPs or other agricultural pesticides, and although child urinary metabolite levels were lower in intervention households compared to controls, the differences were not statistically significant.31 Whereas no significant impact of community intervention to reduce pesticide exposure among farmworkers and their children by measuring in urinary pesticide metabolite concentrations or in pesticide residue concentrations in house and vehicle dust.32 In addition, an educational intervention on OP exposure significantly increased risk perception among adults and schoolchildren; however, child urinary metabolite levels remained unchanged, suggesting the need for a longer observation period.33 These discrepancies may result from variations in participants’ sociodemographic backgrounds, types of biomonitoring used, and differences in intervention design, including study duration and number of follow-ups. Nevertheless, the current study demonstrates an effective intervention for reducing pesticide exposure among young children aged 1–3 years living in agricultural areas.
This parental behavior modification program for preventing pesticide exposure among children living in agricultural areas is both feasible and practical, as it is specifically designed for public health officers at sub-district health promotion hospitals and village health volunteers. The structure of the program enables these personnel to effectively integrate it into their existing activities, aligning with Thailand’s agricultural context. Therefore, it is recommended that policies be developed to target high-risk agricultural areas, along with the implementation of mechanisms to promote sustainable changes in parental health behaviors aimed at reducing pesticide exposure in young children. In addition, the validated program should be further developed into a comprehensive learning package for use by relevant agencies, thereby facilitating knowledge dissemination and providing a foundation for future public health initiatives.
In this study, generalizability may be limited due to the specific characteristics of the participants, including their environmental conditions and socioeconomic backgrounds. Measuring internal exposure among children using additional biomarkers, such as metabolites of other pesticides, may be necessary to strengthen the evidence for the program’s effectiveness. In addition, using questionnaires based on the TPB constructs to assess parents’ or caregivers’ preventive practices, and conducting behavioral observations, is recommended to support the exposure assessment results. Since behavioral change depends on time, further studies should include an extended follow-up period to evaluate the sustainability of the intervention.
Conclusion
The findings on the participants’ blood ChE levels, measured from baseline through the 2nd- and 5th-month follow-up periods, showed a greater increase in the intervention group compared to the control group. This suggests that the Parental Behavior Modification Program for Pesticide Exposure Prevention among Children Living in Agricultural Areas, based on the TPB and incorporating key constructs such as attitude, subjective norm, and perceived behavioral control, had a positive effect on improving parental or caregiver behavior and reducing the risk of pesticide exposure among children. The program serves as a potential model for integration into routine services at Subdistrict Health Promotion Hospitals, supporting efforts to prevent pesticide exposure and mitigate its negative health impacts on young children in agricultural areas of Thailand.
Acknowledgments
This study was supported by the Faculty of Medicine Vajira Hospital and Navamindradhiraj University, Bangkok, Thailand, which fully covered the English language editing service and the article processing charges for the manuscript. The authors would like to express their sincere gratitude to the caregivers of the children who participated in the study and to the staff of the Subdistrict Health Promotion Hospital in Sakon Nakhon, Thailand, for their kind cooperation and support.
Funding
This research was financially supported by the National Research Council of Thailand (grant number N31A650146) and the Faculty of Public Health, Kasetsart University, Chalermphrakiat Sakon Nakhon Province Campus, Thailand.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Quantity and Value of Imports of Hazardous Substances Used in Agriculture, 2019–2021 [Internet]. Bangkok:Office of Agricultural Economics; 2023. Available from: https://www.oae.go.th.
2. Suarez-Lopez JR, Nazeeh N, Kayser G, et al. Residential proximity to greenhouse crops and pesticide exposure (via acetylcholinesterase activity) assessed from childhood through adolescence. Environ Res. 2020;188:109728. doi:10.1016/j.envres.2020.109728
3. Hyland C, Laribi O. Review of take-home pesticide exposure pathway in children living in agricultural areas. Environ Res. 2017;156:559–12. doi:10.1016/j.envres.2017.04.017
4. Buralli R, Nazli SN, Cordoba L, et al. Children’s environmental and occupational exposures to pesticides in low- and middle-income countries rural areas - an elephant in the room. Sci Total Environ. 2025;990:179887. doi:10.1016/j.scitotenv.2025.179887
5. Muenchamnan N, Naksen W, Ong-Artborirak P. A two-pronged educational intervention for caregivers to prevent residential pesticide exposure among Thai young children living in agricultural area. J Multidiscip Healthc. 2023;16:2339–2350. doi:10.2147/JMDH.S422259
6. Curwin BD, Hein MJ, Sanderson WT, et al. Pesticide dose estimates for children of Iowa farmers and non-farmers. Environ Res. 2007;105(3):307–315. doi:10.1016/j.envres.2007.06.001
7. Kunno J, Ong-Artborirak P, Taneepanichskul N, et al. Effect of pyrethroid insecticides exposure in relation to pyrethroid metabolite and GABA concentration of young children, Bangkok Thailand. Hum Ecol Risk Assess. 2019;25:1–14. doi:10.1080/10807039.2019.1615828
8. Siriwat S, Ong-Artborirak P, Ponrachom C, et al. Non-carcinogenic health risk from carbamate pesticide exposure of toddlers living in agricultural areas of Thailand. Int J Environ Health Res. 2023;33:1–11.
9. Siriwat S, Nganchamung T, Ponrachom C, et al. Health risk assessment of dermal exposure to Chlorpyrifos among children in agricultural areas in Sakon Nakhon Province, Thailand. Hum Ecol Risk Assess. 2021;27(9–10):2277–2287. doi:10.1080/10807039.2021.1976102
10. Siriwat S, Rohitrattana J, Nganchamung T, et al. Exposure of chlorpyrifos in toddlers living in an agricultural area in Sakon Nakhon province, North-East Thailand. J Health Res. 2019;33(2):151–161. doi:10.1108/JHR-07-2018-0057
11. Quandt SA, Arcury TA, Rao P, et al. Agricultural and residential pesticides in wipe samples from farmworker family residences in North Carolina and Virginia. Environ Health Perspect. 2004;112(3):382–387. doi:10.1289/ehp.6554
12. Klaimala P, Khunlert P, Chuntib P, et al. Pesticide residues on children’s hands, home indoor surfaces, and drinking water among conventional and organic farmers in Thailand. Environ Monit Assess. 2022;194(6):427. doi:10.1007/s10661-022-10051-6
13. Bravo N, Grimalt JO, Bocca B, et al. Urinary metabolites of organophosphate and pyrethroid pesticides in children from an Italian cohort (PHIME, Trieste). Environ Res. 2019;176:108508. doi:10.1016/j.envres.2019.05.039
14. Coleman B, Asad I, Heng YY, et al. Pesticides and neurodevelopment of children in low and middle-income countries: a systematic review. PLoS One. 2025;20(6):e0324375. doi:10.1371/journal.pone.0324375
15. Buralli RJ, Marques RC, Dórea JG. Pesticide effects on children’s growth and neurodevelopment. Curr Opin Environ Sci Health. 2023;31:100417. doi:10.1016/j.coesh.2022.100417
16. Chen M, Chang CH, Tao L, et al. Residential exposure to pesticide during childhood and childhood cancers: a meta-analysis. Pediatrics. 2015;136(4):719–729. doi:10.1542/peds.2015-0006
17. Van Maele-Fabry G, Gamet-Payrastre L, Lison D. Residential exposure to pesticides as risk factor for childhood and young adult brain tumors: a systematic review and meta-analysis. Environ Int. 2017;106:69–90. doi:10.1016/j.envint.2017.05.018
18. Chaiyamong P, Luangwilai T, Ong-Artborirak P. Symptoms of residential exposure to insecticides and associated factors among young Thai children in urban areas. Children. 2024;11(12):1516. doi:10.3390/children11121516
19. Siriwat S, Wangkahard A, Chuangchaiya S, et al. The application of intervention mapping in developing a parental behavior modification program for pesticide exposure prevention among children in agricultural areas for a sub-district health promotion hospital, Thailand. Int J Environ Rural Dev. 2021;12(2):1–6.
20. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
21. Eldredge LK, Markham CM, Ruiter RAC, Fernández ME, Kok G, Parcel GS. Intervention Mapping: Designing Theory- and Evidence-Based Health Promotion Programs.
22. EQM Research. Test-Mate ChE Cholinesterase Test System (Model 400), Instruction Manual. Cincinnati (OH): EQM Research; 2003.
23. Friedman E, Hazlehurst MF, Loftus C, et al. Residential proximity to greenhouse agriculture and neurobehavioral performance in Ecuadorian children. Int J Hyg Environ Health. 2020;223(1):220–227. doi:10.1016/j.ijheh.2019.08.009
24. Siriwat S, Ong-Artborirak P, Nganchamung T, et al. Health risk assessment of residential exposure to cypermethrin among young children in agricultural communities in northeastern Thailand. Hum Ecol Risk Assess. 2019;25(3):614–623. doi:10.1080/10807039.2018.1539635
25. Farahat TM, Farahat FM, Michael AA. Behavioral-based educational intervention directed toward Egyptian agricultural families to protect children from pesticide exposure. Int Q Community Health Educ. 2008;28(2):97–108. doi:10.2190/IQ.28.2.b
26. Farahat TM, Farahat FM, Michael AA. Evaluation of an educational intervention for farming families to protect their children from pesticide exposure. East Mediterr Health J. 2009;15(1):47–56. doi:10.26719/2009.15.1.47
27. Quandt SA, Grzywacz JG, Talton JW, et al. Evaluating the effectiveness of a lay health promoter-led, community-based participatory pesticide safety intervention with farmworker families. Health Promot Pract. 2013;14(3):425–432. doi:10.1177/1524839912459652
28. Liebman AK, Juárez PM, Leyva C, et al. A pilot program using promotoras de salud to educate farmworker families about the risk from pesticide exposure. J Agromedicine. 2007;12(2):33–43. doi:10.1300/J096v12n02_04
29. Salvatore AL, Chevrier J, Bradman A, et al. A community-based participatory worksite intervention to reduce pesticide exposures to farmworkers and their families. Am J Public Health. 2009;99(Suppl 3):S578–S581. doi:10.2105/AJPH.2008.149146
30. Strong LL, Thompson B, Koepsell TD, et al. Reducing the take-home pathway of pesticide exposure: behavioral outcomes from the Para Niños Saludables study. J Occup Environ Med. 2009;51(8):922–933. doi:10.1097/JOM.0b013e3181ad4995
31. Salvatore AL, Castorina R, Camacho J, et al. Home-based community health worker intervention to reduce pesticide exposures to farmworkers’ children: a randomized-controlled trial. J Expo Sci Environ Epidemiol. 2015;25(6):608–615. doi:10.1038/jes.2015.39
32. Thompson B, Coronado GD, Vigoren EM, et al. Para Niños Saludables: a community intervention trial to reduce organophosphate pesticide exposure in children of farmworkers. Environ Health Perspect. 2008;116(5):687–694. doi:10.1289/ehp.10882
33. Muñoz-Quezada MT, Lucero B, Bradman A, et al. An educational intervention on the risk perception of pesticides exposure and organophosphate metabolites urinary concentrations in rural school children in Maule Region, Chile. Environ Res. 2019;176:108554. doi:10.1016/j.envres.2019.108554
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.