Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
The Effectivity MultiModality Treatment on Rehabilitation Management of Diabetic Foot Disease Patients for Improvement of Clinical Efficacy & Hemorheological Status
Received 7 March 2025
Accepted for publication 18 July 2025
Published 29 July 2025 Volume 2025:18 Pages 2561—2571
DOI https://doi.org/10.2147/DMSO.S526919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Shuo Li,1 Yan Liu,2 Yu Chen3
1Department of Endocrinology, Jinan Third People’s Hospital, Jinan, Shandong, 250132, People’s Republic of China; 2Cardiovascular Department, Jinan Hospital of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 3Public Health Department of Qingdao Fifth People’s Hospital, Qingdao, Shandong, 266002, People’s Republic of China
Correspondence: Yu Chen, Public Health Department of Qingdao Fifth People’s Hospital, Qingdao, Shandong, 266002, People’s Republic of China, Email [email protected]
Objective: To evaluate the effectiveness of a multimodal intervention—comprising rehabilitation management and foot preventive measures—on clinical outcomes, hemorheological parameters, and vascular endothelial function in patients with diabetic foot (DF).
Methods: This retrospective study included 126 DF patients admitted to our hospital from February 2023 to April 2024. Patients were divided into a control group (n = 63, receiving routine nursing care) and an intervention group (n = 63, receiving routine care plus rehabilitation management combined with foot preventive measures). Key outcome measures included: (1) clinical efficacy; (2) hemorheological indicators—whole blood low-shear viscosity (WBLSV), high-shear viscosity (WBHSV), fibrinogen (FIB), and erythrocyte deformability index (EDI); (3) vascular endothelial function indicators—endothelin (ET), basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), and calcitonin gene-related peptide (CGRP); (4) self-management ability—Adult Health Self-Management Scale (AHSMSRS), General Self-Efficacy Scale (GSES); and (5) nursing satisfaction—Newcastle Nursing Service Satisfaction Scale (NSNS).
Results: The intervention group had a significantly higher total treatment efficacy rate (92.06% vs 77.78%, P < 0.05). Post-intervention hemorheological parameters (WBLSV, WBHSV, FIB, EDI) and endothelial markers (ET, bFGF, VEGF, CGRP) showed greater improvement in the intervention group (P < 0.05). Similarly, AHSMSRS scores declined and GSES scores improved more markedly in the intervention group (P < 0.05). Nursing satisfaction was also higher (96.83% vs 71.43%, P < 0.05).
Conclusion: Compared with routine nursing care alone, the multimodal intervention strategy may improve clinical efficacy, hemorheology, endothelial function, self-management capabilities, and patient satisfaction in diabetic foot care. However, these findings should be interpreted with caution given the retrospective design.
Keywords: multimodal intervention, rehabilitation management, foot care, diabetic foot, hemorheology, endothelial function, clinical efficacy
Introduction
Diabetes mellitus (DM) is a common chronic metabolic disease that, when prolonged, can lead to multiple severe complications, among which diabetic foot (DF) is one of the most devastating and difficult-to-heal conditions.1 The occurrence of DF is closely associated with peripheral neuropathy, peripheral vascular disease, and immune dysfunction in the context of chronic hyperglycemia.2 Patients often present with foot ulcers and tissue necrosis, which may ultimately progress to amputation due to infection and inadequate blood supply.3 Studies have shown that the lifetime incidence of foot ulcers in DM patients is as high as 15%–25%,4 and the five-year mortality rate of DF patients is even higher than that of certain malignant tumors. This condition not only severely affects patients’ quality of life but also increases the burden on the healthcare system.5 Therefore, effective prevention and management of DF to improve treatment outcomes and nursing quality has become a major focus of clinical research.
Currently, DF nursing interventions mainly rely on routine nursing management, including blood glucose control, foot hygiene management, wound care, and health education. However, conventional nursing models have certain limitations in improving blood circulation, promoting wound healing, and enhancing self-management ability, making them insufficient to meet the demand for more optimized nursing strategies. In recent years, rehabilitation management and foot preventive measures have been increasingly applied in DF nursing, showing promising prospects in improving patient outcomes. Rehabilitation management, as a comprehensive nursing strategy, encompasses exercise rehabilitation, psychological intervention, nutritional support, and health education, with the core goal of enhancing physical function, improving blood circulation, and increasing disease self-management ability.6,7 Foot preventive measures, on the other hand, involve professional foot care, the proper use of orthotic shoes or insoles, pressure management, and regular check-ups to help reduce the risk of foot injuries, promote ulcer healing, and lower the incidence and recurrence of DF.8,9
Although previous studies have explored individual components of these interventions, comprehensive assessments of their combined effects remain limited.10 Therefore, this study retrospectively analyzed the clinical data of 126 DF patients in our hospital, comparing those who received routine nursing care with those who additionally underwent rehabilitation management combined with foot preventive measures, to explore potential optimization directions for existing DF nursing strategies and provide new insights and guidance for clinical nursing practice.
Subjects and Methods
Study Subjects
A retrospective analysis was conducted on the clinical data of 126 DF patients admitted to our hospital between February 2023 and April 2024. Patients were divided into two groups based on the nursing interventions recorded in their medical files: Control group (n = 63): Received standard nursing care. Intervention group (n = 63): In addition to standard care, received structured rehabilitation management and foot prevention measures, as part of an enhanced care pathway introduced in the hospital’s diabetic foot management program in 2023. The allocation of patients into groups was not randomized; the intervention group comprised patients admitted during periods when the comprehensive nursing program was available or recommended by the multidisciplinary DF care team based on patient needs, willingness, and staffing feasibility. Patients who declined or were deemed less suitable for enhanced interventions due to mild symptoms, resource constraints, or treatment preference remained in standard care. This reflects the real-world implementation characteristics of the program. Although the retrospective design limits the control of confounding variables, this grouping enabled a preliminary assessment of the feasibility and potential benefits of integrated rehabilitation nursing strategies. Inclusion criteria: (1) Met the clinical diagnostic criteria for DF11 and were confirmed as having DF ulcers of Wagner grade 2 or above12 through imaging or clinical examination; (2) Met the clinical diagnostic criteria for T2DM13 with a disease duration of ≥5 years; (3) Aged between 40 and 80 years, regardless of gender; (4) Had chronic foot ulcers or infections with poor healing for at least four weeks; (5) Diagnosed with foot blood supply disorders via ankle-brachial index (ABI) or transcutaneous oxygen pressure (TcPO₂) assessment but not requiring emergency amputation; (6) Had normal cognitive function, were able to cooperate with the nursing interventions in this study, and voluntarily signed the informed consent form; (7) Had no severe coagulation disorders and relatively stable vital signs. Exclusion criteria: (1) Patients with severe acute diabetic complications (such as diabetic ketoacidosis or hyperosmolar nonketotic coma); (2) Patients with severe foot ulcers, infections, or necrosis requiring emergency amputation; (3) Patients with a history of lower limb arterial occlusive diseases (such as severe arteriosclerosis obliterans or deep vein thrombosis) that could affect the study interventions; (4) Patients with severe cardiovascular or cerebrovascular diseases (such as acute myocardial infarction or ischemic/hemorrhagic stroke) who could not tolerate the nursing interventions; (5) Patients with severe liver or kidney dysfunction (such as decompensated liver cirrhosis or end-stage renal disease); (6) Patients with a past or current diagnosis of malignant tumors that could affect DF prognosis; (7) Patients with psychiatric disorders or cognitive impairments who could not comply with the nursing interventions; (8) Pregnant or breastfeeding women; (9) Patients who had received other experimental treatments or nursing interventions for DF within the past three months; (10) Patients with incomplete clinical data or those who discontinued treatment during the intervention period were excluded from the analysis. This study was approved by the Medical Ethics Committee of Qingdao Fifth People’s Hospital. (Approval No.: DXHL0017) and was conducted in strict compliance with the ethical standards of the Declaration of Helsinki.
Nursing Methods
Control Group
Patients in the control group received standardized DF nursing measures, including blood glucose management, basic foot care, wound treatment, and health education, as detailed below: (1) Blood Glucose Management: ① Blood Glucose Monitoring: Daily monitoring of blood glucose levels, adjusting hypoglycemic medications or insulin therapy to maintain stable blood sugar levels. ② Dietary Control: Instructing patients to follow a low-sugar, low-fat, high-fiber diet while controlling total daily carbohydrate intake to prevent large fluctuations in blood glucose. ③ Exercise Recommendations: Encouraging patients to engage in low-intensity exercise (such as walking or Tai Chi) to promote glucose metabolism and blood circulation. (2) Basic Foot Care: ① Foot Hygiene: Advising patients to wash their feet daily with warm water (37°C) and keep the skin dry. ② Toenail Trimming: Guiding patients on proper toenail trimming to avoid cutting them too short or leaving sharp edges. ③ Skin Protection: Recommending the use of moisturizers for dry skin to prevent foot cracks and enhance skin barrier function. (3) Wound Care: ① Wound Disinfection: Cleaning the wound with sterile saline once or twice daily to reduce the risk of bacterial infection. ② Dressing Changes: Selecting appropriate dressings (such as silver ion dressings or alginate dressings) based on wound conditions and regularly replacing them to maintain a clean and moist wound environment. ③ Infection Monitoring: Observing wound healing progress and adjusting treatment plans if signs of redness, increased exudate, or foul odor appear. (4) Health Education: ① Foot Self-Examination: Teaching patients to check their feet daily for injuries, redness, and ulcers, and seek timely medical attention if abnormalities are found. ② Footwear Selection: Recommending breathable, well-fitted shoes and socks to minimize friction and pressure on the feet. ③ Lifestyle Adjustments: Encouraging patients to quit smoking and limit alcohol intake to reduce vascular damage and improve lower limb circulation.
Intervention Group
Patients in the intervention group received systematic rehabilitation management and targeted foot prevention measures in addition to conventional nursing care. The specific measures were as follows: (1) Rehabilitation Management: ① Exercise Rehabilitation: Ankle Pump Exercise: Performed three times daily for 10–15 minutes each session, guiding patients to perform ankle flexion and extension movements in a supine or seated position to promote lower limb blood return and prevent venous stasis. Toe Grasp Training: Using a towel or elastic ball for toe grasp exercises, conducted twice daily for 10 minutes each session, to enhance plantar muscle strength, improve foot stability, and reduce pressure points on the wound. Resistance Training: Incorporating resistance bands or light weights (such as sandbags) for ankle and calf muscle training, performed once daily for 15 minutes to improve lower limb hemodynamics and microcirculation. Walking Training: Under medical supervision, patients gradually resumed low-intensity walking for 20–30 minutes per day to reduce venous return obstruction caused by prolonged sitting, while avoiding excessive walking to prevent foot pressure injuries. ② Physical Therapy: Low-Level Laser Therapy (LLLT): Administered once daily for 15 minutes, irradiating diabetic foot ulcers and surrounding skin to promote local vasodilation and accelerate wound healing. Infrared Therapy: Applied once daily for 20 minutes, targeting the lower limbs and feet to enhance local blood perfusion and improve microvascular permeability. Thermotherapy: Using moist heat compresses (approximately 40°C), applied twice daily for 15 minutes each session, to promote foot blood circulation. ③ Psychological Intervention: Cognitive Behavioral Therapy (CBT): Conducted once a week to help patients correctly understand diabetic foot (DF), enhance self-management confidence, reduce anxiety and depression, and improve adherence to care. Meditation and Relaxation Training: Patients were guided to practice deep breathing and progressive muscle relaxation once daily for 10–15 minutes to alleviate chronic pain associated with diabetes mellitus (DM) and improve psychological endurance. ④ Nutritional Support: High-Protein Diet: Daily intake of high-quality protein (such as fish, egg protein powder, etc) to promote tissue repair and accelerate wound healing. Vitamin and Micronutrient Supplementation: Additional supplementation of vitamin C, vitamin E, zinc, and magnesium to improve vascular health and enhance antioxidant capacity. Personalized Nutrition Plan: Adjusting carbohydrate intake based on patients’ glycemic control to prevent fluctuations that may affect wound healing. (2) Foot Prevention Measures: ① Foot Health Monitoring:
Skin Inspection: Daily examination of foot skin integrity, focusing on ulceration, redness, dryness, or cracks. Neurological Function Assessment: Conducted weekly using a 128 Hz tuning fork to test vibration sense, a pinprick test for pain sensation, and a nylon filament test for plantar pressure sensation to detect diabetic neuropathy at an early stage. Blood Flow Assessment: Performed monthly using the ankle-brachial index (ABI) to evaluate lower limb arterial blood supply, supplemented by Doppler ultrasound if necessary to assess vascular stenosis. ② Pressure Reduction Care: Orthopedic Shoes and Insoles: Providing diabetes-specific shoes to prevent excessive friction and pressure concentration; for high-risk patients with plantar ulcers, customized pressure-relieving insoles were used to reduce localized stress. Silicone Pressure-Relief Pads: For patients with existing foot injuries, silicone pads were applied to reduce pressure around the wound and prevent further deterioration. Negative Pressure Wound Therapy (NPWT): For patients with deep ulcers, negative pressure dressings were used to continuously provide suction, promoting wound healing and enhancing tissue repair. ③ Foot Cleaning and Care: Warm Water Cleansing: Daily foot washing with warm water (37°C) and a mildly acidic foaming cleanser to maintain skin barrier function. Foot Moisturization: Applying urea-based or hyaluronic acid foot cream twice daily to prevent skin cracking and improve skin elasticity. Professional Toenail Trimming: Avoiding self-trimming to prevent cuts or paronychia; toenails were trimmed and cared for regularly by professional nursing staff. ④ Foot Exercise Training: Toe Stretching Exercises: Performed three times daily for 5–10 minutes each session to improve toe flexibility and promote blood circulation. Plantar Fascia Stretching: Conducted twice daily, with each stretch held for 15 seconds in five sets, to reduce foot pain and improve gait stability. Ankle Mobility Training: Performed once daily using circular movements and heel-walking exercises to enhance ankle flexibility and reduce fall risk. Both groups of patients underwent continuous nursing care for one month, after which the effects were evaluated.
Observation Indicators
Clinical Efficacy
Efficacy was assessed based on the improvement in Wagner grading and patient symptoms: Cured: Complete resolution of numbness, tingling, and other symptoms, with full wound healing. Significantly Effective: Ulcer healing rate >60%, with symptoms such as numbness and tingling mostly resolved; Wagner grade decreased by 2 levels. Effective: Ulcer healing rate between 30%-60%, with some improvement in symptoms; Wagner grade decreased by 1 level. Ineffective: No reduction in ulcer size, and no improvement or worsening of clinical symptoms. Total Effective Rate = (Cured + Significantly Effective + Effective) / Total Cases × 100%.
Hemorheological Indicators
Before and after the intervention, 10 mL of fasting venous blood was drawn from the patients’ elbow vein in the early morning. A fully automated hemorheology analyzer (Model: ZL9100, Beijing Zhongchi Weiye Technology Development Co., Ltd., Registration No. Jingxie Guangshen [Wen] 300313–22223) was used to measure whole blood low-shear viscosity (WBLSV), whole blood high-shear viscosity (WBHSV), fibrinogen (FIB), and erythrocyte deformability index (EDI) levels.
Vascular Endothelial Function Indicators
Before and after the intervention, remaining blood samples were centrifuged at 3,000 r/min for 15 minutes to separate serum. Enzyme-linked immunosorbent assay (ELISA) was used to measure levels of endothelin (ET), basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF), and calcitonin gene-related peptide (CGRP). Using commercially available kits from Elabscience Biotechnology Co., Ltd. (Catalog Nos.: E-EL-H6005c, E-EL-H0025, E-EL-H1255c, and E-EL-H0650, respectively; Wuhan, China).
Self-Management Ability Indicators
Before and after the intervention, patients’ self-management ability was assessed using the Adult Health Self-Management Scale (AHSMSRS) (Cronbach’s α = 0.843, validity = 0.822)14 and the General Self-Efficacy Scale (GSES) (Cronbach’s α = 0.861, validity = 0.837).15 AHSMSRS: Evaluates self-management cognition, environment, behavior, and psychological aspects in seven dimensions. Scoring ranges from 1 (disagree) to 3 (fully agree), with higher scores indicating poorer self-management ability. GSES: Includes 20 items covering perception, thinking, action, and compliance. Each item is scored from 1 (completely incorrect) to 4 (completely correct), with higher scores indicating stronger self-efficacy.
Nursing Satisfaction
After the intervention, the Newcastle Satisfaction with Nursing Scale (NSNS) (Cronbach’s α = 0.837, validity = 0.818)16 was used to evaluate patient satisfaction. The scale consists of 19 questions scored using a Likert 5-point system, with higher scores indicating greater satisfaction. Very Satisfied (≥76 points); Satisfied (57–75 points); Neutral (38–56 points); Dissatisfied (<38 points). Total Satisfaction Rate = (Very Satisfied Cases + Satisfied Cases) / Total Cases × 100%.
Statistical Analysis
GraphPad Prism 8 was used for charting, and SPSS 22.0 for data processing. Categorical data were expressed as n (%) and analyzed using χ²-tests. Continuous data were expressed as (eqn and compared using independent sample t-tests between groups and paired t-tests within groups. A P-value <0.05 was considered statistically significant. In addition to p-values, effect sizes (Cohen’s d) and 95% confidence intervals (CI) were calculated for key outcome indicators such as AHSMSRS scores, GSES scores and nursing satisfaction rates to enhance interpretability.
Results
Comparison of Clinical Data
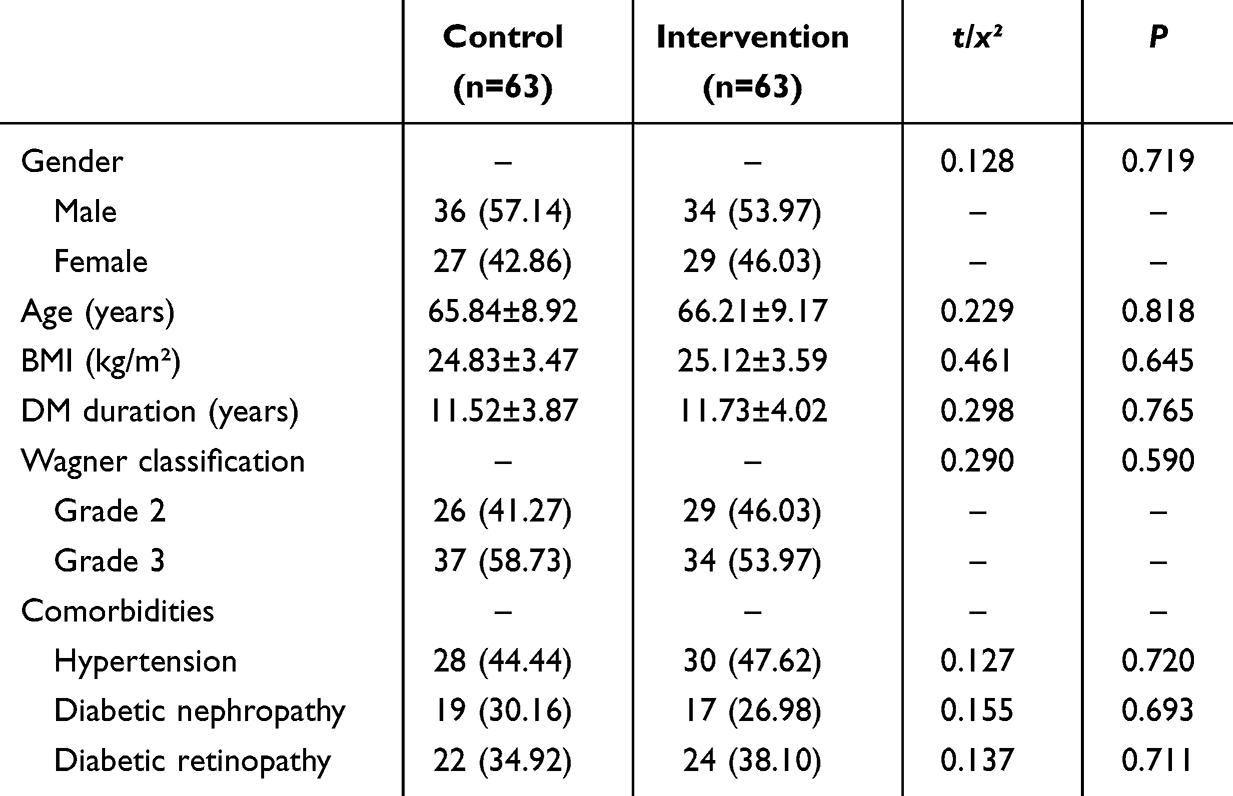
The clinical data, including gender, age, body mass index (BMI), duration of diabetes mellitus (DM), Wagner classification, and comorbidities, were comparable between the two groups (P > 0.05), as shown in Table 1.
 |

Comparison of Clinical Efficacy
Among the 63 patients in the control group, 4 were cured, 10 showed significant improvement, 35 were effective, and 14 were ineffective. In the intervention group, 12 were cured, 19 showed significant improvement, 27 were effective, and 5 were ineffective. The total effective rate in the intervention group (92.06%) was higher than that in the control group (77.78%) (P < 0.05), as shown in Figure 1.
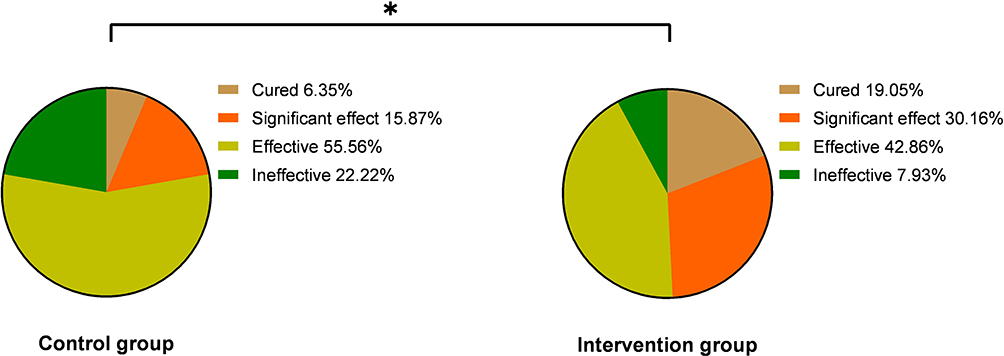 |
Figure 1 Comparison of clinical efficacy [n(%)]. Note: Comparison between groups, *P < 0.05. |
Comparison of Hemorheology Index Levels
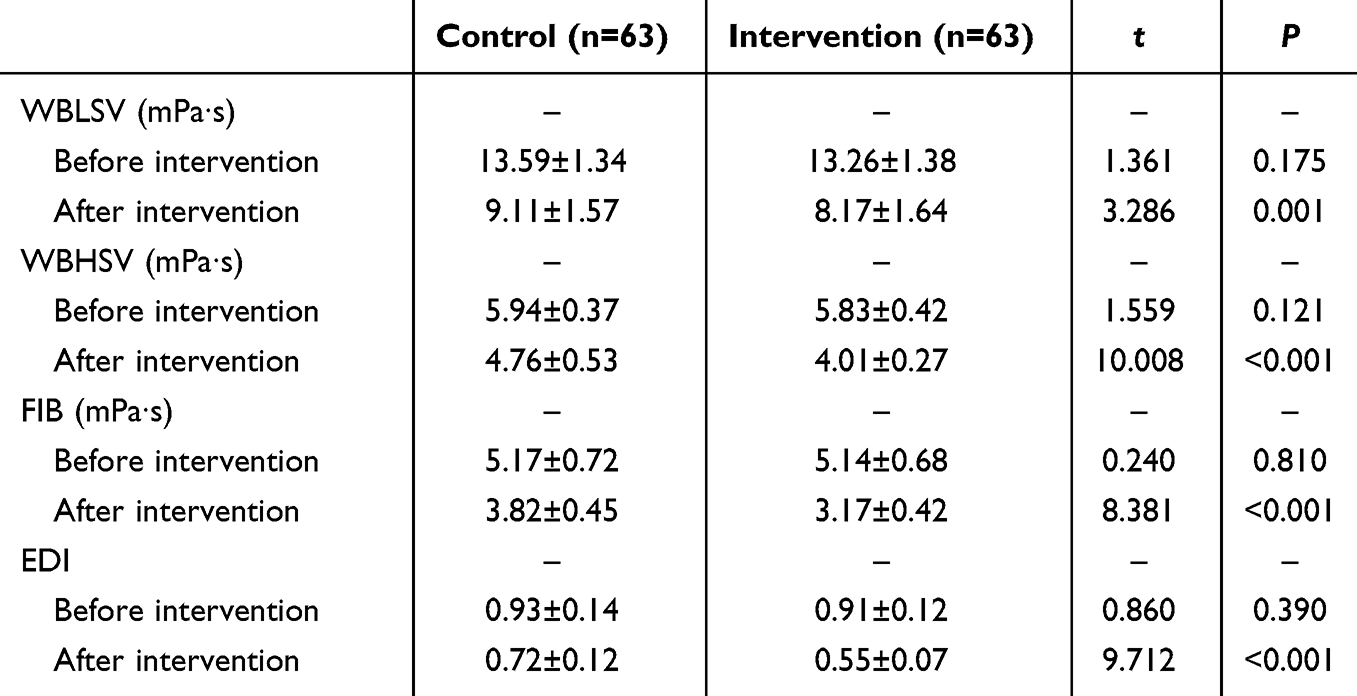
After the intervention, WBLSV, WBHSV, FIB, and EDI levels in both groups decreased compared to before the intervention, with a greater degree of reduction observed in the intervention group (P < 0.05), as shown in Table 2.
 |

Comparison of Vascular Endothelial Function Index Levels
In the control group, ET before and after the intervention was 77.38±5.06 and 60.27±4.25, respectively; bFGF was 31.06±9.43 and 35.41±12.29; VEGF was 83.95±9.27 and 120.16±15.38; CGRP was 19.26±6.42 and 24.37±6.08. In the intervention group, ET before and after the intervention was 77.16±5.12 and 48.13±4.07, respectively; bFGF was 30.89±8.97 and 41.61±11.38; VEGF was 85.43±8.29 and 141.57±15.62; CGRP was 19.21±6.44 and 31.75±6.34. After the intervention, ET levels in both groups decreased compared to before the intervention, while bFGF, VEGF, and CGRP levels increased, with a greater degree of change observed in the intervention group (P < 0.05), as shown in Figure 2.
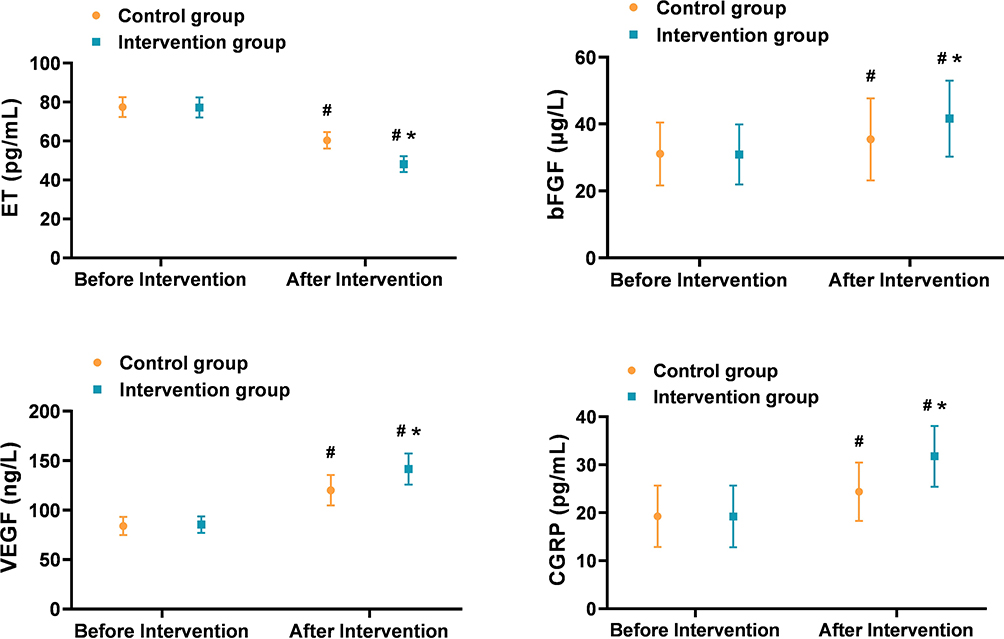 |
Figure 2 Comparison of vascular endothelial function index levels ( Note: Compared with before intervention, #P < 0.05; comparison between groups, *P < 0.05. |

Comparison of Self-Management Ability Index Levels
In the control group, the AHSMSRS score before and after the intervention was 15.06±2.37 and 8.43±1.19, respectively; the GSES score was 24.65±3.74 and 29.31±4.03. In the intervention group, the AHSMSRS score before and after the intervention was 14.58±2.42 and 6.64±1.13, respectively; the GSES score was 24.57±3.92 and 33.48±4.16. After the intervention, AHSMSRS scores in both groups decreased compared to before the intervention, while GSES scores increased, with a greater degree of change observed in the intervention group (P < 0.05), For GSES, the between-group effect size (Cohen’s d) was 1.02 (95% CI: 0.65 to 1.39); for AHSMSRS, Cohen’s d was 1.54 (95% CI: 1.14 to 1.94), indicating large effect sizes for both comparisons, as shown in Figure 3.
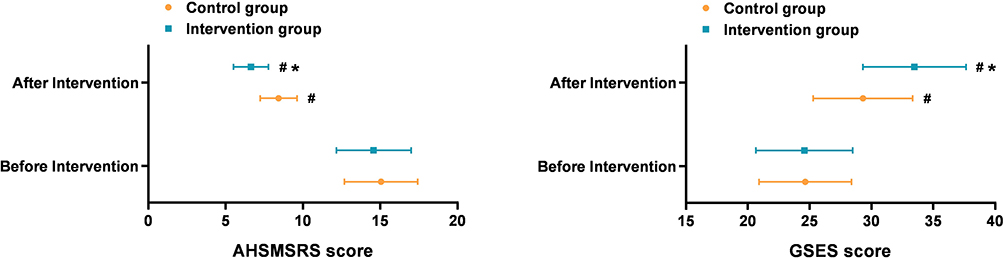 |
Figure 3 Comparison of self-management ability index levels ( Note: Compared with before intervention, #P < 0.05; comparison between groups, *P < 0.05. |

Comparison of Nursing Satisfaction
The total nursing satisfaction in the intervention group was 96.83% (95% CI: 90.21%–99.30%), which was significantly higher than that in the control group 71.43% (95% CI: 59.43%–81.49%) (P < 0.05), as shown in Table 3.
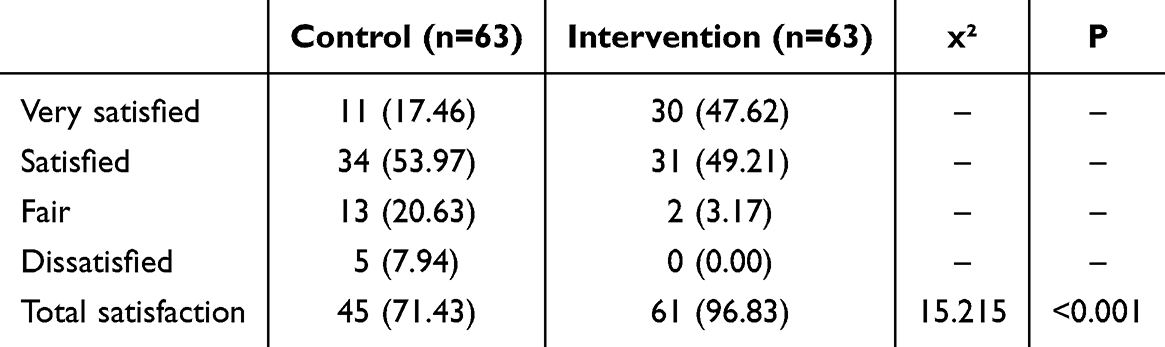 |
Table 3 Comparison of Nursing Satisfaction [n(%)] |
Discussion
DF is one of the most severe chronic complications in DM patients. Its pathological mechanisms involve multiple factors, including diabetic microangiopathy, neuropathy, immune dysfunction, and biomechanical abnormalities, leading to insufficient blood supply to the foot, reduced nerve perception, impaired wound healing, and significantly increased risks of infection and amputation.17,18 Therefore, nursing interventions for DF patients should not only focus on wound treatment but also incorporate strategies to improve blood circulation, regulate metabolism, prevent complications, and enhance patients’ self-management abilities to achieve more comprehensive treatment and rehabilitation goals. The results of this study showed that the overall effective treatment rate in the intervention group was significantly higher than that in the control group (P < 0.05), suggesting that the addition of rehabilitation management combined with foot prevention measures could more effectively promote disease recovery in DF patients. This advantage may be related to the multidimensional mechanism of the additional nursing interventions. First, rehabilitation management supports DF treatment by improving patients’ blood glucose control, nutritional status, and exercise capacity. Second, foot prevention measures emphasize personalized foot care, such as professional wound management, pressure-relief interventions, and foot rehabilitation training, which help reduce foot pressure points, improve local blood supply, and promote tissue repair.19 However, further prospective studies are needed to confirm this relationship.
The occurrence and progression of DF are closely related to abnormalities in hemorheology. Hyperglycemia increases blood viscosity and reduces erythrocyte deformability, thereby affecting microcirculatory perfusion and leading to insufficient blood supply to the foot.20,21 This study found that after intervention, the levels of WBLSV, WBHSV, FIB, and EDI in the intervention group were lower than those in the control group (P < 0.05). The underlying reason is that rehabilitation management combined with foot prevention measures can improve hemorheological status through multiple mechanisms. First, rehabilitation management provides patients with exercise guidance, and moderate physical activity enhances lower limb blood circulation, reduces blood viscosity, increases microvascular permeability, and facilitates oxygen supply to local tissues and the elimination of metabolic waste.22 Second, rehabilitation management regulates patients’ nutritional intake, ensuring a balanced diet with controlled lipid and sugar intake to reduce dyslipidemia, lower blood viscosity, and decrease the risk of thrombosis.23 Furthermore, precise blood glucose control helps reduce the formation of advanced glycation end products, minimize vascular endothelial damage, and optimize vascular function.24 Lastly, foot prevention measures provide professional foot care, and scientific wound care combined with physical therapy (such as negative pressure therapy and red light irradiation) improves local circulation, promotes capillary regeneration, and accelerates wound healing.25 The combined effects of these nursing interventions significantly improved hemorheological indicators in the intervention group, further laying the foundation for DF treatment and recovery.
Studies26 have shown that vascular endothelial dysfunction is common in DF patients, manifested as impaired vasodilation, microcirculatory damage, and reduced angiogenesis capacity. ET is a potent vasoconstrictor, and its reduced levels help improve vasodilation function and enhance local microcirculatory perfusion.27 bFGF and VEGF are crucial growth factors for promoting angiogenesis and tissue repair, and their increased levels accelerate neovascularization and improve tissue ischemia.28 CGRP is a potent neurogenic vasodilator, and its elevated levels further improve neural microcirculation, alleviate neuropathy in DF patients, and enhance lower limb sensory function.29 The results of this study showed that after intervention, ET levels in the intervention group were lower than those in the control group, while bFGF, VEGF, and CGRP levels were significantly higher than those in the control group (P < 0.05). This indicates that rehabilitation management combined with foot prevention measures not only facilitates wound healing but also improves vascular function and reduces the risk of DF complications. This effect is likely associated with exercise training and functional exercises included in rehabilitation management, as moderate physical activity activates endothelial cells and enhances their adaptability to shear stress.30 Studies have shown that physical exercise improves vascular function by increasing nitric oxide (NO) synthesis, reducing oxidative stress, and enhancing endothelial responsiveness.31 Additionally, scientific nursing strategies within foot prevention measures, such as warm water foot baths, massage, and pressure relief, may mitigate long-term hyperglycemia-induced vascular endothelial damage,32 thereby restoring endothelial function, reducing vasoconstriction, and improving local blood supply.
The prevention and management of DF rely not only on medical and nursing interventions but also on patients’ active participation and improved self-management abilities.33,34 The results of this study showed that after intervention, the AHSMSRS score in the intervention group was lower than that in the control group, while the GSES score was higher than that in the control group; additionally, the nursing satisfaction rate in the intervention group was significantly higher than that in the control group (P < 0.05). The possible reason is that rehabilitation management combined with foot prevention measures provides personalized health education, enabling patients to master scientific methods for blood glucose control, foot care, and ulcer prevention, thus enhancing self-management awareness. Psychological counseling and social support interventions improve patients’ disease cognition and self-efficacy, reducing anxiety and dependence. Furthermore, the addition of rehabilitation management combined with foot prevention measures allowed patients in the intervention group to receive more comprehensive nursing care, which may have contributed to the observed improvements in clinical outcomes. The comprehensive effects of these interventions not only enhance patients’ self-care abilities but also improve their satisfaction with nursing services, which is beneficial for the long-term management of DF and the improvement of patients’ quality of life.
Although the results of this study demonstrate the significant advantages of rehabilitation management combined with foot prevention measures in DF care, there are still certain limitations. First, this study is a single-center retrospective study with a relatively limited sample size. Second, the study primarily focused on short-term nursing effects without long-term follow-up. In addition, due to its retrospective design, this study is subject to potential confounding and selection bias. Unmeasured variables such as patients’ socioeconomic status, medication adherence, and lifestyle factors may have influenced the outcomes. Future research should include prospective, multicenter, and long-term studies to validate these findings and improve generalizability.
Conclusion
In conclusion, rehabilitation management combined with foot prevention measures may enhance clinical efficacy in DF patients by improving hemorheology, promoting vascular endothelial function, strengthening self-management ability, and increasing nursing satisfaction. However, the findings should be interpreted with caution due to the retrospective nature of the study, limited sample size, and lack of long-term follow-up. Future prospective or randomized controlled trials are necessary to confirm these results. Moreover, further research is warranted to evaluate the cost-effectiveness, patient adherence, and feasibility of large-scale implementation, which are essential for broader application in clinical nursing practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li W, Liu X, Liu Z, et al. The signaling pathways of selected traditional Chinese medicine prescriptions and their metabolites in the treatment of diabetic cardiomyopathy: a review. Front Pharmacol. 2024;15:1416403. doi:10.3389/fphar.2024.1416403
2. Yu Q, Liu H, Ren BC, et al. The distribution and biomechanical characteristics of foot deformities among elderly diabetic patients based on community screening. Zhonghua Yi Xue Za Zhi. 2024;104(47):4308–4315. doi:10.3760/cma.j.cn112137-20240630-01465
3. Zhu D, Chen Y, Yang CZ, et al. Influencing factors analysis and prediction model establishment of toe-amputation in patients with diabetic foot. Zhonghua Yi Xue Za Zhi. 2025;105(1):63–71. doi:10.3760/cma.j.cn112137-20240814-01866
4. Chinese expert consensus on the endovascular treatment of ischemic lesions in the diabetic foot. Zhonghua Yi Xue Za Zhi. 2023;103(28):2145–2150. doi:10.3760/cma.j.cn112137-20230108-00044
5. Liang J, He Y, Huang C, Ji F, Zhou X, Yin Y. The regulation of selenoproteins in diabetes: a new way to treat diabetes. Curr Pharm Des. 2024;30(20):1541–1547. doi:10.2174/0113816128302667240422110226
6. Aydın E, Ertuğrul MB. The role of rehabilitation in the management of diabetic foot wounds. Turk J Phys Med Rehabil. 2021;67(4):389–398. doi:10.5606/tftrd.2021.8616
7. Ferreira J, Cruvinel Junior RH, Silva EQ, et al. Study protocol for a randomized controlled trial on the effect of the Diabetic Foot Guidance System (SOPeD) for the prevention and treatment of foot musculoskeletal dysfunctions in people with diabetic neuropathy: the FOotCAre (FOCA) trial. I Trials. 2020;21(1):73. doi:10.1186/s13063-019-4017-9
8. Oni D. Foot self-care experiences among patients with diabetes: a systematic review of qualitative studies. Wound Manag Prev. 2020;66(4):16–25. doi:10.25270/wmp.2020.4.1625
9. Chang MC, et al. Orthotic approach to prevention and management of diabetic foot: a narrative review. World J Diabetes. 2022;13(11):912–920. doi:10.4239/wjd.v13.i11.912
10. Qin Q, Oe M, Nakagami G, et al. The effectiveness of a thermography-driven preventive foot care protocol on the recurrence of diabetic foot ulcers in low-medical resource settings: an open-labeled randomized controlled trial. Int J Nurs Stud. 2023;146:104571. doi:10.1016/j.ijnurstu.2023.104571
11. Yue Y, Feng H, Liu P, et al. Progress in clinical diagnosis and treatment of diabetic Charcot neuroarthropathy of foot and ankle. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023;37(11):1438–1443. doi:10.7507/1002-1892.202307068
12. Yang L, Li KL, Pang YX, et al. Clinical effects of free descending branch tissue flap of lateral circumflex femoral artery in repairing Wagner grade 3 or 4 diabetic foot wounds. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2022;38(12):1148–1155. doi:10.3760/cma.j.cn501225-20220321-00076
13. Raveendran AV. Remission of type 2 diabetes mellitus: emerging concepts and proposed diagnostic criteria. World J Methodol. 2024;14(4):95210. doi:10.5662/wjm.v14.i4.95210
14. Ren J, et al. Influencing factors of self-management ability among dry eye patients in west China. Int J Ophthalmol. 2024;17(9):1621–1627. doi:10.18240/ijo.2024.09.07
15. Wu HY, Jin J, Chen C, et al. Effects of three-dimensional quality assessment nursing intervention on efficacy and disease management of patients undergoing esophageal cancer surgery. World J Gastrointest Surg. 2024;16(9):2979–2985. doi:10.4240/wjgs.v16.i9.2979
16. Karadaş A, Ergün S, Kaynak S. Relationship between missed nursing care and patients’ trust in nurses and satisfaction with care: a cross-sectional study. Nurs Health Sci. 2024;26(3):e13149. doi:10.1111/nhs.13149
17. Zhao X, Zhang Y, Yang Y, Pan J. Diabetes-related avoidable hospitalisations and its relationship with primary healthcare resourcing in China: a cross-sectional study from Sichuan Province. Health Soc Care Community. 2022;30(4):e1143–e1156. doi:10.1111/hsc.13522
18. Guo QJ, Ouyang J, Rao JQ, et al. Construction and preliminary validation of a risk prediction model for the recurrence of diabetic foot ulcer in diabetic patients. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2023;39(12):1149–1157. doi:10.3760/cma.j.cn501225-20231101-00166
19. Jan YK, Liao F, Cheing GLY, et al. Differences in skin blood flow oscillations between the plantar and dorsal foot in people with diabetes mellitus and peripheral neuropathy. Microvasc Res. 2019;122:45–51. doi:10.1016/j.mvr.2018.11.002
20. Finžgar M, Frangež HB, Cankar K, et al. Transcutaneous application of the gaseous CO(2) for improvement of the microvascular function in patients with diabetic foot ulcers. Microvasc Res. 2021;133:104100. doi:10.1016/j.mvr.2020.104100
21. Flower RW, Mirza Z, Thom SR. Absolute quantification (mL blood/sec * mm(2) tissue) of normal vs. diabetic foot skin microvascular blood perfusion: feasibility of FM-PPG measurements under clinical conditions. Microvasc Res. 2019;123:58–61. doi:10.1016/j.mvr.2018.12.004
22. Novaković-Bursać S, Talić G, Tomić N, et al. Effect of three-week exercise program on muscle strength and joint mobility in patients with diabetic polyneuropathy: randomized controlled trial. World J Diabetes. 2024;15(12):2311–2321. doi:10.4239/wjd.v15.i12.2311
23. Park S, Jung S, Yoon H. The role of nutritional status in the relationship between diabetes and health-related quality of life. Nutr Res Pract. 2022;16(4):505–516. doi:10.4162/nrp.2022.16.4.505
24. Saintrain MVL, Sandrin RLESP, Bezerra CB, et al. Nutritional assessment of older adults with diabetes mellitus. Diabetes Res Clin Pract. Diabetes Res Clin Practice. 2019;155:107819. doi:10.1016/j.diabres.2019.107819
25. Chen Y, Wu CJ, Duan ZX, et al. Emphasize comprehensive treatment: the cornerstone of the treatment for severe diabetic foot. Zhonghua Yi Xue Za Zhi. 2024;104(47):4279–4283. doi:10.3760/cma.j.cn112137-20241014-02333
26. Zaib S, Ahmad S, Khan I, et al. An evaluation of inflammatory and endothelial dysfunction markers as determinants of peripheral arterial disease in those with diabetes mellitus. Sci Rep. 2024;14(1):15348. doi:10.1038/s41598-024-65188-w
27. Crisologo PA, Davis KE, Ahn J, et al. The infected diabetic foot: can serum biomarkers predict osteomyelitis after hospital discharge for diabetic foot infections? Wound Repair Regen. 2020;28(5):617–622. doi:10.1111/wrr.12836
28. Li T, Huang H, Zhang J. The relationship between the levels of serum VEGF and bFGF and the degree of vascular disease of lower extremities in patients with diabetic foot. Minerva Surg. 2023;78(3):339–341. doi:10.23736/S2724-5691.21.09196-6
29. Tian T, Li H, Zhang S, et al. Characterization of sensory and motor dysfunction and morphological alterations in late stages of type 2 diabetic mice. Front Endocrinol. 2024;15:1374689. doi:10.3389/fendo.2024.1374689
30. Dormer KJ, Gkotsoulias E. The role of hemodynamic shear stress in healing chronic wounds. Wounds. 2022;34(11):254–262. doi:10.25270/wnds/21101
31. Hu QH, Qian YL, Liu XL, Zhu H, Xiao JW. Effects of 12-week Tai Chi exercise on the microvascular reactivity of the middle-aged and elderly patients with mild hypertension and its mechanism. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2021;37(6):683–687. doi:10.12047/j.cjap.6164.2021.080
32. Harithpriya K, Kaussikaa S, Kavyashree S, et al. Pathological insights into cell death pathways in diabetic wound healing. Pathol Res Pract. 2024;264:155715. doi:10.1016/j.prp.2024.155715
33. Oe M, et al. Evaluation of foot ulcer incidence in diabetic patients at a diabetic foot ulcer prevention clinic over a 10-year period. Wound Repair Regen. 2022;30(5):546–552. doi:10.1111/wrr.13039
34. Zhang N, Wang Y, Li W, et al. Association between serum vitamin D level and cardiovascular disease in Chinese patients with type 2 diabetes mellitus: a cross-sectional study. Sci Rep. 2025;15(1):6454. doi:10.1038/s41598-025-90785-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.